Physiological Considerations for Compression Bandaging Harvey N. Mayrovitz, Ph.D. Professor of Physiology College of Medical Sciences Nova Southeastern University [email protected]

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Physiological Considerations for Compression Bandaging
Harvey N. Mayrovitz, Ph.D.Professor of PhysiologyCollege of Medical SciencesNova Southeastern [email protected]

At the completion of this presentation participants will be able to:
1. State the difference between edema andlymphedema
2. State at least one process that can causeedema
3. Describe the basic processes involved inlymphatic transport
4. Describe long-stretch and short-stretchbandages and their use
5. Contrast the effects of resting vs. workingpressures
6. Describe Laplace’s law as it applies tobandaging
Dr. HN Mayrovitz

Relationship to Wound Healing
Impediments to HealingImpediments to Healing• Blood Flow• Oxygenation• Infection• Tissue Environment
Deficit OriginsDeficit Origins• Arterial• Venous• Microvascular• Lymphatic
Compression Therapy
LocalizedEdema/Lymphedema
Dr. HN Mayrovitz

Circulation Schema
H 2O
ArteryArtery
Vein
LymphaticsLymphatics
O2 CO2 CapillaryCapillary
ArteriolesArterioles
Dr. HN Mayrovitz
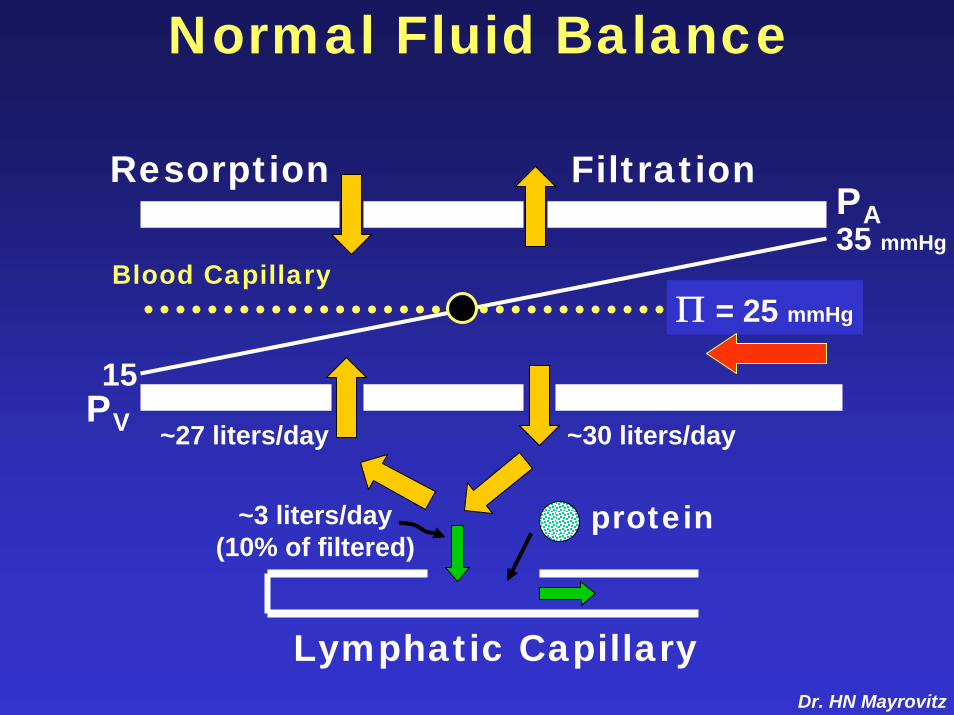
Normal Fluid Balance
35 mmHg
15
Π = 25 mmHg
FiltrationResorption
Lymphatic Capillary
~30 liters/day
PA
PV
protein
Blood Capillary
~27 liters/day
~3 liters/day(10% of filtered)
Dr. HN Mayrovitz

