Potassium Homeostasis Ch4 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Potassium Homeostasis Ch4 1
2
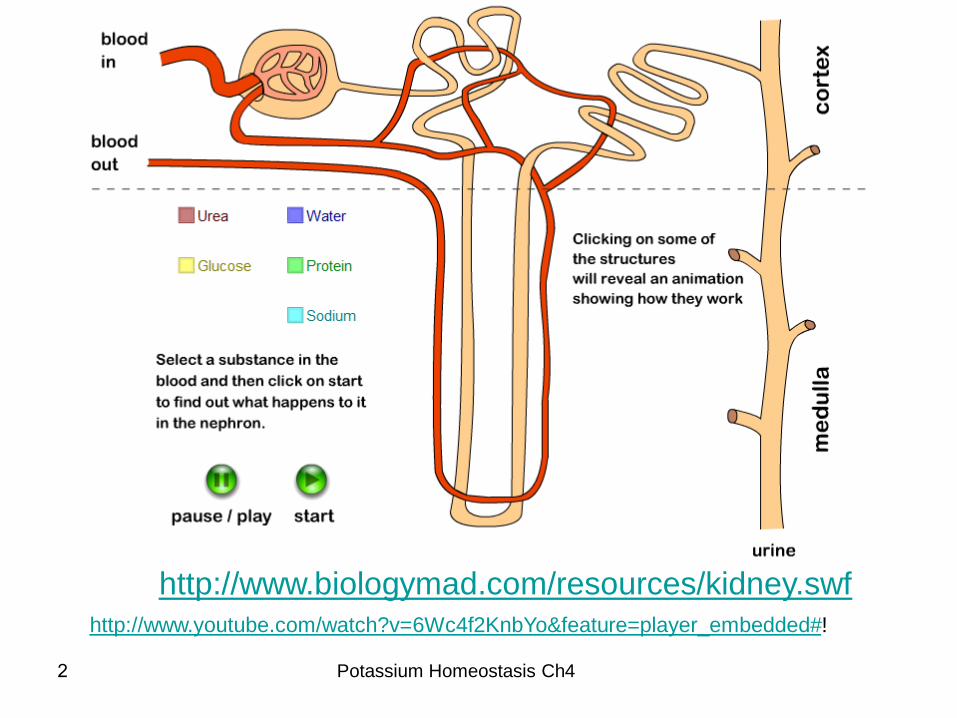
http://www.biologymad.com/resources/kidney.swf
!KnbYo&feature=player_embedded#2f4Wc6http://www.youtube.com/watch?v=
Potassium Homeostasis Ch4

3
ELECTROLYTE BALANCE
• Potassium is the chief intracellular cation
and sodium the chief extracellular cation
• Because the osmotic pressure of the
interstitial space and the ICF are generally
equal, water typically does not enter or
leave the cell
K+
Na+
Potassium Homeostasis Ch4

4
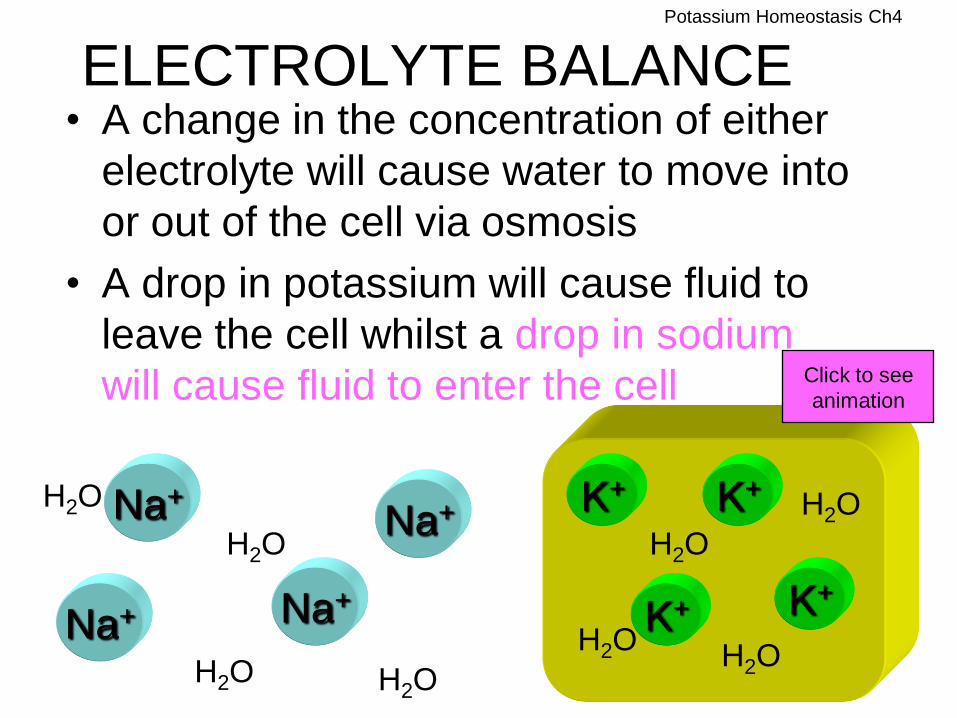
ELECTROLYTE BALANCE • A change in the concentration of either
electrolyte will cause water to move into
or out of the cell via osmosis
• A drop in potassium will cause fluid to
leave the cell whilst a drop in sodium
will cause fluid to enter the cell
K+
H2O
H2O
H2O H2O
H2O
H2O
H2O H2O
K+
K+
K+
Na+
Na+
Na+
Na+
Click to see
animation
Potassium Homeostasis Ch4
5
ELECTROLYTE BALANCE • A change in the concentration of either
electrolyte will cause water to move into
or out of the cell via osmosis
• A drop in potassium will cause fluid to
leave the cell whilst a drop in sodium
will cause fluid to enter the cell
K+
H2O
H2O
H2O H2O
H2O
H2O
H2O H2O
K+
K+
K+
Na+
Na+ Na+
Na+
Click to see
animation
Potassium Homeostasis Ch4

