Sinnar University Faculty of Medicine Obstetric & Gynecology Board Post caesarean section family planning Prepared By: Dr. Samir Abd Elrhman Gorashi M.B.B.S University of Khartoum Assisted professor faculty of medicine Sinnar University

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Sinnar University
Faculty of Medicine
Obstetric & Gynecology Board
Post caesarean section family
planning
Prepared By:
Dr. Samir Abd Elrhman Gorashi
M.B.B.S University of Khartoum
Assisted professor faculty of medicine
Sinnar University

Contents I
List of table II
List of figure III
List of abbreviations IV
English abstract V
CHAPTER ONE
Introduction 1 Literature review 5Objectives 13
CHAPTER TWO
Methodology 14CHAPTER THREE
Results 16

CHAPTER FOUR
Discussion 36Conclusions 38
Recommendations 39References 40
List f Tables
Distribution of study population
according to age Table1
Distribution of study population
according to residence Table2
Distribution of study population
according to level of education Table3
Distribution of study population
according to parity Table4
Distribution of study population
according to occupation Table5
Distribution of study population according to husband education
Table

6Distribution of study population according to economic status
Table7
Distribution of study population
according to source of knowledge Table8
Distribution of study population according to identification type of
contraceptive
Table9
Distribution of study population according to common type of contraceptive used
Table10
Distribution of study population according to reasons for choosing a
particular contraceptive
Table11
Distribution of study population according to husband attitude towards contraceptive
Table12
Distribution of study population according to get pregnant type of
contraceptive used
Table13
Distribution of study population according contraceptive used
prescribed by who
Table14
Distribution of study population according to reasons for not visit family planning centre post
Table15

puerperium Distribution of study population according to difficulties to use
contraceptive
Table16
Distribution of study population according to associated medical disease
Table17

List of Figures
Distribution of study population
according to age Figure 1
Distribution of study population
according to residence Figure 2
Distribution of study population
according to level of education Figure 3
Distribution of study population
according to parity Figure 4
Distribution of study population
according to occupation Figure 5
Distribution of study population according to husband education
Figure 6
Distribution of study population according to economic status
Figure 7

Distribution of study population
according to source of knowledge Figure 8
Distribution of study population according to identification type of
contraceptive
Figure 9
Distribution of study population according to common type of contraceptive used
Figure10
Distribution of study population according to reasons for choosing a
particular contraceptive
Figure11
Distribution of study population according to husband attitude towards contraceptive
Figure12
Distribution of study population according to get pregnant type of
contraceptive used
Figure13
Distribution of study population according contraceptive used
prescribed by who
Figure14
Distribution of study population according to reasons for not visit family planning centre post
puerperium
Figure15
Distribution of study population Figu

according to difficulties to use
contraceptive re16
Distribution of study population according to associated medical disease
Figure17

LIST OF ABBREVIATION
Cu-T Copper-T
DMPA Depot Medroxy Progesterone Acetate
EBF Exclusive Breast Feeding
EE Ethinyl Estradiol
FSH Follicle Stimulating Hormone
GnRH Gonadotropin Releasing Hormone
IUD Intra uterine device
LH Luteinizing Hormone
LAM Lactational Amenorrhoea Method
ML Cu-T Multi loadCopper-T
ME Mestranol

NFP NaturalFamily Planning
NET-EN Norethisterone enanthate
OC Oral Contraceptive
PID Pelvic Inflammatory Disease
POP Progesterone Only Pill
STIs Sexually Transmitted Infections
WHO World Health Organization
ENGLISH ABSTRACT
Objective:- The aim of this study to study the
situation of post caesarean section family
planning in Sinnar teaching hospital.

Methodology: - Descriptive cross sectional hospital
based study among women in Sinnar teaching
hospital. Data collected through designed
questionnaire include: - Socio-demographic
characters, obstetrics characters, knowledge and
attitude towards contraception and post
puerperium counseling regarding contraception
used.
Result:-A total of 946 women interviewed in
postnatal clinic, 325(34.4%) had before unplanned
pregnancy, their reason not used contraception198
(60.9%) and failure of contraception 137(39.1%).
The majority of women want space between
deliveries 798(84.4%), women in this study get
their knowledge about contraceptive from health
worker 322(34%), friends 212(22.4%), and Radio
203(21.5%). Most common type of contraceptive
known to women oral pills 216(22.8%) followed by

the IUCD 201(21.2%). Oral pills the common used
contraceptive 216(24.5%), their reason for that
safe and easy to used 319(33.7%). Husband had not
care about contraceptive used by his wife
402(42.5%). Contraceptive used describe by
doctors 403(42.6%) and friends 367(38.8%). The
majority of couple not counseled about
contraceptive 648(68.5%). Most of difficulties
face used of contraception financials problem
397(41.97%).
Most of the women had no associated disease
630(66.59%), had hypertension 162(17.13%), and
had diabetes mellitus 136(14.38%).
Conclusion: - There was high rate of unplanned
pregnancy, which put the women at risk. Most
women preferred traditional method, husband play
minor role in decided to use contraceptive. The
majority of women not counseled about

