Polylactic-co-glycolic acid mesh coated with fibrin or collagen and biological adhesive substance as a prefabricated, degradable, biocompatible, and functional scaffold for regeneration of the urinary bladder wall Salah Abood Salem, 1,2 Ng Min Hwei, 2 Aminuddin Bin Saim, 3 Christopher C.K. Ho, 1,2 Ismail Sagap, 1 Rajesh Singh, 4 Mohd Reusmaazran Yusof, 5 Zulkifili Md Zainuddin, 1,2 Ruszymah Bt. Hj Idrus 2,6 1 Department of Surgery, UKM Medical Centre, Kuala Lumpur, Malaysia 2 Tissue Engineering Centre, UKM Medical Centre, Kuala Lumpur, Malaysia 3 Department of ENT Ampang Putri Specialist Hospital, Kuala Lumpur, Malaysia 4 Department of Orthopedic, UKM Medical Centre, Kuala Lumpur, Malaysia 5 Malaysian Nuclear Agency, Bangi, 43000 Selangor, Malaysia 6 Department of Physiology, UKM Medical Centre, Kuala Lumpur, Malaysia Received 28 September 2012; accepted 29 October 2012 Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/jbm.a.34518 Abstract: The chief obstacle for reconstructing the bladder is the absence of a biomaterial, either permanent or biodegrad- able, that will function as a suitable scaffold for the natural pro- cess of regeneration. In this study, polylactic-co-glycolic acid (PLGA) plus collagen or fibrin was evaluated for its suitability as a scaffold for urinary bladder construct. Human adipose-derived stem cells (HADSCs) were cultured, followed by incubation in smooth muscle cells differentiation media. Differentiated HADSCs were then seeded onto PLGA mesh supported with col- lagen or fibrin. Evaluation of cell-seeded PLGA composite immersed in culture medium was performed under a light and scanning microscope. To determine if the composite is compati- ble with the urodynamic properties of urinary bladder, porosity and leaking test was performed. The PLGA samples were sub- jected to tensile testing was pulled until PLGA fibers break. The results showed that the PLGA composite is biocompatible to dif- ferentiated HADSCs. PLGA-collagen mesh appeared to be opti- mal as a cell carrier while the three-layered PLGA-fibrin composite is better in relation to its leaking/ porosity property. A biomechanical test was also performed for three-layered PLGA with biological adhesive and three-layered PLGA alone. The tensile stress at failure was 30.82 6 3.80 (MPa) and 34.36 6 2.57 (MPa), respectively. Maximum tensile strain at failure was 19.42 6 2.24 (mm) and 23.06 6 2.47 (mm), respectively. Young’s modulus was 0.035 6 0.0083 and 0.043 6 0.012, respectively. The maximum load at break was 58.55 6 7.90 (N) and 65.29 6 4.89 (N), respectively. In conclusion, PLGA-Fibrin fulfils the crite- ria as a scaffold for urinary bladder reconstruction. V C 2013 Wiley Periodicals, Inc. J Biomed Mater Res Part A: 00A:000–000, 2013. Key Words: PLGA, collagen, fibrin, combosite scaffold, regen- eration of urinary bladder wall How to cite this article: Salem SA, Hwei NM, Saim AB, Ho CCK, Sagap I, Singh R, Yusof MR, Md Zainuddin Z, Bt. Hj Idrus R. 2013. Polylactic-co-glycolic acid mesh coated with fibrin or collagen and biological adhesive substance as a prefabricated, degradable, biocompatible, and functional scaffold for regeneration of the urinary bladder wall. J Biomed Mater Res Part A 2013:00A:000–000. INTRODUCTION Urinary bladder may be subjected to both congenital and acquired disorders, which may lead to organ damage and functional loss, which will require eventual reconstruc- tion. 1 Urinary bladder wall structure organization is similar to other hollow organs, consisting of epithelium (urothelium) on the lumen surrounded by a collagen-rich connective tissue and muscle layer. Thus, an ideal bioma- terial must provide the environment in which cellular components of these layers interact with each other and other proteins to regulate cellular adhesion, proliferation differentiation, and function. 2,3 Tissue engineering is a component of regenerative medicine, following the princi- ple of cell transplantation, material science, and engineer- ing toward the development of biological substitutes that would restore and maintain normal function. 1 The first application of a free tissue graft for bladder substitution was reported by Neuhoff in 1917, when fascia was used to augment bladders in dogs. 4 The first use of the term (tissue engineering) in the literature can be traced to a reference dealing with corneal tissue in 1985. 5 For nearly 100 years, physician and scientists have envisioned that diseased and failing organs may be replaced by healthy ones via organ transplantation. 6 Correspondence to: R. Bt. Hj Idrus; e-mail: [email protected] V C 2013 WILEY PERIODICALS, INC. 1

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Polylactic-co-glycolic acid mesh coated with fibrin or collagen andbiological adhesive substance as a prefabricated, degradable,biocompatible, and functional scaffold for regeneration of theurinary bladder wall
Salah Abood Salem,1,2 Ng Min Hwei,2 Aminuddin Bin Saim,3 Christopher C.K. Ho,1,2
Ismail Sagap,1 Rajesh Singh,4 Mohd Reusmaazran Yusof,5 Zulkifili Md Zainuddin,1,2
Ruszymah Bt. Hj Idrus2,6
1Department of Surgery, UKM Medical Centre, Kuala Lumpur, Malaysia2Tissue Engineering Centre, UKM Medical Centre, Kuala Lumpur, Malaysia3Department of ENT Ampang Putri Specialist Hospital, Kuala Lumpur, Malaysia4Department of Orthopedic, UKM Medical Centre, Kuala Lumpur, Malaysia5Malaysian Nuclear Agency, Bangi, 43000 Selangor, Malaysia6Department of Physiology, UKM Medical Centre, Kuala Lumpur, Malaysia
Received 28 September 2012; accepted 29 October 2012
Published online in Wiley Online Library (wileyonlinelibrary.com). DOI: 10.1002/jbm.a.34518
Abstract: The chief obstacle for reconstructing the bladder is
the absence of a biomaterial, either permanent or biodegrad-
able, that will function as a suitable scaffold for the natural pro-
cess of regeneration. In this study, polylactic-co-glycolic acid
(PLGA) plus collagen or fibrin was evaluated for its suitability as
a scaffold for urinary bladder construct. Human adipose-derived
stem cells (HADSCs) were cultured, followed by incubation in
smooth muscle cells differentiation media. Differentiated
HADSCs were then seeded onto PLGA mesh supported with col-
lagen or fibrin. Evaluation of cell-seeded PLGA composite
immersed in culture medium was performed under a light and
scanning microscope. To determine if the composite is compati-
ble with the urodynamic properties of urinary bladder, porosity
and leaking test was performed. The PLGA samples were sub-
jected to tensile testing was pulled until PLGA fibers break. The
results showed that the PLGA composite is biocompatible to dif-
ferentiated HADSCs. PLGA-collagen mesh appeared to be opti-
mal as a cell carrier while the three-layered PLGA-fibrin
composite is better in relation to its leaking/ porosity property.
A biomechanical test was also performed for three-layered
PLGA with biological adhesive and three-layered PLGA alone.
The tensile stress at failure was 30.82 6 3.80 (MPa) and 34.36 6
2.57 (MPa), respectively. Maximum tensile strain at failure was
19.42 6 2.24 (mm) and 23.06 6 2.47 (mm), respectively. Young’s
modulus was 0.035 6 0.0083 and 0.043 6 0.012, respectively.
