8/5/2020 1 Post-Operative Care for Cardiac Defects By Laura Curl RN Objectives • Discuss physiology of coarctation of the aorta (CoA), Tetrology of Fallot (TOF) and hypoplastic heart syndrome (HLHS). • Determine the pre-operative monitoring of cardiac defects. • Describe surgical repairs for the coarctation of the CoA, TOF, and HLHS. • Recognize post-operative considerations when caring for children with congenital heart surgery. 1 2

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
8/5/2020
1
Post-Operative Care for Cardiac Defects
By Laura Curl RN
Objectives
• Discuss physiology of coarctation of the aorta (CoA), Tetrologyof Fallot (TOF) and hypoplastic heart syndrome (HLHS).
• Determine the pre-operative monitoring of cardiac defects.
• Describe surgical repairs for the coarctation of the CoA, TOF, and HLHS.
• Recognize post-operative considerations when caring for
children with congenital heart surgery.
1
2
8/5/2020
2
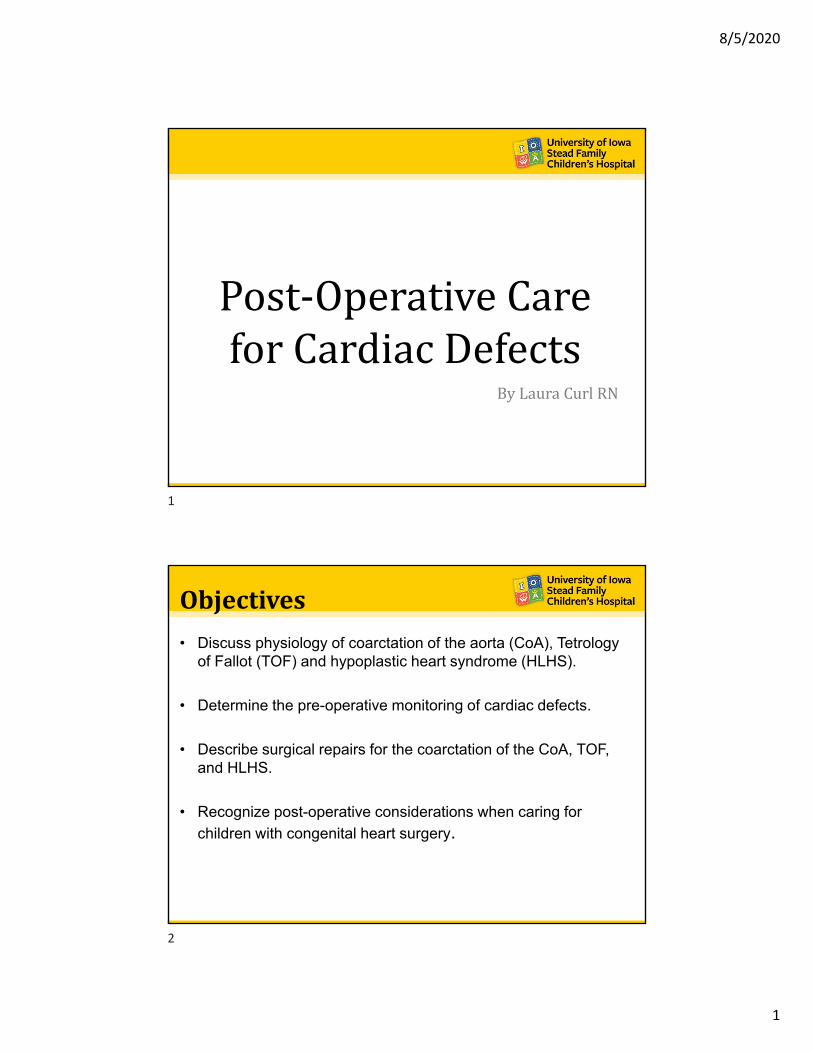
CoarctationoftheAorta
• Narrowing of the aorta– “Speed bump”
– Left ventricle works hard to “pump across bump”
• Left ventricular hypertrophy
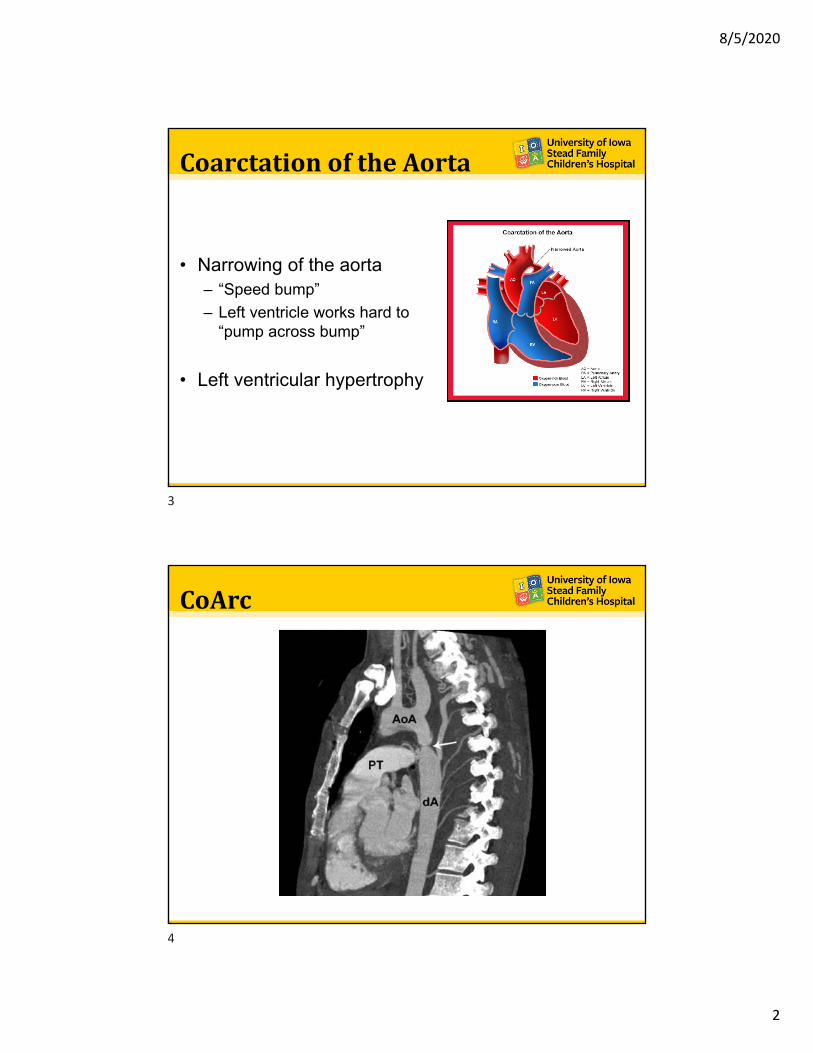
CoArc
3
4