contraceptive in postnatal clinic, financial
problem face the women to get contraceptive.
INTRODUCTION
A person quality of life depends not only on good
healthy physical well being but on variety of

other circumstances these include: family
stability and harmony, the welfare of children
and freedom to enjoy various activities
including: leisure educational or community
pursuit. Family planning can influence nearly all
of these aspects of life ranging from those that
are strictly personal such as individual's health
to factors that are shared by relationships with
the others(1) . The most important problem of
human being today is not infectious diseases but
population. The world problem now is higher than
at any time in its history(2). Statistics showed
that the population of the world was about 1
billion in 1850 eighty years later in 1930 the
number of population doubled. On 1976 it had
doubled again and today it is more than 6
billions. Increase in the population has been
deemed the most important socio-economic and
cultural phenomenon in recent decades. The
ramification of population increase constitutes
serious threat (3.) A country with population
greater than its socio-economic resources can
support would be faced with many problems both
cultural and socioeconomic which in turn would

influence its independence. Family planning is
now accepted as an important health measure of
maternal health and its important contributor to
any effort aiming at the improvement of the
status of women (4).
Both men and women have the right to be informed
and have access to save, effective, affordable
and acceptable method of family planning of their
choice (5).
Since 1960s family planning programs have helped
women around the world to avoid 400 million
unwanted pregnancies (6). As a result many women's
lives have been saved. Therefore, family planning
helps reducing maternal morbidity and mortality
besides high risk pregnancies. Moreover, it
enables women to space out their pregnancies.
Further it gives the parents the chance to give
better care for their children and family .For
these reasons family planning is an important
strategy in promoting maternal and child
health(7).
Today an estimated 350 million couples worldwide
lack access to an effective and affordable family
planning method (8). Family planning does more

than help couples limit their family size , it
safe guards individual health and rights ,
preserve natural resources and can improve the
economic outlook for families and
communities .Family planning also saves lives up
to one third of all maternal illnesses could be
prevented if women had access to contraception (9).
At least 200 million women want to use effective
and safe family planning method but they are
unable to do so because they lack access to
information and services or the support of their
husbands and communities. Therefore the need for
family planning is growing so fast and it is
estimated that the unmet need will grow by 40% by
the next 15yrs (10, 11). Funding is decreasing and
the gap between the need and the available
resources is increasing (12).
Unmet need is defined as the percentage of fecund
married women who are not using an appropriate
method of contraception even though they don’t
want to get pregnant (13,14).
At present time family planning in the third
world countries is well established and is

progressing toward helping family's regulate
their reproductive lives (15). There is evidence
that sporadic cases of family practice in Sudan
had been known since the late 1950s.However,
services were initiated in 1965 and 1985 were
integrated into primary health care system(16,17).
In Sudan use of contraception was reported by 8%
of women but this figure differs according to
education levels of wealth back ground (18). The
most popular method of contraception in Sudan is
the contraceptive pills which is used by almost
one in twenty married women (19).
In Sudan maternal mortality is one of the highest
rates in the world. (1107 death / 100,000 live
birth)(20) .
Despite challenges in providing optimal
counseling effort, the antenatal health care
delivery settings would seem to be an ideal time
to conduct post partum contraceptive counseling.
Based on the result of case-control studies done
in U k , it is found most of women post caesarean
section used oral contraception because easy to

used and available, and can be used for long
duration without complication(21).
Knowledge and attitude towards post partum
counseling a community based study in Northwest
Ethiopia conclude that most of women used the
long term contraception like injection, Marina
and Implanon(21).
OBJECTIVES
General Objectives:

To study the situation of post c/s family
planning in Sinnar teaching hospital.
Specific Objectives:
1.To determine unmet need for family planning
in patients with post caesarean section.
2.To determine women knowledge, attitude
towards post caesarean
Section contraception
3-To determine family planning utilization
rate .
4-To identify the suitable method of
contraception for post caesarean section
women.
5-Explain the benefits of birth spacing.

METHODOLOGY
(1) Study design:
This is a descriptive cross-sectional hospital
based study.
(2) Study Area : Sinnar Teaching Hospital
antenatal clinic.
(3) Study Period : From August 2013 to January
2014.
(4) Study Population:

Sudanese women post caesarean section attending
in the Antenatal clinic at Sinnar Teaching
Hospital for contraception
(5)Sample size.
Sample size will be calculated with the help
of the formula:
N=z²(pq)
d²
Where:
N=sample size
Z=Coefficient level at 1.96 (95%).
P= Prevalence.
q= (p-1)
d= error 5%
Sample size is estimated to be( 1000) Sudanese
women .
(6) Data collections:

Data will be collected by a questionnaire this
will include close-ended questions covering the
following:
(7) Data analysis:-
Data will be analyzed using SPSS Computer
Program.
(8) Exclusion Criteria:-
Refusal of Sudanese women to participate in the
study.
(9) Ethical approval:-
Written consent should be optional from the
manager of Sinnar Teaching Hospital antenatal
clinic. Women will be informed that their
participation is voluntary.

