Prevention Science, Vol. 3, No. 2, June 2002 ( C 2002) Positive Impact of Competence Skills and Psychological Wellness in Protecting Inner-City Adolescents From Alcohol Use Jennifer A. Epstein, 1,2 Kenneth W. Griffin, 1 and Gilbert J. Botvin 1 Research has shown that competence enhancement prevention programs for substance use are effective in reducing alcohol use and other problem behaviors. However, less is known about the mechanisms by which high competence helps youth avoid negative outcomes. This study explored whether greater competence is associated with increased levels of psycholog- ical wellness that in turn deters subsequent alcohol use. Specifically, 1,459 students attending 22 middle and junior high schools in New York City completed surveys that included mea- sures of competence (decision making, self-efficacy), psychological wellness, and alcohol use. Students completed surveys at baseline, 1-year follow-up, and 2-year follow-up. Data collec- tors administered the questionnaire following a standardized protocol during a regular 40-min class period. On the basis of a longitudinal structural equation model, adolescents who were highly competent reported greater psychological wellness, which was then associated with less drinking. These findings highlight the potential of alcohol prevention programs designed to enhance competence and psychological wellness. KEY WORDS: alcohol use; adolescents; psychological wellness; personal competence. INTRODUCTION Alcohol use among teenagers remains a press- ing national problem. Most young people in junior and senior high school use alcohol, in terms of ei- ther experimental use or heavier levels of use. On the basis of the national Monitoring the Future sur- vey, 80% of high school seniors have used alcohol and over 62% have been drunk; moreover, among eighth graders 52% have used alcohol and 25% re- port having been drunk (Johnston et al., 2000). These figures are important because there are a variety of negative consequences resulting for adolescent alco- hol use. For example, another survey of high school seniors and dropouts indicated that more than half 1 Institute for Prevention Research, Weill Medical College, Cornell University, New York. 2 Correspondence should be directed to Jennifer A. Epstein, PhD, Institute for Prevention Research, Weill Medical College, Cornell University, 411 East 69th Street, New York, New York 10021; e-mail: [email protected]. experienced negative consequences of drinking such as feeling sick, missing school or work, getting ar- rested, or being in an automobile accident (Ellickson et al., 1996). Research on the etiology and prevention of al- cohol use is important in increasing our ability to ad- dress this important problem among adolescents. In addition to pointing to the importance of social influ- ences to drink, theory and research have begun to rec- ognize that expanding young people’s skills repertoire is an important way to promote health-enhancing be- havior (Perry & Jessor, 1985). Based on social learning theory (Bandura, 1986) and problem behavior theory (Jessor & Jessor, 1977), the competence enhancement approach to prevention posits that a lack of general social and personal skills for coping with life increases vulnerability to internal and external influences that promote alcohol use and other problem behaviors. According to this approach, alcohol use is viewed as a socially learned, purposeful, and functional behav- ior from the viewpoint of the adolescent with poor competence skills (Botvin, 1998). 95 1389-4986/02/0600-0095/1 C 2002 Society for Prevention Research

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
P1: GNI/GLS/GKJ P2: GDR
Prevention Science [PREV] PP481-373224 May 1, 2002 9:34 Style file version Nov. 04, 2000
Prevention Science, Vol. 3, No. 2, June 2002 ( C© 2002)
Positive Impact of Competence Skills and PsychologicalWellness in Protecting Inner-City AdolescentsFrom Alcohol Use
Jennifer A. Epstein,1,2 Kenneth W. Griffin,1 and Gilbert J. Botvin1
Research has shown that competence enhancement prevention programs for substance useare effective in reducing alcohol use and other problem behaviors. However, less is knownabout the mechanisms by which high competence helps youth avoid negative outcomes. Thisstudy explored whether greater competence is associated with increased levels of psycholog-ical wellness that in turn deters subsequent alcohol use. Specifically, 1,459 students attending22 middle and junior high schools in New York City completed surveys that included mea-sures of competence (decision making, self-efficacy), psychological wellness, and alcohol use.Students completed surveys at baseline, 1-year follow-up, and 2-year follow-up. Data collec-tors administered the questionnaire following a standardized protocol during a regular 40-minclass period. On the basis of a longitudinal structural equation model, adolescents who werehighly competent reported greater psychological wellness, which was then associated with lessdrinking. These findings highlight the potential of alcohol prevention programs designed toenhance competence and psychological wellness.
KEY WORDS: alcohol use; adolescents; psychological wellness; personal competence.
INTRODUCTION
Alcohol use among teenagers remains a press-ing national problem. Most young people in juniorand senior high school use alcohol, in terms of ei-ther experimental use or heavier levels of use. Onthe basis of the national Monitoring the Future sur-vey, 80% of high school seniors have used alcoholand over 62% have been drunk; moreover, amongeighth graders 52% have used alcohol and 25% re-port having been drunk (Johnston et al., 2000). Thesefigures are important because there are a variety ofnegative consequences resulting for adolescent alco-hol use. For example, another survey of high schoolseniors and dropouts indicated that more than half
1Institute for Prevention Research, Weill Medical College, CornellUniversity, New York.
2Correspondence should be directed to Jennifer A. Epstein, PhD,Institute for Prevention Research, Weill Medical College, CornellUniversity, 411 East 69th Street, New York, New York 10021;e-mail: [email protected].
experienced negative consequences of drinking suchas feeling sick, missing school or work, getting ar-rested, or being in an automobile accident (Ellicksonet al., 1996).
Research on the etiology and prevention of al-cohol use is important in increasing our ability to ad-dress this important problem among adolescents. Inaddition to pointing to the importance of social influ-ences to drink, theory and research have begun to rec-ognize that expanding young people’s skills repertoireis an important way to promote health-enhancing be-havior (Perry & Jessor, 1985). Based on social learningtheory (Bandura, 1986) and problem behavior theory(Jessor & Jessor, 1977), the competence enhancementapproach to prevention posits that a lack of generalsocial and personal skills for coping with life increasesvulnerability to internal and external influences thatpromote alcohol use and other problem behaviors.According to this approach, alcohol use is viewed asa socially learned, purposeful, and functional behav-ior from the viewpoint of the adolescent with poorcompetence skills (Botvin, 1998).
