Good morning

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Good morning

PINDBORGS TUMOUR
SHRAVYA.M

CONTENTS • Introduction
• Definition
• Classification
• Pathogenesis
• Clinical Features
• Radiographic Features
• Pathology –Macroscopy
- Microscopy
• IHC Findings
• Differential Diagnosis
• Treatment
• Prognosis & Prediction
• Recent Studies
• References

Introduction Odontogenic tumours• Odontogenic tumors are uncommon lesions that are derived
from the specialized dental tissues.
• Classification of odontogenic tumors has developed over the last 150 years. The French physician Broca was the first to propose a classification of tumors originating from dental tissues.
• It was not until 1971, when a five-year collateral effort organized by the World Health Organization [WHO], resulted in the first consensus on taxonomy of odontogenic tumors.

• At the Editorial and Consensus Conference in Lyon, France in
July 2003, a final classification was developed based on the REICHART revised version of the 1992 WHO classification.
• WHO Blue book -2005

(2005)

Pindborgs Tumour • DEFINITION (WHO)
The calcifying epithelial odontogenic tumour (CEOT) is a locally invasive epithelial odontogenic neoplasm, characterized by the presence of amyloid material that may become calcified.
• First described by Dr Jens J Pindborg (1956)

Jens J Pindborg (left) & Robert Gorlin (right)

Pathogenesis • Acc to pindborg et al – from Odontogenic Epithelium
• Chaudhry & associates - the cells had been derived from the
Reduced Enamel Epithelium of the closely related unerupted
tooth.
• The peripheral location strongly suggests the possibility that
the tumor arises from Rests Of The Dental Lamina or from
the Basal Cells of the oral epithelium.

•Mutations in PTCH gene
AND gene Ameloblastin
(not conclusive)
•From the cells of stratum
intermedium of the enamel
organ

EPIDEMIOLOGY• ~1% Of all Odontogenic tumours
• Age : 20-60 .. Mean- 40yrs
• Male : female – 6:5
• Intraosseous tumours affect the mandible more often than
the maxilla with a ratio of 2:1.
• Premolar/molar region, although any site may be involved.
• Peripheral lesions usually occur in the anterior gingiva

CLINICAL FEATURES
• Painless mass, slow growth
• Associated with an impacted /unerupted tooth.
• Nasal congestion, epistaxis, headache
• The peripheral soft tissue or extraosseous, CEOT appears most
commonly as a painless, firm gingival mass
• Overlying mucosa may show ulceration due to local trauma.
• On surgical removal,an underlying bony depression or saucerization
has been reported in a few cases.

Radiographic features
• Associated with an unerupted tooth• Mixed radiolucent- radioopaque• Unilocular /multilocular• Honey comb /soap bubble• Scattered radioopacities• Wind driven/ falling snow • Gingival CEOT shows bone erosion at the site.

Orthopantomograph showing a CEOT in the left maxilla around the roots of the third molar with involvement of the left sinus.

CT scan of the left maxillary sinus containing multiple,partly coalscent radiopaque bodies

Transversal tomographs showing a mixed radiopaque/radiolucent image

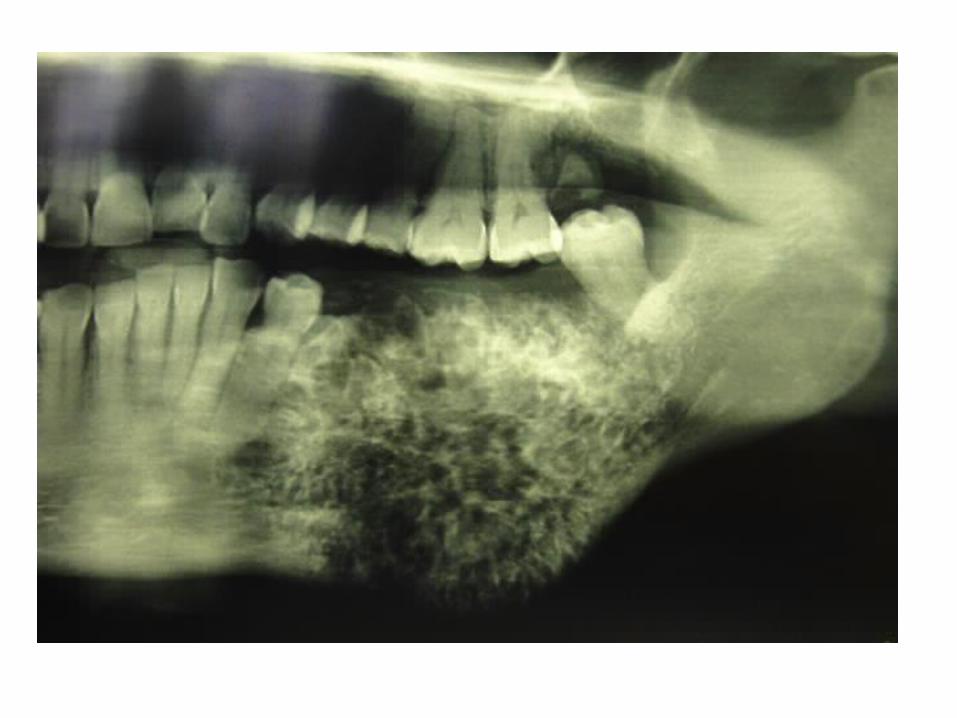
Radiograph of the left mandibular molar region showing an unerupted first molar with a pericoronally located CEOT.
Ceot case report