6
Potassium Homeostasis
Potassium is the major intracellular cation
Plasma potassium is about 3.5-5.0 mmol/L.
In tissue cells, its average concentration is 150 mmol/L.
High intracellular concentrations are maintained because K+ diffuses only slowly
outward through the cell membrane, whereas the Na+-K+ ATPase pump continually
transports K+ into the cells.
The body requirement for K+ is satisfied by a dietary intake of 50 to 150 mmol/day.
Potassium absorbed from GIT is rapidly distributed; a small amount is taken up by cells,
but most is excreted by the kidneys.
Potassium filtered through the golmeruli is almost completely reabsorbed in the
proximal tubules and then secreted in the distal tubule.
The amount of K+ excreted in urine varies relative to intake.
The renal secretory system respond immediately to K+ loading with an increase in K+
output
Intracellular stores of K+ maintain the K+ concentration in the extracellular
compartment at a near normal level until K+ depletion is severe.
Potassium Homeostasis Ch4

7
Na+ / K+ Pump • Cells pump K+ ions in and Na+ ions out
of the cell by using sodium-potassium
pumps
Na+
Na+
Na+
Na+
K+
K+
K+
K+
Potassium Homeostasis Ch4
8
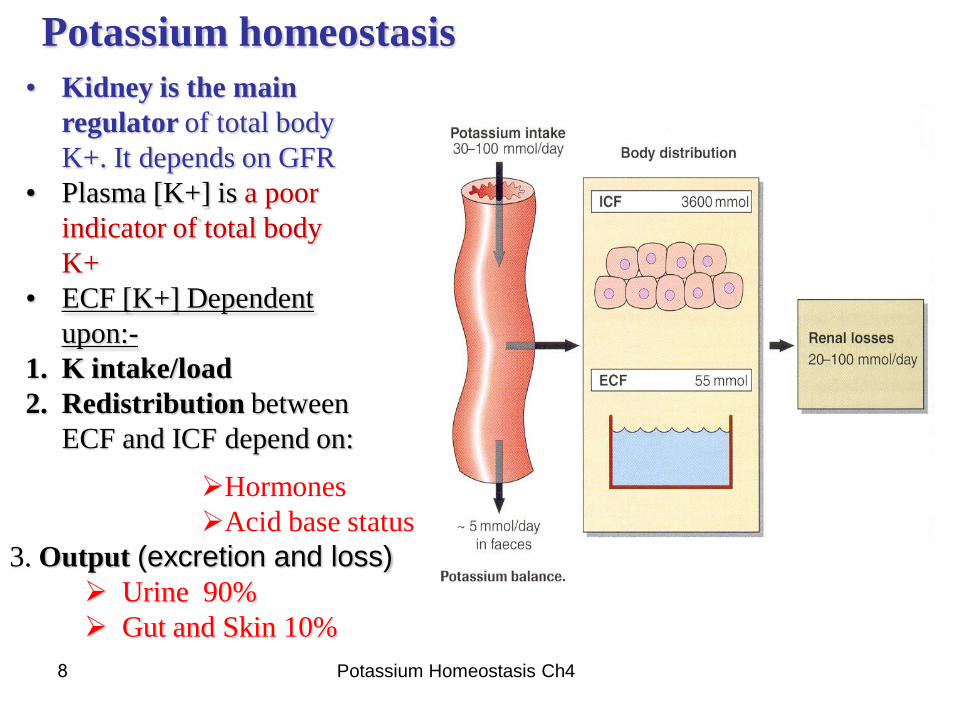
Potassium homeostasis
• Kidney is the main
regulator of total body
K+. It depends on GFR
• Plasma [K+] is a poor
indicator of total body
K+
• ECF [K+] Dependent
upon:-
1. K intake/load
2. Redistribution between
ECF and ICF depend on:
Hormones
Acid base status
3. Output (excretion and loss)
Urine 90%
Gut and Skin 10%
Potassium Homeostasis Ch4

Potassium Homeostasis: 3.5-5.0 mmol/L
ECF [K+] Dependent upon:-
K Intake/Load
Redistribution between ECF and ICF
Output
Excretion & Loss
Urine 90% Gut and Skin 10%
Kidney = Main Regulator of total body K+
Plasma [K+] is a poor indicator of total body K+
Redistribution: ECF and ICF
–Hormones
–Acid base status
–Plasma tonicity
–Plasma [K+]
9 Potassium Homeostasis Ch4

10
Regulation of Potassium Balance • Relative ICF-ECF potassium ion concentration affects a cell’s resting membrane
potential
– Excessive ECF potassium decreases membrane potential
– Too little K+ causes hyperpolarization and nonresponsiveness
• Hyperkalemia and hypokalemia can:
– Disrupt electrical conduction in the heart
– Lead to sudden death
• Hydrogen ions shift in and out of cells
– Leads to corresponding shifts potassium in the opposite direction
– Interferes with activity of excitable cells
– Cellular uptake of potassium is stimulated by insulin
Potassium Homeostasis Ch4