The maximum load at break was 58.55 6 7.90 (N) and 65.29 6
4.89 (N), respectively. In conclusion, PLGA-Fibrin fulfils the crite-
ria as a scaffold for urinary bladder reconstruction. VC 2013 Wiley
Periodicals, Inc. J Biomed Mater Res Part A: 00A:000–000, 2013.
Key Words: PLGA, collagen, fibrin, combosite scaffold, regen-
eration of urinary bladder wall
How to cite this article: Salem SA, Hwei NM, Saim AB, Ho CCK, Sagap I, Singh R, Yusof MR, Md Zainuddin Z, Bt. Hj Idrus R. 2013.Polylactic-co-glycolic acid mesh coated with fibrin or collagen and biological adhesive substance as a prefabricated, degradable,biocompatible, and functional scaffold for regeneration of the urinary bladder wall. J Biomed Mater Res Part A 2013:00A:000–000.
INTRODUCTION
Urinary bladder may be subjected to both congenital andacquired disorders, which may lead to organ damage andfunctional loss, which will require eventual reconstruc-tion.1 Urinary bladder wall structure organization issimilar to other hollow organs, consisting of epithelium(urothelium) on the lumen surrounded by a collagen-richconnective tissue and muscle layer. Thus, an ideal bioma-terial must provide the environment in which cellularcomponents of these layers interact with each other andother proteins to regulate cellular adhesion, proliferationdifferentiation, and function.2,3 Tissue engineering is a
component of regenerative medicine, following the princi-ple of cell transplantation, material science, and engineer-ing toward the development of biological substitutes thatwould restore and maintain normal function.1 The firstapplication of a free tissue graft for bladder substitutionwas reported by Neuhoff in 1917, when fascia was usedto augment bladders in dogs.4 The first use of the term(tissue engineering) in the literature can be traced to areference dealing with corneal tissue in 1985.5 For nearly100 years, physician and scientists have envisioned thatdiseased and failing organs may be replaced by healthyones via organ transplantation.6
Correspondence to: R. Bt. Hj Idrus; e-mail: [email protected]
VC 2013 WILEY PERIODICALS, INC. 1

The chief obstacle over the years to reconstructing thebladder through regeneration has been the absence of a bioma-terial that will function as a suitable scaffold for the naturalprocess of regeneration. The ideal graft material would providea structurally intact low-pressure reservoir, serve as a scaffoldfor the healing and regeneration of the bladder wall, and retainnormal function until it is replaced by host tissues. Biomateri-als in urinary bladder wall tissue engineering function as anartificial extracellular matrix and elicit biological and mechani-cal function of native extracellular matrix found in tissues inthe body.7 Biomaterials facilitate the localization and deliveryof cells and bioactive and bioactive factors (e.g., cell adhesionpeptide and growth factors) to desired sites in the body anddefine a three-dimensional space for the formation of new tis-sue with appropriate function.8 Therefore, ideal biomaterialshould be nontoxic, biocompatible, supporting tissue regenera-tion without induction of severe inflammatory processes. Thebiomaterial should provide adequate structural support for thetissue regeneration against internal pressure, mechanicalforces, and undergo gradual degradation over time as cellsundergo spatial organization.1,9
Generally, three classes of biomaterials have been used forengineering bladder tissue. Naturally derived material (e.g. col-lagen and alginate), acellular tissue matrices, (e.g., bladder sub-mucosa and small intestinal submucosa), and synthetic poly-mers [e.g., polyglycolic acid (PGA), polylactic acid (PLA), andpolylactic-co-glycolic acid (PLGA)]. Naturally derived materialsand acellular tissue matrices have the potential advantage of bi-ological recognition and contain biomimetic factors.7,10 Syn-thetic polymers can be produced on a large scale with con-trolled properties of their strength, degradation rate, andmicrostructure.11 Generally, the ideal biomaterial should be bio-compatible, promote cellular interaction and tissue develop-ment, and possess proper mechanical and physical properties.11
PLGA or poly (lactic-co-glycolic acid) is a copolymer, whichis used in a host of Food and Drug Administration (FDA)-approved therapeutic devices, owing to its biodegradabilityand biocompatibility. PLGA has been successful as a biodegrad-able polymer because it undergoes hydrolysis in the body toproduce the original monomers, lactic acid, and glycolic acid.These two monomers under normal physiological conditionsare by-products of various metabolic pathways in the body.Also, the possibility of tailoring the polymer degradation timeby altering the ratio of the monomers used during synthesishas made PLGA a common choice in the production of a varietyof biomedical devices, such as, grafts, sutures, implants, pros-thetic devices, micro, and nanoparticles.12 Fibrin is an impor-tant component of blood hemostasis and has been used fre-quently as a biopolymer scaffold in tissue engineering. Fibrinhas been used as a biological scaffold to regenerate differentkinds of body tissue, including bone, cartilage, nervous tissue,cardiac tissue, skin, ocular tissue, liver, and tendons. Thus,fibrin represents a versatile biopolymer and show a properpotential in tissue regeneration and organ reconstruction.13–15
MATERIALS AND METHODS
A composite scaffold that was used in this study composedof PLGA, poly (lactic-co-glycolic acid) PLGA mesh MV94 pur-
chased from Johnson & Johnson. VICRYL mesh consists of Poly-glactin 910, a synthetic absorbable copolymer made from 90%glycolic and 10% L-lactic. The mesh was knitted from uncoatedand undyed fiber identical in composition to that used inVICRYL suture, which has been found to be inert, nonantigenic,nonpyrogenic, and to elicit only a mild tissue reaction duringabsorption. PLGA is a biodegradable, biocompatible copolymerwhich under normal physiological conditions, undergoes hy-drolysis in the body to produce the original monomers. Thereis very minimal systemic toxicity associated with using PLGAfor drug delivery or biomaterial applications.12 In this study,the biomaterial composite consists of PLGA plus Collagen orFibrin seeded by cells. Collagen type one from kangaroo tailpurchased from Sigma at a concentration of 1.5 mg/mL in 0.1M acetic acid was used in the PLGA-Collagen composite.Human plasma fibrin with calcium chloride 0.5 M in the con-centration of 30 lg/mL was used in PLGA-Fibrin composite.Human adipose-derived stem cells (HADSCs) were culturedand proliferated until Passage 2 followed by incubation insmooth muscle differentiated media for 6 weeks. Cells aftertrypsinization, performed using 0.05 trypsin, were collected,mixed with 100 lL medium, and pipetted on PLGA polymer ina concentration of 1 � 106/cm2.
