ELSEVIER Schizophrenia Research 16 ( 1995) 175-188 SCHIZOPHRENIA RESEARCH Positive and negative symptoms in neuroleptic-free psychotic inpatients G.W. Stuart a,b,c,d,,, V. Malone a.c, j. Currie a,o, S. Klimidis b,d, I.H. Minas b,d a Neurophysiology and Neurovisual Research Unit, Mental Health Research Institute of Victoria, Melbourne, Australia, b l/Tctorian Transcultural Psychiatry Unit, Melbourne, Australia, ~ The National Health and Medical Research Council Schi-ophrenia Research Unit, Royal Park Hospital, Melbourne, Australia, d Department of Psvchiato'. Melbourne University, Melbourne, Australia Received 3 February 1994; accepted 28 October 1994 Abstract Andreasen's scales for the assessment of positive (SAPS) and negative (SANS) symptoms and the Brief Psychiatric Rating Scale (BPRS) were administered to a group of 70 neuroleptic-free psychotic inpatients. Individual ratings from the SAPS and SANS, together with the 18-item BPRS, were examined to identify clusters of symptoms. The findings, consistent with our previous studies using medicated patients, did not support a simple positive-negative dichotomy. Independent syndromes representing negative symptoms and thought disorder were apparent, although within the negative syndrome there were three related sub-syndromes of flat affect, alogia and social dysfunctions. Hallucinations and delusions did not form a homogeneous group of symptoms. Paranoia emerged as a distinct syndrome, and the remaining symptoms could be subdivided into hallucinations, grandiose delusions, and 'loss of boundar)' delusions (e.g., thought broadcasting, mind reading). These syndromes, with the exception of loss of boundar? delusions, which consisted of SAPS delusions alone, correspond to syndromes of psychosis identified by Lorr and his colleagues thirty years ago. It is concluded that the currently popular 'three syndrome' model does not adequately represent the diversity of psychotic symptoms. Keywords Psychosis; Syndrome structure; Medicated vs. unmedicated patients; Positive symptom; Negative symptom 1. Introduction Within the last ten years, interest in the psycho- pathology of schizophrenia has focused on the distinction between positive and negative symp- toms, that is, the florid expressions of psycho- sis such as hallucinations, delusions and formal thought disorder as opposed to symptoms such as affective blunting, apathy and emotional with- * Corresponding author. Present address: NH&MRC Schizophrenia Research Unit, Private Bag 3, Parkville, Victoria, Australia 3052. 0920-9964/95/$09.50 © 1995 Elsevier Science B.V. All rights reserved SSDI 0920-9964 ( 94 ) 00083-2 drawal. This revived interest can be traced back to the work of Strauss et al. (1974), but probably the major impetus was the proposal by Crow (1980) that positive and negative schizophrenia were distinct subtypes of the disorder, with different causes and prognoses. Initially, interest centred around the question of whether positive and negative symptoms constituted mutually exclusive syndromes or whether there was overlap between them. The view that gained ascendency was that positive and negative symptoms occur independently rather than being mutually exclusive (Andreasen, 1985; Crow, 1985), and that as a

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
E L S E V I E R Schizophrenia Research 16 ( 1995 ) 175-188
SCHIZOPHRENIA RESEARCH
Positive and negative symptoms in neuroleptic-free psychotic inpatients
G.W. Stuart a,b,c,d,,, V. Malone a.c, j. Currie a,o, S. Klimidis b,d, I.H. Minas b,d
a Neurophysiology and Neurovisual Research Unit, Mental Health Research Institute o f Victoria, Melbourne, Australia, b l/Tctorian Transcultural Psychiatry Unit, Melbourne, Australia, ~ The National Health and Medical Research Council
Schi-ophrenia Research Unit, Royal Park Hospital, Melbourne, Australia, d Department o f Psvchiato'. Melbourne University, Melbourne, Australia
Received 3 February 1994; accepted 28 October 1994
Abstract
Andreasen's scales for the assessment of positive (SAPS) and negative (SANS) symptoms and the Brief Psychiatric Rating Scale (BPRS) were administered to a group of 70 neuroleptic-free psychotic inpatients. Individual ratings from the SAPS and SANS, together with the 18-item BPRS, were examined to identify clusters of symptoms. The findings, consistent with our previous studies using medicated patients, did not support a simple positive-negative dichotomy. Independent syndromes representing negative symptoms and thought disorder were apparent, although within the negative syndrome there were three related sub-syndromes of flat affect, alogia and social dysfunctions. Hallucinations and delusions did not form a homogeneous group of symptoms. Paranoia emerged as a distinct syndrome, and the remaining symptoms could be subdivided into hallucinations, grandiose delusions, and 'loss of boundar)' delusions (e.g., thought broadcasting, mind reading). These syndromes, with the exception of loss of boundar? delusions, which consisted of SAPS delusions alone, correspond to syndromes of psychosis identified by Lorr and his colleagues thirty years ago. It is concluded that the currently popular 'three syndrome' model does not adequately represent the diversity of psychotic symptoms.
Keywords Psychosis; Syndrome structure; Medicated vs. unmedicated patients; Positive symptom; Negative symptom
1. Introduction
Within the last ten years, interest in the psycho- pathology of schizophrenia has focused on the distinction between positive and negative symp- toms, that is, the florid expressions of psycho- sis such as hallucinations, delusions and formal thought disorder as opposed to symptoms such as affective blunting, apathy and emotional with-
* Corresponding author. Present address: NH&MRC Schizophrenia Research Unit, Private Bag 3, Parkville, Victoria, Australia 3052.
0920-9964/95/$09.50 © 1995 Elsevier Science B.V. All rights reserved SSDI 0920-9964 ( 94 ) 00083-2
drawal. This revived interest can be traced back to the work of Strauss et al. (1974), but probably the major impetus was the proposal by Crow (1980) that positive and negative schizophrenia were distinct subtypes of the disorder, with different causes and prognoses. Initially, interest centred around the question of whether positive and negative symptoms constituted mutually exclusive syndromes or whether there was overlap between them. The view that gained ascendency was that positive and negative symptoms occur independently rather than being mutually exclusive (Andreasen, 1985; Crow, 1985), and that as a
176 G. W. Stuart et al./Schizophrenia Research 16 (1995) 175-188
consequence many patients will exhibit both types of symptom concurrently.
However, the validity of treating positive symp- toms as a unitary syndrome within a two syndrome model of positive and negative symptoms was subsequently questioned. In particular, both empirical (Bilder et al., 1985; Liddle, 1987) and theoretical (McGrath, 1990) distinctions have been drawn between formal thought disorder and delu- sions/hallucinations. There are now many studies supporting 'three syndrome' models (i.e. negative symptoms, formal thought disorder, and delusions/ hallucinations). A number of these studies are based on global ratings from Andreasen's (1983, 1984) scales for the assessment of negative (SANS) and positive (SAPS) symptoms (see Peralta et al., 1992; and Klimidis et al., 1993 for reviews). The three-syndr0me model based on global ratings alone appears to be valid for both schizophrenia and other pyschoses (Klimidis et al., 1993). A serious limitation of such studies is that there are only nine global ratings (only four of which mea- sure positive symptoms), and so these results, although sufficient to reject a simple dichotomy, may underestimate the true number of underlying dimensions.
The second line of evidence for the three- syndrome model comes from studies of chronic medicated schizophrenic patients. An influential study is that of Liddle (1987). This study used a sample of 40 patients suffering from chronic schizophrenia. Separate factor analyses were car- ried out using symptoms from the SAPS/SANS, and from the Present State Examination (PSE) (Wing et al., 1974). However, because many posi- tive symptoms could not be analysed because of their low frequency of occurrence, only 16 symp- toms from the SAPS/SANS, and 14 ratings from the PSE were retained in the analyses. Despite this, some single symptoms did not load on any factor, and others, such as persecutory delusions, did not fit the factor structure well. In addition, the analysis of the PSE yielded two factors repre- senting hallucinations and delusions. One factor represented delusions of reference, persecution and grandiose delusions, the other the 'nuclear syndrome' - Schneiderian first-rank symptoms of schizophrenia such as auditory hallucinations and
delusions of thought broadcasting, intrusion, with- drawal or control. Subsequent attempts to replicate this model have involved similar limitations. Silver et al. (1993) excluded all symptoms with a fre- quency of less than 25%, and restricted their factor analyses of different scales to three factors 'to enable comparison with each other and with other published studies' (p. 69). Liddle and Barnes (1990) used single global ratings of hallucinations and delusions, making further differentiation of these symptoms impossible, as did Brown and White (1992).
