PRESENTER: DR VARSHA V. HIRANI FACILITATOR: PROF. MUSOKE

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
PRESENTER: DR VARSHA V. HIRANI
FACILITATOR: PROF. MUSOKE
OBJECTIVES:
Understand the structure of the breast
Describe the stages of lactation
Composition of breast milk
Factors affecting lactation
Medications that affect lactation
2
Definition of lactationLactation describes the production of breast milk and its secretion from the mammary gland after delivery
3
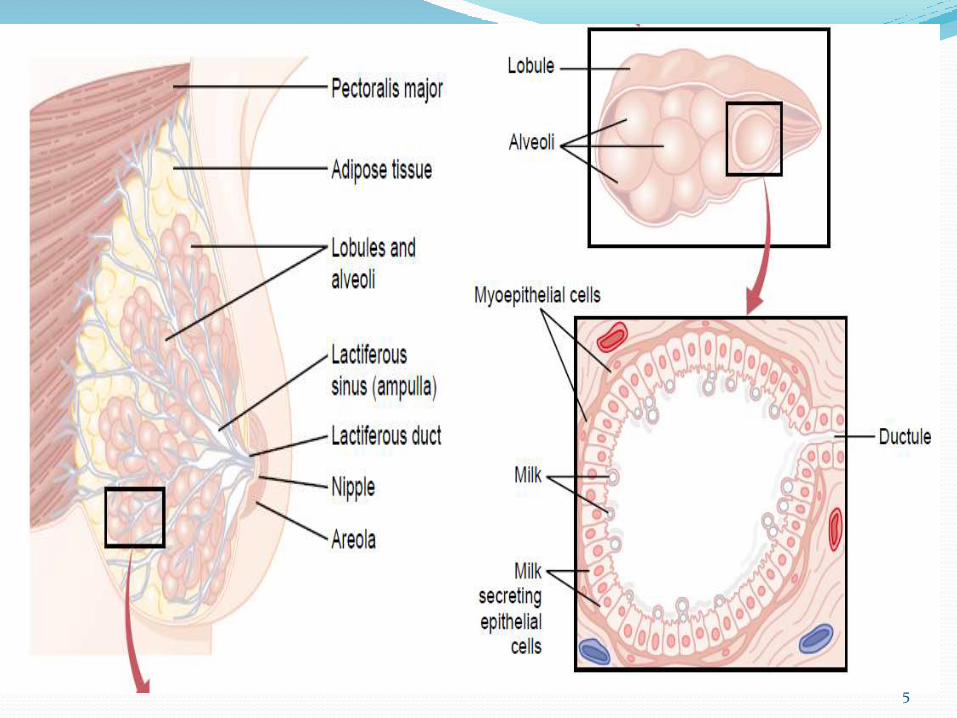
Structure of the breast Parenchyma consists of 10-15 ducts extending from
the nipple to terminate in grape-like clusters known as alveoli (basic unit) via ductules from lobules
There are 15-20 pyramid shaped lobes separated by cooper ligament and each contains lobules which are further separated by fat and connective tissue(stroma)
Nipple surrounded by area of hyperpigmented skin –areola
4
5
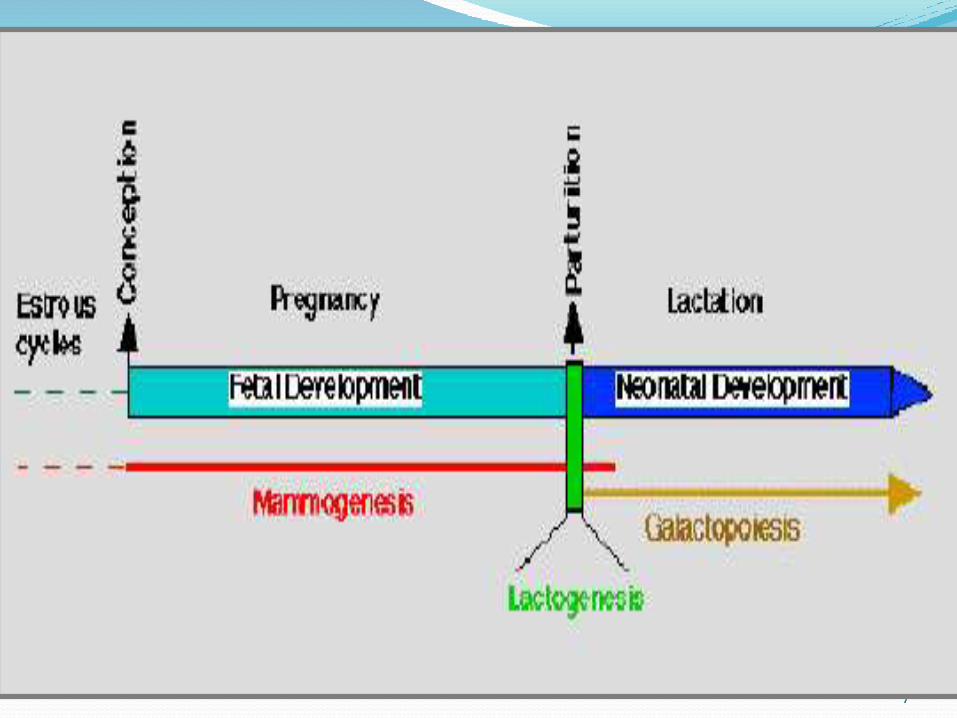
Physiology of Lactation.Lactation can be divided into 5 stages:
1. Mammogenesis-Development of breasts to a functional state
2. Lactogenesis-Synthesis and secretion of milk from the breast alveoli
3. Galactokinesis-Ejection of milk outside the breast
4. Galactopoiesis-Maintenance of lactation
5. Involution-regression and atrophy post lactation