Evaluation of a cell-seeded PLGA composite scaffoldPLGA composite preparation and light microscopic eval-uation. A rounded single layer piece of PLGA knitted mesh,undyed, absorbable (VICRYL, Polyglactin), manufactured byJohnson & Johnson, Belgium, was placed in the floor of thefour-well cell culture plate. The mesh was covered by colla-gen gel of concentration 1.5 mg/mL in 0.1 M acetic acid ,800 lL of collagen solution, added to it 100 lL of 10� me-dium buffered with HEPES, and adjustment of pH to physio-logical level with 100 lL 1M sodium hydroxide. Kangarootail collagen purchased from (Sigma) was used. Collagen so-lution was dispensed onto the PLGA mesh covering a depthof 1–2 mm (PLGA-Collagen Group). Another group of PLGAmesh was coated by human fibrin mixed with 0.5 M calciumchloride (PLGA-Fibrin Group). Third group of PLGA meshwithout collagen or fibrin was used as control (PLGA onlyGroup). Adipose tissue samples were digested with 0.075%Collagenase Type I and culture-expanded in vitro. ADSCs atPassage 2 were differentiated by incubation for 3 and 6weeks in smooth muscle inductive media (SMIM) consistingof MCDB 131 medium, 1% fetal bovine serum (FBS), and100 U/mL heparin. HADSCs in noninductive media wereused as control. Characterization was performed by cellmorphology, gene, and protein expression. Differentiatedcells became elongated and spindle-shaped, and toward theend of 6 weeks, sporadic cell aggregation appeared, whichis typical for smooth muscle cells culture. For the geneexpression study, smooth muscle markers, that is, Alfasmooth muscle actin (ASMA), calponin, and Myosin heavychain (MHC) were used. Expression of these genes wasdetected by PCR after 3 weeks and 6 weeks differentiation.At the protein expression level, ASMA, MHC, smoothelinwere expressed after 6 weeks differentiation. However, onlyASMA and smoothelin were expressed after 3 weeks
2 SALEM ET AL. PLGA-COLLAGEN/FIBRIN COMPOSITE FOR REGENERATION OF URINARY BLADDER WALL
differentiation. Six weeks differentiated cell group wasselected to be incorporated in this study. Cells were trypsi-nized, and 1 � 106 cells were suspended in 100 lL mediumand seeded onto a scaffold. The cell-seeded constructs wereincubated at 37
�C, 5% CO2 with media change every third
day. All three groups of PLGA mesh were seeded with cellsand cultured in a 24-well plate. Inspections of cell-seededsynthetic absorbable mesh under a microscope were per-formed regularly every third day.
Scanning electron microscopic evaluationSimilar groups of PLGA mesh were prepared for evaluatingsome of PLGA mesh physical properties and the interactionwith seeded cells by visualization of surface features undera scanning electron microscope (SEM). Quanta 200 SEMwith a software Quanta 250 (fourth edition) with a magnifi-cation range 50–150,000� was used for visualization thesamples. Briefly, samples were sputter-coated with gold-pal-ladium in the presence of argon gas at room temperatureand visualized at 500� 2,500�, and 5,000� magnification.Also, four groups of PLGA mesh were prepared. Scaffoldpreparation and cell seeding were performed as previouslydescribed for a light microscopy sample. A cell-seeded scaf-fold was incubated in 37�C, 5% CO2, at the time of examina-tion sample fixation with 4% formaldehyde in phosphatebuffered saline (PBS) for 10 min followed by washing with0.1 M phosphate buffer for 10 min three times at room tem-perature. Secondary fixation with 1% osmium tetraoxide for1 hour at room temperature, followed by washing threetimes with 0.1 M phosphate buffer for 10 min each time atroom temperature. Dehydration in serial steps using differ-ent ethanol concentrations, followed by sample drying, wasdone using CO2 for half an hour. Sample mounting with sil-ver paste and coating with gold were done before sendingthe sample for observation under a microscope.
Leaking and porosity testThree types of construct composed of PLGA with collagenand cells, PLGA with fibrin and cells, and PLGA with cells only,each type constructed to be of different thickness determinedby using single, double, and triple PLGA mesh layers, weretested for porosity and leaking properties aiming to choosethe proper biomaterial compatible with the urodynamic prop-erties of urinary bladder and suitable reconstruction. Addi-tional fourth and fifth groups of three-layered PLGA meshwere evaluated for leaking properties; the fourth group wassupported with biological adhesive hydrogel (BioGlue) on oneside, whereas the fifth group was supported with biologicaladhesive hydrogel (BioGlue) on one side and fibrin sealant(Tisseel) on the other side. In the test, composite biomaterialwas clamped between two flat round glass discs with a cen-tral hole of 1 cm2 surface area and was subjected to differingfluid pressure. For porosity assessment, the flow-throughmethod was applied. Porosity was defined as the flow ofwater through the biomaterial per unit time and per unit sur-face area at a defined pressure.16 The biomaterial was placedat the neck of a special glass bottle with another glass piece,representing the upper segment, and between them the
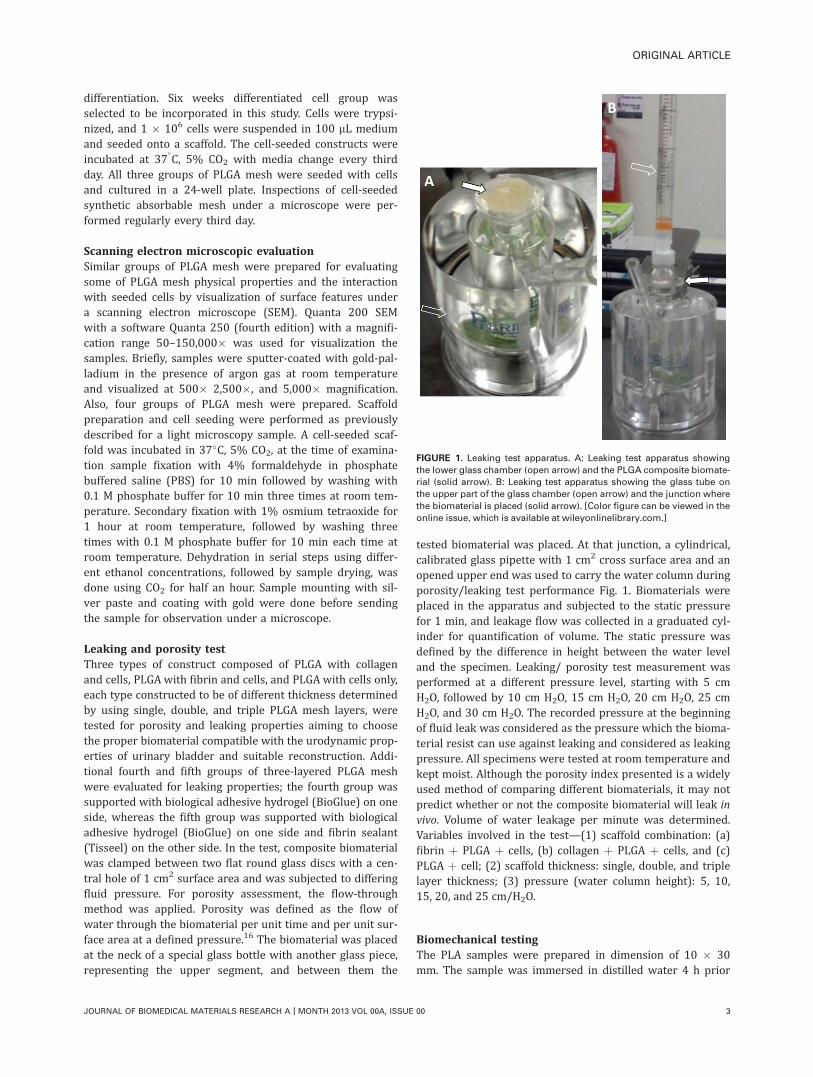
tested biomaterial was placed. At that junction, a cylindrical,calibrated glass pipette with 1 cm2 cross surface area and anopened upper end was used to carry the water column duringporosity/leaking test performance Fig. 1. Biomaterials wereplaced in the apparatus and subjected to the static pressurefor 1 min, and leakage flow was collected in a graduated cyl-inder for quantification of volume. The static pressure wasdefined by the difference in height between the water leveland the specimen. Leaking/ porosity test measurement wasperformed at a different pressure level, starting with 5 cmH2O, followed by 10 cm H2O, 15 cm H2O, 20 cm H2O, 25 cmH2O, and 30 cm H2O. The recorded pressure at the beginningof fluid leak was considered as the pressure which the bioma-terial resist can use against leaking and considered as leakingpressure. All specimens were tested at room temperature andkept moist. Although the porosity index presented is a widelyused method of comparing different biomaterials, it may notpredict whether or not the composite biomaterial will leak invivo. Volume of water leakage per minute was determined.Variables involved in the test—(1) scaffold combination: (a)fibrin þ PLGA þ cells, (b) collagen þ PLGA þ cells, and (c)PLGA þ cell; (2) scaffold thickness: single, double, and triplelayer thickness; (3) pressure (water column height): 5, 10,15, 20, and 25 cm/H2O.
