http://nnr.sagepub.com/ Repair Neurorehabilitation and Neural http://nnr.sagepub.com/content/26/3/247 The online version of this article can be found at: DOI: 10.1177/1545968311415862 2012 26: 247 originally published online 8 September 2011 Neurorehabil Neural Repair Ching-yi Wu, Yi-an Chen, Hsieh-ching Chen, Keh-chung Lin and I-ling Yeh to Grasp and Trunk Kinematics Pilot Trial of Distributed Constraint-Induced Therapy With Trunk Restraint to Improve Poststroke Reach Published by: http://www.sagepublications.com On behalf of: American Society of Neurorehabilitation can be found at: Neurorehabilitation and Neural Repair Additional services and information for http://nnr.sagepub.com/cgi/alerts Email Alerts: http://nnr.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: What is This? - Sep 8, 2011 OnlineFirst Version of Record - Feb 16, 2012 Version of Record >> at NATIONAL TAIWAN UNIV LIB on August 20, 2012 nnr.sagepub.com Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

http://nnr.sagepub.com/Repair
Neurorehabilitation and Neural
http://nnr.sagepub.com/content/26/3/247The online version of this article can be found at:
DOI: 10.1177/1545968311415862 2012 26: 247 originally published online 8 September 2011Neurorehabil Neural Repair
Ching-yi Wu, Yi-an Chen, Hsieh-ching Chen, Keh-chung Lin and I-ling Yehto Grasp and Trunk Kinematics
Pilot Trial of Distributed Constraint-Induced Therapy With Trunk Restraint to Improve Poststroke Reach
Published by:
http://www.sagepublications.com
On behalf of:
American Society of Neurorehabilitation
can be found at:Neurorehabilitation and Neural RepairAdditional services and information for
http://nnr.sagepub.com/cgi/alertsEmail Alerts:
http://nnr.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
What is This?
- Sep 8, 2011 OnlineFirst Version of Record
- Feb 16, 2012Version of Record >>
at NATIONAL TAIWAN UNIV LIB on August 20, 2012nnr.sagepub.comDownloaded from

Neurorehabilitation and Neural Repair26(3) 247 –255© The Author(s) 2012Reprints and permission: http://www. sagepub.com/journalsPermissions.navDOI: 10.1177/1545968311415862http://nnr.sagepub.com
415862 NNRXXX10.1177/1545968311415862Wu et alNeurorehabilitation and Neural Repair© The Author(s) 2010
Reprints and permission: http://www.sagepub.com/journalsPermissions.nav
1Chang Gung University, Taoyuan, Taiwan2National Taipei University of Technology, Taipei, Taiwan3National Taiwan University, Taipei, Taiwan4National University Hospital, Singapore
Corresponding Author:Keh-chung Lin, School of Occupational Therapy, National Taiwan University College of Medicine, and Division of Occupational Therapy, Department of Physical Medicine and Rehabilitation, National Taiwan University Hospital, 17, F4, Xu Zhou Road, Taipei, Taiwan Email: [email protected]
Pilot Trial of Distributed Constraint- Induced Therapy With Trunk Restraint to Improve Poststroke Reach to Grasp and Trunk Kinematics
Ching-yi Wu, ScD1, Yi-an Chen, MS1, Hsieh-ching Chen, PhD2, Keh-chung Lin, ScD3, and I-ling Yeh, MS4
Abstract
Background. Constraint-induced therapy (CIT) is effective in improving upper extremity motor function, but evidence is lacking about effectiveness grasp and trunk control. Objective. This study investigated whether distributed CIT combined with trunk restraint (dCIT + TR) benefited movement kinematics of grasping and the trunk, as well as motor ability of the upper extremity, more than dCIT alone. Methods. A total of 45 stroke participants received 2 hours of dCIT + TR, dCIT, or the dose-matched control intervention for 3 weeks. Movement kinematics, motor ability, and daily function were the outcome measures. Movement kinematics included grasping, joint range, and trunk movement at various phases of reach-to-grasp tasks. Motor ability and daily function of all participants were evaluated using the Fugl-Meyer Assessment and the Motor Activity Log. Results. Four to 5 participants in each group were not included for kinematic analysis because of their inability to grasp a can. The dCIT + TR group showed better preplanned grasping movement and less trunk motion at the early phase of the reach-to-grasp movements than the dCIT or control groups. Compared with the controls, the dCIT + TR participants showed better motor ability in the overall and distal arm scores of the Fugl-Meyer Assessment. The dCIT + TR and dCIT participants demonstrated significantly greater functional use of the affected arm. Conclusions. Administering dCIT + TR produced additional benefits by improving grasping control and reversing the compensatory trunk movement at the early phase of a reach-to-grasp movement. The use of experimental tasks beyond and within arm’s length might improve our understanding of optimal upper extremity rehabilitation.