951389-4986/02/0600-0095/1 C© 2002 Society for Prevention Research

P1: GNI/GLS/GKJ P2: GDR
Prevention Science [PREV] PP481-373224 May 1, 2002 9:34 Style file version Nov. 04, 2000
96 Epstein, Griffin, and Botvin
Youth typically begin to acquire a variety of so-cial and personal competence skills (e.g., decisionmaking, assertiveness, self-control, etc.) during child-hood, and as they mature these skills increase. Byadolescence, most young people have acquired arepertoire of skills learned through a combinationof modeling and reinforcement. The development ofsocial and personal skills depends upon having op-portunities to observe, practice, and master them andto build one’s self-efficacy in being able to use theseskills. However, youth with poor competence skillsmay fail at various developmental tasks (e.g., aca-demic or interpersonal) and in turn drink alcohol as analternative means of achieving popularity, social sta-tus, or self-esteem. Therefore, enhancing competenceskills has been posited as a means of helping ado-lescents meet developmental challenges and avoid avariety of negative outcomes (Masten & Coatworth,1998; Masterpasqua, 1989). In fact, a large bodyof research indicates that competence enhancementprograms designed to prevent alcohol and other druguse using life skills training have been highly effectivein reducing drug and alcohol use (Botvin, 2000). Onesuch drug abuse prevention study found long-term ef-fectiveness up to 6 years after the intervention withadolescents residing in New York State who were pre-dominantly White (Botvin et al., 1995a). Anotherstudy utilizing the competence enhancement ap-proach found lower alcohol use among inner-cityyouth who were predominantly Black and Hispanic(Botvin et al., 1995b).
Etiology studies have shown that early initiationof alcohol use is more likely among youth with poorcompetence skills. For example, a study of elemen-tary school youth showed that those scoring poorly onself-reported and teacher-rated measures of compe-tence were more likely to drink alcohol (Jackson et al.,1997). Other studies have shown that the majority ofadolescent nondrinkers score in the competent to verycompetent range on social skills (Hover & Gaffney,1991), whereas deficient social skills predicted alcoholinvolvement (Gaffney et al., 1998).
Broad Conceptualizations of Health
Examining multiple domains of prevention in-cluding mental health and drug use reveals a commonset of risk and protective factors influencing adoles-cents (Durlak, 1997). Broad skills may affect a varietyof health behaviors by improving social competence,coping skills, and self-esteem (Kolbe, 1997). In the
mental health field, some prevention programs em-phasize enhancing competence to promote psycho-logical wellness (Cowen, 1994). Specifically, Cowensuggested five pathways to psychological wellness:(1) forming wholesome early attachment, (2) acquir-ing age and ability appropriate competencies, (3) en-gineering settings that promote adaptive outcomes,(4) fostering empowerment, and (5) acquiring skillsneeded to cope effectively with life stressors. In addi-tion to competence, emotional profile has been iden-tified as a protective factor for adolescent alcoholuse (Pandina, 1998). For example, poor psycholog-ical wellness was found to predict problem drinking5 years later in a study of Finnish adolescents followedto young adulthood (Pitkaenen, 1999), and anotherstudy found that positive mood was inversely relatedto tobacco, alcohol, and marijuana use among urbanadolescents (Wills et al., 1995).
Although comprehensive skills programs de-creased adolescent alcohol use, research must deter-mine why these types of interventions are effective.Because a variety of factors can lower effectivenessof an intervention (Resnicow & Botvin, 1993), longi-tudinal etiologic research is a useful means of testingthe theory behind the interventions. This study onlyincluded adolescents from the control group of a pre-vention trial. By examining the naturally occurringprocesses, it is possible to develop an increased under-standing of how competence enhancement programsoperate. In one such longitudinal investigation usingthe same sample as this study, greater levels of generalcompetence enabled adolescents to engage in morefrequent drug-specific refusal skills that in turn de-terred subsequent alcohol use (Epstein et al., 2000c).This model was replicated in a similar investigation ofcigarette smoking (Epstein et al., 2000a). Of course,general competence may affect other important pro-cesses. In another study with the same sample, lowerlevels of general competence were related to the per-ceived social benefits of smoking that then increasedadolescent smoking (Epstein et al., 2000b). However,these earlier investigations did not focus on mentalhealth.
This study tested whether broader competence(i.e., decision-making skills and self-efficacy) affectsmental health (i.e., psychological wellness). Thesemeasures of competence correspond to the path-ways Cowen (1994) identified as acquiring age andability appropriate competencies and acquiring skillsneeded to cope effectively with life stressors. Highlevels of psychological wellness should protect adoles-cents from alcohol use. It is predicted that adolescents

P1: GNI/GLS/GKJ P2: GDR
Prevention Science [PREV] PP481-373224 May 1, 2002 9:34 Style file version Nov. 04, 2000
Wellness Protects Youth From Alcohol Use 97
with greater competence (who most likely enjoy moremastery and success in their lives) will experiencehigher levels of psychological wellness, which makesthem less likely to drink alcohol. A model will betested to determine if (1) greater competence rep-resented by measures of decision making and self-efficacy collected in the 1st year of middle or juniorhigh school enhances psychological wellness mea-sured in the 2nd year of middle or junior high schooland (2) this increased psychological wellness is asso-ciated with less alcohol use in the 3rd year of middleor junior high school controlling for earlier alcoholuse. This would help elucidate whether competenceenhancement programs also increase psychologicalwellness.
METHOD
Overview
Participants in this study were from the controlschools of a longitudinal smoking prevention trialconducted in 47 schools (described in greater de-tail in Botvin et al., 1992). A total of 22 middle andjunior high schools in New York City with 25% ormore Hispanic students participated in this study.These schools served students from families with aver-age incomes below the Federal poverty level. All sixthand seventh graders in English-speaking, mainstreamclasses were eligible to participate by completing thestudy questionnaires. Approximately 90% of eligiblestudents completed the initial baseline survey. Stu-dents also completed surveys at a 1-year follow-up,and a 2-year follow-up. Consent procedures were ap-proved by the Institutional Review Board at CornellUniversity Medical College.