Evidence for the three syndrome model has therefore come mainly from two sources: from studies which use very restrictive symptom lists such as the global ratings of the SAPS and SANS, or from studies which use chronic medicated schiz- ophrenics where the range of positive symptoms is reduced. There is evidence that when more extens- ive symptom lists, and more representative samples of patients with schizophrenia or psychotic dis- order are used, a greater number of syndromes emerge. Lorr et al. (1963), summarising early factor analytic studies, identified ten syndromes of psychosis based on extensive symptom checklists and large, diagnostically heterogeneous groups of inpatients. These syndromes consisted of a single negative syndrome of retardation and apathy, the psychotic syndromes of paranoid projection, gran- diosity, perceptual distortion, conceptual disorgan- isation, disorientation and motor disturbance (mannerisms and posturing); and affective syn- dromes of hostile belligerence, excitement, and anxious depression. Excluding the affective syn- dromes, this represents a seven-syndrome model of psychosis. Subsequent studies confirmed the existence of these psychotic syndromes and elabo- rated the affective syndromes even further (Lorr, 1988).
In a recent study using the 30-item Positive and Negative Syndrome Scale (PANSS), Kay and Sevy (1990) also supported a higher-dimensional model of schizophrenic symptoms. Factor analysis of the items of the PANSS, applied to a broad sample of patients satisfying the DSM-III criteria for schizo- phrenia, yielded seven factors. Four of these factors encompassed psychotic symptoms, including nega- tive symptoms, positive symptoms (hallucinations
G. W. Stuart et al./Schizophrenia Research 16 (1995) 175 188 177
and delusions) cognitive disturbances (thought dis- order and others) and suspiciousness/persecution. The other factors reflected excitement, depression and stereotyped thinking. Of particular interest in the present context is the factor representing suspi- ciousness/persecution. Although Kay and Sevy (1990) considered this factor unreliable, due to the small amount of variance it explained, it consti- tutes a recognisable clinical entity. In addition to its defining symptom, this factor was also corre- lated (but not uniquely) with hostility, uncoopera- tiveness, and active social avoidance. The independence of this factor may be more important than its strength, which may simply reflect the item content of the PANSS. Thus, Kay and Sevy's (1990) results provide support for at least a four- dimensional model of psychotic symptoms within the domain of schizophrenia.
In a study using the full SAPS and SANS in a broad diagnostic group of medicated psychotic inpatients (Minas et al., 1992, 1993) we have also found a higher dimensionality than that reported in studies which used only the global or subscale ratings of the SAPS and SANS. This places in doubt the general validity of the subscale structure of these scales. When the correlations between individual items of the sub-scales were examined, it was found that only two correlated factors were needed to represent negative symptoms (negative signs and social dysfunctions) as opposed to the five subscales of the SANS which are currently in use. Conversely, while item-level analyses broadly validated the thought disorder and hallucinations subscales of the SAPS, and the independence (but not the internal consistency) of the bizarre behavi- our scale, there was considerable heterogeneity within the delusions subscale. Somatic delusions were correlated with hallucinations. Grandiose delusions, persecutory delusions, and 'loss of boundarv' delusions (e.g., thought broadcasting) all showed a degree of independence. This indicates that a considerable amount of information may be lost by using a single global summary measure of delusions, and hence that studies using such measures are likely to underestimate the dimen- sionality of psychosis. These findings remained valid when the sample was divided into diagnostic subgroups of schizophrenia and other psychoses.
The purpose of the present study was to deter- mine whether the syndrome structure that was obtained in a sample of medicated patients was also present in a sample of patients who were not receiving anti-psychotic medication. It is possible that such medication may exacerbate negative symptoms (Prosser et al., 1987) while reducing both the range and severity of positive symptoms. Even though there is evidence that there may be more than three syndromes even in chronic medi- cated schizophrenics, we have chosen to study this question in a broad sample of psychotic patients. As positive and negative symptoms are not unique to schizophrenia, the most generally applicable syndrome model is likely to be obtained from a diverse patient group, especially when free from the effects of anti-psychotic medication. A second advantage of this strategy is that it allows the inclusion of patients in the early stages of their illness, who would not have met the DSM-III-R chronicity criterion for a diagnosis of schizophre- nia. Finally, in order to ensure that the number of syndromes was not limited by an inadequate cover- age of symptoms, all the individual items of the SAPS and SANS, as well as the 18-item Brief Psychiatric Rating Scale (BPRS) (Overall and Gorham, 1962: Guy, 1976) were rated for each patient.
2. Methods
2.1. Subjects
The sample consisted of 70 patients, 53 males and 27 females, with DSM-III-R (American Psychiatric Association, 1987) diagnoses of psy- chotic disorder. All were neuroleptic-free for a period greater than one month for oral administra- tion and three months for depot administration. Of the total sample, 10 were neuroleptic-naive. However, 26 (37%) of the patients had been stabi- lised using benzodiazepines, which may have some antipsychotic properties (Wolkowitz and Picar, 1991). The sample consisted mainly of acute patients. Nearly half (52.9%) were inpatients for the first time, and a further 21.4% were second admissions. Only 24.3% were third or subsequent
178 G. W. Stuart et al./Schizophrenia Research 16 (1995) 175-188
admissions. The mean age of the sample was 32.0 years (median 30.2) and the standard deviation 10.29 years. A breakdown of DSM-III-R diagnoses is listed in Table 1.
The sample was representative of the hospital inpatient population, which is a public, state gov- ernment funded institution with a catchment cover- ing a third of the Melbourne metropolitan area. Keks et al. (1991) carried out a study of the characteristics of patients consenting and refusing to take part in research in this hospital. The only bias was a reduced participation rate for patients rated as uncooperative, but not for paranoid patients. In the process of recruitment of the present sample, all unmedicated patients satisfying the above criteria who were admitted to the hospi- tal were invited, within 24 hours of admission, to take part in neurophysiological investigations. On obtaining informed consent according to guidelines specifed by the National Health and Medical Research Council, patients were interviewed, assessed and rated for psychopathology.
studies of medicated patients (Minas et al., 1992), and was blind to hypotheses about the relationship between symptoms.
2.3. Statistical methods
Both the individual item ratings and the sum- mary global subscale ratings of the SAPS/SANS are scored on a 6-point ordinal scale. The 18 items of the BPRS are scored on a 7-point ordinal scale. Matrices of the intercorrelations between symp- toms scores from both scales were calculated, and were then subjected to principal components analy- sis (e.g., Gorsuch, 1983) and cluster analysis (Everitt, 1974) to identify related groups of symp- toms. The results of these analyses were verified using the technique of full-information factor analysis (Bock et al., 1988), which is described in more detail in the next section.