RESULTS
The interviews were conducted between 1st of
August 2013 to 1st of January 2014. The
participants' were sampled when women post
caesarean section they attended post natal clinic
at Sinnar teaching hospital, and accepted to
participate. The results were represented in
three major sections: Socia-demographic
characteristics, Obstetrics characteristics,
Knowledge and attitude regarding contraceptive
used. A total of 946 pregnant women interviewed.

Women with an unplanned pregnancy were 325(34.4%)
while women with planed pregnancy were
621(65.6%)). Those who had unplanned pregnancy
before, (60.9%) of them did not use
contraceptives and the rest (39.1%) due to
failure of contraceptives.
The majority of women agreed with spacing between
deliveries 798(84.4%), only 115(12.2%) did not
agree, while 33(3.4%) don’t know.
Couples who were counseled for contraceptive
before were 298(31.5%) and those not counseled
were 648(68.5%).
Women who visited the family planning center
postnatal before were 432(45.7%) and those did
not were 514(54.3%).

Women who knew the benefits and side effects of
contraceptives were 325(34.4%) and those did not
know were 621(65.6%) .
Table 1: shows the age of the study group, less
than 20 years old 93(9.9%), between (20-40) years
old 748(79%) and more than 40 years old
105(11.1%).
Table 2: shows the residence of the study
population, rural 332(35.1%), urban 225(23.8%)
and suburban 389(41.1%).
Table 3: shows the Level of education of the
study population, illiterate 30(3.2%), Khalwa
21(2.2%), primary school 266(28.1%), secondary
school 502(53.1%), university graduate 86(9.1%)
and postgraduate 41(4.3%).

Table 4: shows the parity of the study group,
para one 212(22.4%), multipara 452(47.8%) and
grandmultipra 282(29.8%).
Table 5: shows the occupation of the study group,
housewife 575(60.78%), laborer 132(13.95),
employee 186(19.66%) and professional
53(5.61%).
Table 6: shows the husband education of the study
group, illiterate 121(12.8%), Khalwa 103(10.9%),
primary school 210(22.2%), secondary school
439(46.4%), university graduate 42(4.4%) and
postgraduate 31(3.3%).
Table 7: shows the economic status of the study
group, high 96(10.2%), moderate 420(44.4%), low
319(33.7%) and very low 111(11.7%).
Table 8: shows the study population get their
source of knowledge from, Radio 203(21.5%),

Television 188(19.9%), friend 212(22.4%), health
worker 322(34%) and news paper 21(2.2%).
Table 9: shows the identification types of
contraception study population know, coitus
interrupts 212(22.4%), safe period 197(20.8%),
IUCD 201(21.2%), implants 111(11.7%), injection
193(20.4%), oral pill232 (24.5%), sperm suicide
21(2.2%), condom 83(8.8%), vaginal barrier
11(1.2%), sterilization 101(10.7%) and IUS
71(7.5%).
Table 10: shows the most common type of
contraceptive used by the couple, coitus
interrupts153 (16.2%), safe period 167(17.7%),
pills216 (22.8%), injection 183(19.4%), IUCD
100(10.6%) and condom 22(2.3%).
Table 11: shows the reasons for choosing
particular contraceptive, safe and easy
319(33.7%), husband preference 152(16.1%),

advised by doctors or friends 227(23.9%), has no
complications 270(28.5%) and the only known to
the women 91(9.6%).
Table 12: shows the husband attitude towards
contraception, positive 359(37.9%), against
185(19.6%) and don’t care 402(42.5%).
Table 13: shows those get pregnant during
contraception use, coitus interrupts 87(28.9%),
safe period 177(58.8%), pills 21(6.9%) and condom
16(5.4%).
Table 14: shows contraceptive used that
prescribed by: doctors 403(42.6%), midwife
77(8.1%), used alone 99(10.5%) and friends
367(38.8%).
Table 15: shows their reasons for not visiting
family planning centre post puerperium, not
interest 148(28.8%), not told to came back after
puerperium 182(35.4%), financial problem
96(18.7%) and no needs to came 88(17.1%).
Table 16: shows difficulties to used
contraception, financial 397(41.97%), religious
154(16.28%), husband attitude 172(18.18%) and
accessibility 223(23.57%).
Table 17: shows associated medical disease, heart
disease 11(1.16%), diabetes mellitus 136(14.38%),
hypertension 162(17.13%), thromboembolism
7(0.74%), and no associated disease 630(66.59%).

