Clinical Investigations Polymorphisms of Matrix Metalloproteinases in Systolic Heart Failure: Role on Disease Susceptibility, Phenotypic Characteristics, and Prognosis F ABIO M. VELHO, MD, * ,1 CAROLINA R. COHEN, BSc,* ,1 K ATIA G. SANTOS, PhD, 1,2 DAIANE SILVELLO, BSc, 1 NIDIANE MARTINELLI, BSc, 1 ANDR EIA BIOLO, MD, ScD, 1 NADINE CLAUSELL, MD, PhD, 1 AND LUIS E. ROHDE, MD 1 Porto Alegre, Brazil ABSTRACT Background: The role of matrix metalloproteinases (MMPs) polymorphisms on heart failure (HF) susceptibility, phenotypic characteristics, and prognosis has been poorly explored. Methods and Results: We studied 313 HF patients with left ventricular systolic dysfunction and 367 healthy control subjects. Genotyping of MMP-1 (1607 1G/2G), MMP-3 (1171 5A/6A), and MMP-9 (1562 C/T) polymorphisms was performed by polymerase chain reaction. Allelic and genotypic frequen- cies of MMP-1, -3, and -9 were similar in HF patients and controls. MMP1 2G allele carriers were pos- itively associated to ischemic etiology and history of myocardial infarction (all P values !.05). Patients were followed-up for a median of 40 months and 58 HF-related deaths occurred during this period. HF-related survival was significantly better in MMP1 2G allele carriers (71% versus 42% for 1G/1G patients, P 5 .002) and in MMP-3 6A allele carriers (70% versus 61% for 5A/5A patients, P 5 .064), particularly in non-ischemic patients (P 5 .039). MMP1 2G allele was independently associated to HF survival after adjustment for several other predictors of risk (hazard ratio 0.47, 95% confidence interval 0.27 to 0.82; P 5 .008). Conclusions: MMP-1, -3, and -9 polymorphisms were not associated to HF susceptibility. However, MMP1 2G allele carriers were related to a higher prevalence of ischemic etiology among patients with systolic HF and better HF-related prognosis. (J Cardiac Fail 2011;17:115e121) Key Words: Heart failure, metalloproteinases, polymorphism. Heart failure (HF) represents the end-stage of several heart diseases and remains a major cause of morbidity and mortality worldwide. 1 Experimental and clinical stud- ies have demonstrated that left ventricular (LV) remodeling and dilation occur along with LV failure progression, cul- minating with end-stage and refractory HF. 2 Restructuring of the collagen matrix plays a central role in the adaptations of the failing myocardium and the ultimate transition to car- diac decompensation. 3 Matrix metalloproteinases (MMPs), an endogenous family of zinc-dependent enzymes, have been identified as key players in this process. Collagenases (MMP-1), gelatinases (MMP-2 and MMP-9), and stromely- sins (MMP-3) have all been linked to matrix remodeling in the different stages of HF progression. 4e6 Genetic polymorphisms of MMPs substantially influence the overall gene transcriptional efficiency, resulting in het- erogeneous gene expression. 7,8 A common variant in the promoter region of the MMP-1 gene with 1 (1G) or 2 (2G) guanine nucleotides has been described at position-1607 relative to the transcriptional start site of the gene. 9 It has been shown that the 2G allelic promoter of the MMP-1 gene has a 20-fold higher transcriptional ac- tivity than the 1G allelic promoter. The 2G allele was From the 1 Heart Failure and Cardiac Transplant Unit,Cardiology Divi- sion at Hospital de Cl ınicas de Porto Alegre, and the Post-Graduate Pro- gram in Cardiology and Cardiovascular Science, Medical School of the Federal University of Rio Grande do Sul, Porto Alegre, Brazil and 2 Re- search Center, Medical Sciences, Luteran University of Brazil, Canoas, Brazil. Manuscript received April 19, 2010; revised manuscript received September 18, 2010; revised manuscript accepted September 30, 2010. Reprint requests: Luis E. Rohde, MD, Heart Failure and Transplant Unit, Cardiology Division, Hospital de Cl ınicas de Porto Alegre, Rua Ramiro Barcelos 2350, Sala 2061, Porto Alegre, RS, Brazil 90035-003. Tel/Fax: 55 51 33598344. E-mail: [email protected] See page 121 for disclosure information. * These authors contributed equally to this manuscript. 1071-9164/$ - see front matter Ó 2011 Elsevier Inc. All rights reserved. doi:10.1016/j.cardfail.2010.09.017 115 Journal of Cardiac Failure Vol. 17 No. 2 2011

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Journal of Cardiac Failure Vol. 17 No. 2 2011
Clinical Investigations
Polymorphisms of Matrix Metalloproteinases in Systolic HeartFailure: Role on Disease Susceptibility, Phenotypic
Characteristics, and Prognosis
F�ABIO M. VELHO, MD,*,1 CAROLINA R. COHEN, BSc,*,1 K�ATIA G. SANTOS, PhD,1,2 DAIANE SILVELLO, BSc,1
NIDIANE MARTINELLI, BSc,1 ANDR�EIA BIOLO, MD, ScD,1 NADINE CLAUSELL, MD, PhD,1 AND LUIS E. ROHDE, MD1
Porto Alegre, Brazil
From the 1Hearsion at Hospital dgram in CardioloFederal Universitsearch Center, MBrazil.Manuscript rec
September 18, 20Reprint requests