11
Potassium Homeostasis
Urinary potassium excretion depends upon several factors:
* The amount of sodium available for reabsorption in the distal
convoluted tubules and collecting ducts: The active reabsorption of
sodium generates a membrane potential which is ----> neutralised by
the movement of potassium and hydrogen ions from the tubular cells into the
lumen.
* The circulating concentration of aldosterone.
Aldosterone stimulates potassium excretion both :
directly, by increasing active potassium secretion in distal part
of the distal convoluted tubules.
Indirectly, by increasing the active reabsorption of sodium in
the distal convoluted tubules and the collecting ducts,
Potassium Homeostasis Ch4

Potassium Homeostasis Ch4 12
13
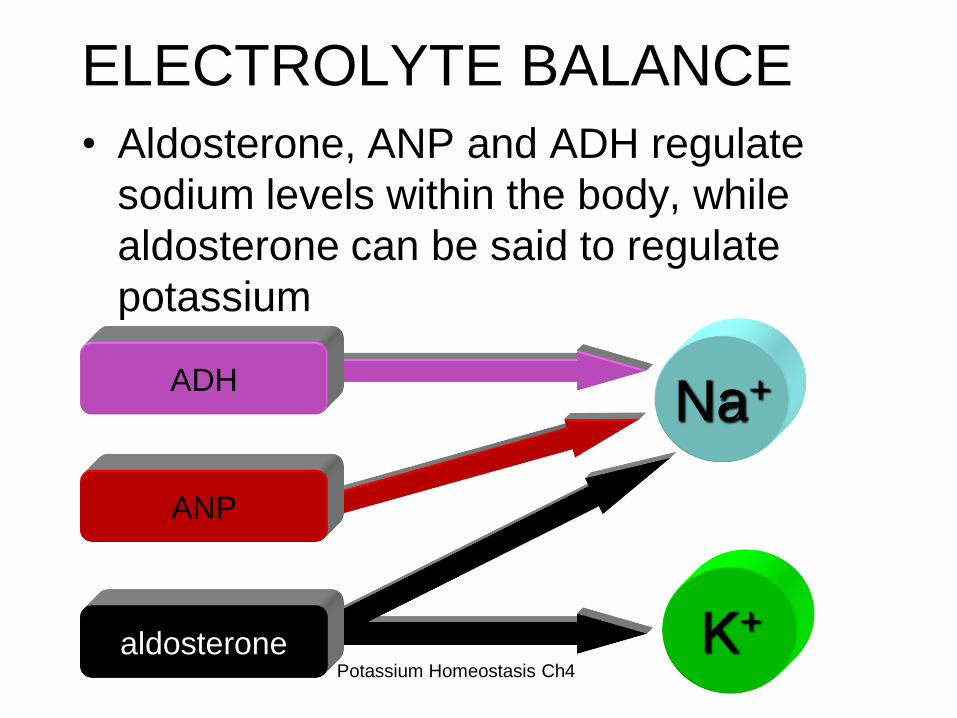
ELECTROLYTE BALANCE
• Aldosterone, ANP and ADH regulate
sodium levels within the body, while
aldosterone can be said to regulate
potassium
K+
Na+
aldosterone
ADH
ANP
Potassium Homeostasis Ch4
14
Potassium Homeostasis
* Disturbances of K+ homeostasis has serious consequences.
* Decrease of extracellular K+ is characterized by:
Clinical features related primarily to disturbances of neuromuscular
function; muscular weakness, constipation and paralytic ileus
(Non mechanical obstruction of the bowel from paralysis of the bowel)
Irritability and paralysis
Fast heart rate and specific conduction effects that are apparent on
electrocardiographic examination
Cardiac arrhythmias.
Plasma K+ levels less than 3.0 mmol/L are associated with marked
neuromuscular symptoms and are evidence of a critical degree of
intracellular depletion.
Potassium Homeostasis Ch4

Factors favouring K+ secretion
Increased intra-cellular K+: High K+ Intake
• Stimulates renal cell uptake and secretion of K+.
• Stimulation of aldosterone secretion.
Increased fluid delivery to lumen causes
increased K+ excretion
– Wash out.
• diuretics
• poorly absorbed anions
• osmotic diuresis
15 Potassium Homeostasis Ch4

