MUNICIPALITY OF PIRIPIRI MUNICIPAL HEALTH SECRETARIAT HEALTH EVIDENCE TEAM BRASIL SUMMARY OF EVIDENCE # 01/2010 Health Evidence Team of the Piripiri Municipal Health Secretariat (MHS): Almiro Mendes da Costa Neto (Nurse at Piripiri MHS); Carliane Maria de Araújo Souza (Nurse at Piripiri MHS); Evaldo Sales Leal (Nurse at Piripiri MHS); Maria Erinelda de Araújo Souza (Nurse at Piripiri MHS); Michell Lucilane dos Santos Holanda (Nurse at Piripiri MHS); and Yluska Myrna Meneses Brandão e Mendes (Nurse at Piripiri MHS). Coordination: Jorge Otávio Maia Barreto (MSc, Municipal Health Secretary of Piripiri, PI) THEME: Physical activity and prevention/control of arterial hypertension in primary healthcare (Atenção Primária à Saúde, APS). 1 KEY MESSAGES PROBLEM Healthcare in Brazil has invested in formulating, implementing, and putting into practice policies related to the promotion, protection, and recovery of health. In the construction of the primary health care model, great emphasis has been placed on the improvement of the quality of life of collective subjects (Brazil 2006). Improvements in access to and the quality of the services provided by Brazil’s public health service, the Unified Healthcare System (Sistema Único de Saúde), are among the biggest priorities in healthcare, with an emphasis on strengthening the Family Health Program (Programa Saúde da Família). This includes the promotion of good health; health-related information and education; the promotion of physical activity, healthy eating, and healthy lifestyle habits; the control of tobacco and alcohol consumption; and care for the elderly. In Piripiri, the Gym on the Square Project (Projeto Academia na Praça) encouraged the local population to exercise to improve their quality of life. What is the best way, however, to include physical activity in the context of primary healthcare? What type of physical activity is most beneficial? Which groups would benefit the most? How much exercise is recommended? Are there risks related to physical exercise? This summary presents the best available evidence found on physical activity at the individual and community level, and discusses the benefits, obstacles, and implications that physical activity offers. OPTIONS Option 1: Prescription of physical activity as part of primary healthcare to prevent and treat arterial hypertension at the individual level. Option 2: Encouragement of aerobic physical activity at the community level.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
MUNICIPALITY OF PIRIPIRI MUNICIPAL HEALTH SECRETARIAT
HEALTH EVIDENCE TEAM
BRASIL
SUMMARY OF EVIDENCE # 01/2010 Health Evidence Team of the Piripiri Municipal Health Secretariat (MHS): Almiro Mendes da Costa Neto (Nurse at Piripiri MHS); Carliane Maria de Araújo Souza (Nurse at Piripiri MHS); Evaldo Sales Leal (Nurse at Piripiri MHS); Maria Erinelda de Araújo Souza (Nurse at Piripiri MHS); Michell Lucilane dos Santos Holanda (Nurse at Piripiri MHS); and Yluska Myrna Meneses Brandão e Mendes (Nurse at Piripiri MHS). Coordination: Jorge Otávio Maia Barreto (MSc, Municipal Health Secretary of Piripiri, PI) THEME: Physical activity and prevention/control of arterial hypertension in primary healthcare (Atenção Primária à Saúde, APS). 1 KEY MESSAGES PROBLEM Healthcare in Brazil has invested in formulating, implementing, and putting into practice policies related to the promotion, protection, and recovery of health. In the construction of the primary health care model, great emphasis has been placed on the improvement of the quality of life of collective subjects (Brazil 2006). Improvements in access to and the quality of the services provided by Brazil’s public health service, the Unified Healthcare System (Sistema Único de Saúde), are among the biggest priorities in healthcare, with an emphasis on strengthening the Family Health Program (Programa Saúde da Família). This includes the promotion of good health; health-related information and education; the promotion of physical activity, healthy eating, and healthy lifestyle habits; the control of tobacco and alcohol consumption; and care for the elderly. In Piripiri, the Gym on the Square Project (Projeto Academia na Praça) encouraged the local population to exercise to improve their quality of life. What is the best way, however, to include physical activity in the context of primary healthcare? What type of physical activity is most beneficial? Which groups would benefit the most? How much exercise is recommended? Are there risks related to physical exercise? This summary presents the best available evidence found on physical activity at the individual and community level, and discusses the benefits, obstacles, and implications that physical activity offers. OPTIONS Option 1: Prescription of physical activity as part of primary healthcare to prevent and treat arterial hypertension at the individual level. Option 2: Encouragement of aerobic physical activity at the community level.

