DR.TARIG MAHMOUD MD SUDAN HAIL UNIVERSITY KSA Post partum collapse

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
DR.TARIG MAHMOUD
MD SUDAN
HAIL UNIVERSITY KSA
Post partum collapse
Maternal collapse is defined as an acute event involving the cardiorespiratory systems and/or brain, resulting in a reduced or absent conscious level (and potentially death).
causes
Shock- eg postpartum haemorrhage.
Pulmonary embolus
Amniotic fluid embolus
Cardiac causes
Intracranial events
Drug overdose/toxicity
Biochemical causes –e.g. hypoglycaemia

Primary PPH Secondary PPH
Loss of MORE than or EQUAL to 500mL blood from the genital tract within 24 hours of delivery
Loss of MORE than or EQUAL to 500mL blood from the genital tract between 24 hours and 12 weeks post delivery
Postpartum haemorrhage

PPH CAUSES:
1.Uterine atony
2.Retained placenta
3.Genital tract laceration
4.Coagulopathy
5.Acute inversion of uterus
REMEMBER
4“T”s
Uterine atony
Retained placenta and/ormembranes
Clotting disorder
Tone
Tissue
Trauma
Thrombin
Injury to vagina, perineum and uterine tears at C/S
1.Uterine atony
Predisposing conditions:
Multiparity.
Over distension of uterus (Macrosomia,polyhydramnios).
Prolong labour (uterine inertia).
Fibroid.
Placenta previa.
Oxytocin induce labour.

2.Retained placenta
Prevent a uterus from contracting .
Causes:
Placenta separated but undelivered.
Placenta partly or wholly attached.
Placenta accreta.

3.Genital tract laceration
Perineal or vaginal tears.
Causes:
Instrumental delivery (Cervical & vaginal tears).
Extension of episiotomy .
Uterine rupture.

4.Coagulopathy
Causes:
Von Willebrand's Disease, Platelet disorder.
Placenta abruption (retro placental clot leadsto consumption of clotting factors).
Unidentified dead fetus.
Amniotic fluid embolus (amniotic fluidentering maternal circulation)

5.Acute inversion of uterus
Caused by traction on the umbilical cord before placenta has separated.
Associated factors:
-Fundal placenta
-Short cord
-Morbidly adherent placenta
Lead to Cardiovascular collapse & shock.

Mangment of PPH
ABC (fluid resuscitation).
Feel abdomen-uterus poorly contracted rub the fundus gently (see wether uterus contract and bleeding arrested).
Set up IV line & IV infusion of 40 units of syntocinon.
Bimanual compression
potent drugs can also be used these include ergometrine, prostaglandin F2α or misoprostol.
The bladder should be catheterized as an empty bladder aids uterine contraction.
Send blood for group and cross matching. Examine placenta to see if it is complete(If
uncompleted, sent to theatre for manual remove).
If complete(Examine vagina and cervix in lithotomy position for laceration)
No laceration(allow further measures (eg. uterine tamponade,radioloical occlusion)
Exploratory Laporotomy(iliac artery ligation) or B lynch (sutures which are placed in double loop surround the uterus & aim to squeeze whole uterus) .
Hysterectomy correction of clotting factors using fresh frozen
plasma, platelets and cryoprecipitate.

Bimanual compression
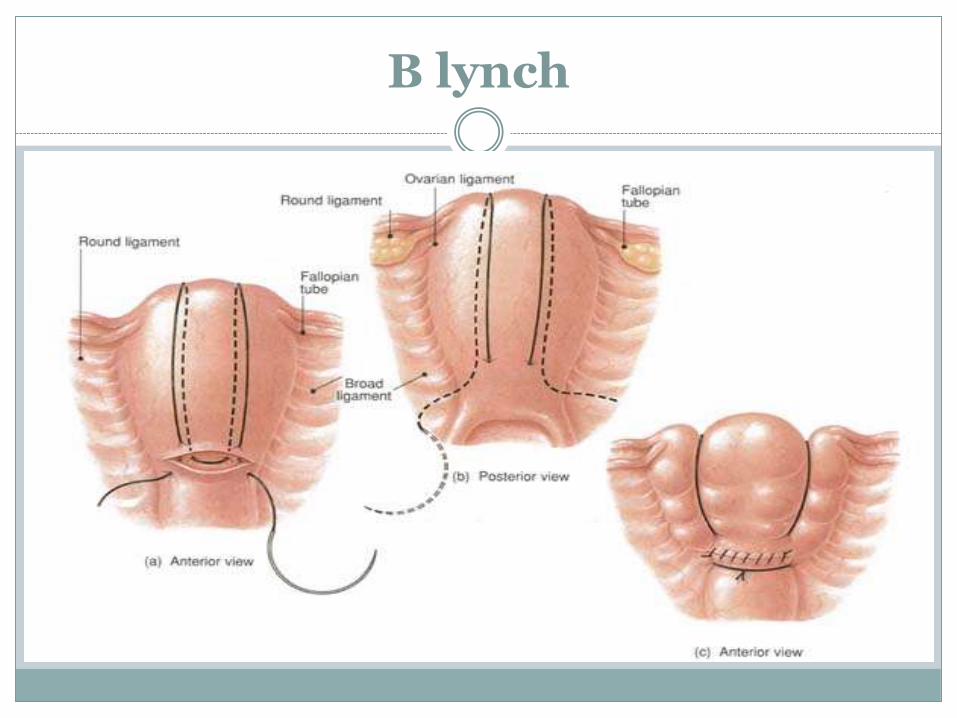
B lynch

Pulmonary embolism
Thrombosis is the most common cause ofmaternal death in the UK.
The most common presentation is of mildbreathlessness, or inspiratory chest pain, in awoman who is not cyanosed but may beslightly tachycardic (90 bpm) with a mildpyrexia (37.5ºC).
massive PE may present with suddencardiorespiratory collapse.
Diagnosis and management:
o PE can be a cause of sudden cardiorespiratorycollapse.
o In this situation, diagnosis and managementshould occur simultaneously.
o Urgent resuscitation using the structured ABCapproach is needed.
o If PE is suspected, anticoagulation should beinstituted.

Amniotic fluid embolism
caused by amniotic fluid entering the maternal circulation.
This causes acute cardiorespiratory compromise and severe DIC.
Difficult to diagnose in life, and is typically diagnosed at postmortem, with the presence of fetal cells (squames or hair) in the maternal pulmonary capillaries.
Diagnosis and management:
Symptoms occurring just before the collapse may be helpful in diagnosis.
• breathlessness.
• chest pain.
• feeling cold.
• lightheadedness.
• restlessness, distress and panic.
• pins and needles in the fingers.
• nausea and vomiting.

The prognosis is poor, with around 30 per cent of patients dying in the first hour and only 10 per cent surviving overall.
Management is supportive, requiring intensive care and there are no specific therapies available.

Cardiac causes
The main cardiac events are myocardial infarction, aortic dissection and cardiomyopathy.
signs and symptoms such as central chest or interscapular pain, a wide pulse pressure, and a new cardiac murmur.
Management by ABC approach and seek help of cardiologist.

Intracranial events
Intracranial haemorrhage is complication of uncontrolled hypertension, but can also result from ruptured aneurysms and arteriovenous malformations.
severe headache often precedes maternal collapse.
Drug overdose/toxicity
In obstetric practice, the two main drugs that can give rise to overdose or toxic problems are magnesium sulphate and local anaesthetic agents.
The antidote to magnesium toxicity is 10 ml 10% calcium gluconate given I.V .
Intralipid 20%should be used in cases of collapse secondary to local anaesthetic toxicity.

Thank You for
Related Documents