Table 1: Distribution of study population
according to age-:
PercentFrequency Age 09.9%093 ≤2079.0%74820 -4011.1%105 >40100%946Total

Table 2:- Distribution of study population
according to residence-:
Percent Frequency Residence 35.1%332Rural
23.8%225Urban
41.1%389Suburban
100%946Total

Table 3:- Distribution of study population
according to level of education:-
Percent Frequency Level of
education
03.2%030Illiterate

02.2%021Khalwa 28.1%266Primary school 53.1%502Secondary
school 09.1%086University
graduate 04.3%041Postgraduate 100%946Total

Table 4:- Distribution of study population
according to parity-:
Percent Frequency Parity 22.4%212Prim Para
47.8%452Para 2- 5
29.8%282Para > 5
100%946Total

Table 5:- Distribution of study population
according to occupation:-
Percent Frequency Occupation 60.78%575Housewife
13.95%132Laborer
19.66%186Employee
05.61%053Professional

100.00%946Total
Table 6:- Distribution of study population
according to husband education-:

Percent Frequency Husband
education
12.8%121Illiterate 10.9%103Khalwa 22.2%210Primary school 46.4%439Secondary
school 04.4%042University
graduate
03.3%310Postgraduate 100.0%946Total

Table 7:- Distribution of study population
according to economic status-:
Percent Frequency Economic status 10.2%094High
33.7%319Moderate
44.4%420Low
11.7%111Very low
100.0%946Total

Table 8:- Distribution of study population
according to source of knowledge-:
Percent Frequency Source of
knowledge

21.5%203Radio 19.9%188Television 22.4%212Friend 34.0%322Health worker 02.2%021News paper
100.0%946Total

Table 9:- Distribution of study population
according to identification of types of
contraception the women know:-
Percent Frequency Type of
contraception 24.5%232Oral pills 22.4%212Coitus interrupts 21.2%201IUCD 20.8%197Safe period 20.4%193Injection 11.7%111Implant 10.7%101Sterilization 08.8%083Condom 07.5%071 IUS 02.2%021Sperm suicide 01.2%011Vaginal barrier

Table 10:- Distribution of study population
according to contraceptive used by the women or
husband:-
Percent Frequency Type of
contraceptive 22.8%216Oral pills 19.4%183Injection 17.7%167Safe period 16.2%153Coitus interrupts 10.6%100IUCD 02.3%022Condom
100.%946Total
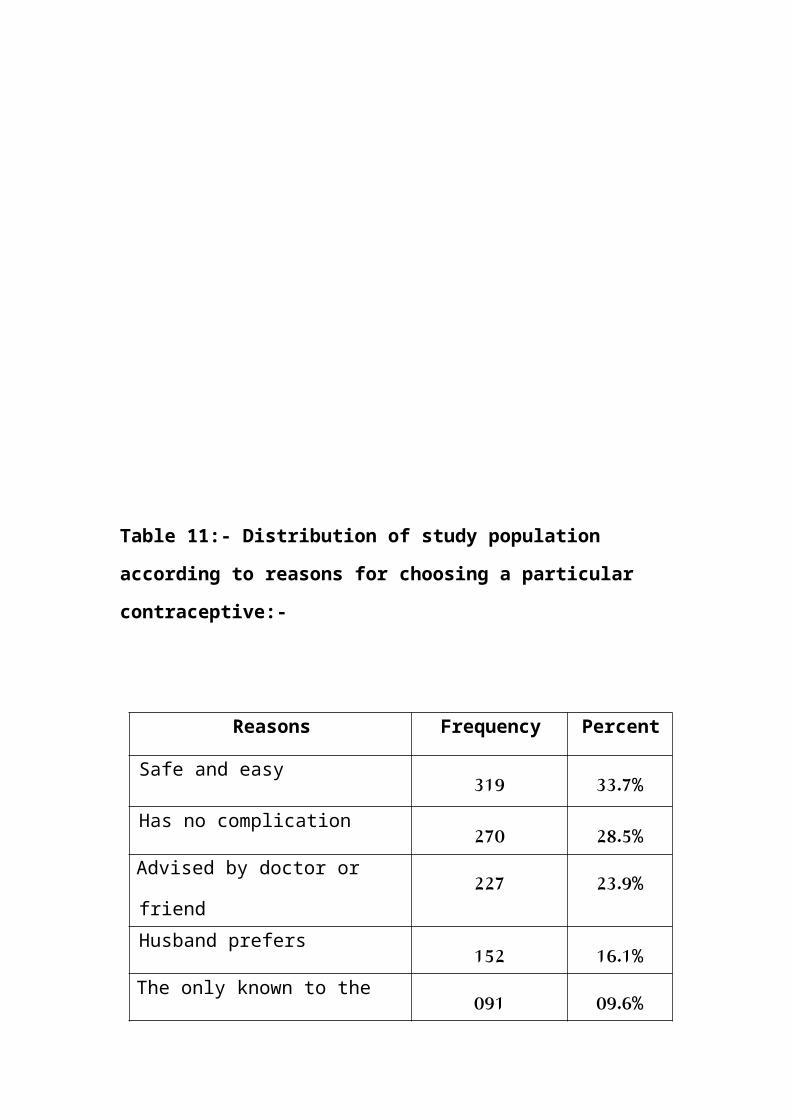
Table 11:- Distribution of study population
according to reasons for choosing a particular
contraceptive:-
Percent Frequency Reasons 33.7%319Safe and easy 28.5%270Has no complication 23.9%227Advised by doctor or
friend 16.1%152Husband prefers 09.6%091The only known to the

