PICU Primer II Kevin M. Creamer M.D. Pediatric Critical Care Walter Reed AMC

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PICU Primer II
Kevin M. Creamer M.D.
Pediatric Critical Care
Walter Reed AMC

The Primer Outline
Physiology
– Hypoxia / Hypoxemia– ABG’s and Acidosis
– Sodium and H2O metabolism
– Hemodynamics and Cardiopulmonary interactions
ICU Care
– Postoperative issues
– Mechanical Ventilation
Common Problems – Head trauma– Toxicology
Postoperative Issues Borrowed in part from Akron syllabus Know the surgery
– what can you expect from a posterior spinal fusion is different than a tracheal reconstruction
Know the patient– Age, PMHx, Syndromes
Be there when they get out of the OR

Postoperative Evaluation
ABC’s Look at the breathing pattern Listen to the chest--breath sounds,
stridor? Listen to the heart--gallop, murmur? Feel the pulses--strong, weak, thready?
– Cap refill?, Extremity warmth?

The Anesthesia Report “History of present illness” for surgical
patients– Difficulties with induction or intubation?– Drugs used during case– Regional techniques employed?– Extubation-problems?
Vital signs- BP, HR, RR, SaO2, temp– Patients are frequently cold!

The Anesthesia Report
Ventilation parameters/difficulties Fluids--ins and outs Any “events”? Lines and tubes

Intraoperative Fluids Pediatrician: “Why do they always get
so much fluid?” Anesthesiologist: “Because they need
it”– maintenance + replacement of “third
space” losses• “third space” losses can be 15 cc/kg/hr
+ replacement of 3 X blood loss

Anesthesia and Fluid Balance
General anesthesia produces vasodilation and some decrease in myocardial contractility.
Increased intrathoracic pressure, and stress response to surgical stimulus, may lead to increased ADH production and decreased urine output

BLOOD loss and replacement
Blood loss is estimated Transfusion Criteria - it depends
– Check Hct, HR, UOP, pH, ongoing loss, Hemodynamics …
When do you need Component Tx?– after a “massive” transfusion or ( 0.75-
3.0 blood volumes)

Blood Products - How much?
PRBCs - 4cc/kg of will Hb 1gm/dl Platelets - 1unit/5kg will count by
50000 FFP - 10 ml/kg round up/down to
closest unit Cryoprecipitate - 1bag/every 5-10kg
Surgeons get extremely persnickety if you transfuse THEIR patient without letting them know ahead of time!

The Surgical Report Since we are not surgeons we need to know
what they anticipate and worry about– Amount of pain – Third spacing– Possible complications
Their wish list:– Extubate tomorrow, MRI at midnight– Special meds: antibiotic and stress ulcer
prophylaxis

The Surgical Report What to touch and not to touch?
– NG, foley, chest tube, rectum, etc. Check all their orders for appropriate
dosing and fluids– mg/kg/dose is not in surgical vocabulary
Who is in Charge? (Us vs. Them) Surgical POC?
– Interface with surgeons before they return to the OR in AM regarding the plan

Assessment of Fluid Balance:
Vital signs (HR/BP) Urine output Extremity warmth, CRT Acid-base status Occasionally invasive monitoring
– Remember the Liver!

Extubation Time? Adequate airway (edema? ,Leak?) Maintain oxygenation and ventilation Neurologically able to protect the
airway and maintain adequate drive. Small/young infants are at increased
risk of apnea– Especially if post-conceptual age <
50weeks

Sedation and Analgesia Analgesia for painful diseases and
procedures Compliance with controlled ventilation
and routine intensive care Sedation for amnesia for the periods of
noxious stimuli Reduce the physiologic responses to
stress

Sedation and Analgesia The idea of titrating drugs to effect--
there is no “dose”.– Keep in mind what the “target” response is.
Consider Round-the-clock Tylenol for 24-48 hours as adjunct– First PR dose may be 30-40 mg/kg
Anesthesia service manages Epidurals Consider a continuous drip

Drug Morphine Fentanyl Versed Ativan
Dose 0.05- 0.1mg/kg
0.5- 1.0mcg/kg
0.05- 0.1mg/kg
0.05- 0.1mg/kg
Timing(I/S)
5-10 min /2-4 hours
5-10 min/ 1-2
hours
5-10 min /1-2 hours
5-10 min /2-4 hours
Sideeffects
BP, H, A A, CWR BP, A BP, A
Reversal Narcan 2-10 mcg/kg
Narcan 2-10mcg/kg
Flumazenil0.1-0.2 mg
Flumazenil0.1-0.2 mg
BP: hypotension, H: Histamine, A: Apnea,
CWR: chest wall rigidity

Muscle Relaxants They provide ZERO sedation/analgesia. Indications (always relative)
– Mechanical ventilation where risk of extubation is great, or risk of baro/volutrauma is high
– Procedures such as central line placement or biopsy in the intubated patient
– Intractable intracranial hypertension (IF ICP being monitored)

Problems with Blockade Fluid retention Long term weakness
– continuous infusions – most commonly the steroid based NMBs – myopathy associated with Atracurium– consider using cis-Atracurium
Consider Train of Four testing FREQUNTLY OVERUSED

NEXT UP
– Mechanical ventilation
This is not the NICU!

