PTK By Dr. Safaa Refaat 1

Phototherapeutic keratectomy By Dr. Safaa Refaat
Jul 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PTK By Dr. Safaa Refaat 11

PTK By Dr. Safaa Refaat 22
PHOTOTHERAPEUTIC KERATECTOMYPHOTOTHERAPEUTIC KERATECTOMYFORFOR
SUPERFICIAL CORNEAL OPACITIESSUPERFICIAL CORNEAL OPACITIES
ByDr. Safaa Refaat
FRCSG , MSc, MBBS

INTRODUCTION

PTK By Dr. Safaa Refaat 44
Over the years, many surgical procedures have been
established to restore the corneal clarity & regularity, or to
replace the opacified cornea.

PTK By Dr. Safaa Refaat 55
Excimer Laser
The term “excimer” “excited dimer”First described by Houtermans in 1969.In 1976 commercially introduced.In 19851st excimer laser Corneal Photoablation by Seiler.In 19881st PRK by Mc Donald et al.

PTK By Dr. Safaa Refaat 66
Excimer Lasers Emissions
Gas Medium Wave Length (nm)
F2 157 nm
Xe2 170 nm
ArF 193 nm
KrCl 222 nm
KrF 248 nm
XeCl 308 nm
XeF 351 nm
PTK By Dr. Safaa Refaat 77
Ablative photodecomposition
breaking intra molecular bonds molecular fragmentsGas plum
condensation
pseudomembrane.
Mechanism of action:
PTK By Dr. Safaa Refaat 88
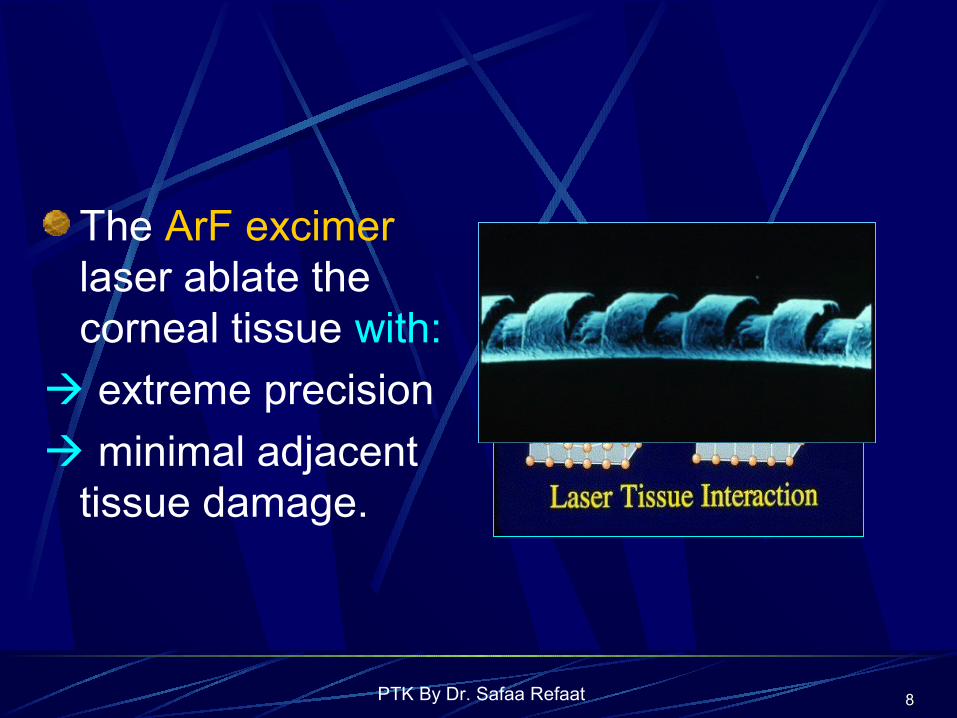
The ArF excimer laser ablate the corneal tissue with:
extreme precision
minimal adjacent tissue damage.