Keywords
grasping, stroke rehabilitation, kinematics, trunk restraint, constraint-induced therapy, compensatory movement
Introduction
Studies on constraint-induced therapy (CIT)1,2 and its less intensive derivatives3-6 found improved motor ability and functional use of the affected upper extremity (UE) in patients with residual motor control of the wrist and finger extensors in hemiparetic subjects after stroke. Participants demonstrated greater gains in the distal compared with the proximal affected UE,4-6 as measured by the Fugl-Meyer Assessment (FMA). However, gains in distal motor ability did not reflect improvement in the control strategy of move-ments such as grasping.3 In addition, CIT may not reduce the compensatory strategy of trunk movement during reach-ing.1 The absence of changes in these control strategies points out the need to develop CIT further if the goal is to restore more normative control strategies.1
Patients after stroke often recruit an additional degree of freedom from the trunk to assist reach-to-grasp movements.7-10
Compensatory truncal movements may improve with prac-tice that restricts excessive trunk motion during the UE movement. Trunk restraint may induce better coordination of the arm joints, reduce additional trunk movement, and improve the movement pattern of the affected arm.7,10-12 Woodbury et al13 combined CIT with trunk restraint and found better reaching control (straighter hand paths), improved
Clinical Research Articles
at NATIONAL TAIWAN UNIV LIB on August 20, 2012nnr.sagepub.comDownloaded from
248 Neurorehabilitation and Neural Repair 26(3)
Eligible participants (n = 168)
Randomized (n = 45)
Excluded (n = 123)Not meeting inclusion criteria (n = 107)
Refused to participate (n = 16)
dCIT+TR (n = 15) Control (n = 15)
Analyzed (n = 11 for kinematicanalysis, n = 15 for clinical measures)
dCIT (n = 15)
Analyzed (n = 10 for kinematicanalysis, n = 15 for clinical measures)
Analyzed (n = 10 for kinematicanalysis, n = 15 for clinical measures)
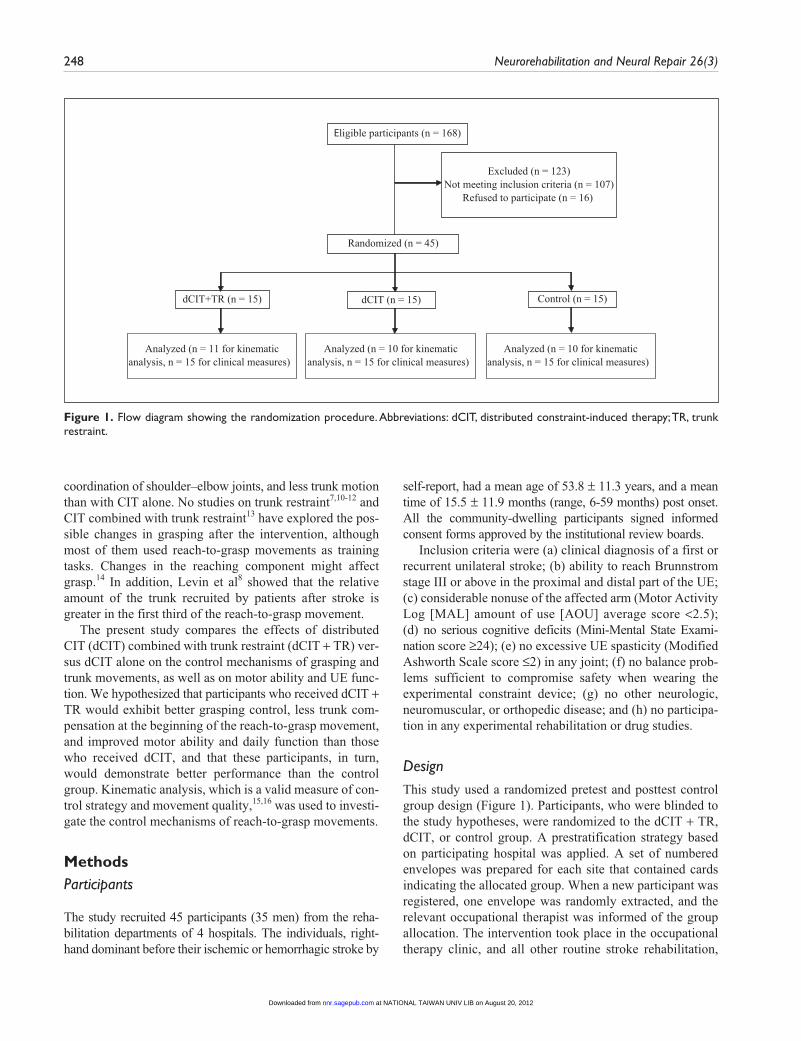
Figure 1. Flow diagram showing the randomization procedure. Abbreviations: dCIT, distributed constraint-induced therapy; TR, trunk restraint.
coordination of shoulder–elbow joints, and less trunk motion than with CIT alone. No studies on trunk restraint7,10-12 and CIT combined with trunk restraint13 have explored the pos-sible changes in grasping after the intervention, although most of them used reach-to-grasp movements as training tasks. Changes in the reaching component might affect grasp.14 In addition, Levin et al8 showed that the relative amount of the trunk recruited by patients after stroke is greater in the first third of the reach-to-grasp movement.
The present study compares the effects of distributed CIT (dCIT) combined with trunk restraint (dCIT + TR) ver-sus dCIT alone on the control mechanisms of grasping and trunk movements, as well as on motor ability and UE func-tion. We hypothesized that participants who received dCIT + TR would exhibit better grasping control, less trunk com-pensation at the beginning of the reach-to-grasp movement, and improved motor ability and daily function than those who received dCIT, and that these participants, in turn, would demonstrate better performance than the control group. Kinematic analysis, which is a valid measure of con-trol strategy and movement quality,15,16 was used to investi-gate the control mechanisms of reach-to-grasp movements.
MethodsParticipants
The study recruited 45 participants (35 men) from the reha-bilitation departments of 4 hospitals. The individuals, right-hand dominant before their ischemic or hemorrhagic stroke by
self-report, had a mean age of 53.8 ± 11.3 years, and a mean time of 15.5 ± 11.9 months (range, 6-59 months) post onset. All the community-dwelling participants signed informed consent forms approved by the institutional review boards.
Inclusion criteria were (a) clinical diagnosis of a first or recurrent unilateral stroke; (b) ability to reach Brunnstrom stage III or above in the proximal and distal part of the UE; (c) considerable nonuse of the affected arm (Motor Activity Log [MAL] amount of use [AOU] average score <2.5); (d) no serious cognitive deficits (Mini-Mental State Exami-nation score ≥24); (e) no excessive UE spasticity (Modified Ashworth Scale score ≤2) in any joint; (f) no balance prob-lems sufficient to compromise safety when wearing the experimental constraint device; (g) no other neurologic, neuromuscular, or orthopedic disease; and (h) no participa-tion in any experimental rehabilitation or drug studies.
DesignThis study used a randomized pretest and posttest control group design (Figure 1). Participants, who were blinded to the study hypotheses, were randomized to the dCIT + TR, dCIT, or control group. A prestratification strategy based on participating hospital was applied. A set of numbered envelopes was prepared for each site that contained cards indicating the allocated group. When a new participant was registered, one envelope was randomly extracted, and the relevant occupational therapist was informed of the group allocation. The intervention took place in the occupational therapy clinic, and all other routine stroke rehabilitation,
at NATIONAL TAIWAN UNIV LIB on August 20, 2012nnr.sagepub.comDownloaded from

Wu et al 249
Figure 2. (A) The intervention setup of dCIT + TR group. (B) The setup for kinematic tests. Seated participants were asked to reach and grasp a cylindrical can using their affected arm with self-paced speed. Abbreviations: dCIT, distributed constraint-induced therapy; TR, trunk restraint.
including physical therapy or speech therapy, proceeded as usual. The outcome measures were administered before and after a 3-week intervention by 3 trained occupational thera-pists blinded to group allocation.
InterventionOne-to-one treatments were designed, and all groups received treatment of equal intensity (2 h/d, 5 d/wk, for 3 consecutive weeks). The treating therapists were trained in the administration of these 3 protocols by the investiga-tors to provide consistent intervention protocols. The tar-gets used in the training tasks in the 3 groups were placed inside the individual’s reachable workspace.
