Points, QOF & Points, QOF & QMAS QMAS VTS Awayday 10/11/04 VTS Awayday 10/11/04

Points, QOF & QMAS VTS Awayday 10/11/04. Relevant issues: Screen set up (we use INPS Vision but the principles should apply to any system) Screen set.
Dec 14, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Points, QOF & Points, QOF & QMASQMAS
VTS Awayday 10/11/04VTS Awayday 10/11/04

Relevant issues:Relevant issues:
Screen set up (we use INPS Vision but Screen set up (we use INPS Vision but the principles should apply to any the principles should apply to any system)system)
Read Codes Read Codes GuidelinesGuidelines Disease Registers Disease Registers CDM areas CDM areas Exception reportingException reporting Other data to collectOther data to collect Medication reviewsMedication reviews SmearsSmears Capturing Data/SummarizingCapturing Data/Summarizing Clinical AuditClinical Audit QOF and QMASQOF and QMAS

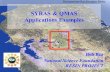
Screen showing NSMC view -Screen showing NSMC view -

GuidelinesGuidelines
Enable essential data to be Enable essential data to be collected consistentlycollected consistently
Make sure correct Read Codes Make sure correct Read Codes are being usedare being used
Have been customised by INPS Have been customised by INPS and NSMCand NSMC
Care & commitment needed to Care & commitment needed to use correctlyuse correctly







Read Codes - 1Read Codes - 1
We have a Read Code formulary We have a Read Code formulary for every patient contact – clinical for every patient contact – clinical & administrative& administrative
We aim to use codes that are We aim to use codes that are straightforward and Contract-straightforward and Contract-compatiblecompatible
We use GuidelinesWe use Guidelines We use Keywords = mnemonicsWe use Keywords = mnemonics We use Holding Codes when We use Holding Codes when
diagnosis not yet establisheddiagnosis not yet established

Read Codes - 2Read Codes - 2 Use Read Code at top of hierarchy Use Read Code at top of hierarchy Do not use “H/o …” codesDo not use “H/o …” codes Do not use “PMH of …”Do not use “PMH of …” We use Priorities rather than We use Priorities rather than
ProblemsProblems Crucial to use the Recall facility and Crucial to use the Recall facility and
use it correctlyuse it correctly Avoid multiple entries of same Avoid multiple entries of same
diagnosis as “new diagnosis diagnosis as “new diagnosis actions” would then apply e.g. actions” would then apply e.g. anginaangina

Disease RegistersDisease Registers Crucial for the new ContractCrucial for the new Contract Need to ensure right patients are in Need to ensure right patients are in
the right registerthe right register No need to use the set “registers” in No need to use the set “registers” in
Vision now - Asthma, CHD, DM, HT – Vision now - Asthma, CHD, DM, HT – becausebecause
Virtual registers best i.e. the Virtual registers best i.e. the diagnostic codediagnostic code
Need to clean registers – to correct Need to clean registers – to correct inaccuracies and to determine inaccuracies and to determine prevalenceprevalence
System needed for capturing new System needed for capturing new patients/diagnosespatients/diagnoses

AsthmaAsthma
Those prescribed asthma related Those prescribed asthma related drugs in past 12 months with Read drugs in past 12 months with Read Code H33Code H33
Could use active and inactive Could use active and inactive register register
What we are doing - if no longer What we are doing - if no longer suffering or history unclear use suffering or history unclear use “Asthma resolved” - will remove “Asthma resolved” - will remove from disease registerfrom disease register
Need to validate with those with Need to validate with those with respiratory drugs but no diagnosisrespiratory drugs but no diagnosis

CancerCancer Cancers excluding non-melanotic Cancers excluding non-melanotic
skin cancers diagnosed after 1/4/03skin cancers diagnosed after 1/4/03 Virtual register fine if coding correctVirtual register fine if coding correct Using appropriate Read Codes in B Using appropriate Read Codes in B
hierarchy – put Neoplasm as well as hierarchy – put Neoplasm as well as diagnosis diagnosis
Care over event type – has to show Care over event type – has to show as “First ever”as “First ever”
Cancer review is straightforwardCancer review is straightforward

COPDCOPD Register made by appropriate Read Register made by appropriate Read
Code = H32Code = H32 Confirmation of diagnosis since April Confirmation of diagnosis since April
20032003 More accurate diagnosis of existing More accurate diagnosis of existing
patientspatients Sorting out COPD from asthmaSorting out COPD from asthma Finding patients – those on Finding patients – those on
anticholinergics, oxygen, frequent oral anticholinergics, oxygen, frequent oral steroids, asthmatic smokers over 50steroids, asthmatic smokers over 50

