PLANNING OF Cardiac catheterization laboratory DR PRIYANKA SATALKAR, PGDHM&HC, 4 TH SEM

Planning of - cathlab
Nov 08, 2014
cathlab plannning
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PLANNING OF Cardiac catheterization laboratory
DR PRIYANKA SATALKAR, PGDHM&HC, 4TH SEM
Catheterization Laboratory
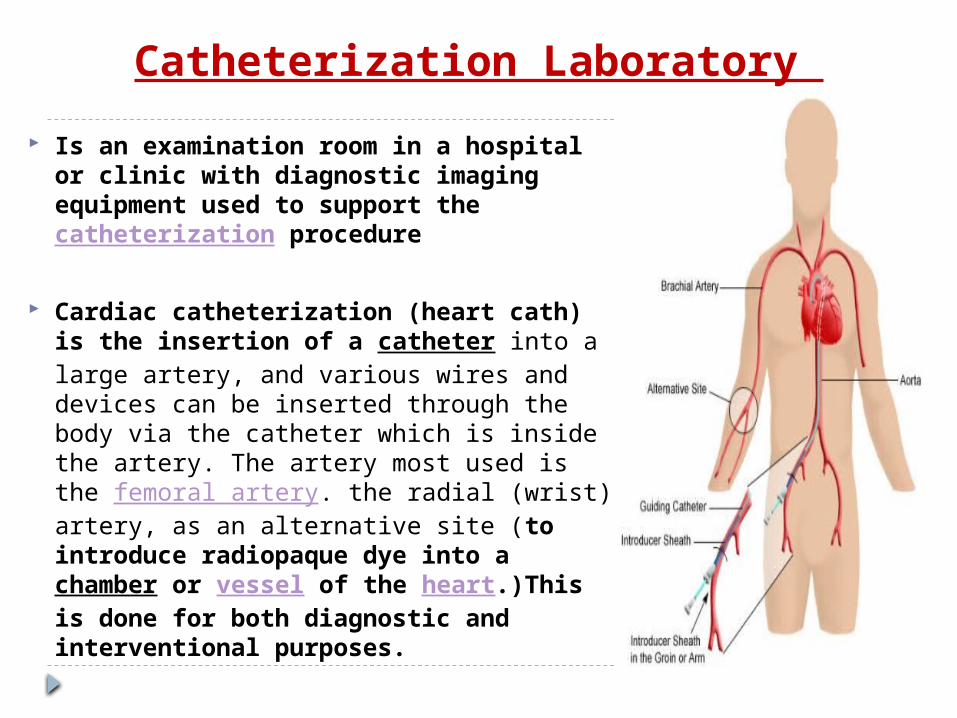
Is an examination room in a hospital or clinic with diagnostic imaging equipment used to support the catheterization procedure
Cardiac catheterization (heart cath) is the insertion of a catheter into a large artery, and various wires and devices can be inserted through the body via the catheter which is inside the artery. The artery most used is the femoral artery. the radial (wrist) artery, as an alternative site (to introduce radiopaque dye into a chamber or vessel of the heart.)This is done for both diagnostic and interventional purposes.

The cath department is an important part of any hospital for several reasons.
First, coronary catheterization one of the most common interventional procedures practiced, which leads to high volumes and high revenues.
Second, the procedures conducted in a cath lab are far less invasive than those performed in the operating room, which means that patients can often be treated as outpatients, which results in reduced costs for the hospital

Services and Procedures: The cath lab provides a number of invasive procedures
that enable a cardiologist to check the heart and coronary arteries, measure blood flow and inter-cardiac pressure, assess how well the heart valves work, and check for structural defects.
The procedures performed are categorized as either diagnostic or interventional.
Diagnostic procedures help the physician to determine the cause of a patient’s condition, while
interventional procedures attempt to cure the condition