6
7
1.Mammogenesis Growth of ducts and lobuloalveolar systems
This starts from birth to puberty and continues in pregnancy
Ductal sprouting predominates in 1st trimester and lobular sprouting occurs more in 2nd trimester hence the breast will contain more glandular epithelial cells than stroma
Just before and during parturition there is a new wave of mitotic activity causing growth growth and maturation
8
Hormonal influence during mammogenesisPrepubertal growth-
depends on estrogen and progesterone.
Secretion of prolactin and somatotropin by the pituatory gland results in mammary growth.
Adrenocorticotrophic hormone(ACTH) and thyroid stimulating hormone(TSH) acting on the adrenal gland and thyroid gland also play a minor role in growth of the mammary gland
9
10
Pubertal growth-
When the hypophyseal-ovarian –uterine cycle is established, there is extensive branching of the duct system and parenchymal proliferation and canalization of the lobuloalveolar units controlled by estrogen and progesterone
Hormonal influence during mammogenesis…
11
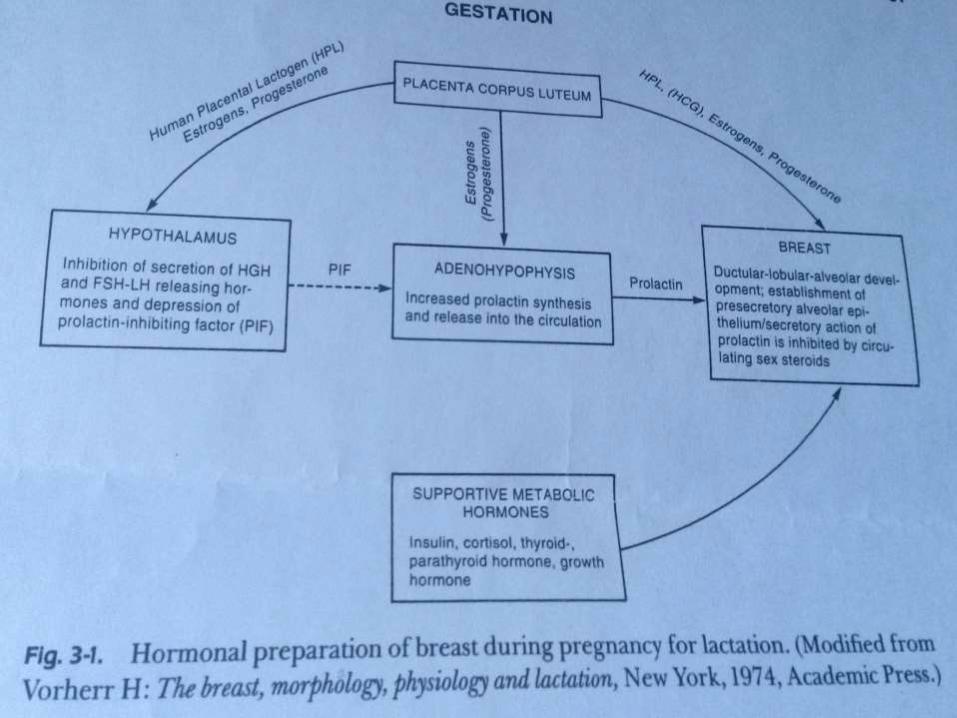
During pregnancy
In early pregnancy a marked increase in ductular sprouting, branching and lobular formation is evoked by luteal and placental hormones.