women
Table 12:- Distribution of study population
according to husband attitude towards
contraceptives-:

Percent Frequency Husband
attitude 37.9%359Positive 19.6%185Against
42.5%402Don’t care 100%946Total

Table 13:- Distribution of study population
according to contraceptive used before getting
pregnant:-
Percent Frequency(n=301
) Contraceptive
used 28.9%087Coitus
interrupts 58.8%177Safe period
other NFP 06.9%021Oral pill
05.4%016Condom 100%301Total
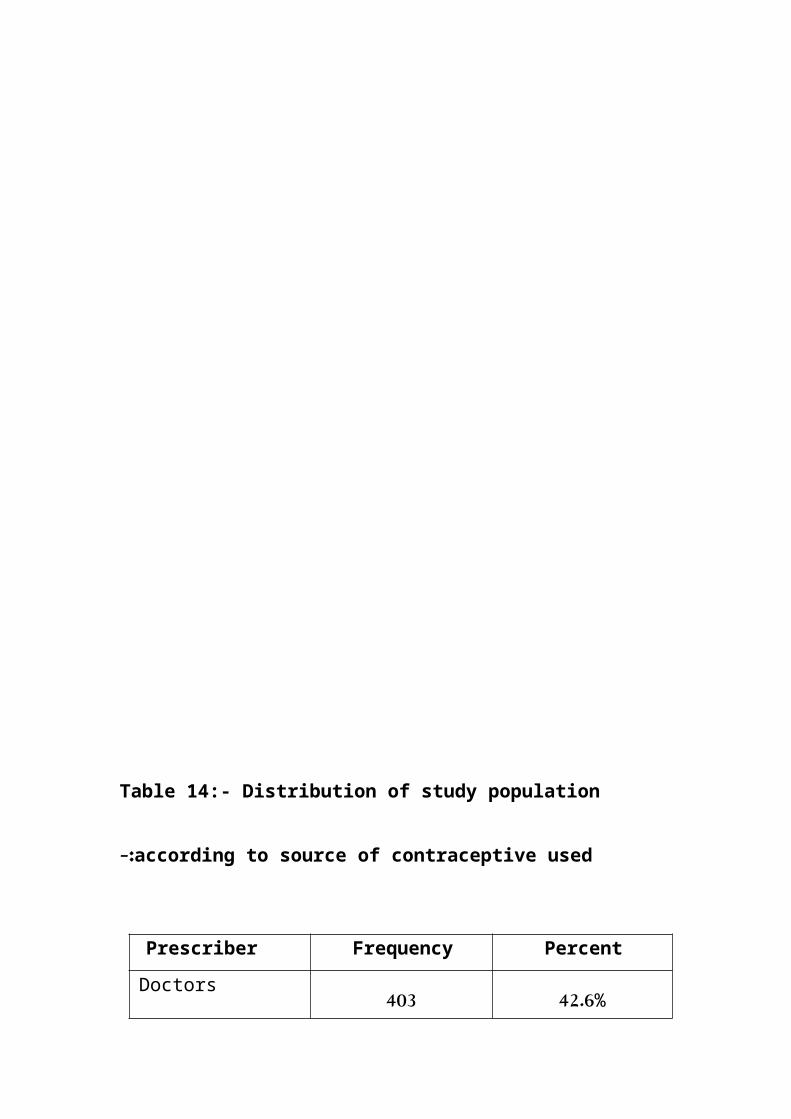
Table 14:- Distribution of study population
according to source of contraceptive used-:
Percent Frequency Prescriber 42.6%403Doctors

38.8%367Friends 10.5%099Used alone 08.1%077Midwife 100%946Total

Table 15:- Distribution of study population
according to reasons for not visiting family
planning center postnatal-:
Percent Frequency(n=5
14) Reasons
35.4%182Not told to came
back after
puerperium
28.8%148Not interested
18.7%096Financial problem
17.1%088No need to came
back 100%514Total