Participants
At baseline, 2,400 students completed question-naires. The panel sample across baseline, 1-yearfollow-up, and 2-year follow-up consisted of 1,459 stu-dents (61% of baseline participants). The retentionrate over the course of the 3-year study comparedfavorably with school-based studies whose 2-yearfollow-up rates ranged from 60% (Botvin et al., 1995b)to 79% (Snow & Tebes, 1992). The mean age at base-line for the panel sample was 12.4 (SD = 0.75), andthe sample was 46% boys. In terms of ethnicity, thissample was 54% Hispanic, 20% Black, 7% Asian,
16% White, and 3% other. Approximately 70% ofrespondents lived in two-parent households.
Procedure
Participating students completed questionnairesthat measured self-reported drinking and several psy-chological factors hypothesized to be related to drink-ing initiation. Surveys were administered accordingto a standardized protocol during a regular 40-minclass period by a team of three to five data collectorsof the same ethnic groups as participants. Studentswere assured that their answers would remain confi-dential, and classroom teachers were not involved indata collection activities. Student identification codeswere used rather than names to emphasize the confi-dential nature of the surveys.
Measures
Questionnaires included items that assessedstudents’ drinking behavior, self-efficacy, decision-making skills, and psychological wellness. Because themeasures had originally been developed for use withWhite, middle-class students, the individual scaleswere pilot-tested and revised based on the results of aprevious study that examined their suitability for thetarget population (Botvin et al., 1989). The reliabili-ties (Cronbach’s alpha) for the scales relevant to thisstudy are indicated below.
Alcohol Consumption
A dichotomous (yes/no) item assessed whetherthe participant had “had a drink of alcohol in thelast month.” Drinking frequency and drunkennessfrequency were assessed with a 9-point drinkingscale. Specifically, students responded to the ques-tion, “How often (if ever) do you drink alcoholic bev-erages?” with the following response options: Never(1), Tried them, but don’t use them now (2), Less thanonce a month (3), Once a month (4), Two or threetimes a month (5), Once a week (6), Few times a week(7), Once a day (8) and More than once a day (9). Par-ticipants responded to “How often (if ever) do youget drunk?” with the following response options: Idon’t drink (1), I drink but never get drunk (2), Lessthan once a month (3), Once a month (4), Two or threetimes a month (5), Once a week (6), Few times a week(7), Once a day (8), More than once a day (9). Students

P1: GNI/GLS/GKJ P2: GDR
Prevention Science [PREV] PP481-373224 May 1, 2002 9:34 Style file version Nov. 04, 2000
98 Epstein, Griffin, and Botvin
rated the quantity of drinking per drinking occasionon a 6-point scale: I don’t drink (1), 1 drink (2), 2 drinks(3), 3 or 4 drinks (4), 5 or 6 drinks (5), and More than6 drinks (6).
Decision-Making
Five items derived from a subscale of the Cop-ing Inventory (Wills, 1986) related to problem-solving and direct action measured decision-makingskills (α = .80). These items assessed sound decision-making skills (e.g., “When I have a problem I thinkabout which of the alternatives is best”). Responseswere rated on a 5-point scale ranging from 1 (never)to 5 (almost always).
Self-Efficacy
Five items from the personal efficacy subscale ofthe Spheres of Control Scale (Paulhus, 1983) assessedSelf-Efficacy (α = .75). This scale measured the ex-tent to which respondents believed they could achievepersonal goals through their own efforts (e.g., “I canlearn almost anything if I set my mind to it”). Re-sponses were scored on a 5-point Likert Scales rang-ing from 1 (strongly disagree) to 5 (strongly agree).
Psychological Wellness
Four items (α = .77) from the Mental HealthInventory (Veit & Ware, 1983) assessed psychologicalwellness (e.g., “I generally enjoyed the things that Idid”). Each item had response options on a 5-pointLikert Scale ranging from 1 (None of the time) to5 (Most of the time), and students responded with atime of “over the last month.”
Data Analysis
The EQS program (Bentler, 1995) was used forthe confirmatory factor analysis (CFA) and structuralequations modeling (SEM) analyses. First, a CFAmodel was examined to determine how well the ob-served measures reflect the hypothesized latent con-structs (decision making, self-efficacy, psychologicalwellness, and drinking). Next, an SEM was testedto examine the relationships between the predictorlatent factors (Decision-Making, Self-Efficacy, and
Psychological Wellness) and outcome Drinking latentfactor. The SEM differs from the CFA model in thatpath coefficients for the hypothesized direction of re-lationships among the latent factors are calculated.A saturated model was tested (as recommended byMacCallum et al., 1992) that estimated the paths fromall exogenous latent factors to the construct of Psy-chological Wellness and to the Two-Year Follow-UpDrinking latent factor. In addition, the covariancesamong all exogenous latent factors were estimatedin testing the saturated model. The error terms foreach matching drinking indicator at baseline and the2-year follow-up were initially freely estimated be-cause it was expected that measurement error wouldbe similar. This was true for drinking frequency anddrinking quantity; thus, these correlated errors werefreely estimated.
The following criteria were used to evaluate theoverall fit of the CFA model and subsequent SEMs:(1) the chi-square p value, which if p > .05 indicatesthat there are no statistically significant discrepan-cies between the observed data and the hypothesizedmodel; (2) the chi-square to degree of freedom ratio,which should be less than 5.0 (Bollen, 1989); (3) thestandardized root mean squared residual (SRMR),which should be less than .05; and (4) the Compara-tive Fit Index (CFI). The CFI is derived by comparingthe predicted covariation in the hypothesized modelto that of the null model after adjusting for samplesize. CFI values greater than .90 indicate a good fit ofthe model to the data.
RESULTS
According to the first survey, 41% of studentsreported trying alcohol and 21% drank in the pastmonth. Alcohol use escalated from baseline (sixth andseventh grade) to the 2-year follow-up (eighth andninth grade). At the 2-year assessment, 60% of stu-dents reported trying alcohol at least once and 24%reported drinking in the past month.