Lesson Learned:VALI –Predisposing Factors High lung Volumes
– With high peak pressure and alveolar overdistension
Repeated alveolar collapse and reopening
High inspired oxygen Concentrations Preexisting lung injury
Slutsky Am J Resp CCM, 1999, Dreyfuss Am J Resp CCM 1998

Mechanical Ventilation
Do’s and Don’ts– Avoid Overdistension and High Pressure by
limiting Tv– Avoid Hyperoxic Lung damage by turning FIO2
down (Sat 90% okay)– Avoid cyclic collapse by using PEEP to recruit
FRC and keep it above Closing volume Infant high risk 2° high elastic recoil and
complaint chest wall

Zone of Overdistension
Zone of Atelectasis
Open Lung Strategy

Getting Started (Parameters)Oxygenation Ventilation (MV)
PEEP Rate
I-time (flow) Tidal Volume (P)
FIO2

Getting Started (Mode)Volume Pressure
Pro’s Preserve MV Avoid PP
Easy Familiar (NICU)
Decelerating Flow
Con’s PP ?? MV??
Constant flow

Constant vs. Decelerating flow
Time
F L O w
Time
F L O w
Time
P R E S S U R E
Time
P R E S S U R E

Getting Started (Settings)
FIO2 - 50%, if sick 100%
It - minimum .5 sec, older kids 1 sec Rate - age appropriate 15 -30 to start Tv - 10ml/kg to start Look / Listen / Ask PEEP - 4cm, higher if FRC
compromised

IT and Time Constants
• The time to fill each alveolus is determined by its time constant
• TC= Resistance X Compliance
• A Short IT decreases TV, or increases PIP
Full equilibration
IE
EI
TT
TPEEPPIPTMAP
)()(

Mechanical Ventilation First hour
– CXR and “Blood Gas”– Watch peak pressures as compliance
estimate• PP << 20 ideal• PP 20-30 moderately compliance• PP >> 30 severely compliance• PP >> 35 high risk for VALI, DO
SOMETHING

Mechanical Ventilation
Change Tv only for inappropriate chest rise or for elevated inspiratory pressures (Don’t WEAN Tv)
Sedation to allow patient - ventilator synchrony (Paralytics aren’t required)

Monitoring adjuncts Pulse oximeter End tidal CO2 - can use for Dead space
estimate ABG’s and CBG’s Calculate Compliance, A-a gradient,
Oxygenation Index (OI), check for Autopeep
Graphics - PV and flow-volume loops

Equations
Dead Space = 1 - (EtCO2/PaCO2)
Static Comp. = Tv/ (Pplat- PEEP)
A-a gradient =
– (Pb-PH2O) x FIO2 - (PCO2/.8) - PaO2
OI = (Paw x FIO2 x 100)/ PaO2

When things go wrong Don’t be a DOPE Hypoxemia - PEEP to FRC, to allow FIO2
wean to < 50% Elevated peak pressures - suction, adopt
Permissive hypercapnia, consider changing to pressure mode
Check circuit size– an inappropriately large circuit can gobble up
lots of tidal volume

PEEP
PIP
TI
RateFlow
Pressure
TimeTI TE
PEEP
PIP
Paw (Area Under Curve )increases with increasing:PIP, PEEP, TI/TE Ratio, Rate, and
Flow

Circuit compliance
When using volume ventilation the ventilator circuit or tubing will stretch – Neonatal 0.35 ml / cm H2O
– Pediatric 1.4 ml / cm H2O
– Adult 2.8 ml / cm H2O
This means the stiffer the lung the more volume is lost in the circuit

Mechanical Ventilation First day and beyond
– Watch for fluid overload• all patients on positive pressure ventilation retain
lung water
– Assist patient efforts• Pressure support or volume support
• Trigger sensitivity (age and disease appropriate)
– Treat underlying condition– Feed patient

Weaning Get condition under control Stop paralytics (PEEP < 8) Encourage patient’s efforts
Rate (slow then fast)– add Pressure support (2/3 P)
Wean PEEP and PS slowly in 1-2 cm H2O increments
Wean FIO2 to 30% if possible

Signs of weaning failure
Increased Work of breathing– fast spontaneous RR
– small spontaneous Tv
Increased FIO2requirement
Hemodynamic compromise

Time for Extubation?
Think SOAP– Secretions / Sedation / Spontaneous Tv
(>5ml/kg)
– Oxygenation <35%
– Airway - Maintainable?, Leak? , Steroids?
– Pressures - PP <25, PEEP < 5