Cardiology DivisiBarcelos 2350, Sa55 51 33598344.See page 121 fo* These author1071-9164/$ - s� 2011 Elseviedoi:10.1016/j.ca
ABSTRACT
Background: The role of matrix metalloproteinases (MMPs) polymorphisms on heart failure (HF)susceptibility, phenotypic characteristics, and prognosis has been poorly explored.Methods and Results: We studied 313 HF patients with left ventricular systolic dysfunction and 367healthy control subjects. Genotyping of MMP-1 (�1607 1G/2G), MMP-3 (�1171 5A/6A), and MMP-9(�1562 C/T) polymorphisms was performed by polymerase chain reaction. Allelic and genotypic frequen-cies of MMP-1, -3, and -9 were similar in HF patients and controls. MMP1 2G allele carriers were pos-itively associated to ischemic etiology and history of myocardial infarction (all P values !.05). Patientswere followed-up for a median of 40 months and 58 HF-related deaths occurred during this period.HF-related survival was significantly better in MMP1 2G allele carriers (71% versus 42% for 1G/1Gpatients, P 5 .002) and in MMP-3 6A allele carriers (70% versus 61% for 5A/5A patients, P 5 .064),particularly in non-ischemic patients (P 5 .039). MMP1 2G allele was independently associated to HFsurvival after adjustment for several other predictors of risk (hazard ratio 0.47, 95% confidence interval0.27 to 0.82; P 5 .008).Conclusions: MMP-1, -3, and -9 polymorphisms were not associated to HF susceptibility. However,MMP1 2G allele carriers were related to a higher prevalence of ischemic etiology among patients withsystolic HF and better HF-related prognosis. (J Cardiac Fail 2011;17:115e121)Key Words: Heart failure, metalloproteinases, polymorphism.
Heart failure (HF) represents the end-stage of severalheart diseases and remains a major cause of morbidityand mortality worldwide.1 Experimental and clinical stud-ies have demonstrated that left ventricular (LV) remodeling
t Failure and Cardiac Transplant Unit, Cardiology Divi-e Cl�ınicas de Porto Alegre, and the Post-Graduate Pro-gy and Cardiovascular Science, Medical School of they of Rio Grande do Sul, Porto Alegre, Brazil and 2Re-edical Sciences, Luteran University of Brazil, Canoas,
eived April 19, 2010; revised manuscript received10; revised manuscript accepted September 30, 2010.: Luis E. Rohde, MD, Heart Failure and Transplant Unit,on, Hospital de Cl�ınicas de Porto Alegre, Rua Ramirola 2061, Porto Alegre, RS, Brazil 90035-003. Tel/Fax:E-mail: [email protected] disclosure information.s contributed equally to this manuscript.ee front matterr Inc. All rights reserved.rdfail.2010.09.017
115
and dilation occur along with LV failure progression, cul-minating with end-stage and refractory HF.2 Restructuringof the collagen matrix plays a central role in the adaptationsof the failing myocardium and the ultimate transition to car-diac decompensation.3 Matrix metalloproteinases (MMPs),an endogenous family of zinc-dependent enzymes, havebeen identified as key players in this process. Collagenases(MMP-1), gelatinases (MMP-2 and MMP-9), and stromely-sins (MMP-3) have all been linked to matrix remodeling inthe different stages of HF progression.4e6
Genetic polymorphisms of MMPs substantially influencethe overall gene transcriptional efficiency, resulting in het-erogeneous gene expression.7,8 A common variant in thepromoter region of the MMP-1 gene with 1 (1G) or2 (2G) guanine nucleotides has been described atposition-1607 relative to the transcriptional start site ofthe gene.9 It has been shown that the 2G allelic promoterof the MMP-1 gene has a 20-fold higher transcriptional ac-tivity than the 1G allelic promoter. The 2G allele was

116 Journal of Cardiac Failure Vol. 17 No. 2 February 2011
associated to increased risk of coronary heart disease(CHD)10, increased risk of carotid artery stenosis,11 and en-hanced LV remodeling after an acute myocardial infarction(AMI).12 A common polymorphism at the -1171 position inthe promoter region of MMP-3 (1 allele having a run of6 adenines [6A] and another allele having 5 adenines[5A]) has also been described.9 Transfection assays haveshown that the MMP-3 gene promoter containing the 5A al-lele has 2- to 4-fold higher transcriptional activity than pro-moter constructs containing the 6A allele.7 Initial studieshave suggested that the 5A allele is associated to the riskof idiopathic dilated cardiomyopathy13 and might have animpact on HF prognosis.14 Finally, the T allele of theMMP-9 polymorphism at position -1562 (a transition C toT) has also been associated to increased promoter activityand to the extent of coronary artery disease.15
In the present study, we hypothesized that geneticallymediated variability of MMPs are related to disease suscep-tibility, phenotypic characteristics and prognosis in Brazil-ian HF patients. We evaluated these hypotheses byanalyzing the above mentioned polymorphisms in a cohortof HF outpatients with moderate to severe LV systolic dys-function.