Biomechanical testingThe PLA samples were prepared in dimension of 10 � 30mm. The sample was immersed in distilled water 4 h prior
FIGURE 1. Leaking test apparatus. A: Leaking test apparatus showing
the lower glass chamber (open arrow) and the PLGA composite biomate-
rial (solid arrow). B: Leaking test apparatus showing the glass tube on
the upper part of the glass chamber (open arrow) and the junction where
the biomaterial is placed (solid arrow). [Color figure can be viewed in the
online issue, which is available at wileyonlinelibrary.com.]
ORIGINAL ARTICLE
JOURNAL OF BIOMEDICAL MATERIALS RESEARCH A | MONTH 2013 VOL 00A, ISSUE 00 3

to testing. The sample thickness of 0.20 mm was obtainedby using a SEM (FEI, Quanta 400). Four groups of PLGAwere incorporated in biomechanical testing, representingPLGA single layer, PLGA double layer, PLGA triple layer, andPLGA triple layer with biological adhesive substances. Thetensile test was conducted using a Biomedical Material Test-ing Machine, Instron 8874 fitted with 5 kN load transducerat 0.1 mm/min of crosshead velocity. The hydraulic type ofgripping system equipped with jaw faces was applied togrip the PLGA sample. The sample was pulled until it broke,and Merlin software was used to record and displaythe properties of each test. Six samples were measured ineach group.
Biomaterial degradationBiomaterial degradation was tested by placing small pieces (1� 1) cm of composite biomaterial composed of PLGA withcollagen or fibrin seeded by cells in a 6-well plate, with FD þFBS 10% medium changed every third day. Biomaterial wasconsidered as foreign body if implanted in living tissue.Therefore, it is subjected to degradation, elimination, andpost implant substitution by new tissue. Inspection of PLGAfibers morphological degradation changes, such as loss offibers integrity, change of media color, and cell–biomaterial
interaction, such as cell attachment and bridging of interven-ing gaps, were observed carefully under microscope for 8weeks regularly every third day at the time of media change.
Bladder shape configurationTo form a scaffold in the shape of a subtotal bladder, threelayers of PLGA mesh were sutured together using 0.5 Vicrylsynthetic absorbable sutures, covered with either fibrin orcollagen, and molded to take the shape of upper two thirdof the experimental animal urinary bladder. PLGA biomate-rial physical properties, such as rigidity and flexibility, pro-vided the required property for scaffold shape modification.As this study was related to urinary bladder reconstruction,the required scaffold was prepared in the form and the sizeof bladder dome of the involved experimental animal (nuderat). Preparation of bladder scaffold in the size of full blad-der is mandatory in reconstruction of a hollow, inflatable–deflatable organ. For that, the upper part of urinary bladder(bladder dome) scaffold was prepared with a side-walllength of 10 mm and the dome height of 4–5 mm; associ-ated bladder wall thickness composed of three layers withan average construct thickness of 1–1.2 mm sutured to-gether using synthetic absorbable suture. Biomaterial rigid-ity provided by PLGA mesh represents an important aspect
FIGURE 2. PLGA composite scaffold with cells under a light microscope. A: PLGA mesh without fibrin or collagen substances and no cells. B:
PLGA composite mesh without fibrin or collagen substances, seeded with cells showing cells occupying the inter fiber spaces. C: PLGA compos-
ite mesh with fibrin and no cells showing fibrin occupying the inter fiber spaces. D: PLGA composite mesh with fibrin and cells showing cells
and fibrin occupying the inter fiber spaces. E: PLGA composite mesh with collagen and no cells showing collagen occupying the inter fiber
spaces. F: PLGA composite mesh with collagen and cells showing cells and collagen occupying the inter fiber spaces. G: PLGA composite mesh
with biological adhesive substance covering the mesh and obliterate the mesh gaps. H: PLGA composite mesh (6 weeks after cell seeding)
show biodegradation and cell detachment.
4 SALEM ET AL. PLGA-COLLAGEN/FIBRIN COMPOSITE FOR REGENERATION OF URINARY BLADDER WALL

in the maintenance of full bladder shape during reconstruc-tion and represent important reconstruction aspect againstscaffold shrinkage and collapse.
RESULTS
LightmicroscopyCell growth. Inspections of cell-seeded synthetic absorb-able mesh were performed regularly at the time of mediachange using a light microscope (Fig. 2). No signs of infec-tions or contaminations were noted during the whole pro-cedure. Cells growing at the mesh intervening spaces andon the mesh fibers were noted in considerable cells num-ber impeded within a thin collagen or fibrin film seenspread in spaces intervening the knitted mesh fibers. Thevisible attached cells were large in number, occupying thewhole knitted mesh spaces, nearly no gaps among cellsleft. Cells seen healthy elongated with a clear shape andboundaries. Cells in PLGA only mesh were seen growing inthe PLGA knitted mesh fiber spaces in considerableamount but lesser than that growing with collagen andwith less distinct shape and configurations (morphology).The visible result of the cell–biomaterial interaction wasevident in cells attachment and filling of the interveningspaces, which indicate that the PLGA composite biomate-rial is suitable as a cell carrier device during the regenera-tion process.
Biomaterial degradation. Inspection of PLGA mesh fibersintegrity and degradation was regularly performed duringmedia change every third day. During the first two weeks,the PLGA mesh fibers were intact without any disintegra-tion; cell proliferation and attachment were proper to thefibers; and mesh gaps were fulfilled with growing, prolifer-ating cells. At the third week, PLGA mesh fibers started toundergo degradation, which built up gradually over time,beginning in the form of minimal fibers cracking, breaking,and separation, which increased with subsequent days andweeks. The changes associated with cells detachment andloss of its organization were gaps that started to appear inthe mesh intervening spaces, which were stuffed by cellsand increased gradually as the cell detachment increasedwith time. This gives rise to the hypothesis of degradationof cells anchoring sites, and the accumulation of degradedtoxic substances, which cannot be removed immediately asin vivo. These manifestations became marked by the 6–8weeks where fibers degradations became excessive and cellsdetachment with appearance of wide gaps at the interven-ing spaces of PLGA mesh became more prominent.