MUNICIPALITY OF PIRIPIRI MUNICIPAL HEALTH SECRETARIAT
HEALTH EVIDENCE TEAM
BRASIL
Search Strategy The search strategy for scientific evidence on the proposed problem involved searching for systematic reviews in the Online Health Library (Biblioteca Virtual em Saúde, http://regional.bvsalud.org). The key terms used were “physical activity,” “targeted physical activity,” “physical activity and arterial hypertension,” “control of hypertension without medication,” “physical activity and chronic disease,” “supervised physical activity,” “physical activity and diabetes,” and “physical activity and quality of life.” Additional studies were used for contextualization, such as Brazil’s policies on dyslipidemias, the prevention of atherosclerosis in adults, children, and adolescents, and studies on high blood pressure from the Brazilian Society of Cardiology (Sociedade Brasileira de Cardiologia).
CONSIDERATIONS REGARDING THESE OPTIONS Option 1: Prescription of physical activity as part of primary healthcare to prevent and treat arterial hypertension at the individual level. In Brazil, the picture of cardiovascular health is made up mainly of smoking, hypertension, diabetes mellitus, and obesity. The estimated prevalence of hypertension in Brazil is 35% in those over 40. This represents a total of 17 million people with the disease, according to the 2004 estimate of the Brazilian Institute of Statistical Geography (Instituto Brasileiro de Geografia Estatística). Around 75% of these people turn to the Unified Healthcare System for basic care. To cater to those with hypertension, the National Arterial Hypertension and Diabetes Mellitus Awareness program was created. The program covers a range of health-promoting actions, such as the prevention, diagnosis, and treatment of the consequences of hypertension, and aims to reduce hospitalizations, emergency-room visits, and expenses related to treatment complications, early retirement, and the cardiovascular death rate. Lifestyle-related strategies involved giving up smoking, the therapeutic benefits of physical activity, and the importance of a good diet. The association between physical exercise and the risk of developing coronary artery disease (CAD) is testament to the need for the promotion of physical activity to become a public health priority. However, studies still indicate that the prevalence of educational guidance on physical activity within health units is still very low when compared to individuals’ needs. Option 2: Encouragement of aerobic physical activity at the community level. The encouragement of physical activity in basic health units has become more evident recently. A preoccupation with lifestyle is undoubtedly one of the factors contributing to this phenomenon (Matsudo 1992). Aging is accompanied by a series of effects on different systems within the body that tend to diminish physical aptitude and performance, which increases the importance of exercise. Advice to users is facilitated by the family healthcare teams that cover the population, the social practices that make up collective healthcare, and healthcare professionals with expertise in public health.

MUNICIPALITY OF PIRIPIRI MUNICIPAL HEALTH SECRETARIAT
HEALTH EVIDENCE TEAM
BRASIL
Low-impact aerobic exercise (swimming, walking, cycling, water aerobics) may be associated with a decreased risk of injury and provide great benefits at the anthropometric, neuromuscular, metabolic, and psychological levels. Aside from aiding the prevention of diseases such as arterial hypertension, coronary disease, and osteoporosis, to name a few, these types of exercise also significantly improve the quality of life of individuals and aid their independence, especially at a more advanced age. According to the IV Brazilian Guidelines of the Brazilian Society of Cardiology on dyslipidemias and the prevention of atherosclerosis, the practice of physical aerobic exercise helps to reduce plasma triglyceride levels and increase levels of HDL cholesterol (good cholesterol).

