Prof. Marius Keel, MD, FACS General, Trauma and Orthopaedic Surgeon EBSQ Traumatology Emergency Physician Leitender Arzt für Becken- und Wirbelsäulenchirurgie Teamleiter Wirbelsäulenchirurgie Universitätsklinik für Orthopädische Chirurgie Inselspital, Bern (Poly)trauma during Pregnancy

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Prof. Marius Keel, MD, FACS
General, Trauma and Orthopaedic Surgeon
EBSQ Traumatology
Emergency Physician
Leitender Arzt für Becken- und Wirbelsäulenchirurgie
Teamleiter Wirbelsäulenchirurgie
Universitätsklinik für Orthopädische Chirurgie
Inselspital, Bern
(Poly)trauma during
Pregnancy

El Kady, et al. Am J Obstet Gynecol 2004;190:1661-8
> Motor vehicle crashes
> Falls
> Suicide attempts
> Assaults
> Fires
> Guns
0.08
0.09
0.00
0.02
0.00
0.00
Per 1000 deliveries
Group 1: Women who deliverd at time of trauma hospitalization
0.67
0.30
0.05
0.25
0.01
0.06
Group 2: Women who were hospitalized for trauma up to 9 months preceding the obstetric delivery hospitalization
Occurrence Rates of Injuries of Pregnant Women
> Retrospective cohort study 1991-1999
> 10„316 deliveries with injuries at delivery (group 1; n=2494) or injury prenatally (group 2; n=7822) in 4„833„286 total deliveries (0.2%)
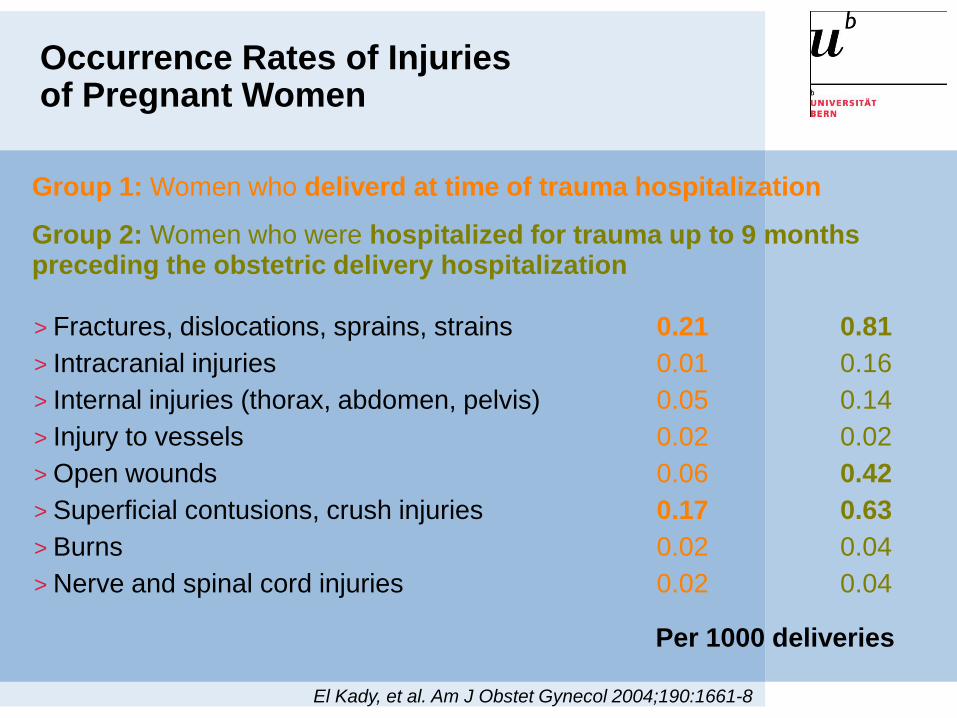
> Fractures, dislocations, sprains, strains
> Intracranial injuries
> Internal injuries (thorax, abdomen, pelvis)
> Injury to vessels
> Open wounds
> Superficial contusions, crush injuries
> Burns
> Nerve and spinal cord injuries
El Kady, et al. Am J Obstet Gynecol 2004;190:1661-8
Occurrence Rates of Injuries of Pregnant Women
0.21
0.01
0.05
0.02
0.06
0.17
0.02
0.02
0.81
0.16
0.14
0.02
0.42
0.63
0.04
0.04
Per 1000 deliveries
Group 1: Women who deliverd at time of trauma hospitalization
Group 2: Women who were hospitalized for trauma up to 9 months preceding the obstetric delivery hospitalization
Trauma-Management and Acute Surgery of Injured Pregnant Women
Pathophysiology
Damage Control
High qualified surgeon !
Obstetrician
„Life Saving Surgery“ and „Damage Control“
Who has the Lead ?

„Life Saving Surgery“ and „Damage Control“ of Two Patients !

Polytrauma during Pregnancy
>Trauma is the leading cause of maternal mortality and an important source of maternal morbidity.
> Initial treatment priorities for pregnant patient remain the same as for the non-pregnant patient.
>Best initial treatment for the fetus is the provision of optimal resuscitation of the mother and early assessment of the fetus.

Polytrauma
> Severity of injuries (ISS ≥17 pts.)
> Physiological status
Hypothermia
Acidosis
Coagulopathy
Lethal Triad
> Host defense
Keel et al. n=1191, 1.96-9.04; ISS≥17pts.
76%
25%
60%
32%
23%
58%
> Injury pattern
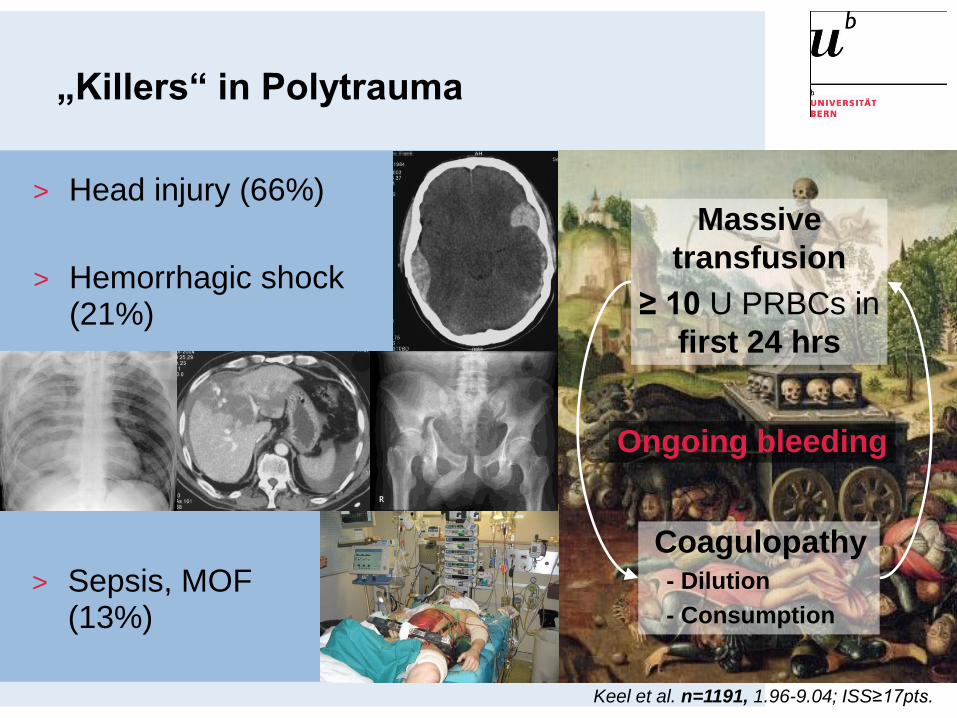
„Killers“ in Polytrauma
> Head injury (66%)
Keel et al. n=1191, 1.96-9.04; ISS≥17pts.
Coagulopathy- Dilution
- Consumption
Massive
transfusion
≥ 10 U PRBCs in
first 24 hrs
Ongoing bleeding
> Sepsis, MOF (13%)
> Hemorrhagic shock (21%)
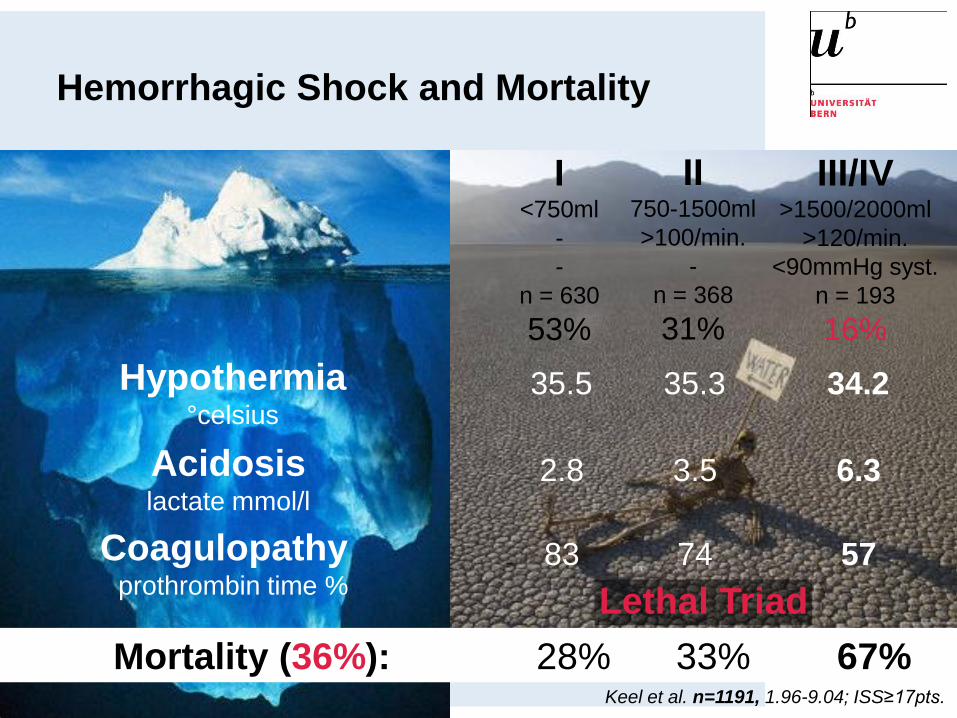
35.5Hypothermia°celsius
Acidosis lactate mmol/l
Coagulopathy prothrombin time %
2.8
83
35.3
3.5
74
34.2
6.3
57
Lethal Triad
Mortality (36%): 28% 33% 67%
Hemorrhagic Shock and Mortality
I<750ml
-
-
n = 630
53%
II750-1500ml
>100/min.
-
n = 368
31%
III/IV>1500/2000ml
>120/min.
<90mmHg syst.
n = 193
16%
Keel et al. n=1191, 1.96-9.04; ISS≥17pts.

