Physician’s Orders for Life-Sustaining Treatment Sharmon Figenshaw, ARNP, Bruce Smith, MD Washington POLST Task Force Co-Chairs

POLST Skills Development - Sharmon Figenshaw and Bruce Smith
Aug 14, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Physician’s Orders for Life-Sustaining TreatmentSharmon Figenshaw, ARNP, Bruce Smith, MDWashington POLST Task Force Co-Chairs

POLST Update for Professionals

POLST Update for Professionals
What is POLST?
“Portable” medical orders for treatment decisions, including end-of-life care; conforms to medical standards of care.
Defines patient preference for health care options based on current physical/medical condition.
POLST can translate an advance directive into physician’s orders or reflect change in preferences based on change in medical condition.
POLST Update for Professionals
What is POLST?
Patient & provider shared decision-making model: Brings together patient goals/values and practitioner-guided consideration of current medical condition.
Translates patient wishes into orders that can be followed by EMS (and hopefully other bedside providers).
Options include range of care from full code/full measures to DNR/comfort.
Power and portability
REMEMBER: Conversations for goals of care come first!

POLST Update for Professionals
Philosophy of POLST
Individuals have the right to make their own health care decisions. These rights include:
Making decisions about accepting or refusing life-sustaining treatment.
Having their decisions honored by health care providers. Comfort care while having wishes honored.
POLST allows people to “opt out” of the default “full code” of standard emergency/medical care.
POLST Update for Professionals
POLST: Who Should Have One?
Who should have POLST form: Persons with advanced or chronic illness, or frailty. Condition for which resuscitation is inappropriate including when
survival is unlikely. Anyone who “you wouldn’t be surprised” if they were to die
within the next year.
Good clinical documentation Especially when surrogates are decision makers.

POLST Update for Professionals
POLST: Who Could Have One?
Anyone choosing: To limit medical treatments Do Not Resuscitate/No Code/Allow Natural Death Advanced age >80 years old (without mental instability)
This covers our healthy seniors who want to make sure that they do not receive unwanted CPR or burdensome hospitalizations.*
*There is some debate about this in religious circles.
It is important to remember: POLST is always voluntary!
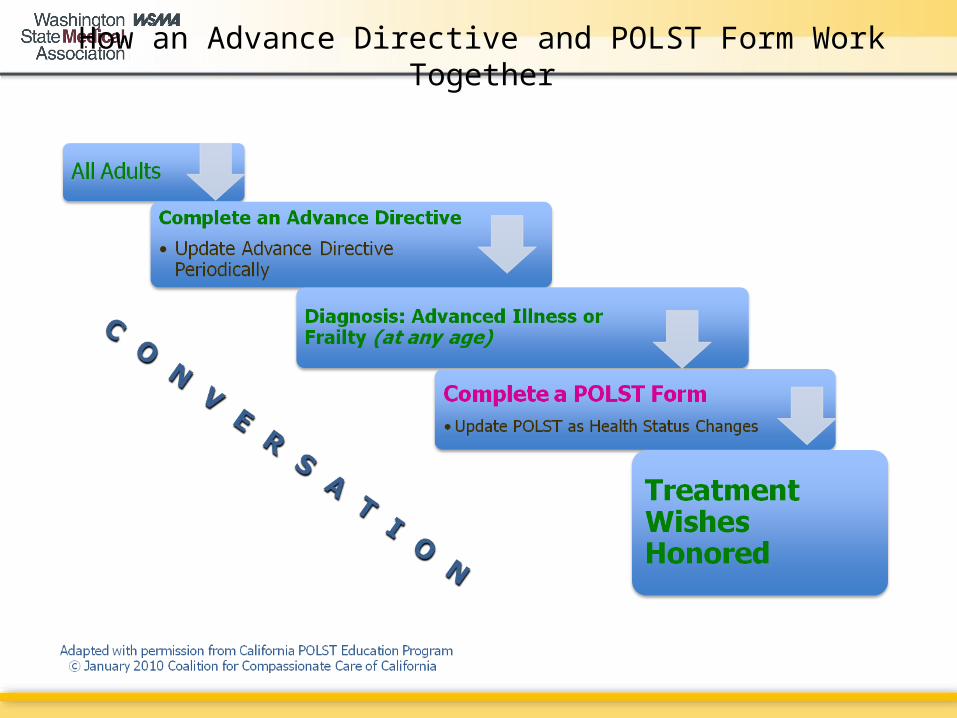
How an Advance Directive and POLST Form Work Together
POLST Update for Professionals
Establish Goals of Care
Shared decision-making based on the patient’s values and goals in light of their current medical condition:
“What do you understand about your condition?” Informed consent: Patients need information about risks
and benefits of life-saving measures! “What are you hoping for? What might you be afraid of?” Initiate in the hospital by the time of discharge if not
already done by primary care provider. “How would you like to live your life?”

How POLST Works
The POLST Form (Front)
Medical Condition/Patient Goals
A simple description of medical condition A direct statement of the patient/family’s goals in their own
words is one of the most important pieces of information we can gather.
This may guide care decisions when nothing else can.
Agency Info/Sticker
Write in, or place sticker here for an agency.

The POLST Form (Front)
Part A: Code Status
Instructions regarding Cardiopulmonary Resuscitation (CPR): Includes EMS
Patient has no pulse and is not breathing
CPR/Resuscitate Do Not Attempt Resuscitation (DNAR) / Allow Natural
Death (AND) Comfort measures will always be provided

The POLST Form (Front)
Part B: Medical Interventions
Patient/resident has pulse and/respirations
Comfort Measures Only: Medication by any route, positioning, wound care. Other measures to relieve pain and suffering. Use oxygen, oral suction and manual treatment of airway
obstruction as needed for comfort. Patient prefers no transfer: EMS contact medical control to
determine if transport indicated.