PTK By Dr. Safaa Refaat 99
PHOTOTHERAPEUTIC KERATECTOMY
DEFINITION:
The use of the excimer laser in treatment of corneal pathology is termed PTK as opposed to PRK.
PTK By Dr. Safaa Refaat 1010
Indications The best results of PTK are obtained when pathology is limited to the anterior one fifth.
Patients with deeper corneal scars may also benefit from PTK.
The corneal thickness after PTK should be < 250 μm.

PTK By Dr. Safaa Refaat 1111
There are four distinct PTK treatment groups:
1- REE & painful BK.
2- Surface irregularities.
3- Corneal opacities.
4- Complications of PRK and LASIK.
1-

PTK By Dr. Safaa Refaat 1212
1- Recurrent Corneal erosionsPainful REE syndrome abnormalities in the Ep.-BM complex.
The aim of PTK
Removal of enough part of Bowman`s layer.
PTK By Dr. Safaa Refaat 1313
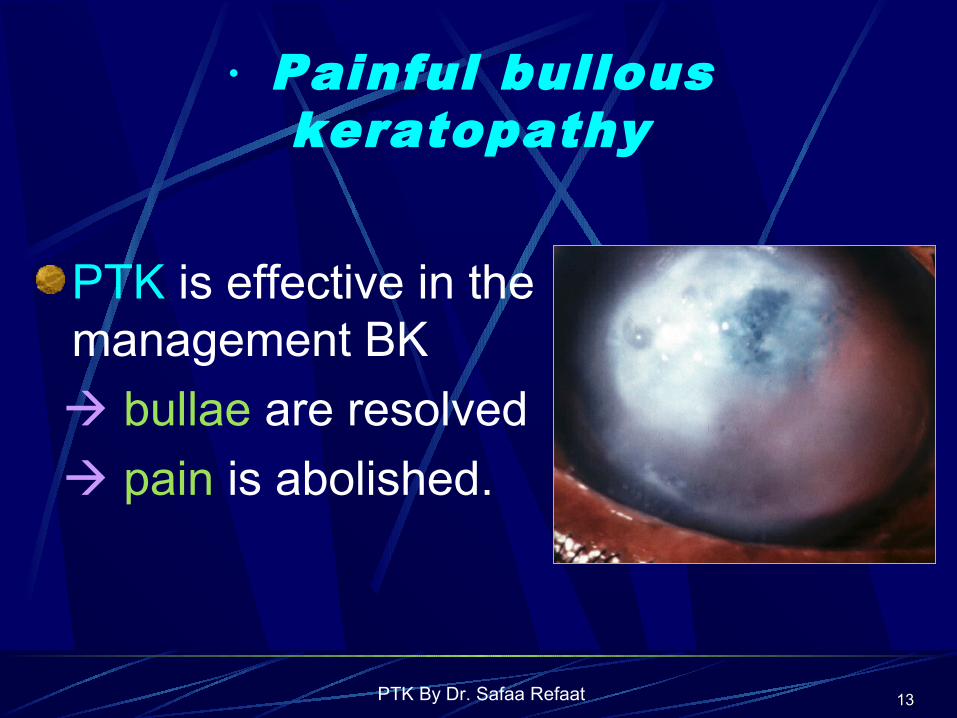
· Painful bullous keratopathy
PTK is effective in the management BK
bullae are resolved
pain is abolished.

PTK By Dr. Safaa Refaat 1414
Due to:Degenerations Salzmann’s nodules
Band keratopathy.
2- Irregular surface

PTK By Dr. Safaa Refaat 1515
Granular dystrophy
Lattice dystrophy.
With Anterior Corneal Dystrophies

PTK By Dr. Safaa Refaat 1616
keratoconus
Reis-Buckler’s dystrophy.
Irregular astigmatism after refractive surgery.

PTK By Dr. Safaa Refaat 1717
3- Corneal opacitiesCorneal dystrophies
Map dot finger print D.
Reis-Bückler’s D.