Progesterone:causes increased growth of alveoli size and lobes,
Estrogen:Stimulates milk duct system to grow and differentiate, deposition of fat.
Prolactin:contributes to increased growth and differentiation of the alveoli and ductal structures
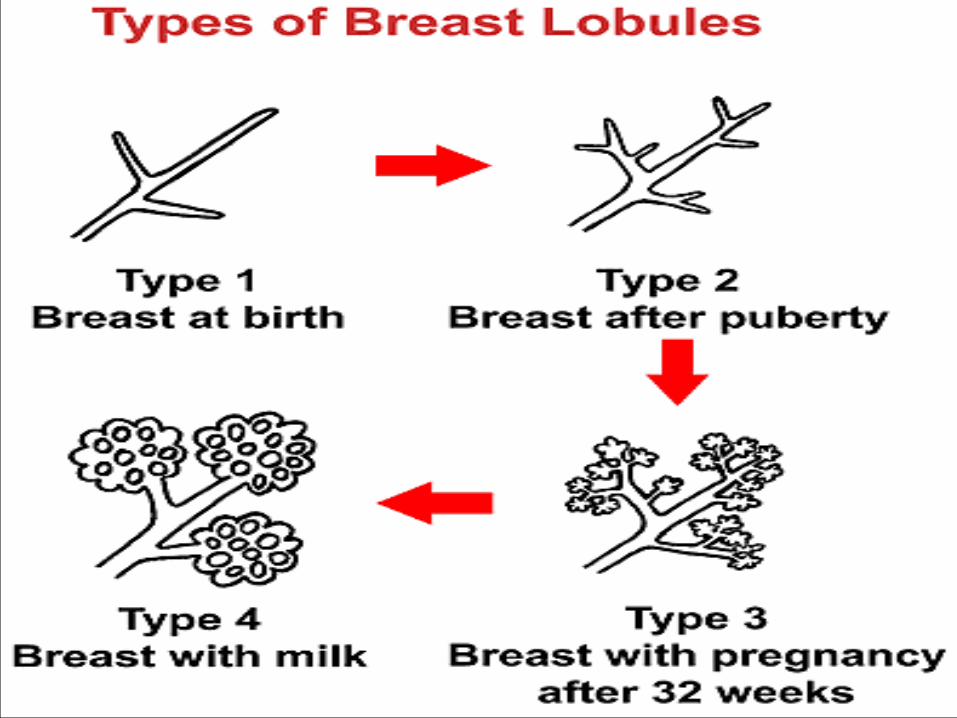
Types of lobules Type 1- (virginal lobule) when an average of 11 alveolar
buds/ductules cluster around a terminal duct, this is apparent within 1 to 2 years after onset ofmenses
Type 2 - changing levels of estrogen and progesteron during menstrual cycle stimulates type 1 lobules to sprout new alveolar buds and evolve to mature structures, type 2-47 lobules
Type 3- in pregnancy, 80 lobules
Type 4-attained in late pregnancy with breast milk
12
13
2. LACTOGENESIS(stage 1)Stage 1: occurs in mid pregnancy
There is initiation of milk synthesis,
alveoli differentiates into secretory cells and prolactin stimulates mammary secretory cells to produce milk.
insulin and serum growth factor induced cell division of stem cells of the gland and presence of cortisol for formation of alveoli is required for induction of milk synthesis .
