21.01.2016 1 Post-ASH 2015 Koblenz 03.02.2016 Hartmut Goldschmidt Autologous Transplantation For Multiple Myeloma in the Era of new Drugs: a Phase 3 Study of the “Intergroupe Francophone du Myélome”. Second Interim Analysis of the IFM 2009 Trial. Michel Attal, Valerie Lauwers-Cances, Cyrille Hulin, Thierry Facon, Denis Caillot, Martine Escoffre, Bertrand Arnulf, Margaret Macro, Karim Belhadj, Laurent Garderet, Murielle Roussel, Claire Mathiot, Hervé Avet-Loiseau, Nikhil Munshi, Paul Richardson, Kenneth Anderson, Jean Luc Harousseau, and Philippe Moreau for the IFM.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

21.01.2016
1
Post-ASH 2015Koblenz
03.02.2016 Hartmut Goldschmidt
Autologous Transplantation For Multiple Myeloma in
the Era of new Drugs: a Phase 3 Study of the
“Intergroupe Francophone du Myélome”.
Second Interim Analysis of the IFM 2009 Trial.
Michel Attal, Valerie Lauwers-Cances, Cyrille Hulin, Thierry
Facon, Denis Caillot, Martine Escoffre, Bertrand Arnulf, Margaret
Macro, Karim Belhadj, Laurent Garderet, Murielle Roussel, Claire
Mathiot, Hervé Avet-Loiseau, Nikhil Munshi, Paul Richardson,
Kenneth Anderson, Jean Luc Harousseau, and Philippe Moreau
for the IFM.

21.01.2016
2
Registration
)
RVD 1
Lenalidomide + Bortezomib + Dexamethasone25mg/d (d1 to 14) 1.3mg/m2 (d 1, 4, 8, 11) 20mg/d (d1,2,4,5,8,9,11,12)
) Randomization (stratified on ISS and FISH)
Arm AArm A Arm BArm B
RVD 2 and 3
PBSC Collection
(cyclophosphamide 3g/m2 and G-CSF)
10mcg/kg/d)
ASCT HDM 200mg/m2 RVD 4 to 8
RVD 4 and 5
Lenalidomide Maintenance
12 months (10-15 mg/d)
RVD 2 and 3
PBSC Collection
(cyclophosphamide 3g/m2 and G-CSF)
IFM 2009 : Study Design
Lenalidomide Maintenance
12 months (10-15 mg/d)
IFM 2009: Objectives.
�Primary objective:
• To compare PFS between the 2 arms.
�Secondary objectives:
• To compare RR, MRD (by FCM) between the 2
arms.
• To compare TTP between the 2 arms.
• To compare OS between the 2 arms.
• To compare toxicity between the 2 arms.

21.01.2016
3
IFM 2009: Inclusion Criteria
�De novo myeloma patients.
�Age between 18 and 65 years.
�ECOG performance status <2.
�Symptomatic myeloma with organ damage related
to myeloma.
�Measurable disease : serum M-protein > 10 g/l,
and/or urine M-protein > 200 mg/24 h, and/or
serum FLC assay: involved FLC level > 100 mg/l
provided serum FLC ratio is abnormal.
IFM 2009: Patient characteristics (1)
RVD Arm
N=350
Transplant Arm
N=350P-value
Total
N=700
Age, yr 59 60 NS 59
Sex, n (%)
-Male
-Female
208 (59)
142 (41)
214 (61)
136 (39)
NS
422 (60)
278 (40)
Type of Myeloma, n (%)
-IgG
-IgA
-Light chain
-other
209 (60)
71 (20)
57 (16)
13 (4)
223 (64)
73 (21)
46 (13)
8 (2)
NS
432 (62)
144 (21)
103 (15)
21 (3)
ISS stage, n (%)
-I
-II
-III
115 (33)
170 (49)
65 (19)
118 (34)
171 (49)
61 (17)
NS
233 (33)
341 (49
126 (18)