MUNICIPALITY OF PIRIPIRI MUNICIPAL HEALTH SECRETARIAT
HEALTH EVIDENCE TEAM
BRASIL
2 CONTEXT AND PRIORS Studies indicate that a reduction in mortality rates from diseases of the circulatory system are directly related to changes in lifestyle, such as good eating habits, not smoking, and the practice of physical activity. Many studies indicate that a sedentary lifestyle brings serious medium-term consequences to individuals, such as increase in body weight, arterial hypertension, and diabetes and its consequences, which can include cardiovascular disease leading to poor quality of life and even death. As such, the tracking of sedentary habits and the encouragement of physical exercise are even more necessary. In Piripiri, physical exercise has never been so widespread, but the prescription of physical activity as a way of avoiding and treating illness is still inconsistent in Piripiri, especially within primary healthcare, where it is often merely a professional recommendation. The average income and the historic lack of publicly accessible exercise equipment may also put most of the population at a disadvantage, as not everyone is able to sign up for private gym membership. At the end of 2009, the Municipality of Piripiri implemented the Gym on the Square Project, which proposed that coordinated activities be carried out by physical education professionals under the direction of the Family Health Strategy. The project intended to include varied age groups, regardless of whether they suffer from chronic illness. As part of the Gym on the Square Project, the municipality has also opened the Center for Integrated Physical Activity for users with limited movement or motor skills, who take part in physical education and physio- and occupational therapies, also under the guidance of the Family Health Strategy. Though quantitative data is not available, it is hoped that with increased physical activity, a reduction in ailments will be observed.

MUNICIPALITY OF PIRIPIRI MUNICIPAL HEALTH SECRETARIAT
HEALTH EVIDENCE TEAM
BRASIL
3 DESCRIPTION OF THE PROBLEM According to the Brazilian Ministry of Health’s Mortality Information System (Sistema de Informação sobre Mortalidade), diseases of the circulatory system constitute the main cause of death in the population of Piripiri, with CVAs and myocardial infarctions (the main consequences of uncontrolled arterial hypertension) being the major causes of death between 2002 and 2008. Intervention in the prevention and control of these conditions has become urgent. For years, the non-essential care model adopted in Piripiri was outpatient assistance, mainly conducted by the regional hospital located in the city. With the emergence of programs run by Community Agents and the Family Health Program, the primary healthcare system began to direct and coordinate the local system, prioritizing activities at the community level, but still with great demand for outpatient care and visits to doctors or other health professionals, following the professional-patient model. Even so, the population’s focus on and perception of health is changing, as groups of pregnant women, people with hypertension, diabetics, and children are being better provided for through therapies beyond mere medication and examinations. Among these practices are home visits, educational sessions, immunizations, counseling, and physical activity. However, although physical activity is often recommended during doctor’s visits, professionals do not place sufficient importance on it, in that they usually merely suggest that the patient exercise more, without a definite routine or schedule, such as with medication. Studies indicate that moderate and cumulative physical activity significantly reduces the risk of developing coronary artery disease in individuals of any age group, as well as consequences of this, such as myocardial infarctions and CVAs. Exercise also controls blood pressure levels and contributes to psychological well-being. The problem under consideration is the following: can physical activity be used as a tool to prevent and treat of hypertension at the individual and community levels?