Macroscopy•The intraosseously located CEOT is often
easily enucleated
• Size - 1 to 4 cm in diameter.
•Color from grayish white or yellow to
tanpink
•Bisecting the specimen usually reveals
calcified particles that makes a crunching
sound during cutting.
•The tumor may be solid
or contain minute cystic spaces.
•If associated with an
unerupted tooth, the crown
can be found embedded in
the tumour mass.

MICROSCOPY• HISTOLOGIC DEFITION OF CEOT – (WHO 1992)
"a locally invasive epithelial neoplasm characterized by the
development of intraepithelial structures, probably of an
amyloid-like nature,which may become calcified and which
may be liberated as the cells break down."

“A locally invasive epithelial neoplasm consisting of
sheets and strands of polyhedral,pleomorphous cells
with well-defined cell borders often showing
intercellular bridges. A characteristic feature is an
amyloid-like material that may become calcified, is
formed intraepithelially and may be liberated as the
cells breakdown”.

H/P Findings • EPITHELIAL CELLS: are polyhedral in the form of sheets, strands or nests. The cells are usually closely packed with few areas showing intercellular bridges.
• They have indistinct outline, eosinophilic & homogenous cytoplasm. The cells resemble the cells of stratum intermedium of enamel organ.
• The nucleus is vesicular with distinct nucleoli, hyperchromatic or pyknotic nuclei, even giant nuclei of 100nm & mitoses may be seen rarely. If seen malignacy .

• EOSINOPHILIC MATERIAL: is seen between the epithelial cells & in the stroma.• It is thought to be synthesized by the epithelial cells & is PAS
positive.
• Vickers has shown it to be amyloid as it stains positively with Congo red, methly violet & fluorosces with thioflavine T.
• Electron microscopically the fibrillar arrangement in this differs from that of the amyloid seen elsewhere. Therefore it is thought to be altered amyloid or amyloid –like.

• CALCIFIC DEPOSITS: are seen to be associated with the amyloid deposits & can be either calcified amyloid or calcified collagen.
• As the amyloid gets calcified, it looses it`s congo red positivity.

• The calcifications can be in the form of lamellae formed by the fusion of small calcific deposits at different foci & they are refered to as "Liesegang rings".
• Cementum-like deposition is seen only after the amyloid is fully calcified, probably the mesenchymal cells around the calcified amyloid differentiates into cementoblasts. This cementum-like substance has a basophilic appearance.

Photomicrograph showing anastomosing sheets ofepithelial,eosinophilic cells with cellularand nuclear polymorphism (hematoxylin eosin[H&EJ, x8O).

Higher magnification of epithelial sheet. Note the nuclear polymorphismand intercellular bridges (H&E, x 150).

Calcified amyloid-likebodies revealingLiesegang rings. (H&E, x8O).

Variations In Histopathology
• Occurence of Amyloid-like material in CEOT
• Occurence of Cementum-like components of
CEOT stroma
• Occurence of Clear-Cells
• Occurence of Langerhans cells in CEOT
• Occurence of Myoepithelial Cells in CEOT
• Combined Epithelial Odontogenic Tumour

Occurence of Amyloid-like material in CEOT
• The biologic and biochemical significance, as well as the origin of this material, is far from being understood.
• An origin from light chain fragments of immunoglobulin molecules has been proposed for some forms of systemic amyloid.
• Another type is possibly associated with endocrine tumors such as the medullary carcinoma of the thyroid derived from the endocrine polypeptide cells of the amine precursor uptake decarboxylation (APUD) system

• Ultrastructural studies have shown that this amyloid-like material is composed of at least three different types of fibrils, but that they have a smaller size than the fibers of 'conventional' amyloid.
• Some forms of amyloid are now suggested to arise from light chain fragments of immunoglobulin molecules, called immunamyloid, while another form is thought to originate from cells of certain endocrine tumors (e.g. medullary carcinoma of the thyroid) which may be derived from the endocrine polypeptide cells of neural crest origin of the amine precursor uptake and decarboxylation (APUD) system, called APUD-amyloid.
• On the evidence available at present, the exact nature of the amyloid like substance in the CEOT cannot be definitively assessed.

