Pleomorphic Adenoma of the Soft Palate Authors: Kishore C Shetty*, Vadisha Bhat**, Shubha P Bhat*** *Professor of ENT, **Associate Professor of ENT, ***Assistant Professor of Pathology Institution: K S Hegde Medical Academy, Deralakatte, Mangalore- 575018, Karnataka, India Corresponding Author: Dr Vadisha Bhat Associate Professor of ENT K S Hegde Medical Academy Deralakatte, Mangalore 575018 Karnataka, India Email: [email protected] Abstract: The majority of minor salivary gland tumors are malignant. Pleomorphic adenoma is a benign neoplasm which is commonly encountered in parotid and other major salivary glands. Occasionally, they may develop in minor salivary glands of the palate. We report a case of pleomorphic adenoma of minor salivary glands in the soft palate. Introduction: Salivary gland tumors account for less than 3% of the head and neck tumors. 1 Mixed tumor of the salivary gland, or pleomorphic adenoma, is a benign tumor arising mainly in the major salivary glands (65%), especially in the parotid and, less frequently, in accessory salivary glands (35%). 2 A small minority (8%) are located in the oral cavity, neck and nasal cavity. 3 The most common site for minor salivary gland pleomorphic adenoma is the palate, though it can also occur in the upper lip, cheek, floor of the mouth, larynx and trachea. 4 Intraoral pleomorphic adenoma appears as a slowly growing, painless mass, usually in the fourth or fifth decade. 5 It has its highest incidence between 30 to 60 years of age with female predominance. 6 Fine-needle aspiration cytology (FNAC) and incisional biopsy can aid as diagnostic tools. 1,7,8 Surgical resection is the treatment of choice. 6 Pleomorphic adenoma generally does not recur after adequate surgical excision. 8 The potential risk of malignant transformation of the pleomorphic adenoma is about 6%. The risk is increased by delay in diagnosis. 2 We report a case of pleomorphic adenoma of the soft palate in an elderly lady, which was treated surgically. Case Report:

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Pleomorphic Adenoma of the Soft Palate
Authors: Kishore C Shetty*, Vadisha Bhat**, Shubha P Bhat***
*Professor of ENT, **Associate Professor of ENT, ***Assistant Professor of Pathology
Institution: K S Hegde Medical Academy, Deralakatte, Mangalore- 575018, Karnataka, India
Corresponding Author:
Dr Vadisha Bhat
Associate Professor of ENT
K S Hegde Medical Academy
Deralakatte, Mangalore 575018
Karnataka, India
Email: [email protected]
Abstract:
The majority of minor salivary gland tumors are malignant. Pleomorphic adenoma is a benign
neoplasm which is commonly encountered in parotid and other major salivary glands.
Occasionally, they may develop in minor salivary glands of the palate. We report a case of
pleomorphic adenoma of minor salivary glands in the soft palate.
Introduction:
Salivary gland tumors account for less than 3% of the head and neck tumors.1 Mixed tumor of
the salivary gland, or pleomorphic adenoma, is a benign tumor arising mainly in the major
salivary glands (65%), especially in the parotid and, less frequently, in accessory salivary glands
(35%).2 A small minority (8%) are located in the oral cavity, neck and nasal cavity.
3 The most
common site for minor salivary gland pleomorphic adenoma is the palate, though it can also
occur in the upper lip, cheek, floor of the mouth, larynx and trachea.4 Intraoral pleomorphic
adenoma appears as a slowly growing, painless mass, usually in the fourth or fifth decade.5 It
has its highest incidence between 30 to 60 years of age with female predominance.6 Fine-needle
aspiration cytology (FNAC) and incisional biopsy can aid as diagnostic tools.1,7,8
Surgical
resection is the treatment of choice.6 Pleomorphic adenoma generally does not recur after
adequate surgical excision.8 The potential risk of malignant transformation of the pleomorphic
adenoma is about 6%. The risk is increased by delay in diagnosis.2 We report a case of
pleomorphic adenoma of the soft palate in an elderly lady, which was treated surgically.