16
Factors favouring K+ secretion
The relative availability of hydrogen and potassium ions in the cells of the distal
convoluted tubules and collecting ducts.
Since both hydrogen and potassium ions can neutralise the membrane potential
generated by active sodium reabsorption There is close relationship between
potassium and hydrogen ion homeostasis.
in a state of acidosis, hydrogen ions will tend to be secreted in preference to
potassium;
in alkalosis, fewer hydrogen ions will be available for excretion and there will
be an increase in potassium excretion.
Thus, there is a tendency to hyperkalaemia in acidosis
and to hypokalaemia in alkalosis.
The relationship between the excretion of hydrogen and potassium ions also explains
why potassium depletion tends to produce alkalosis.
If there is insufficient potassium available for excretion as sodium is reabsorbed, then
the excretion of hydrogen ions will be increased.
Potassium Homeostasis Ch4
17
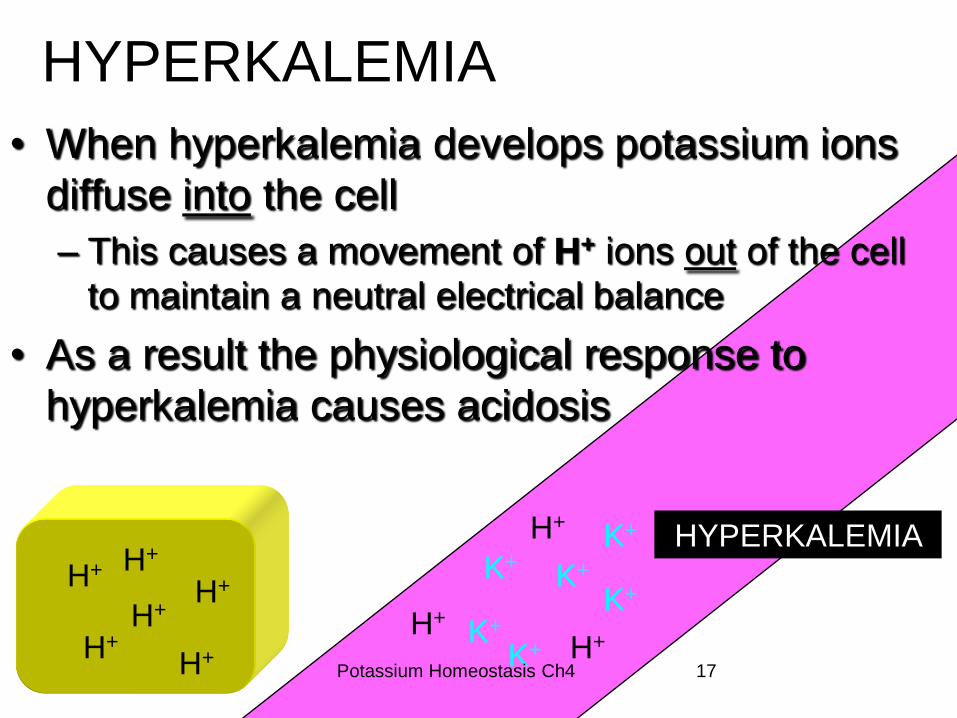
HYPERKALEMIA
• When hyperkalemia develops potassium ions
diffuse into the cell
– This causes a movement of H+ ions out of the cell
to maintain a neutral electrical balance
• As a result the physiological response to
hyperkalemia causes acidosis
K+
K+
K+
K+
K+
K+ H+
H+
H+
H+
H+ H+
H+ H+
H+
HYPERKALEMIA
Potassium Homeostasis Ch4
18
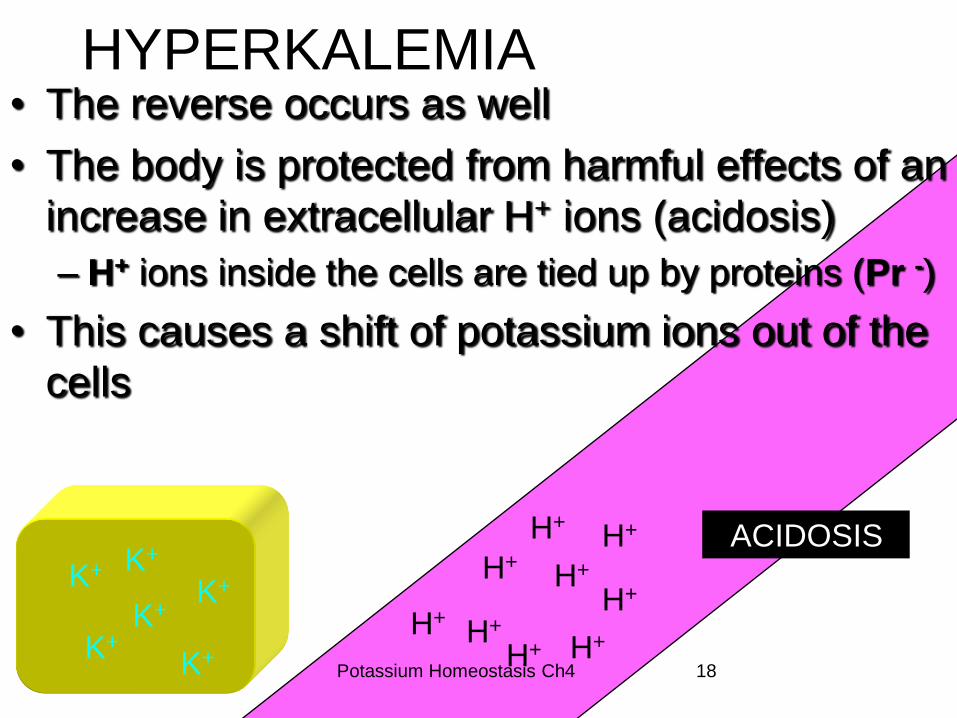
HYPERKALEMIA • The reverse occurs as well
• The body is protected from harmful effects of an
increase in extracellular H+ ions (acidosis)
– H+ ions inside the cells are tied up by proteins (Pr -)
• This causes a shift of potassium ions out of the
cells
H+
H+
H+
H+
H+
H+ H+
H+
H+
K+
K+ K+
K+ K+
K+
ACIDOSIS
Potassium Homeostasis Ch4

POTASIUM DISTRIBUTION
In 70 kg
Intracellular 98%
3430 meq
K content = 50 meq/kg
Total body K = 3500 meq
Extracellular 2%
70 meq
Plasma
20%
15 meq
Na-K ATPase
19 Potassium Homeostasis Ch4

Plasma potassium concentration
Potassium
Intake
Intercompartmental
distribution
Potassium
Excretion
20 Potassium Homeostasis Ch4