Methods
Patients
We included a total of 313 consecutive patients, older than18 years, with HF and LV systolic dysfunction (ejection fractionlower than 45%). Patients with other serious illnesses or with re-duced life-expectancy were excluded. Patients were recruited con-secutively between July 2003 and November 2007 from the heartfailure and transplant outpatient clinic in a tertiary care universityhospital in Porto Alegre, Brazil. Patients underwent clinical andlaboratory evaluation consisting of a standardized questionnaire,physical examination, evaluation of echocardiographic parametersand laboratory tests. Ischemic etiology was defined as a previoushistory of an acute myocardial infarction associated to the ex-pected alterations on surface electrocardiogram, echocardiogra-phy, or nuclear medicine scans. Coronary angiography was nota requirement to define ischemic etiology, but the majority of pa-tients (O85%) had an invasive evaluation demonstrating the ex-pected coronary lesions. Patients without a clear clinical historyof myocardial infarction could also be defined as ischemic, if elec-trocardiogram, echocardiographic/nuclear medicine, and invasivecoronary angiography were consistent with a silent myocardial in-farction, particularly in the diabetic patient.HF patients were followed in the outpatient clinic at our institu-
tion and vital status was evaluated at hospital electronic records,by telephone contact, and at a local death certificate database.The outcome of interest was HF-related death, defined as suddenunexpected death (within 1 hour of initiation of symptoms) orcaused by advanced refractory disease. All-cause mortality wasalso registered.We also evaluated 367 apparently healthy blood donors from
the hemotherapy center of the same hospital. Before blood dona-tion, volunteers that accepted to participate in the protocol under-went a systematic interview to evaluate personal or family historyof premature sudden death or cardiovascular diseases, the
presence of atherosclerotic risk factors, or any overt clinical dis-ease. No additional laboratory data were collected from blood do-nors. The study protocol was approved by the local institutionalreview board and by the National Agency of Ethics in Researchand conforms to the principles outlined in the Declaration of Hel-sinki. All subjects provided written informed consent before en-rollment.
Genotyping
Genomic DNAwas extracted from peripheral blood according toa nonenzymatic method previously described.16 The polymerasechain reaction method was used to amplify fragments containingthe MMP-1 1G/2G, MMP-3 5A/6A, and MMP-9 C/T polymor-phisms, using primers and conditions as described by Dunleaveyet al8,17 and Zhang et al,18 respectively. The polymerase chain reac-tion productswere then subjected to digestion by restriction endonu-cleaseXmnI orPaeI following themanufacturer’s instructions (MBIFermentas, St Leon-Rot, Germany). The digested fragments wereseparated by electrophoresis in a 8% polyacrylamide gel and visual-ized with silver nitrate staining (MMP-1 and MMP-3 polymor-phisms) or a 2% agarose gel and visualized with ethidiumbromide under ultraviolet light (MMP-9 polymorphism).
Statistical Analysis
Data are presented as mean 6 standard deviation or absolutenumbers and percentages. Continuous variables were comparedby the Student t-test or Mann-Whitney U test, and categorical vari-ables by the chi-square test or Fisher Exact test, as appropriate. Chi-square was also used to test the Hardy-Weinberg equilibrium and tocompare the allele and genotype frequencies between cases and con-trol subjects. Haplotype frequencies were estimated by a Bayesianmethod using PHASE, version 2.1.19,20 The linkage disequilibriumbetween MMP-1 and -3 genetic polymorphisms was calculated andexpressed in terms of D0 and r.2,21 Multivariate logistic regressionanalysis was used to assess the independent role ofMMP-1 as a pre-dictor of ischemic etiology, as in univariate analysis therewas a clearassociation between MMP-1 polymorphism and several ischemiccharacteristics. For this analysis, the model was adjusted for age,gender, diabetes, blood pressure, hypercholesterolemia, serum cre-atinine, and ethnicity. For the prognostic analysis, Kaplan-Meiersurvival curves were constructed from the date of entry at the outpa-tient clinic up to the last registry of follow-up or death, and com-pared by the log-rank statistics. Then, Cox proportional hazardmodels were created and adjusted for variables that might influenceHF-related mortality. For this analysis, models were adjusted forfunctional class, gender, ethnicity, systolic blood pressure, LV di-mensions, serum levels of creatinine and sodium. All data were an-alyzed using SPSS for Windows 16.0 or SAS 9.0 for Windows.A P value of!.05 was considered statistically significant.
Results
Patients and Controls
HF patients enrolled in this study were predominantlymales (69%) and Caucasian (70%), with a mean age of60 6 13 years, moderate to severe LV dysfunction and inNew York Heart Association (NYHA) Class I or II(76%). The etiology of HF was ischemic in 118 (38%) pa-tients and idiopathic in 91 (29%) patients. The majority ofpatients used angiotensin-converting enzyme (ACE)
istics
ofHFPatients
Accordingto
MMP-1,-3,and-9
GenePolymorphisms
MMP-3
MMP-9
carriers
5244
PValue
6A6A
n5
109
5A
carriers
n5
197
PValue
CC
n5
250
Tcarriers
n5
57
PValue
596
12
.18
616
12
596
13
.27
606
13
596
13
.36
165(68)
.05
72(66)
144(73)
.009
174(70)
43(75)
.48
101(41)
.014
44(40)
69(35)
.35
91(36)
23(40)
.68
61(25)
.002
25(23)
64(32)
.08
76(30)
14(25)
.47
57(23)
.97
30(27)
43(22)
.26
60(24)
12(21)
.76
186(78)
O.99
86(81)
148(76)
.90
190(78)
44(79)
.99
88(36)
.008
36(33)
61(31)
.71
76(30)
22(39)
.30
256
33
.001
1226
32
1316
35
.041
1316
35
1186
29
.011
.56
1.1
.23
5.4
61.1
5.7
61.0
.04
6.6
60.9
6.6
61.2
.51
326
8.17
316
8316
8.79
316
8326
9.43
88(38)
.006
39(37)
58(31)
.26
77(32)
20(36)
.70
inase;
NYHA,New
York
HeartAssociation.
percentages).
