Polyomavirus nephropathy: updated Helmut Hopfer, Basel, Switzerland

Polyomavirus nephropathy: updated Helmut Hopfer, Basel, Switzerland.
Jan 02, 2016
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Polyomavirus nephropathy: updated
Helmut Hopfer, Basel, Switzerland
Agenda
• SV40 immunohistochemistry and BK viremia• PVN treatment: implications for morphology• PVN and rejection
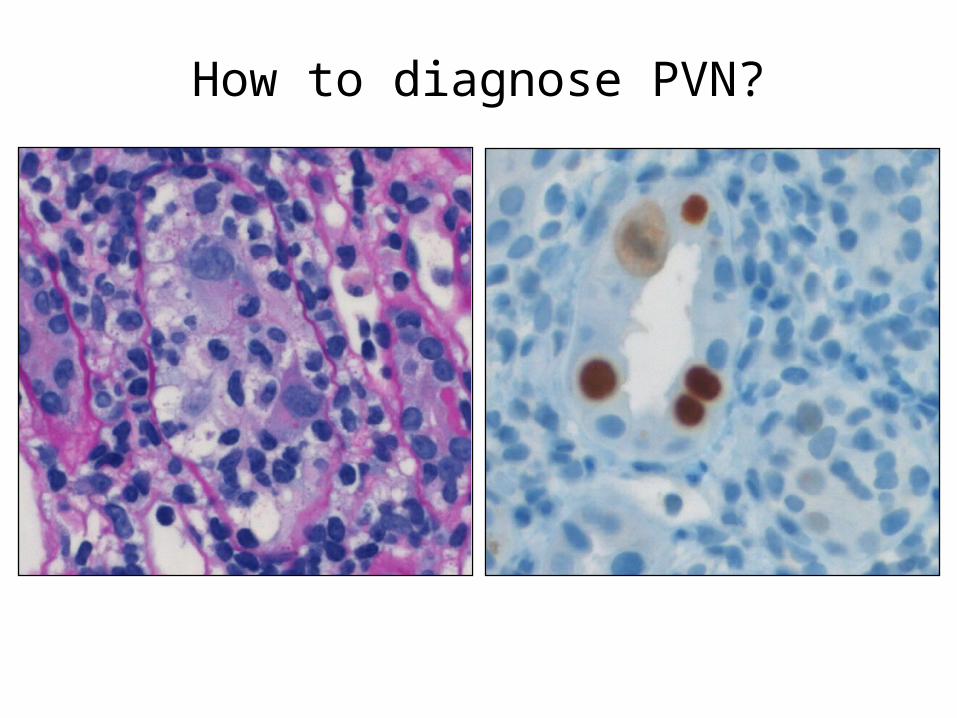
How to diagnose PVN?

BK-BIFQUIT: trial design
inter-observer variability
SV40 IHC
participants scoreintensity and extent
inter-laboratory variability
SV40 IHC
organizers scoreintensity and extent
SV40 IHC
SV40 IHC
SV40 IHC
SV40 IHC
SV40 IHC
SV40 IHC
participantsSV 40 IHC
SV40 IHC: inter-observer variability
Substantial agreement (staining intensity and extent of infection)
unpublished data, M. Mengel, Edmonton
SV40 IHC: inter-laboratory variability
Below chance (staining intensity and extent of infection)Substantial agreement (positive vs. negative cores)
unpublished data, M. Mengel, Edmonton
BK-BIFQUIT: summary
• BK "best practice": automated stainer, heat induced epitope retrieval (>30 minutes), either citrate or EDTA buffer, monoclonal antibody (PAB416) <1:100 for 25-35 minutes, polymer detection system
• Scoring of staining intensity and percentage tubules infected is not reproducible
Binary categorization of cases as positive/ negative gives acceptable inter-laboratory and inter-observer reproducibility