Table 16:- Distribution of study population
according to difficulties to use contraceptives:-
Percent Frequency Difficulties 41.97%397Financial 23.57%223Accessibility 18.18%172Husband
attitude 16.28%154Religious

100%946Total
Table 17: Distribution of study population
according to associated medical diseases:

Medical disease Frequency Percent
Heart disease 011 01.16%
Diabetes mellitus 136 14.38%
Hypertension 162 17.13%
Thromboembolism 007 00.74%
No associated disease 630 66.59%
Total 946 100.0%

Figure 1:
Age
9.90%
79%
11.10%
0.00%10.00%20.00%30.00%40.00%50.00%60.00%70.00%80.00%90.00%
>20 20 - 40 >40

Figure 2:
Residence
35.10%
23.80%
41.10% Rural Urban Suburban

Figure 3:
Level of Education
9.10%
4.30% 3.20% 2.20%
28.10%
53.10%
IlliterateKhalwaPrim ary schoolSecondary schoolUniversity graduate Postgraduate

Figure 4:
Parity
22.40%
47.80%
29.80%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
Prim para Para 2 - 5 Para > 5

Figure 5:
Occupation
60.78%
13.95% 19.66%
5.61%
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
Housewife Laborer Em ployee Professional

Figure 6:

Husband Education
12.80%
10.90%
22.20%
46.40%
4.40%
3.30%
0.00% 10.00% 20.00% 30.00% 40.00% 50.00%
Illiterate
Khalwa
Prim ary school
Secondary school
University graduate
Postgraduate

Figure 7:
Econom ic status
10.20%
33.70%44.40%
11.70%HighM oderateLowVery low

Figure 8:
21.50%
19.90%
22.40%
34%
2.20%
0.00% 5.00% 10.00% 15.00% 20.00% 25.00% 30.00% 35.00%
Radio
Television
Friend
Health worker
News paper
Source of know ledge

Figure 9:
Type of contraception know n by the w om en
20.40%
11.70%
10.70%
8.80%7.50%
2.20% 1.20%
24.50%
22.40%
21.20%20.80%
Oral pills Coitus interruptsIUCD Safe period Injection Im plant Sterilization Condom IUS Sperm suicide Vaginal barrier

Figure 10:
Contraceptive used by the w om en
22.80%
19.40%
17.70%
16.20%
10.60%
2.30%
0.00% 5.00% 10.00% 15.00% 20.00% 25.00%
Oral pills
Injection
Safe period
Coitus interruptus
IUCD
Condom

Figure 11:

Reasons of used particular contraceptive
33.70%
28.50%
23.90%
16.10%
9.60% Safe & easy
Had no com plication
Advised by doctor orfriendHusband prefers
The only known to thewom en

Figure 12:
Husband attitude
37.90%
19.60%
42.50%
0.00%5.00%10.00%15.00%20.00%25.00%30.00%35.00%40.00%45.00%
Positive Against Don’t care

Figure 13:
Contraceptive used before getting pregnant
58.80%
6.90%5.40%
28.90%
Coitus interruptsSafe periodOral pillCondom

Figure 14:
42.60%
38.80%
10.50%
8.10%
0.00% 10.00% 20.00% 30.00% 40.00% 50.00%
Doctors
Friends
Used alone
m idwife
Sources of contraceptive used

Figure 15:
Reasons for not visiting FPC postnatal
35.40%
28.80%
18.70%
17.10%Not told Not interestedFinancial problemNo need

Figure 16:
Difficulties to used contraception
41.97%
23.57%18.18% 16.28%
0.00%5.00%10.00%15.00%20.00%25.00%30.00%35.00%40.00%45.00%
Financial Accessibilty Husband attitude Religious

Figure 17:

Associated m edical disease
1.16% 14.38%
17.13%
0.74%66.59%
Heart diseaseDiabetes m ellitusHypertensionThrom boem bolismNo associated disease

DISCUSSION
Counseling for contraception applies discussion
of contraceptive needs, taking into account
reproductive goals and protection against
sexually transmitted diseases, information and
counseling about methods, their effectiveness
rates, and side effects, short- and long-term
method choices, assurance of contraceptive
resupply & access to follow-up care.
Postpartum contraception is the initiation and
use of family planning methods in the first six
weeks after delivery to prevent unintended
pregnancy particularly in the first 1-2 years
after childbirth, when another pregnancy can be
harmful to the mother or a breast feeding baby.
Unplanned pregnancy in this study is high
(34.4%), this well increase women risk of

complication of pregnancy, repetitive delivery
stress on women health and the effect on her baby
and breast feeding, and will increased chances of
unsafe abortion. The majority of the women
(60.9%) not used modern, but using natural method
(safe period and coitus interrupts) and those
used contraceptive (39.1%) are not using it
regularly. Here came the role of post partum
counseling about contraceptive and used
appreciated one for the women.
A similar study done in India found that
unplanned pregnancy was (45.5%), mainly due to
traditional and community believes, contraceptive
make infertility (34).
Health worker, friends and mass media are main
source of knowledge for women about
contraception.