PTK By Dr. Safaa Refaat 1818
Schnyder’s crystallinedystrophy.
Avellino Latticedystrophy.
PTK By Dr. Safaa Refaat 1919
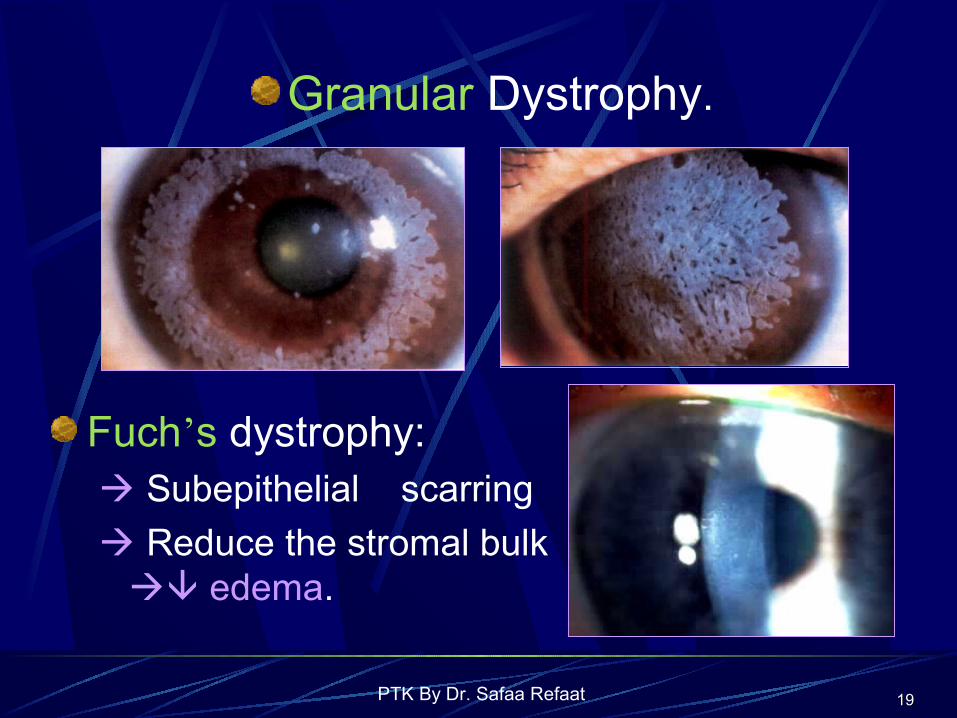
Granular Dystrophy.
Fuch’s dystrophy: Subepithelial scarring
Reduce the stromal bulk edema.
PTK By Dr. Safaa Refaat 2020
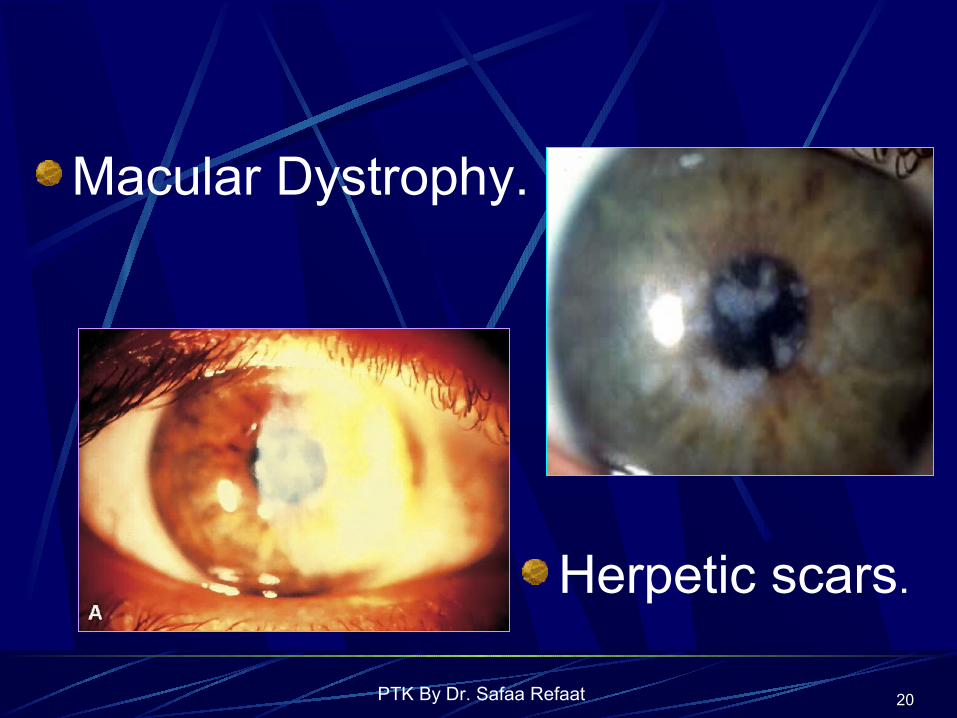
Macular Dystrophy.
Herpetic scars.