CHDCHD Most points available in this area Most points available in this area
of the new contractof the new contract G3 hierarchy (except CABG)G3 hierarchy (except CABG) ““Referral to cardiology” will bypass Referral to cardiology” will bypass
some actions and is a useful codesome actions and is a useful code Validating -Validating -
Search Read CodesSearch Read Codes Search drugs e.g. nitrates, beta Search drugs e.g. nitrates, beta
blockers, statins, ACE inhibitorsblockers, statins, ACE inhibitors Lots of cleaning of data has been Lots of cleaning of data has been
donedone

LVFLVF May be different from patients on CHD May be different from patients on CHD
register but may need CHD in additionregister but may need CHD in addition Read Code = G58Read Code = G58 Validate by looking for patients with Validate by looking for patients with LVF, LVF,
CCF, Heart Failure and CCF, Heart Failure and EchocardiographyEchocardiography
Drug searchesDrug searches Review those with diagnosis without Review those with diagnosis without
echocardiogramechocardiogram

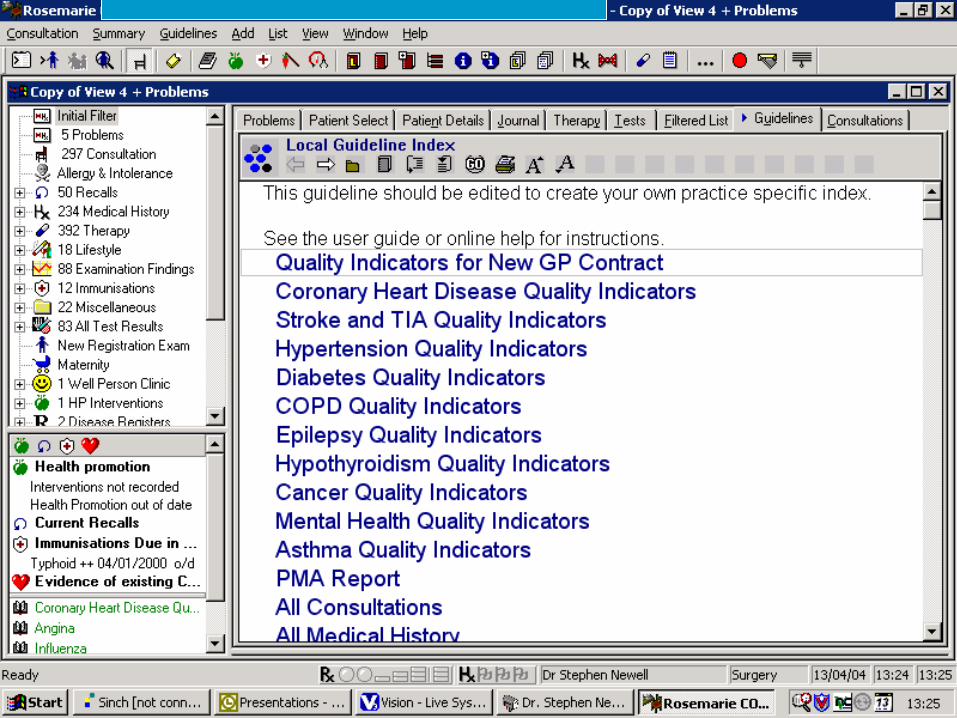
DiabetesDiabetes
Read Code C10Read Code C10 Double code Type 1 (C10E) and Double code Type 1 (C10E) and
2 (C10F)2 (C10F) Drug searching on oral Drug searching on oral
medication and blood testing medication and blood testing reagentsreagents
Contract does not require Contract does not require confirmation of diagnosisconfirmation of diagnosis
At risk pre-diabetics need to be At risk pre-diabetics need to be in systemin system

EpilepsyEpilepsy
Those currently receiving Those currently receiving treatment (in last year) treatment (in last year) age 16 and overage 16 and over
Read Code F25Read Code F25 Need to validate as there Need to validate as there
will be some patients will be some patients taking some anti-epileptic taking some anti-epileptic drugs for other reasonsdrugs for other reasons