The dCIT + TR group. Participants in this group focused on the intensive training of the affected arm in functional activi-ties with behavioral shaping and combination with trunk restraint. The functional tasks included, for example, flip-ping pages of magazines and picking up coins. The shaping skills involved individualized task selection, graded task dif-ficulty (eg, practicing deficient parts of the selected activity and then performing the entire activity), verbal feedback, prompting, physical assistance with movements, and model-ing. To limit trunk movement when sitting, participants wore a harness that was secured to the chair back by Velcro straps and adjusted to allow for arm movement (Figure 2A). Par-ticipants were also required to place their unaffected hand and wrist in a mitt for 6 hours a day during the 3-week period and documented mitt compliance in daily logs.
The dCIT group. The dCIT group participants received an intervention protocol that resembled the dCIT + TR inter-vention, except for the lack of trunk restraint.
The control intervention group. The control group primar-ily employed neurodevelopmental treatment techniques and focused on improving strength, muscle tone, range of motion, body posture, and functional task performance. Participants used the affected arm, or both arms with the unaffected arm assisting the affected arm, for performing unilateral or bilat-eral functional activities. The control intervention was con-sidered as the baseline treatment and allowed us to estimate if specific intensive treatments, such as dCIT and dCIT + TR, would confer greater treatment benefits for participants with hemiparesis after stroke than the intervention usually used in the clinics.
Primary Outcome Measures: Kinematic AnalysisThe experimental task used in the kinematic analysis was reaching to grasp a can (5.3 cm in diameter and 10.5 cm in height; Figure 2B) along the participants’ midsagittal plane. The reach-to-grasp task was suggested to be a sensitive task item representing motor improvement of the affected arm.17 We measured the arm’s length as the distance from the acromion to the third fingertip and standardized the task distances to 90% and 125% of this distance to explore the trunk compensation in different task demands. During the tasks, the participant sat without trunk restraint on a
at NATIONAL TAIWAN UNIV LIB on August 20, 2012nnr.sagepub.comDownloaded from

250 Neurorehabilitation and Neural Repair 26(3)
height-adjustable chair with the seat height set to 100% of the lower leg length, measured from the lateral knee joint to the floor. Adjacent to the chair was a table with a height adjusted to 5 cm below the elbow while the participant sat on the chair. The participant’s affected hand was initially posi-tioned on the edge of the table with elbow flexion at 90°.
After a practice trial, 3 data-producing trials with self-paced speed were performed. A 7-camera motion analysis system (VICON MX; Oxford Metrics Inc, Oxford, UK) was used with a personal computer to capture the move-ment of the reference markers. Reference markers were placed on the seventh cervical vertebra (C7), the fourth tho-racic vertebra (T4), midsternum, the bilateral clavicles, and the affected side of acromion, middle of humerus, lateral epicondyle, styloid process of the ulna and radius, thumb nail, and index nail. Movements were recorded at 120 Hz and digitally low-pass filtered at 5 Hz using a second-order dual-pass Butterworth filter. Movement onset and offset were defined for each trial using the time at which the tan-gential wrist velocity rose 5% above and fell 5% below its peak value for 3 consecutive samples based on the rules used in the previous studies.9,18
Data reduction for kinematic variables. Kinematic vari-ables were chosen to indicate the control strategy and move-ment quality for grasping, joint range of the UE (the shoulder and elbow joints), and trunk movement.
The variables of the grasping component were maxi-mum grip aperture (MGA) and the percentage of time to maximum grip aperture (TMGA), which represent the con-trol strategy of grasping. The MGA was calculated as the maximum distance between the markers on the thumb and index nails, representing the extent of hand opening. A skillful grasping movement normally is made without widely opening the hand. The TMGA, reflecting where the MGA occurs in a percentage of movement time, is an indi-cator of online grasping correction during enclosure. A high TMGA amplitude refers to a low percentage of time con-tributing to online correction and indicates a well pre-planned grasp.19
The joint range included the active angular change of shoulder and elbow joints, defined as the difference in degrees from the beginning to the end of the movement. Because the task distance varied across participants, the angular changes of shoulder and elbow joints were normal-ized to correct for variations in task distance; that is, the angular change was divided by the task distance measured in millimeters.
The slope value represents the ratio of trunk/UE move-ment of which the displacement in the sagittal plane was obtained. The slope indicates the contribution of trunk motion to the total end point motion. The slope was calcu-lated separately in 3 parts (the start, middle, and the end phase of reach-to-grasp motion) to probe the particular con-tributed proportion between the UE and trunk. The slope
was zero if all of the movement was due to trunk motion and infinite if the trunk did not contribute to the end point movement.8 The negative value of the slope shows that the trunk moved backward while the UE still reached forward during the reach-to-grasp phase.