Priorities of Acute Treatment
1. Shock treatment
2. Control of hemorrhage
3. Treatment of coagulopathy
Hypothermia
Acidosis
Coagulopathy
Lethal Triad
4. Prevention of septic
complications
5. Organ-/limb saving

Primary survey ATLS
X-ray (thorax, pelvis)
FAST
Multislice CT (7-12mSv)
Resuscitation:
Preservation of
perfusion and
oxygenation
Vital functions?
Response?Life saving
surgery_
„in extremis“
Keel M, Labler L, Trentz O.
Eur J Trauma 2005; 31:212

Diagnosticworkup is not a
warmup !
Primary survey
X-ray (thorax, pelvis) + FAST
versus
Multislice CT

Effect of Whole-body CT during Resuscitation on Survival Huber-Wagner et al. Lancet
2009;373:1455-61
> Retrospective, multicentre study(DGU) of patients with ISS >=16 pts. and blunt trauma
> N=4621 (ISS: 29.7 pts.; SBP<90: 15%)
> Whole-body CT: n=1494 (32%)
> Non-whole-body CT: n=3127 (no CT 22%, selective CT 78%)
> Standardised mortality ratio (SMR, ratio of recorded to expectedmortality)
> Whole-body CT is an independentpredictor for survival

MSCT: The Focus on SelectionDeunk et al. Ann Surg 2010;251

MSCT: The Focus on Radiation
> Retrospective cross-sectional study
> N=1119
> Effective doses
> Head CT: 2 mSv
> Abdominal/pelvis CT: 31 mSv
> Lifetime attributable risk (LAR) of cancer
> Head CT: 0.23 cancer/1000 pat. (20 year old women); 1/8105 (40 y.); 1/12250
> Abdom. CT: 4/1000 pat. (20 y.)
Smith-Bindmanet al. Arch Intern Med 2009;169:2078-86
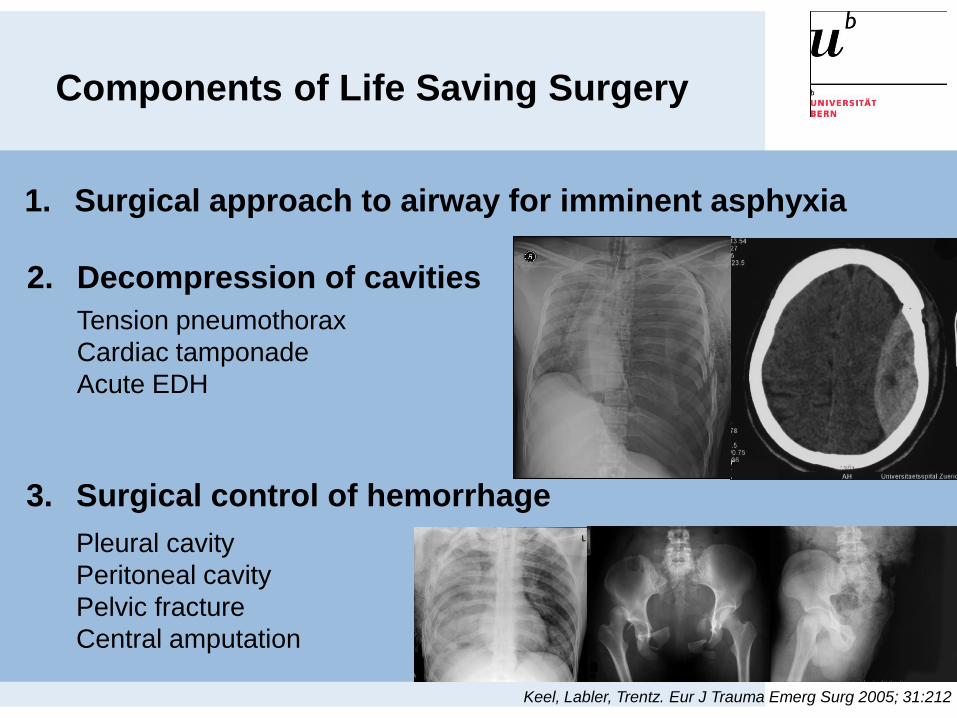
1. Surgical approach to airway for imminent asphyxia
3. Surgical control of hemorrhage
Pleural cavity
Peritoneal cavity
Pelvic fracture
Central amputation
Components of Life Saving Surgery
2. Decompression of cavities
Tension pneumothorax
Cardiac tamponade
Acute EDH
Keel, Labler, Trentz. Eur J Trauma Emerg Surg 2005; 31:212
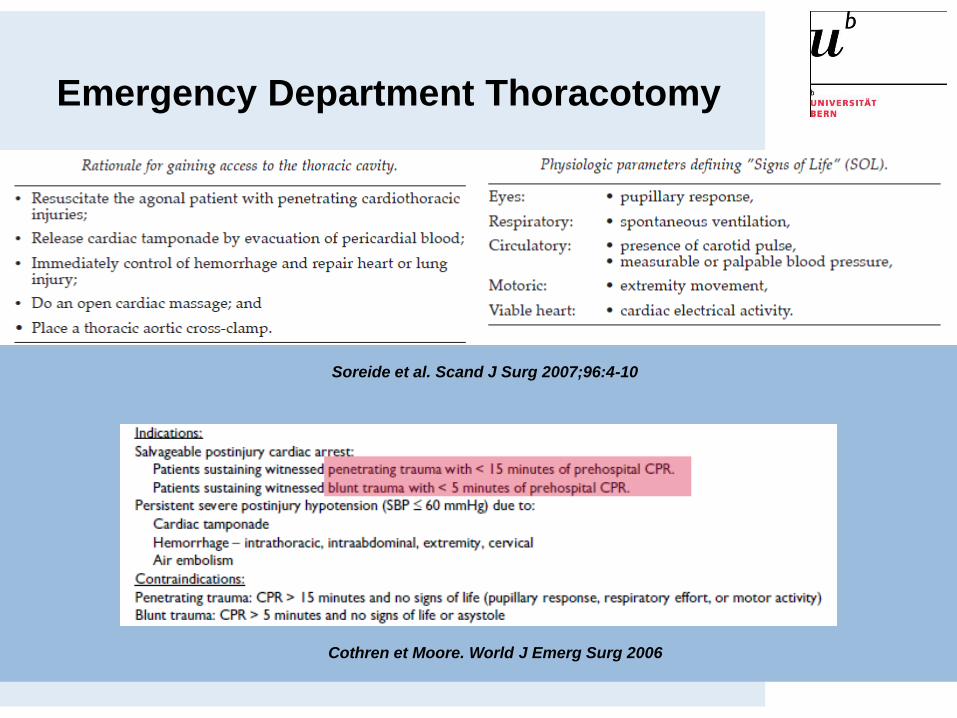
Emergency Department Thoracotomy
Soreide et al. Scand J Surg 2007;96:4-10
Cothren et Moore. World J Emerg Surg 2006
Physiologic Disorders -Posttraumatic CHAOS
> Cardiovascular shock
> Homeostasis
> Apoptosis
> Organ dysfunctions
> Immune Suppression
Bone. Crit Care Med 1996; 24:1125
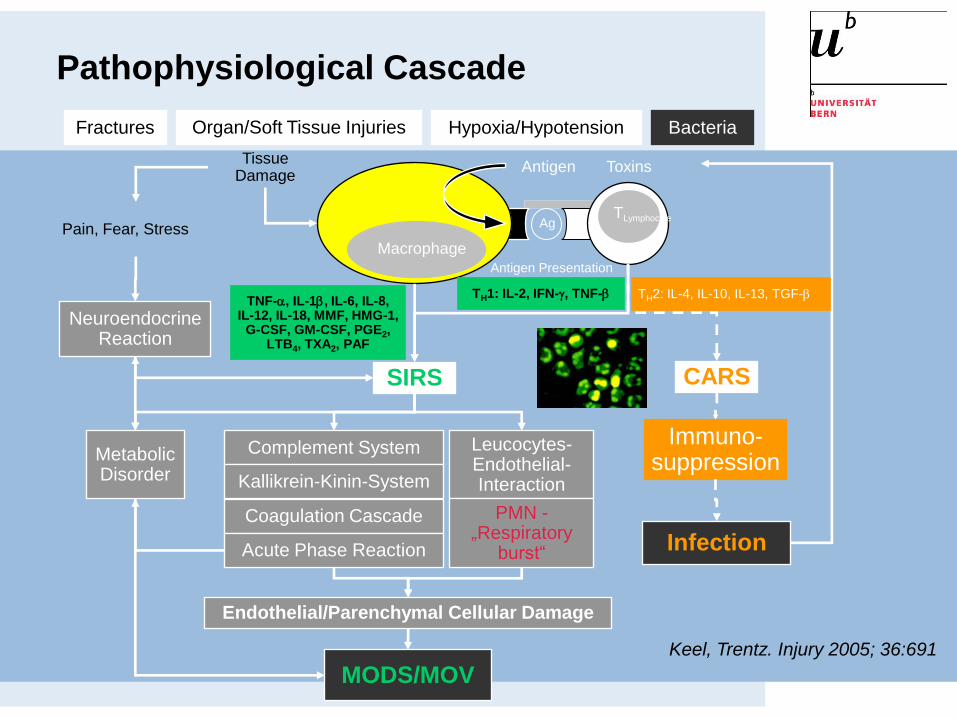
Pathophysiological Cascade
Endothelial/Parenchymal Cellular Damage
MODS/MOV
Neuroendocrine Reaction
Pain, Fear, Stress
Complement System Leucocytes-Endothelial-Interaction
PMN -„Respiratory
burst“
Coagulation Cascade
Acute Phase Reaction
Metabolic Disorder Kallikrein-Kinin-System
SIRS
AgTLymphocyte
Antigen Presentation
Antigen ToxinsTissue
Damage
Macrophage
TNF-a, IL-1b, IL-6, IL-8, IL-12, IL-18, MMF, HMG-1,
G-CSF, GM-CSF, PGE2, LTB4, TXA2, PAF
TH1: IL-2, IFN-g, TNF-b
Fractures BacteriaHypoxia/Hypotension
Keel, Trentz. Injury 2005; 36:691
CARS
Immuno-suppression
Infection
TH2: IL-4, IL-10, IL-13, TGF-b
Organ/Soft Tissue Injuries
21
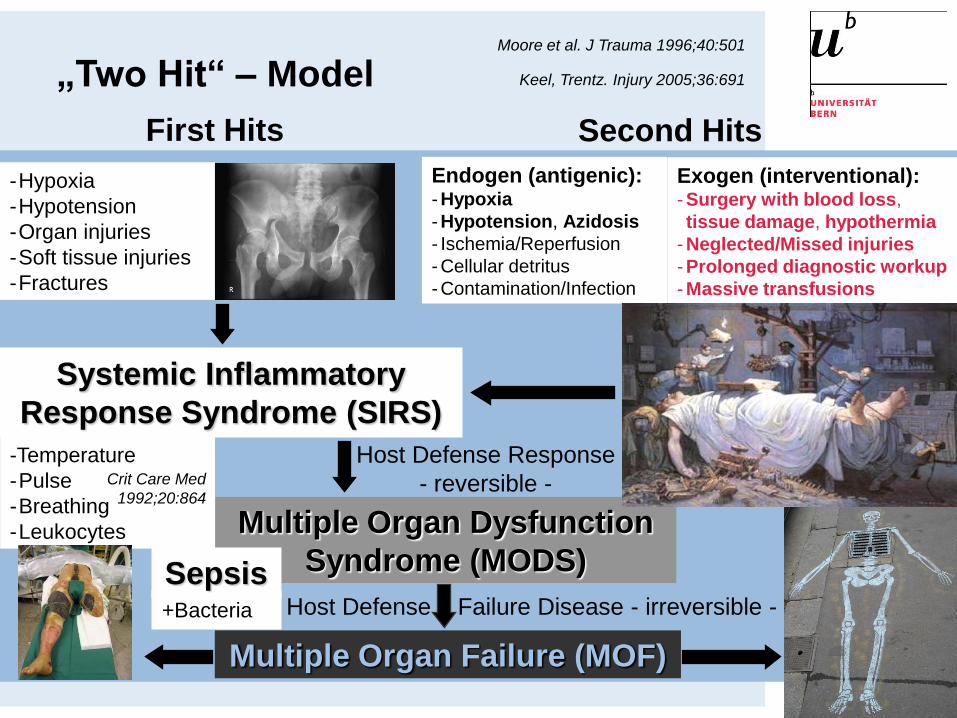
Multiple Organ Dysfunction
Syndrome (MODS)
Host Defense Response
- reversible -
„Two Hit“ – Model Keel, Trentz. Injury 2005;36:691
Moore et al. J Trauma 1996;40:501
First Hits
-Hypoxia
-Hypotension
-Organ injuries
-Soft tissue injuries
-Fractures
Systemic Inflammatory
Response Syndrome (SIRS)
-Temperature
-Pulse
-Breathing
-Leukocytes
Crit Care Med
1992;20:864
Multiple Organ Failure (MOF)
Host Defense Failure Disease - irreversible -+Bacteria
Sepsis
Second Hits
Endogen (antigenic): - Hypoxia
- Hypotension, Azidosis
- Ischemia/Reperfusion
- Cellular detritus
- Contamination/Infection
Exogen (interventional): - Surgery with blood loss,
tissue damage, hypothermia
- Neglected/Missed injuries
- Prolonged diagnostic workup
- Massive transfusions
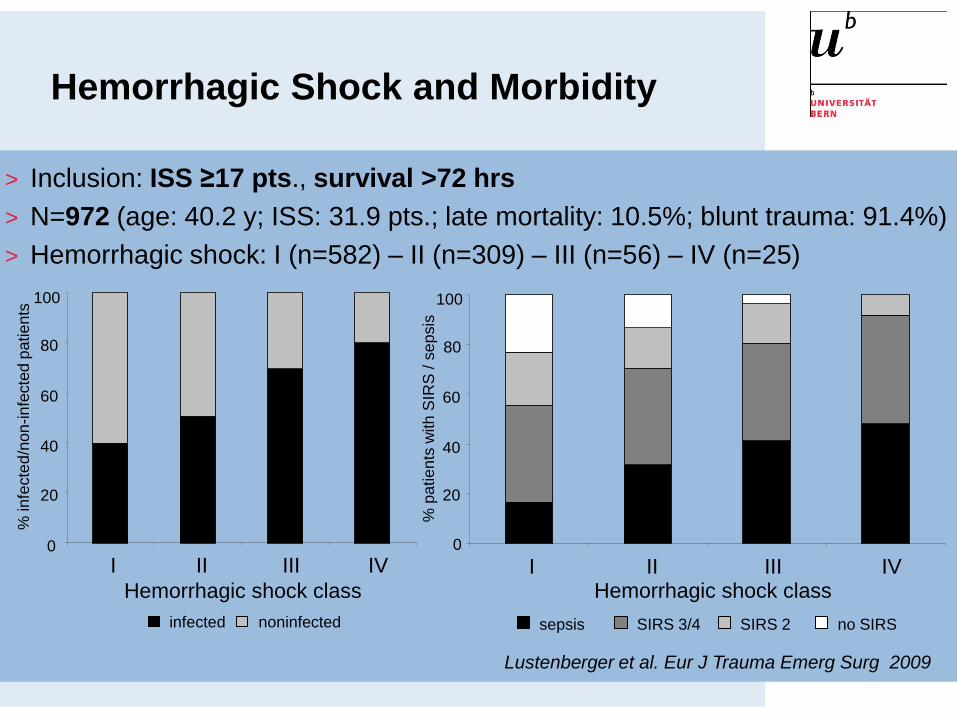
Hemorrhagic Shock and Morbidity
100
80
60
40
20
0
% infe
cte
d/n
on
-infe
cte
d p
atie
nts
infected noninfected
Hemorrhagic shock class
I II III IV
% p
atie
nts
with
SIR
S / s
ep
sis
100
80
60
40
20
0
no SIRSSIRS 3/4sepsis SIRS 2
I II III IVHemorrhagic shock class
> Inclusion: ISS ≥17 pts., survival >72 hrs
> N=972 (age: 40.2 y; ISS: 31.9 pts.; late mortality: 10.5%; blunt trauma: 91.4%)
> Hemorrhagic shock: I (n=582) – II (n=309) – III (n=56) – IV (n=25)
Lustenberger et al. Eur J Trauma Emerg Surg 2009
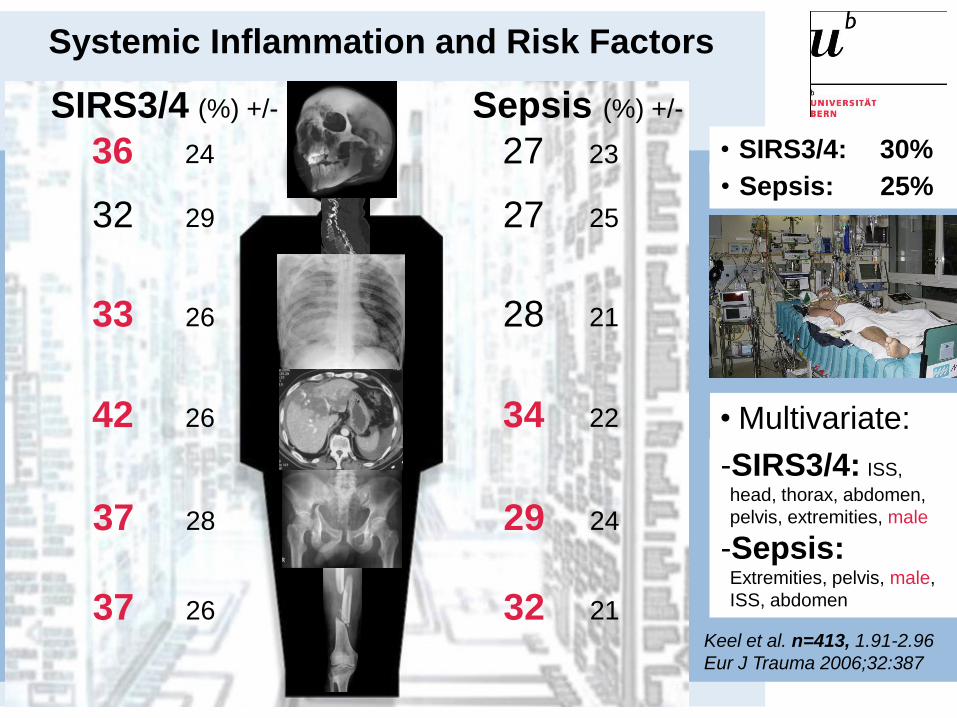
Systemic Inflammation and Risk Factors