35 mmHg
Filtration
Lymphatic Capillary
Increased Venous Pressureor Capillary Permeability
••Less ResorptionLess Resorption
20PV
PA
•More Filtration
Resorption
Blood Capillary
Dr. HN Mayrovitz

If Net Filtration ExceedsLymphatic Transport Capacity
Overload = Edema+ [Protein]
= Lymphedema= Lymphedema
Therapy Options• Reduce Filtration• Increase Transport
Dr. HN Mayrovitz

Normal Lymph TransportNormal Lymph Transport
••Lymphangion ContractionLymphangion Contraction
••Skeletal Muscle PumpSkeletal Muscle Pump
••Arterial PulsationsArterial Pulsations
••Body MovementsBody Movements
••RespirationRespiration
All are Dynamic ProcessesDr. HN Mayrovitz

Lymphatic Capillaries
EC
Lumen PL
PT
EC
Lumen PL
+PT
PL > PT
PL < PT
AnchoringFilaments Blood Capillary
Lymphatic Capillary
Dr. HN Mayrovitz

Lymphatic ‘Hearts’
ValveLymphangion(lymph micro heart)
LymphCapillary
Walls have amuscular media
Peristaltic-like contractionspropel lymph to next segment
LymphangionLymphCapillary
Contraction force is preload andafterload dependent - analogous to heart
Dr. HN Mayrovitz

Calf Muscle Pump and Calf Muscle Pump and Normal ValvesNormal Valves
Superficial Deep
Rel
axed
FasciaSkin
Superficial Deep
Con
trac
ted
Skin FasciaDr. HN Mayrovitz

Calf Muscle Pump and Valve Dysfunction
Rel
axed
Resting Venous PressureResting Venous PressureINCREASEDINCREASED
VeinsVeinsDistendedDistended C
ontr
acte
d
•• High pressure transmittedHigh pressure transmittedto Superficial Veinsto Superficial Veins
•• Pump Efficiency ReducedPump Efficiency Reduced

Venous Valve DysfunctionChronic venous hypertension due toChronic venous insufficiency (CVI)
predisposes to developing venous ulcersIncreased Ambulatory Venous Pressure
VenousVenousPressurePressure
NormalNormal
CVIResting
Dr. HN Mayrovitz

ExternalCompression
TissueTissuePressurePressure
Vein Vein Diameter
TransTrans--locatelocateVolumeVolume
VenousVenousPressurePressure
Diameter
ArteriolarVasodilation VelocityVelocity
Shear Shear StressStress
NitricOxide Promote
FluidAbsorptionNormalize
PermeabilityWBC WBC
AdherenceAdherenceDr. HN Mayrovitz

Types of Compression
•Bandage
•Bandage-like
•Pumps
•Stockings
Short-StretchLong -Stretch
Short-Stretch
Dynamic
PreventionMaintenance
Dr. HN MayrovitzDr. HN Mayrovitz

Arrangement
Superficial
Facia
Skin
VascularSheath
MuscleDeep
Bone
DrainsSkin andSubcutis
Dr. HN Mayrovitz

Vascular Sheath
V
VA
L
L
Arterial Pulsations Can Mechanically Arterial Pulsations Can Mechanically Augment Lymph TransportAugment Lymph Transport
Dr. HN Mayrovitz

Arterial Flow Pulses Below Knee Blood Flow via Nuclear Magnetic Resonance Below Knee Blood Flow via Nuclear Magnetic Resonance
Control Leg Treated LegControl Leg Treated LegBeforeBefore
Bandage52 47
49 74
ml/min Bandage
WithWithBandageBandage
Increased pulses Increased pulses likely augment likely augment Lymph/venousLymph/venous
transporttransport
ml/min
Dr. HN Mayrovitz

Compartments
SuperficialPosterior
DeepPosterior
Anterior
Lateral
GreaterSaphenous
Lesser Saphenous
PosteriorTibial
Peroneal
AnteriorTibial
Skin
Tibia
Fibula
Want Therapy to Affect Superficial and DeepDr. HN Mayrovitz