Diagnostic Coronary Angiography – Insertion of a catheter into heart to deliver
contrast. Electrophysiology Testing – Tests electrical conduction within the heart. Cardiac Shunt Detections – Blood flow analysis to identify a shunt. Structure Assessment and Confirmation – Verify structure of heart and
veins. Intravascular Ultrasounds – Determine plaque buildup.
Interventional Cardiac Angioplasty – Balloon insertion to open an obstructed artery. Cardiac Stent Placement – Placement of stent to keep artery open. Ablations – Removal of faulty electrical pathways. Atherectomy/Rotablation – Removal of material blocking an artery. Closure of Congenital Heart Defects – Correct blood flow pattern. Treatment of Stenotic Heart Valves – Correct blood flow amount. Thrombectomy - Removal of blood clots
Other Pacemaker Implantations – Implant device to regulate beating of the
heart. Internal Cardiac Defibrillator Implants – Implant device to jolt heart in case
of cardiac arrest.
planning considerations
Planning a catheterization laboratory depends on various factors like the, the need for interventional procedures, types of angiography procedures, building size, and the budget available for equipment and running costs.
Usually the suppliers of the angio-equipment will play an integral part in planning and developing a catheterisation
laboratory.
Cath lab planning is also based on projected volumes for inpatient and outpatient volumes.
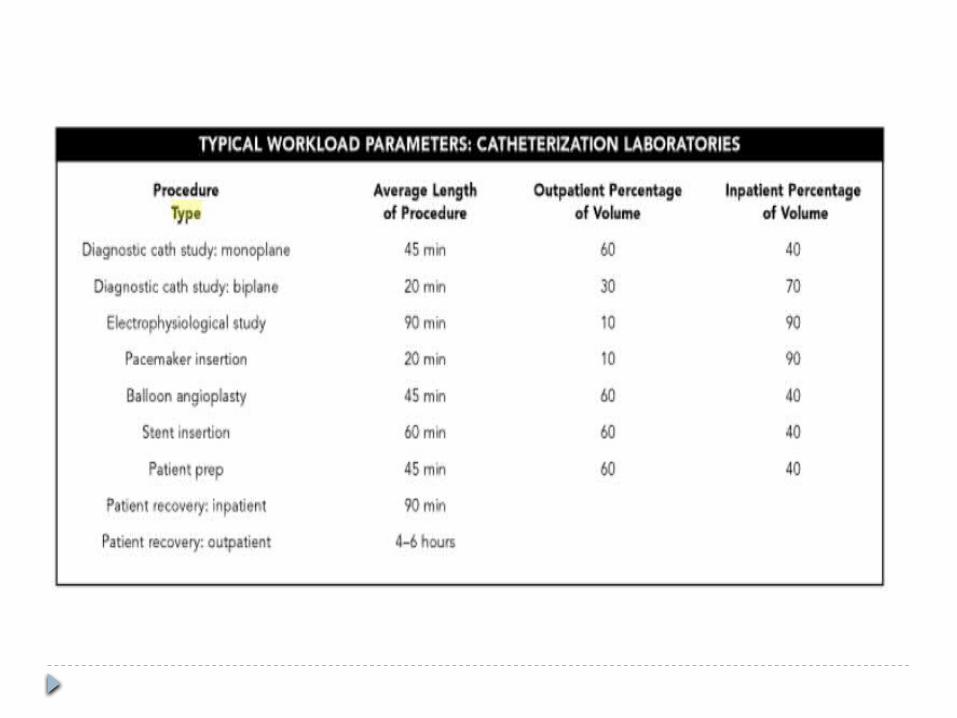
Workload aggregated into average procedure time and distribution between inpatient and outpatient volume

Catheterization Laboratory Market – India Indian market for cath labs is expected to show steady
growth in coming years, providing strong opportunities to present and potential players to earn high revenues and increase their profits
With sales of 135 units, the market for cath labs is estimated at Rs. 240 crore in 2010.
The premium segment (fixed) cath labs continued to dominate the market in 2010, with sales contribution of Rs. 191.4 crore and unit-wise sales of 87 numbers. The market for value segment (mobile and fixed) cath labs, with an average selling price at Rs. 1 crore remained almost stagnant at 48 units.
Philips and Siemens continued to dominate the cath labs market with a combined market share of 74 percent. GE Healthcare is an aggressive player in this market. Other players include Allengers, Toshiba, Shimadzu, Masters Medical, and Komega Impex.
The market for interventional cardiology products in India is growing in line with a dramatic rise in cardiovascular disease among increasingly affluent and urbanized Indians with a resulting surge in demand for high quality cardiac care.
Established interventional cardiology procedures - diagnostic angiography, PTCA, and coronary stenting - are performed widely in India, across medium-sized and larger hospitals equipped with catheterization laboratories.
Innovative products such as drug-eluting coronary stents, rapid exchange balloon catheters, and novel vascular closure devices are providing new market opportunities
New drug eluting stent designs are expected to assist physicians in treating vulnerable plaque, thus accelerating market acceptance of the products.
Key demand drivers include a surge in disease incidence due to affluence and lifestyle changes, resulting increase in demand for diagnosis and treatment, and infrastructure expansion driven partly by a fast-growing cluster of corporate hospitals, among other factors.