Occurence of Cementum-like components of CEOT stroma
• Mechanism is still unclear
• In the study by El-Labban- ' it was found that the outer layer of the calcified lamellar bodies consisted of typical banded calcified collagen with an arrangement like that seen in cemental Sharpey fibers .
• Slootweg suggested that the amyloid-like material is an inductive stimulus for the stroma cells to differentiate toward production of a collagenous matrix that is destined to mineralize and resembles cementum.

Occurence of Clear-Cells
• Sheets of classic polyhedral epithelium with abundant eosinophilic cytoplasm may alternate with zones of epithelium characterized by large cells with clear , foamy cytoplasm and distinct cell borders.
• Yamaguchi et al believed that the clear tumor cells represent a feature of cytodifferentiation rather than a simple degenerative phenomenon.

CEOT with clear cell differentiation and scattered calcified bodies

Occurence of Langerhans cells in CEOT
• Only 2 cases reported
• Asano et al and Takata et al.
• In both cases the tumor cells were positive for S-100
protein,Lysozome,MT1, LN-3, and OKT6 antibodies, but not for keratin
antibody.
• Almost no calcification of homogenous eosinophilic materials was
observed.
• S-100-positive cells were identified as Langerhans cells based on the
finding of rod and tennis racket- shaped Birbeck granules
• LC in CEOT’s-antigen presentation or regression of the tumor.

Occurence of Myoepithelial Cells in CEOT
• Ultrastructure - the tumor sheets and islands consisted of two cell populations:- Classic polyhedral epithelial cells
Cells arranged peripherally with elongated profiles and juxtaposed to the tumor epithelial cells. These cells were found to extend basally around the tumor epithelium in most of the epithelial islands
• The ultrastructural characteristics of these cells were interpreted to be those of myoepithelial cells.

Combined Epithelial Odontogenic Tumour
• In 1983 Damm et al first described the presence of CEOT-like areas within two cases of adenomatoid odontogenic tumors and named them combined epithelial odontogenic
tumors (CEOT/AOTs).

CEOT with AMELOBLASTOMA

CEOT without Calcification
-Aggressive Variant

Malignant CEOT • Malignant CEOT shows nuclear pleomorphism with
frequent mitotic figures including tripolar figures are seen and increased proliferative activity, as assessed by immunostaining for Ki-67, 5times higher as compared to typical CEOT’s, theres vascular invasion and increased proliferating index.
• Only 2 cases reported

ULTRASTRUCTURE
• CEOT epithelial tumor cells consist of polyhedral epithelial cells and myoepithelial-like cells, containing large numbers of electron-dense tonofilament bundles, electron-dense bodies, and fine lamina densa filaments.
• Amyloid-like materials compose fine filament sheets measuring 10-12 nm in diameter and lamina densa fragment aggregates, which are probably secreted by polyhedral epithelial and myoepithelial-like cells.

• The fine filamentous materials are a form of amyloid, and their formation results from lamina densa material degradation.
• Recently, the odontogenic ameloblast-associated protein (ODAM) fibril-forming region was found in CEOT amyloid-like materials, thus suggesting ODAM might have amyloidogenic potential
• A number of dendritic cells, which are frequently found among CEOT epithelial sheets, are strongly positive for S-100 and CD-1a antisera.
• Ultrastructurally, these dendritic cells show indented nuclei and Birbeck’s granules similar to Langerhans cells. Thus, they are likely to be Langerhans cells, and play a role in antigen presentation from epithelial tumor cell abortive products

Differential diagnosis • Ameloblastoma • Histologically when dentine & enamel is present - Regional odontodysplasia
• Complete radiolucent lesions - Dentigerous cyst, Odontogenic keratocyst, ameloblastoma & Odontogenic myxoma
• Mixed radiopaque & radiolucent lesions - COC, AOT, Ossifying fibroma & fibro-odontoma
Treatment • From Surgical enucleation with macroscopically normal tissue
to hemimandibulectomy /hemimaxillectomy.
• Clear cell variant of ceot may prove to be a sign of increased aggresiveness indicating more radical surgical approach.
• Maxillary CEOT requires more aggresive resection when compared to mandibular CEOT.