The POLST Form (Front)
Part B: Medical Interventions
Patient/resident has pulse and/respirations
Limited Additional Interventions: Includes care listed above in comfort care. Medical treatment, IV fluids and cardiac monitor as indicated.
Do not use intubation or mechanical ventilation. Transfer if indicated, avoid ICU if possible.

The POLST Form (Front)
Part B: Medical Interventions
Patient/resident has pulse and/respirations
Full Treatment and Interventions: All care in both sections above plus intubation and
cardioversion. Transfer to hospital if indicated. Includes intensive care.
Additional Orders: (e.g. dialysis, etc.) Use this section to state specific therapies, like dialysis and
blood transfusions and the goals or time limits for these.

The POLST Form (Front)
Signatures
Statement of Intent: The signatures below verify that these orders are consistent
with the patient’s medical condition, known preferences and best known information. If signed by a surrogate, the patient must be decisionally incapacitated and the person signing is the legal surrogate.
Indicate who was involved in decision-making: Patient Parent of minor Guardian with Health Care Authority Spouse (or Domestic Partner. Indicate this) Health Care Agent (DPOAHC)
The POLST Form (Front)
Signatures
Patient signature always preferred. If patient present but surrogate signing, note presence and
agreement of patient.
Surrogates for signing (Washington state): Guardian DPOA Spouse/Registered domestic partner Adult children Parent Adult sibling
Beyond that, there is no regulatory guidance. Consult ethics. Use team-decision making model with any family available.

The POLST Form (Front)
Signatures
Physician (MD, DO) or Advanced Care Practitioner (ARNP or PA-C) must sign.
Verbal orders are acceptable with follow-up signature by physician, ARNP or PA in accordance with existing policies.
Signatures attest to the informed consent process having occurred.
Different health care settings designate/train different personnel for this purpose.

The POLST Form (Back)
Part D
Additional Patient Preferences (Optional) This includes antibiotics and nutrition therapy options. Formerly Parts C & D on front of form. Meant to guide therapies in non-emergent situations. Patient and provider signatures testify that conversation has
taken place.

The POLST Form (Back)
Part D: Antibiotic Therapy
Antibiotics for infection: whatever the choice, notify physician of new infection
No antibiotics: use other measures to relieve symptoms. Determine use or limitation of antibiotics when infection occurs,
with comfort as goal. Use antibiotics with the goal of prolonging life.

The POLST Form (Back)
Part D: Medically Assisted Nutrition
Artificially Administered Nutrition by parenteral or enteral route
No artificial nutrition by tube. Trial period of artificial nutrition by tube. (Goal: Write in how
long, till what event or goal is reached.) Long-term artificial nutrition by tube.
Always offer food and liquids by mouth if feasible. Additional orders:
Name specific goals of patient.
The POLST Form (Back)
Directions for Health Care Professionals
Completing POLST Must be completed by health care professional.
Members of the health care team, RN, MSW, with proper training are well-positioned to have the appropriate conversations.
Should reflect the person’s current preferences and medical indications. Encourage completion of an advance directive. Advance directive should indicate congruent choices.
POLST must be signed by a physician (MD or DO)/ARNP/PA-C to be valid. Verbal orders are acceptable with follow-up signature per facility policy (see sample policies available at awphd.org or wsha.org).

The POLST Form (Back)
Directions for Health Care Professionals
Using POLST Any incomplete section of POLST implies full treatment for that
section. This POLST is effective across all settings including hospitals
until replaced by new physician’s orders. The health care professional should inquire about other
advance directives. In the event of a conflict, the most recently completed POLST form takes precedence.

The POLST Form (Back)
Directions for Health Care Professionals
Using POLST: SECTION A Patient has no pulse/no respirations No defibrillator (internal or external) should be used on a person
who has chosen “Do Not Attempt Resuscitation.”

The POLST Form (Back)
Directions for Health Care Professionals
Using POLST: SECTION B When comfort cannot be achieved in the current setting, the
person, including someone with “Comfort Measures Only,” should be transferred to a setting able to provide comfort (e.g., treatment of a hip fracture).
An IV medication to enhance comfort may be appropriate for a person who has chosen “Comfort Measures Only.”
Treatment of dehydration with IV fluids may prolong life. A person who desires IV fluids should indicate “Limited Additional Interventions” (or “Full Treatment” if more aggressive care desired).

The POLST Form (Back)
Directions for Health Care Professionals
Using POLST: SECTION D Oral food and fluids must be offered if feasible.

The POLST Form (Back)
Directions for Health Care Professionals
Reviewing POLST: Review when:1) The person is transferred from one care setting or care level to
another, or
2) There is a substantial change in the person’s health status, or
3) The person’s treatment preferences change. A person with capacity, or the surrogate of a person without
capacity, can void the form and request alternative treatment. FORM CAN BE VOIDED; changes require new POLST. (Desire for
CPR and full treatment do not require POLST.)

POLST Resources
POLST Resources
Washington State Medical Association Provides POLST forms and information. Order at www.wsma.org/polst or call (206) 441-9762. For general POLST information contact: Graham
Short, WSMA associate director of communications, (206) 329-6851, [email protected].
Washington POLST Task Force Co-Chairs: Bruce Smith, MD: [email protected]. Sharmon Figenshaw, ARNP: [email protected].
Related Documents