8/5/2020
3
NewbornPre‐OperativeCare• Some coarcs are not found until the child gets older
– Ex. Child has school physical and murmur is found
• 4 pt blood pressures– New newborn screening– Can have decreased pulses and circulation
• Alprostadil (prostaglandins) are used to increase pulmonary blood flow and alternatively decreased the amount of blood flow back to the heart
• PGE also helps left ventricle by off loading blood flow by diversion across the PDA
SurgicalRepair
• End to end anastomosis
• Flap repair
– Large coarc
• Balloon Angioplasty
5
6

8/5/2020
4
Post‐OperativeCare• Left ventricle continues to pump hard (no one tells it to chill out
after coming out of the OR)
• Needs time to remold
– Amount of time depends on how long the coarc has been there
• Pt will need antihypertensives
1. Nipride with Sodium Thiosulfate (*byproduct of breakdown is cyanide)
2. Phentolamine
3. Nicardipine
Post‐OperativeCareCont.
• Arterial Lines
– Upper and lower extremity
– To monitor the gradient across the surgical site
– Gradient may still be there post-op but should lessen
• NPO
– Digestive organs need to get used to the new flow of blood
– Have been used to “living” in a decreased blood flow state
– If fed to soon may have a reperfusion injury
– NPO status determined usually by TCV
7
8

8/5/2020
5
TetralogyofFallot• Tetra, Meaning “4”
1. VSD2. Pulmonary Stenosis3. Overriding Aorta4. Right ventricle
hypertrophy
• Pink or Blue Tets– Depends on the degree
of pulmonary stenosis
Pre‐OperativeCare
• Cyanotic or “blue” tetsrequire PGE
• Babe too small– BT Shunt then home to
grow
– Repair @ 4-6 months
BT Shunt
9
10

8/5/2020
6
Pre‐OperativeCareCont.• Tet Spells
– Cyanotic spells that occur with
• Extreme crying
• Stress
• Dehydration
• Fever
– Pulmonary beds clamp down causing worsening right to left shunting across VSD
– Treatment
• Calm patient
• Give O2
• Sedation
– “These babes are spoiled”
Repair
• VSD Closure– Fixes overriding aorta
• Repair pulmonary stenosis
• Right ventricle will remold over time
11
12

