Chest Case # 10

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Chest Case #10

34 YOM with no chronic medical problems presents with the complaint of 2 days of right-sided chest pain that began while walking. The pain is worse with deep inspiration and radiates into the right aspect of his neck and into his “shoulderblade”. He denies previous similar episodes; no associated nausea/vomiting, cough/congestion, fevers/chills, no diaphoresis/dyspnea. He has been otherwise well free of illness or injury. At presenation he is awake/alert and in no distress. He has a 20 pk/yr hx of tobacco use.
History and Physical T 98.7 P 80 BP 126/84 O2
99% Gen: WDWN, NAD CV: RRR, no m/r/g Pulm: Lungs CTA , chest
wall is free of injury with no reproducible pain
bilaterally. Abd: s/nt/nd, Ext: No cy/cl/ed – pain is
not worsened with manipulation of right arm

Ches
t X
-Ray

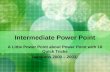
Diagnosis: Pneumothorax
The visceral pleura at the edge of the collapsed lung is barely visible. It can be identified by looking for a fine line that parallels the curve of the lateral chest wall

Oxygen Treatment decisions are based on the clinical status of the patient,
the size of the pneumothorax (large or small), and the presence of underlying lung disease
Outpatient Patients with no underlying lung disease who have only mild
symptoms and normal vital signs in the setting of a first/small primary spontaneous pneumothorax can be managed with observation alone
If this is the patient's first primary spontaneous pneumothorax and the patient is reliable and able to return promptly to the ED if symptoms worsen, the patient may be discharged home and scheduled for a return visit with repeat radiography in 12–48 hours. Prior to discharge, it is recommended that the patient be observed in the ED for 3–6 hours and a repeat chest film be obtained to assure that the pneumothorax size has not increased.
ED Management

Inpatient Patients with a large pneumothorax require catheter or
chest tube placement to re-expand the lung. Patients with a second spontaneous pneumothorax
should be hospitalized and referred to a surgeon. Whenever tension pneumothorax is suspected, catheter
aspiration should be performed immediately Patients with a traumatic pneumothorax will require
admission for observation and evaluation/management of associated injuries .
ED Management

Size Three approximations of the size of pneumothorax can be distinguished:
small, medium, and large . A small pneumothorax is confined to the apex of the thorax and a thin rim around the lung (less than 1 or 2 cm) . A medium pneumothorax occupies up to one-half of the thoracic diameter. With a large pneumothorax, the lung is completely or nearly completely collapsed
Classification A primary spontaneous pneumothorax occurs in patients without
underlying lung disease A secondary spontaneous pneumothorax is associated with an
underlying pulmonary disorder. Such disorders include chronic obstructive pulmonary disease (COPD), cysts or cavities due to necrotizing pneumonia (staphylococcus aureus), malignancies, tuberculosis, or pneumocystis pneumonia, and interstitial lung diseases such as sarcoidosis, collagen vascular diseases, pneumoconiosis, or idiopathic pulmonary fibrosis.
A traumatic pneumothorax is associated with blunt or penetrating trauma to the thoracic cavity.
Pearls

Presentation Chest pain is the primary symptom, occurring in 90% of cases. Dyspnea is present in 80% of patients. Severe dyspnea can also occur with a relatively small pneumothorax
in patients who have significant underlying lung disease such as COPD or in the setting of tension pneumothorax.
Diagnosis Bedside ultrasonography can be used to rapidly detect a
pneumothorax and can be incorporated into the FAST exam . The radiograph should be taken with the patient in an upright
position. When the patient is supine, a pneumothorax collects anteriorly and may be impossible to detect
In patients whose radiographic findings are equivocal, an expiratory radiograph can make a small pneumothorax more conspicuous. Expiration compresses the lung and increases the relative size of the pneumothorax
Pearls

Additional Images
“small” left apical pneumothorax

Additional Images: Pneumothorax
Supine chest radiograph of a neonate illustrates the deep sulcus sign with abnormal deepening and lucency of the left lateral costophrenic angle (asterisk).
Deep sulcus sign.

Additional Images: Pneumothorax
Large right-sided pneumothorax
Moderate right-sided pneumothorax

Additional Images: Pneumothorax
Tension pneumothorax – The radiograph that should never be taken
After tube thoracostomy

Additional Images
Questionable findings of a pneumothorax (inspiratory view)
Same pneumothorax visualized with repeat film during expiration
Related Documents