SV40 IHC and BK viremia
• Number of tubules with SV40+ cells per mm biopsy length significantly correlates with number of BK copies in the blood
• High number of SV40 negative biopsies: <10'000 copies/ml ~90% of cases, >10'000 copies/ml ~
unpublished data, H. Hopfer, Basel
Summary 1
• High sampling error< 10’000 c/ml: ~90% negative≥ 10’000 c/ml: ~40% negative• YES / NO scoring of SV40 immunohistochemistry
Agenda
• SV40 immunohistochemistry and BK viremia• PVN treatment: implications for morphology• PVN and rejection
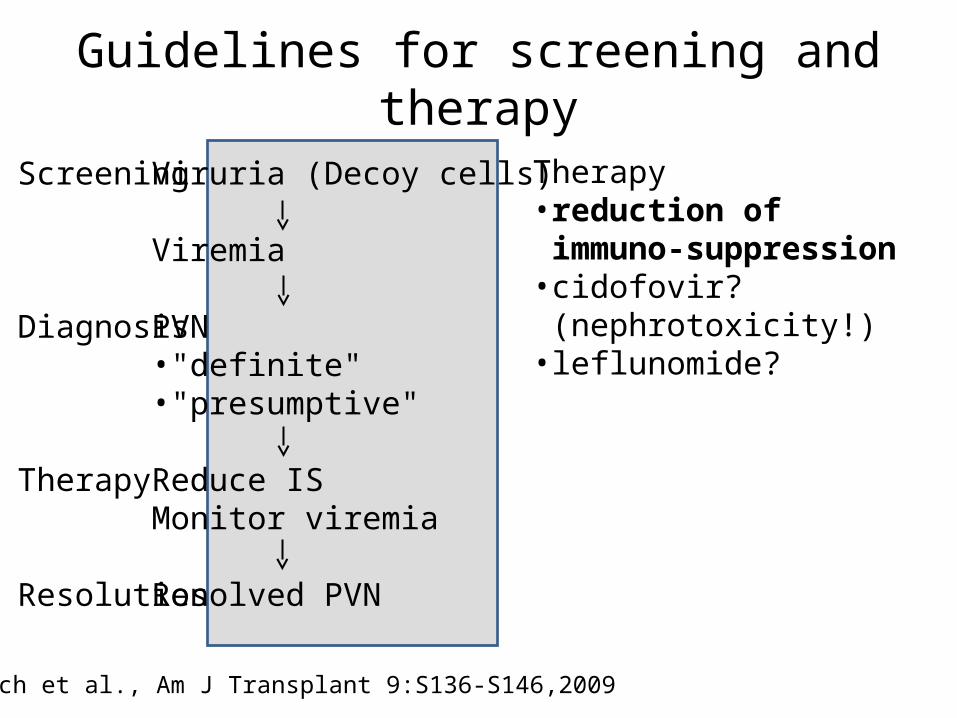
Therapy• reduction of immuno-
suppression• cidofovir? (nephrotoxicity!)• leflunomide?
Guidelines for screening and therapy
Hirsch et al., Am J Transplant 9:S136-S146,2009
Viruria (Decoy cells)
Viremia
PVN•"definite"•"presumptive"
Reduce ISMonitor viremia
Resolved PVN
Screening
Diagnosis
Therapy
Resolution