Scanning electron microscopyDetermination of PLGA composite scaffold properties usinga SEM were aimed to assess cells–scaffold interaction ascells attachment, the composite that has higher affinity forcell anchoring and attachment, as well as the appearanceof attached cells, its size, and configuration. PLGA meshfibers physical properties were similar in all the threetypes of the composite. The differences of biomaterial com-posite were related to the biologically active substancesand attached cells. PLGA mesh fibers bundle have an aver-age diameter of 179.56 6 12.30 lm, whereas the PLGAfibers have an average diameter of 14.65 6 0.24 lm. Theaverage of inter fibers bundle gaps was 214.57 lm. The
FIGURE 3. PLGA mesh biomaterial with cells (no fibrin or collagen)
under SEM. A: Overview of PLGA mesh biomaterial, 50� magnifica-
tion. B: PLGA mesh with attached cells, 500� magnification. C: PLGA
mesh showing measurement of intervening space, 100� magnifica-
tion. [Color figure can be viewed in the online issue, which is avail-
able at wileyonlinelibrary.com.]
ORIGINAL ARTICLE
JOURNAL OF BIOMEDICAL MATERIALS RESEARCH A | MONTH 2013 VOL 00A, ISSUE 00 5
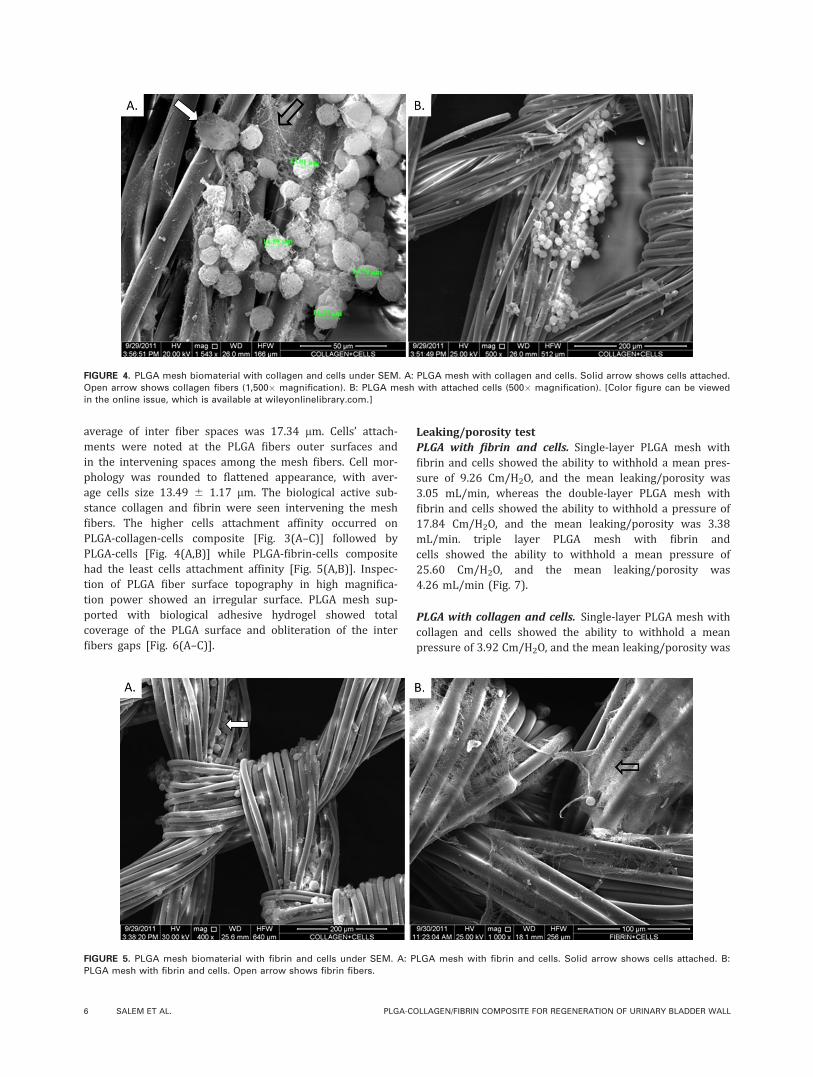
average of inter fiber spaces was 17.34 lm. Cells’ attach-ments were noted at the PLGA fibers outer surfaces andin the intervening spaces among the mesh fibers. Cell mor-phology was rounded to flattened appearance, with aver-age cells size 13.49 6 1.17 lm. The biological active sub-stance collagen and fibrin were seen intervening the meshfibers. The higher cells attachment affinity occurred onPLGA-collagen-cells composite [Fig. 3(A–C)] followed byPLGA-cells [Fig. 4(A,B)] while PLGA-fibrin-cells compositehad the least cells attachment affinity [Fig. 5(A,B)]. Inspec-tion of PLGA fiber surface topography in high magnifica-tion power showed an irregular surface. PLGA mesh sup-ported with biological adhesive hydrogel showed totalcoverage of the PLGA surface and obliteration of the interfibers gaps [Fig. 6(A–C)].
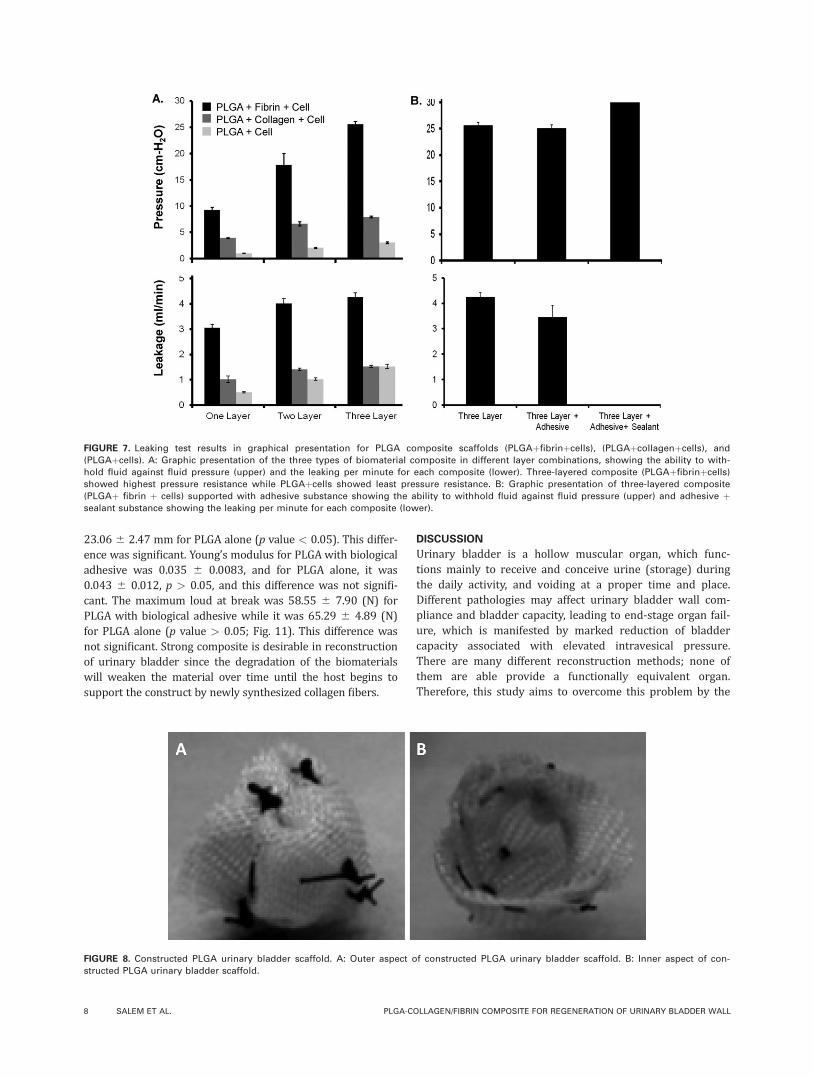
Leaking/porosity testPLGA with fibrin and cells. Single-layer PLGA mesh withfibrin and cells showed the ability to withhold a mean pres-sure of 9.26 Cm/H2O, and the mean leaking/porosity was3.05 mL/min, whereas the double-layer PLGA mesh withfibrin and cells showed the ability to withhold a pressure of17.84 Cm/H2O, and the mean leaking/porosity was 3.38mL/min. triple layer PLGA mesh with fibrin andcells showed the ability to withhold a mean pressure of25.60 Cm/H2O, and the mean leaking/porosity was4.26 mL/min (Fig. 7).