Pressures of Interest
Skin
••SubSub--bandagebandage••SurfaceSurface••ContactContact
CompressionBandage or Device
••TissueTissue••InterstitialInterstitial
••IntramuscularIntramuscular
Tibialis m.
Soleus m.
Gastroc m.
Popliteus m.Tibialis m.
Peroneus
Tibia
Fibula
2
3
1
Dr. HN Mayrovitz

Edema and Tissue Pressure
Normal
PT
Loose Fibrous Trabeculae
PT
Dr. HN Mayrovitz
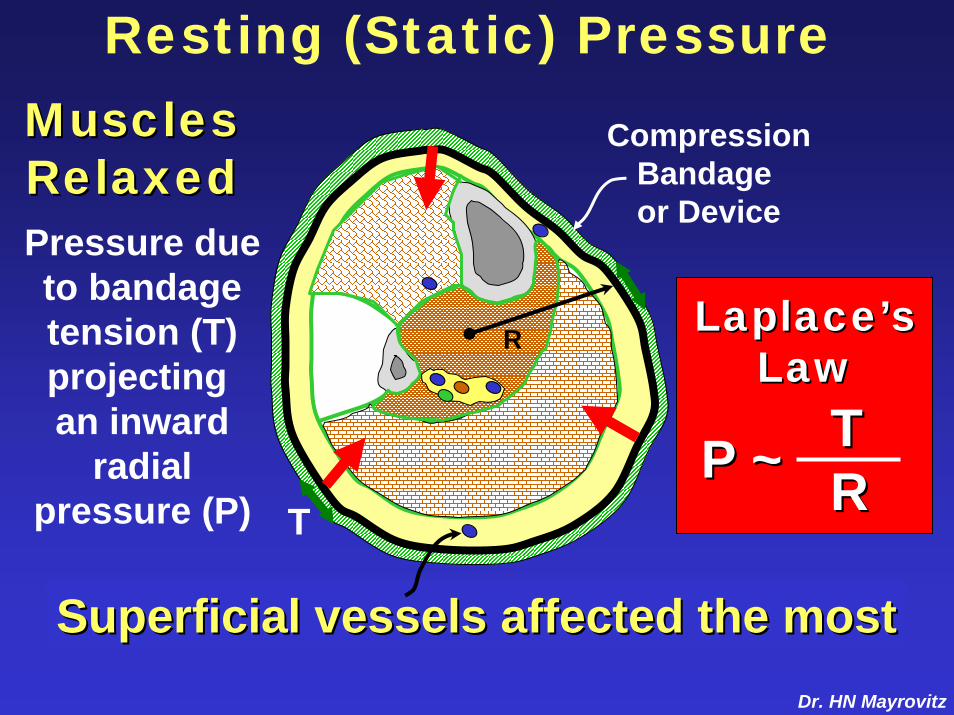
Resting (Static) Pressure
P ~ P ~ TTRR
Superficial vessels affected the mostSuperficial vessels affected the most
LaplaceLaplace’’ssLawLaw
MusclesMusclesRelaxedRelaxed
R
CompressionBandage or Device
T
Pressure dueto bandagetension (T)projecting an inward
radialpressure (P)
Dr. HN Mayrovitz

Pressure Gradient Concept
Compression Appliedat Constant Tension
P ~ P ~ TTRR
Increasing RIncreasing RDecreasing PDecreasing P
Mimics Normal Intravascular
PressureGradient
Dr. HN Mayrovitz

Working (Dynamic) PressureBandage acts as a Bandage acts as a restraint to muscle restraint to muscle
expansion expansion
P ~ Contraction Force x P ~ Contraction Force x ‘‘RigidityRigidity’’
P
ContractedContractedMusclesMuscles
Positive Positive affect on affect on
deeperdeepervesselsvessels
Pressure isPressure isdevelopeddeveloped
from from ‘‘withinwithin’’
Dr. HN Mayrovitz