Prognosis• Recurrence Rates -10% -15%
• Franklin and Pindborg 1976 recurrence rate of 24%
• Clear cell variant – 22%

Stains and markers• Congo red , thioflavin T,Crystal violet,lugols iodine –
POSITIVE FOR AMYLOID but negative for COMASSIE BLUE
• The clear polyhedral cells often exhibit stained granules after periodic acid-Schiff staining. Therefore, these hyaline materials are considered amyloid-like
• Epithelial cells express positivity to laminin 1 & 5 ,fibronectin ,cytokeratins and vimentin , KL1 ,TK 1, PKK1 but the amyloid material does not. Epithelial cells are –ve to DESMIN

• In CEOT, Amyloid +ve CD138 and amyloid ACalcification +ve CK5, CD138, and amyloid A. CEOT showed ↑ Ki-67 protein and minichromosome maintenance complex component 2 (MCM-2) labeling indices.

Calcifying epithelial odontogenic tumour.Congo red staining shows green birefringencewhen subjected to polarized light.

Recent studies• The X-ray diffraction studies have shown the mineral phase of
CEOT to consist of apatite crystals & that the crystallinity of the crystals to be higher than that of the bone apatite.
• The Electron Spin Resonance studies has shown a higher crystallinity coefficient for these calcific deposits higher than that of the the bone.
• All these imply that the calcification in CEOT has higher crystalline structure than the cortical bone.
• Thus it is seen that the calcifications seen in CEOT is either due to the dystrophic calcifications or due to the stromal reaction /induction

Note:• The use of fine-needle aspiration biopsy in
the diagnosis of CEOT was recently reported.
• 13 Cytologic smears were characterized by clusters, sheets, and
rare isolated pleomorphic cells of the squamoid type; blocks of
amorphous material encircled by fibroblasts; and occasional
calcifications.
• A cytologic diagnosis of CEOT was made, which was confirmed
by histopathologic examination.

References • Shafers textbook of oral pathology – 7th edition
• Reichart P, Philipsen HP. Odontogenic tumours and allied lesions.London: Quintessence Books, 2004.
• Lucas’s pathology of tumor of the oral tissue - HA Cawson
• Text Book of oral and maxillofacial pathology – Neville .
• Odontogenic tumours: a short version.
• Bouckaert MM, Raubenheimer EJ, Jacobs FJ. Calcifying epithelial odontogenic tumor with intracranial extension: report of a case and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000; 90: 656–62.

• Barnes L, Eveson JW, Reichart P, Sidransky D. WHO classification of tumors. Pathology and genetics of head and neck tumours. Lyon:IARC Press, 2005.
• Murphy CL, Kestler DP, Foster JS, et al. Odontogenic ameloblastassociated protein nature of the amyloid found in calcifying epithelial odontogenic tumors and unerupted tooth follicles. Amyloid 2008; 15: 89–95
• New findings and controversies in odontogenic tumors-Adalberto Mosqueda Taylor-Med Oral Patol Oral Cir Bucal. 2008 Sep1;13(9):E555-8.
• Bingham RA, Adrian JC. Combined epithelial odontogenic tumor‑adenomatoid odontogenic tumor and calcifying epithelial odontogenic tumor: Report of a case. J Oral Maxillofac Surg 1986;44:574‑7

• Calcifying epithelial odontogenic tumor showing microscopic features of potential malignant behavior April 27-May 2, 2001.
Yi-Shing Lisa Cheng,John M. Wright ,William R. Walstad,Maxwell D. Finn
• A rare case of hybrid odontogenic tumor: Calcifying epithelial odontogenic tumor combined with ameloblastoma, Vijay Wadhwan, Preeti Sharma, Vishal Bansal 2015
• WHO
• Montes Ledesma C, Mosqueda Taylor A, Romero de Leon E, de la Piedra Garza M, Goldberg Jaukin P, Portilla Robertson J. Adenomatoid odontogenic tumour with features of calcifying epithelial odontogenic tumour (The so-called combined epithelial odontogenic tumour): clinico-pathological report of 12 cases. Eur J Cancer B Oral Oncol 1993; 29B: 221-4.


….BULLETS
• Differential diagnosis (correct it)• Metachromasia • Principle of congo red• Crystal violet property• Y non-calcifying ceot recurrent ??• Differentiate CEOT from COC • Types of calcifications• Areas other than oral cavity where calcifications seen?
Related Documents