MMP Polymorphisms and Heart Failure � Velho et al 117
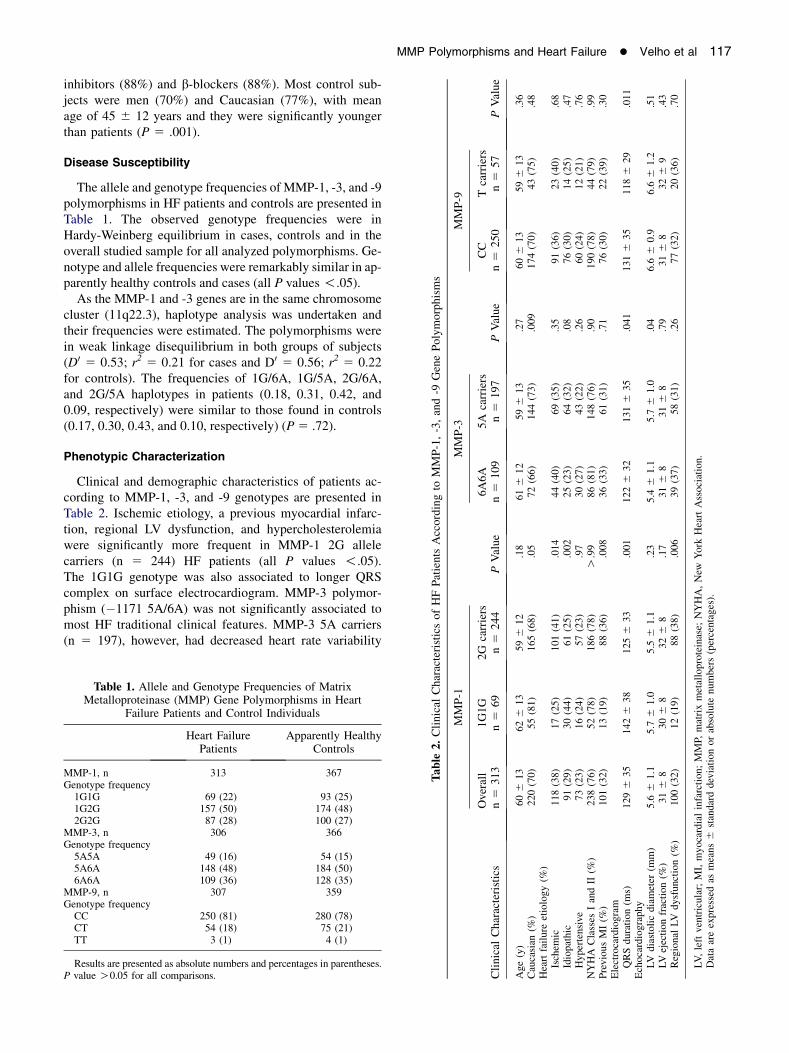
inhibitors (88%) and b-blockers (88%). Most control sub-jects were men (70%) and Caucasian (77%), with meanage of 45 6 12 years and they were significantly youngerthan patients (P 5 .001).
Disease Susceptibility
The allele and genotype frequencies of MMP-1, -3, and -9polymorphisms in HF patients and controls are presented inTable 1. The observed genotype frequencies were inHardy-Weinberg equilibrium in cases, controls and in theoverall studied sample for all analyzed polymorphisms. Ge-notype and allele frequencies were remarkably similar in ap-parently healthy controls and cases (all P values !.05).As the MMP-1 and -3 genes are in the same chromosome
cluster (11q22.3), haplotype analysis was undertaken andtheir frequencies were estimated. The polymorphisms werein weak linkage disequilibrium in both groups of subjects(D0 5 0.53; r2 5 0.21 for cases and D0 5 0.56; r2 5 0.22for controls). The frequencies of 1G/6A, 1G/5A, 2G/6A,and 2G/5A haplotypes in patients (0.18, 0.31, 0.42, and0.09, respectively) were similar to those found in controls(0.17, 0.30, 0.43, and 0.10, respectively) (P 5 .72).
Phenotypic Characterization
Clinical and demographic characteristics of patients ac-cording to MMP-1, -3, and -9 genotypes are presented inTable 2. Ischemic etiology, a previous myocardial infarc-tion, regional LV dysfunction, and hypercholesterolemiawere significantly more frequent in MMP-1 2G allelecarriers (n 5 244) HF patients (all P values !.05).The 1G1G genotype was also associated to longer QRScomplex on surface electrocardiogram. MMP-3 polymor-phism (�1171 5A/6A) was not significantly associated tomost HF traditional clinical features. MMP-3 5A carriers(n 5 197), however, had decreased heart rate variability
Table 1. Allele and Genotype Frequencies of MatrixMetalloproteinase (MMP) Gene Polymorphisms in Heart
Failure Patients and Control Individuals
Heart FailurePatients
Apparently HealthyControls
MMP-1, n 313 367Genotype frequency1G1G 69 (22) 93 (25)1G2G 157 (50) 174 (48)2G2G 87 (28) 100 (27)
MMP-3, n 306 366Genotype frequency5A5A 49 (16) 54 (15)5A6A 148 (48) 184 (50)6A6A 109 (36) 128 (35)
MMP-9, n 307 359Genotype frequencyCC 250 (81) 280 (78)CT 54 (18) 75 (21)TT 3 (1) 4 (1)
Results are presented as absolute numbers and percentages in parentheses.P value O0.05 for all comparisons.