MUNICIPALITY OF PIRIPIRI MUNICIPAL HEALTH SECRETARIAT
HEALTH EVIDENCE TEAM
BRASIL
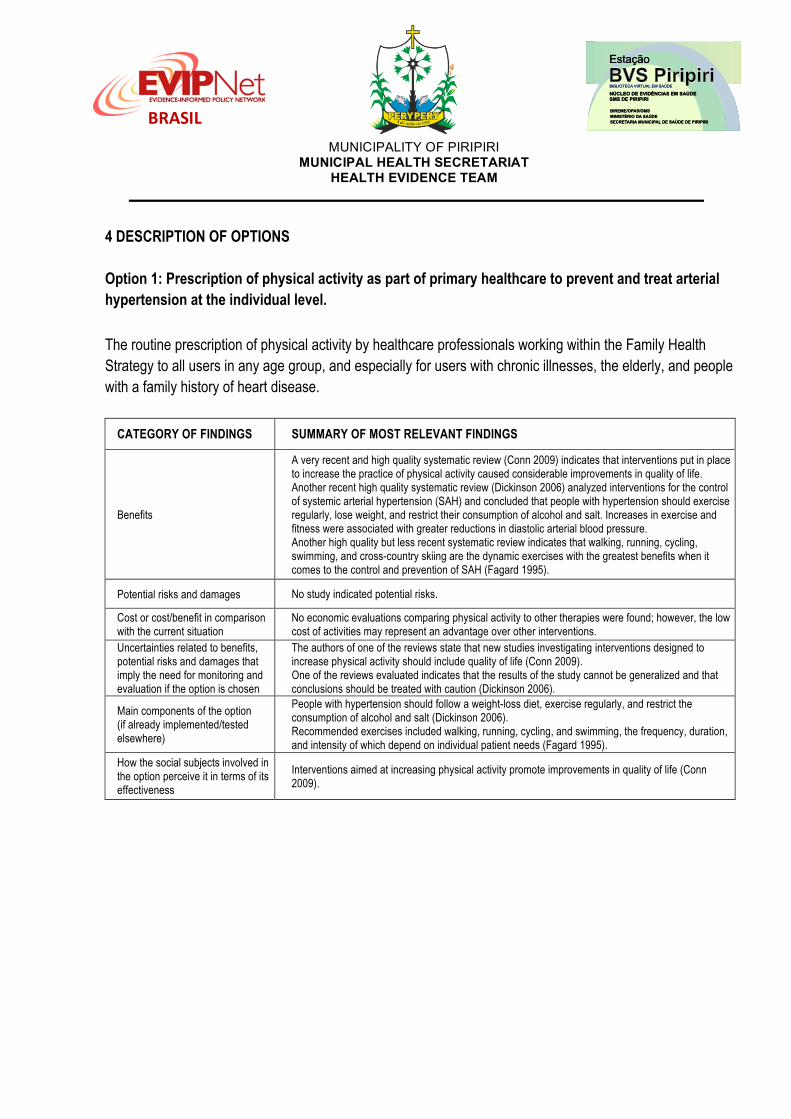
4 DESCRIPTION OF OPTIONS Option 1: Prescription of physical activity as part of primary healthcare to prevent and treat arterial hypertension at the individual level. The routine prescription of physical activity by healthcare professionals working within the Family Health Strategy to all users in any age group, and especially for users with chronic illnesses, the elderly, and people with a family history of heart disease.
CATEGORY OF FINDINGS SUMMARY OF MOST RELEVANT FINDINGS
Benefits
A very recent and high quality systematic review (Conn 2009) indicates that interventions put in place to increase the practice of physical activity caused considerable improvements in quality of life. Another recent high quality systematic review (Dickinson 2006) analyzed interventions for the control of systemic arterial hypertension (SAH) and concluded that people with hypertension should exercise regularly, lose weight, and restrict their consumption of alcohol and salt. Increases in exercise and fitness were associated with greater reductions in diastolic arterial blood pressure. Another high quality but less recent systematic review indicates that walking, running, cycling, swimming, and cross-country skiing are the dynamic exercises with the greatest benefits when it comes to the control and prevention of SAH (Fagard 1995).
Potential risks and damages No study indicated potential risks.
Cost or cost/benefit in comparison with the current situation
No economic evaluations comparing physical activity to other therapies were found; however, the low cost of activities may represent an advantage over other interventions.
Uncertainties related to benefits, potential risks and damages that imply the need for monitoring and evaluation if the option is chosen
The authors of one of the reviews state that new studies investigating interventions designed to increase physical activity should include quality of life (Conn 2009). One of the reviews evaluated indicates that the results of the study cannot be generalized and that conclusions should be treated with caution (Dickinson 2006).
Main components of the option (if already implemented/tested elsewhere)
People with hypertension should follow a weight-loss diet, exercise regularly, and restrict the consumption of alcohol and salt (Dickinson 2006). Recommended exercises included walking, running, cycling, and swimming, the frequency, duration, and intensity of which depend on individual patient needs (Fagard 1995).
How the social subjects involved in the option perceive it in terms of its effectiveness
Interventions aimed at increasing physical activity promote improvements in quality of life (Conn 2009).

MUNICIPALITY OF PIRIPIRI MUNICIPAL HEALTH SECRETARIAT
HEALTH EVIDENCE TEAM
BRASIL
Option 2: Encouragement of aerobic physical activity at the community level. Offering professionally supervised aerobic physical activity as a way of preventing and treating chronic disease.
CATEGORY OF FINDINGS SUMMARY OF MOST RELEVANT FINDINGS
Benefits
A high quality but not very recent systematic review (Kelley 1999) showed that aerobic exercise promotes a reduction in resting blood pressure in adult women. Another review confirmed the effectiveness of aerobic exercise in the reduction of resting systolic blood pressure in the elderly (Kelley 1999), (Kelley 2001). Another more recent review, but of equally high quality, concluded that aerobic exercise reduces blood pressure in hypertensive individuals and those with normal blood pressure. An increase in aerobic physical activity should be considered an important part of lifestyle modification in order to prevent and treat high blood pressure (Whelton 2002). An even more recent and high quality systematic review (Kodama 2007) demonstrated that regular aerobic exercise modestly increase levels of HDL cholesterol. A less recent but equally high quality systematic review indicates that physical aerobic training was capable of producing a small but significant drop in blood pressure, regardless of its intensity or frequency (Halbert 1999).