3. Results
2.2. Procedure 3.1. Pearson correlations
DSM-III-R diagnoses were derived from the initial interview and subsequent follow-up inter- views where necessary over a six month period. Symptom ratings were performed at initial inter- view, according to the SAPS, SANS and 18 item BPRS (Nursing Modification) schedules (McGorry et al., 1988). The single experienced rater (V.M.) was a psychiatric nurse who had completed training in the use of the instruments which required good inter-rater reliability with other raters. She was not involved in our previous
Table 1 DSM-III-R diagnoses for the patient sample (n = 70)
Diagnoses n Diagnosis n
Schizophrenia 40 Bipolar disorder 7 Undifferentiated 23 Delusional Disorder 5 Paranoid 12 Atypical psychosis 4 Disorganised 3 Brief reactive psychosis 1 Residual 2 Depression with psychotic
Schizophreniform 7 features 1 Schizoaffective 3 Psychosis (not specified) 2
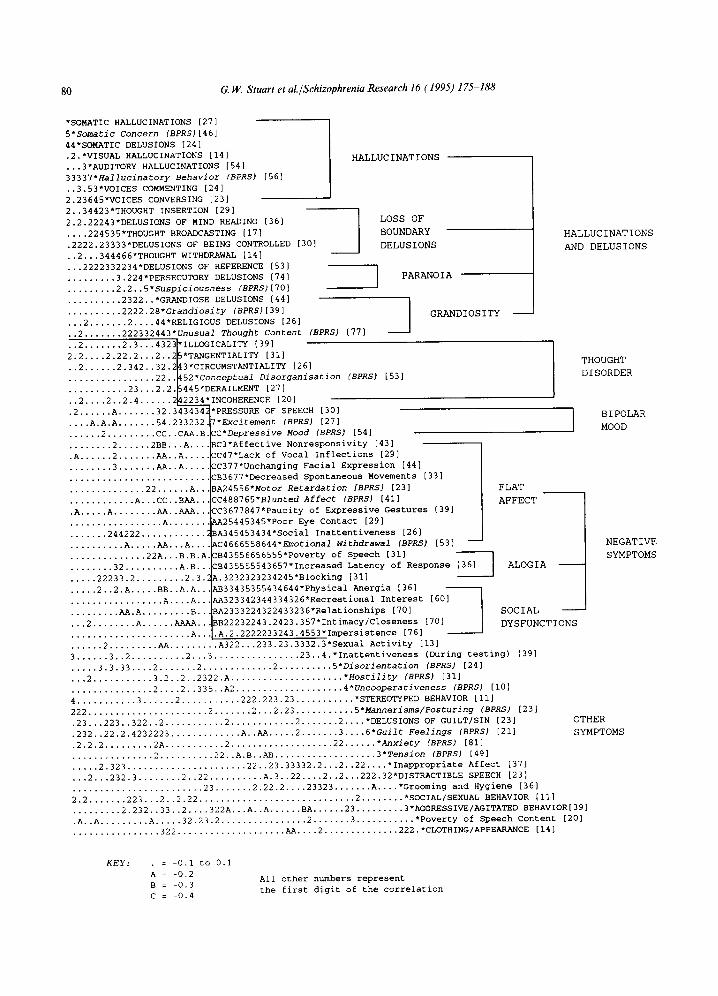
In the initial analysis, Pearson correlations between individual ratings from the SAPS, SANS and BPRS were examined. Only three items were omitted from the analysis due to low base rates (less than 10%). These were the SAPS items 'olfac- tory hallucinations', 'clanging associations' and 'delusions of jealousy'. Various cluster and princi- pal components analyses were then carried out. These initial analyses are not reported separately, but were used to construct a sorted correlation matrix, by placing variables that consistently loaded on the same factor, or within the same cluster, close together within the matrix structure. If discrete syndromes exist, the matrix can be sorted so that high correlations fall into separate blocks along the diagonal of the matrix, with low correlations elsewhere. Fig. 1 shows the original correlation matrix, sorted in this manner. The matrix entries represent the first digit of the corre- lation between a pair of ratings. Inverse correla- tions are represented by letters. Correlations above 0.3 are significant at the 0.01 level in the case of two-tailed significance tests. Correlations of 0.4 or
G, W. Stuart et al./Schizophrenia Research 16 (1995) 175-188 179
greater are significant at the 0.001 level. Hence these clusters are reliable in the statistical sense. This is a direct way to identify clusters of related symptoms, and has the additional advantage (in contrast to factor analysis) that no information is lost.
Inspection of Fig. 1 shows that the sorted matrix does contain a number of clusters of correlated symptoms. At the coarsest level of analysis, four broad classes of symptoms can be indentified, which correspond to the three-syndrome model of hallucinations and delusions, thought disorder, and negative symptoms, plus an affective syndrome representing bipolar mood. This latter syndrome is treated separately, because although the depres- sive pole is correlated with the negative syndrome, the 'manic' pole, represented by the symptoms of excitement and pressure of speech, is correlated with grandiose delusions and the thought disorder symptoms. In addition, there are a number of symptoms, or pairs of symptoms, which do not clearly fit into any of these major groups, and are placed at the bottom of the sorted matrix.
It is apparent from this figure that hallucinations and delusions do not constitute a uniformly inter- correlated block of symptoms. There was not a clear simple structure: instead, hallucinations and delusions seem to lie along a continuum, with high correlations along the diagonal of the matrix, and weak correlations away from it. We have sub- divided this spectrum of symptoms into four subgroups: Hallucinations, 'loss of boundary' delu- sions, paranoia and grandiosity. This was partly motivated by theoretical considerations, due to the lack of clear internal boundaries in some cases. These lbur syndromes are the same as those observed within this spectrum of symptoms in our sample of medicated patients (Minas et al., 1992).
In contrast to hallucinations and delusions, all the negative symptoms are intercorrelated to some degree, but there are three subgroups of more closely related symptoms. There is a large group of negative symptoms representing flat affect. This includes the majority of symptoms from the affec- tive flattening subscale of the original version of the SANS (excluding inappropriate affect) together with the BPRS items blunted affect, emotional withdrawal and motor retardation, and the SANS
attention subscale item of social inattentiveness. Related to this group is a set of three symptoms from the alogia subscale of the SANS. Of these three symptoms, only thought blocking does not have high correlations with the flat affect symp- toms. In our previous study of medicated patients (Minas et al., 1992), this symptom was not strongly correlated with any major syndrome, and the flat affect and alogia symptoms merged into a single syndrome which we termed 'negative signs'. The third subgroup of negative symptoms consists of items from the SANS avolition/apathy and anhedonia/asociality subscales which we have termed ~social dysfunctions'. This subgroup was also apparent in our medicated sample.
With the addition of BPRS ratings to the item set, it is apparent that in this sample there is evidence for all the syndromes identified by Lorr et al. (1963), which are listed in Table 2 for com- parison. Despite the different labels, the first six syndromes listed correspond well to the first seven groups of symptoms labelled in the sorted correla- tion matrix, excluding 'loss of boundary' delusions which is composed of SAPS delusions only. This class of symptoms was not well represented in the studies reviewed by Lorr et al. (1963), due to an emphasis on observable behaviors. The syndrome of excitement corresponds to one pole of the bipolar mood group in the correlation matrix. In the ten-syndrome model, there is only a single negative syndrome, compared to the three related subgroups of negative symptoms in the correlation matrix. Consistent with this, all BPRS negative symptom ratings fall within the flat affect subgroup of symptoms. The syndromes of disorientation, hostile belligerence and motor disturbance listed in Table 2 are represented in the correlation matrix by pairs of symptoms which, while correlated with each other, show little relationship with other symptoms. Finally, consistent with the later review by Lorr (1988), anxious intropunitiveness is not apparent as a single syndrome. While depression contributes to one pole of the bipolar mood syn- drome, anxiety and guilt are independent. There are a number of possible reasons for this. One is the very high frequency of anxiety in this sample, which might be expected given that the patients
80 G. W. Stuart et al./Schizophrenia Research 16 (1995) 175-188
*SOMATIC HALLUCINATIONS [27]
5*Somatic Concern (BPRS)[46] 44*SOMATIC DELUSIONS [24]
.2.*VISUAL HALLUCINATIONS [14]
...3*AUDITORY HALLUCINATIONS [54]
33337*Hallucinatory Behavior (BPRS) [56]
..3.53*VOICES COMMENTING [24]
2.23645*VOICES CONVERSING [23]
2..34423*THOUGHT INSERTION [29]
2.2.22243*DELUSIONS OF MIND READING [36]
.... 224535*THOUGHT BROADCASTING [17]
.2222.23333*DELUSIONS OF BEING CONTROLLED [30]
..2...344466*THOUGHT WITHDRAWAL [14]
...2222332234*DELUSIONS OF REFERENCE [53] I
......... 3.224*PERSECUTORY DELUSIONS [74] I ......... 2.2..5*Suspiciousness (BPRS)[70]
.......... 2322..*GRANDIOSE DELUSIONS [44]
.......... 2222.28*Grandiosity (BPRS)[39]
...2 ....... 2 .... 44*RELIGIOUS DELUSIONS [26]
..2 ....... 222332443*Unusual Thought Content (BPRS) [77]
..2 ....... 2.3...43231*ILLOGICALITY [39]
2.2 .... 2.22.2... 2.. 2~*TANGENTIALITY [31] H
..2 ...... 2.342..32.2~3*CIRCUMSTANTIALITY [26]
................ 22..~52*Conceptual Disorganisation (BPRS) [53]
........... 23...2.2.{5445*DERAILMENT [27]
..2 .... 2..2.4 ...... 2~2234*INCOHERENCE [20]
.2 ...... A ....... 32.3434342*PRESSURE OF SPEECH [30]
7*Excitement (BPRS) [27]
~C*Depressive Mood (BPRS) [54]
SC3*Affective Nonresponsivity [43]
CC47*Lack of Vocal Inflections [29]
.... A.A.A ....... 54.233232.