HypertensionHypertension Large numbers and therefore Large numbers and therefore
workloadworkload
Read Code G2Read Code G2
Looking for patients – those Looking for patients – those known & with Read codes for known & with Read codes for HT, drug searches, those with HT, drug searches, those with last BP > 150/90 not on Rx (up last BP > 150/90 not on Rx (up to 50% of over 60s)to 50% of over 60s)
HypothyroidismHypothyroidism
Those on levothyroxine with Those on levothyroxine with recorded diagnosis of recorded diagnosis of hypothyroidismhypothyroidism
Read Code C03 & C04Read Code C03 & C04
New contract requires TSH in New contract requires TSH in last 15/12last 15/12

Stroke & TIAStroke & TIA
Read Codes = TIA (G65), Read Codes = TIA (G65), Haemorrhagic Stroke (G61), Non Haemorrhagic Stroke (G61), Non Haemorrhagic Stroke (G64), Haemorrhagic Stroke (G64), Stroke NOS (G66)Stroke NOS (G66)
Validation needed because new Validation needed because new Contract distinguishes these Contract distinguishes these types of strokes & suggests types of strokes & suggests different actionsdifferent actions
Mental HealthMental Health
Entry onto register is Entry onto register is discretionarydiscretionary
Suggestions are those with Suggestions are those with psychosis e.g. schizophrenia & psychosis e.g. schizophrenia & bipolar disorder, those on a care bipolar disorder, those on a care programme or with complex care programme or with complex care packagespackages
Read Code 9H8 = On severe Read Code 9H8 = On severe mental illness registermental illness register
Remember Lithium monitoringRemember Lithium monitoring


Exception Reporting - 1Exception Reporting - 1
From whole domain or individual From whole domain or individual indicatorsindicators
What could be exception coded?What could be exception coded? Refusal to attend after 3 invitationsRefusal to attend after 3 invitations New patients or recently diagnosedNew patients or recently diagnosed Not clinically appropriate e.g. perhaps age, Not clinically appropriate e.g. perhaps age,
frailtyfrailty Informed dissentInformed dissent Unable to tolerate RxUnable to tolerate Rx Maximum medicationMaximum medication Another supervening conditionAnother supervening condition

Exception Reporting - 2Exception Reporting - 2
• Two levels for each clinical category:Two levels for each clinical category:
- - High levelHigh level (Read Codes 9h) – applied to all (Read Codes 9h) – applied to all Indicators Indicators
within category – need to be noted annually within category – need to be noted annually
- Patient unsuitable- Patient unsuitable - Informed dissent- Informed dissent
- - Indicator levelIndicator level – applied to individual – applied to individual Indicators onlyIndicators only - Maximum tolerated - Maximum tolerated medication dosagemedication dosage
- Drug allergy / - Drug allergy / contraindicationcontraindication
- Patient recently registered- Patient recently registered- Patient recently diagnosed- Patient recently diagnosed- Procedure / treatment - Procedure / treatment
declineddeclined

Exception Reporting - 3Exception Reporting - 3
• Duration of exceptions: Duration of exceptions:
- - Expiring exceptionsExpiring exceptions – annual, as above – annual, as above- - Persisting exceptionsPersisting exceptions e.g. drug allergies e.g. drug allergies
- - Aspirin etc contraindicated Aspirin etc contraindicated – needs – needs contraindications contraindications or allergies to ALL THREE drug types or allergies to ALL THREE drug types annuallyannually
- - ACE / A2 contraindicatedACE / A2 contraindicated – needs – needs contraindications or contraindications or allergies to BOTH drug types annuallyallergies to BOTH drug types annually
- Buttons within Guidelines to enter all these- Buttons within Guidelines to enter all these

Exception Reporting - 4Exception Reporting - 4
• Who should be excepted at the Who should be excepted at the High level –patient unsuitable High level –patient unsuitable and informed dissent?and informed dissent?
• No national or local guidanceNo national or local guidance
• Practice needs to take a view Practice needs to take a view about thisabout this
• May be appropriate to write a May be appropriate to write a practice protocol practice protocol

Other data to collectOther data to collect
BP every 5 years age BP every 5 years age 45+45+
Smoking status age Smoking status age 15-7515-75
Medication ReviewMedication Review
Needs to be recorded in previous Needs to be recorded in previous 15 months for those on 4 or 15 months for those on 4 or more repeat medicationsmore repeat medications
All patients on repeat medication All patients on repeat medication – needs to be in SDA in Vision– needs to be in SDA in Vision
Additional specific disease area Additional specific disease area medication reviews - buttonsmedication reviews - buttons
Smears – what is needed?Smears – what is needed?
Performance – age 25-64 every 3-5yrsPerformance – age 25-64 every 3-5yrs
Policies – e.g. one crucial area is in Policies – e.g. one crucial area is in the area of dissent – needs 3 the area of dissent – needs 3 invitations, must sign a disclaimer, invitations, must sign a disclaimer, must be given the opportunity to must be given the opportunity to dissent again next time rounddissent again next time round
AuditAudit

Capturing data / SummarizingCapturing data / Summarizing
Agreement in-house about CodesAgreement in-house about Codes Issues around new diagnosesIssues around new diagnoses Protocol for data entryProtocol for data entry External sources - hospitalsExternal sources - hospitals New patient checksNew patient checks Community nurses?Community nurses? Nursing homes?Nursing homes? Housebound?Housebound?