HYPOKALAEMIA
(K ion less than 3.5 meq/L)
Causes:
1-Inadequate k intake.
2-Intercompartmental shift of K.
3-Increase k loss.
a. Renal loss
b. Body fluid’s loss
4- Others 21 Potassium Homeostasis Ch4
K+
22
Hypokalaemia
* Causes of hypokalaemia (decreased plasma K+ concentration) can be
grouped into:
1. Decreased intake: Include chronic starvation and
postoperative therapy with K+ poor fluids.
2. Redistribution of extracellular K+ into intracellular fluid: When
insulin therapy of diabetic hyperglycemia starts cellular uptake of
glucose is accompanied by uptake of K+ and water. Hypokalaemia
Hypokalaemia is a feature also of alkalosis, …….where K+ moves from
extracellular fluid into the cell as H+ moves in the opposite direction;
thus, all other things being equal, alkalosis itself causes hypokalaemia.
3. Renal loss of K+ can also be caused by the use of thiazides, loop
diuretics, and chronic anhydrase inhibitors
Renal losses renal tubular acidosis, primary or secondary
aldosteronism, or Cushing’s syndrome Potassium Homeostasis Ch4

23
Hypokalaemia
4. Increased loss of K+ rich body fluids.
Gastrointestinal loss in the case of vomiting, diarrhoea.
5. Other conditions may be associated with low serum K+ levels include
cirrhosis, Conn’s syndrome, and digitalis toxicity.
The effect of hypokalemia
Most of the patients are asymptomatic until K level below 3 meq/L
Cariovascular effects are most prominent
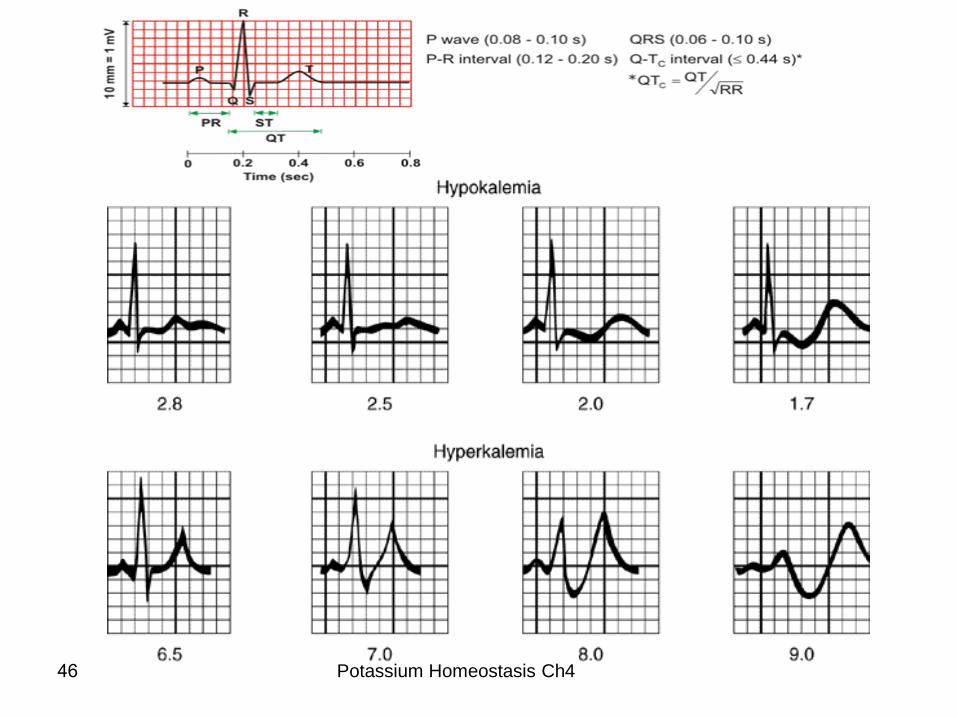
Effect on the ECG
Venticular repolarization is prolonged.
ECG changes include
a prominent U wave.
Potassium Homeostasis Ch4
ventricular The T wave represents
repolarization
24
CELLULAR-EXTRACELLULAR SHIFTS
• Insulin deficiency predisposes an
individual to hyperkalemia
• Cellular uptake of K+ ions is enhanced
by insulin, aldosterone and epinephrine
– Provides protection from extracellular
K+ overload
Insulin K+
K+
K+
K+
K+ K+
Click to view
animation Potassium Homeostasis Ch4
25
ALKALOSIS • Alkalosis causes and is caused by
hypokalemia
• Alkalosis is defined as a decrease of
hydrogen ions or an increase of
bicarbonate in extracellular fluids
– Opposite of acidosis
K+
H+
HCO3-
Potassium Homeostasis Ch4