Further differentiation is inhibited by high levels of progesterone from the placenta and loss of progesterone receptors in the lactating breast
14
Prolactin: exerts its effects through receptors for initiation of milk
secretion located on the alveolar surfaces. stabilizes and promotes transcription of mRNA and
stimulates synthesis of lactoalbumin, which is a regulatory protein of the lactose synthetase enzyme system
Increases lipoprotein activity in the mammary gland In conjunction with estrogen and progetserone it attracts
and retain Ig-A immunoblasts estrogen enhances prolactin production by 10-20 fold. This
is regulated by human placental lactogen which has an inhibitory effect
Its inhibited by prolactin inhibiting factor under control of catecholamines in the hypothalamus.
15
LACTOGENESIS-stage 2 Stage 2: from late pregnancy to day 8.
This is triggered by rapid drop in progesterone levels after placental delivery
requires the presence of elevated levels of prolactin and cortisol , insulin, growth hormone and parathyroid hormone to facilitate mobilization of nutrients and minerals
there is a switch from endocrine to autocrine control
16
2. Lactogenesis. Pathways for milk secretion by the mammary epithelial cellI - Exocytosis : milk protein and lactose are
transported in Golgi-derived secretory vesicles, with water and electrolytes in to the alveolar lumen
II – Reverse Pinocytosis: lipid formed in smooth ER forms droplets and covered by phospholipid membrane transported as milk-fat globule
III – Apical transport: Direct movement of monovalent ions, water, and glucose across the apical membrane of the cell.
17
Lactogenesis……IV – Transcytosis. sodium, potassium,
chlorides, some monosaccharides, and water
V - The paracellular pathway for some interstitial fluid components and leukocytes to pass by diapedesis through the tight junctions.
18
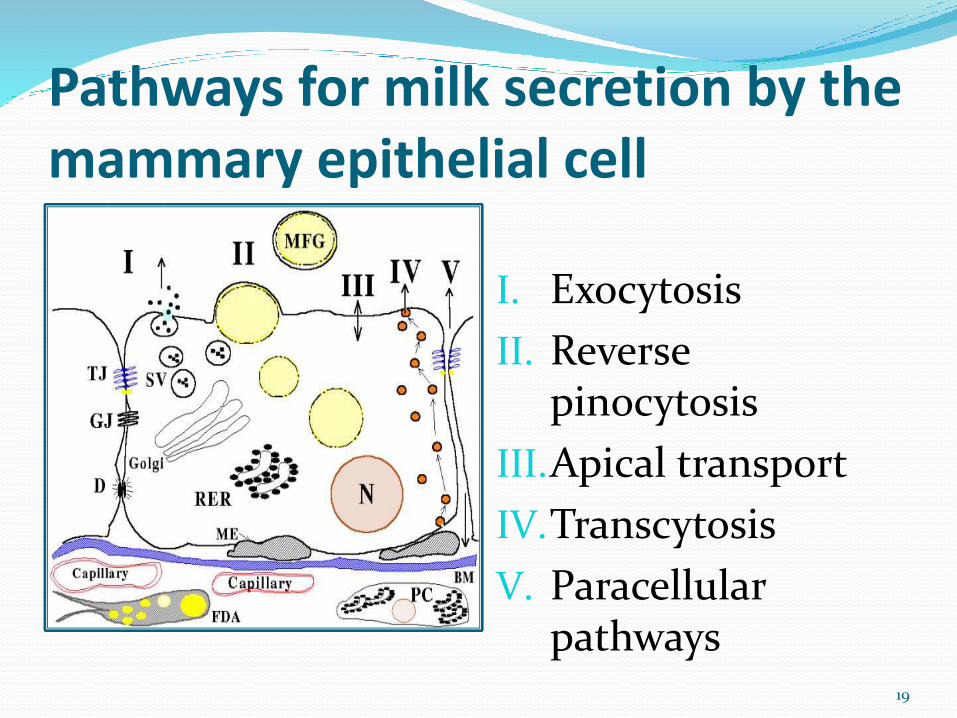
Pathways for milk secretion by the mammary epithelial cell
I. Exocytosis
II. Reverse pinocytosis
III.Apical transport
IV.Transcytosis
V. Paracellular pathways
19
20
galactokinesis• Depends on the suckling mechanism of the
baby and the contractile action which will express milk from the alveoli into the ducts.