Keel et al. n=413, 1.91-2.96
Eur J Trauma 2006;32:387
• SIRS3/4: 30%
• Multivariate:
-SIRS3/4: ISS,
head, thorax, abdomen,
pelvis, extremities, male
-Sepsis:Extremities, pelvis, male,
ISS, abdomen
27
Sepsis (%) +/-
27
28
34
29
32
23
25
21
22
24
21
• Sepsis: 25%
36
SIRS3/4 (%) +/-
32
33
42
37
37
24
29
26
26
28
26
Impact of Pregnancy on Trauma Mortality
John, et al. Surgery 2011;149:94.
> 1.46 million patients in The National Trauma Data Bank 2001-2005
> age 12-49; nonpregnant (n=214,394) and pregnant (HCG positive) (n=3„763
(1.72%)) women
> Pregnant women: younger, more minority groups, less severe injuries (ISS <9
pts.), lower proportion of severe head, abdominal or penetrating injuries
> Mortality for pregnant women 1.2% vs nonpregnant women 2.7%
> Multivariate analysis: Reduced mortality in younger pregnant women und
women with blunt trauma; no survival benefit in severely injured patients
> Survival advantage in premenopausal women with higher estrogen levels !
Deitch, et al. Ann Surg 2007;246:447.
> Estrogen and progesterone production by placenta throughout the gestation.
> Beneficial immunomodulatory and vasodilatory effects.
Angele, et al. Shock 2000;14:81.
Physiologic Alterations of Pregnancy
> Blood:
Plasma volume↑↑ and RBC(↑) – Hematocrit↓ (32%, physiologic anemia)
White-blood-cell↑ (15„000/mm3)
Fibrinogen↑
Prothrombin and partial thromboplastin times↓
Albumin↓, serum protein↓
pH↑
> Hemodynamics:
Cardiac output↑ (uterus and placenta receive 20% of CO in 3rd trimester; in supine position vena cava-compression 30%↓ of CO)
Heart rate↑ (10-15 beats/min. in 3rd trimester)
Blood pressure↓ (5-15mmHg in 2nd trimester, „Supine hypotensive syndrome“)
CVP↑ in lower extremities in 3rd trimester
ECG (shift leftward by 15°, flattened or inverted T waves)
Shock Tolerance during Pregnancy
>Better organ perfusion !
>Improved maternal tolerance to hemorrhage !
>Increased resistance to the „shock“ state in pregnant women !
> Respiratory system:
Tidal volume↑, residual volume↓ (diaphragmatic elevation)
PaCO2↓ (hypocapnia; values of 35-40mmHg may indicate impending respiratory failure during pregnancy)
Oxygen consumption↑
> GI-system:
Gastric emptying time↑
Early gastric tube decompression to avoid aspiration
> Urinary system:
Glomerular filtration rate↑, renal blood flow↑
Creatinine↓ und serum urea nitrogen↓
Dextrorotation of uterus lead to dilatation of right renal collection system
> Neurologic system:
Eclampsia mimic head injury (seizures, hypertension, hyperreflexia, proteinuria and peripheral edema)
Physiologic Alterations of Pregnancy
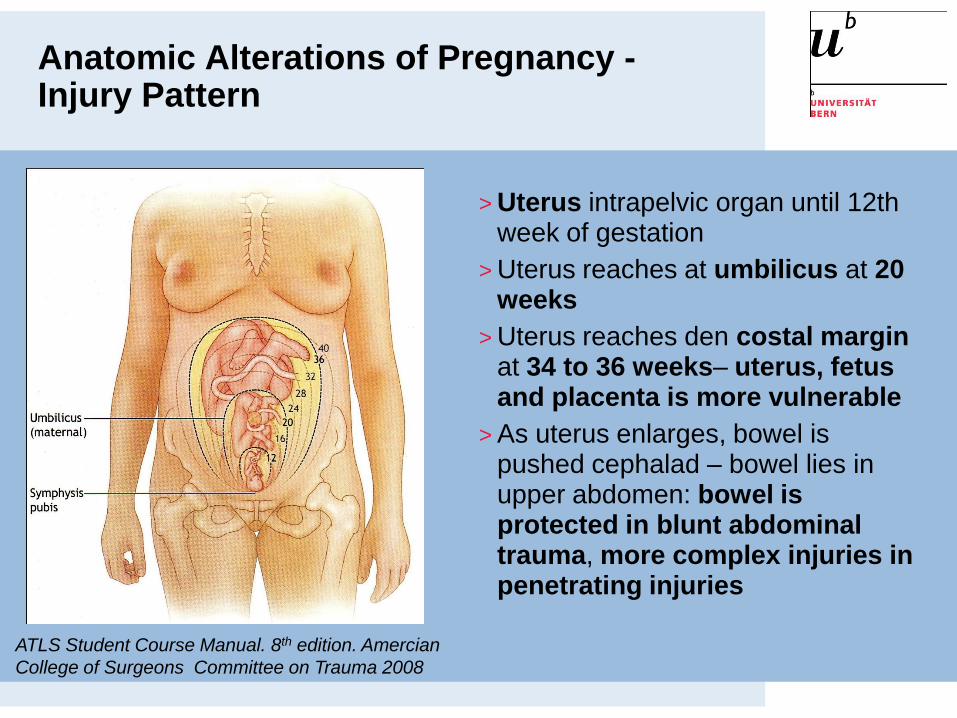
Anatomic Alterations of Pregnancy -Injury Pattern
ATLS Student Course Manual. 8th edition. Amercian
College of Surgeons Committee on Trauma 2008
> Uterus intrapelvic organ until 12th week of gestation
> Uterus reaches at umbilicus at 20 weeks
> Uterus reaches den costal marginat 34 to 36 weeks– uterus, fetus and placenta is more vulnerable
> As uterus enlarges, bowel is pushed cephalad – bowel lies in upper abdomen: bowel is protected in blunt abdominal trauma, more complex injuries in penetrating injuries
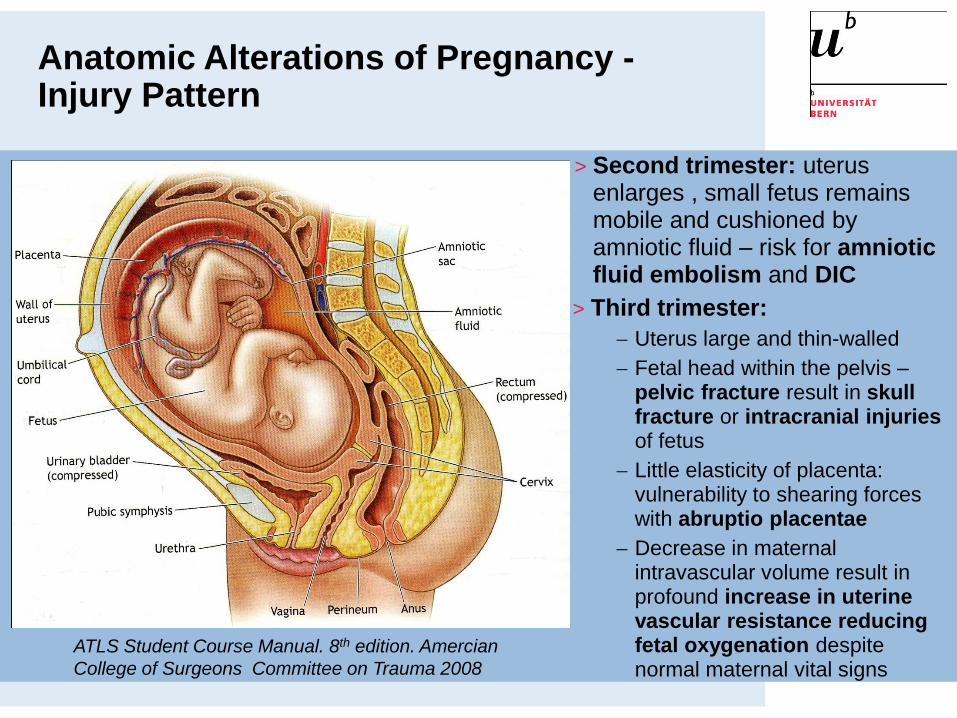
ATLS Student Course Manual. 8th edition. Amercian
College of Surgeons Committee on Trauma 2008
> Second trimester: uterus enlarges , small fetus remains mobile and cushioned by amniotic fluid – risk for amniotic fluid embolism and DIC
Anatomic Alterations of Pregnancy -Injury Pattern
> Third trimester:
Uterus large and thin-walled
Fetal head within the pelvis –pelvic fracture result in skull fracture or intracranial injuries of fetus
Little elasticity of placenta: vulnerability to shearing forces with abruptio placentae
Decrease in maternal intravascular volume result in profound increase in uterine vascular resistance reducing fetal oxygenation despite normal maternal vital signs
Damage Control Concept
Stop the bleeding –
Life Saving Surgery
Damage Control Surgery (DCO)
> Surgical control of hemorrhage
> Angiographic control of hemorrhage (Transcatheter arterial embolisation (TAE))
> Massive transfusion protocols (MTPs)
> Correction of coagulopathy
> Correction of hypothermia
Mitigate the lethal triad –
Damage Control Resuscitation