..... 2 ......... CC.. CAA.B.
........ 2 ...... 2BB. . .A. . .
.A ...... 2 ....... AA. .A ....
........ 3 ....... AA. .A ....
.............. 22 ...... A..
............ A...CC..BAA..
.A ..... A ........ AA..AAA..
................. A .......
....... 244222 ............
.......... A ..... AA...A...
.............. 22A. . .B.B.A
........ 32 .......... A.B..,
..... 22233.2 ......... 2.3.~
..... 2..2.A ..... BB..A.A..
................. A .... A..
......... AA,A ......... B, .
. . .2 ........ A ...... AAAA..
HALLUCINATIONS
LOSS OF
BOUNDARY
DELUSIONS
PARANOIA
GRANDIOSITY
HALLUCINATIONS
AND DELUSIONS
THOUGHT
DISORDER
BIPOLAR
MOOD
CC377*Unchanging Facial Expression [44]
CB3677*Decreased Spontaneous Movements [33]
BA24556*Motor Retardation [BPRS] [23] FLAT
CC488765*Blunted Affect (BPRS) [41] AFFECT
CC3677847*Paucity of Expressive Gestures [39]
AA25445345*Poor Eye Contact [29]
BA345453434*Social Inattentiveness [26]
AC4666558644*Emotiona1 withdrawal (BPRS) [53] --
CB43556656555*Poverty of Speech [31]
CB435555543657*Increased Latency of Response [36] I ALOGIA
%.3232323234245*Blocking [31]
%B33435355434644*Physical Anergia [36]
%A323342344334326*Recreational Interest [60]
~A2333224322433236*Relationships [70] SOCIAL
~B22232243.2423.357*Intimacy/Closeness [70] DYSFUNCTIONS
...................... A.. .A.2.2222233243.4553*Impersistence [76]
...... 2 ......... AA ......... A322...233.23.3332.3*Sexual Activity [13]
3 ...... 3..2 .......... 2...3 ................ 23..4.*Inattentiveness (During testing) [39]
..... 3.3.33 .... 2 ....... 2 ............. 2 .......... 5*Disorientation (BPRS) [24]
...2 ........... 3.2..2..2322.A ..................... *Hostility (BPRS) [31]
............... 2 .... 2..335..A2 .................... 4*Uncooperativeness {BPRS) [10]
4 ........... 3 ...... 2 ........... 222.223.23 ........... *STEREOTYPED BEHAVIOR [ii]
222 ...................... 2 ....... 2...2.23 ........... 5*Mannerisms~Posturing (BPRS) [23]
.23...223..322..2 ........... 2 ............ 2 ....... 2 .... *DELUSIONS OF GUILT/SIN [23]
.232..22.2.4232223 ............. A..AA ..... 2 ....... 3 .... 6*Guilt Feelings (BPBS) [21]
.2.2.2 ......... 2A ........... 2 ................... 22 ...... *Anxiety (BPRS) [81]
............... 2 .......... 22..A.B..AB ................... 3*Tension (BPRS) [49]
..... 2.323 ...................... 22..23.33332.2...2..22 .... *Inappropriate Affect [37]
...2...232.3 ........ 2..22 .......... A.3..22 .... 2..2...222.32*DISTRACTIBLE SPEECH [23]
........................ 23 ....... 2.22.2 .... 23323 ....... A .... *Grooming and Hygiene [36]
2.2 ....... 223...2..2.22 ............................. 2 ........ *SOCIAL/SEXUAL BEHAVIOR [II]
......... 2.232..33..2 .... 322A...A..A ...... BA ...... 23 ......... 3*AGGRESSIVE/AGITATED BEHAVIOR[39]
.A..A ......... A ..... 32.23.2 ................ 2 ....... 3 ........... *Poverty of Speech Content [20]
................ 322 .................... AA .... 2 .............. 222.*CLOTHING/APPEARANCE [14]
OTHER
SYMPTOMS
NEGATIVE
SYMPTOMS
KEY: . = -0.I to 0.I
A = -0,2
B = -0.3
C = -0.4
All other nu/nbers represent
the first digit of the correlation

G.W. Stuart et al./Schizophrenia Research 16 (1995) 175-188 181
Table 2 A list of the ten syndromes of psychosis derived from an extensive review by Lorr et al. (1963) of early factor- analytic research
Syndromes of psychosis (Lorr et al., 1963)
1. Perceptual Distortion 2. Paranoid Projection 3. Grandiose Expansiveness 4. Conceptual Disorganisation 5. Excitement
6. Retardation and Apathy 7. Disorientation 8. Hostile Belligerence 9. Motor Disturbance
10. Anxious Intropunitiveness
had been recently admitted to hospital and the majority were unmedicated.
Several individual symptoms from the SAPS/SANS did not correlate well with any other symptoms. These included inappropriate affect, poverU¢ of speech content, distractible speech, poor grooming and hygiene, inattention during men- tal status testing, and reduced sexual activity. Although the latter symptom had a number of weak correlations with the negative symptom group, we have placed it outside of this syndrome because the validity and reliability of this rating in a recently hospitalised sample is questionable. Finally, it can be seen that the ratings from the bizarre behavior subscale of the SAPS are not correlated with each other, as in our study of medicated patients (Minas et al., 1992), placing in doubt the validity of this subscale.
3.2. Full in formation factor analysis
In the next phase of the analysis, full- information factor analysis (Bock et al., 1988) was used to determine the internal structure of each of the three major syndromes. Separate analyses were carried out within the major syndromes because the full-information method, due to its computa- tional complexity, is limited to a maximum of five factors. A problem with the use of conventional factor analysis at the item level is the possibility
of spurious 'difficulty factors' (Gorsuch, 1983). These may arise if ratings tap the same underlying phenomena, but have markedly different score distributions which preclude high correlations (Bernstein and Teng, 1989). The most likely cause is that symptoms represent different levels of sever- ity of the same underlying trait. Full-information factor analysis does not suffer from this problem, because it uses all information about the presence or absence of symptoms, rather than pairwise correlations, as the basis of factor analysis. Although it cannot be used for graded ratings, this may not be a serious drawback, as it has been shown that some of the categories used in the SAPS/SANS may not be used consistently, and in particular that delusions may be difficult to rate in a graded fashion (Bell et al., 1994). A further advantage of the method is that significance tests for the addition of successive factors to the model are possible. The analyses were carried out using the TESTFACT computer program ( Wilson et al., 1991 ). Prior to analysis, all ratings were rescored as present if the rating was 'mild' or above on either scale.
Three criteria were used to determine the number of factors (i) The solution had to provide an acceptable communality for all symptoms (ii) No factor that explained less variance than a single item was retained in the analysis (iii) Significance tests for the improvement in the fit of the model were also taken into account. However, because the small sample size may have resulted in infla- ted significance values (Haberman, 1977) non- significant results are more likely to be robust. An initial analysis showed that a single factor was sufficient to account for the correlations between thought disorder items, with a second factor not producing a significant improvement in the model (zz= 1.20, df=5, n.s.). Separate analyses of nega- tive symptoms, and hallucinations and delusions, confirmed and extended the structure that was apparent in the sorted correlation matrix.
Fig. 1. Sorted matrix of correlations between SAPS/SANS ratings and BPRS ratings. Base rates (percentages) for the presence of a symptom ('mild' or above) are shown in brackets. The numbers represent the first digit of the Pearson correlation coefficient. Negative correlations are represented by letters. There are consistent correlations between symptoms within the block representing thought disorder and also within the group of negative symptoms, but this is not the case for hallucinations and delusions. There are also a number of individual symptoms and symptom pairs, which do not fit into any of these major syndromes.