• This contraction is brought about by the action of Oxytocin
• Milk let down reflex/milk ejection reflex
• Inhibited by psychic condition /pain /breast engorgement
21
oxytocin: Released from posterior lobe of the pituatory gland
during nipple stimulation or sensory stimulation( visual, tactile , olfactory or auditary)
Causes ejection of milk from the alveoli gland by contraction of the myoepithelial cells into ductules and ducts
22
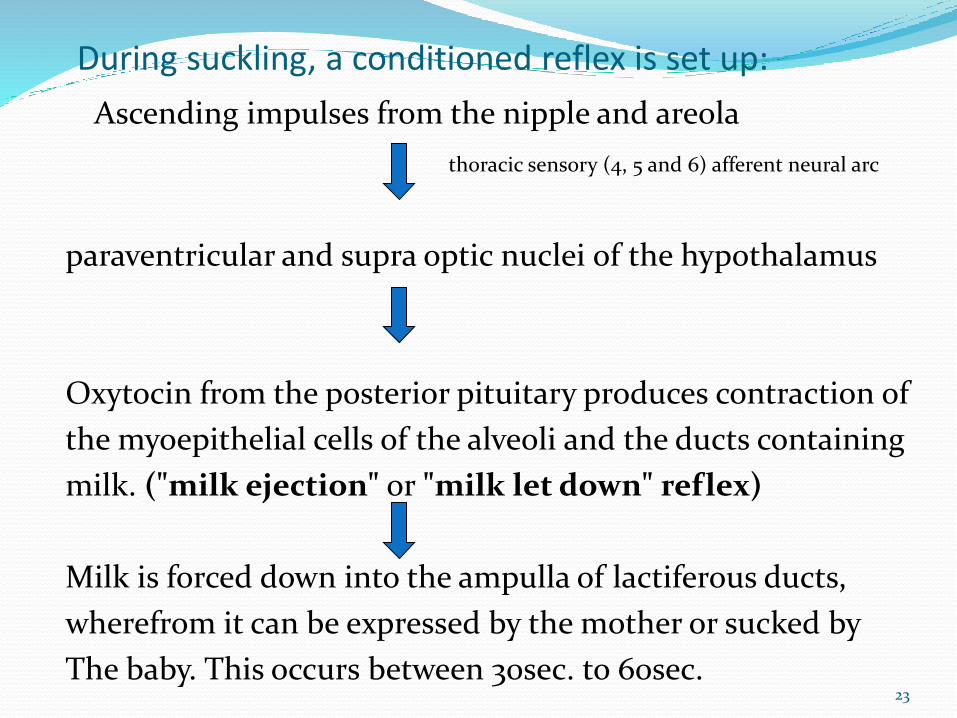
Ascending impulses from the nipple and areola
thoracic sensory (4, 5 and 6) afferent neural arc
paraventricular and supra optic nuclei of the hypothalamus
Oxytocin from the posterior pituitary produces contraction of
the myoepithelial cells of the alveoli and the ducts containing
milk. ("milk ejection" or "milk let down" reflex)
Milk is forced down into the ampulla of lactiferous ducts,
wherefrom it can be expressed by the mother or sucked by
The baby. This occurs between 30sec. to 60sec.