Attrition Analyses
Mean differences on the alcohol measures be-tween panel and dropout students over the course ofthe study were tested. No differences were found forthe frequency of drinking between panel and dropoutsat the 1-year follow-up, but at the 2-year follow-up dropouts drank more often (M = 1.74) than the

P1: GNI/GLS/GKJ P2: GDR
Prevention Science [PREV] PP481-373224 May 1, 2002 9:34 Style file version Nov. 04, 2000
Wellness Protects Youth From Alcohol Use 99
panel sample, M = 1.64; F(1, 2353) = 4.61, p < .05.In addition, dropouts at the 1-year follow-up dranka greater quantity of alcohol per occasion com-pared with the panel students, Ms = 1.47 vs. 1.40;F(1, 2362) = 3.88, p < .05, and dropouts at the 2-yearfollow-up drank more than panel students, Ms = 1.49vs. 1.37; F(1, 2362) = 16.20, p < .001. There was nodifference in drunkenness between dropouts at the1-year follow-up and panel students. Dropouts atthe 2-year follow-up were drunk more frequentlythan panel students, Ms = 1.36 vs. 1.28; F(1, 2363) =9.94, p < .05. The association between attrition anddrinking at least once a month was tested and no dif-ferences were found. Thus there was only a small ef-fect due to participant loss based on the continuousalcohol use measures and no differential loss based onthe proportional analyses. Dropouts had lower com-posite self-efficacy scores (M = 19.51) than panel stu-dents, (M = 20.16); F(1, 1933) = 15.11, p < .001, butno significant differences in decision-making skills. Inthis study, we acknowledge that caution is warrantedin generalizing any findings, in particular to those whowere heavier drinkers and less efficacious.
To examine differential attrition by gender andethnicity, mean differences on the three baseline al-cohol measures were tested between students who re-mained in the sample and those who did not. Theseanalyses indicated that there was not any differen-tial attrition by gender or ethnicity on the alcoholmeasures.
Regressions with retention status as a dependentmeasure (dropouts were coded as 0, and panel sam-ple members were coded as 1) with the alcohol andpsychosocial measures as predictors were run as inpast work (e.g., Scheier & Botvin, 1998). Althoughseveral predictors (drink in past month, drinkingquantity, and self-efficacy) were significant (p < .05),the regression model only accounted for 2% of thevariance.
Treatment of Missing Data
Of the original panel sample of 1,459 students,22 cases were missing 12 or more of the items rele-vant to this study and as a consequence were elim-inated from the final sample (N = 1,438). Completedata for all relevant items was available from 969 stu-dents. Listwise deletion is considered inefficient be-cause of the discarding of potentially useful data, andprocedures to maximize the available data are recom-mended (Bentler, 1995). Furthermore, Graham et al.
(1997) point out that prevention data are rarely miss-ing completely at random and that there are severalreasons why missing data imputation should be usedeven when the missingness mechanism is inaccessibleor unmeasured. For example, imputation results inless biased results than other more traditional meth-ods such as complete case analysis or analysis withpairwise deletion. Consequently, a full-informationmaximum likelihood regression-based procedure wasused to impute missing data points (Wothke, 1998).Using this procedure, missing values for a particularvariable were calculated based on a regression analy-sis using the remaining variables, as well as gender andacademic performance, as predictors. This procedurewas completed for all 20 variables involved, includ-ing the alcohol outcome measures. It should be notedthat the vast majority of participants with missing datahad very few missing items (102 had only 1 item miss-ing, 248 had only 2–5 items missing). Thus only about8% of the final sample was originally missing morethan five items prior to imputation. In addition, forthe alcohol outcome items the number of individu-als missing any data was very low (between 8 and15 cases).
Confirmatory Factor Analysis
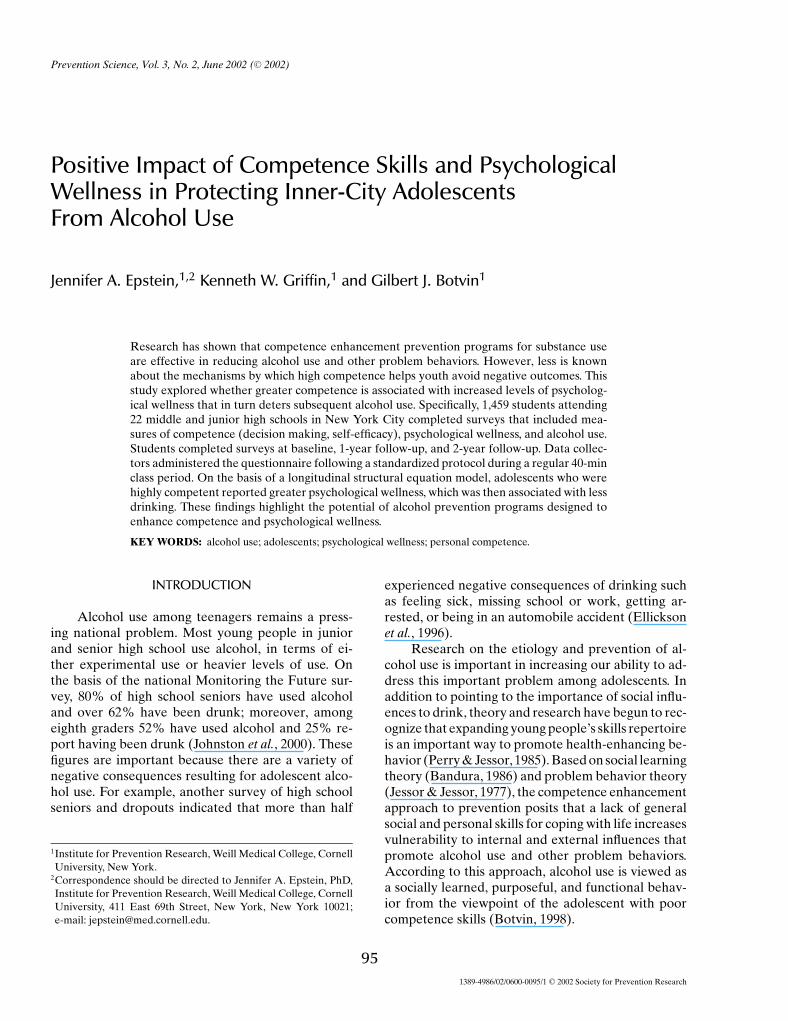
Figure 1 shows the five latent factors specified inthe CFA or measurement model. Each one had fourindicator items. Three latent factors were measuredat the baseline assessment (sixth or seventh grade):loadings for Baseline Drinking ranged from .71 to .87;those for Decision-Making ranged from .60 to .70,and those for Self-Efficacy ranged from .52 to .75.The Psychological Wellness latent factor measured1 year later (seventh or eighth grade) had loadingsthat ranged from .61 to .79. The Two-Year Follow-Up Drinking latent factor (eighth or ninth grade) hadloadings that ranged from .72 to .87. Factor loadingsfor all latent constructs were in the expected direc-tion and highly significant (all ps < .001). Therefore,the measurement model was properly specified, andeach factor was statistically reliable based on thehypothesized model.