Secondary Outcome Measures: Clinical MeasuresThe clinical measures included the FMA and the MAL. The UE part of the FMA20 assesses several dimensions of motor impairment, including movements of the proximal (shoul-der, elbow, and forearm) and distal (wrist and hand) struc-tures.21-23 The MAL is a semistructured interview that obtains information about how participants use their affected limbs during 30 important daily activities and assesses the AOU and the quality of movement (QOM) of the affected arm.24-27
Data AnalysisThe χ2 test and the analysis of variance test were used to determine comparability at baseline characteristics of partici-pants. Analysis of covariance was used to compare the rela-tive effects of the treatment on participants for each variable. The pretest score was the covariate, the group was the inde-pendent variable, and the posttest score was the dependent variable. Post hoc analysis was performed based on signifi-cant group effects by the least significant difference test. To index the magnitude of group differences in performance, η2 = SS
b/SS
total was calculated for each outcome variable.28 A
large effect is represented by a η2 of at least .138, a moderate effect by a η2 of .059, and a small effect by a η2 of .01.29
ResultsCharacteristics of Participants
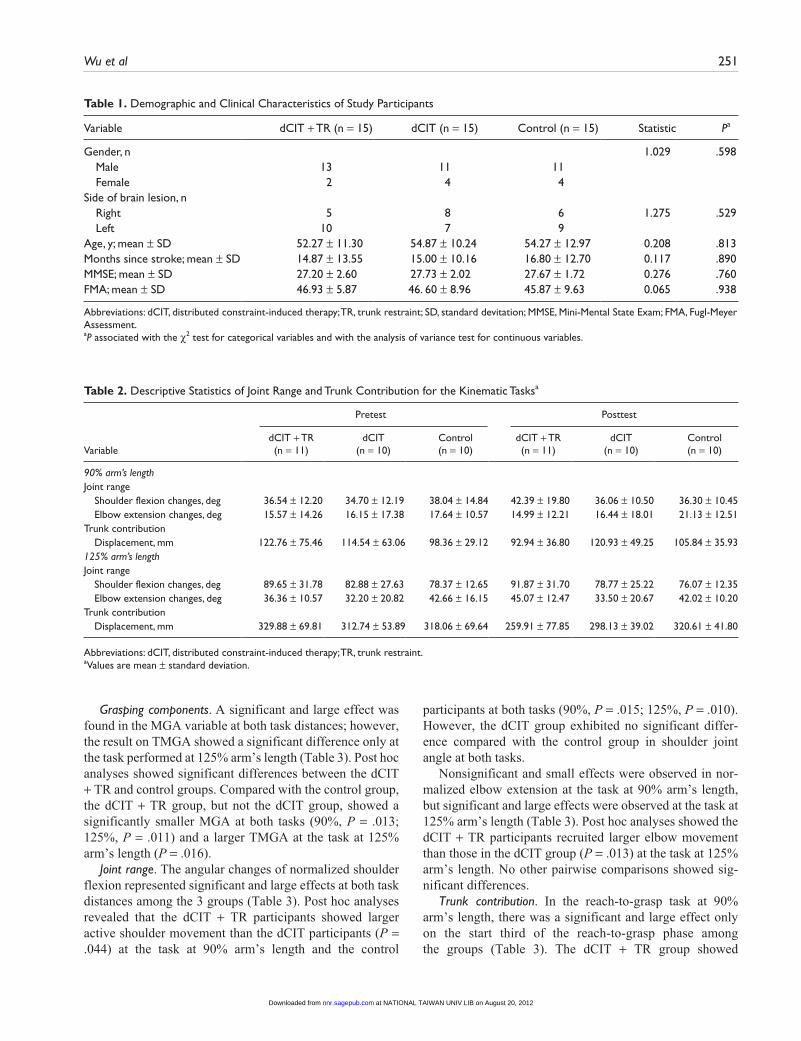
All demographic and clinical characteristics at baseline were comparable among the participants in the 3 groups (Table 1). There were no preexisting significant differences between the 3 groups on any of the outcome measures (P = .529 to .938).
Primary Outcome Measures: Kinematic AnalysisNo kinematic data were obtained from 4 to 5 participants in each group because they were unable to successfully grasp a can. Consequently, kinematic data of 11, 10, and 10 par-ticipants were analyzed in the dCIT + TR, dCIT, and con-trol groups, respectively. Table 2 shows descriptive statistics of the joint angle and trunk contribution for the kinematic tasks in each group at pretest and posttest.
at NATIONAL TAIWAN UNIV LIB on August 20, 2012nnr.sagepub.comDownloaded from
Wu et al 251
Table 1. Demographic and Clinical Characteristics of Study Participants
Variable dCIT + TR (n = 15) dCIT (n = 15) Control (n = 15) Statistic Pa
Gender, n 1.029 .598 Male 13 11 11 Female 2 4 4 Side of brain lesion, n Right 5 8 6 1.275 .529 Left 10 7 9 Age, y; mean ± SD 52.27 ± 11.30 54.87 ± 10.24 54.27 ± 12.97 0.208 .813Months since stroke; mean ± SD 14.87 ± 13.55 15.00 ± 10.16 16.80 ± 12.70 0.117 .890MMSE; mean ± SD 27.20 ± 2.60 27.73 ± 2.02 27.67 ± 1.72 0.276 .760FMA; mean ± SD 46.93 ± 5.87 46. 60 ± 8.96 45.87 ± 9.63 0.065 .938
Abbreviations: dCIT, distributed constraint-induced therapy; TR, trunk restraint; SD, standard devitation; MMSE, Mini-Mental State Exam; FMA, Fugl-Meyer Assessment.aP associated with the χ2 test for categorical variables and with the analysis of variance test for continuous variables.
Table 2. Descriptive Statistics of Joint Range and Trunk Contribution for the Kinematic Tasksa
Pretest Posttest
VariabledCIT + TR (n = 11)
dCIT (n = 10)
Control (n = 10)
dCIT + TR (n = 11)
dCIT (n = 10)
Control (n = 10)
90% arm’s length Joint range Shoulder flexion changes, deg 36.54 ± 12.20 34.70 ± 12.19 38.04 ± 14.84 42.39 ± 19.80 36.06 ± 10.50 36.30 ± 10.45 Elbow extension changes, deg 15.57 ± 14.26 16.15 ± 17.38 17.64 ± 10.57 14.99 ± 12.21 16.44 ± 18.01 21.13 ± 12.51Trunk contribution Displacement, mm 122.76 ± 75.46 114.54 ± 63.06 98.36 ± 29.12 92.94 ± 36.80 120.93 ± 49.25 105.84 ± 35.93125% arm’s length Joint range Shoulder flexion changes, deg 89.65 ± 31.78 82.88 ± 27.63 78.37 ± 12.65 91.87 ± 31.70 78.77 ± 25.22 76.07 ± 12.35 Elbow extension changes, deg 36.36 ± 10.57 32.20 ± 20.82 42.66 ± 16.15 45.07 ± 12.47 33.50 ± 20.67 42.02 ± 10.20Trunk contribution Displacement, mm 329.88 ± 69.81 312.74 ± 53.89 318.06 ± 69.64 259.91 ± 77.85 298.13 ± 39.02 320.61 ± 41.80
Abbreviations: dCIT, distributed constraint-induced therapy; TR, trunk restraint.aValues are mean ± standard deviation.