Case Report:
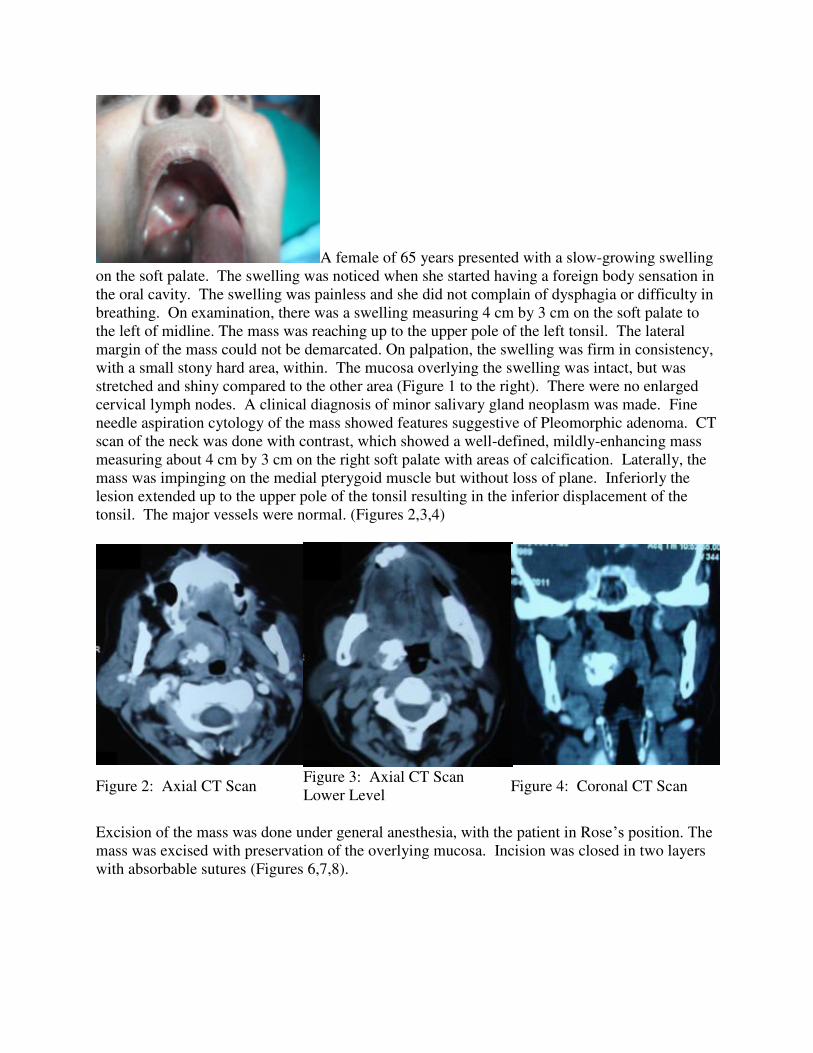
A female of 65 years presented with a slow-growing swelling
on the soft palate. The swelling was noticed when she started having a foreign body sensation in
the oral cavity. The swelling was painless and she did not complain of dysphagia or difficulty in
breathing. On examination, there was a swelling measuring 4 cm by 3 cm on the soft palate to
the left of midline. The mass was reaching up to the upper pole of the left tonsil. The lateral
margin of the mass could not be demarcated. On palpation, the swelling was firm in consistency,
with a small stony hard area, within. The mucosa overlying the swelling was intact, but was
stretched and shiny compared to the other area (Figure 1 to the right). There were no enlarged
cervical lymph nodes. A clinical diagnosis of minor salivary gland neoplasm was made. Fine
needle aspiration cytology of the mass showed features suggestive of Pleomorphic adenoma. CT
scan of the neck was done with contrast, which showed a well-defined, mildly-enhancing mass
measuring about 4 cm by 3 cm on the right soft palate with areas of calcification. Laterally, the
mass was impinging on the medial pterygoid muscle but without loss of plane. Inferiorly the
lesion extended up to the upper pole of the tonsil resulting in the inferior displacement of the
tonsil. The major vessels were normal. (Figures 2,3,4)
Figure 2: Axial CT Scan Figure 3: Axial CT Scan
Lower Level Figure 4: Coronal CT Scan
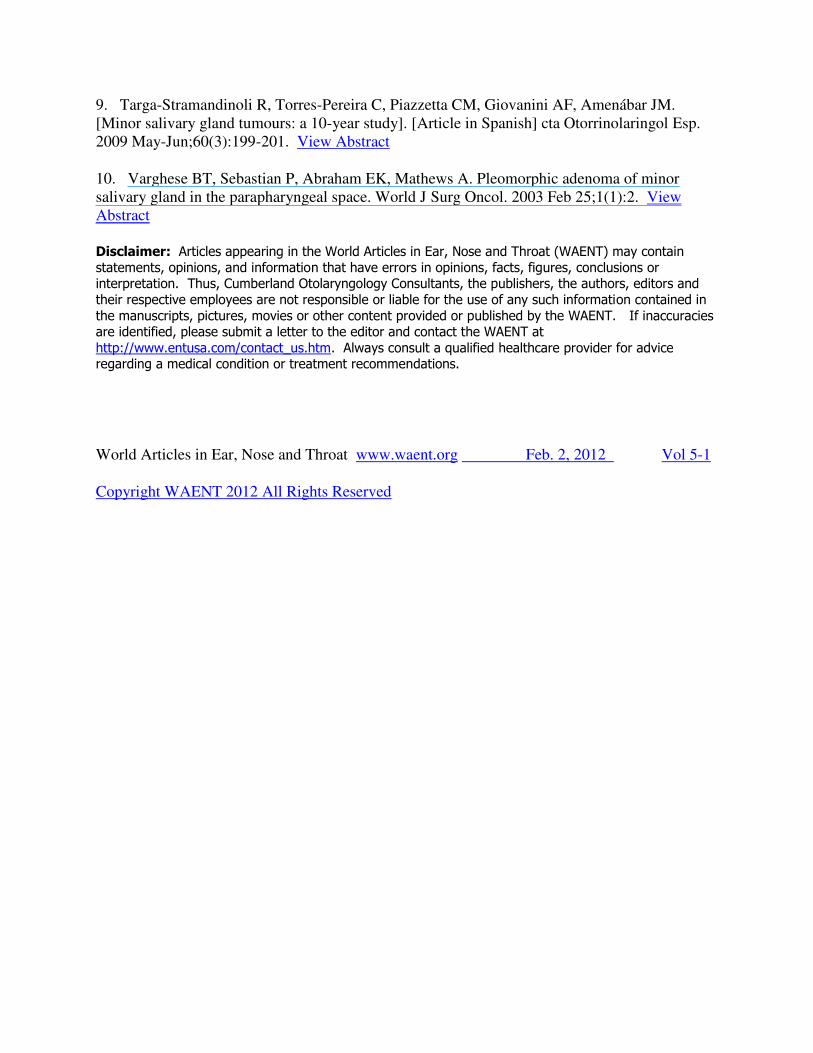
Excision of the mass was done under general anesthesia, with the patient in Rose’s position. The mass was excised with preservation of the overlying mucosa. Incision was closed in two layers