The CFA model was a good-to-excellentfit, χ2(158, N = 1,437) = 508, p < .001;χ2/df = 3.2;SRMR = .031; CFI = .97. Although the chi-squarep value was significant (which indicates that addi-tional models could be fit to the data), this is notuncommon with large models and large sample sizes(Bentler & Bonnett, 1980; Marsh et al., 1988).
P1: GNI/GLS/GKJ P2: GDR
Prevention Science [PREV] PP481-373224 May 1, 2002 9:34 Style file version Nov. 04, 2000
100 Epstein, Griffin, and Botvin
Fig. 1. Confirmatory factor analysis model. Large circles represent latent constructs, rectanglesare measured variables, and single-headed arrows designate residual variances.
Table 1 presents the latent factor intercorre-lations based on the CFA model. The strongestrelationship was between Baseline Drinking and Two-Year Follow-Up Drinking (r = .46, p < .001). Base-line Decision-Making and Self-Efficacy were alsostrongly associated (r = .31, p < .001). PsychologicalWellness was significantly correlated with each of theother latent factors in the expected directions. Con-sequently, according to the CFA, the measurement
Table 1. Correlations Among Latent Factors From ConfirmatoryFactor Analysis
Latent factor 1 2 3 4 5
1. Baseline Drinking —2. Decision-Making −.11∗∗ —3. Self-Efficacy −.02 .31∗∗∗ —4. Psychological −.11∗∗ .18∗∗∗ .14∗∗∗ —
Wellness5. Two-Year Drinking .46∗∗∗ −.08∗ −.01 −.19∗∗∗ —
Note. ∗ p < .05. ∗∗ p < .01. ∗∗∗ p < .001.
model was good and had high factor loadings for allindicator variables.
Structural Equations Modeling
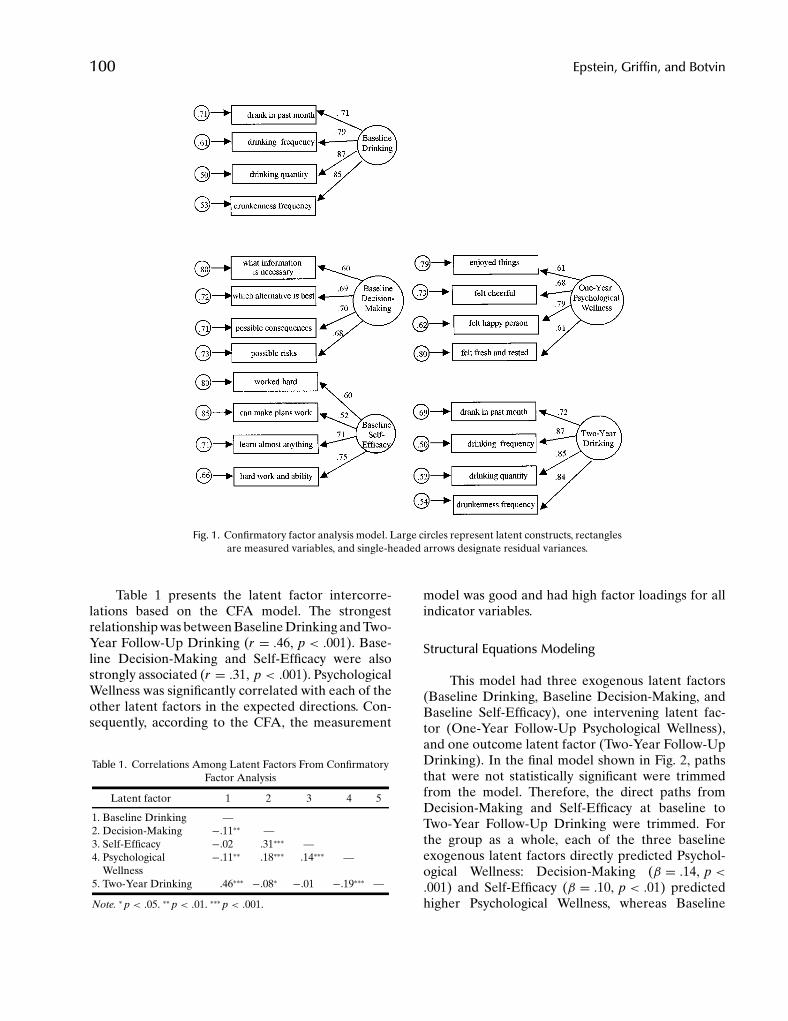
This model had three exogenous latent factors(Baseline Drinking, Baseline Decision-Making, andBaseline Self-Efficacy), one intervening latent fac-tor (One-Year Follow-Up Psychological Wellness),and one outcome latent factor (Two-Year Follow-UpDrinking). In the final model shown in Fig. 2, pathsthat were not statistically significant were trimmedfrom the model. Therefore, the direct paths fromDecision-Making and Self-Efficacy at baseline toTwo-Year Follow-Up Drinking were trimmed. Forthe group as a whole, each of the three baselineexogenous latent factors directly predicted Psychol-ogical Wellness: Decision-Making (β = .14, p <.001) and Self-Efficacy (β = .10, p < .01) predictedhigher Psychological Wellness, whereas Baseline
P1: GNI/GLS/GKJ P2: GDR
Prevention Science [PREV] PP481-373224 May 1, 2002 9:34 Style file version Nov. 04, 2000
Wellness Protects Youth From Alcohol Use 101
Fig. 2. Structural equations model. Large circles represent latent factors, and small circles withnumbers reflect residual variances.