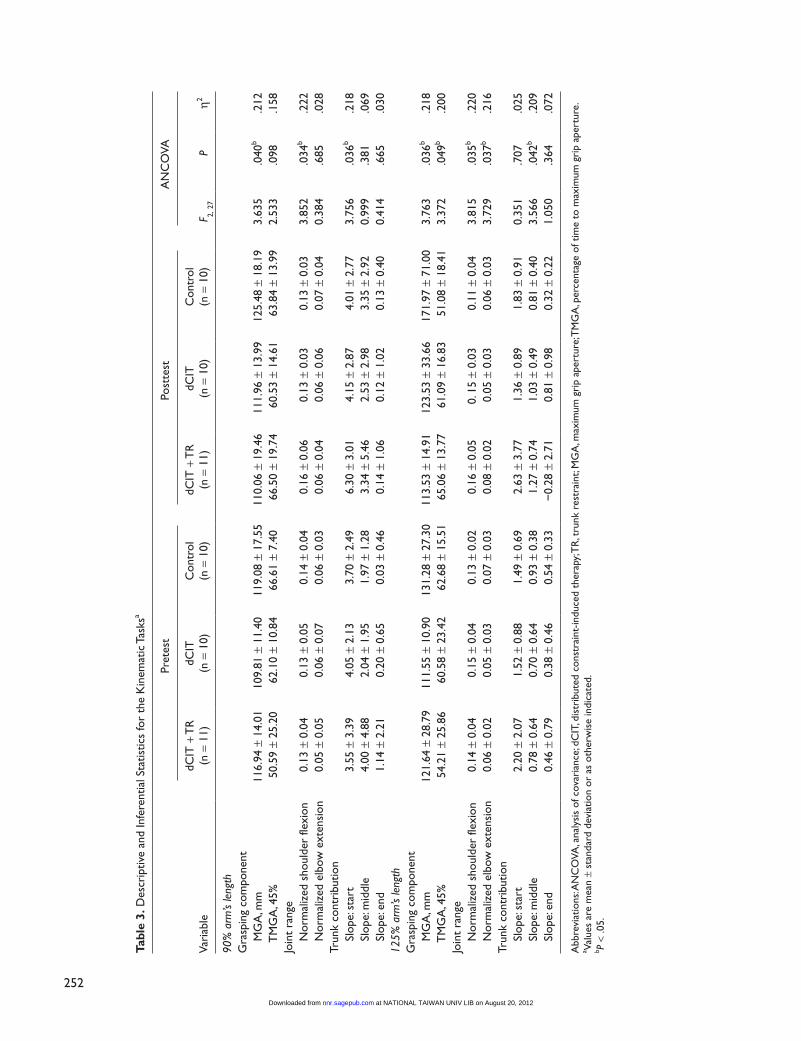
Grasping components. A significant and large effect was found in the MGA variable at both task distances; however, the result on TMGA showed a significant difference only at the task performed at 125% arm’s length (Table 3). Post hoc analyses showed significant differences between the dCIT + TR and control groups. Compared with the control group, the dCIT + TR group, but not the dCIT group, showed a significantly smaller MGA at both tasks (90%, P = .013; 125%, P = .011) and a larger TMGA at the task at 125% arm’s length (P = .016).
Joint range. The angular changes of normalized shoulder flexion represented significant and large effects at both task distances among the 3 groups (Table 3). Post hoc analyses revealed that the dCIT + TR participants showed larger active shoulder movement than the dCIT participants (P = .044) at the task at 90% arm’s length and the control
participants at both tasks (90%, P = .015; 125%, P = .010). However, the dCIT group exhibited no significant differ-ence compared with the control group in shoulder joint angle at both tasks.
Nonsignificant and small effects were observed in nor-malized elbow extension at the task at 90% arm’s length, but significant and large effects were observed at the task at 125% arm’s length (Table 3). Post hoc analyses showed the dCIT + TR participants recruited larger elbow movement than those in the dCIT group (P = .013) at the task at 125% arm’s length. No other pairwise comparisons showed sig-nificant differences.
Trunk contribution. In the reach-to-grasp task at 90% arm’s length, there was a significant and large effect only on the start third of the reach-to-grasp phase among the groups (Table 3). The dCIT + TR group showed
at NATIONAL TAIWAN UNIV LIB on August 20, 2012nnr.sagepub.comDownloaded from
252
Tabl
e 3.
Des
crip
tive
and
Infe
rent
ial S
tatis
tics
for
the
Kin
emat
ic T
asks
a
Pret
est
Post
test
AN
CO
VA
Vari
able
dCIT
+ T
R
(n =
11)
dCIT
(n
= 1
0)C
ontr
ol
(n =
10)
dCIT
+ T
R
(n =
11)
dCIT
(n
= 1
0)C
ontr
ol
(n =
10)
F 2, 27
Pη2
90%
arm
’s le
ngth
G
rasp
ing
com
pone
nt
M
GA
, mm
116.
94 ±
14.
0110
9.81
± 1
1.40
119.
08 ±
17.
5511
0.06
± 1
9.46
111.
96 ±
13.
9912
5.48
± 1
8.19
3.63
5.0
40b
.212
T
MG
A, 4
5%50
.59
± 25
.20
62.1
0 ±
10.8
466
.61
± 7.
4066
.50
± 19
.74
60.5
3 ±
14.6
163
.84
± 13
.99
2.53
3.0
98.1
58Jo
int
rang
e
N
orm
aliz
ed s
houl
der
flexi
on0.
13 ±
0.0
40.
13 ±
0.0
50.
14 ±
0.0
40.
16 ±
0.0
60.
13 ±
0.0
30.
13 ±
0.0
33.
852
.034
b.2
22
Nor
mal
ized
elb
ow e
xten
sion
0.05
± 0
.05
0.06
± 0
.07
0.06
± 0
.03
0.06
± 0
.04
0.06
± 0
.06
0.07
± 0
.04
0.38
4.6
85.0
28Tr
unk
cont
ribu
tion
Slop
e: s
tart
3.55
± 3
.39
4.05
± 2
.13
3.70
± 2
.49
6.30
± 3
.01
4.15
± 2
.87
4.01
± 2
.77
3.75
6.0
36b
.218
Sl
ope:
mid
dle
4.00
± 4
.88
2.04
± 1
.95
1.97
± 1
.28
3.34
± 5
.46
2.53
± 2
.98
3.35
± 2
.92
0.99
9.3
81.0
69
Slop
e: e
nd1.
14 ±
2.2
10.
20 ±
0.6
50.
03 ±
0.4
60.
14 ±
1.0
60.
12 ±
1.0
20.
13 ±
0.4
00.
414
.665
.030
125%
arm
’s le
ngth
G
rasp
ing
com
pone
nt
M
GA
, mm
121.
64 ±
28.
7911
1.55
± 1
0.90
131.
28 ±
27.
3011
3.53
± 1
4.91
123.
53 ±
33.
6617
1.97
± 7
1.00
3.76
3.0
36b
.218
T
MG
A, 4
5%54
.21
± 25
.86
60.5
8 ±
23.4
262
.68
± 15
.51
65.0
6 ±
13.7
761
.09
± 16
.83
51.0
8 ±
18.4
13.
372
.049
b.2
00Jo
int
rang
e
N
orm
aliz
ed s
houl
der
flexi
on0.
14 ±
0.0
40.
15 ±
0.0
40.
13 ±
0.0
20.
16 ±
0.0
50.
15
± 0.
030.
11 ±
0.0
43.
815
.035
b.2
20
Nor
mal
ized
elb
ow e
xten
sion
0.06
± 0
.02
0.05
± 0
.03
0.07
± 0
.03
0.08
± 0
.02
0.05
± 0
.03
0.06
± 0
.03
3.72
9.0
37b
.216
Trun
k co
ntri
butio
n
Sl
ope:
sta
rt2.