PTK By Dr. Safaa Refaat 2121
Surgical scars ex. Pterygium excision.
Recurrence of dystrophic changes after PKP.

PTK By Dr. Safaa Refaat 2222
4- Treatment of PRK and LASIK complications
A-Central Islands: 6 months after PRK 2 months after LASIK
B-Corneal Haze after PRK
Wait 6 to 12 months.

PTK By Dr. Safaa Refaat 2323
C – Decentered Ablations: If >1mm symptomatic. PTK can be effective.
D – LASIK flap complications: Irregular astigmatism
loss of BCVA. PTK to restore regular
corneal surface.

PTK By Dr. Safaa Refaat 2424
Other indications
Superficial infectious keratitis resistant to medical treatment
”controversial”
Corneo- conjunctival carcinoma:Spadea et al.(2002); reported the
successful use of PTK in the treatment of a case with recurrent intraepithelial corneo-conjunctival carcinoma.

PTK By Dr. Safaa Refaat 2525
ContraindicationsContraindications
Systemic Ocular
Generalized deblitating diseases
Ocular surface diorder&infections
Auto immune disease
Uncontrolled DM.
Uveitis, glaucoma
Significant corneal thining or Neovascularization.
PTK By Dr. Safaa Refaat 2626
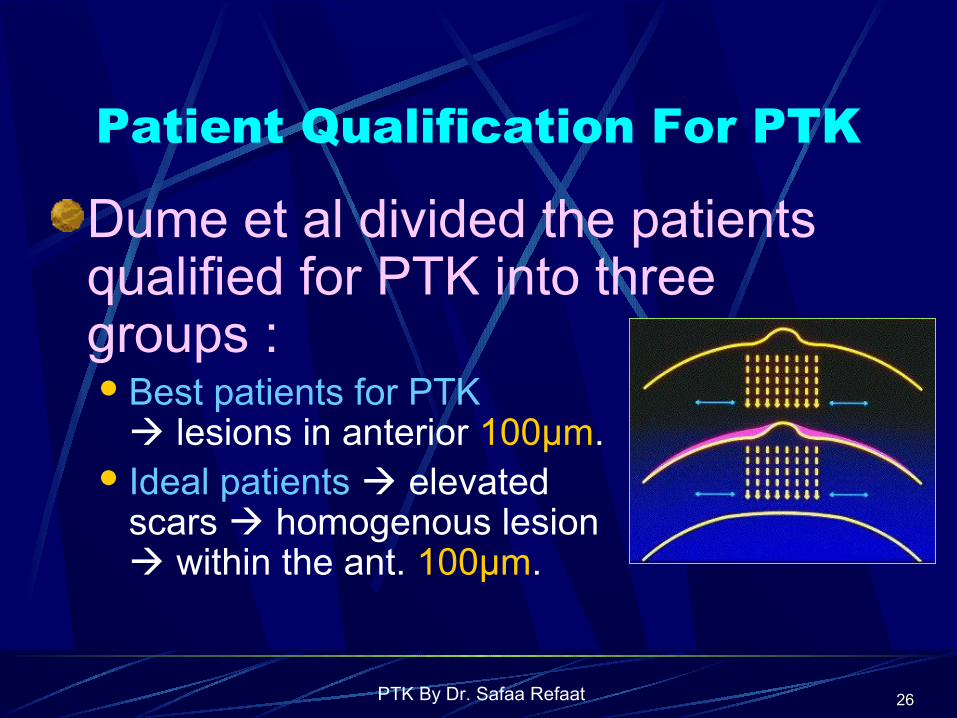
Patient Qualification For PTK
Dume et al divided the patients qualified for PTK into three groups :Best patients for PTK
lesions in anterior 100μm. Ideal patients elevated
scars homogenous lesion within the ant. 100μm.
PTK By Dr. Safaa Refaat 2727
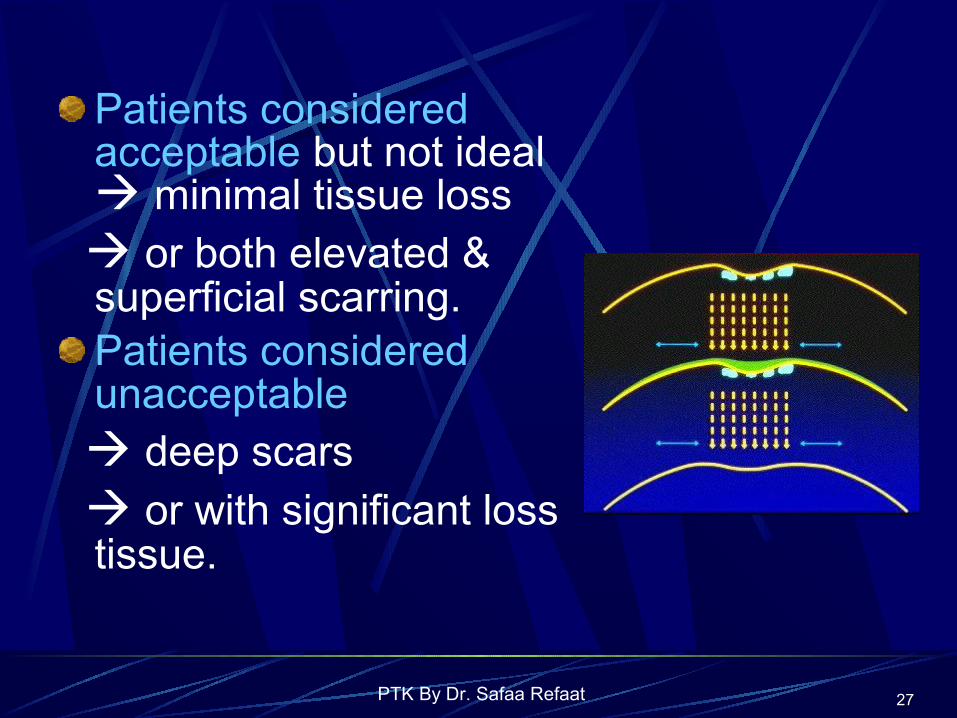
Patients considered acceptable but not ideal minimal tissue loss
or both elevated & superficial scarring.Patients considered unacceptable
deep scars or with significant loss
tissue.
PTK By Dr. Safaa Refaat 2828
Surgical techniques1. Epithelial debridement:
An ideal method for epithelial debridement will be: Rapid to prevent dehydration. Would leave a clean and smooth
epithelial defects. Reproducible.

PTK By Dr. Safaa Refaat 2929
Variable techniques :Mechanical debridment.Laser trans-epithelial ablation.High speed rotating brushes.Diluted ethanol.
OR, Various combinations : laser scrape methods.ethanol- assisted mechanical debridement.