Table
2.Clinical
Character
Clinical
Characteristics
MMP-1
Overall
n5
313
1G1G
n5
69
2G n
Age(y)
606
13
626
13
Caucasian
(%)
220(70)
55(81)
Heartfailure
etiology(%
)Ischem
ic118(38)
17(25)
Idiopathic
91(29)
30(44)
Hypertensive
73(23)
16(24)
NYHA
Classes
IandII
(%)
238(76)
52(78)
PreviousMI(%
)101(32)
13(19)
Electrocardiogram
QRSduration(m
s)1296
35
1426
38
1Echocardiography
LV
diastolicdiameter
(mm)
5.6
61.1
5.7
61.0
5LVejectionfraction(%
)316
8306
8Regional
LV
dysfunction(%
)100(32)
12(19)
LV,leftventricular;MI,myocardialinfarction;MMP,
matrixmetalloprote
Dataareexpressed
asmeans
6standard
deviationorabsolute
numbers(

Fig. 1. Kaplan-Meier survival curves comparing heart failure (HF) patients with 1G1G genotype (MMP-1 polymorphism) and 2G allelecarriers (A) all HF patients; (B) nonischemic etiology; (C) ischemic etiology.
118 Journal of Cardiac Failure Vol. 17 No. 2 February 2011
and increased LV dimensions and longer QRS complex du-ration. Finally, we did not observe significant associationsbetween the MMP-9 polymorphism (�1562 C/T) with HFclinical characteristics, except for a longer QRS complexduration in CC homozygous patients (n 5 250).
Because the MMP-1 2G allele was associated to ische-mic HF etiology, we performed multiple logistic regressionanalysis to examine other potential predictors of ischemicetiology in our cohort. The adjusted model showed that2G carriers status was independently associated to ischemicetiology (adjusted OR5 2.15, 95% confidence interval [CI]1.1 to 4.16, P 5 .023) after adjustment for other significantrisk factors (hypercholesterolemia, age, diabetes mellitus,and diastolic blood pressure).
Follow-up and Prognosis
Clinical follow-up data were obtained for all enrolled pa-tients. During a median follow-up of 40 months, there were58 HF-related deaths and 38 deaths from other causes.
Fig. 2. Kaplan-Meier survival curves comparing heart failure (HF) paticarriers (A) all HF patients; (B) nonischemic etiology; (C) ischemic et
Figures 1, 2, and 3 depict theKaplan-Meier survival curves ac-cording to MMP-1, MMP-3, and MMP-9 genotypes, respec-tively (A, all patients; B, nonischemic etiology; C, forischemic etiology). HF-related survival was significantly bet-ter over time inMMP-1 2Gcarriers (log-rankP5 .002).Anal-ysis stratified by etiology demonstrated a similar survivalprofile in non-ischemic patients (Fig. 1B), although we ob-served only a statistical trend in ischemic patients (log rankP5 .091; Fig. 1C). MMP-3 6A carriers also depicted a betterHF-related prognosis, particularly in the nonischemic group(log rank P 5 .039; Fig. 2B). MMP-9 polymorphism had noimpact on HF-related survival, irrespective of etiology(Fig. 3). We performed addition analysis to evaluate the asso-ciation of MMPs polymorphisms to overall mortality and thesame trendwere observed (log rank5 0.05 for decreasedmor-tality for 2G carriers [MMP-1] and 6A carriers [MMP-3]; logrank5 0.23 for the MMP-9 polymorphism).
Cox proportional hazard models were created to evaluatepredictors of HF-related mortality. 2G allele carriers of theMMP-1 gene were independently associated to HF survival
ents with 5A5A genotype (MMP-3 polymorphism) and 6A alleleiology.

Fig. 3. Kaplan-Meier survival curves comparing heart failure (HF) patients with CC genotype (MMP-9 polymorphism) and T allele carriers(A) all HF patients; (B) nonischemic etiology; (C) ischemic etiology.
MMP Polymorphisms and Heart Failure � Velho et al 119
after adjustment for functional class, systolic blood pres-sure, ethnicity, LV dimensions, and serum levels of creati-nine and sodium (OR 0.47; 95% confidence interval 0.27to 0.82; P 5 .008). This association was attenuated ina model that was additionally adjusted for QRS complexduration (model 2 in Table 3), suggesting that part of theinteraction between MMP-1 genotype and HF-relatedsurvival was modulated by intraventricular conductionabnormalities. MMP-3 variants were not independently as-sociated to mortality after adjustment for other risk predic-tors in a Cox regression analysis (OR 1.2; 95% confidenceinterval 0.58 to 2.4; P 5 .64).
Discussion
In the present study, we have demonstrated that a com-mon genetic polymorphism of MMP-1 (�1607 1G/2G)was associated to a higher prevalence of ischemic etiologyamong patients with systolic HF and better HF-relatedprognosis. However, MMPs polymorphisms were not asso-ciated to increased HF susceptibility. Interestingly, thesepolymorphisms implicated in differences on QRS complexduration in surface electrocardiogram, suggesting that theobserved associations could be modulated, at least in part,by intraventricular conduction abnormalities.