21.01.2016
4
IFM 2009: Patient characteristics (2)
RVD Arm
N=350
Transplant Arm
N=350p-value
Total
N=700
Evaluable FISH, n (%) 256 (73) 259 (73) NS 515 (74)
Cytogenetic risk, n (%)
-Standard risk
-High risk
212 (83)
44 (17)
213 (82)
46 (18)
NS 425 (83)
90 (17)
t(4-14), n (%)
-No
-Yes
230 (90)
26 (10)
230 (89)
28 (11)
NS
460 (89)
54 (11)
Del (17p), n (%)
-No
-Yes
241 (94)
15 (6)
242 (94)
15 (6)
NS
483 (94)
30 (6)
t (14-16), n (%)
-No
-Yes
250 (98)
6 (2)
252 (98)
6 (2)
NS
502 (98)
12 (2)
IFM 2009: Best Response
RVD arm
N=350
Transplant arm
N=350p-value
CR 49% 59%
VGPR 29% 29% 0.02
PR 20% 11%
<PR 2% 1%
At least VGPR 78% 88% 0.001
Neg MRD by FCM , n (%) 228 (65%) 280 (80%) 0.001

21.01.2016
5
IFM 2009: VGPR rate
During each Treatment Phase.
RVD arm
N=350
Transplant arm
N=350p-value
Post induction 47% 50% NS
Post transplant or at C4 55% 73% <0.0001
Post consolidation 71% 81% <0.006
Post maintenance 78% 88% <0.001
IFM 2009: PFS (9/2015)
RVD arm
N=350
Transplant arm
N=350p-value
Median follow-up, months 41 41
Progression or Death, n 204 158
Median PFS, months 34 43
4-year PFS 35% 47%
Hazard ratio (95% CI) 1 0.69 (0.56-0.84) <0.001

21.01.2016
6
IFM 2009: PFS (9/2015)
P<0.001
0
10
20
30
40
50
60
70
80
90
100
Pa
tie
nts
(%
)
350 296 228 128 24no HDT350 309 261 153 27HDT
N at risk
0 12 24 36 48
Months of follow-up
HDT
no HDT
IFM 2009: OS (9/2015)
RVR arm
N=350
Transplant
N=350
P-value
Death, n 48 54
4-year survival 83% 81%
Hazard ratio (95% CI) 1 1.2 (0.7-1.8) NS

21.01.2016
7
P NS
0
10
20
30
40
50
60
70
80
90
100
Patients
(%
)
350 338 320 244 56no HDT350 328 309 226 55HDT
N at risk
0 12 24 36 48
Months of follow-up
HDT
no HDT
IFM 2009: OS (9/2015)
IFM 2009: Cause of Death (9/2015)
RVD arm
N=48
Transplant
N=54
Myeloma, n (%) 40/48 (83%) 35/54 (65%)
Toxicity, n (%) 4/48 (8%) 9*/54 (16%)
SPM 1/48 (2%) 6/54 (11%)
Others 3/48 (6%) 4/54 (7%)
*Including 5 transplant related deaths.

21.01.2016
8
IFM 2009: Conclusions
� This second interim analysis demonstrates that transplantation :
• Is feasible: 93%
• Is associated with an acceptable Transplant Related Mortality: 1.4%.
• Is associated with an increased rate of neg MRD (80% vs 65%, p<0.01).
• Is associated with an improved 4-year PFS (47% vs 35%, p<0.001).
• Is associated with an improved 4-year TTP (49% vs 35%, p<0.001).
� A longer follow up is required to draw any conclusion concerning OS,
• Since the 4-year survival is high in both arms (81% vs 83%).
• However, transplantation is already associated with a reduced risk of
death due to myeloma.
� in the era of new drugs, Transplantation should Remain
“A Standard of Care”.
Registration
)
RVD 1
Lenalidomide + Bortezomib + Dexamethasone25mg/d (d1 to 14) 1.3mg/m2 (d 1, 4, 8, 11) 20mg/d (d1,2,4,5,8,9,11,12)
) Randomization (stratified on ISS and FISH)
Arm AArm A Arm BArm B
RVD 2 and 3
PBSC Collection
(cyclophosphamide 3g/m2 and G-CSF)
10mcg/kg/d)
ASCT HDM 200mg/m2 RVD 4 to 8
RVD 4 and 5
Lenalidomide Maintenance
Until progression (10-15 mg/d)
RVD 2 and 3
PBSC Collection
(cyclophosphamide 3g/m2 and G-CSF)
US Trial = Study Design
Lenalidomide Maintenance
Until progression (10-15 mg/d)