PLGA with collagen and cells. Single-layer PLGA mesh withcollagen and cells showed the ability to withhold a meanpressure of 3.92 Cm/H2O, and the mean leaking/porosity was
FIGURE 5. PLGA mesh biomaterial with fibrin and cells under SEM. A: PLGA mesh with fibrin and cells. Solid arrow shows cells attached. B:
PLGA mesh with fibrin and cells. Open arrow shows fibrin fibers.
FIGURE 4. PLGA mesh biomaterial with collagen and cells under SEM. A: PLGA mesh with collagen and cells. Solid arrow shows cells attached.
Open arrow shows collagen fibers (1,500� magnification). B: PLGA mesh with attached cells (500� magnification). [Color figure can be viewed
in the online issue, which is available at wileyonlinelibrary.com.]
6 SALEM ET AL. PLGA-COLLAGEN/FIBRIN COMPOSITE FOR REGENERATION OF URINARY BLADDER WALL

1.02 mL/min, whereas double-layer PLGA mesh with collagenand cells showed the ability to withhold a pressure of 6.64Cm/H2O, and the mean leaking/porosity was 1.42 mL/min.Treble-layer PLGA mesh with collagen and cells showed theability to withhold a mean pressure of 7.95 Cm/H2O, and themean leaking/porosity was 1.53 mL/min (Fig. 7).
PLGA with cells. Single-layer PLGA mesh with cells showedthe ability to withhold a mean pressure of 1.03 cm/H2O,and the mean leaking/porosity was 0.51 mL/min. On theother hand, double-layer PLGA mesh and cells showed theability to withhold a pressure of 2.05 cm/H2O, and themean leaking/porosity was 1.02 mL/min. Treble-layer PLGAmesh and cells showed the ability to withhold a mean pres-sure of 3.06 Cm/H2O, and the mean leaking/porosity was1.53 mL/min (Fig. 7).
PLGA with fibrin and cells supported with surgical adhe-sive hydrogel (BioGlue). Treble-layer PLGA mesh withfibrin and cells supported with a layer of surgical adhesivehydrogel (BioGlue) showed the ability to withhold a meanpressure of 25.02 Cm/H2O, and the mean leaking/porositywas 3.39 mL/min (Fig. 7).
PLGA with fibrin and cells supported with surgical adhe-sive hydrogel (BioGlue) and fibrin sealant. Treble-layer PLGAmesh with fibrin and cells supported with a layer of surgicaladhesive hydrogel (BioGlue) and fibrin sealant showed theability to withhold a mean pressure of 30.00 cm/H2O, andthe mean leaking/porosity was 00.00 mL/min (Fig. 7).
Native bladder has a mean resting pressure of 5–6 Cm/H2O and a mean voiding pressure of 18–19 cm/H2O. Meanbladder volume was 1.40 6 0.02 mL. Bladder wall thicknesswas 1–2 mm.
Bladder shape configurationThe PLGA mesh is malleable and was easily molded to forma dome shape as shown in Figure 8(A,B). For scaffold modu-lation and preparation, three layers of PLGA mesh weresutured together using absorbable sutures. Preparation ofbladder scaffold in the size of full bladder is mandatory inreconstruction of hollow, inflatable–deflatable organ. Forthat, the upper part of urinary bladder (bladder dome) ofthe involved experimental animal (nude rat) and scaffoldwas prepared with a side wall length 10 mm and the domeheight 4–5 mm. Associated bladder wall thickness com-posed of three layers with an average construct thickness of1–1.2 mm sutured together using synthetic absorbablesuture. As the inner (urothelium) layer of the bladder actedmainly as a sealing layer, the inner layer of the constructwas covered by biological adhesive substance to act as asealing layer. Biomaterial properties provided by PLGAmesh represent the important aspect in the maintenance ofa full bladder shape during reconstruction and also againstscaffold shrinkage and collapse.
Biomechanical testingThe results showed that the PLGA biomaterial has the follow-ing mechanical properties (Figs. 9 and 10). Six samples weremeasured in each group. The tensile stress at failure was30.82 6 3.80 MPa for PLGA with biological adhesive. How-ever, it was 34.36 6 2.57 MPa for three-layered PLGA alone(p value > 0.05). The difference was not significant.Maximum tensile strain at failure was 19.42 6 2.24 mm forPLGA with biological adhesive substance while it was
FIGURE 6. PLGA mesh biomaterial with biological adhesive substances
under SEM At 100� magnification (A,B) and 300� magnification (C).
ORIGINAL ARTICLE
JOURNAL OF BIOMEDICAL MATERIALS RESEARCH A | MONTH 2013 VOL 00A, ISSUE 00 7
23.06 6 2.47 mm for PLGA alone (p value < 0.05). This differ-ence was significant. Young’s modulus for PLGA with biologicaladhesive was 0.035 6 0.0083, and for PLGA alone, it was0.043 6 0.012, p > 0.05, and this difference was not signifi-cant. The maximum loud at break was 58.55 6 7.90 (N) forPLGA with biological adhesive while it was 65.29 6 4.89 (N)for PLGA alone (p value > 0.05; Fig. 11). This difference wasnot significant. Strong composite is desirable in reconstructionof urinary bladder since the degradation of the biomaterialswill weaken the material over time until the host begins tosupport the construct by newly synthesized collagen fibers.
DISCUSSION
Urinary bladder is a hollow muscular organ, which func-tions mainly to receive and conceive urine (storage) duringthe daily activity, and voiding at a proper time and place.Different pathologies may affect urinary bladder wall com-pliance and bladder capacity, leading to end-stage organ fail-ure, which is manifested by marked reduction of bladdercapacity associated with elevated intravesical pressure.There are many different reconstruction methods; none ofthem are able provide a functionally equivalent organ.Therefore, this study aims to overcome this problem by the
FIGURE 7. Leaking test results in graphical presentation for PLGA composite scaffolds (PLGAþfibrinþcells), (PLGAþcollagenþcells), and
(PLGAþcells). A: Graphic presentation of the three types of biomaterial composite in different layer combinations, showing the ability to with-
hold fluid against fluid pressure (upper) and the leaking per minute for each composite (lower). Three-layered composite (PLGAþfibrinþcells)
showed highest pressure resistance while PLGAþcells showed least pressure resistance. B: Graphic presentation of three-layered composite
(PLGAþ fibrin þ cells) supported with adhesive substance showing the ability to withhold fluid against fluid pressure (upper) and adhesive þsealant substance showing the leaking per minute for each composite (lower).