Table 3. Univariate Analysis and Cox Proportion
Clinical Characteristics
Univariate Analysis
HR 95% CI P Value H
NYHA functional Class III or IV 3.17 1.86e5.42 !.001 2SBP, each 1 mm Hg 0.98 0.96e0.99 !.001 0Creatinine, each 1 mg/dL 1.94 1.23e3.08 .005 1Sodium, each 1 mEq/L 0.84 0.78e0.91 !.001 0QRS duration, each 10 ms 1.17 1.10e1.25 !.001LV diastolic diameter, each 1 mm 1.47 1.14e1.88 .003 1MMP-1 2G allele carriers 0.44 0.26e0.76 .003 0
LV, left ventricular; MMP, matrix metalloproteinase; NYHA, New York HearQRS duration; Model 2 was adjusted for all variables.
Restructuring of the collagen matrix, performed in partby MMPs, has a pivotal role in LV remodeling of the failingmyocardium and the ultimate transition to cardiacdecompensation.2,3,22e26 MMP expression and activity areelevated in HF of various etiologies, suggesting that extra-cellular matrix remodeling is a common and deliberate re-sponse to myocardium tissue damage.3 Several MMPspolymorphisms have been described and are implicated insignificant effects on gene expression. In particular,MMP-1 and MMP-3 genes have variants in their promoterregions (�1607 1G/2G and -1171 5A/6A, respectively) thatresult in significantly higher transcriptional activity andhave been associated to disease susceptibility and clinicaloutcomes in several cardiovascular conditions.9 Also, theT allele of MMP-9 polymorphism at position �1562 hasbeen associated to the severity of coronary artery diseasein angiographic studies.18 Tang et al13 have investigatedsimilar genetic polymorphisms in Chinese Han patientswith idiopathic dilated cardiomyopathy and found that the5A allele of MMP-3 was associated to HF susceptibility.This association was not replicated in our patients, butthe genetic ancestrality of our study sample is not compara-ble to the Chinese population. In the present study, no sig-nificant differences in the frequencies of MMP-1, MMP-3,and MMP-9 genotypes or alleles were identified between
al Hazard Model for HF-related Mortality
Adjusted Model 1 Adjusted Model 2
R 95% CI P Value HR 95% CI P Value
.88 1.64e5.04 !.001 2.40 1.36e4.22 .002
.98 0.97e0.99 .008 0.99 0.97e0.99 .028
.59 0.97e2.65 .07 1.34 0.79e2.26 .27
.86 0.79e0.93 !.001 0.86 0.79e0.93 !.001e e e 1.13 1.01e1.21 .001.39 1.06e1.82 .016 1.19 0.87e1.61 .27.47 0.27e0.82 .008 0.70 0.39e1.26 .24
t Association; SBP, systolic blood pressure. Model 1 was not adjusted for

Table 4. Previous Studies with MMP-1, -3, and -9 Polymorphisms in Heart Diseases
Studies Patients MMP-1 MMP-3 MMP-9
PrognosisVelho and Cohen et al. HF Y mortality in 2G allele [ mortality* in 5A5A No effectMizon-Gerard et al.14 HF NA [ mortality* in 5A5A [ mortality in T carriers
HF SusceptibilityVelho and Cohen et al. HF No effect No effect No effectTang et al. 13 IDC No effect [ in 5A allele No effectYe et al. 10 CHD Y in 2G2G No effect NAGhilardi et al. 11 ICA stenosis No effect [ in 6A6A NA
[ 6A/2G haplotypeDalepiane et al.27 CHD No effect No effect No effectNojiri et al. 29 MI No effect [ in 5A allele NA
[ in 5A/1G haplotypeHorne et al. 28 CHD [ in 5A/1G haplotype No effect
PhenotypeVelho and Cohen et al. HF [ 2G allele in ischemic etiology No effect No effect
CHD, coronary heart disease; HF, heart failure; IDC, idiopathic cardiomyopathy; ICA, internal carotid stenosis; MI, myocardial infarction; NA, data notavailable.
*The 5A5A genotype was associated to cardiac mortality particularly in non-ischemic patients.
120 Journal of Cardiac Failure Vol. 17 No. 2 February 2011
HF patients and controls in the overall population. (seecomparison with previous studies in Table 4).10,11,13,14,27e29
The association of MMPs polymorphisms and athero-sclerosis has been previously explored in distinct clinicalscenarios leading to somewhat conflicting findings.10,11
Our data suggest that ischemic etiology, previous acutemyocardial infarction, and LV segmental abnormalitieswere more frequent in 2G allele carriers of the MMP-1gene in HF patients. One could speculate that subjectswith the more active genetic variant of the MMP-1 genemight have a reduced chance to develop atherosclerotic dis-ease, as suggested by Ye et al10; but whenever the atheromais already present, the enhanced proteolytic activity couldincrease the risk of plaque instability and implicate inrisk for acute events and ventricular dysfunction, as sug-gested by our findings.