Drinking predicted lower Psychological Wellness(β = −.09, p < .01). Further, One-Year Psycholog-ical Wellness predicted less Two-Year Follow-UpDrinking (β = −.14, p < .001). Lastly, as expected,Baseline Drinking predicted Two-Year Follow-UpDrinking (β = .44, p < .001). In terms of goodness-of-fit indices, there was an excellent fit of themodel to the data, χ2(160, N = 1,437) = 508.9, p <.001;χ2/df = 3.2; SRMR = .032; CFI = .97. Thus thethree exogenous latent factors significantly predictedpsychological wellness that then predicted drinking atthe 2-year follow-up.
Multigroup Analysis
A gender multigroup SEM analysis was also con-ducted. An ethnic multigroup analysis was not run be-cause of insufficient power. For the gender multigroupSEM, the paths were constrained to be equal basedon the assumption that there were no differences be-tween the two groups. However, it was necessary tofreely estimate the path between decision making andpsychological wellness because of a gender difference.Decision making significantly predicted psychologi-cal wellness for boys (β = .15, p < .001) but not for
girls (β = .06). All other paths were invariant acrossgender.
DISCUSSION
Competence skills had an indirect negative asso-ciation with subsequent alcohol use through psycho-logical wellness. Students who felt more competent(as measured by decision making and self-efficacy)reported higher positive mental health (as measuredby psychological wellness) that in turn protectedthese adolescents from subsequent alcohol behav-ior. Earlier research determined such general com-petence was an important building block for drug-related refusal assertiveness skills that then deterredadolescent drinking (Epstein et al., 2000c). The find-ings from the present study are consistent withprevious work showing that competence skills andpsychological well-being are protective in terms ofadolescent substance use (Griffin et al., 2002). Thisstudy expands on this work providing support forthe theory underlying the competence enhancementapproach to adolescent alcohol prevention. In bothcases, models were tested among adolescents who didnot receive a prevention program and these findings
P1: GNI/GLS/GKJ P2: GDR
Prevention Science [PREV] PP481-373224 May 1, 2002 9:34 Style file version Nov. 04, 2000
102 Epstein, Griffin, and Botvin
applied to a predominantly minority sample of urbanyouth. It is important to study this population to elu-cidate how to develop effective alcohol preventionprograms for them.
Competence enhancement approaches have ahistory of effectiveness in preventing adolescent al-cohol use (Botvin, 2000). These programs emphasizethe teaching of personal and social skills includingsound decision-making skills and methods to en-hance self-efficacy. Yet other competence enhance-ment approaches have been designed to focus pri-marily on mental health outcomes (Weissberg &Greenberg, 1998; Zins et al., 2000). According to ameta-analysis of primary prevention mental healthprograms (Durlak & Wells, 1997a), interventions rely-ing on interpersonal problem-solving skills did not re-duce maladjustment, suggesting that problem-solvingtraining should be combined with other programelements (Weissberg & Bell, 1997). Moreover, all theprograms that were evaluated were for young chil-dren aged 2–11. Weissberg and Bell (1997) also arguedthat no weighting was done in the meta-analysis toaccount for improvements in conceptualization, cur-riculum design, training of teachers, and classroomimplementation of the problem-solving programs.The findings from this study appear to fit into a broadconceptualization of health that includes psychologi-cal, social, and personal domains of health as definedby Perry and Jessor (1985). Moreover, the results sug-gest that enhanced competence had a positive im-pact on mental health, as measured by psychologicalwellness.
In this study, a repertoire of personal skills (rep-resented by both decision making and self-efficacy)positively influenced psychological wellness, whichdecreased alcohol behavior. Specifically, possessingsound decision-making skills increased feelings ofwellness, as did being more self-efficacious. Individ-uals who were more competent may have more adap-tive ways to cope in their daily lives, as reflectedby their apparent better mental health (measuredby psychological wellness). As a result, they mightnot turn to alcohol to cope with their problems.This implies that one reason competence enhance-ment programs prevent drinking is that the trainingin generic personal and social skills affects mentalhealth. The findings seem compatible with the viewthat the acquisition of skills and behaviors promotingthe experience of interest and joy should be includedin alcohol prevention programs (Labouvie, 1986). Yet,a host of factors undoubtedly explains why these typesof approaches work. For example, it may be the ex-
tent that generic skills impact on drug-specific refusalassertiveness, as well as psychological wellness, thatdetermines the effectiveness of competence enhance-ment approaches on alcohol behavior. Past researchidentified the link between generic skills and drug-specific refusal assertiveness as a key mechanism insubsequently deterring alcohol use (Epstein et al.,2000c). Based on the little evidence that exists, teach-ing such generic skills without domain-specific ma-terial concerning alcohol use may only be minimallyeffective (Caplan et al., 1992).
Although the overall model was significant,multigroup analyses showed that there was a genderdifference in one path in the model. Specifically, de-cision making did not predict psychological wellnessfor girls. Yet self-efficacy, another measure of compe-tence, did predict psychological wellness for girls. Itmay well be that other measures of competence thatwere not measured in this study could also predict psy-chological wellness for girls. Future research will haveto determine which forms of competence are relatedto psychological wellness based on gender.