21.01.2016
9
Evaluation of Minimal Residual Disease (MRD) Evaluation of Minimal Residual Disease (MRD)
by Next Generation Sequencing (NGS)by Next Generation Sequencing (NGS)
is highly predictive of PFS in the IFM/DFCI 2009 trial.is highly predictive of PFS in the IFM/DFCI 2009 trial.
Herve Avet-Loiseau, MD, PhD1*, Jill Corre2*, Valerie Lauwers-Cances, MD3*, Marie-
Lorraine Chretien4*, Nelly Robillard,5*, Xavier Leleu, MD, PhD6, Cyrille Hulin, MD7*,
Catherine Gentil, Engineer8*, Bertrand Arnulf9*, Karim Belhadj, MD10*, Sabine
Brechignac, MD11*, Laurent Garderet, MD12, Lionel Karlin13*, Gerald Marit14*, Lotfi
Benboubker15*, Frederique Orsini-Piocelle, MD16*, Bruno Royer, MD17,18*, Bernard
Drenou, MD19*, Mourad Tiab, MD20*, Thierry Lamy, MD, PhD21, Margaret MACRO,
MD22*, Paul G. Richardson, MD23, Kenneth C Anderson, MD24, Malek Faham, MD,
PhD25, Thierry Facon26, Philippe Moreau27,28,29*, Michel Attal30 and Nikhil C. Munshi,
MD31
Diagnosis 1012
CR 1010
iCR 108-107
mCR 106
Sensitivity matters
80% HD trials

21.01.2016
10
What are the available tests?
Advantages/Disadvantages
Flow Cytometry: +: Feasible in 100% of the patients
Does not require diagnostic sample
-: Fresh sample (< 24-48 h)
Sensitivity 10-4-10-5
Worlwide acceptability of a common protocol
NGS (Sequenta): +: Sensitivity < 10-6
Frozen samples
Fully standardized (almost FDA-cleared)
-: Requires diagnostic sample (clone ID)
Feasibility ~ 92% (somatic hypermutations)
IFM DFCI 2009 Trial
700 patients < 66y, Newly diagnosed symptomatic MM
3 RVD
5 RVD MEL200 + ASCT
2 RVD
12 months Lenalidomide maintenance
MRD*MRD*
MRD*MRD*
MRD*MRD*
MRD*MRD*
* Primary objective = 7-color Flow, Secondary objective = Molecular
21.01.2016
11
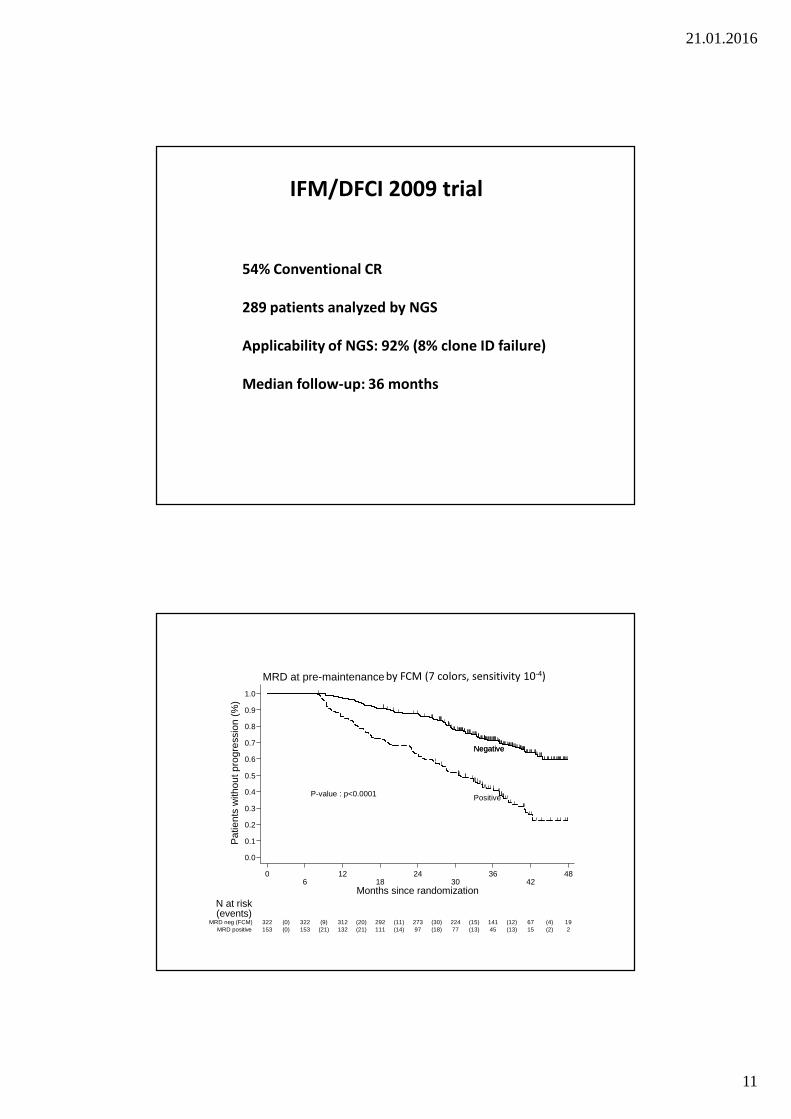
54% Conventional CR
289 patients analyzed by NGS
Applicability of NGS: 92% (8% clone ID failure)
Median follow-up: 36 months
IFM/DFCI 2009 trial
P-value : p<0.0001
NegativeNegative
Positive
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pat
ient
s w
ithou
t pro
gres
sion
(%
)
153 153(0) 132(21) 111(21) 97(14) 77(18) 45(13) 15(13) 2(2)MRD positive322 322(0) 312(9) 292(20) 273(11) 224(30) 141(15) 67(12) 19(4)MRD neg (FCM)
N at risk(events)
06
1218
2430
3642
48
Months since randomization
MRD at pre-maintenance by FCM (7 colors, sensitivity 10-4)