with absorbable sutures (Figures 6,7,8).
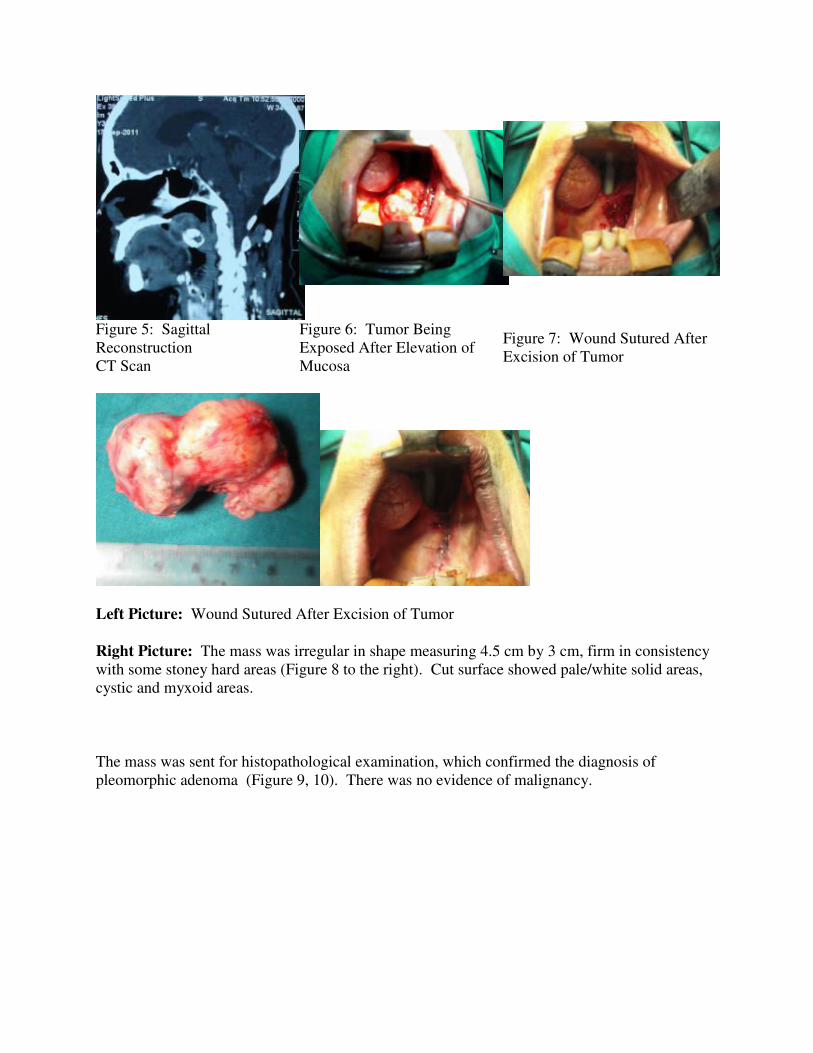
Figure 5: Sagittal
Reconstruction
CT Scan
Figure 6: Tumor Being
Exposed After Elevation of
Mucosa
Figure 7: Wound Sutured After
Excision of Tumor
Left Picture: Wound Sutured After Excision of Tumor
Right Picture: The mass was irregular in shape measuring 4.5 cm by 3 cm, firm in consistency
with some stoney hard areas (Figure 8 to the right). Cut surface showed pale/white solid areas,
cystic and myxoid areas.
The mass was sent for histopathological examination, which confirmed the diagnosis of
pleomorphic adenoma (Figure 9, 10). There was no evidence of malignancy.

Figure 9: Histopathology: Pleomorphic
Adenoma
Figure 10: Histopathology: Pleomorphic
Adenoma
High Magnification
The postoperative period was uneventful and the patient was allowed to take clear liquids after 4
hours, liquid and semisolids on the next day. She started taking regular food after 2 days and
was discharged on the third day. She is under regular follow up and there is no evidence of
recurrence or any other lesion in a 5 month follow-up period.
Discussion:
Neoplasms of the minor salivary glands are rare and represent 9%-23% of glandular tumors.9
The majority (40%-50%) of them are malignant,7 with only 18% being benign. Pleomorphic
adenoma is the commonest benign minor salivary gland tumor. It is commonly found in females
than in males, with a male/female ratio varying from 1:1.4 to 1:1.76. The palate being the most
common site, followed by lip, buccal mucosa, floor of mouth, tongue, tonsil, pharynx, retromolar