Extubation success predictors
Variable Low risk <10% High Risk >25%
VTspont
>6.5 ml/kg <3.5 ml/kg
FIO2 <.30 >.40
OI <1.4 >4.5
PIP <25 >30
Khan, CCM 1996Khan, CCM 1996

Special situations I
Obstructive Diseases– Asthma and RSV Bronchiolitis
– Watch for air trapping / breath stacking• Low rate, larger Tidal volume, long
Expiratory time• check Autopeep• preserve I-time • Consider Heliox, Ketamine, Halothane

Special situations II ARDS
– Limit Tv accept hypercapnia– Increase PEEP for FRC– Prone positioning CaO2 and tolerate lower Sat %– consider High Frequency Oscillatory
Ventilation>>> Surfactant>>> Nitric Oxide
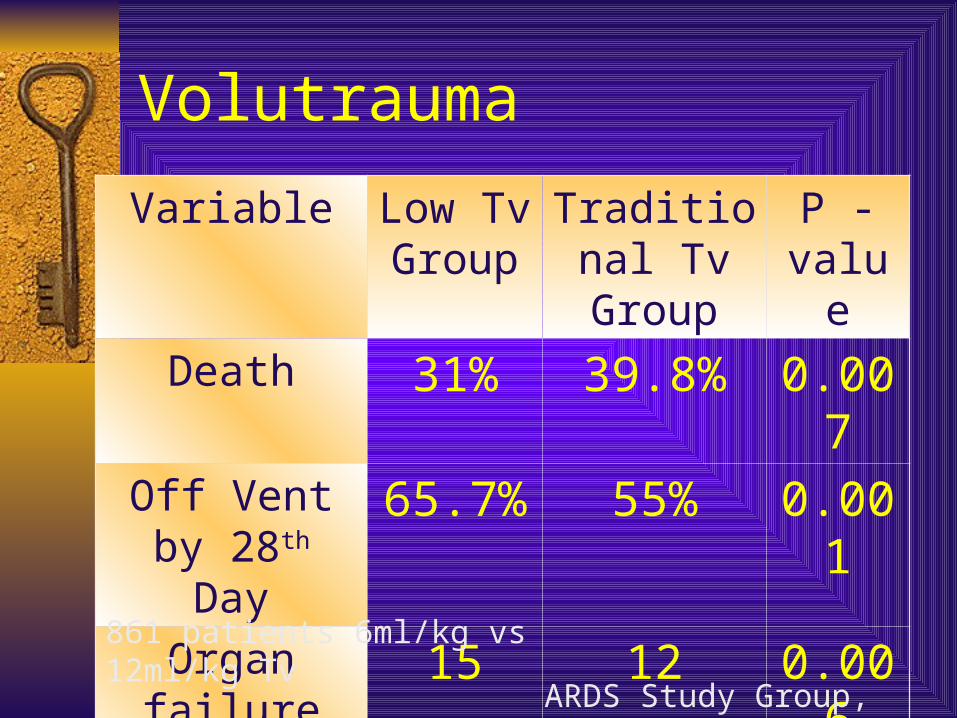
Volutrauma
Variable Low Tv Group
Traditional Tv Group
P - value
Death 31% 39.8% 0.007
Off Vent by 28th Day
65.7% 55% 0.001
Organ failure free days
15 12 0.006
861 patients 6ml/kg vs 12ml/kg Tv
ARDS Study Group, NEJM, 2000

Biotrauma
RCT 44 adults with ARDS– TV 7.6 vs. 11.1
– PP 24 vs. 31 cm H2O
At 36° patients in low TV group had significantly lower levels of TNF and IL-1ra in both plasma and BAL fluid
0
5
10
15
20
25
30
35
40
StandardTV
Low TV
Organ Failure
Entry
3-4 days
Ranieri, JAMA,1999; Ranieri JAMA, 2000
Organ Failure

Special situations III
Head Trauma– Avoid Hypercarbia (PCO2 < 35)
– Avoid Hypoxemia
– PEEP may adversely effect venous return and ICP
– Coughing/gagging extremely bad (Use paralytics)

Special situations IV HFOV Indications
– ARHF with OI > 13 for 6 hours– Contraindicated in High airway
resistance, ICP, unstable hemodynamics
Part of an Open lung strategy with Mean airway pressure and Tv < dead space

HFOV vs. CMV
Crossover study acute hypoxemic respiratory failure in children
HFOV 17/29 responded, 0/17 died CMV 10/29 responded, 4/10 died X-over to HFOV 11/19 survived X-over to CMV 2/11 survived
Arnold, CCM 1994Arnold, CCM 1994

Ventilation Simulator
Not for the weak of heart

The EndMind what you have
learned. Save you it can.

Questions?
Related Documents