FIGURE 8. Constructed PLGA urinary bladder scaffold. A: Outer aspect of constructed PLGA urinary bladder scaffold. B: Inner aspect of con-
structed PLGA urinary bladder scaffold.
8 SALEM ET AL. PLGA-COLLAGEN/FIBRIN COMPOSITE FOR REGENERATION OF URINARY BLADDER WALL
usage of tissue engineering technique to regenerate a neworgan that has similar properties of the native organ. Forthat purpose, a cell carrier device (biomaterial) was selectedto be used for urinary bladder reconstruction. In this study,the composite scaffold consisting of PLGA VICRYL meshwould provide the required physical strength required towithhold the scaffold against in vivo mechanical forces, pre-venting collapse and shrinkage, while the collagen or fibrinwill provide the biological recognition component requiredfor cell attachment, proliferation, and organization.
In this study, we wanted to determine the biomaterialproperties and also wanted to know whether it can act as acell carrier device, which has proper cells attachment affin-ity, by which we can assess biocompatibility and the degreeof toxicity of the biomaterial. Besides that, we also wantedto study whether the biomaterial can be degraded graduallyafter cell seeding allowing native matrix tissue formation.We also wanted to investigate whether the biomaterial canconfine urine within the bladder against intravesical pres-sure, and whether the nutritional material can reach theinter fiber spaces supplying the cells. Adequate cell culture,proliferation, and differentiation lead to production ofhealthy cells, which when harvested and seeded on suitablethree-dimensional biomaterial could attach, grow, and prolif-erate. The adequate cell–biomaterial interaction, which indi-cate nontoxic biocompatible PLGA mesh substance, was visi-ble by proper cells attachment and filling of inter fiberspaces in vitro as seen under a light microscope. The begin-ning of cells detachment and breaking of PLGA fibers at thethird week indicated the beginning of biomaterial degrada-tion. For that, cell culture and proliferation in vitro shouldnot exceed 2 weeks, followed by implantation in vivo.
Cells growing in multilayer PLGA mesh mean that theinter fibers bundle gaps were well reduced markedly by
overlapping fibers and by the growing cells filling thatspaces. In this way, the composite scaffold could act as blad-der wall (barrier) between the organ cavity and surround-ing external spaces. Urine confinement within the urinarybladder during regeneration depended on seeded cells pro-liferation and growth, and the usage of multiple layers ofPLGA mesh for scaffold construction leading to fibers over-lapping and minimizing the inter fiber spaces, which, whenstuffed with cells and inter cellular matrix, act as a sealagainst urine spillage outside the urinary bladder.
Cells attachment to biomaterial was also visible underan electron microscope with higher affinity of cells attach-ment shown by PLGA-collagen composite. This higher scalebiomaterial-cells interaction by attachment and proliferationindicated that PLGA–collagen composite represent the bestcomposite cells carrier. PLGA with cells only composite alsoreveal a considerable cellular attachment, which indicatedthat PLGA biomaterial can act as a suitable cell carrier de-vice with or without biological active substances. Lowernumber of cells attachment in PLGA-fibrin composite maybe related to the entrapment of cells within solidified por-tion before cell seeding.
For the leaking/porosity test, which is related toimplanted cells’ nutrition and urine confinement within thebladder during regeneration, three kinds of composite scaf-fold were tested, with single, double, and triple layers, aim-ing to determine the proper composite, which can withholdurine within the bladder during regeneration and allowingproper nutritional supplies to the implanted cells. The reachof nutritional supplies was mandatory as the entire compos-ite was permeable to a certain degree. The choice of suita-ble biomaterial to prevent urinary leaking was determinedby the ability of biomaterial to withhold fluid pressure simi-lar to that expressed by native bladder. In this study, the
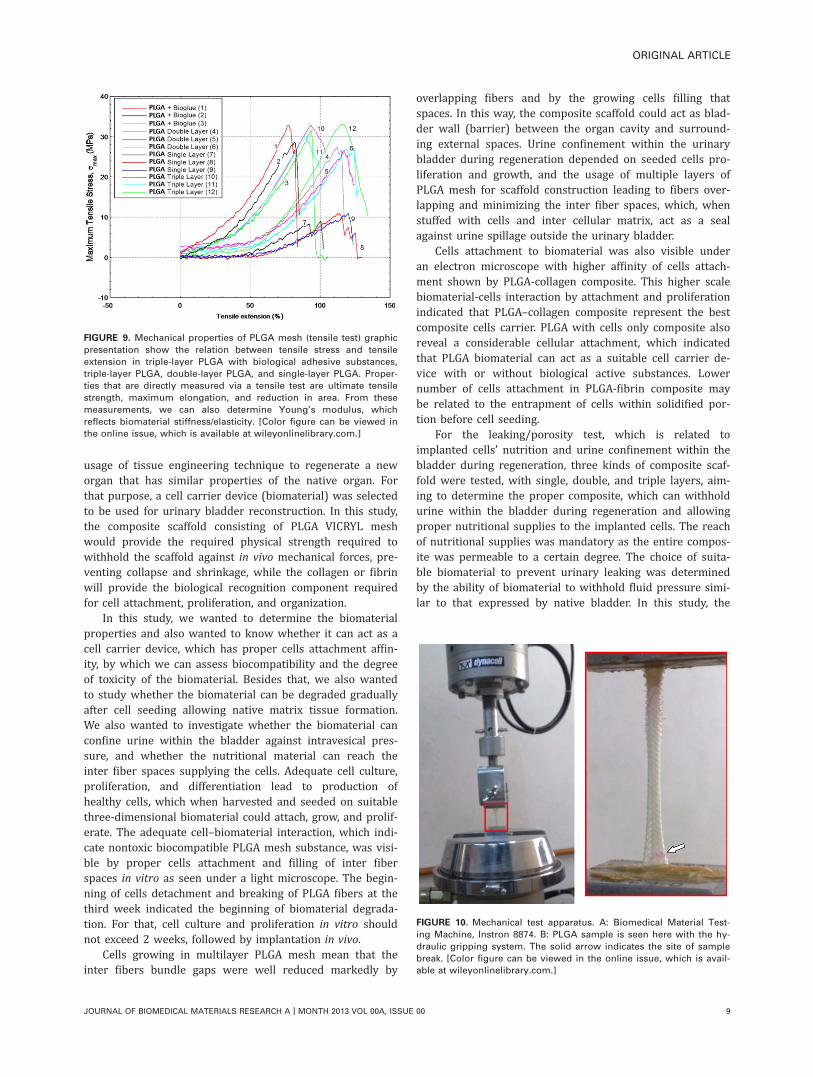
FIGURE 9. Mechanical properties of PLGA mesh (tensile test) graphic
presentation show the relation between tensile stress and tensile
extension in triple-layer PLGA with biological adhesive substances,
triple-layer PLGA, double-layer PLGA, and single-layer PLGA. Proper-
ties that are directly measured via a tensile test are ultimate tensile
strength, maximum elongation, and reduction in area. From these
measurements, we can also determine Young’s modulus, which
reflects biomaterial stiffness/elasticity. [Color figure can be viewed in
the online issue, which is available at wileyonlinelibrary.com.]
FIGURE 10. Mechanical test apparatus. A: Biomedical Material Test-
ing Machine, Instron 8874. B: PLGA sample is seen here with the hy-
draulic gripping system. The solid arrow indicates the site of sample
break. [Color figure can be viewed in the online issue, which is avail-
able at wileyonlinelibrary.com.]