PTK By Dr. Safaa Refaat 3030
smoothing of the anterior corneal
surface:It is of particular importance Excimer laser will reproduce surface irregularities deeper within the stroma.
PTK By Dr. Safaa Refaat 3131
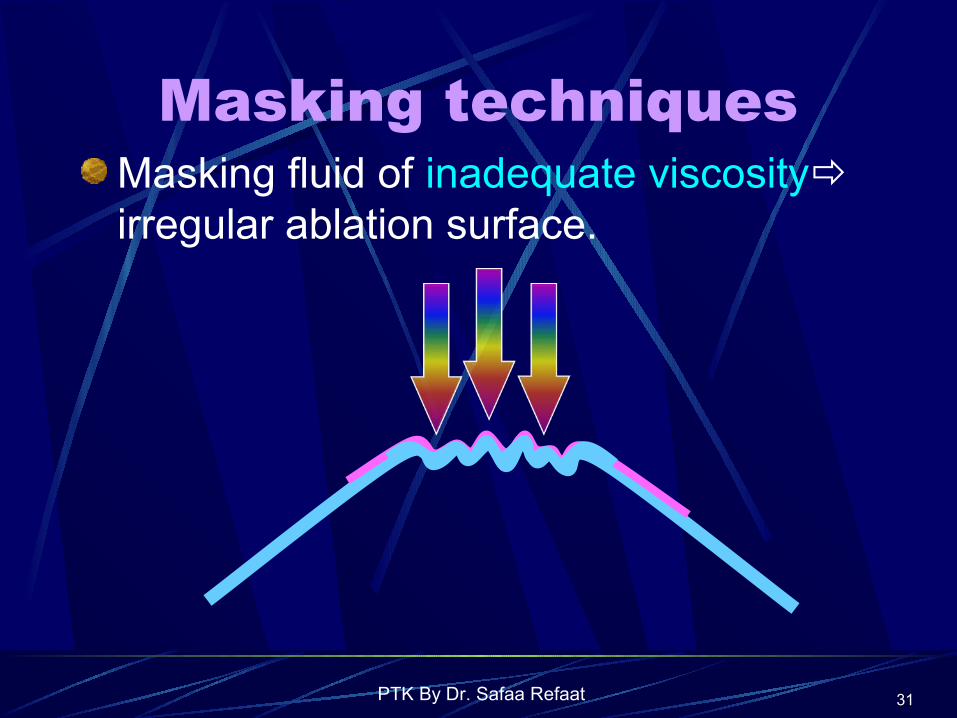
Masking techniquesMasking fluid of inadequate viscosity irregular ablation surface.

PTK By Dr. Safaa Refaat 3232
Masking fluid of high viscosity irregular ablation surface.
PTK By Dr. Safaa Refaat 3333
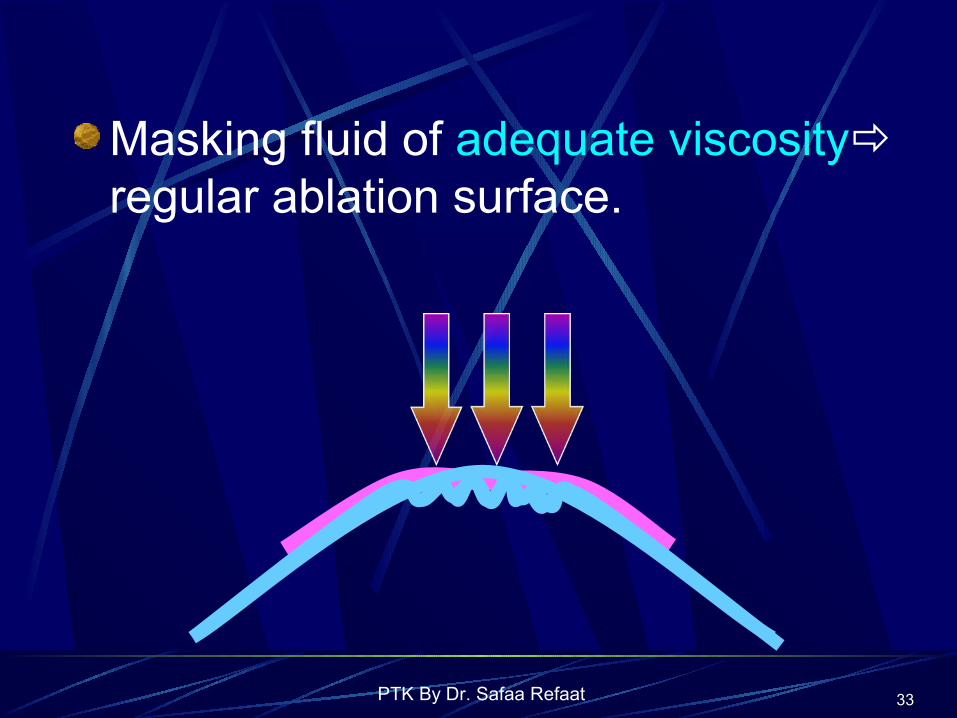
Masking fluid of adequate viscosity regular ablation surface.