Potential risks and damages No study pointed to potential risks.
Cost or cost/benefit in comparison with the current situation
No economic evaluation comparing physical activity to other therapies were found; however, the low cost of activities (such as walking) may represent an advantage over medication-based therapies.
Uncertainties related to benefits, potential risks and damages that imply the need for monitoring and evaluation if the option is chosen
Almost all participants were American or Japanese, so the results may not be able to be generalized. One systematic review (Halbert 1997) indicates that changes in systemic arterial blood pressure may not be clinically significant in the majority of hypertensive patients.
Main components of the option (if already implemented/tested elsewhere)
Aerobic activities are effective in the prevention and treatment of high blood pressure. The aerobic activities analyzed included walking, cycling, swimming, water aerobics, and aerobic dance.
How the social subjects involved in the option perceive it in terms of its effectiveness
An increase in aerobic physical activity can be an important component of changes in lifestyle for the prevention and treatment of high blood pressure (Whelton 2002).

MUNICIPALITY OF PIRIPIRI MUNICIPAL HEALTH SECRETARIAT
HEALTH EVIDENCE TEAM
BRASIL
5 CONSIDERATIONS REGARDING THE IMPLMENTATION OF OPTIONS Potential barriers to the implementation of options Option 1: Prescription of physical activity as part of primary healthcare to prevent and treat arterial hypertension at the individual level.
LEVEL BARRIERS
Patient/Individual The benefits of physical activity must be approached taking into account cultural—notably gender-related—implications for all individuals at all moments of contact with healthcare services.
Healthcare workers Primary healthcare professionals must be trained in how to approach and prescribe physical exercise. Primary healthcare professionals and those working in physical activity referral centers must be integrated more consistently, so that users are received and guided more effectively.
Organization
A protocol for the prescription of physical activity within primary healthcare must be created, implemented, monitored, and evaluated. Spaces in the city that encourage physical activity must be expanded. Structural barriers must not be so relevant as to hinder the implementation of this option.
System There is a lack of specific Unified Healthcare System funding for physical activities related to primary healthcare. Costs can represent a barrier to the sustainability of hiring and maintaining professionals, as well as the necessary infrastructure for physical activity.
Option 2: Encouragement of aerobic physical activity at the community level.
LEVEL BARRIERS
Patient/Individual Men may offer greater resistance to undertaking regular physical activity. Social efforts must be expanded by mobilizing all segments of society in order to encourage physical activity within the community. We must spread awareness of the benefits of physical exercise consistently and at every possible opportunity.
Healthcare workers
Physical education professionals should be encouraged to create exercise programs that cater to the public and the existing infrastructure. We must spread awareness of the benefits of physical exercise consistently and at every possible opportunity. The evaluation of results obtained by adopting these practices should form part of health professionals’ activities, in order to improve planning.
Organization
The offer of spaces in the city that encourage physical exercise must be expanded. Universal access to these must be ensured, while still respecting individual users’ needs. The availability of professionally supervised physical exercise must be ensured. Basic infrastructure and materials for areas designed for physical activity must be ensured. Partnerships for the use and maintenance of existing infrastructure must be developed.
System
There is a lack of specific funding from the Unified Healthcare System and primary healthcare for physical activities. Costs can represent a barrier to the sustainability of hiring and maintaining professionals, as well as the necessary infrastructure for physical activity. Success depends more on political commitment and organizational ability than on the availability of resources.