182 G. W. Stuart et al./Schizophrenia Research 16 (1995) 175-188
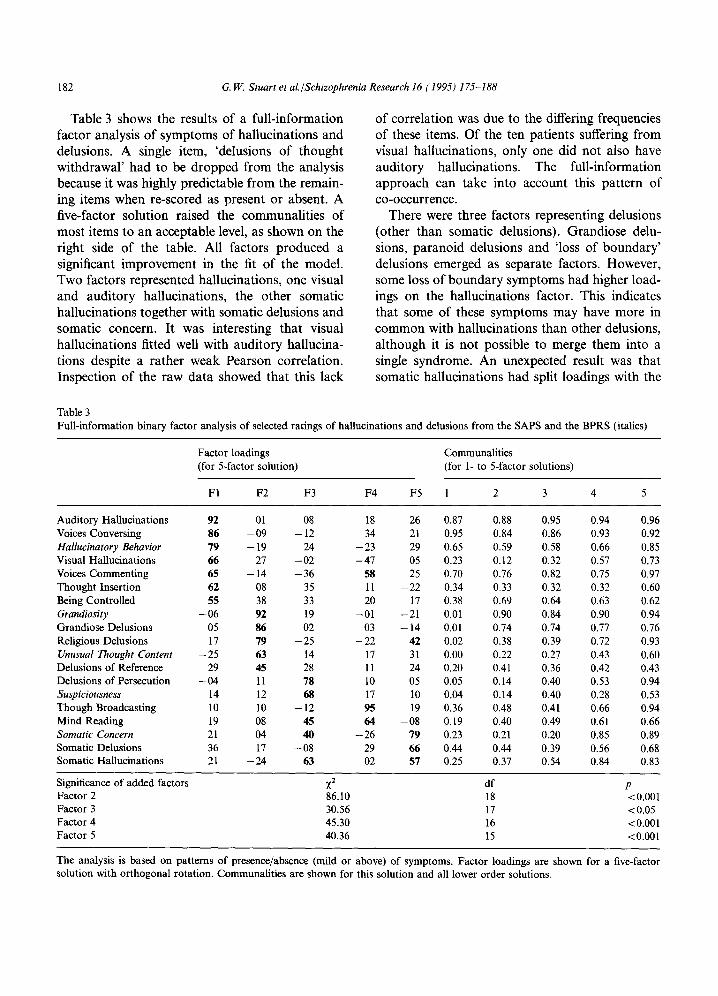
Table 3 shows the results of a full-information factor analysis of symptoms of hallucinations and delusions. A single item, 'delusions of thought withdrawal' had to be dropped from the analysis because it was highly predictable from the remain- ing items when re-scored as present or absent. A five-factor solution raised the communalities of most items to an acceptable level, as shown on the right side of the table. All factors produced a significant improvement in the fit of the model. Two factors represented hallucinations, one visual and auditory hallucinations, the other somatic hallucinations together with somatic delusions and somatic concern. It was interesting that visual hallucinations fitted well with auditory hallucina- tions despite a rather weak Pearson correlation. Inspection of the raw data showed that this lack
of correlation was due to the differing frequencies of these items. Of the ten patients suffering from visual hallucinations, only one did not also have auditory hallucinations. The full-information approach can take into account this pattern of co-occurrence.
There were three factors representing delusions (other than somatic delusions). Grandiose delu- sions, paranoid delusions and 'loss of boundary' delusions emerged as separate factors. However, some loss of boundary symptoms had higher load- ings on the hallucinations factor. This indicates that some of these symptoms may have more in common with hallucinations than other delusions, although it is not possible to merge them into a single syndrome. An unexpected result was that somatic hallucinations had split loadings with the
Table 3 Full-information binary factor analysis of selected ratings of hallucinations and delusions from the SAPS and the BPRS (italics)
Factor loadings (for 5-factor solution)
Communalities (for 1- to 5-factor solutions)
F1 F2 F3 F4 F5 1 2 3 4 5
Auditory Hallucinations 92 01 08 18 26 0.87 0.88 0.95 0.94 0.96 Voices Conversing 86 - 0 9 - 12 34 21 0.95 0.84 0.86 0.93 0.92 Hallucinatory Behavior 79 - 19 24 - 23 29 0.65 0.59 0.58 0.66 0.85 Visual Hallucinations 66 27 - 0 2 - 4 7 05 0,23 0.12 0.32 0.57 0.73 Voices Commenting 65 - 14 - 36 58 25 0,70 0.76 0.82 0.75 0.97 Thought Insertion 62 08 35 11 - 2 2 0.34 0.33 0.32 0.32 0.60 Being Controlled 55 38 33 20 17 0,38 0.69 0.64 0.63 0.62 Grandiosity - 0 6 92 19 - 0 1 - 2 1 0.01 0.90 0.84 0.90 0.94 Grandiose Delusions 05 86 02 03 - 14 0.01 0.74 0.74 0.77 0.76 Religious Delusions 17 79 - 2 5 - 2 2 42 0.02 0.38 0.39 0.72 0.93 Unusual Thought Content - 2 5 63 14 17 31 0.00 0.22 0.27 0.43 0.60 Delusions of Reference 29 45 28 11 24 0.20 0.41 0.36 0.42 0.43 Delusions of Persecution - 0 4 11 78 10 05 0.05 0.14 0.40 0.53 0.94 Suspiciousness 14 12 68 17 10 0.04 0.14 0.40 0.28 0.53 Though Broadcasting 10 10 - 12 95 19 0.36 0.48 0.41 0.66 0.94 Mind Reading 19 08 45 64 - 0 8 0.19 0.40 0.49 0.61 0.66 Somatic Concern 21 04 40 - 2 6 79 0.23 0.21 0.20 0.85 0.89 Somatic Delusions 36 17 --08 29 66 0.44 0.44 0.39 0.56 0.68 Somatic Hallucinations 21 - 2 4 63 02 57 0.25 0.37 0.54 0.84 0.83
Significance of added factors )~2 df p Factor 2 86.10 18 < 0.001 Factor 3 30.56 17 <0.05 Factor 4 45.30 16 <0.001 Factor 5 40.36 15 <0.001
The analysis is based on patterns of presence/absence (mild or above) of symptoms. Factor loadings are shown for a five-factor solution with orthogonal rotation. Communalities are shown for this solution and all lower order solutions.
G. W. Stuart et al./Schizophrenia Research 16 ( 1995j 175-188 183
factors representing somatic disturbances and paranoia. However, both the original correlations and an inspection of the binary patterns of co-occurrence with paranoia symptoms indicated that this result was not genuine, but due to the residual lack of fit of the five-factor model.
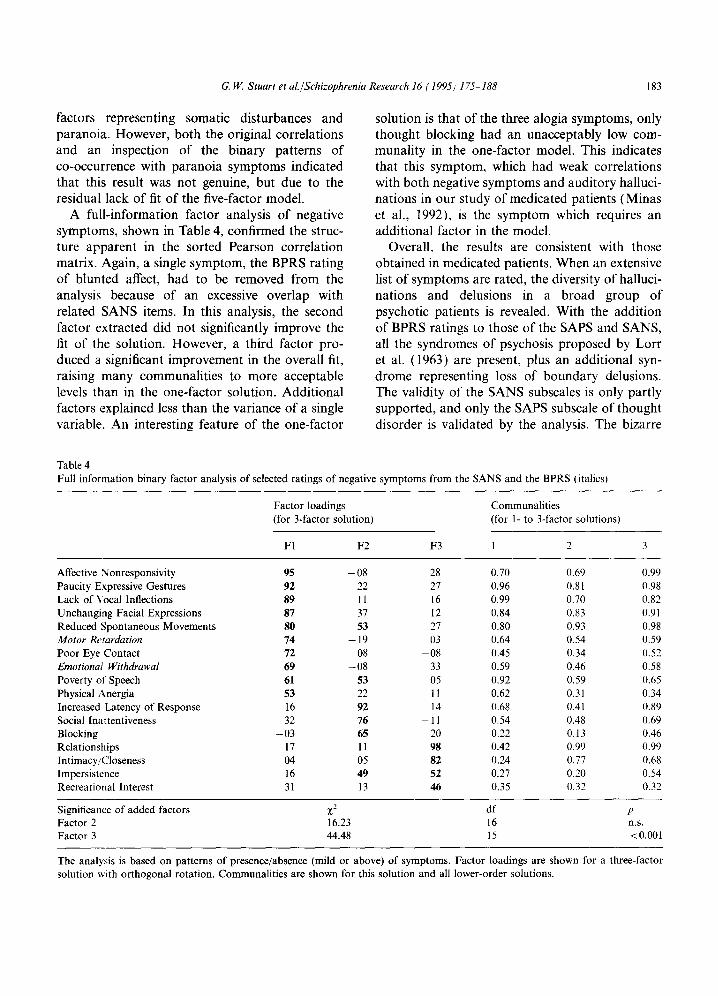
A full-information factor analysis of negative symptoms, shown in Table 4, confirmed the struc- ture apparent in the sorted Pearson correlation matrix. Again, a single symptom, the BPRS rating of blunted affect, had to be removed from the analysis because of an excessive overlap with related SANS items. In this analysis, the second factor extracted did not significantly improve the fit of the solution. However, a third factor pro- duced a significant improvement in the overall fit, raising many communalities to more acceptable levels than in the one-factor solution. Additional factors explained less than the variance of a single variable. An interesting feature of the one-factor
solution is that of the three alogia symptoms, only thought blocking had an unacceptably low com- munality in the one-factor model. This indicates that this symptom, which had weak correlations with both negative symptoms and auditory halluci- nations in our study of medicated patients (Minas et al., 1992), is the symptom which requires an additional factor in the model.