Damage Control – History – US Navy
> …keeping afloat a badly damaged ship by procedures tolimit flooding, stabilize the vessel, isolate fires andexplosions and avoid their spreading…
History: DC – DCO
> Pringle-maneuver Pringle. Ann Surg. 1908; 48:541
> Intra-abdominal packing Feliciano, et al. J Trauma. 1981; 21:285
> Damage Control as approach Rotondo, et al. J Trauma. 1993; 35:375
> Early packing – outcome Garrison, et al. J Trauma. 1996; 40:923
> Timing of fracture treatment – DCO (Damage Control Orthopaedic Surgery) Pape, et al. Am J Surg. 2002; 183:622

Trauma – Care
Primary survey
X-ray (thorax, pelvis)
FAST
Multislice CT ?
Resuscitation:
Preservation of
perfusion and
oxygenation
Vital functions?
Response?
Early total
care+
Intensive
care unit
Day-1-
surgery
_„borderline“
Keel, Labler, Trentz.
Eur J Trauma 2005; 31:212
Physiologic
balance?
Scoring?
Ressources?
Secondary survey
X-ray (extremities)
Multislice CT
+
„responder“
?„transient
responder“
Damage control:
• Preemptive intervention
Life saving
surgery
_„in extremis“
Damage control:
• Preemptive intervention
• „Bail-out“ procedure
Assessment and Treatment of Pregnant Women
>For optimal outcome of mother and fetus:
–Primary survey and resuscitation of mother
–Assess fetus
–Secondary survey of mother
>ABCDE - Adjuncts (CVP, pulse oximetry, arterial blood gas)
>Uterine compression of vena cava reduces CO - Pregnant patient should be logrolled 15° to left and uterus displaced manually to left !
>Because of increased intravascular volume pregnant patient with significant blood loss without clinical shock signs - fetus in distress and placenta is deprived of vital perfusion.
>Dense uterine muscle, amniotic fluid absorb energy frompenetrating injuries - low incidence of severe visceral inj.
Assessment and Treatment of Fetus
>Causes of fetal death:
–Maternal shock and maternal death
–Placental abruption: 70% vaginal bleeding, uterine tenderness, frequent uterine contractions, uterine tetany, uterine irritability (cave minor injuries)
–Uterine rupture: rare, abdominal tenderness/rigidity, repound tenderness, profound shock, abnormal fetal lie, easy palpation of extrauterine location of fetus
–Direct fetal injuries: late pregnancy and serious maternal injuries (blunt trauma (dashboard, wheel, blunt instrument), penetrating injuries
>Adjuncts: Uterine ultrasonography, X-ray, Doppler ultrasound (fetal heart tones)

Assessment and Treatment of Fetus
>Fetal heart rate is a sensitive indicator of both maternal blood volume satus and fetal well-being: Continuous fetal monitoring 6 hrs. (<20-24 weeks of gestation) - with risk factors for 24 hrs.
–Maternal heart rate >110 beats/min.
–ISS >9 pts.
–Placental abruption
–Fetal heart rate >160 or <120
–Ejection during a motor vehicle accident, motorcycle or pedestrian collisions