MUNICIPALITY OF PIRIPIRI MUNICIPAL HEALTH SECRETARIAT
HEALTH EVIDENCE TEAM
BRASIL
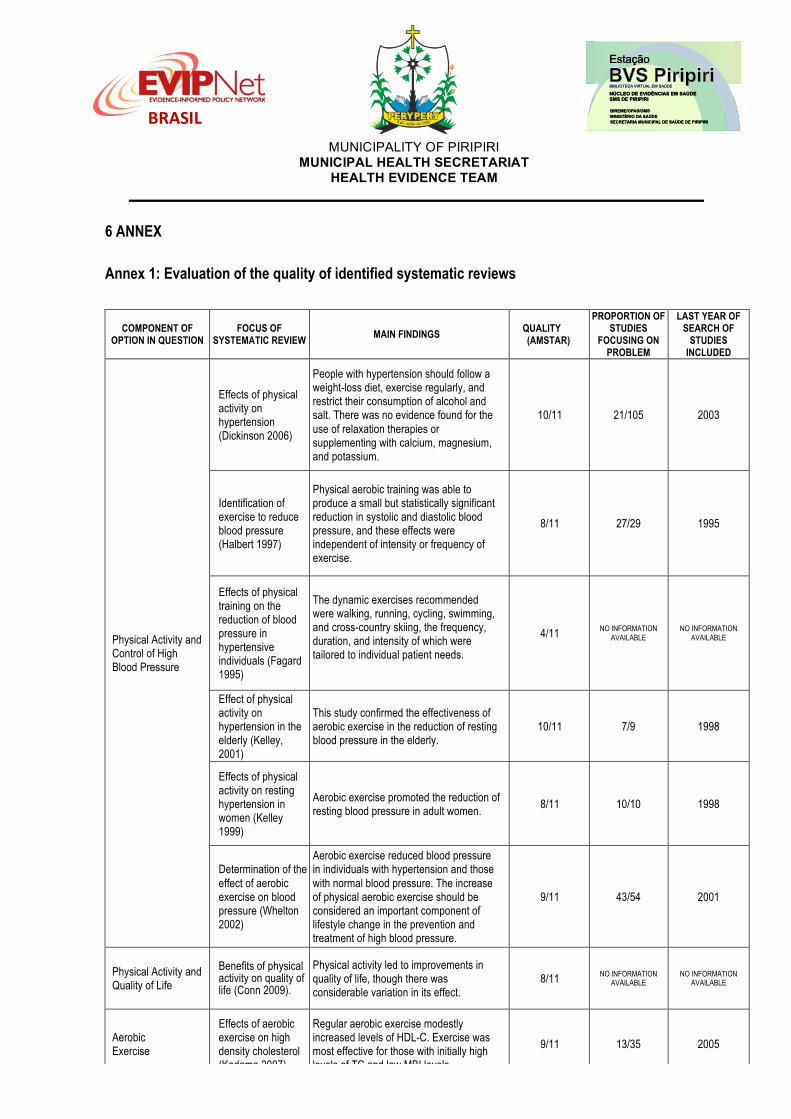
6 ANNEX Annex 1: Evaluation of the quality of identified systematic reviews
COMPONENT OF OPTION IN QUESTION
FOCUS OF SYSTEMATIC REVIEW
MAIN FINDINGS QUALITY (AMSTAR)
PROPORTION OF STUDIES
FOCUSING ON PROBLEM
LAST YEAR OF SEARCH OF
STUDIES INCLUDED
Physical Activity and Control of High Blood Pressure
Effects of physical activity on hypertension (Dickinson 2006)
People with hypertension should follow a weight-loss diet, exercise regularly, and restrict their consumption of alcohol and salt. There was no evidence found for the use of relaxation therapies or supplementing with calcium, magnesium, and potassium.
10/11 21/105 2003
Identification of exercise to reduce blood pressure (Halbert 1997)
Physical aerobic training was able to produce a small but statistically significant reduction in systolic and diastolic blood pressure, and these effects were independent of intensity or frequency of exercise.
8/11 27/29 1995
Effects of physical training on the reduction of blood pressure in hypertensive individuals (Fagard 1995)
The dynamic exercises recommended were walking, running, cycling, swimming, and cross-country skiing, the frequency, duration, and intensity of which were tailored to individual patient needs.
4/11 NO INFORMATION AVAILABLE
NO INFORMATION AVAILABLE
Effect of physical activity on hypertension in the elderly (Kelley, 2001)
This study confirmed the effectiveness of aerobic exercise in the reduction of resting blood pressure in the elderly.
10/11 7/9 1998
Effects of physical activity on resting hypertension in women (Kelley 1999)
Aerobic exercise promoted the reduction of resting blood pressure in adult women.
8/11 10/10 1998
Determination of the effect of aerobic exercise on blood pressure (Whelton 2002)
Aerobic exercise reduced blood pressure in individuals with hypertension and those with normal blood pressure. The increase of physical aerobic exercise should be considered an important component of lifestyle change in the prevention and treatment of high blood pressure.