21.01.2016
12
P-value (trend) : p<0.0001
<10-6
[10-6;10-5[
[10-5;10-4[
>=10-4
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
Pat
ient
s w
ithou
t pro
gres
sion
(%
)
79 79(0) 70(9) 59(11) 50(9) 38(11) 28(6) 6(9) 0(3)[10-4;10
-3[
49 49(0) 47(2) 45(2) 43(2) 34(7) 22(4) 8(6) 2(0)[10-5;10
-4[
31 31(0) 30(1) 28(2) 27(0) 22(4) 17(1) 8(2) 4(1)[10-6;10
-5[
87 87(0) 87(0) 85(2) 83(2) 74(6) 54(4) 31(3) 8(0)<10-6
N at risk(events)
06
1218
2430
3642
48
Months since randomization
MRD at pre-maintenance
CONCLUSION
MRD NGS is feasible in 92% of the patients
MRD NGS is highly sensitive (< 10-6)
This sensitivity is achieved in 100% of the patients
10-6 level is the most powerful cutoff for PFS
13/26 pts with t(4;14) achieved MRD negativity vs no with del(17p)
May identify patients cured from myeloma

21.01.2016
13
Prospective Evaluation of MRI and PET-CTat Diagnosis and before Maintenance Therapy
in Symptomatic Patients with Multiple Myeloma Included in the IFM/DFCI 2009 Trial
P.Moreau, M.Attal, L.Karlin, L.Garderet, T.Facon, L.Benboubker, M.Macro, D.Caillot, M.Escoffre-Barbe, A.M.Stoppa, K.Laribi, C.Hulin, G.Marit, J.R.Eveillard,
F.Caillon, C.Bodet-Millin,J.M.Nguyen, B.Pégourié, V.Dorvaux, C.Chaleteix, K.Anderson, P.Richardson, H.Avet-Loiseau,
A.Gaultier, J.M.Nguyen, B.Dupas and F.Bodéré
Rationale
MRI and PET-CT are important imaging techniques to detect bone lesions in multiple myeloma at diagnosis
Both MRI and PET-CT have been described to have pronostic value for PFS and/or OS (at diagnosis, during follow-up)