Drivers: Increasing cardiovascular diseases Improving technology Improving hospital infrastructure Changing demographic structure. Growing medical tourism Increasing healthcare spending.
Technological Trends: Rotational Angiography Biplane Digital Subtraction Angiography 3D Rotational Angiography Hybrid Cath Lab / OR Remote Magnetic Swing Lab Stent Boost Robotic-Operated Systems
Location of the cath lab
In the radiology Dept. preferred to be in the corner
Easy access to the OPD/IPD patients
Close to the cardiology dept
Lift should be near to shift the patient to O.T. in case of emergency

A Physician (normally either a senior cardiologist or interventional radiologist)
-An Anesthetist
-Junior Radiologist
-A Cardiac Physiologist
-A Nurse
-A Radiology technician

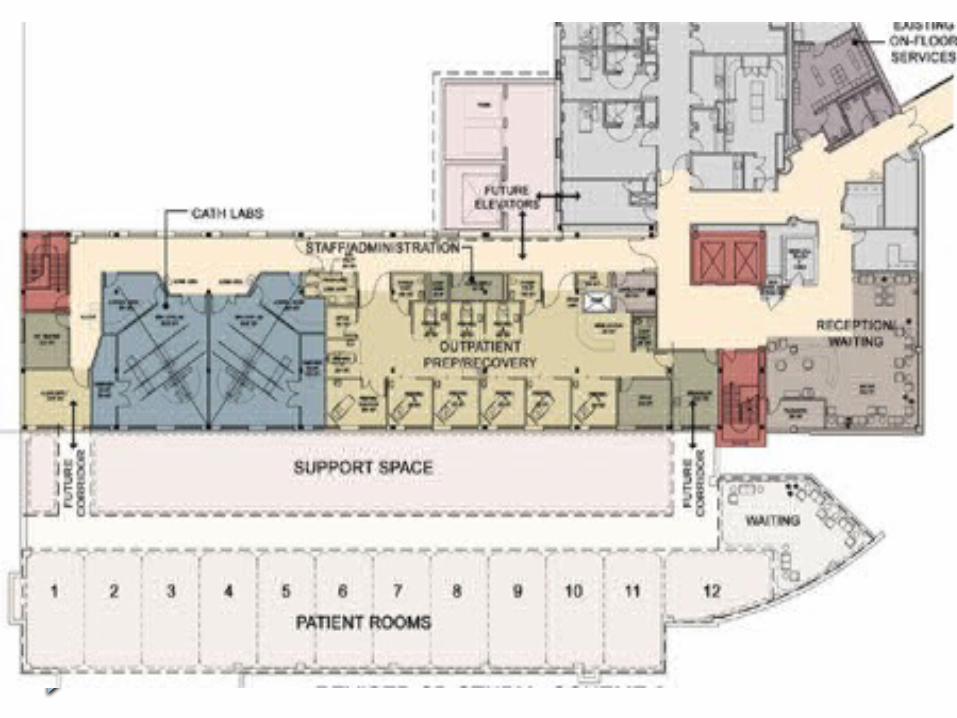
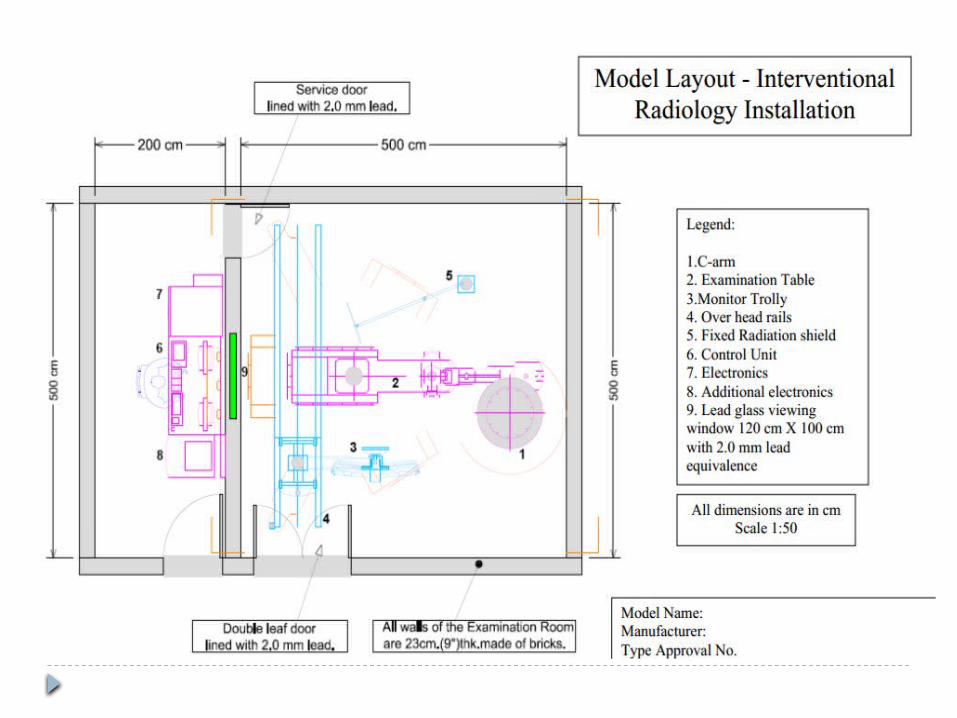
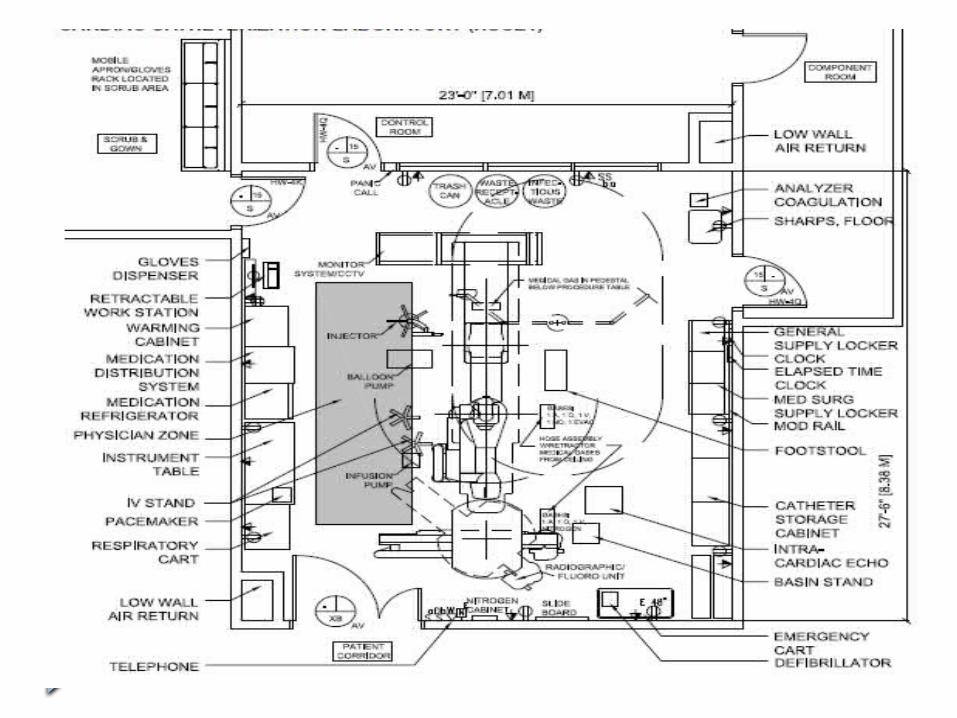
Layout of cath lab