9/11 43/54 2001
Physical Activity and Quality of Life
Benefits of physical activity on quality of life (Conn 2009).
Physical activity led to improvements in quality of life, though there was considerable variation in its effect.
8/11 NO INFORMATION AVAILABLE
NO INFORMATION AVAILABLE
Aerobic Exercise
Effects of aerobic exercise on high density cholesterol (Kodama 2007)
Regular aerobic exercise modestly increased levels of HDL-C. Exercise was most effective for those with initially high levels of TC and low MBI levels.
9/11 13/35 2005
MUNICIPALITY OF PIRIPIRI MUNICIPAL HEALTH SECRETARIAT
HEALTH EVIDENCE TEAM
BRASIL
7. REFERENCES (Systematic Reviews) 1. Dickinson HO; Mason JM; Nicolson DJ; Campbell F; Beyer FR; Cook JV; Williams B; Ford GA. Lifestyle interventions to reduce raised blood pressure: a systematic review of randomized controlled trials. Journal of Hypertension 2006; 24 (2): 215–233.
2. Conn VS; Hafdahl AR; Brown LM. Meta-analysis of quality-of-life outcomes from physical activity interventions. Nursing Research 2009; 58 (3):175–183.
3. Fagard RH. Prescription and results of physical activity. Journal of Cardiovascular Pharmacology 1995; 25 (Supplement 1): S20–S27.
4. Halbert JA; Silagy CA; Finucane P; Withers RT; Hamdorf PA; Andrews GR. The effectiveness of exercise training in lowering blood pressure: a meta-analysis of randomized controlled trials of 4 weeks or longer. Journal of Human Hypertension 1997; 11 (10): 641–649.
5. Kelley GA; Sharpe Kelley K. Aerobic exercise and resting blood pressure in older adults: a meta-analytic review of randomized controlled trials. Journals of Gerontology Series A—Biological Sciences and Medical Sciences 2001; 56A (5): M298–M303.
6. Kelley GA. Aerobic exercise and resting blood pressure among women: a meta-analysis. Preventive Medicine 1999; 28 (3): 264–275.
7. Kodama S; Tanaka S; Saito K; Shu M; Sone Y; Onitake F; Suzuki E; Shimano H; Yamamoto S; Kondo K; Ohashi Y; Yamada N; Sone H. Effect of aerobic exercise training on serum levels of high-density lipoprotein cholesterol: a meta-analysis. Archives of Internal Medicine 2007; 167 (10): 999–1008.
8. Whelton S P; Chin A; Xin X; He J. Effect of aerobic exercise on blood pressure: a meta-analysis. Annals of Internal Medicine 2002; 136 (7): 493–503.
OTHER COMPLEMENTARY REFERENCES
9. Siqueira FV; Nahas MV; Facchini LA; Silveira DS; Piccini RX; Tomasi E; Thumé E; Hallal PC. Counseling for physical activity as a health education strategy. Public Health Journal, vol. 25, no. 1, Rio de Janeiro, 2009.
10. Silva MP; Santos Filho JAA; Gobbi S. Functional aptitude of elderly women under supervised general physical activity program or regular unsupervised walks. Brazilian Journal of Physical Activity and Health 2006, 11(2): p.3-12.
11. Franchi KMB; Monteiro LZ; Medeiros AIA; Almeida SB; Pinheiro MHNP, Montenegro RM; Junior RMM. Comparative study of knowledge and practice of physical activity for type 2 elderly diabetics and non-diabetics. Brazilian Journal of Geriatric Gerontology 2008; 11 (3): 327–339.
12. Brazilian Society of Cardiology. Department of Atherosclerosis. IV Brazilian Guidelines on Dyslipidemias and the Prevention of Atherosclerosis. Brazilian Archives of Cardiology – volume 88, supplement I, April 2007.
13. Brazilian Society of Cardiology. Department of Atherosclerosis. I Brazilian Guidelines in the Prevention of Atherosclerosis in Childhood and Adolescence. Brazilian Archives of Cardiology – volume 85, supplement VI, December 2005.
14. Brazilian Society of Cardiology. V Brazilian Guideline of Arterial Hypertension. Brazilian Archives of Cardiology, Brazil, 2006.
15. Brazil, 2006. Ministry of Health. Health Awareness Secretariat. National Policy on the Promotion of Health / – Brasília: Ministry of Health, 2006.
Related Documents