area and nasal cavity.10
It presents as a painless slow-growing mass.6 Our patient was a 65-year-
old female who presented with a slow-growing, painless swelling on the soft palate for one-year
duration. Differential diagnoses for this case include: Odontogenic and nonodontogenic cysts,
soft-tissue tumors, lymphomas and salivary gland tumors.8 The diagnosis of pleomorphic
adenoma is established on the basis of history, physical examination, cytology and
histopathology. CT scan and MRI can provide information of the location, size and extension of
tumor to surrounding superficial and deep structures.5
Fine-needle aspiration cytology and
incisional biopsy can aid in the diagnosis. The treatment of choice for pleomorphic adenoma in
the minor salivary gland is wide local excision with the removal of periosteum or bone if they
are involved.8
Our patient underwent excision of the mass in total with preservation of the
overlying mucosa. Microscopically, the intraoral pleomorphic adenoma lacks a well-defined
fibrous capsule. The tumor tissue is composed of epithelial and a mesenchymal component. The
epithelial component consists of tumor cells arranged in ducts, cords and sheets. Ducts are lined
by inner cuboidal and outer spindle-shaped myoepithelial cells. The mesenchymal area is
present in the hypocellular area and is composed of stellate and spindle-shaped myoepithelial
cells dispersed in a chondromyxoid matrix.2,5

Immunohistochemical stains prove positive for various cytokeratins, S100 protein, glial fibrillary
acid protein, vimentin, and smooth muscle actin. This describes the “mixed” nature of the tumor, both, stromal and epithelial lined.