26
ALKALOSIS
• Alkalosis elicits a compensatory response
causing H+ ions to shift from cells to
extracellular fluids
– This corrects the acid-base
imbalance
HCO3-
HCO3-
HCO3-
HCO3-
HCO3-
HCO3-
H+
H+ H+
H+ H+
H+
H+ H+
Potassium Homeostasis Ch4
27
ALKALOSIS • H+ ions are exchanged for K+
(potassium moves into cells)
– Thus serum concentrations of K+ are
decreased
• And alkalosis causes
hypokalemia
HCO3-
HCO3-
HCO3-
HCO3-
HCO3-
HCO3-
H+
H+ H+
H+ H+
H+
H+ H+
K+ K+
K+
K+
K+
K+
K+
K+
Potassium Homeostasis Ch4
28 Potassium Homeostasis Ch4
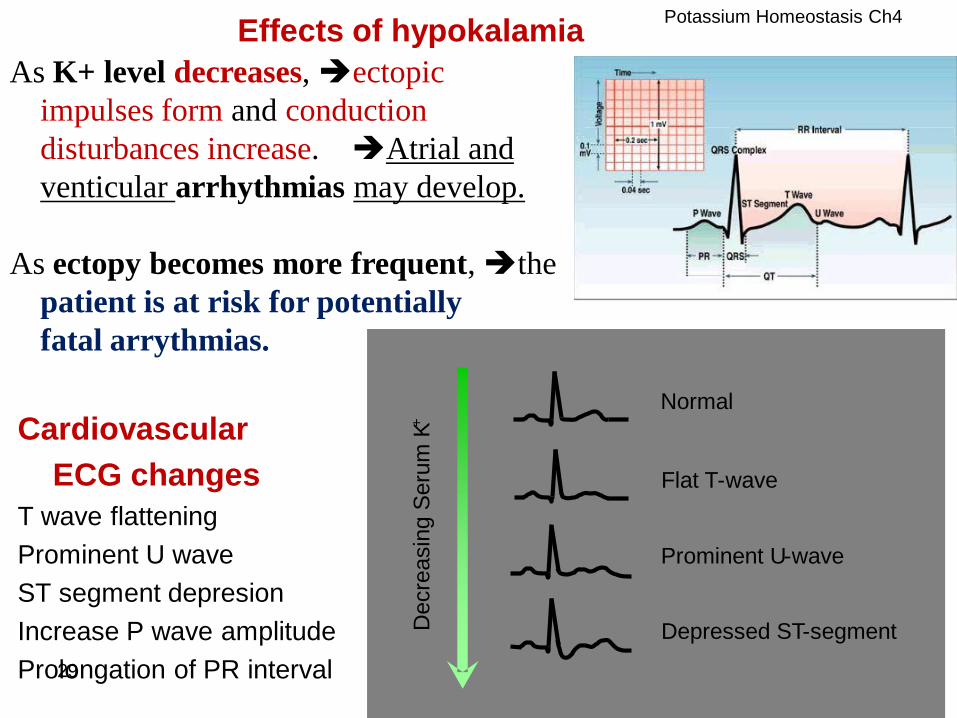
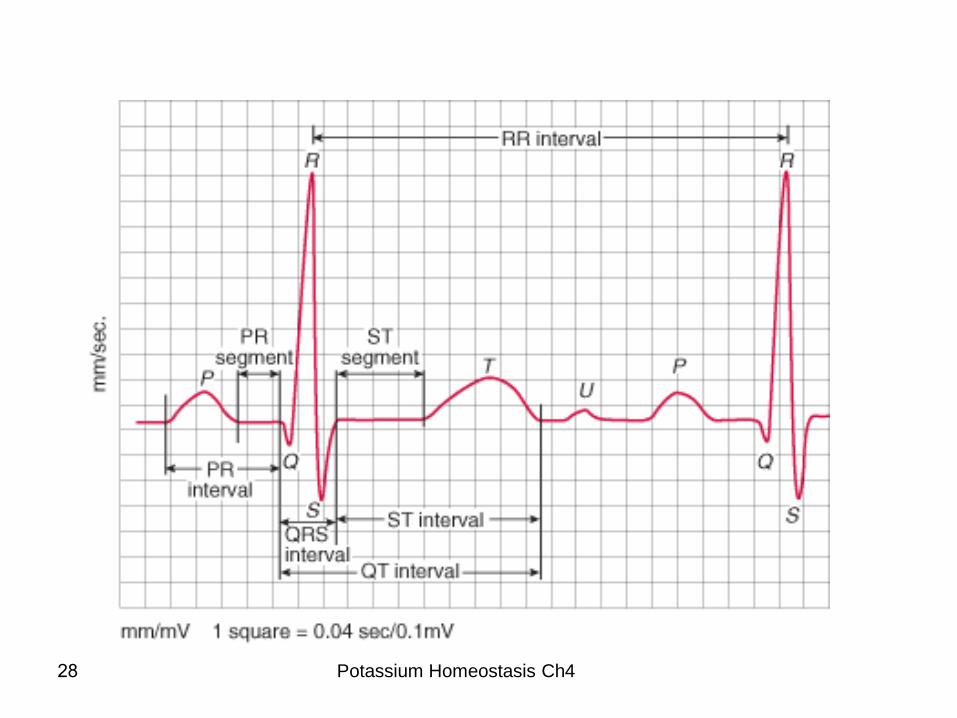
Effects of hypokalamia
Cardiovascular
ECG changes
T wave flattening
Prominent U wave
ST segment depresion
Increase P wave amplitude
Prolongation of PR interval
Prominent U - wave
Flat T - wave
Depressed ST - segment
Normal D
ecre
asin
g S
eru
m K
+
As K+ level decreases, ectopic
impulses form and conduction
disturbances increase. Atrial and
venticular arrhythmias may develop.
As ectopy becomes more frequent, the
patient is at risk for potentially
fatal arrythmias.
29
Potassium Homeostasis Ch4

30
Potassium Homeostasis Ch4
31
Treatment
Is not urgent UNLESS complications
* Oral is preferable to IV therapy
* The K+ shortage is almost entirely from the ICF and since administered
potassium first enters the ECF, replacement must be undertaken with care,
particularly when intravenous route is used.
When treating hypokalaemia, plasma concentrations should be
monitored during treatment.
* If unusually large amounts of potassium are necessary and particularly if
there is impaired renal function, electrocardiograph (ECG)
monitoring is useful since= characteristic changes in the wave form
occur with changing plasma potassium concentrations.
Potassium Homeostasis Ch4