21.01.2016
14
Few trials have compared prospectively
MRI and PET-CT
in the setting of recent frontline intensive therapy programs
IMAJEM (NCT01309334), 134 patients
RVDx3
RVD x 2
RVD x 5
Revlimid 1 year
Melphalan 200mg/m 2* +
ASCT
CY (3g/m2) MOBILIZATIONGoal: 5 x10 6 cells/kg
RVDx3
CY (3g/m2)MOBILIZATIONGoal: 5 x10 6 cells/kg
Randomize
Revlimid 1 year
ARM A ARM B
ASCT at relapse
PET-CT / MRI at diagnosis
PET-CT / MRI after 3 cycles
PET-CT / MRI before maintenance
21.01.2016
15
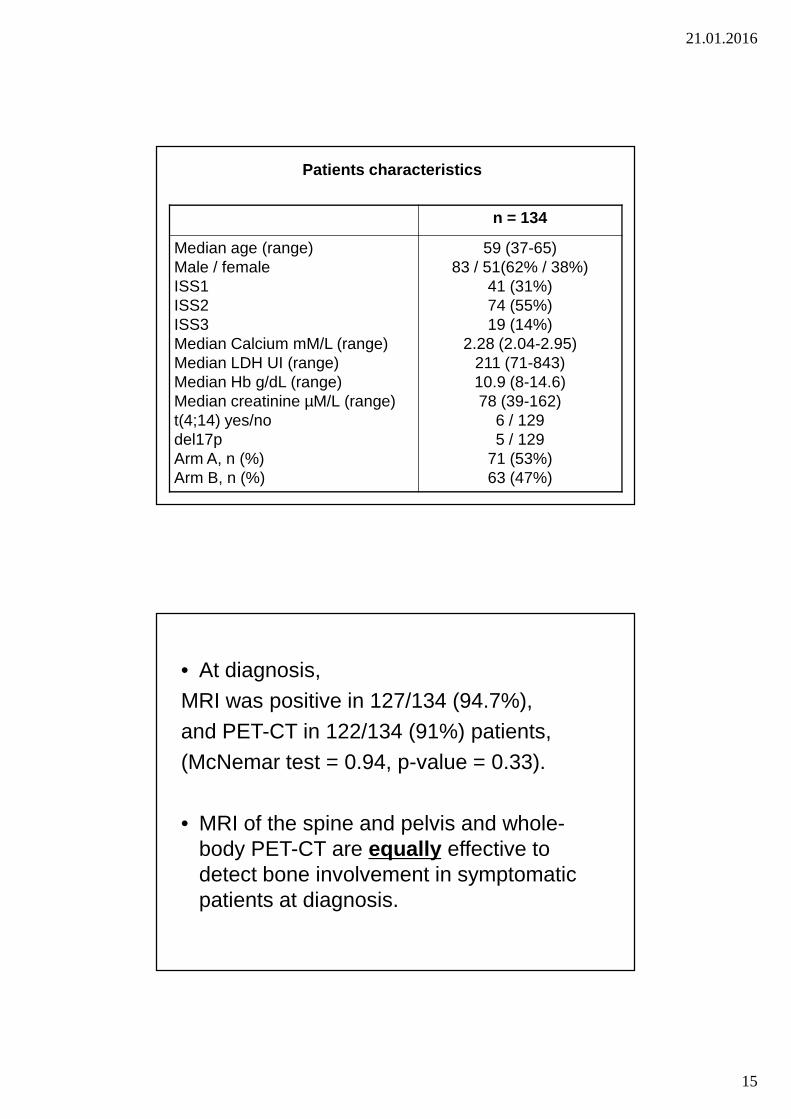
n = 134
Median age (range)Male / femaleISS1ISS2ISS3Median Calcium mM/L (range)Median LDH UI (range)Median Hb g/dL (range)Median creatinine µM/L (range)t(4;14) yes/nodel17pArm A, n (%)Arm B, n (%)
59 (37-65)83 / 51(62% / 38%)
41 (31%)74 (55%)19 (14%)
2.28 (2.04-2.95)211 (71-843)10.9 (8-14.6)78 (39-162)
6 / 1295 / 129
71 (53%)63 (47%)
Patients characteristics
• At diagnosis,MRI was positive in 127/134 (94.7%),and PET-CT in 122/134 (91%) patients,(McNemar test = 0.94, p-value = 0.33).
• MRI of the spine and pelvis and whole-body PET-CT are equally effective to detect bone involvement in symptomatic patients at diagnosis.