Blood
↓ ↓ ↑
time after transplantation
BK-specific cellular immunity
vire
mia
(c/m
l)
viru
ria (c/
ml)
adapted from Comoli et al., Curr Opin Organ Transplant 13:569-574, 2009
BK-specifi
c im
munity
IFNg S
FU/1
05 PBMC
Immunosuppression
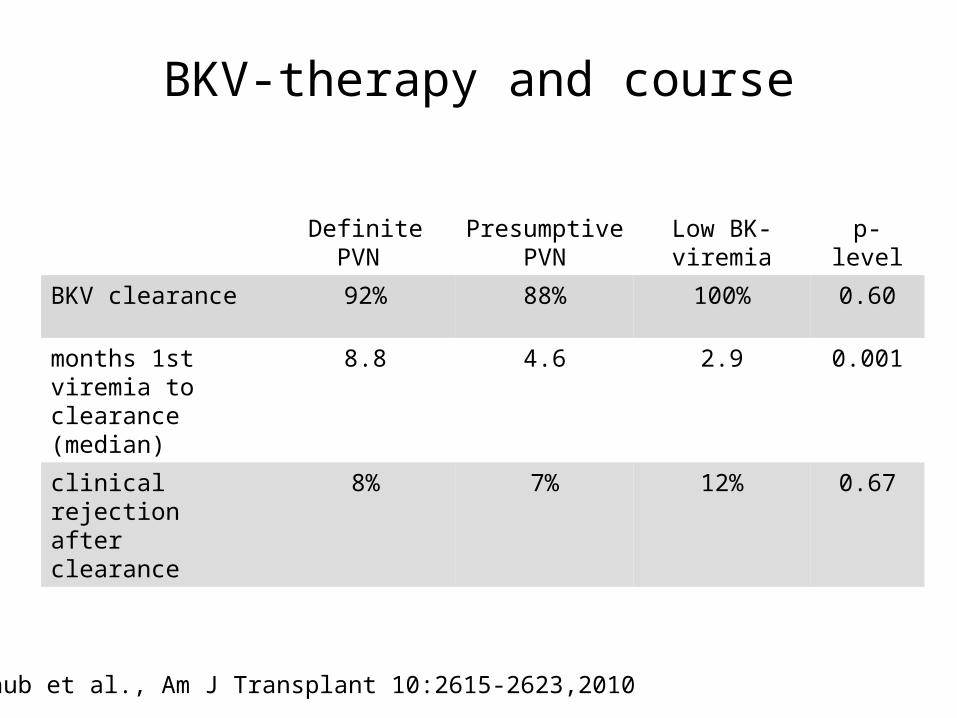
BKV-therapy and course
Definite PVN Presumptive PVN
Low BK-viremia p-level
BKV clearance 92% 88% 100% 0.60
months 1st viremia to clearance (median)
8.8 4.6 2.9 0.001
clinical rejection after clearance
8% 7% 12% 0.67
Schaub et al., Am J Transplant 10:2615-2623,2010
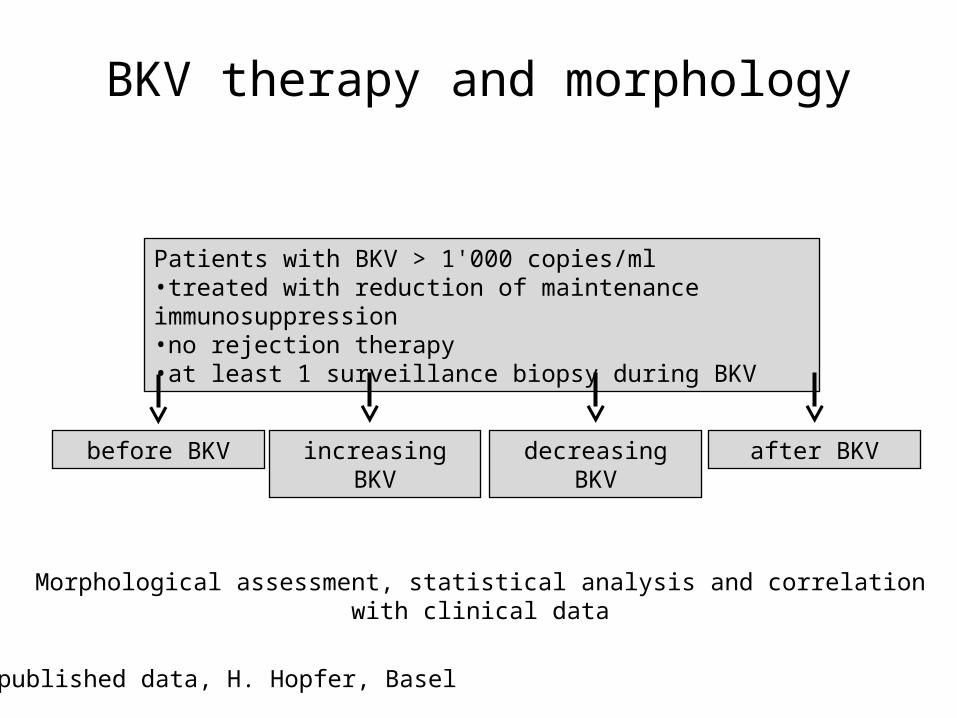
BKV therapy and morphology
decreasing BKVincreasing BKVbefore BKV after BKV
Patients with BKV > 1'000 copies/ml•treated with reduction of maintenance immunosuppression•no rejection therapy•at least 1 surveillance biopsy during BKV
Morphological assessment, statistical analysis and correlation with clinical data
unpublished data, H. Hopfer, Basel
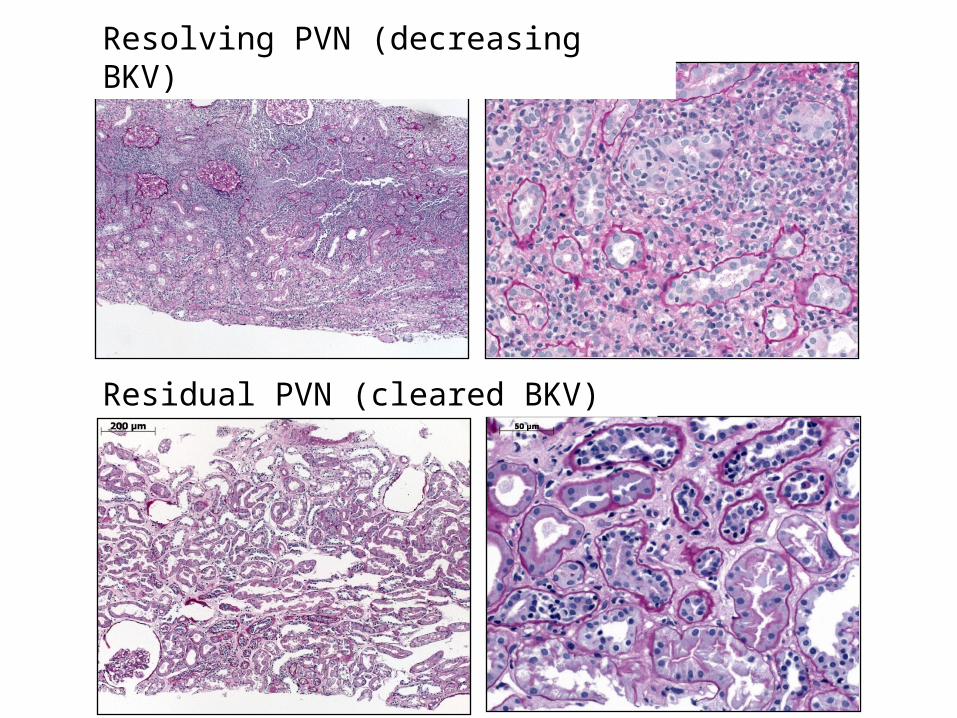
Resolving PVN (decreasing BKV)
Residual PVN (cleared BKV)
"Tubulitis " and inflammation
• During decreasing viremia there was a significant increase in the Banff tubulitis score (t) as well as the extent of interstitial inflammatory infiltrate.
• Persistence of intraepithelial lymphocytes and interstitial inflammation after viral clearance.
unpublished data, H. Hopfer, Basel