32
HYPERKALEMIA
• Normal serum potassium level
(3.5-5 mmol / liter)
– As compared to Na+ (142 mmol / liter)
• Intracellular levels of potassium
(140-150 mmol / liter)
– This high intracellular level is maintained by
active transport by the sodium-potassium pump
K+ Potassium Homeostasis Ch4
33
HYPERKALEMIA • Hyperkalemia is an elevated serum
potassium (K+) ion level
• A consequence of hyperkalemia is acidosis
– an increase in H+ ions in body fluids
• Changes in either K+ or H+ ion levels
causes a compartmental shift of the other
K+
Potassium Homeostasis Ch4
34
HYPERKALEMIA
• When hyperkalemia develops potassium ions
diffuse into the cell
– This causes a movement of H+ ions out of the cell
to maintain a neutral electrical balance
• As a result the physiological response to
hyperkalemia causes acidosis
K+
K+
K+
K+
K+
K+ H+
H+
H+
H+
H+ H+
H+ H+
H+
HYPERKALEMIA
Potassium Homeostasis Ch4
35
HYPERKALEMIA
• The reverse occurs as well
• The body is protected from harmful effects of an
increase in extracellular H+ ions (acidosis)
– H+ ions inside the cells are tied up by proteins (Pr -)
• This causes a shift of potassium ions out of the cells
H+
H+
H+
H+
H+
H+ H+
H+
H+
K+
K+ K+
K+ K+
K+
ACIDOSIS
Potassium Homeostasis Ch4

36
HYPERKALEMIA • Summarized:
– Hyperkalemia causes acidosis
– Acidosis causes hyperkalemia
HYPERKALEMIA
H+
H+
H+
H+
H+
H+
H+ H+
K+
K+
K+
K+
K+
K+
K+ K+
ACIDOSIS Potassium Homeostasis Ch4
37
HYPERKALEMIA • Summarized:
– Hyperkalemia causes acidosis
– Acidosis causes hyperkalemia
HYPERKALEMIA
H+
H+
H+
H+
H+
H+
H+ H+
K+
K+
K+
K+
K+
K+
K+ K+
ACIDOSIS Potassium Homeostasis Ch4
38
Hyperkalaemia
Increased plasma K+ concentration
It is the commonest and most serious electrolyte emergency encountered in
clinical practice
1. May be precipitated by intravenous infusion of K+ at high rate.
Over treatment is unlikely to produce hyperkalaemia so long as renal
function is normal, because excess K+ is readily excreted in the urine.
2. Transfer of intracellular K+ into extracellular fluid may occur in
cases of dehydration and shock with tissue hypoxia,
diabetic ketoacidosis, thrombocytosis, and in
leukocytosis (damaged cells).
3. Decreased excretion of K+ in acute renal failure or end-stage renal
failure with oliguria or anuria and acidosis
is a common cause of hyperkalaemia. Potassium Homeostasis Ch4

39
Hyperkalaemia
The hyperkalaemia in acidosis is the result of K+ moving from intracellular fluids into
the plasma as H+ moves ….into the cells from extracellular fluid.
Hyperkalaemia occurs along with Na+ depletion in adrenocortical insufficiency,
because in the absence of adequate amounts of aldosterone and other
mineralocorticoids,…. diminished Na+ reabsorption and Na+_K+ exchange
and decreased K+ secretion lead to retention of K+.
Other causes of hyperkalaemia include administration of diuretics that block distal
tubular K+ secretion (e.g., amiloride, triamterene and spironolactone)
Artifactually hyperkalaemia (Pseudohyperkalemia) Movement of K+ out of cells
during or after blood drawing is commonly seen if hemolysis has occurred in
collecting the sample, or there has been a delay in separating the serum from the clotted
blood sample.
Potassium Homeostasis Ch4
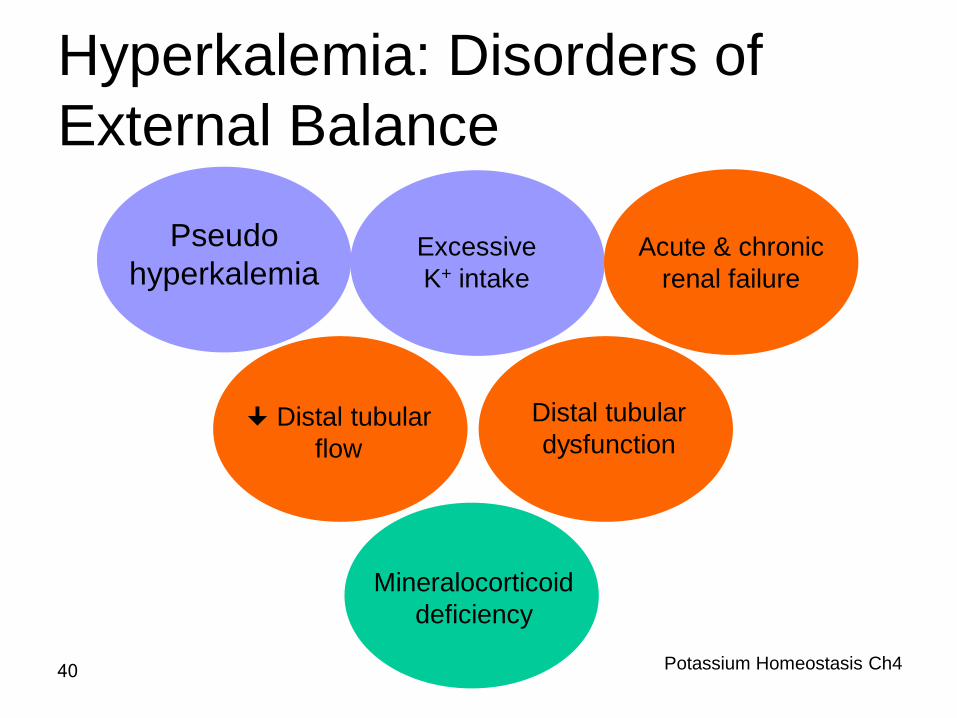
Hyperkalemia: Disorders of
External Balance
Excessive
K+ intake
Distal tubular
flow
Mineralocorticoid
deficiency
Acute & chronic
renal failure
Distal tubular
dysfunction
Pseudo
hyperkalemia
40 Potassium Homeostasis Ch4