21.01.2016
16
Secondary end-point : PROGNOSTIC IMPACT
PET-CT vs MRI
after 3 cycles of induction therapy with RVD
MRI normalisation following 3 cycles of RVD
Impact on PFS (3% normalised)
61.6%
p = 0.29

21.01.2016
17
PET-CT normalisation following 3 cycles of RVD
Impact on PFS (32% normalised)
p = 0.04
78.7%
54.8%
Conclusions
- PET-CT and MRI are equally effective to detect bone involvement in symptomatic patients at diagnosis.
- MRI is not a good imaging method during follow-up
- PET-CT after 3 cycles of RVD and pre-maintenance is a powerful prognostic marker for PFS
- PET-CT pre-maintenance is a powerful prognostic marker for OS
- PET-CT and CMF are complementary tools to evaluate minimal residual disease
21.01.2016
18
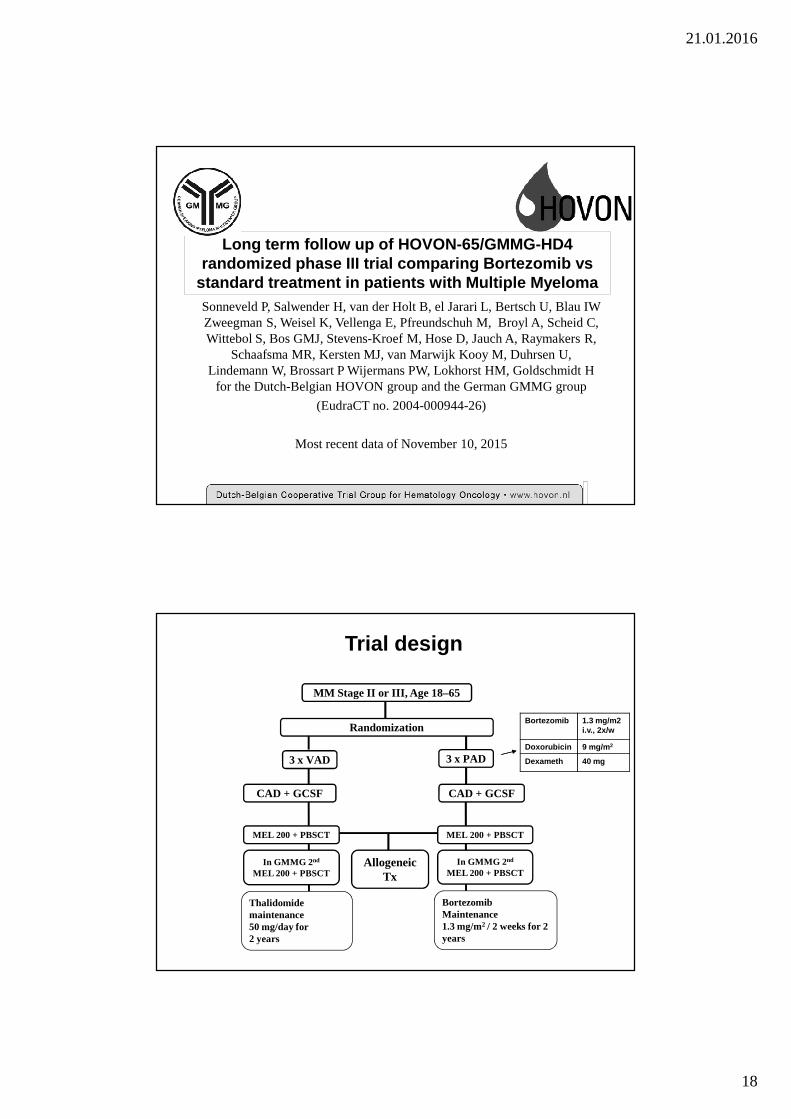
Sonneveld P, Salwender H, van der Holt B, el Jarari L, Bertsch U, Blau IW Zweegman S, Weisel K, Vellenga E, Pfreundschuh M, Broyl A, Scheid C, Wittebol S, Bos GMJ, Stevens-Kroef M, Hose D, Jauch A, Raymakers R,
Schaafsma MR, Kersten MJ, van Marwijk Kooy M, Duhrsen U, Lindemann W, Brossart P Wijermans PW, Lokhorst HM, Goldschmidt H
for the Dutch-Belgian HOVON group and the German GMMG group
(EudraCT no. 2004-000944-26)
Most recent data of November 10, 2015
Long term follow up of HOVON-65/GMMG-HD4 randomized phase III trial comparing Bortezomib vs
standard treatment in patients with Multiple Myelom a
Randomization
MM Stage II or III, Age 18–65
CAD + GCSF
3 x VAD
CAD + GCSF
3 x PAD
MEL 200 + PBSCT
In GMMG 2 nd
MEL 200 + PBSCT
MEL 200 + PBSCT
In GMMG 2 nd
MEL 200 + PBSCT
Thalidomidemaintenance50 mg/day for 2 years
Allogeneic Tx
Bortezomib Maintenance1.3 mg/m2 / 2 weeks for 2 years
Trial design
Bortezomib 1.3 mg/m2i.v., 2x/w
Doxorubicin 9 mg/m 2
Dexameth 40 mg