This in contrast to study in Ethiopia where the
source of knowledge was midwives and friends
respectively (35).
Oral contraceptives most common contraceptive
known to all women followed by IUCD and
injection, this result similar to a study in
India and Ethiopia but in contrast to study done
in Ireland in which most common contraceptive
used was condom, sperm suicide and vaginal
barrier, these methods women had low knowledge
about it because not commonly used or accepted in
Sudan (34, 35, 36).
Most common methods of contraceptive used by the
women in this
study were oral pills (24.5%), followed by
coitus interrupts (22.4%) and safe period. Last
two methods an unsafe and not accurate if not
used properly. This explains why unplanned

pregnancy increased in number. The reasons for
women to use a particular contraceptive, safe and
easy (33.7%) and had no complication (28.5%).
This result is similar to India study, where
their reasons safe and easy to use.
The husband had major role in post partum
contraceptive to choose with his wife and discuss
the complication but in this study the husband
attitude is negative or does not care (42.5%) (34).
In this study found most of contraceptive
prescribed by doctors (42.6%) and near friends
(38.8%). This result in contrast to Ethiopia
study where used alone most common (34%) (35)
Regarding counseling of both couple post natal
about contraceptive, most of them were not
counseled (68.5%) and only (31.5%) counseled,
this similar to India and Ethiopia study (34, 35).

More than half of the women did not visit post
natal family planning centre, a (54.3%) of them
because they have not been told to come back
after puerperium.
Most of the women (65.6%) did not know the
benefits and the side effects of contraceptive
use. This result is better than in Ethiopia and
India study, but in contrast to Ireland study all
the women know the side effect and the benefit of
the contraceptive used(34,35).
The difficulties face the use of contraceptive by
the women was financials problem in the most of
women (41.97%) and in according accessibility
(23.57%).
Most of the women in this study (66.59%) used
contraception and had no associated medical
problem.
CONCLUSIONS

The study show a relatively high unplanned
pregnancy, due to poor counseling and
communication for family planning, the husband has
no role in improving utilization of family
planning. Most of women do not visit post natal
care centre routinely in spite of presence of
family planning and post natal clinic, there is no
detailed counseling for both couple.

RECOMMONDATIONS
♦ Involve both couple in post natal counseling.
♦ Details information about contraception must
be given for both
couple.
♦ Told women to came routinely to post natal
clinic.
♦ Attempts should be made to overcome the
resistance expressed by men for family

planning methods besides involving them in
the whole process of family planning.
♦ Extensive collaboration, with different
media means: TV, radio,
presses to deliver message to women
about the important of post
natal counseling.
REFERENCES
1) Recosta D, Ray V, Haney S. A study
of knowledge & attitude of married women
regarding family planning, Department
of health & Environment, Faculty of

Health science, Human Reproductive
Growth and Development, 3rd ed.
Philadelphia: W. B. Saunders; 1998. p
360.
2) Lihera-Karmer JA, Klea M. A study of
knowledge, attitude and Practice towards
family planning methods conducted in
Japan: center of AIDS Prevention studies
(CAPSL) University of California, San
Francisco, USA 2001. Eur J 2005; 312:
160-66.
3) Ashasy N, Rasheeds D. A study of Family
Planning unmet need among Iraq Kurds:
Department of Public Health, Collage of
Medicine, University of Dohuk, Dohuk,
Iraq 2003. Gynaecol Obstet J 1998;
65(3): 415-22.

4) Sudan House Hold Survey (SHHS).
Reproductive health commodility Security
Situation Analysis of Northern State,
Ministry of Health UNFPA John Show, Inc.
Eur J 2005; 312:211-18.
5) Freedman R, Blanc A K . Fertility
transition: an update. Intern Family
Plan g Perspect 1992; 18 (2): 44-50.
6) Weldegerima B, Denekew A. Women
Knowledge , preference and practice of
modern Contraceptive methods in Woreta ,
Ethiopia .Reserch in Soc Administ
pharmacy 2008; 4:302-7.
7) Ibnawf AH, Vanden Borne Hw, Mearse J.
Study of family planning service by
married woman of reproductive age. East
Mediterran Hlth J 2007; 13 (6): 87-
90.

8) Hammed K, Salem M, Salem M. a study
of knowledge & attitude of married
Tunisian women regarding family planning
. Department of Family Science Faculty
of health science, University of Tunis
2008, 6: 122-142
9) Yolascan SA, Cetino MO. A study of
family use in rural Adana Turkey:
Cukurwa University; Adana Turkey 2006.
Eur J 2008; 96: 133-40.
10) Jellbas S, Syel-Sjo K, Glebek G. A
study of knowledge & attitude of married
Swedish women regarding family planning
Department of health & Environment,
Faculty of Health science, Linkoping
University, Sweden 2007. Am J Obst
Gynaecol 2009; 239(12): 199-205.