Secondary Survey of Pregnant Women
>Abdominal CT
>Uterine contractions?
>Evaluation of perineum
>Presence of amniotic fluid in vagina
>Vaginal examination
>Decision for emergency cesarean section (obstetrician)
>At time of maternal hypovolemic cardiac arrest fetus already sufferd prolonged hypoxia - perimortem cesarean section may be successful if performed within4-5 min. of arrest
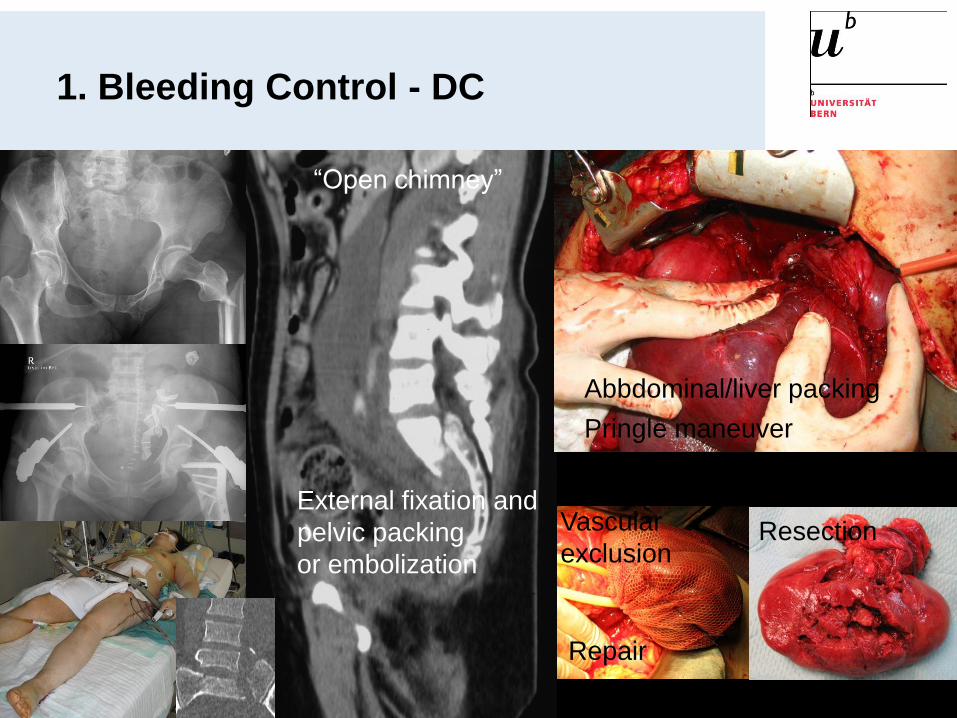
1. Bleeding Control - DC
“Open chimney”
Abbdominal/liver packing
Pringle maneuver
External fixation and
pelvic packing
or embolization
Repair
Vascular
exclusionResection
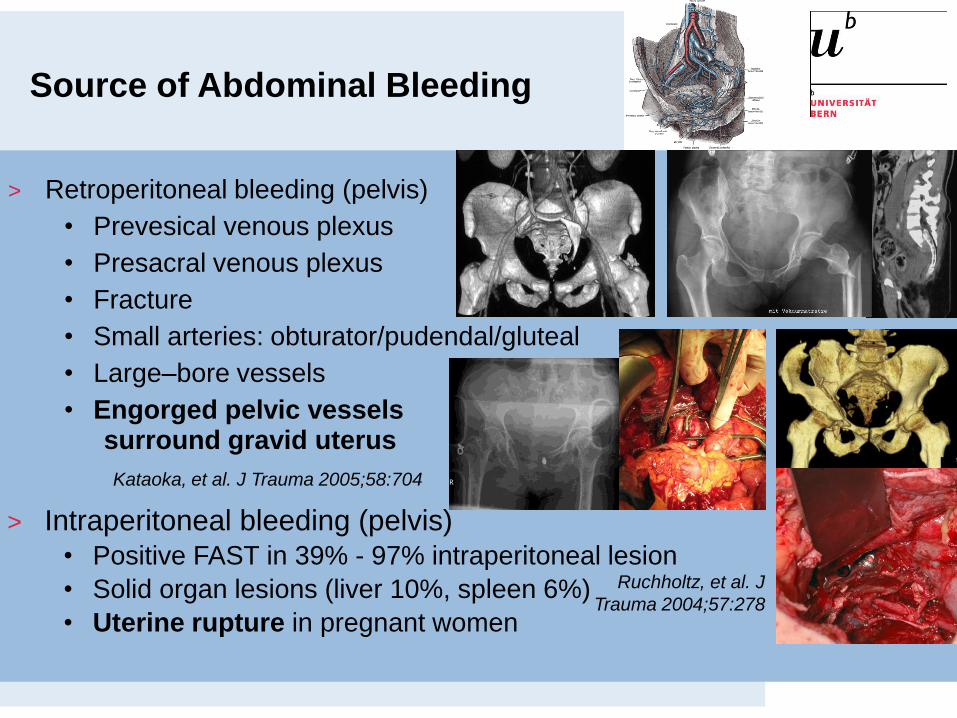
Source of Abdominal Bleeding
> Retroperitoneal bleeding (pelvis)
• Prevesical venous plexus
• Presacral venous plexus
• Fracture
• Small arteries: obturator/pudendal/gluteal
• Large–bore vessels
• Engorged pelvic vessels surround gravid uterus
> Intraperitoneal bleeding (pelvis)• Positive FAST in 39% - 97% intraperitoneal lesion
• Solid organ lesions (liver 10%, spleen 6%)
• Uterine rupture in pregnant women
Ruchholtz, et al. J
Trauma 2004;57:278
Kataoka, et al. J Trauma 2005;58:704

Lustenberger, et al. J Emerg
Trauma Shock 2011 (in press)
Characteristics
Early
Survivors
(n=34)
Non-
Survivors
(n=16)
All
(n=50)
Laparotomy 26 (77%) 14 (88%)34
(77%)
Cross-clamping
Aorta2 (6%) 8 (50%)
10
(20%)
Pelvic packing 23 (68%) 12 (75%)35
(70%)
Thoracotomy 0 7 (44%) 7 (14%)
Mortality4 (12%):
MOF 3,
head injury 1
16: hemorrhage
13, head injury
3
20
(40%)
Time to C-clamp (min)
39.5 2.2
Days till definitive pelvic stabilization
3.5 0.5
Age: 45 y
m:w=26:24
ISS: 42 pts.
12 years
Pelvic Clamp and Packing

AUC 95% CI p-value
BE at admission 0.856 0.751 – 0.961 <0.001
BE 1 h after admission 0.915 0.836 – 0.993 <0.001
Lactate at admission 0.784 0.651 – 0.917 0.001
Lactate 1 h after admission 0.825 0.705 – 0.944 <0.001
pH at admission 0.804 0.671 – 0.938 <0.001
pH 1 h after admission 0.905 0.819 – 0.992 <0.001
Pelvic Clamp and Packing
Abt, et al. Eur J Trauma Emerg Surg 2009
Fetomaternal Hemorrhage and isoimmunization
>0.01 mL of Rh-positive blood will sensitize 70% of Rh-negative patients, presence of fetomaternal hemorrhage in Rh-negative mother should warrant Rh immunoglobulin therapy within 72 hrs. unless the injury is remote from the uterus (isolated distal extremity injury)

> Multislice CT
> Retrograde
cystography
(intraop or preop)
> Explorative
laparotomy
2a. Reduction of Contamination (Diagnostics)
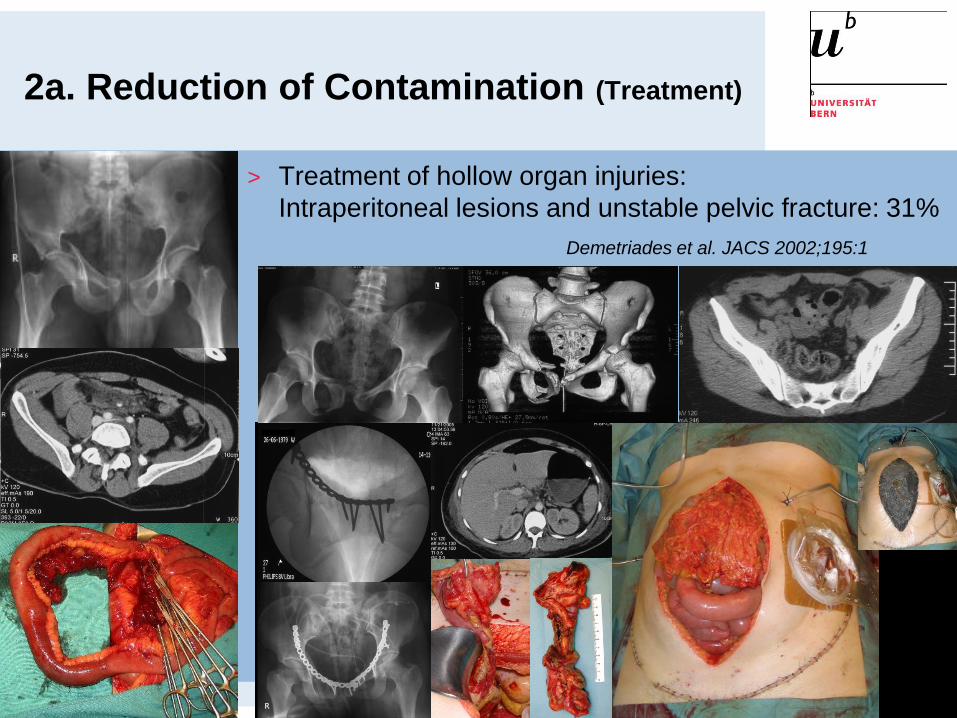
2a. Reduction of Contamination (Treatment)
> Treatment of hollow organ injuries:
Intraperitoneal lesions and unstable pelvic fracture: 31%
Demetriades et al. JACS 2002;195:1

2a. Reduction of Contamination (Treatment)