Overall, the results are consistent with those obtained in medicated patients. When an extensive list of symptoms are rated, the diversity of halluci- nations and delusions in a broad group of psychotic patients is revealed. With the addition of BPRS ratings to those of the SAPS and SANS, all the syndromes of psychosis proposed by Lorr et al. (1963) are present, plus an additional syn- drome representing loss of boundary delusions. The validity of the SANS subscales is only partly supported, and only the SAPS subscale of thought disorder is validated by the analysis. The bizarre
Table 4 Full information binary factor analysis o f selected ratings of negative symptoms from the SANS and the BPRS (italicsj
Factor loadings (for 3-factor solution)
Communali t ies (for 1- to 3-factor solutionsl
F1 F2 F3 1 2 3
Affective Nonresponsivity 95 - 0 8 28 0.70 0.69 0.99 Paucity Expressive Gestures 92 22 27 0.96 0.81 0.98 Lack of Vocal Inflections 89 ! 1 16 0.99 0.70 0.82 Unchanging Facial Expressions 87 37 12 0.84 0.83 0.91 Reduced Spontaneous Movements 80 53 27 0.80 0.93 0.98 Motor Retardation 74 - 19 03 0.64 0.54 0.59 Poor Eye Contact 72 08 - 0 8 0.45 0.34 0.52 Emotional Withdrawal 69 - 0 8 33 0.59 0.46 0.58 Poverty of Speech 61 53 05 0.92 0.59 0.65 Physical Anergia 53 22 11 0.62 0.31 0.34 Increased Latency of Response 16 92 14 0.68 0.41 0.89 Social Inattentiveness 32 76 - 11 0.54 0.48 0.69 Blocking - 03 65 20 0.22 0.13 0.46 Relationships 17 11 98 0.42 0.99 0.99 Intimacy/Closeness 04 05 82 0.24 0.77 0.68 Impersistence 16 49 52 0.27 0.20 0.54 Recreational Interest 31 13 46 0.35 0.32 0.32
Significance of added factors Z z d f p Factor 2 16.23 16 n.s. Factor 3 44.48 15 < 0.001
The analysis is based on patterns of presence/absence (mild or above) of symptoms. Factor Ioadings are shown for a three-factor solution with orthogonal rotation. Communali t ies are shown for this solution and all lower-order solutions.
184 G. W. Stuart et al./Schizophrenia Research 16 (1995) 175-188
behavior subscale is not internally consistent, and hallucinations and delusions are spread over five factors, rather than the two subscales of the SAPS.
4. Discussion
This study has confirmed and extended the syndrome structure that we previously uncovered in a sample of medicated patients, whether suffer- ing from schizophrenia or other psychotic disor- ders (Minas et al., 1992; 1993). The small sample size prevented such a comparison in the present sample, but two thirds of the sample were diag- nosed with either schizophrenia or schizophreni- form disorder, and so the model is likely to be valid for this subgroup. Neither the positive-nega- tive dichotomy, nor its successor, the three syn- drome model, are adequate descriptive models of the symptoms of psychosis. In the domain of symptoms defined by the SAPS/SANS, the syn- drome structure was very similar in both medicated and neuroleptic-free patients, despite the lower frequency of negative symptoms in the present sample. In both cases, thought disorder emerged as a coherent syndrome, as in the three-syndrome model. All the core negative symptoms were inter- correlated, although there was some additional structure which may reflect the presence of three related syndromes, one representing fiat affect, the others alogia (particularly 'blocking') and social dysfunctions (apathy and anhedonia). Hallucinations and delusions fell into the five syndromes of somatic disturbances, visual/audi- tory hallucinations, loss of boundary delusions, grandiosity and paranoia, all phenomenologically distinct, but most importantly, showing a degree of statistical independence.
The finding that there is additional structure within the negative syndrome group, but which does not correspond exactly to the subscales of the SANS, is consistent with previous research, despite some variation in the names used for different factors. Both Gibbons et al. (1985) and Berenbaum et ai. (1987) desribed factors which corresponded to the syndromes of flat affect and social dysfunctions. In the present sample, the symptom of 'blocking' formed the basis of an
additional negative syndrome. This symptom was not part of any major syndrome in our medicated sample (Minas et al., 1992), which is consistent with other studies (Andreasen and Olsen, 1982; Miller et al., 1993). Others have argued for more than three negative syndromes on the basis of orthogonal factor analysis (Alphs et al., 1989) However, since only the highest factor loading for each item was given, this claim is difficult to evaluate. It has been shown in other joint analyses of the SANS and the BPRS that all SANS subs- cales are correlated quite highly with the negative symptom ratings of the BPRS, although the SANS subscales each carry a small amount of additional information (Thiemann et al., 1987; Czobor et al., 1991; Gur et al., 1991). This supports our finding that syndromes within the broad group of negative symptoms are not independent.
It was notable that although in neuroleptic-free patients there was an independent negative syn- drome, it was associated with the BPRS symptom of depression, and inversely correlated with the symptoms excitement and pressure of speech, and to a lesser extent, grandiosity. This raises the question of whether some of the negative symp- toms seen in this sample represent vegetative symp- toms of depression, rather than negative symptoms of psychosis. This finding is inconsistent with those of Prosser et al. (1987), Jackson et al. (1989) and Kulhara et al. (1989), who reported that in neuroleptic-medicated patients depression and affective blunting occurred independently. It is possible that, in medicated patients, parkinsonian side-effects may mimic negative symptoms (Prosser et al., 1987). If such symptoms are induced by medication in the absence of depression, they will show a reduced relationship with depressive symp- toms. As Carpenter et al. (1985) have argued, either class of symptoms (vegetative symptoms of depression, or medication side effects) may be difficult to distinguish on a cross-sectional basis from the true 'deficit state' which is characterised by a more persistent course.
Turning to the positive symptoms, hallucina- tions and delusions clearly do not represent a unitary syndrome. In our view, the principal defi- ciency with the subscale structure of the SAPS, as well as with the 'three-syndrome' model, is the

G. W. Stuart et al./Schizophrenia Research 16 (1995) 175-188 185
lack of a separate scale which measures paranoia. The independence of this syndrome has been estab- lished since the first factor-analytic studies were carried out (Lorr et al., 1963). It consistently emerges in studies which use the BPRS (Guy et al., 1976; Simpson and Davis, 1985). In a recent study which also used unmedicated patients, Bigelow and Berthot (1989), using a modified BPRS, found three 'positive symptoms' factors, one of which clearly represented paranoid symptoms. Paranoia is clinically a very important syndrome. Of all the possible subtypes of schizophrenia, it has been suggested that the paranoid/nonparanoid distinc- tion is best supported empirically (Nicholson and Neufeld, 1993).