20 ±
2.0
71.
52 ±
0.8
81.
49 ±
0.6
92.
63 ±
3.7
71.
36 ±
0.8
91.
83 ±
0.9
10.
351
.707
.025
Sl
ope:
mid
dle
0.78
± 0
.64
0.70
± 0
.64
0.93
± 0
.38
1.27
± 0
.74
1.03
± 0
.49
0.81
± 0
.40
3.56
6.0
42b
.209
Sl
ope:
end
0.46
± 0
.79
0.38
± 0
.46
0.54
± 0
.33
−0.
28 ±
2.7
10.
81 ±
0.9
80.
32 ±
0.2
21.
050
.364
.072
Abb
revi
atio
ns: A
NC
OVA
, ana
lysi
s of
cov
aria
nce;
dC
IT, d
istr
ibut
ed c
onst
rain
t-in
duce
d th
erap
y; T
R, t
runk
res
trai
nt; M
GA
, max
imum
gri
p ap
ertu
re; T
MG
A, p
erce
ntag
e of
tim
e to
max
imum
gri
p ap
ertu
re.
a Valu
es a
re m
ean
± st
anda
rd d
evia
tion
or a
s ot
herw
ise
indi
cate
d.b P
< .0
5.
at NATIONAL TAIWAN UNIV LIB on August 20, 2012nnr.sagepub.comDownloaded from
Wu et al 253
significantly less trunk contribution during the start third phase than the dCIT group (P = .024) and the control group (P = .028), but the dCIT group was not significantly differ-ent from the control group.
The results of trunk contribution in the task at 125% arm’s length showed that only the middle phase achieved statistical significance and a large effect (Table 3). In this phase, the dCIT + TR group exhibited less trunk compensa-tion than the control group (P = .013), but no significant differences were noted between the dCIT + TR and dCIT groups or between the dCIT and control groups.
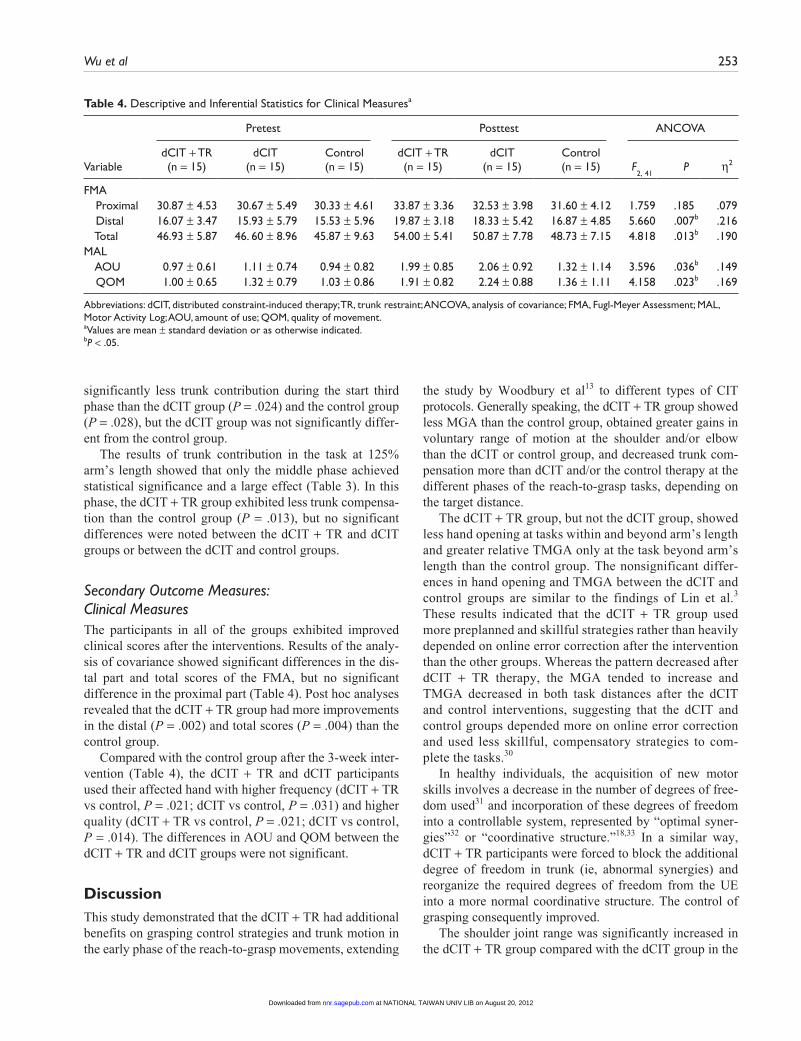
Secondary Outcome Measures: Clinical MeasuresThe participants in all of the groups exhibited improved clinical scores after the interventions. Results of the analy-sis of covariance showed significant differences in the dis-tal part and total scores of the FMA, but no significant difference in the proximal part (Table 4). Post hoc analyses revealed that the dCIT + TR group had more improvements in the distal (P = .002) and total scores (P = .004) than the control group.
Compared with the control group after the 3-week inter-vention (Table 4), the dCIT + TR and dCIT participants used their affected hand with higher frequency (dCIT + TR vs control, P = .021; dCIT vs control, P = .031) and higher quality (dCIT + TR vs control, P = .021; dCIT vs control, P = .014). The differences in AOU and QOM between the dCIT + TR and dCIT groups were not significant.
DiscussionThis study demonstrated that the dCIT + TR had additional benefits on grasping control strategies and trunk motion in the early phase of the reach-to-grasp movements, extending
Table 4. Descriptive and Inferential Statistics for Clinical Measuresa
Pretest Posttest ANCOVA
VariabledCIT + TR (n = 15)
dCIT (n = 15)
Control (n = 15)
dCIT + TR (n = 15)
dCIT (n = 15)
Control (n = 15) F
2, 41
P η2
FMA Proximal 30.87 ± 4.53 30.67 ± 5.49 30.33 ± 4.61 33.87 ± 3.36 32.53 ± 3.98 31.60 ± 4.12 1.759 .185 .079 Distal 16.07 ± 3.47 15.93 ± 5.79 15.53 ± 5.96 19.87 ± 3.18 18.33 ± 5.42 16.87 ± 4.85 5.660 .007b .216 Total 46.93 ± 5.87 46. 60 ± 8.96 45.87 ± 9.63 54.00 ± 5.41 50.87 ± 7.78 48.73 ± 7.15 4.818 .013b .190MAL AOU 0.97 ± 0.61 1.11 ± 0.74 0.94 ± 0.82 1.99 ± 0.85 2.06 ± 0.92 1.32 ± 1.14 3.596 .036b .149 QOM 1.00 ± 0.65 1.32 ± 0.79 1.03 ± 0.86 1.91 ± 0.82 2.24 ± 0.88 1.36 ± 1.11 4.158 .023b .169
Abbreviations: dCIT, distributed constraint-induced therapy; TR, trunk restraint; ANCOVA, analysis of covariance; FMA, Fugl-Meyer Assessment; MAL, Motor Activity Log; AOU, amount of use; QOM, quality of movement.aValues are mean ± standard deviation or as otherwise indicated.bP < .05.