2b. Reduction of Contamination
> Débridement of open fractures
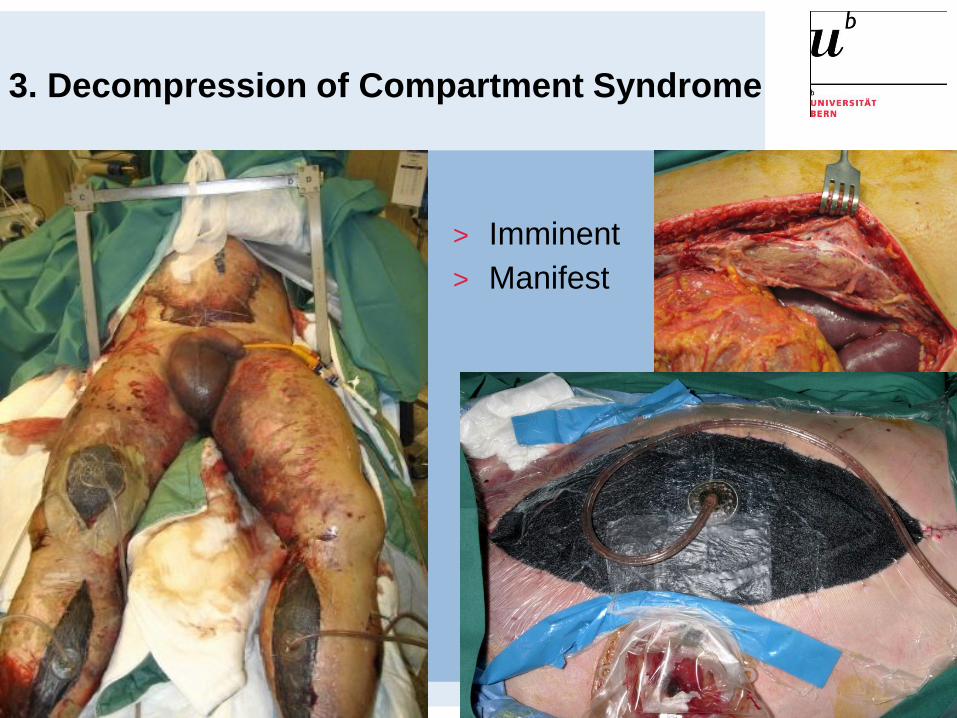
3. Decompression of Compartment Syndrome
> Imminent
> Manifest
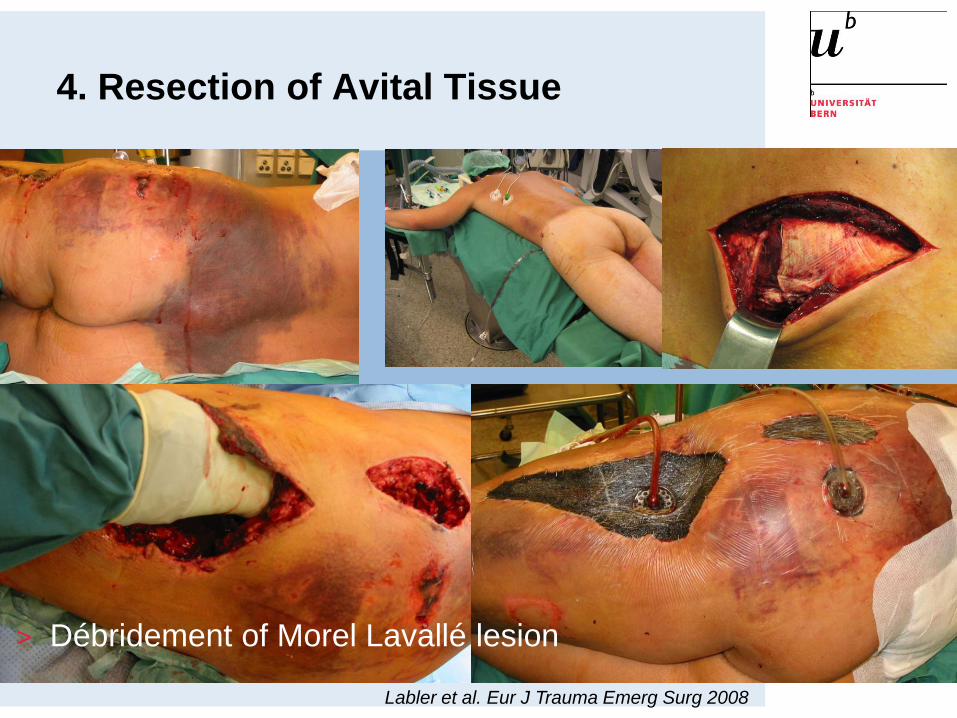
4. Resection of Avital Tissue
Labler et al. Eur J Trauma Emerg Surg 2008
> Débridement of Morel Lavallé lesion
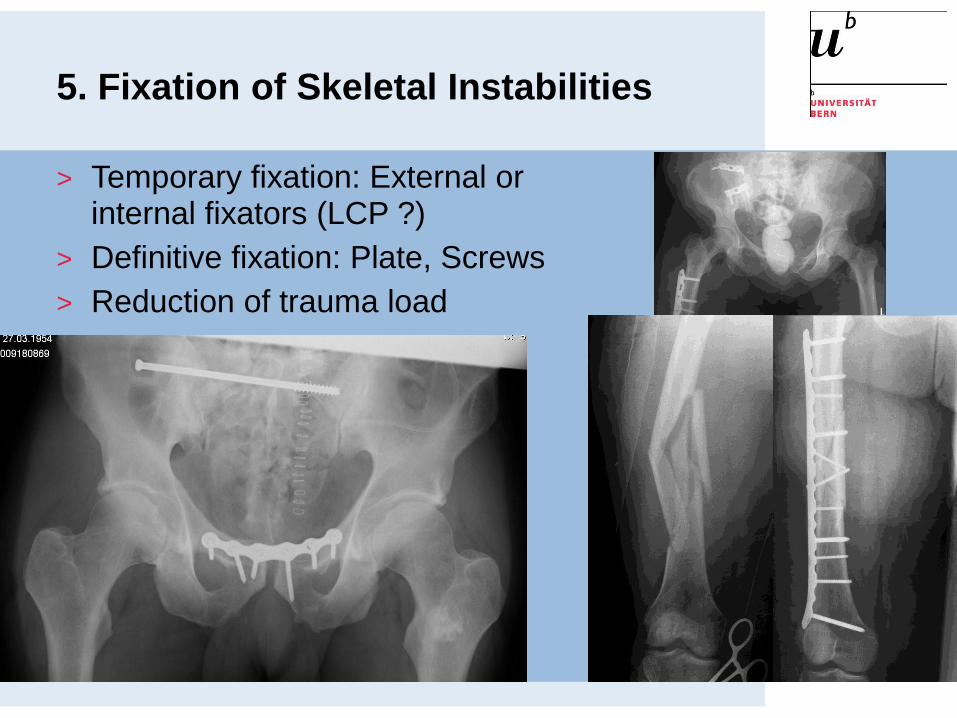
5. Fixation of Skeletal Instabilities
> Temporary fixation: External or internal fixators (LCP ?)
> Definitive fixation: Plate, Screws
> Reduction of trauma load

Case - Damage Control Surgery

-OP-time: 2:45
-Lactate: 2,1 mmol/L (initial: 3.2)
-Voluven 2200 mL; RL 8000 mL
-No RBC, FFP, Tc
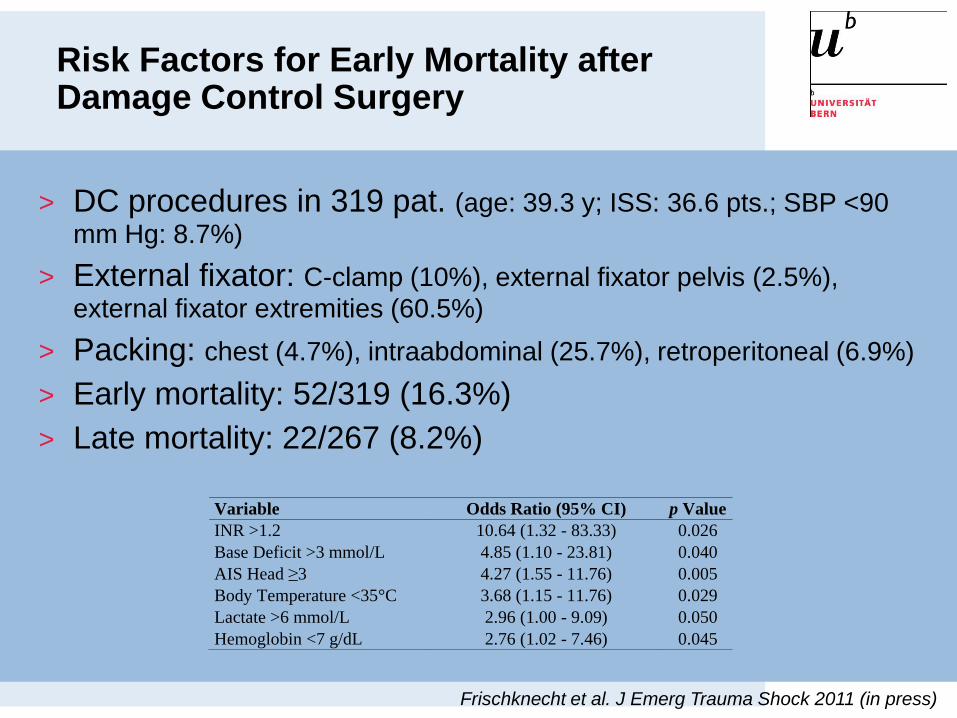
Risk Factors for Early Mortality after Damage Control Surgery
Variable Odds Ratio (95% CI) p Value
INR >1.2 10.64 (1.32 - 83.33) 0.026
Base Deficit >3 mmol/L 4.85 (1.10 - 23.81) 0.040
AIS Head ≥3 4.27 (1.55 - 11.76) 0.005
Body Temperature <35°C 3.68 (1.15 - 11.76) 0.029
Lactate >6 mmol/L 2.96 (1.00 - 9.09) 0.050
Hemoglobin <7 g/dL 2.76 (1.02 - 7.46) 0.045
Frischknecht et al. J Emerg Trauma Shock 2011 (in press)
> DC procedures in 319 pat. (age: 39.3 y; ISS: 36.6 pts.; SBP <90
mm Hg: 8.7%)
> External fixator: C-clamp (10%), external fixator pelvis (2.5%),
external fixator extremities (60.5%)
> Packing: chest (4.7%), intraabdominal (25.7%), retroperitoneal (6.9%)
> Early mortality: 52/319 (16.3%)
> Late mortality: 22/267 (8.2%)
Damage Control Resuscitation (DCR)
> Permissive hypotension (Cave head injury)
> Minimizing crystalloid-based resuscitation strategies
> Massive transfusion protocols (MTPs): predifined blood products
- PRBCs
- FFP
- platelets
> Adjuncts to massive transfusion:
- Pharmacological adjuncts:
- fibrinogen
- rfVIIa,…
- Auto-transfusion/cell saverNunez et Cotton. Curr Opin Crit Care 2009;15:536-41
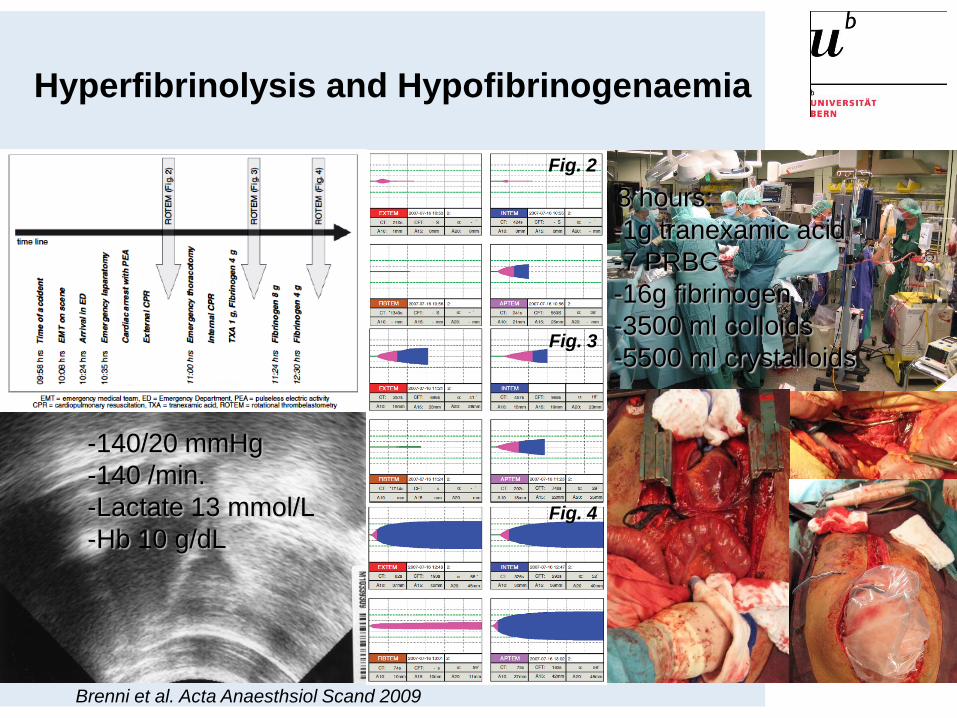
Hyperfibrinolysis and Hypofibrinogenaemia
Brenni et al. Acta Anaesthsiol Scand 2009
Fig. 2
Fig. 3
Fig. 4
-140/20 mmHg
-140 /min.
-Lactate 13 mmol/L
-Hb 10 g/dL
-1g tranexamic acid
-7 PRBC
-16g fibrinogen
-3500 ml colloids
-5500 ml crystalloids
3 hours:

rFVIIa (Novoseven®)
> Trial phase 2 (143 blunt trauma and
134 penetrating trauma, rFVIIa): In blunt
trauma significant reduction of RBC
after rFVIIa (trend in penetrating
injuries); no influence on mortality
Boffard et al. J Trauma 2005;59:8-15
CONTROLTM-„Clinical Trial on the Effect of rFVIIa
on Traumatic Blood Loss“: F7Trauma-1711-Study –multi-
center, randomized, double-blind, parallel group, placebo
controlled trial to evaluate the efficacy and safety of activated
recombinant factor VII (rFVIIa/NovoSeven®/ NiaStase®) in
severely injured trauma patients with bleeding refractory to
standard treatment. Trial Phase 3Global CONTROL Results Meeting
December 2008, Madrid
> Trial phase 3:
- 481 blunt trauma and 92 penetrating
trauma (576 randomized), rFVIIa (200
mcg/kg-1+3h 100mcg/kg)
- in blunt and penetrating trauma
significant reduction of RBC and
FFP after rFVIIa (1.3 U RBC and 2.7
U FFP)
- no influence on mortality or morbidity
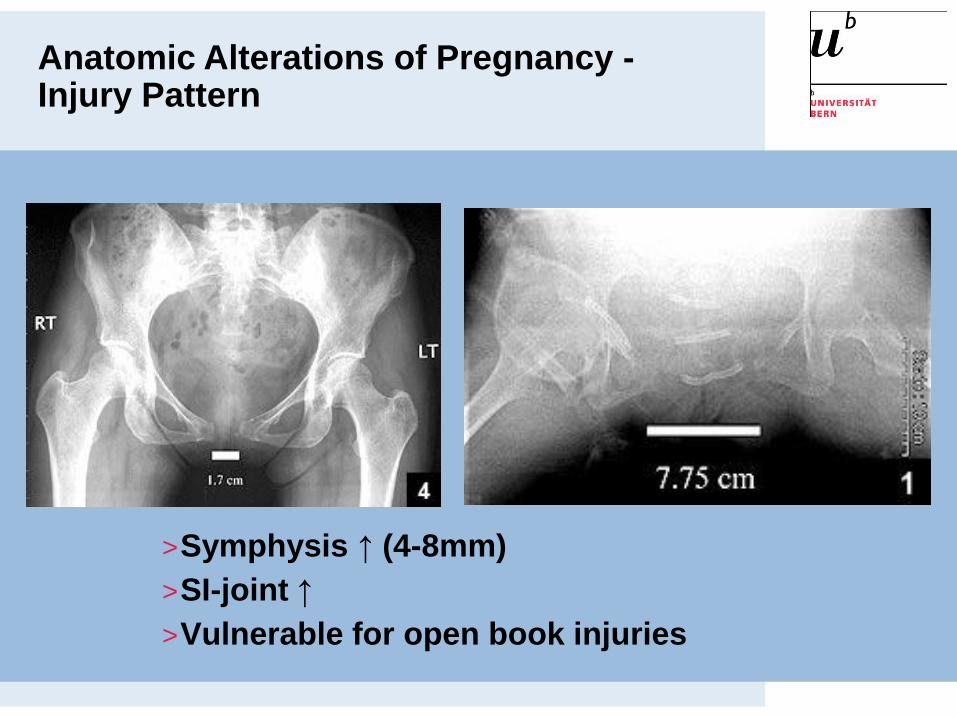
>Symphysis ↑ (4-8mm)
>SI-joint ↑
>Vulnerable for open book injuries
Anatomic Alterations of Pregnancy -Injury Pattern
> Retrospective 16 year period (1987-2002)
> 15 pregnant (1.1%) vs 1330 nonpregnant patients with pelvic or acetabular fractures: 1 mother died (6.7%)
> Conservative treatment n=11
> Operative treatment n=4
> 16 fetus: 12 survival, 4 died (25%)
Almog, et al. Am J Orthop 2007;36(11):E153-9
Pelvic Fractures During Pregnancy

23.7.2008
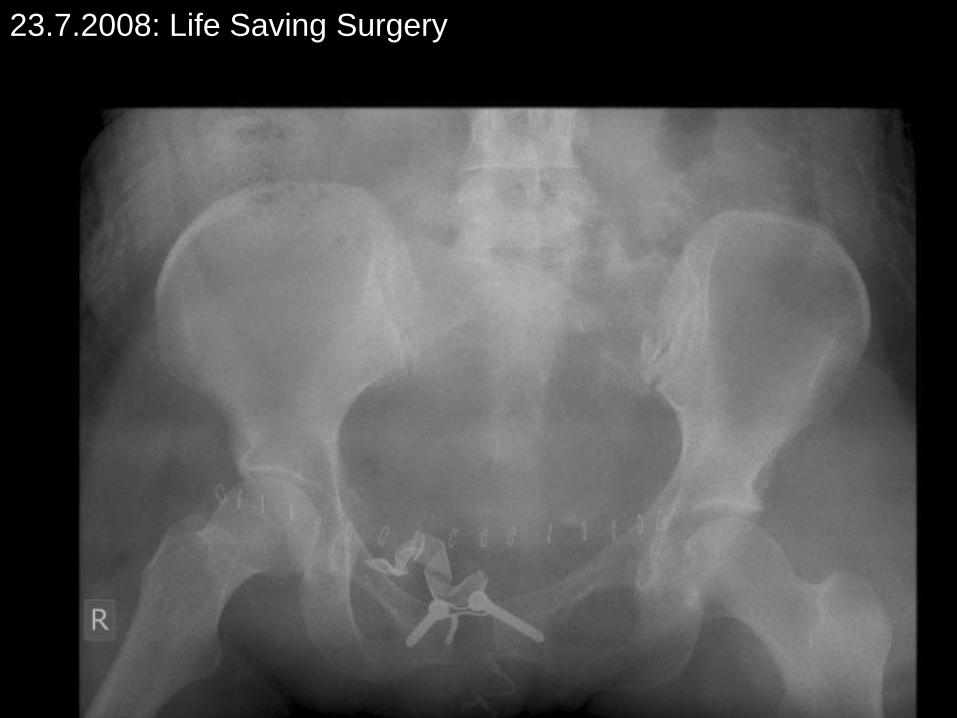
23.7.2008: Life Saving Surgery