Space considerations in
planning Cardiac catheterization
laboratory


Procedure Room

Procedure Room The catheterization laboratory procedure
room should provide ample space for the equipment, in-room storage and movement of the patient into and out of the room via stretcher or patient bed. It is generally recommended that 500–600 square feet for the procedure area and 150– 200 square feet should be allotted to the control room.
Items for consideration in the procedure room include in-room storage cabinetry, standing-height counter space, a clinical sink, Likewise, at least one phone line into the procedure room itself is recommended.

If your lab is performing permanent pacemaker insertions or some of the more advanced percutaneous aortic repair procedures in this setting, ventilation and airflow must meet operating room standards.
The vascular laboratory should be equipped with excellent lighting. Lights should automatically switch off during fluoroscopy.
A small ceiling-mounted light is practical during difficult catheterisation procedures, i.e. when brachial artery entrance is used or when putting up IV canulas in patients with ‘difficult’ veins, i.e. children and cancer patients.
A theatre light should be suspended from the ceiling in such a way that there is no interference with the C-arms but close enough so that the angiographic table can be used as an operating table

Gas fittings should also be available to connect to an anaesthetic machine.
Enough power sockets are essential to connect different apparatus in the vascular theatre, i.e. ECG machine, ultrasound, heating equipment for contrast agents, etc. Some of these power sockets should also be connected to an emergency power supply in case of power loss.
Control Room
Control Room
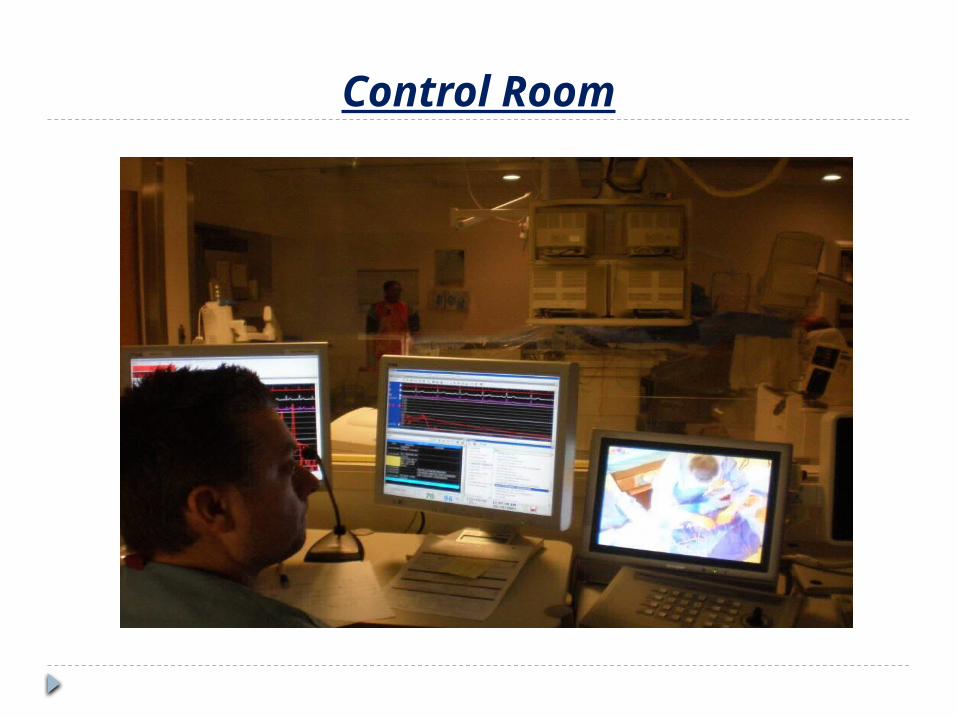
The control room is another critical space. The room should be of adequate size to allow staff movement and required equipment (such as imaging control panels and hemodynamic monitors).
The control room floor should also be elevated by one or two steps to allow for full visualization of the field. An elevated floor also allows for computer and monitor cables to be run underneath.
The window for viewing into the procedure room should be as large as the space will allow, making sure that the viewing space is also low enough to allow visualization of the table from the elevated angle.

The preferred position for the control room in relation to the procedure room is at the “foot” end of the patient table. This allows for full viewing of the field, regardless of whether the physician works on the left or right side of the table.
From this foot position, the staff member in the control room has a view that is unrestricted by the backs of staff members working at the table or overhead hanging monitors, as is sometimes the case in control rooms positioned on one side of the procedure room.
a minimum of one phone line should also be installed in the control room. Multiple phone lines may be beneficial when dictation of reports is provided by phone access.
Patient Holding area

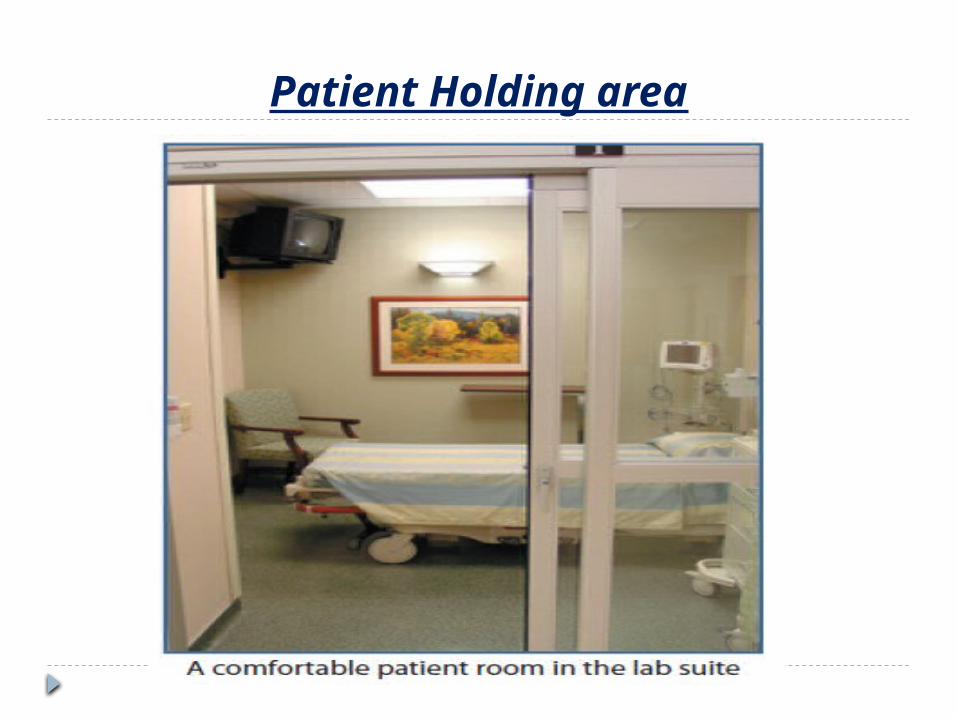
Patient Holding area Many cardiac catheterization laboratories provide only
Stage I recovery (immediate post-procedure vital sign and anaesthesia recovery monitoring) in the holding area. If that is the case, a minimum of two beds or stretchers per procedure room is needed to facilitate patient flow in and out of the lab.
Some facilities admit outpatients directly to the cath lab area and recover Stage I and Stage II (ongoing monitoring for the remainder of the recovery period) patients as well as discharge outpatients from this area.
In the latter case, the number of beds required should be based on average daily case volumes and should allow for efficient patient flow, eliminating “waiting for a bed” situations.