Dynamic Pressure Depends onBandage Material Features
Bandage ‘Stretchibility’
No externalcompression
0
Form fitted steel pipe
‘shortstretch’
‘longstretch’
Dyn
amic
Pre
ssur
e (∆
P)
Dr. HN Mayrovitz

Working vs. Resting PressuresRole of Compression Material
ShortShortStretchStretch LongLong
StretchStretch
Filling Filling
Resting
Tiss
ue P
ress
ure
(PT)
Time
Emptying
Dr. HN Mayrovitz
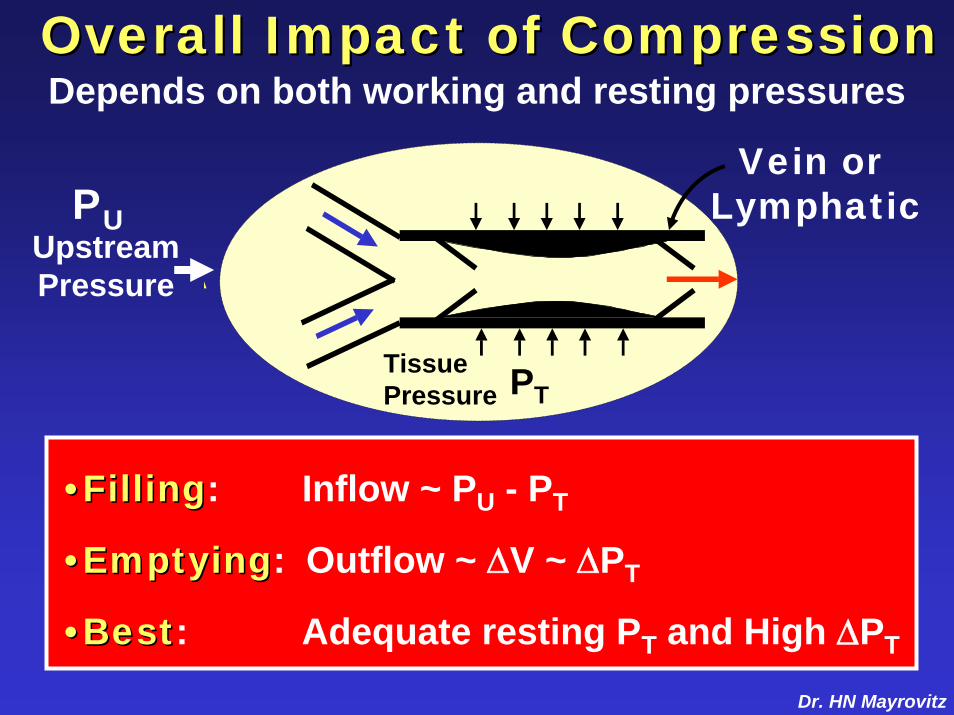
Overall Impact of Compression Overall Impact of Compression Depends on both working and resting pressures
A
PT
PUUpstreamPressure
TissuePressure
Vein or Lymphatic
••FillingFilling: Inflow ~ PU - PT
••EmptyingEmptying: Outflow ~ ∆V ~ ∆PT
••BestBest: Adequate resting PT and High ∆PT
Dr. HN Mayrovitz

PneumaticSensor*
ElectronicSensor*
ElectronicPressureReadout
Sub-Bandage Pressure Measurements
Compression set at various static levels to compare dynamic sub-bandage pressuresachieved with different bandages duringcalf muscle contraction and relaxation
*Pneumatic sensor: Talley Oxford Pressure Monitor*Electronic Sensor: http://bioscience-research.net
Dr. HN Mayrovitz