In the present study, we have demonstrated, for the firsttime, a significant association of a common MMP-1(�1607 1G/2G) functional polymorphism with cardiac mor-tality. Patients carrying the more transcriptionally active 2Gallele of the MMP-1 gene had a substantially reduced HF-related mortality. The mechanism of this association has yetto be determined, as 2G allele carriers had similar LV di-mensions, similar prevalence of ventricular arrhythmiason Holter monitoring and received the same pharmacolog-ical treatment. Interestingly, besides the increased preva-lence of ischemic etiology, a recognized marker for worseprognosis in HF, 2G allele carriers were also associatedto a reduced QRS complex duration, a factor that could ex-plain in part the relative favorable evolution of this subsetof patients.30,31 Finally, our prognostic analysis resemblesprevious finding that have independently associated the5A5A genotype (MMP-3) to cardiac mortality only in non-ischemic patients.14
Some methodological aspects of our study deserve care-ful consideration. Considering the theoretical possibilitythat the associations observed in this analysis occur onlyin specific ethnic groups, our results should be viewed
with caution, because there is some degree of genetic ad-mixture in the Caucasian-Brazilian population (w70% ofour sample). However, the prevalence of the studied poly-morphisms was similar to that reported in other Europeanand American populations and our data was fully adjustedfor ethnicity. As expected, our sample of apparently healthycontrols was younger than our HF patients, because thesesubjects were derived from a blood donor clinic. We per-formed a case control analysis restricted to aged controls(O50 years old) and the results were not substantially al-tered (data not shown). Finally, it is well-recognized thatthe net final effect of isolated nucleotide polymorphismsmight be outweighed by other compensatory or regulatorypathways. Measurements of MMPs serum levels or identi-fication of MMPs tissue expression might also enhancethe understanding of the processes involved in HF prognos-tication.
In conclusion, our data suggest that MMP-1 (�1607 1G/2G) polymorphism contributes to the variability of clinicalpresentation and to relevant clinical outcomes in HF pa-tients. We have demonstrated that MMP1 2G allele maypredispose to ischemic disease but is also associated withmore favorable HF survival, probably through differingmechanisms (plaque remodeling vs. myocardial remodel-ing). Because MMPs are expressed in several cell types,these differential effects are biologically sound, but shouldbe evaluated in future studies. Further studies are alsoneeded to explore potential pharmacogenetic interactionsof MMPs polymorphisms. Genetic studies involving differ-ent compensatory pathways 32e34 can set the backgroundfor the development of the ‘‘so-called’’ individualized strat-egies to manage and treat HF.
Acknowledgments
Supported in part by grants from Conselho Nacional deDesenvolvimento Cientifico e Tecnol�ogico (CNPq), Secre-taria de Ciencia e Tecnologia e Fundac~ao de Amparo

MMP Polymorphisms and Heart Failure � Velho et al 121
a Pesquisa do Estado do Rio Grande do Sul (FAPERGS)and Fundo de Incentivo a Pesquisa (FIPE-HCPA).
Disclosures
None.
References
1. Davis RC, Hobbs FDR, Lip GYH. ABC of heart failure: history and
epidemiology. BMJ 2000;320:39e42.2. Spinale FG. Matrix metalloproteinases: regulation and dysregulation
in the failing heart. Circ Res 2002;90:520e30.
3. Fedak PWM, Verma S, Weisel RD, Li R. Cardiac remodeling and fail-
ure: from molecules to man (Part II). Cardiovasc Pathol 2005;14:
49e60.
4. Creemers E, Cleutjens J, Smits J, Daemen M. Matrix metalloprotei-
nase inhibition after myocardial infarction. A new approach to prevent
heart failure? Circ Res 2001;89:201e10.
5. Spinale FG. Matrix metalloproteinase gene polymorphisms in heart
failure: new pieces to the myocardial matrix puzzle. Eur Heart J
2004;25:631e3.6. White AJ, Duffy SJ, Walton AS, Ng JF, Rice GE, Mukherjee S, et al.
Matrix metalloproteinase-3 and coronary remodelling: implications
for unstable coronary disease. Cardiovasc Res 2007;75:813e20.7. Ye S, Eriksson P, Hamsten A, Kurkinen M, Humphries SE,
Henney AM. Progression of coronary atherosclerosis is associated
with a common genetic variant of the human stromelysin-1 promoter
which results in reduced gene expression. J Biol Chem 1996;271:
13055e60.
8. Dunleavey L, Beyzade S, Ye S. Rapid genotype analysis of the matrix
metalloproteinase-1 gene 1G 2G polymorphism that is associated with
risk of cancer. Matrix Biol 2000;19:175e7.9. Ye S. Influence of matrix metalloproteinase genotype on cardiovascular
disease susceptibility and outcome. Cardiovasc Res 2006;69:636e45.
10. Ye S, Gale CR, Martyn N. Variation in the matrix metalloproteinase-1
gene and risk of coronary heart disease. Eur Heart J 2003;24:
1668e71.
11. Ghilardi G, Biondi ML, DeMonti M, Turri O, Guagnellini E,
Scorza R. Matrix metalloproteinase-1 and matrix metalloproteinase-
3 gene promoter polymorphisms are associated with carotid artery ste-
nosis. Stroke 2002;33:2408e12.
12. Martin TN, Penney DE, Smith JA, Groenning BA, Dargie HJ,
Hillis GS. Matrix metalloproteinase-1 promoter polymorphisms and
changes in left ventricular volume following acute myocardial infarc-
tion. Am J Cardiol 2004;94:1044e6.
13. Tang L, Chen X, Zhu M, Jiang JJ, Lu XB, Du YX, et al. Matrix
metalloproteinase-1, -3 and -9 gene polymorphisms and the risk of id-
iopathic dilated cardiomyopathy in Chinese Han population. Clin Bio-
chem 2007;40:1427e30.