This study had several potential limitations thatwarrant discussion. First, all data were self-reportedby students, which is common in the alcohol etiol-ogy field. Yet prior research found high consistency inresponses across different self-report items from stu-dent survey data on alcohol use, which creates greaterconfidence in self-report data (Johnston et al., 2000).Moreover, strong relationships between self-reportsof drinking and collateral peer reports for adoles-cents have been shown (Smith et al., 1994). A sec-ond limitation of this study is that the surveys wereconducted in schools, and so the findings may notapply to adolescents not attending school. However,some of the problems associated with collecting datafrom older, more transient high school students werelessened. Specifically, dropout rates are low in middleschool, and at least two attempts were made to col-lect data from absentee students participating in thestudy. Third, because the present sample consistedprimarily of urban Black and Hispanic youth, theseresults might not generalize to adolescents residingin suburban or rural regions or those of other eth-nic groups. Fourth, because only a limited number ofvariables were included in this study, it is not a com-plete model of alcohol use for inner-city adolescents.In particular, only two of the five pathways (acquiringage and ability appropriate competencies and acquir-ing skills needed to cope effectively with life stressors)to psychological wellness identified by Cowen (1994)were addressed. Measures of the three other pathways

P1: GNI/GLS/GKJ P2: GDR
Prevention Science [PREV] PP481-373224 May 1, 2002 9:34 Style file version Nov. 04, 2000
Wellness Protects Youth From Alcohol Use 103
were not available. Nor were decision making andself-efficacy meant to represent the full range of com-petency measures. Future research should explore afuller model of the pathways to psychological well-ness and its subsequent relationship with alcohol use.Fifth, because of attrition, the retained panel sam-ple may be more representative of a lower deviancesample of adolescents. Sixth, because there was insuf-ficient power to conduct ethnic multigroup analyses,it is not certain that the findings would apply equallyto all ethnic groups as the sample was predominantlyHispanic. Finally, the sample of inner-city adolescentsmay have a decreased level and a restricted range ofpsychological wellness due to social disorganization,witnessing community violence, and other factors as-sociated with poverty and neighborhood disorganiza-tion that were not included in the tested model.
In closing, the findings of this study suggest thatcompetence and its positive impact on psychologicalwellness protect adolescents from drinking alcohol.Adolescents who were able to make sound decisionsand felt more capable experienced greater wellnessand engaged in less alcohol use. This implies compe-tence skills offer protection and promote both men-tal health and positive behavioral outcomes that af-fect health. Based on the results of this study, alcoholprevention programs should emphasize competenceenhancement as a means of creating higher psycho-logical wellness and reducing adolescent alcohol be-havior. Moreover, the findings demonstrate one possi-ble mechanism that may help to explain the success ofcompetence enhancement programs for ethnic minor-ity adolescents residing in inner-city neighborhoods,as shown in past prevention studies with this popula-tion (Botvin et al., 1995a, 1997).
ACKNOWLEDGMENTS
This study was supported by Grant 1 R21AA11434 from the National Institute on AlcoholAbuse and Alcoholism to Dr Epstein. Data collectionfor this study was supported by Grant 1 R18 CA 39280from the National Cancer Institute to Dr Botvin.
REFERENCES
Bandura, A. (1986). Social foundations of thought and action: Asocial cognitive theory. Englewood Cliffs, NJ: Prentice-Hall.
Bentler, P. M. (1995). EQS structural equations program manual.Encino, CA: Multivariate Software, Inc.
Bentler, P. M., & Bonnett, D. G. (1980). Significance tests and good-ness of fit in the analysis of covariance structures. PsychologicalBulletin, 88(3), 588–605.
Bollen, K. A. (1989). Structural equations with latent variables.New York: Wiley.
Botvin, G. J. (1998). Preventing adolescent drug abuse throughLife Skills Training: Theory, methods and effectiveness. In J.Crane (Ed.), Social programs that really work (pp. 225–257).New York: Russell Sage Foundation.
Botvin, G. J. (2000). Preventing drug abuse in schools: Social andcompetence enhancement approaches targeting individual-level etiologic factors. Addictive Behaviors, 25, 887–897.
Botvin, G. J., Baker, E., Dusenbury, L., Botvin, E. M., & Diaz, T.(1995a). Long-term follow-up results of a randomized drugabuse prevention trial in a white middle-class population.JAMA, 273, 1106–1112.
Botvin, G. J., Dusenbury, L., Baker, E., James-Ortiz, S., Botvin,E. M., & Kerner, J. (1992). Smoking prevention among urbanminority youth: Assessing effects on outcome and mediatingvariables. Health Psychology, 11, 290–299.
Botvin, G. J., Dusenbury, L., Baker, E., James-Ortiz, S., & Kerner,J. (1989). A skills training approach to smoking preventionamong Hispanic youth. Journal of Behavioral Medicine, 12,279–296.
Botvin, G. J., Epstein, J. A., Baker, E., Diaz, T., & Ifill-Williams,M. (1997). School-based drug abuse prevention with inner-city minority youth. Journal of Child and Adolescent SubstanceAbuse, 6, 5–19.
Botvin, G. J., Schinke, S. P., Epstein, J. A., Diaz, T., & Botvin,E. M. (1995b). Effectiveness of culturally focused andgeneric skills training approaches to alcohol and drug abuseprevention among minority adolescents: Two-year follow-up results. Psychology of Addictive Behaviors, 9, 183–194.
Caplan, M., Weissberg, R. P., Grober, J. S., Sivo, P., Grady, K., &Jacoby, C. (1992). Social competence promotion with inner-cityand suburban young adolescents: Effects on social adjustmentand alcohol use. Journal of Consulting and Clinical Psychology,60, 56–63.
Cowen, E. L. (1994). The enhancement of psychological wellness:Challenges and opportunities. American Journal of Commu-nity Psychology, 22, 149–180.
Durlak, J. A. (1997). Successful prevention programs of child andadolescents. New York: Plenum.
Durlak, J. A., & Wells, A. M. (1997a). Primary prevention mentalhealth program for children and adolescents: A meta-analyticreview. American Journal of Community Psychology, 25, 115–152.
Durlak, J. A., & Wells, A. M. (1997b). Primary prevention mentalhealth programs: The future is exciting. American Journal ofCommunity Psychology, 25, 233–243.
Ellickson, P. L., McGuigan, K. A., Adams, V., Bell, R. M., &Hays, R. D. (1996). Teenagers and alcohol misuse in theUnited States: By any definition, it’s a big problem. Addiction,91, 1489–1503.
Epstein, J. A., Griffin, K. W., & Botvin, G. J. (2000a). Competenceskills help deter smoking among inner-city adolescents.Tobacco Control, 9, 33–39.
Epstein, J. A., Griffin, K. W., & Botvin, G. J. (2000b). A model ofsmoking among inner-city adolescents: The role of personalcompetence and perceived social benefits of smoking. Preven-tive Medicine, 31, 107–114.
Epstein, J. A., Griffin, K. W., & Botvin, G. J. (2000c). Role of gen-eral and specific competence skills in protecting inner-city ado-lescents from alcohol use. Journal of Studies on Alcohol, 61,379–386.