The holding area should contain a small “nurses station” area to allow for documentation, computer terminals, a scheduling secretary, etc. Patient bays should preferably be walled cubicles with breakaway doors. This will allow for increased patient privacy.
The patient bays should also be equipped with gases, call light, monitors (including EKG, NIBP and SaO2), stretchers and a small storage cart or cabinet. Phone lines should also be installed at the nurses station area.

Family Waiting Area.
The final area to be discussed is the need for a family waiting area that is in close proximity to the procedure room. This allows the family to feel they are close to the patient and makes it easier for the cardiologist to visit the family post procedure to explain procedure results and treatment options.

Dirty utility room Most procedures use fully disposable supplies. For this
reason the dirty utility room should be equipped
Storage for equipment and consumables The example layout of the catheter laboratory is based
on the assumption that a core supply of consumables and equipment, including catheters, is held within the room. The example schedules include an additional space allowance for a central stock of consumables and less frequently used bulky equipment, such as intravascular ultrasound (IVUS) machines, rota blation, robotic equipment, pressure wire workstations, balloon pumps and implantable devices. Facilities for charging syringes and IV pumps should be provided.

Equipment Selection for the
Cardiac catheterization laboratory

Innova cathlab with spin from GE

Imaging equipment is the core of the cardiac catheterization laboratory. An early decision regarding this equipment and its features is essential to allow the architects to best utilize its specifications in the procedure room layout.
The specifications are also needed to determine power supply needs as well as air cooling considerations.
The facility should select equipment based on program needs (current and long term) and physician/staff preferences, while still keeping in mind the hospital’s financial constraints.
There is a choice between a single-plane and dual-plane system. Numerous health-care facilities just do not have the patient volume to justify a separate cardiac lab and a separate vascular-imaging suite.
Dual-plane is the perfect solution. Dual-plane incorporates the use of two hyperspeed C-arms that share a common angiographic table. One C-arm can then be equipped with a 9-inch image intensifier that is optimal for cardiac imaging and the second C-arm is equipped with a 16- inch image intensifier that is optimal for complete vascular imaging.
The C-arms and imaging systems are interfaced with a dual-plane software computer program and the result is complete and total optimisation For each physician specialist.
The dual-plane C-arms can both be ceiling- suspended or one ceiling-suspended and the other floor-mounted.
Different C-arms are on the market with capabilities of producing 3D images with a recording speed of up to 30 frames per second.
C-arms equipped with flat-panel detectors (FPDs) are replacing the image-intensifying screens. The FPDs have many advantages over the image intensifier:
• Uniform brightness across image• Increased resolution and no distortion• High dynamic range• Better technique control & One powerful PC to
review MR, CT, and vascular 3D images. Radiation exposure is lower with FPD
products. This is very important as any decrease in radiation makes a procedure safer for both Screening personnel and patients.