During suckling, a conditioned reflex is set up:
23
24
Galactopoiesis.Prolactin is the hormone for maintenance of
lactation
And suckling is essential for maintenance of milk secretion
Periodic breast feeding relieves pressure in the ducts and promotes more secretion
Controlled by autocrine system(supply-demand)
25
5. Involution Apoptotic cell death and tissue remodelling
post lactation
Requires a combination of lactogenic hormone deprivation and local signals to undergo regression and atrophy
26
27
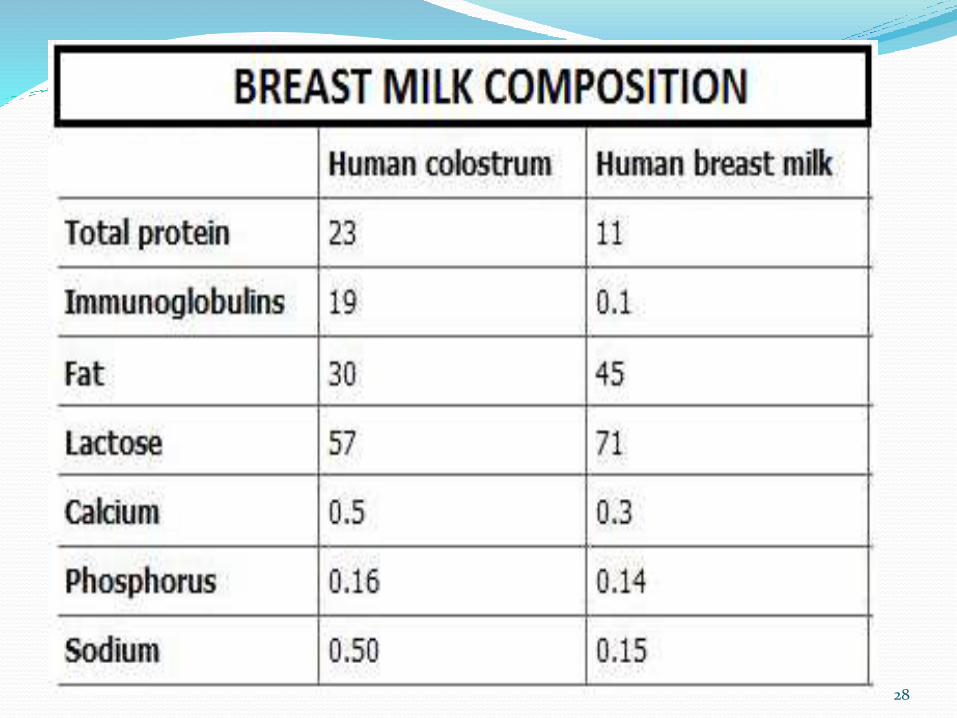
Variations in composition :Colostrum(1-5 days) – is reacher in proteins ,minerals,
immunoglobulins , anti inflammatory factors(PGE1 and PGE2, cytokines), phagocytes and lymphocytes.
Mature milk(>30 days)-larger quantity than colostrum,
Foremilk –thin, proteins, lactose, water and other nutrients.
Hindmilk –more fat therefore whiter, provides much of the energy of a feed.
Other components include human growth factors, cortisol, insulin, thyroxine and prolactin
28
FACTORS AFFECTING LACTATIONMaternal problems:
stress(post c/s,stressful vaginal delivery or other psychosocialstresses) opiates and beta-endorphins are released that blockthe stimulus-secretion coupling thus reducing oxytocin release
polycystic ovarian syndrome,
theca lutein cysts,
obesity,
labour analgesia,
dm type 1,
placental retention-increased circulating progesterone
Alcohol dependence
12/7/2014 6:55 PM 29
FACTORS AFFECTING LACTATION.. Infrequent suckling/failure to empty breast
causes Elevated intrammary pressure also disruptsconnections between cells and their attachment tothe basement membrane disrupting synthesis andsecretion of milk components.
Premature infants-prolactin may not besufficient
30
MEDICATIONS AND LACTATIONMedications that increase lactation-
metoclopramide
domperidone
phenothiazine neuroleptics -chlorpromazine
risperine
Hypoglycemics
H2 antagonists-cimetidine
Antihypertensives-methyl dopa, b blockers
31
MEDICATIONS AND LACTATIONMedications that reduce lactation- Bromocryptine(dopamine agonist) Progesterone,estrogen-OCP Clomiphene citrate ergotamine pseudoephedrine(in cough syrups) Pyridoxine Prostaglandins- PGE/F2alpha Levodopa/carbidopa
32
Advise to the mother to improve lactation Good health;
Early and sufficient treatment of illnesses;
Proper balance between rest and exercise;
Freedom from worry
Care of the breast /nipples during pregnancy
Post natally frequent breast feeding
Avoid breast engorgement
Plenty of fluids
Adequate nutrition.
33
Thank you!
ANY QUESTIONS?
35
References
E-medicine – Human milk and lactation.
Breastfeeding and human lactation-Jones and Bartlett Series.
Breast feeding, guide for medical proffesion by Ruth Lawrence.
Related Documents