24.7.2008: Damage Control Surgery
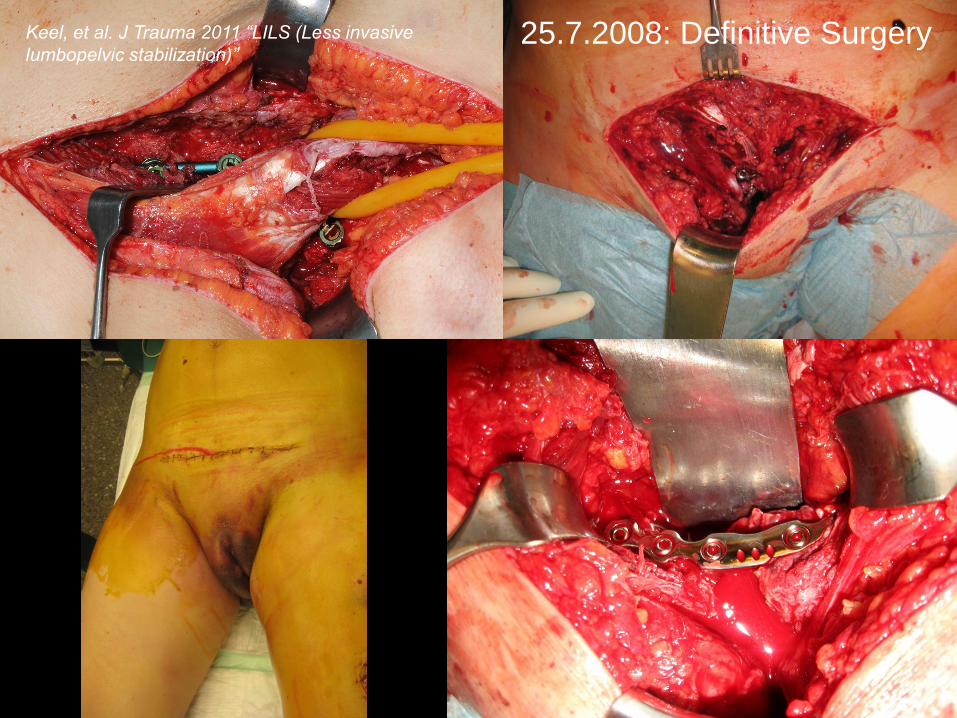
Keel, et al. J Trauma 2011 “LILS (Less invasive
lumbopelvic stabilization)”25.7.2008: Definitive Surgery
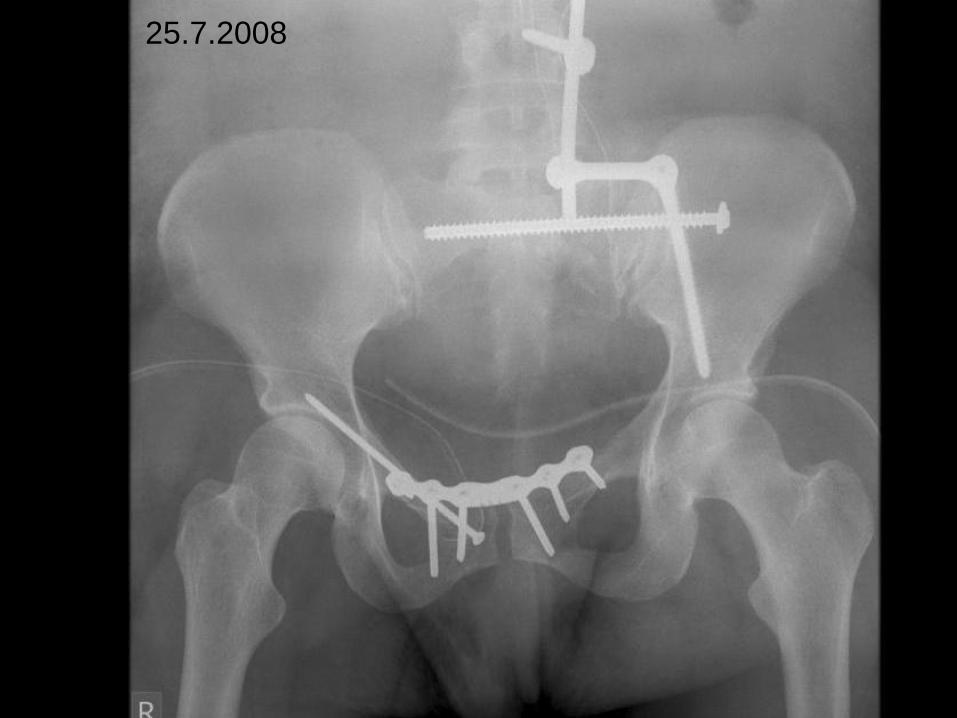
25.7.2008
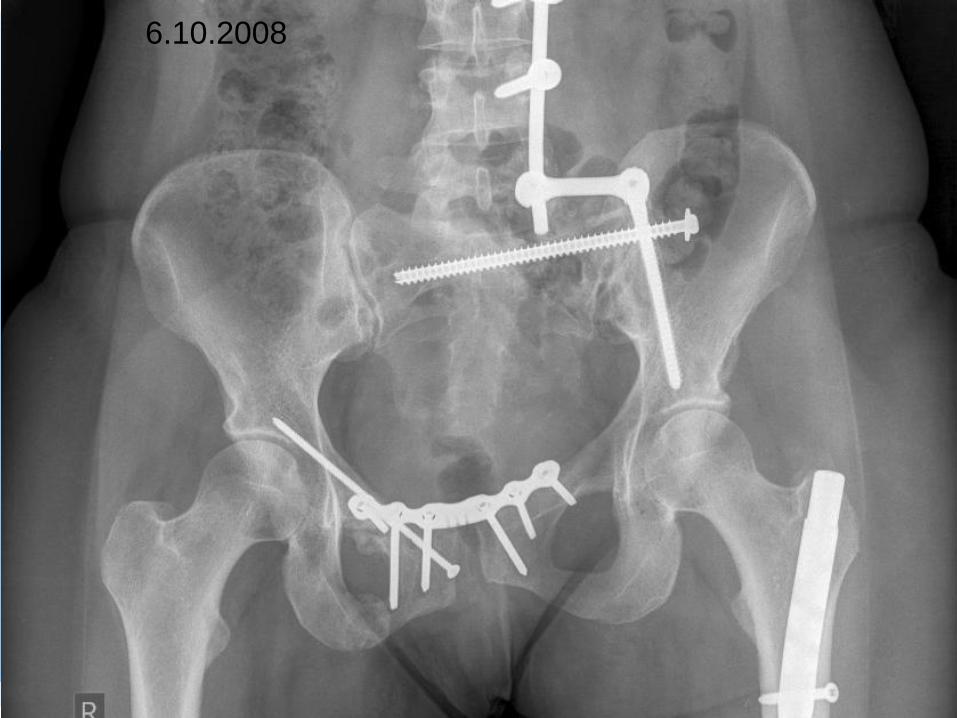
6.10.2008

> Retrospective 6 year period
> 8 pregnant (1.5%) vs 818 nonpregnant patients with acetabular fractures
> Gestational age 5-26 weeks
> Infant delivery 27 weeks from time of surgery with normal Apgar score
> 4 PW - 3 Transverse + PW - 1 PC (car accidents)
> Intraoperative fluoroscopy 39 seconds
> CT: calculated radiation exposure dose to fetus 5 cGy
> Conclusion: minimal risk to baby - acceptable articular reduction
Porter, et al. J Orthop Trauma 2008;22(8):508-16
Operative Fixation of Acetbular Fractures in Pregnant Patient - Acceptable Reduction ?



>Limited use of intra- and postoperative X-ray
>Qualified specialist with experience in acetabular surgery (joint visualization)
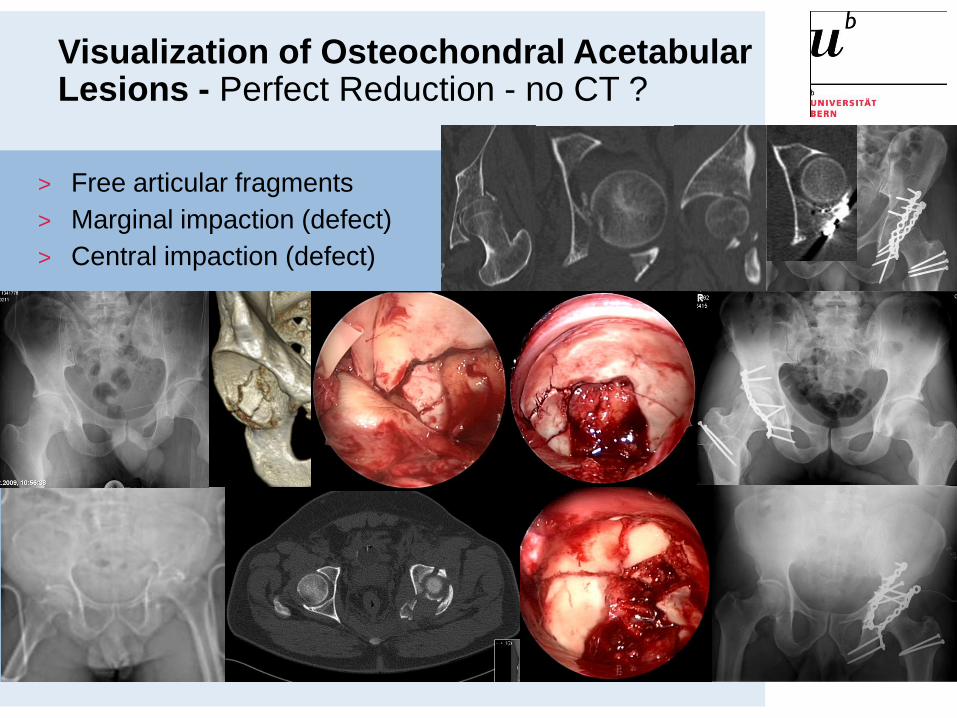
Visualization of Osteochondral Acetabular Lesions - Perfect Reduction - no CT ?
> Free articular fragments
> Marginal impaction (defect)
> Central impaction (defect)

Pregnancy Outcomes after Orthopaedic Trauma ?
Cannada, et al. J Trauma 2010;69:694.
> Observational study 1995-2007 (12 years) - delivery at trauma
center during or after trauma admission
> 65 pregnant women with (6%) vs 990 without orthopeadic
trauma - surgical treatment for orthopaedic trauma 49%
> Gestational age 28 weeks (vs 31 weeks)
> Increased risk of preterm birth before 37 weeks (31% vs 3%)
> Increased Cesarean delivery (40% vs 25%)
> Increased risk of placental abruption (8% vs 1%), esp. pelvic
fractures (30%)
> Increased risk of perinatal mortality (fetal or neonatal death; 8%
vs 1%), esp. pelvic fractures (30%)
> Conclusion: Referral to medical center capable of handling both
primary injury and potential preterm birth
Pregnancy Outcomes after Orthopaedic Trauma ?
Pregnancy Outcomes after Orthopaedic Trauma ?
Rozycki. Editorial Comment. J Trauma 2010;69:698.
> Maternal shock
> Acidosis - hypoxia - hypothermia
> Medications
> Diagnostic radiation ?
> Surgery (opertive length, blood loss) ?
> Anesthesia (pre- or intraoperative hypotension, acidosis,
episodes of hypothermia; type of anesthetic) ?

Trauma-Management of Pregnant Patient
Cannada, et al. J Trauma 2010;69:694.
> Stage 4: Second Look„s and Schedulded Definitive Surgery
> Stage 5: Secondary Reconstructive Surgery
Damage Control Stages
> Stage 1: Indications
> Stage 2: Damage Control Surgery
> Stage 3: Resuscitation in ICU
Experience
Tactics
Dynamic
FlexibilityWindow of Opportunity
Days 4-10
Prevent Maternal and Fetal Death !
> Life Saving Surgery:
– Operative control of airway
– Decompression of cavities
– Surgical control of hemorrhage
– Team
– Tactic
- Time> Fast decision
making for Life
Saving Surgery,
DCS/DCO,
cesarean section
– Bleeding control
– Reduction of contamination
– Decompression of compartment syndrome
– Resection of avital tissue
– Fixation of skeletal instabilities
> Damage Control Concept
> Anticipate physiologic and anatomic alterations during pregnancy
> Fetal monitoring
> Cesarean Section
Related Documents