Table options. Make sure that the table weight capacity is as high as possible. Previous tables accommodated 325–350 pounds, which created some limitations for patient imaging. Most vendors will offer a table with a capacity of up to 450 pound.
To allow for stretcher positioning, the table should also be able to rotate laterally a minimum of ninety degrees. Tables may be floor or ceiling-mounted and are generally selected as to what is available from a particular vendor (not all offer ceiling-mounted tables)And what is required by the room’s physical limitations.
Standard equipment options that should be packaged with the imaging equipment include:
• Table accessories such as arm boards and extenders
• Overhead and table lead shielding;• Overhead surgical light;• The power injector.
While most of these items can be purchased from other vendors, having a single vendor responsible for the installation of all equipment helps ensure everything will be mounted and interact properly
Additional equipment
A dedicated ultrasound machine is very useful in a vascular laboratory. It can be very helpful during difficult catheterisations and when one is performing various interventional procedures, i.e. kidney biopsies or liver carcinoma ablations. Additional equipment like a defibrillator, refrigerator, oven and light boxes should be available.
A contrast pump is essential in the vascular laboratory. The choice between a ceiling- or a floor-mounted unit depends on the size of the vascular laboratory and the type of equipment in the laboratory.
DICOM and PACS
Angiographic equipment is available with a DICOM network interface, meaning that the examination information leaving the system is already formatted according to the DICOM standards. This has two advantages:
(1) data equivalence is assured; and (2) any receiving system that supports this interface can be used for storing and reviewing images and data.
The DICOM system can be linked to the picture archiving and communications system (PACS). PACS digital images are stored in computer memory and can be retrieved in seconds. This reduces the time between exam and therapy, and has potential to impact on the overall length of hospital stay.
With digital imaging, doctors can immediately look up a patient’s new and past images on a PC, instead of waiting for films to be de-archived from a shelf and delivered. In addition, a doctor can electronically transmit a digital X-ray or other images to a hospital or clinic anywhere in the world.
The network system between DICOM-compatible machines and a PACS should have a 1-gigabyte cable for efficient transfer of data.

Changing to a digital system creates a filmless network with the following advantages:
• Elimination of film • Handling and storage costs reduced • Increased efficiency and exam throughput • Instant access to previous studies online • Optimised diagnostic review with true 1024x1024
images acquisition transfer and storage.
A voice-recognition system is a very practical program. This allows The radiologist to dictate directly onto a computer system. With the help of a radiological information system (RIS)/PACS and the hospital information system interface, this report can be immediately available on the hospital network. This method is especially helpful during after-hour procedures when secretaries are not on duty.
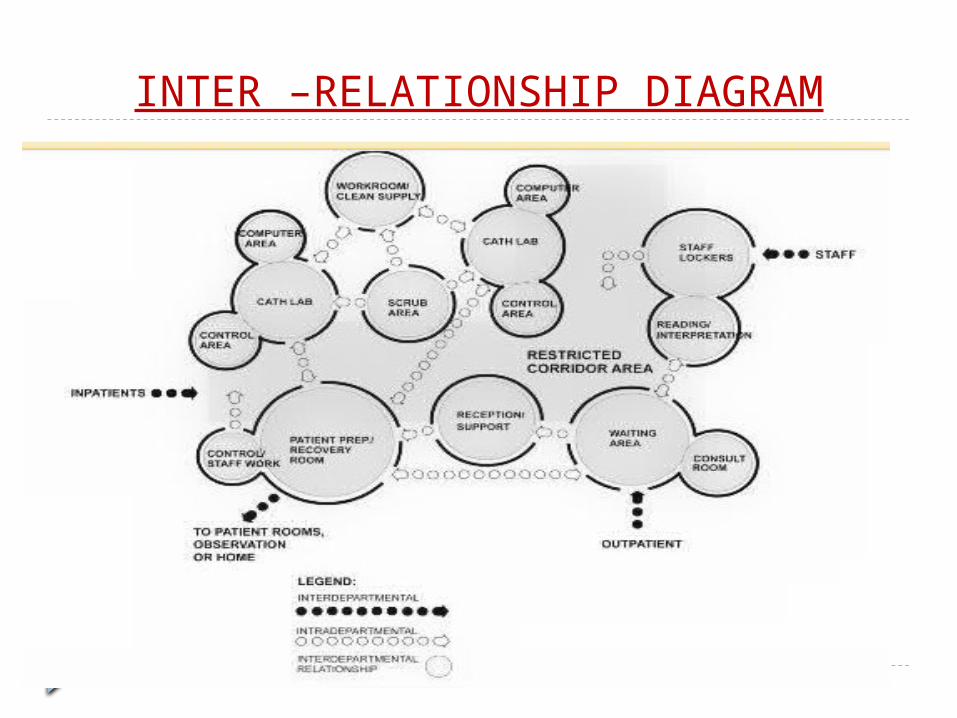
INTER –RELATIONSHIP DIAGRAM

Work Process Flow
While the Doctor and Nurses are focused on the blood flow and function of a patient’s heart, it is the flow of information, supplies, patients and available beds and equipment that determines how well the CathLab itself functions.