21.01.2016
19
A: VADB: PADCox LR Stratified P =0.001
N414413
F324300
A: VADB: PAD
10 Nov 2015
At risk:414413
202240
101123
4977
1830
A: VAD
B: PAD
0
25
50
75
100
Cum
ulat
ive
perc
enta
ge
months0 24 48 72 96
Randomization armProgression free survival
Primary endpoint PFS by treatment arm
PFS at 96m: 17% vs 10%HR:0.77, 95% confidence interval (CI) = 0.65-0.90; P = 0.001
A: VADB: PADCox LR Stratified P =0.22
N414413
D217204
A: VADB: PAD
10 Nov 2015
At risk:414413
327341
261278
199231
8488
A: VAD
B: PAD
0
25
50
75
100
Cum
ulat
ive
perc
enta
ge
months0 24 48 72 96
Randomization armOverall survival
OS by treatment arm
OS at 96m: 48% vs 45%HR: 0.87, 95% C.I. 0.71-1.04; P=0.22
RMST8y: 4.8 months (95% CI 0.2-9.5; P=0.04)

21.01.2016
20
PAD vs VAD response
PFSHR
P-value OSHR
P-value
Treatment arm 0.75 0.000 0.86 0.11
ISS 1.18 0.006 1.20 0.02
LDH > n 1.26 0.04 1.55 0.000
RI 1.11 0.5 1.58 0.07
double HDM 0.90 0.2 0.79 0.02
del/13q KA 1.28 0.02 1.52 < 0.001
IgA 1.60 0.000 1.70 <0.01
Multivariate Cox regression analysis
Original observation : single vs double ASCT
Rel Risk P-value
Treatment
VAD single HDT HR 1.00 Ref.
PAD single HDT HR 0.86 ns
VAD double HDT HR 0.88 ns
PAD double HDT HR 0.57 0.0005
Sonneveld P, et al. Blood. 2013;122: abstract 404. Updated data presented at ASH 2013.