2
Recurrences are not frequent. Simple enucleation of this tumor is believed to lead to a high local
recurrence rate and should be avoided. Rupture of the capsule, or tumor spillage, is also believed
to increase the risk of recurrence, so meticulous dissection is necessary.8 Rare cases of a
metastatic nature and malignant transformation have been reported.4
Conclusion:
The majority of minor salivary gland tumors of the soft palate are malignant in nature.
Nonulcerated, firm, dome shaped, nontender palatal masses of long duration should raise a high
index of suspicion for pleomorphic adenoma. CT scan with contrast and Fine Needle Aspiration
Cytology will aid in diagnosis. Complete extramucosal excision of the mass by a transoral route
provides cure.
References:
1. Dhanuthai K, Sappayatosok K, Kongin K. Pleomorphic adenoma of the palate in a child: a
case report. Med Oral Patol Oral Cir Bucal. 2009 Feb 1;14(2):E73-5. View Abstract
2. Sciandra D, Dispenza F, Porcasi R, Kulamarva G, Saraniti C. Pleomorphic adenoma of the
lateral nasal wall: case report. Acta Otorhinolaryngol Ital. 2008 Jun;28(3):150-3. View Abstract
3. Gana P, Masterson L. Pleomorphic adenoma of the nasal septum: a case report. J Med Case
Reports. 2008 Nov 17;2:349. View Abstract
4. Bae CH, Kim YD, Song SY. Benign pleomorphic adenoma of the soft palate metastasizing to
the sphenoid sinus. Clin Exp Otorhinolaryngol. 2010 Sep;3(3):172-5. Epub 2010 Sep 17. View
Abstract
5. Kaur S, Thami GP, Nagarkar NM. Pleomorphic adenoma of the hard palate. Indian J
Dermatol Venerol Leprol 2003 69:74-5. View Article
6. Noghreyan A, Gatot A, Maor E, Fliss DM. latal pleomorphic adenoma in a child. J Laryngol
Otol. 1995 Apr;109(4):343-5. View Abstract
7. Thakur JS, Mohindroo NK, Mohindroo S, Sharma DR, Thakur A. Pleomorphic adenoma of
minor salivary gland with therapeutic misadventure: a rare case report. BMC Ear Nose Throat
Disord. 2010 Jan 8;10:2. View Abstract
8. Srinivas SD. Pleomorphic adenoma of the palate: A case report. Journal of the Indian Dental
Association 2011 5(4):557-58. View Article
9. Targa-Stramandinoli R, Torres-Pereira C, Piazzetta CM, Giovanini AF, Amenábar JM.
[Minor salivary gland tumours: a 10-year study]. [Article in Spanish] cta Otorrinolaringol Esp.
2009 May-Jun;60(3):199-201. View Abstract
10. Varghese BT, Sebastian P, Abraham EK, Mathews A. Pleomorphic adenoma of minor
salivary gland in the parapharyngeal space. World J Surg Oncol. 2003 Feb 25;1(1):2. View
Abstract
Disclaimer: Articles appearing in the World Articles in Ear, Nose and Throat (WAENT) may contain
statements, opinions, and information that have errors in opinions, facts, figures, conclusions or interpretation. Thus, Cumberland Otolaryngology Consultants, the publishers, the authors, editors and
their respective employees are not responsible or liable for the use of any such information contained in
the manuscripts, pictures, movies or other content provided or published by the WAENT. If inaccuracies are identified, please submit a letter to the editor and contact the WAENT at
http://www.entusa.com/contact_us.htm. Always consult a qualified healthcare provider for advice regarding a medical condition or treatment recommendations.
World Articles in Ear, Nose and Throat www.waent.org Feb. 2, 2012 Vol 5-1
Copyright WAENT 2012 All Rights Reserved
Related Documents








![Ductal Adenocarcinoma Ex Pleomorphic Adenoma of the ... · lesions [2, 5]. Carcinoma ex pleomorphic adenoma (Ca ex PA) is a rare transformation of a benign primary PA to a malignant](https://static.cupdf.com/doc/110x72/60bd399bb7acaf776f026cd1/ductal-adenocarcinoma-ex-pleomorphic-adenoma-of-the-lesions-2-5-carcinoma.jpg)