Despite this evidence, in more recent research paranoia has been given reduced emphasis, or has been incorporated into a general delusions factor. There are several reasons which can be identified for this development. The SAPS was developed on an a priori theoretical basis, and then was valid- ated using an analysis of internal consistency (Andreasen and Grove, 1986). This approach has two drawbacks: alternative models are not exam- ined, and the unidimensionality of subscales may be accepted due to the use of internal consistency measures which do not necessarily reveal multidi- mensionality (Green et al., 1975). In the case of subsequent studies using the SAPS, this has had the unfortunate side effect of excluding paranoia at the subscale or global rating level. Most recent studies which discount paranoia as a separate syndrome have either (i) followed the precedent of employing a global rating of delusions which subsumes delusions of persecution (Liddle and Barnes, 1990; and see Klimidis et al., 1993), (ii) have oxerlooked a single rating of persecutory delusions because factor analysis has been used, which (in contrast to principal components analy- sis) excludes the unique variance of individual measures from consideration (Liddle, 1987; Silver et al., 1993), or (iii) have been prepared to discard it from the symptom model when it does not fit (Kay and Sevy, 1990; Bell et al., 1994). When delusions of persecution is the only paranoid symp- tom included it then (at best) becomes part of a 'weak' factor, or appears as an outlier variable in factor analysis.
Aside from paranoia, within the domain of hallucinations and delusions four other syndromes have been identified: auditory and visual hallucina- tions, loss of boundary delusions, grandiosity and somatic disturbances. In our previous study of medicated patients (Minas et al., 1992) loss of boundary phenomena did not fall clearly into either category of hallucinations or delusions. In the present study, factor analysis indicated that they may be more closely associated with halluci- nations. In a recent study which used the individual ratings from the SAPS and SANS, Malla et al. (1992) obtained results which are consistent with this view. Although a three factor solution was reported, the hallucinations and delusions factor had high loadings from both auditory hallucina- tions and loss of boundary delusions. Religious and grandiose delusions had weak loadings on this factor, and persecutory delusions loaded weakly on both the thought disorder and hallucinations/ delusions factors. This finding provides further evidence for a closer relationship between loss of boundary delusions and hallucinations than other types of delusion.
Frith and Done (1988) have argued that both hallucinations and loss of boundary phenomena, in particular thought insertion, are due to a failure to distinguish self-generated from externally gener- ated experiences. Hence loss of boundary delusions might be regarded as false perceptions as much as false beliefs. Nonetheless, loss of boundary delu- sions show a degree of independence from both hallucinations and other delusions. It would seem appropriate, given this degree of independence, and their status in many instances as Schneiderian first-rank symptoms of schizophrenia, to treat them as a distinct psychotic syndrome, rather than merge them with either hallucinations or other types of delusion.
In addition to symptoms which fit within the syndromes discussed so far, there is evidence for Lorr et al.'s syndromes (1963) of hostile belliger- ence, mannerisms/posturing and disorientation. Although each of these was represented by only a pair of symptoms, they were not strongly corre- lated with any other syndrome. Neither were some single ratings such as inappropriate affect, which occupies an uncertain status within the scheme of

186 G. I41.. Stuart et al./Schizophrenia Research 16 (1995) 175-188
positive and negative symptoms, being originally proposed as a negative symptom (Andreasen, 1983), but now thought to be more related to thought disorder (Miller et al., 1993). In particu- lar, it is not clear that the items of the bizarre behaviour subscale form a coherent syndrome. We have found little correlation between individual symptoms in medicated patients (Minas et al., 1992), and symptoms such as aggression, socially inappropriate behaviors, and stereotypies are phe- nomenologically distinct. Perhaps their 'bizarre- ness' does not reflect any common underlying cause. At this point, there would seem to be more justification for recognising a syndrome limited to particular forms of motor disturbance, as sug- gested by Lorr et al. (1963).
At a practical level, it can be concluded from the above discussion that the BPRS seems to be a better-balanced and more extensive short instru- ment for ratings of psychotic symptoms than the global ratings of the SAPS and SANS. The BPRS differentiates paranoid and grandiose delusions. However it may be useful to further discriminate between 'other' delusions represented by the item 'unusual thought content', as it is clear that loss of boundary delusions in particular might usefully be rated separately. Perhaps this item could be redefined to specifically exclude grandiose or para- noid delusions, as the analysis suggests that in our sample these were the main components of unusual thought content. The tight correlation between BPRS negative symptoms, particularly blunted affect and emotional withdrawal, suggests that these could be merged, and new items tapping negative symptoms of alogia or apathy/anhedonia could be added. However the existing structure has the advantage that it taps the 'core' features of the negative syndrome. Nevertheless, it is clear that further improvements to the BPRS, or the development of an alternative brief rating scale, are possible.
To conclude, we would argue strongly in favour of historical continuity in research into psychopa- thology. Models such as that proposed by Lorr et al. (1963) should not be abandoned in favour of lower-dimensional models unless it is established that the rating instruments and the patient groups are extensive enough, and the statistical methods
appropriate, to reveal the relevant syndromes. The three-syndrome model may be reasonably valid in studies of medicated chronic schizophrenia (although there is evidence that some elaboration of the three-syndrome model is possible with more detailed measurement of symptoms). This group of patients, who often have enduring, treatment resistant negative symptoms, are suitable subjects for studying the biological basis of negative symp- toms and evaluating new treatments for them. However, the three-syndrome model has gained a wider currency, as a result of studies of more broad groups of patients using restricted symptom lists such as the global ratings of the SAPS and SANS. For example, Miller et al. (1993) have recently argued that 'the use of three dimensions may be a robust way to further explore the rela- tionship between signs and symptoms and their underlying mechanisms' (p. 221 ). Given the results of item-level analyses of the SAPS and SANS, and the historical evidence for the existence of more than three psychotic syndromes, the use of the three-syndrome model has the potential to hinder studies of the underlying mechanisms of positive symptoms. The three-syndrome model treats as equivalent symptoms as diverse as visual hallucina- tions and grandiose delusions - symptoms which have been demonstrated to belong to distinct syn- dromes outside the realm of chronic schizophrenia.
References
American Psychiatric Association (1987) Diagnostic and Statistical Manual of Mental Disorders (Third Edition, Revised). Washington, DC, American Psychiatric Association.
Alphs, L.D., Summerfelt, B.S., Lann, H. and Muller, R.J. (1989) The Negative Symptom Assessment: A new instru- ment to assess negative symptoms of schizophrenia. Psychopharmacol. Bull. 25. 159-163.
Andreasen, N.C. (1983) Scale for the Assessment of Negative Symptoms (SANS). Iowa City, IA, University of Iowa.
Andreasen, N.C. (1984) Scale for the Assessment of Positive Symptoms (SAPS). Iowa City, 1A, University of Iowa.
Andreasen, N.C. (1985) Positive vs. negative schizophrenia: a critical evaluation. Schizophr. Bull. 11, 380-389.
Andreasen, N.C. and Grove, W. (1986) Evaluation of positive and negative symptoms in schizophrenia. Psychiat. Biol. 1, 108-121
G. IV.. Stuart et al./Schizophrenia Research 16 (1995) 175-188 187
Andreasen, N.C. and Olsen, S. (1982) Negative vs positive schizophrenia: Definition and validation. Arch. Gen. Psychiatry. 39, 789-794.
Bell, R.C., Low, L.H., Jackson, H.J., Dudgeon, P.L., Copolov, D.L. and Singh, B.S. (1994) Latent trait modelling of symptoms of schizophrenia. Psychol. Med. 24, 335-345.
Berenbaum, S.A., Abrams, R., Rosenberg, S. and Taylor, M.A. (1987) The nature of emotional blunting: A factor- analytic study. Psychiatry Res. 20, 57-57.
Bernstein. I.H. and Teng, G. (1989) Factoring items and factoring scales are different: Spurious evidence for multidi- mensionality due to item categorization. Psychol. Bull. 105, 46 ~ 477.
Bigelow, L.B. and Berthot, B.D. (1989) The Psychiatric Symptom Assessment Scale (PSAS) Psychopharmacol. Bull. 25, 168-177.
Bilder, R M., Mukherjee, S., Reider, R.O. and Pandurangi, A.K. (19851 Symptomatic and neuropsychological compo- nents of defect states. Schizophr. Bull. 11,409-419.