the study by Woodbury et al13 to different types of CIT protocols. Generally speaking, the dCIT + TR group showed less MGA than the control group, obtained greater gains in voluntary range of motion at the shoulder and/or elbow than the dCIT or control group, and decreased trunk com-pensation more than dCIT and/or the control therapy at the different phases of the reach-to-grasp tasks, depending on the target distance.
The dCIT + TR group, but not the dCIT group, showed less hand opening at tasks within and beyond arm’s length and greater relative TMGA only at the task beyond arm’s length than the control group. The nonsignificant differ-ences in hand opening and TMGA between the dCIT and control groups are similar to the findings of Lin et al.3 These results indicated that the dCIT + TR group used more preplanned and skillful strategies rather than heavily depended on online error correction after the intervention than the other groups. Whereas the pattern decreased after dCIT + TR therapy, the MGA tended to increase and TMGA decreased in both task distances after the dCIT and control interventions, suggesting that the dCIT and control groups depended more on online error correction and used less skillful, compensatory strategies to com-plete the tasks.30
In healthy individuals, the acquisition of new motor skills involves a decrease in the number of degrees of free-dom used31 and incorporation of these degrees of freedom into a controllable system, represented by “optimal syner-gies”32 or “coordinative structure.”18,33 In a similar way, dCIT + TR participants were forced to block the additional degree of freedom in trunk (ie, abnormal synergies) and reorganize the required degrees of freedom from the UE into a more normal coordinative structure. The control of grasping consequently improved.
The shoulder joint range was significantly increased in the dCIT + TR group compared with the dCIT group in the
at NATIONAL TAIWAN UNIV LIB on August 20, 2012nnr.sagepub.comDownloaded from

254 Neurorehabilitation and Neural Repair 26(3)
task within arm’s length and the control group in both tasks, in agreement with previous studies,7,13 which may preserve the ability to adapt movements to various external conditions. Furthermore, voluntary shoulder flexion is more amenable to change than elbow extension.30 Limiting trunk compen-sation may force participants to focus on important ele-ments of the movement pattern and encourage the recovery of shoulder joint flexibility.
In normal reach-to-grasp tasks, adults maintain some elbow flexion at the end of reaching to facilitate final adjust-ments to hand location and orientation.34 We speculated that the dCIT + TR participants might use a similar strategy and primarily use shoulder flexion for accomplishing the reach-to-grasp task. The elbow joint was significantly more recruited in the dCIT + TR group than in the dCIT group only at the task at 125% arm’s length, which is partially consistent with previous research.1,7,10-13 The differential results—the present study showed improvements in the elbow but the previous studies did not7,11,13—might have occurred because of the difference in the experimental tasks or in the control strategies that participants individually learned and adopted during training.
Less relative trunk contribution in the early phase of reach-to-grasp movements was found in the dCIT + TR group. Truncal support and restraint may trigger an implicit learning strategy that enabled more normal trunk adapta-tion.7,13,31 A possible reason for decreased trunk segment motion in the middle third of reaching for the task at 125% arm’s length might be that the long reach-to-grasp distance required the generation of high force at the initial stage of the movements.34,35 Trunk assistance at the start of reaching might facilitate higher force generation, and therefore, decreased compensatory trunk motion was shifted to the middle third of reaching.
The positive effects on the distal FMA score were paral-leled by gains in grasping kinematics after dCIT + TR, but not after dCIT, indicating that adding trunk restraint to dCIT helps augment the treatment effects on UE motor function, especially distally. As with the kinematic improve-ments, FMA gains in distal UE motor function may rely on developing more normal movement strategies rather than just adapting to compensatory or undesired movement pat-terns. The dCIT + TR and dCIT interventions showed similar beneficial effects in the AOU and QOM scores of the MAL, but this test includes few activities requiring UE–trunk motion.13 Moreover, the dCIT participants might successfully achieve the tasks required in the MAL by com-pensatory movements.
A few study limitations are of note. First, our sample size was too small to reach a definite conclusion, and the find-ings may not be generalized beyond the scope of the par-ticular participants in the study. Second, we did not address retention of the intervention effects. In addition, our
therapies excluded practice at distances farther than 125% arm’s length and sideways reaching.36
ConclusionThis study demonstrated the additional benefits of trunk restraint when integrated into dCIT to improve the control of grasp and decrease truncal compensatory motion. Both, the dCIT + TR and dCIT, led to more improvement on functional use of the affected arm than the control therapy. The findings suggest the need for further research in a broader population and for outcome measures that best reflect gains in UE-truncal activities.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the National Health Research Institutes (NHRI-EX99-9920PI and NHRI-EX100-10010PI) and the National Science Council (NSC-97-2314-B-002-008-MY3, NSC-97-2314-B-182-004-MY3, and NSC-99-2314-B-182-014-MY3) in Taiwan.
References
1. Massie C, Malcolm MP, Greene D, Thaut M. The effects of constraint-induced therapy on kinematic outcomes and com-pensatory movement patterns: an exploratory study. Arch Phys Med Rehabil. 2009;90:571-579.
2. Wolf SL, Winstein CJ, Miller JP, et al. Retention of upper limb function in stroke survivors who have received con-straint-induced movement therapy: the EXCITE randomised trial. Lancet Neurol. 2008;7:33-40.
3. Lin KC, Wu CY, Wei TH, Lee CY, Liu JS. Effects of modi-fied constraint-induced movement therapy on reach-to-grasp movements and functional performance after chronic stroke: a randomized controlled study. Clin Rehabil. 2007;21: 1075-1086.
4. Page SJ, Levine P, Leonard A, Szaflarski JP, Kissela BM. Modified constraint-induced therapy in chronic stroke: results of a single-blinded randomized controlled trial. Phys Ther. 2008;88:333-340.
5. Wu CY, Chuang LL, Lin KC, Chen HC, Tsay PK. Random-ized trial of distributed constraint-induced therapy versus bilateral arm training for the rehabilitation of uper-limb motor control and function after stroke. Neurorehabil Neural Repair. 2011;25:130-139.