14. Mizon-Gerard F, Groote P, Lamblin N, Hermant X, Dallongeville J,
Amouyel P, et al. Prognostic impact of matrix metalloproteinase
gene polymorphisms in patients with heart failure according to the ae-
tiology of left ventricular systolic failure according to the aetiology of
left ventricular systolic dysfunction. Eur Heart J 2004;25:688e93.15. Haberbosch W, Gardemann A. Gelatinase B C(-1562) T polymor-
phism in relation with ischemic heart disease. Scand J Clin Lab Invest
2005;65:513e22.
16. Lahiri DK, Nurnberger JI. A rapid non-enzymatic method for the prep-
aration of HMW DNA from blood for RFLP studies. Nucleic Acids
Res 1991;19:5444.
17. Dunleavey L, Beyzade S, Ye S. Rapid genotype analysis of the strome-
lysin gene 5A/6A polymorphism. Atherosclerosis 2000;151:587e9.
18. Zhang B, Ye S, Herrmann SM, Eriksson P, De Maat M, Evans A, et al.
Functional polymorphism in the regulatory region of gelatinase
B gene in relation to severity of coronary atherosclerosis. Circulation
1999;99:1788e94.
19. Stephens M, Scheet P. Accounting for decay of linkage disequilibrium
in haplotype inference and missing data imputation. Am J Human
Genet 2005;76:449e62.
20. Stephens M, Smith NJ, Donnelly P. A new statistical method for hap-
lotype reconstruction from population data. Am J Human Genet 2001;
68:978e9.
21. Hedrick PW. Gametic disequilibrium measures: proceed with caution.
Genetics 1987;17:331e41.
22. D’Armiento J. Matrix metalloproteinase disruption of the extracellular
matrix and cardiac dysfunction. TCM 2002;12:97e101.
23. Lee RT. Matrix metalloproteinase inhibition and the prevention of
heart failure. TCM 2001;11:202e5.
24. Felkin LE, Birks EJ, George R, Wong S, Khaghani A, Yacoub MH,
et al. A quantitative gene expression profile of matrix metalloprotei-
nases (MMPs) and their inhibitors (TIMPs) in the myocardium of pa-
tients with deteriorating heart failure requiring left ventricular assist
device support. J Heart Lung Transplant 2006;25:1413e9.25. Rohde LE, Ducharme A, Arroyo LH, Aikawa M, Sukhova GH, Lopez-
Anaya A, et al. Matrix metalloproteinase inhibition attenuates early
left ventricular enlargement after experimental myocardial infarction
in mice. Circulation 1999;99:3063e70.
26. Creemers EE, Cleutjens JP, Smits JF, Daemen MJ. Matrix metallopro-
teinases inhibition after myocardial infarction: a new approach to pre-
vent heart failure? Circ Res 2001;89:201e10.
27. Dalepiane VLN, Silvello DN, Paludo CA, Roisenberg I, Simon D. Ma-
trix metalloproteinase gene polymorphisms in patients with coronary
artery disease. Genet Mol Biol 2007;30:505e10.
28. Horne BD, Camp NJ, Carlquist JF, Muhlestein JB, Kolek MJ,
Nicholas ZP, et al. Multiple-polymorphism associations of 7 matrix
metalloproteinase and tissue inhibitor metalloproteinase genes with
myocardial infarction and angiographic coronary artery disease. Am
Heart J 2007;154:751e8.
29. Nojiri T, Morita H, Imai Y, Maemura K, Ohno M, Ogasawara K, et al.
Genetic variations of matrix metalloproteinase-1 and -3 promoter re-
gions and their associations with susceptibility to myocardial infarc-
tion in Japanese. Int J Cardiol 2003;92:181e6.
30. De Winter O, Van de Veire N, Van Heuverswijn F, Van Pottelberge G,
Gillebert TC, De Sutter J. Relationship between QRS duration, left
ventricular volumes and prevalence of nonviability in patients with
coronary artery disease and severe left ventricular dysfunction. Eur J
Heart Fail 2006;8:275e7.
31. Attar MN, Wong K, Groves DG, Newall N, Ramsdale DR, Moore RK.
Clinical implications of QRS duration and QT peak prolongation in
patients with suspected coronary disease referred for elective cardiac
catheterization. Ann Noninvasive Electrocardiol 2008;13:106e12.
32. McNamara DM, Tam SW, Sabolinski ML, Tobelmann P, Janosko K,
Venkitachalam L, et al. Endothelial nitric oxide synthase (NOS3)
polymorphisms in African Americans with heart failure: results
from the A-HeFT trial. J Card Fail 2009;15:191e8.
33. Biolo A, Clausell N, Santos KG, Salvaro R, Ashton-Prolla P,
Borges A, Rohde LE. Impact of beta1-adrenergic receptor polymor-
phisms on susceptibility to heart failure, arrhythmogenesis, prognosis,
and response to beta-blocker therapy. Am J Cardiol 2008;102:726e32.
34. McNamara DM, Holubkov R, Postava L, Janosko K, MacGowan GA,
Mathier M, et al. Pharmacogenetic interactions between angiotensin-
converting enzyme inhibitor therapy and the angiotensin-converting
enzyme deletion polymorphism in patients with congestive heart failure.
J Am Coll Cardiol 2004;44:2019e26.
Related Documents