ORIGINAL ARTICLE
JOURNAL OF BIOMEDICAL MATERIALS RESEARCH A | MONTH 2013 VOL 00A, ISSUE 00 9

native bladder had a mean resting pressure of 5–6 Cm/H2Oand a mean voiding pressure of 18–19 Cm/H2O. PLGA þfibrin and cells represent the suitable composite in relationto fluid confinement and leaking prevention, as double-layerPLGA mesh with fibrin and cells showed ability to withholda pressure of 17.84 Cm/H2O, and the mean leaking/porositywas 3.38 mL/min. Treble-layer PLGA mesh with fibrin andcells showed the ability to withhold a mean pressure of25.60 Cm/H2O, and the mean leaking/porosity was 4.26mL/min. Both double- and triple-layer scaffold had the high-est pressure reading, which mimicked a voiding pressure ofthe experimental animal native bladder. In this study, wechose the three-layered PLGAþ fibrinþ cells composite asthe resulting mesh fibers overlapping produced more reduc-tion in the fibers intervening spaces, and the intravesicalpressure during regeneration was expected to be higherthan that of the native bladder due to subtotal urinary blad-der wall replacement with the synthetic composite scaffold.
PLGA biomaterial physical properties, such as rigidityand flexibility, provided the required property for scaffoldshape modification. As this study was related to urinarybladder reconstruction, the required scaffold was preparedin the form and the size of the bladder dome. Preparationof bladder scaffold in the size of full bladder is mandatoryin reconstruction of hollow, inflatable–deflatable organ. Forthat reason, the upper part of urinary bladder (bladderdome) scaffold was prepared with a side wall length of 10mm and the dome height of 4–5 mm; associated bladder
wall thickness composed of three layers with average con-struct thickness 1–1.2 mm sutured together using syntheticabsorbable suture. As the inner (urothelium) layer of thebladder act mainly as the sealing layer, the inner layer ofthe construct was covered by biological adhesive substanceto act as a sealing layer. Biomaterial rigidity provided byPLGA mesh represents an important aspect in the mainte-nance of full bladder shape during reconstruction and pro-tection against scaffold shrinkage and collapse.
CONCLUSION
Urinary bladder reconstruction requires suitable biomaterialto act as a cell carrier device during native tissue regenera-tion. In this study, the selected biomaterial was scaffoldcomposite consisting of PLGA polymer with collagen orfibrin seeded by cells. The scaffold provided the suitablephysical and biological properties. The biocompatibilityproperty enables proper cells growth and multiplication onthe biomaterial, and the biodegradability trait enables nativetissue substitution. The PLGA mesh modulation ability andsatisfactory stiffness enable the formation of urinary blad-der-shaped scaffold that can resist in vivo forces and main-tain the urinary bladder shape during bladder regeneration.PLGA composite showed the ability to act as a barrieragainst fluid leakage under certain pressure in vitro (leak-ing/porosity test). All these properties makes PLGA compos-ite scaffold suitable for urinary bladder reconstruction.However, this may not predict whether the composite
FIGURE 11. Tensile test results in graphical presentation for four specimens of PLGA biomaterial in different layer combinations, that is, three-
layered PLGA with biological adhesive substance (hydrogel), triple-layer PLGA, double-layer PLGA, and single-layer PLGA mesh (n ¼ 3 for each
group). A: Graphic presentation showing maximum tensile strength (MPs) at break (failure). B: Graphic presentation of maximum tensile strain
(mm) at failure. C: Graphic presentation of Young’s modulus at failure. D: Graphic presentation of maximum load (N) at break. [Color figure can
be viewed in the online issue, which is available at wileyonlinelibrary.com.]
10 SALEM ET AL. PLGA-COLLAGEN/FIBRIN COMPOSITE FOR REGENERATION OF URINARY BLADDER WALL

biomaterial will be suitable in vivo; therefore, further stud-ies will be needed to verify this.
REFERENCES1. Atala A. Tissue engineering in the genitourinary system. In: Atala
A, Moony D, editors. Tissue Engineering. Boston: Birkhauser
Press; 1997. p 49–150.
2. Eberli D, Susaeta R, Yoo JJ, Atala A. Tunica repair with a cellular
bladder matrix maintains corporal tissue function. Int J Impot Res
2007;19:602–609.
3. Ziats NP, Miller KM, Anderson JM. In vitro and in vivo interaction
of cells with biomaterials. Biomaterials 1988;9:5–13.
4. Yoo JJ, Meng J, Oberpenning F, Atala A. Bladder augmentation
using allogenic bladder submucosa seeded with cells. Urology
1998;51:221–225.
5. Walter JR, Meyer RF. Sessile macrophages forming clear endo-
thelium like membrane of successful keratoprosthesis. Trans Am
Ophthalmol Soc 1985;82:187–202.
6. 2001 Annual Report of the U.S Organ Procurement and transplan-
tation Network and the scientific registry for transplant recipient:
Transplant Data 1991–2000. Department of health and human
services, Health Resources and services administration, office of
special programs, Division of transplantation, Md; united network
for organ sharing, Richmond, Va; University renal research and
education Association, Ann Arbor, MI. Available at: www.optn.
org/data/annual report asp. Accessed December 9, 2002.
7. Alberts B, Bray D, Lewis J, Raff, M., Roberts, K., Watson, J.D. The
extracellular matrix of animal. In: Alberts B, Bray D, Lewis J, Raff
M, Roberts K, Watson JD, editors. Molecular Biology of the Cell.
New York: Garland; 1994. p 971–995.
8. Kim BS, Mooney DJ. Development of biocompatible synthetic
extracellular matrices for tissue engineering. Trends Biotechnol
1998;16:224–230.
9. Kim BS, Mooney DJ. Engineering smooth muscle tissue with a
predefined structure. J Biomed Mater Res 1998;41:322–332.
10. Atala A. Bioengineered tissues for urogenital repair in children.
Pediatr Res 2008;63:569–575.
11. Pariente JL, Kim BS, Atala A. In vitro biocombatibility assessment
of naturally-derived and synthetic biomaterials using normal
human urothelial cells. J Biomed Mater Res 2001;55:33–39.
12. Astete, CE, Sabliov, CM. Synthesis and characterization of PLGA
nanoparticles. J Biomat Sci-Polym E 2006;17:247–289.
13. Osathanon T, Linnes ML, Rajachar RM, Ratner BD, Somerman
MJ, Giachelli CM. Nanofibrous fibrin-based scaffolds for bone tis-
sue engineering. Biomaterials 2008;29:4091–4099.
14. Ruszymah BHI. Autologous human fibrin as the biomaterial for
tissue engineering. Med J Malaysia 2004;59(Suppl. B):30–31.
15. Ahmed TA, Dare EV, Hincke M. Fibrin: a versatile scaffold for tis-
sue engineering applications. Tissue Eng Part B Rev 2008;14:
199–215.
16. David Heeley (Understanding Pressure and Pressure Measure-
ment) Free scale Semiconductor AN1573 Rev 1, 05/2005.
JOURNAL OF BIOMEDICAL MATERIALS RESEARCH A | MONTH 2013 VOL 00A, ISSUE 00 11
ORIGINAL ARTICLE
Related Documents