8/5/2020
7
Post‐OperativeCare
• May need anti-hypertensives
• Give O2 to help dilate pulmonary bed
• May show signs of pulmonary hypertension – Right ventricle pumping hard– Pre-Op “speed bumps” causes increased lung pressure
• Good pain control
• Babe can still have “Tet spells”
SingleVentricles• Hypoplastic Left Heart Syndrome
– Hypoplastic left ventricle, open PDA, hypoplastic aorta, ASD
• Hypoplastic Right Heart Syndrome
– Hypoplastic right ventricle, open PDA, pulmonary atresia, ASD
– Better prognosis than hypoplastic left
13
14

8/5/2020
8
SingleVentricles• Can be caused by numerous defects
• Babes with defect may seem normal until the PDA closes
• Alprostadil (Prostaglandins)– Can cause increased body temp and apnea– May need intubated to control breathing, saturations and apnea
• PVR high and systemic resistance low– Prevents pulmonary overcirculation which in turn causes decreased systemic
circulation (as shown by BP)
• DO NOT NEED O2– Oxygen floods the lungs and decreases PVR which steals blood from the systemic
blood flow (as shown by BP)– To keep PVR increased- keep O2 sats between 75-85%
• May need sedated and paralyzed– ↑RR > ↑Sats > ↓ PVR
Repair:FirstStageSurgery
BT Shunt– Blalock Taussig Shunt
– Movie on HBO & Youtube: “Something the Lord Made”
– Gortex tube sown between R subclavian to pulmonary artery
– Mostly seen in hypoplastic right
15
16

8/5/2020
9
Repair:FirstStageSurgeryNorwood with Sano
– Used in hypoplastic left when arch is compromised
– Norwood• Rebuild the arch• The main PA is used to rebuild the arch• Pulmonary blood flow is established
through the sano
– Sano Shunt• Central shunt• Gortex tube from RV to PA• Preferred d/t higher velocity flow• “Less likely to clot”
NorwoodPost‐operativeCare• Rule of 40’s
– MAP = 40’s (good cardiac output)– SVO2= 40’s– pH= 7.40 (Balance pulmonary flow)– HCT= 40’s (Trucks to deliver O2)
• Will come back with an open chest• Use decreased O2 content• Keep BP under control
– Lots of little sutures on that rebuilt arch!• Maintain good shunt flow by maintaining
good cardiac output• Will be paralyzed and sedated• To weigh pt or not to weight open chest
pt → That is the question!
17
18

8/5/2020
10
Repair:SecondStageSurgery
Bidirectional Glenn• Completed around 4-6 months old
• SVC connected to the R branch PA
• Blue blood flows directly from head, neck into the lungs– Think of it as a waterfall! Gravity and
thoracic pressure helps to return blood to the heart
• All blood flow is passive now
• Extubation is key to a “happy” Glenn
SecondStage:PostoperativeCare
• Head and neck will be edematous
• Bluish tint to head= venous congestion
• Glenn Headache– From increased ICP patient was not
used to
• Pt very irritable and difficult to console– Crying clamps down pulmonary
bed, ↓ blood flow to lungs, ↑ ICP
• Give O2 to open pulmonary beds to increase forward flow for a “happy” Glenn
19
20

8/5/2020
11
GlennPostoperativeCare
• Anticoagulation
• Good pain control
• HOB elevated
• Quiet/dark room
• Low stimulation
• Sedation
• “Mama Bear” your patient
Repair:ThirdStageSurgery
• Fontan Procedure– Extra cardiac fenestrated
Fontan– Done ~2 years old, maybe
sooner– Gortex conduit from IVC
which is sown to right pulmonary artery branch under the Glenn
– Fenestration • Small opening from conduit
to RA• Acts as a “pop off” valve to
allow for cardiac output when pulmonary pressures is increased
21
22

8/5/2020
12
FontanPostoperativeCare
• CVPs of mid teens to 20’s– Needed to help “push” blood to
lungs. Passive flow return
• ALL blood flow passive to the lungs now
• EXTUBATE!
• Give O2
• Anticoagulation therapy
• If PVR remains high– Blood can back up in the liver and
ascites
• At risk for chylo, monitor chest tube output closely
ChestTubeCare• Need to see the site
• Transparent dressing after operative dressing removed by TCV
• Mark with a black mark to watch position
• If the dressing is off, mark tube and skin with black marks
• Even if sutures are intact, tube can slip out
23
24
Related Documents