Dynamic (Working) Pressures
0
150
mm
Hg
30 40 50
Static
Static Pressures Set by Compression
Dynamic pressures via calf muscle contractionDynamic pressures via calf muscle contractionDynamic
CohesiveCohesive ElasticElastic MultilayerMultilayer0
150
mm
Hg
Comparison of Different Bandage TypesInefficient Low
Dynamic Pressure Efficient
Dynamic Pressure
Dr. HN Mayrovitz
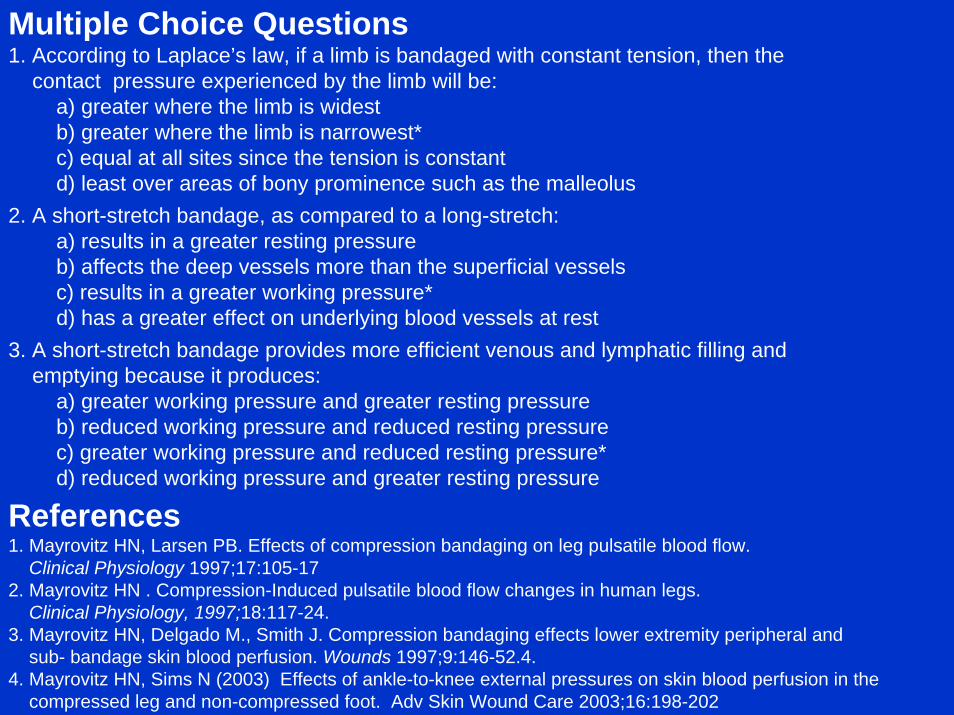
Multiple Choice Questions1. According to Laplace’s law, if a limb is bandaged with constant tension, then the
contact pressure experienced by the limb will be:a) greater where the limb is widestb) greater where the limb is narrowest*c) equal at all sites since the tension is constantd) least over areas of bony prominence such as the malleolus
2. A short-stretch bandage, as compared to a long-stretch:a) results in a greater resting pressureb) affects the deep vessels more than the superficial vesselsc) results in a greater working pressure*d) has a greater effect on underlying blood vessels at rest
3. A short-stretch bandage provides more efficient venous and lymphatic filling andemptying because it produces:
a) greater working pressure and greater resting pressureb) reduced working pressure and reduced resting pressurec) greater working pressure and reduced resting pressure*d) reduced working pressure and greater resting pressure
References1. Mayrovitz HN, Larsen PB. Effects of compression bandaging on leg pulsatile blood flow.
Clinical Physiology 1997;17:105-172. Mayrovitz HN . Compression-Induced pulsatile blood flow changes in human legs.
Clinical Physiology, 1997;18:117-24.3. Mayrovitz HN, Delgado M., Smith J. Compression bandaging effects lower extremity peripheral and
sub- bandage skin blood perfusion. Wounds 1997;9:146-52.4.4. Mayrovitz HN, Sims N (2003) Effects of ankle-to-knee external pressures on skin blood perfusion in the
compressed leg and non-compressed foot. Adv Skin Wound Care 2003;16:198-202
Related Documents