21.01.2016
21
HOVON-VADHOVON-PADGMMG-VADGMMG-PAD
N213219201194
D1191239881
HOVON-VADHOVON-PADGMMG-VADGMMG-PAD
10 Nov 2015
At risk:213219201194
164179163162
137144124134
10512494
107
50463442
HOVON-VAD
HOVON-PADGMMG-VAD
GMMG-PAD
0
25
50
75
100C
umul
ativ
e pe
rcen
tage
months0 24 48 72 96
Study group + treatment armOverall survivalOS by study group and by
treatment arm
OS by study group and by treatment armHOVON: single HDM/ASCTGMMG: double HDM/ASCT
PAD + Single vs Double HDM/ASCT at 96 m: 42% vs 55%Cox all arms: HR:0.71, 95%, (CI) = 0.54-0.94; P = 0.018
NoYesCox LR P <.001
N368
45
F28439
No
Yes
20 Nov 2015
At risk:36845
18714
974
47
2
17
1
No
Yes0
25
50
75
100
Cum
ulat
ive
perc
enta
ge
months0 24 48 72 96
Renal impairment at entry (arm A:VAD)Progression free survival (censored at allo-SCT)
NoYesCox LR P =0.62
N37636
F274
25
No
Yes
20 Nov 2015
At risk:37636
21722
11112
689
26
4
No
Yes
0
25
50
75
100
Cum
ulat
ive
perc
enta
ge
months0 24 48 72 96
Renal impairment at entry (arm B:PAD)Progression free survival (censored at allo-SCT)
PFS by treatment armSubgroup with renal impairment
VAD PAD
p<0.001 p: 0.6

21.01.2016
22
NoYesCox LR P <.001
N368
45
D17838
No
Yes
20 Nov 2015
At risk:36845
30521
248
12
191
7
812
No
Yes
0
25
50
75
100
Cum
ulat
ive
perc
enta
ge
months0 24 48 72 96
Renal impairment at entry (arm A:VAD)Overall survival
NoYesCox LR P =0.68
N37636
D186
18
No
Yes
20 Nov 2015
At risk:37636
312
28
252
25
213
17
83
5
No
Yes
0
25
50
75
100
Cum
ulat
ive
perc
enta
gemonths0 24 48 72 96
Renal impairment at entry (arm B:PAD)Overall survival
OS by treatment armSubgroup with renal impairment
PADVAD
p<0.001 p: 0.6
At 96m: 12 vs 42 % At 96m: 47 vs 48 %
Conclusions
• Bortezomib based treatment improves PFS and OS in
patients with newly diagnosed MM who are transplant
candidates. This benefit is confirmed at long follow-up.
• Bortezomib plus double HDM/ASCT improves OS at 96
months from 42% to 55%
• Subgroup analysis indicates that:
• Prolonged Bortezomib treatment mostly abrogates
del(17/17p) effect on PFS and OS
• Limited benefit is observed in t(4;14) and gain(1q)
• Prolonged Bortezomib largely abrogates the negative
prognosis in patients with renal impairment

21.01.2016
23
symptomatic MM 1st line treatment
18-70a
3 x PAd
Lenalidomide
for 2 years
CAD + leukapheresis
3 x VCD
HDM + TPL
2. HDM + TPL (if no nCR/CR)
2 x Lenalidomide
Randomization
Lenalidomide
for 2 years
Lenalidomideif no CR
Lenalidomideif no CR
A1 B1 A2 B2
A1 + B1 A2 + B2
1) 1)
MM5-Trial
Flowsheet 31.03.20111) High Risk Patients, optional in Phase II trial
Standard intensification according to local protocol (GMMG standard)
1) Revlimid ® (Lenalidomide) 25mg p.o., day 1-21; Dexamethasone 40mg p.o., day 1, 8, 15, 222) stem cell mobilization only if no useable stem cells from earlier mobilization are available 3) Revlimid ® (Lenalidomide) - maintenance 10mg/dayR-Revlimid ® (Lenalidomide), d-Dexamethasone, HD Mel - high dose chemotherapy Melphalan, Auto Tx - autologous stem cell transplantation
Relapsed Multiple Myeloma (1 st - 3rd relapse)age 18-75 years
3x Rd 1)
Cyclophosphamide + G-CSFstem cell collection 2)
3x Rd 1)
Rd 1)
until progressive disease
Randomization
Cylophosphamide + G-CSFstem cell collection 2)
HD Mel 200mg/m²+ autologous transplantation
R-maintenance 3)
until progressive disease
for patients with progressive disease HD Mel + Auto Tx recommended
(outside this trial)
ReLApsE trial282 patients

21.01.2016
24
Thank You for Your Attention!
Related Documents