Clinical features
• Hyperkalaemia can kill without warning
It lowers the resting membrane potential
Shortens the cardiac action potential and
Increases the speed of repolarization.
Cardiac arrest with ventricular fibrillation
(condition in which there is
uncoordinated contraction of the
cardiac muscle of the ventricles
in the heart, making them tremble
rather than contract properly)
may be the
first sign of hyperkalaemia.
Characteristic ECG changes precede the onset of
ventricular fibrillation.
Potassium Homeostasis Ch4
41
42
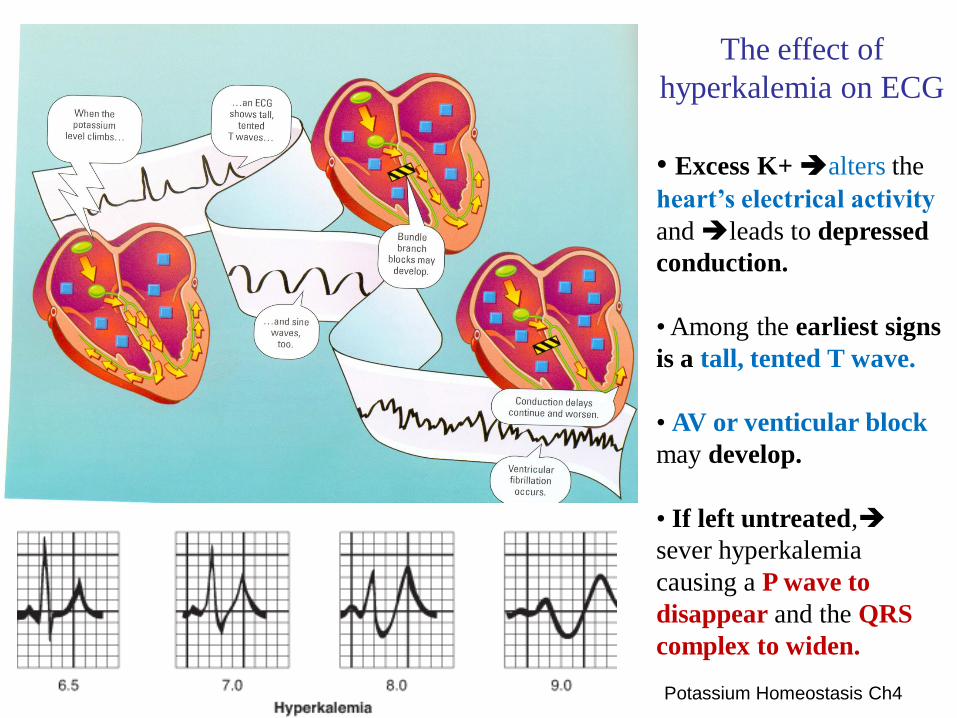
The effect of
hyperkalemia on ECG
• Excess K+ alters the
heart’s electrical activity
and leads to depressed
conduction.
• Among the earliest signs
is a tall, tented T wave.
• AV or venticular block
may develop.
• If left untreated,
sever hyperkalemia
causing a P wave to
disappear and the QRS
complex to widen.
Potassium Homeostasis Ch4
43
Management
* Treatment is URGENT if K > 7.0 mmol/L
* Intravenous calcium gluconate (10 ml of a 10% solution, given over one minute
and repeated as necessary) affords some degree of immediate protection to the
myocardium by antagonizing the effect of hyperkalaemia on myocardial
excitability.
* Intravenous glucose and insulin promotes intracellular potassium uptake.
* Salbutamol, which activates Na+-K+ ATPase, has similar effect.
* In the acidic patient, hyperkalaemia can be controlled temporarily by bicarbonate
infusion.
* When there is slow rise in the plasma potassium this may be stopped or reversed
by oral administration of a cation exchange resin such as Resonium A.
* ECG monitoring can be valuable in patients with hyperkalaemia. Changes in
the plasma potassium concentration are reflected by changes in the ECG wave
form more rapidly than could be determined by biochemical measurements.
Potassium Homeostasis Ch4
Laboratory assessment of potassium
Proper collection and handling of samples for K analysis is extremely importantbecause there are many causes of artfactual hyperkalemia:
1. The coagulation process releases K from platelets, so that serum K may be 0.1-0.5 mmol/L higher than plasma K concentrations. If the patient’s platelet count is elevated, serum K may be further elevated.
2. If a tourniquet is left on the arm too long during blood collection or if patients excessively clench their fists or otherwise exercise their forearms before venipuncture, cells may release K into the plasma.
The first situation may be avoided by using heparinized tube to prevent clotting of specimen and the second by using proper care in the drawing of blood.
3. storing blood on ice promotes the release of K from cells, whole blood samples for K determinations should be stored at room temp. (never iced) and analyzed promptly or centrifuged to remove cells.
4. If hemolysis occurs after the blood is drawn, K may be falsely elevated-the most common cause of artifactual hyperkalemia.
44
Potassium Homeostasis Ch4

Specimens • Serum, heparinised plasma, and urine (24 hr).
• Hemolysis must be avoided because of high K+ content of
erythrocytes
• Urine specimens should be collected over 24-hour period to
eliminate the influence of diurnal variations.
• Potassium is determined electrochemically with an ion-selective
electrode (ISE) or by flame emission spectrophotometry (FES).
Reference intervals
The interval for serum K+ is 3.4 to 5 mmol/L from infancy
throughout life.
45 Potassium Homeostasis Ch4
Potassium Homeostasis Ch4 46
Related Documents