Remember non-clinical protocolsRemember non-clinical protocols
Points to be earned in the new Points to be earned in the new contract for having practice protocolscontract for having practice protocols
Some are clinical and need clinical Some are clinical and need clinical input e.g. Infection Control, Smear input e.g. Infection Control, Smear TakingTaking
Some are not primarily clinical e.g. Some are not primarily clinical e.g. Health and Safety, Complaints Health and Safety, Complaints ProcedureProcedure
Potentially a lot of work for the Potentially a lot of work for the practice managerpractice manager
Very tricky without some practice Very tricky without some practice managementmanagement

How can we make all this work?How can we make all this work?
Involve everyone - who all have Involve everyone - who all have to be committed to the processto be committed to the process
Agree what is importantAgree what is important Work together on policiesWork together on policies Use different skills within the Use different skills within the
teamteam Value what they contributeValue what they contribute ? Financial incentives – e.g. ? Financial incentives – e.g.
with set-up moneywith set-up money

Some of the North Street teamSome of the North Street team

What is QOF? - 1What is QOF? - 1
•Quality Outcomes Quality Outcomes FrameworkFramework
• The new Contract The new Contract “scoring” system“scoring” system
•Clinical and administrative Clinical and administrative componentscomponents
•Clinical criteria translate to Clinical criteria translate to clickable buttons within clickable buttons within GuidelinesGuidelines

What is QOF? - 2What is QOF? - 2
•Points achieved against 146 Points achieved against 146 criteria will affect practice criteria will affect practice payment in 2005payment in 2005
•QOF points will not simply be QOF points will not simply be paidpaid
• ““Voluntary” assessment Voluntary” assessment provides validation and opens provides validation and opens way for paymentway for payment
•Stated aims of assessment are Stated aims of assessment are to be formative, helpful & to be formative, helpful & developmentaldevelopmental
How points are assessed - 1How points are assessed - 1
• Clinical Audit will measure points Clinical Audit will measure points – –
correct Read Codes requiredcorrect Read Codes required
• Practices will need to report on Practices will need to report on QOF QOF
monthlymonthly
• “ “The bit in the middle” reports The bit in the middle” reports the the
achievement – this is QMASachievement – this is QMAS

So what is QMAS?So what is QMAS?
• Quality Management and Analysis Quality Management and Analysis SystemSystem
• The software that will interrogate The software that will interrogate
practices’ (compatible) IT systemspractices’ (compatible) IT systems• Can be run from now, fully live by Can be run from now, fully live by
3/053/05• Once registered, can get current Once registered, can get current
level of points or forecast level for level of points or forecast level for 31/3/0531/3/05

How points are assessed - 2How points are assessed - 2
• Year-end report used for payment Year-end report used for payment calculationcalculation
• Prevalence will be taken into accountPrevalence will be taken into account
• Between 2 and 18 Quality Indicators for Between 2 and 18 Quality Indicators for 11 Clinical Categories, 1 Organisational 11 Clinical Categories, 1 Organisational Category, 1 Additional Services Category, 1 Additional Services categorycategory
• Validated by QOF assessment visitValidated by QOF assessment visit

How points are assessed – 3How points are assessed – 3
• First Indicator in each clinical category – the First Indicator in each clinical category – the diagnostic code - is Virtual Disease Register – diagnostic code - is Virtual Disease Register – no need to use Disease Registers nowno need to use Disease Registers now
• Other Indicators are scored against different Other Indicators are scored against different target populations i.e. Denominatorstarget populations i.e. Denominators
• Denominators and Indicators take Exceptions Denominators and Indicators take Exceptions into accountinto account
• Exceptions do not affect Virtual Disease Exceptions do not affect Virtual Disease RegistersRegisters