Patients originate either as admissions on the day of the procedure or as In-Patients from a Nursing
Unit
There is a Prep process that includes checking the latest lab tests, consent forms and other documentation
and administering some pre-procedure medications.
The Patient is then moved to a Holding area adjacent to the CathLab treatment rooms either in a
wheelchair or on a stretcher

Next stop is the operating table in a Procedure Room. Catheterization procedures can range in length from less than 30 minutes for diagnostics to an hour or more for interventional procedures.
Once off the table and onto a stretcher the Patient spends time in the Holding area. About 45 minutes is normally spent insuring that the
patient is stable and that the site of the catheter insertion is problem free.
Some patients move back to the original Prep area and are later discharged. Others will be moving to a
Nursing Unit to stay overnight, or longer in some cases

Process Mapping
The cath lab can be a stressful place to work. Days can be hectic and unpredictable. The staff is often struggling with balancing a schedule full of emergent cases and scheduled ones.
Some cases are often delayed, leaving patients hungry, anxious and nervous. Cardiologists dislike unpredictability and delay while hospital administrators are concerned with the time inefficiencies by these delays.
Hospitals are finding ways to improve patient flow in a timely manner, reduce the time to prepare the Cath lab for the next patient, and providing quality of care, which can all help reduce cost.


LABORATORY PERSONNEL—THE PRIMARY OPERATOR AND STAFF
-Observe proper hand hygiene procedures either by 1) Washing hands with conventional antiseptic-
containing soap or with waterless alcohol gels or foams.
2) Observe hand hygiene before & after palpating catheter
insertion sites, as well as before & after inserting, replacing, accessing, repairing, or dressing an intravascular catheter

Gowns and Shoe Covers:The operator should wear a scrub suit or other clean hospital uniforms, in the cardiac catheterization Laboratory.
-Shoe covers are not required solely to prevent a surgical site infection, but are required by Occupational Safety and Health Administration (OSHA) if soiling of shoes is likely, in order to reduce contamination of other areas of the healthcare facility (i.e., room-to-room transmission).
Caps, Masks, and Eye Protection:-Masks protect the operator’s mucous membranes from contamination by a patient’s body fluids,
-Caps and mask are standard attire in a surgical suite.
Use aseptic technique, including the use of a cap, mask, eye protection, sterile gown, and sterile gloves, for the insertion of catheters or for guide wire exchange.
-Maximum sterile barrier precaution is required during catheter insertion. The operator should ensure that assistants also use maximal barriers.
Ancillary Personnel• Technicians, nurses & any other personnel in the
cath lab should wear scrub suits, cap, mask, and gloves when they assist within the sterile field of the procedure.
• Visitors in the laboratory should wear either a scrub suit or other appropriate available attire over their street clothes & should remain an acceptable distance from the table as to avoid potential contamination of either the patient or the equipment
Vaccination:-Vaccination for hepatitis B virus should be strongly
considered, if not mandatory, for all operators and other personnel who work in the cath lab.
LABORATORY ENVIRONMENT
The lab should be completely cleaned once a day & spot-cleaned between each case.
-The floor should be wet-mopped or wiped if gross spillage is evident.
-Trash should be removed between each case.
CDC recommendations.:-After the last catheterization procedure of
the day or night, wet-vacuum or mop the lab room floors with a single
mop & an EPA-registered hospital disinfectant .
Fixed and Disposable Laboratory Equipment:Single-use disposable catheters are the current
standard for the majority of equipment utilized in the cath lab.
-Standard techniques should be employed to ensure proper sterilization of equipment that is reused.
-Equipment near the catheter entry site, which has the potential for blood contamination, such as foot switches, should be covered.
Disposal of Waste:-Blood-contaminated drapes, gowns, gloves, and
sponges should be discarded in special containers & labeled as healthcare waste.
-Needles and blades should be placed in puncture-proof containers.

Air Vents:The air vents should be cleaned at least
monthly.-The ventilation system should ideally
provide at least 15 air exchanges per hour of which at
least three should be fresh air . Maintenance of Environment:The doors to the cath lab should be kept
closed, except as necessary for passage of equipment, personnel, and the patient .
- After a catheterization procedure has started, the number of personnel allowed to leave or enter should be kept to a minimum

THANK YOU
Related Documents