Creatinine course
• Serum creatinine values overall remained stable (baseline - 1st replication - peak replication - clearance - last follow up)
• Increase of serum creatinine ≥40 umol/l during decreasing viremia in ~40% of patients, which returned to baseline without additional treatment
unpublished data, H. Hopfer, Basel
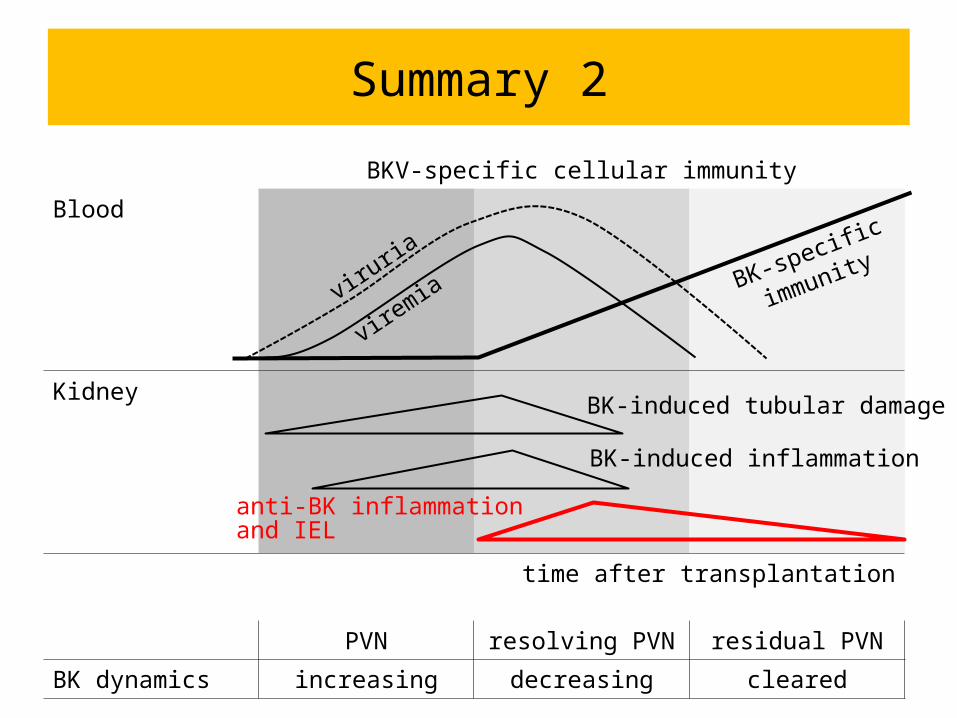
Summary 2
BKV-specific cellular immunity
Blood
Kidney
time after transplantation
PVN resolving PVN residual PVN
BK dynamics increasing decreasing cleared
viruria
viremiaBK-specific
immunity
BK-induced tubular damage
BK-induced inflammation
anti-BK inflammationand IEL
PVN and rejection – a matter of faith?
• Do you believe in PVN and rejection?• Can you distinguish PVN from rejection?• How do you treat PVN and rejection?

BK-specific, rejection or "innocent"?
• BK-specific lymphocyte? (anti-BK immune response)
• HLA-specific lymphocyte? (rejection?)
• "innocent" lymphocyte? (unspecific infiltrate)
Distinction PVN and ICR?
• SV40 immunohistochemistry?• Severity and extent of tubulitis and inflammation?• Cellular composition of infiltrate?
How to treat PVN and rejection?
• Individualize decisions in patients with concurrent vascular or humoral rejections
• PVN is more important than ICR

Take-home messages
• PVN is focal, high number of falsly negative cases• Resolving PVN is an anti-viral acute interstitial nephritis• Give BK-specific immunity a chance• Clinicopathological correlation is key to the correct diagnosis
(clinical history, viral dynamics, creatinine course, morphologi-cal findings)
Related Documents