QOF Assessment Visits - 1QOF Assessment Visits - 1
•Start in 10/04 – NSMC will be Start in 10/04 – NSMC will be visited in 1/05visited in 1/05
•QOF visiting teams consist of 1 QOF visiting teams consist of 1 PCT manager, 1 clinician (a GP PCT manager, 1 clinician (a GP although some nurses have although some nurses have been trained), 1 lay memberbeen trained), 1 lay member
•Havering PCT planning 2.5 Havering PCT planning 2.5 hours – how realistic? 4 may be hours – how realistic? 4 may be more likelymore likely

QOF Assessment Visits – 2QOF Assessment Visits – 2
• Visiting team will have a practice Visiting team will have a practice profile, a timetable for the visit and profile, a timetable for the visit and access to current level of QOF points access to current level of QOF points
• May have other information e.g. May have other information e.g. prescribing dataprescribing data
• Will look at QOF criteria – not clear at Will look at QOF criteria – not clear at present how many of the 146 but could present how many of the 146 but could be all or anybe all or any
• Stated aim is to be light-touch, high Stated aim is to be light-touch, high trust, trust,
low bureaucracylow bureaucracy
QOF Assessment Visits - 3QOF Assessment Visits - 3
• Will interview representative team Will interview representative team from practice & will discuss from practice & will discuss aspects other than points e.g. aspects other than points e.g. patient experiencepatient experience
• Not a full quality review but will Not a full quality review but will seek to validate QOF pointsseek to validate QOF points
• There may be other agendae There may be other agendae including a change agendaincluding a change agenda

(Some of the) Unresolved issues (Some of the) Unresolved issues
• Information for visits & amount of Information for visits & amount of preparation by practices preparation by practices
• Time for visits & disruption to Time for visits & disruption to normal activitiesnormal activities
• Confidentiality of clinical dataConfidentiality of clinical data• Formative vs. summative usageFormative vs. summative usage• Possible aims of PCT vs. aims of Possible aims of PCT vs. aims of
practicespractices• What happens to all the “other” What happens to all the “other”
data?data?• Preparation & workload of visiting Preparation & workload of visiting
teamsteams• Membership and payment of Membership and payment of
teamsteams


Data for NSMC on Data for NSMC on QMAS as at 9/04QMAS as at 9/04

Clinical domains - PointsClinical domains - Points
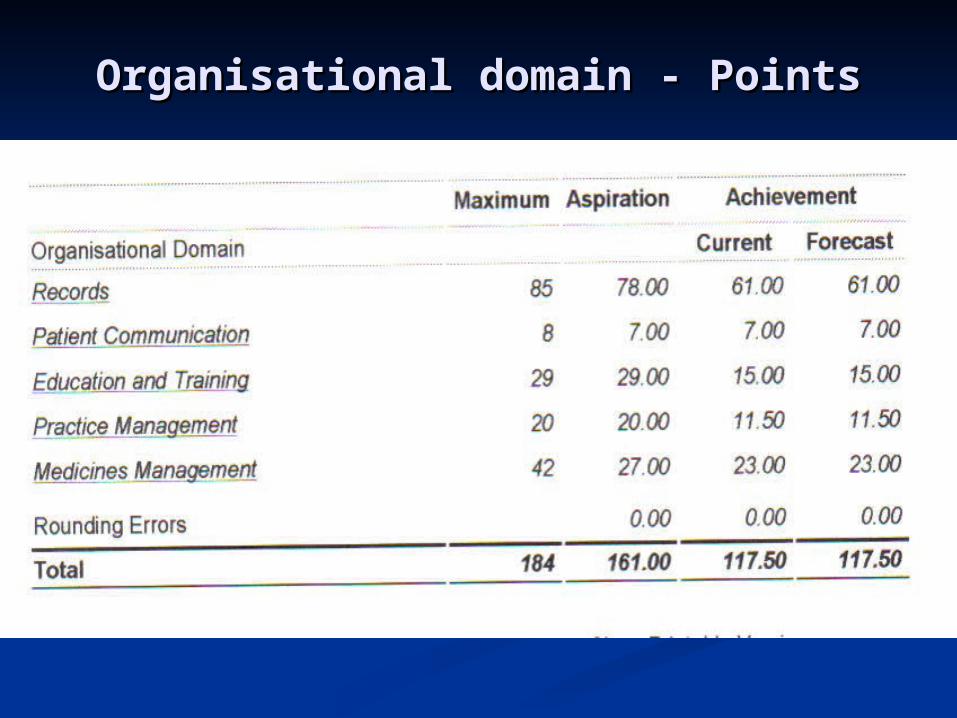
Organisational domain - PointsOrganisational domain - Points

Total PointsTotal Points
Related Documents