6. Koyama T, Sano K, Tanaka S, Hatanaka T, Domen K. Effec-tive targets for constraint-induced movement therapy for patients with upper-extremity impairment after stroke. Neuro-Rehabilitation. 2007;22:287-293.
at NATIONAL TAIWAN UNIV LIB on August 20, 2012nnr.sagepub.comDownloaded from
Wu et al 255
7. Michaelsen SM, Luta A, Roby-Brami A, Levin MF. Effect of trunk restraint on the recovery of reaching movements in hemiparetic patients. Stroke. 2001;32:1875-1883.
8. Levin MF, Michaelsen SM, Cirstea CM, Roby-Brami A. Use of the trunk for reaching targets placed within and beyond the reach in adult hemiparesis. Exp Brain Res. 2002;143:171-180.
9. Levin MF, Kleim JA, Wolf SL. What do motor “recovery” and “compensation” mean in patients following stroke? Neu-rorehabil Neural Repair. 2009;23:313-319.
10. Michaelsen SM, Dannenbaum R, Levin MF. Task-specific training with trunk restraint on arm recovery in stroke: ran-domized control trial. Stroke. 2006;37:186-192.
11. Michaelsen SM, Levin MF. Short-term effects of practice with trunk restraint on reaching movements in patients with chronic stroke: a controlled trial. Stroke. 2004;35:1914-1919.
12. Thielman G, Kaminski T, Gentile AM. Rehabilitation of reaching after stroke: comparing 2 training protocols utiliz-ing trunk restraint. Neurorehabil Neural Repair. 2008;22: 697-705.
13. Woodbury ML, Howland DR, McGuirk TE, et al. Effects of trunk restraint combined with intensive task practice on post-stroke upper extremity reach and function: a pilot study. Neu-rorehabil Neural Repair. 2009;23:78-91.
14. Alberts JL, Saling M, Stelmach GE. Alterations in transport path differentially affect temporal and spatial movement parameters. Exp Brain Res. 2002;143:417-425.
15. Subramanian SK, Yamanaka J, Chilingaryan G, Levin MF. Validity of movement pattern kinematics as measures of arm motor impairment poststroke. Stroke. 2010;41:2303-2308.
16. Murphy MA, Willen C, Sunnerhagen KS. Kinematic variables quantifying upper-extremity performance after stroke during reaching and drinking from a glass. Neurorehabil Neural Repair. 2011;25:71-80.
17. Bogard K, Wolf S, Zhang Q, Thompson P, Morris D, Nichols-Larsen D. Can the Wolf Motor Function Test be streamlined? Neurorehabil Neural Repair. 2009;23:422-428.
18. Cirstea MC, Levin MF. Compensatory strategies for reaching in stroke. Brain. 2000;123:940-953.
19. Grosskopf A, Kuhtz-Buschbeck JP. Grasping with the left and right hand: a kinematic study. Exp Brain Res. 2006;168: 230-240.
20. Fugl-Meyer AR, Jaasko L, Leyman I, Olsson S, Steglind S. The post-stroke hemiplegic patient. 1. A method for evaluation of physical performance. Scand J Rehabil Med. 1975;7:13-31.
21. Duncan PW, Propst M, Nelson SG. Reliability of the Fugl-Meyer Assessment of sensorimotor recovery following cere-brovascular accident. Phys Ther. 1983;63:1606-1610.
22. Hsieh YW, Wu CY, Lin KC, Chang YF, Chen CL, Liu JS. Responsiveness and validity of three outcome measures of
motor function after stroke rehabilitation. Stroke. 2009;40: 1386-1391.
23. Rabadi MH, Rabadi FM. Comparison of the action research arm test and the Fugl-Meyer assessment as measures of upper-extremity motor weakness after stroke. Arch Phys Med Reha-bil. 2006;87:962-966.
24. van der Lee JH, Beckerman H, Knol DL, de Vet HCW, Bouter LM. Clinimetric properties of the motor activity log for the assessment of arm use in hemiparetic patients. Stroke. 2004;35:1410-1414.
25. Uswatte G, Taub E, Morris D, Light K, Thompson PA. The Motor Activity Log-28: assessing daily use of the hemiparetic arm after stroke. Neurology. 2006;67:1189-1194.
26. Hammer AM, Lindmark B. Responsiveness and validity of the Motor Activity Log in patients during the subacute phase after stroke. Disabil Rehabil. 2010;32:1184-1193.
27. Lang CE, Edwards DF, Birkenmeier RL, Dromerick AW. Estimating minimal clinically important differences of upper-extremity measures early after stroke. Arch Phys Med Reha-bil. 2008;89:1693-1700.
28. Rosenthal R, Rosnow RL. Essentials of Behavioral Research: Methods and Data Analysis. 2nd ed. New York, NY: McGraw- Hill; 1991.
29. Cohen J. Statistical Power Analysis for the Behavioral Sci-ences. 2nd ed. Hillsdale, NJ: Lawrence Erlbaum; 1988.
30. Malcolm MP, Massie C, Thaut M. Rhythmic auditory-motor entrainment improves hemiparetic arm kinematics dur-ing reaching movements: a pilot study. Top Stroke Rehabil. 2009;16:69-79.
31. Ma S, Feldman AG. Two functionally different synergies dur-ing arm reaching movements involving the trunk. J Neuro-physiol. 1995;73:2120-2122.
32. Bernstein N. The Coordination and Regulation of Movements. New York, NY: Pergamon Press; 1967.
33. Turvey MT, Shaw RE, Mace W. Issues in the theory of action: degrees of freedom, coordinative structures and coalitions. In: Requin J, ed. Attention and Performance VII. Hillsdale, NJ: Lawrence Erlbaum; 1978:557-595.
34. Dean C, Shepherd R, Adams R. Sitting balance I: trunk-arm coordination and the contribution of the lower limbs during self-paced reaching in sitting. Gait Posture. 1999;10:135-146.
35. Rohrer B, Fasoli S, Krebs HI, et al. Movement smooth-ness changes during stroke recovery. J Neurosci. 2002;22: 8297-8304.
36. Verheyden G, van Duijnhoven HJ, Burnett M, Littlewood J, Kunkel D, Ashburn AM. Kinematic analysis of head, trunk, and pelvis movement when people early after stroke reach side-ways [published online ahead of print March 30, 2011]. Neu-rorehabil Neural Repair. doi:10.1177/1545968311401628.
at NATIONAL TAIWAN UNIV LIB on August 20, 2012nnr.sagepub.comDownloaded from
Related Documents