11) Mahmod S, Ringhim K. Knowledge
approval & communication about Family
planning as correlates of desired
fertility among spouses in Pakistan.
Intern family Plan Perspect 1997;
23:122-29.
12) UNICEF. The state of the world children.
New York: Oxford university press; 2009;
567-571 .
13) Sudan Demographic And Health Survey,
1989-1990. Ministry of Economic and
National planning Khartoum , Sudan.
SMJ 1991; 33-74 .
14) Westoff CF, Bankole A. Unmet need: 1990–
1994. Calverton, Maryland, Macro
International, 1995 (Demographic and
health survey comparative reports No.
16; 231-236.

15) Askew I. Mensch B, Adewuyi A ,
indication for measuring the quality of
family planning services in Nigeria.
Studies Family Planning Eur J
1994;25(5):268-83.
16) Huezo L, Amphora U. Choice and use
method of contraception : A multi center
, study , London ; international planned
parenthood federation ,1993:and paring
S, Hear DM and Van Ardor MD ,dose choice
make difference to contraception were
Evidence from East Java. Studies Family
Planning . Eur J 1991; 22(6 ) : 384-90.
17) Mary l. Institute for Resource Development
and Macro International, 1991 Westoff CF,
Ochoa LH. Unmet need and demand for family
planning. Colombia, (Demographic and health
survey comparative reports No. (5): 43-46

18) Kim Y. Metal, client participation and
provider communication in family
planning counseling: transcript analysis
in Kenya. Hlth Commun Forth Coming
1998; 10: 48-52.
19) Gimbel H, Settenos A, Tabor A. Modernization
and family planning programms . Acta Scand
Gynaecol Obstet 2001; 80: 267 – 272.
20) Bulatao RA . The Value of Family
Planning Programs in developing
countries . Santa Monica , California ,
Rand ,1998 . Obst Gynaecol 2001; 77(50-
a): 68-75.
21) Gilliam ML , Knights MC, Cartly M.
Importance and knowledge of
contraceptives in post partum , low –
income , African – American

adolescents . J Pediatr Adolesc Gyrecol
2003;16:355-60.
22) Vanlandingham M, Tussel J, Grummer Y,
Strawn L. Contraceptive and health
benefits of breast-feeding :a review of
the recent evidence . International
family planning prospective. Eur J
1991;17(4):131-36 .
23) World health report, statistical annex.
Geneva, World Health Organization, 2002;
190-198.
24) Millennium Project. Investing in
development. A practical plan to achieve
the Millennium Development Goals. New
York: U N; 2005.p.2-83.
25) Seltzer JR. The origins and evaluation
of family planning programs in
developing countries .Santa Monica ,

California , Rands. Br Med J 2000; 63:
185.
26) Collaborative Group Hormonal
contraceptives and reduction of maternal
mortality. A joint WHO/UNICEF/WORLD
Bank Statement. Geneva: WHO;1999; 11-34.
27) Ross JA, Frankenberg E. Findings from
two decades of family planning research.
New York, Population Council, 1993.
http://www.meip.org/mer/mer205/kaKamran.
htm. Accessed on 12 August 2007; 135-
156.
28) Cushman LF. IUD use among women .
choosing long-term hormonal
contraception. Family Plan Perspect
1998; 30(5):240-43.
29) Bankole A, Darroch JE, Singh S. Barrier
method use in the United States, 1988-

1995. Family Plan Perspect 1999;
31(6):264-71.
30) Janowitz B. Natural family planning methods
in Sao Paolo State, Brazil. Intern Family
Plan Perspect 2004; 6(1):10–20.
31) Rajasekar D, Bigrigg A. Pill W.
sterilization methods (tubal occlusion )
in Scotland: facts, myth and fantasies
EurJ Contrapet Reprod hlth Care
2005;123-147.
32) Caldwell JC, Caldwell P. Female
sterilization . Popul Develop Rev 2007;
13(3):409–37.
33) Blenning CE, Paladine H. An approach to
the postpartum
office visit. Am Fam Physician
2005,15(12):43-46.

34) Ashrotri AV, Shankor S, Sutar A, Joshi
N, Awanshi H, Pisal
, Bharucha MA, Phadke RC, Bollinger
JS. Post partum
counseling in India. 2009; 1:
83-89.
35) Shiraye A, Nuru A, Getu D, Yared W,
Solomon A. Knowledge
and attitude towards post partum
counseling a community based
study in Northwest Ethiopia. Ethiop J
Health Dev 2004; 18(2):
82 – 88.
36) Addo VN. Post partum counseling in
Ireland. Med J 2005;
39(2): 50-53.

Related Documents