Gaffney, L. R., Thorpe, K., Young, R., Collett, R., & Occhipinti, S.(1998). Social skills, expectancies, and drinking in adolescents.Addictive Behaviors, 23, 587–599.
P1: GNI/GLS/GKJ P2: GDR
Prevention Science [PREV] PP481-373224 May 1, 2002 9:34 Style file version Nov. 04, 2000
104 Epstein, Griffin, and Botvin
Graham, J. W., Hofer, S. M., Donaldson, S. I., MacKinnon, D. P., &Schafer, J. L. (1997). Anaysis with missing data in preventionresearch. In K. J. Bryant, M. Windle, West, S. G. (Eds.), Thescience of prevention: Methodological advances from alcoholand substance abuse research (pp. 325–366). Washington, DC:American Psychological Association.
Griffin, K. W., Botvin, G. J., Scheier, L. M., Epstein, J. A., & Diaz, T.(2002). Personal competence skills, distress, and well-being asdeterminants of substance use in a predominantly minorityurban adolescent sample. Prevention Science, 3, 23–33.
Hover, S., & Gaffney, L. R. (1991). The relationship between socialskills and adolescent drinking. Alcohol and Alcoholism, 26(2),207–214.
Jackson, C., Henriksen, L., Dickinson, D., & Levine, D. W. (1997).The early use of alcohol and tobacco: Its relation to children’scompetence and parents’ behavior. American Journal of PublicHealth, 87, 359–364.
Jessor, R., & Jessor, S. L. (1977). Problem behavior and psychoso-cial development: A longitudinal study of youth. New York:Academic Press.
Johnston, L. D., O’Malley, P. M., & Bachman, J. G. (2000). NationalSurvey results on drug use from the Monitoring the Future study,1975–1999: Vol. 1. Secondary school students. Rockville, MD:National Institute of Drug Abuse.
Kolbe, L. J. (1997). Meta-analysis of programs to prevent mentalhealth problems among youth. American Journal of Commu-nity Psychology, 25, 227–232.
Labouvie, E. W. (1986). Alcohol and marijuana use in relation toadolescent stress. The International Journal of the Addictions,21(3), 333–345.
MacCallum, R. C., Roznowski, M., & Necowitz, L. B. (1992). Modelmodifications in covariance structure analysis: The problem ofcapitalization on chance. Psychological Bulletin, 111(3), 490–504.
Marsh, J. W., Balla, J. R., & McDonald, R. P. (1988). Goodness-of-fit indexes in confirmatory factor analysis: The effect of samplesize. Psychological Bulletin, 103, 391–410.
Masten, A. S., & Coatsworth, J. D. (1998). The development of com-petence in favorable and unfavorable environments: Lessonsfrom research on successful children. American Psychologist,53, 205–219.
Masterpasqua, F. (1989). A competence paradigm for psychologicalpractice. American Psychologist, 44, 1366–1371.
Pandina, R. J. (1998). Risk and protective factor models inadolescent drug use: Putting them to work for prevention.National Conference on Drug Abuse Prevention Research:Presentations, Papers and Recommendations (pp. 17–26).Rockville, MD: National Institute on Drug Abuse.
Paulhus, D. (1983). Sphere-specific measures of perceived control.Journal of Personality and Social Psychology, 44, 1253–1265.
Perry, C. L., & Jessor, R. (1985). The concept of health promotionand the prevention of adolescent drug abuse. Health EducationQuarterly, 12, 169–184.
Pitkaenen, T. (1999). Problem drinking and psychological well-being: A five-year follow-up study from adolescence to youngadulthood. Scandinavian Journal of Psychology, 40, 197–207.
Resnicow, K., & Botvin, G. J. (1993). School-based substanceuse prevention programs: Why do effects decay. PreventiveMedicine, 22(4), 484–490.
Scheier, L. M., & Botvin, G. J. (1998). Relations of social skills,personal competence, and adolescent alcohol use: A develop-mental exploratory study. Journal of Early Adolescence, 18,77–114.
Smith, G. T., McCarthy, D. M., & Goldman, M. S. (1994). Self-reported drinking and alcohol-related problems among earlyadolescents: Dimensionality and validity over 24 months. Jour-nal of Studies on Alcohol, 56, 383–394.
Snow, D. L., & Tebes, J. K. (1992). Panel attrition and external valid-ity in adolescent substance use research. Journal of Consultingand Clinical Psychology, 60, 804–807.
Veit, C. T., & Ware, J. E. (1983). The structure of psychologicaldistress and well-being in general populations. Journal ofConsulting and Clinical Psychology, 51, 730–742.
Weissberg, R. P., & Bell, D. N. (1997). A meta-analytic review ofprimary prevention program for children and adolescents:Contributions and caveats. American Journal of CommunityPsychology, 25, 207–214.
Weissberg, R. P., & Greenberg, M. T. (1998). School and commu-nity competence-enhancement and prevention programs. InW. Damon (Series Ed.) & I. E. Sigel & K. A. Renninger (Vol.Eds.), Handbook of child psychology: Vol. 4. Child psychologyin practice (5th ed., pp. 877–954). New York: Wiley.
Wills, T. A. (1986). Stress and coping in early adolescence: Re-lationships to substance use in urban school samples. HealthPsychology, 5, 503–529.
Wills, T. A., DuHamel, K., & Vaccaro, D. (1995). Activity and moodtemperament as predictors of adolescent substance use: Testof a self-regulation mediational model. Journal of Personalityand Social Psychology, 68, 901–916.
Wothke, W. (1998). Longitudinal and multigroup modeling withmissing data. In T. D. Little, K. U. Schnabel, & J. Baumert(Eds.), Modeling longitudinal and multiple group data: Practi-cal issues, applied approaches, and specific examples. Mahwah,NJ: Erlbaum.
Zins, J. E., Elias, M. J., Greenberg, M. T., & Weissberg, R. P.(2000). Promoting social and emotional competence in chil-dren. In K. M. Minke & G. C. Bear (Eds.), Preventing schoolproblems—Promoting school success: Strategies and programsthat work (pp. 71–99). Bethesda, MD: National Association ofSchool Psychologists.
Related Documents