Bock, R.D., Gibbons, R. and Muraki, E. (1988) Full- information item factor analysis. Appl. Psychol. Meas. 12, 261 -280.
Brown, K.W. and White, T. (1992) Syndromes of chronic schizophrenia and some clinical correlates. Br. J. Psychiat. 161, 31--322.
Carpenter. W.T., Heinrichs, D.W. and Alphs, L.D. (1985) Treatment of negative syndromes. Schizophr. Bull. 11, 440 452.
Crow, T.J (1980) Molecular pathology of schizophrenia: more than one disease process? Br. Med. J. 280, 66-68.
Crow, T..I. (1985) The two-syndrome concept: origins and current status. Schizophr. Bull. 11,471-486.
Czobor, P., Bitter, I. and Volavka, J. (1991) Relationship between the Brief Psychiatric Rating Scale and the Scale for the Assessment of Negative Symptoms: A study of their correlauon and redundancy. Psychiatry Res. 36, 129-139.
Everitt, B.S. Cluster Analysis. Heinemann, London, UK. Fenton, V~ .S. and McGlashan, T.H. (1991) Natural history of
schizophrenia subtypes. II. Positive and negative symptoms and long-term course. Arch. Gen. Psychiatry 48, 978 986.
Frith, C.D and Done, D.J. (1988) Towards a neuropsychology of schizophrenia. Br. J. Psychiat. 153, 437 443.
Green, S.B., Lissitz, R.W. and Mulaik, S.A. (1977) Limitations of coefficient alpha as an index of test unidimensionality. Educat. Psychol. Meas. 37, 827-838.
Gibbons, R.D., Lewine, R.R.J., Davis, J.M., Schooler, N.R. and Cole, J.O. (1985) An empirical test of a Kraepelinian vs a Blealerian view of negative symptoms. Schizophr. Bull. 11, 390 396.
Gorsuch, R.L. (1983) Factor Analysis (2nd ed.) Hillsdale, N J, Earlbaum.
Guy, W. (Editor) (1976) ECDEU Assessment Manual for Psychopharmacology, Revised Edition. Washington, DC: U.S, Department of Health, Education and Welfare. Publication No (ADM) 76-338, 157-169.
Gur, R.E.. Mozley, P.D., Resnick, S.M., Levick, S., Erwin, R., Saykin, A.J. and Gur, R.C. (1991) Relations among
clinical scales in schizophrenia. Am. J. Psychiat. 148, 472-478.
Haberman, S.J. (1977) Log-linear models and frequency tables with small expected counts. Ann. Stat. 5, 1148-1169.
Jackson, H.J., Minas, I.H., Burgess, P.M., Joshua, S.D., Charisou, J. and Campbell, I,M. (1989) Is social skills performance a correlate of schizophrenia subtypes? Schizophr. Res. 2, 301-309.
Jorgensen, P. and Jensen, J. (1990) A dimensional approach to severe delusional psychoses. Psychopathology, 23, 9-14.
Kay, S.R. and Sevy, S. (1990) Pyramidical model of schizophre- nia. Schizophr. Bull. 16, 537-545.
Keks, N., Copolov, D.L., Mackie, B., Stuart, G.W., Singh, B.S., McGorry, P.D and Coffey, C. (1991) Comparison of participants and nonparticipants in a neuroendocrine investi- gation of psychosis. Acta Psychiatr. Scand. 83, 373-376.
Klimidis, S., Stuart, G.W., Minas, I.H., Copolo~, D.L. and Singh, B.S. (1993) Positive and negative symptoms in the psychoses: Re-analysis of published SAPS and SANS global ratings. Schizophr. Res. 9, 11 18.
Kulhara, P., Avasthi, A., Chadda, R., Chandiramani. K., Mattoo, S.K., Kota, S.K. and Joseph, S. (1989) Negative and depressive symptoms in schizophrenia. Br. J. Psychiat. 154, 207 211.
Liddle, P.F. (1987~ The symptoms of chronic schizophrenia: A re-examination of the positive-negative dichotomy. Br. J. Psychiat. 151, 145-151.
Liddle, P.F. and Barnes, T.R.E. (1990) Syndromes of chronic schizophrenia. Br. J. Psychiat. 157, 558-561.
Lorr, M. (1988) Classifying psychotics: Dimensional and categorical approaches. In T. Millon and G.L. Klerman (Editors). Contemporary Directions in Psychopathology: Toward the DSM-IV. The Guilford Press: New York.
Lorr, M., Klett, C.J. and McNair, D.M. (1963) Syndromes of Psychosis. MacMillan: New York.
Malla, A.K., Norman, R.M.G., Williamson, P., Cortese, L. and Diaz, F. (1992) Three-syndrome concept of schizophre- nia: A factor-analytic study. Schizophr. Res. 10, 143 150.
McGorry, P.D., Goodwin, R.J. and Stuart, G.W. (1988) The development, use and reliability of the brief psychiatric rating scale (nursing modification)-an assessment procedure for the nursing team in clinical and research settings. Compr. Psychiat. 29, 575 -587.
McGrath, J. ( 1991 ~ Ordering thoughts on thought disorder. Brit. J. Psychiat. 158, 307 316.
Miller, D.D., Arndt, S. and Andreasen, N.C. (1993) Alogia, attentional impairment and inappropriate affect: their status in the dimensions of schizophrenia. Compr. Psychiat. 34, 221-226.
Minas, I.H., Stuart, G.W., Klimidis, S., Jackson, H.J., Singh, B.S. and Copolov, D.L. (1992) Positive and negative symptoms in the psychoses: Multidimensional scaling of SAPS and SANS items. Schizophr. Res. 8, 143 156.
Minas, I.H., Klimidis, S., Stuart, G.W., Copolov, D.L. and Singh, B.S. (1993) Positive and negative symptoms in the psychoses: Principal components analysis of SAPS and SANS items. Compr. Psychiat. 35, 135-144.

188 G. IV.. Stuart et al./Schizophrenia Research 16 (1995) 175-188
Nicholson, I.R. and Neufeld, R.W.J. (1993) Classification of the schizophrenias according to symptomatology: A two- factor model. J. Abnorm. Psychol. 102, 259-270.
Overall, J.E. and Gorham, D.R. (1962) Brief Psychiatric Rating Scale. Psychol. Rep. 10, 799-812.
Peralta, V., de Leon, J. and Cuesta, M.J. (1992) Are there more than two syndromes in schizophrenia? A critique of the positive-negative dichotomy. Br. J. Psychiat. 161, 335-343.
Prosser, E.S., Csernansky, J.G., Kaplan, J., Thiemann, S., Becker, T.J., Hollister, L.E. (1987) Depression, Parkinsonian symptoms and negative symptoms in schizophrenics treated with neuroleptics. J. Nerv. Ment. Dis. 175, 100-105.
Silver, H., David, D., Kaplan, M., Hadjez, J., Tubi, N., Darnel, A., Calev, A. and Lerer, B. (1993) Factor analysis of schizophrenic symptoms and comparison of different rating scales. Schizophr. Res. 10, 67-75.
Simpson, D.M. and Davis, G.C. (1985) Measuring thought
disorder with clinical rating scales in schizophrenic and nonschizophrenic patients. Psychiatr. Res. 15, 313-318.
Strauss, J.S., Carpenter, W.T. and Bartko, J.J. (1974) The diagnosis and understanding of schizophrenia, part III: Speculations on the processes that underlie schizophrenic symptoms and signs. Schizophr. Bull. 11, 61-75.
Thiemann, S., Csernansky, J.G. and Berger, P.A. (1987) Rating scales in research: The case of negative symptoms. Psychiatry Res. 20, 47 55.
Wilson, D.T., Wood, R. and Gibbons, R. (1991) TESTFACT: Test scoring, item statistics and item factor analysis. Chicago, Scientific Software Inc.
Wing, J.K., Cooper, J.E. and Sartorius, N. (1974) The Measurement and Classification of Psychiatric Symptoms. University of Cambridge Press: Cambridge.
Wolkowitz, O.M. and Pickar, D. (1991) Benzodiazepines in the treatment of schizophrenia: A review and reappraisal. Am. J. Psychiat. 148, 714-726.
Related Documents