PTK By Dr. Safaa Refaat 3434
There are many types of masking agents.
Modified collagen gel modulators are of the most recent &ideal
masking agents ex. the BioMask & PALM gel

PTK By Dr. Safaa Refaat 3535
The PALM Technique.

PTK By Dr. Safaa Refaat 3636
The technique and depth indication and the aim of ttt.
PTK in REE:Epithelium debridement.
Large spot size such as 6.5 mm.
Depth 8 -10 μm.
2- Stromal ablation:

PTK By Dr. Safaa Refaat 3737
Bullous keratopathy:
Moderately deep ablation: pain neural plexus. the swelling quantity of MPS
osmotic load. Scarring epithelial stability.
PTK By Dr. Safaa Refaat 3838
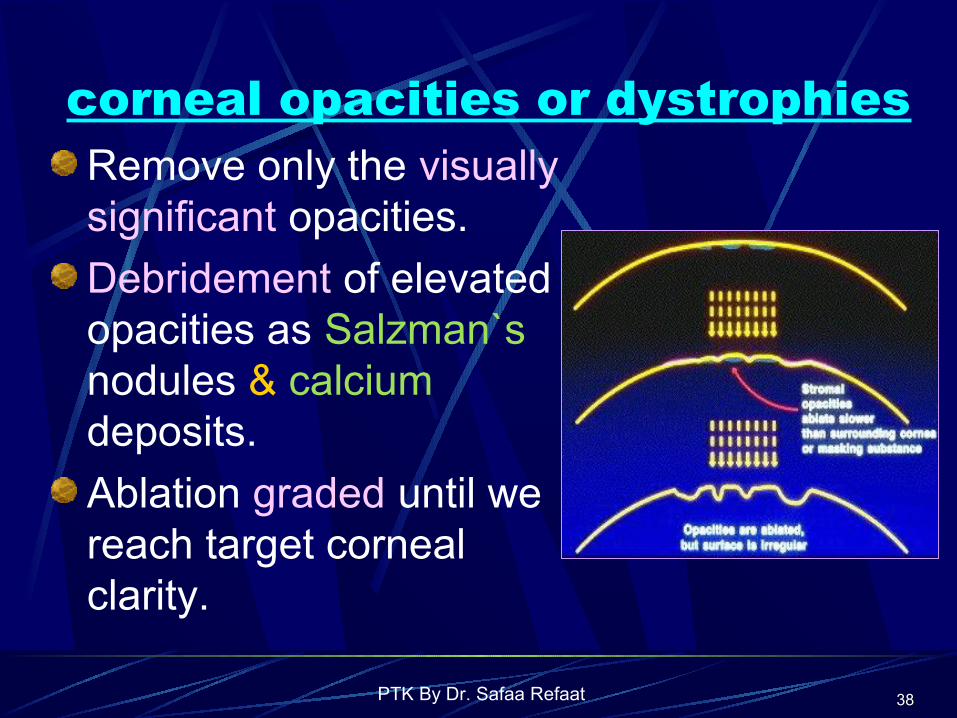
corneal opacities or dystrophiesRemove only the visually significant opacities.
Debridement of elevated opacities as Salzman`s nodules & calcium deposits.
Ablation graded until we reach target corneal clarity.

PTK By Dr. Safaa Refaat 3939
Complications and side effects
1. Post operative pain.
2. Delayed re-epithelialization
3. Corneal infiltrates
4. Stromal haze
5. Glare and halos
6. Hyperopic shift
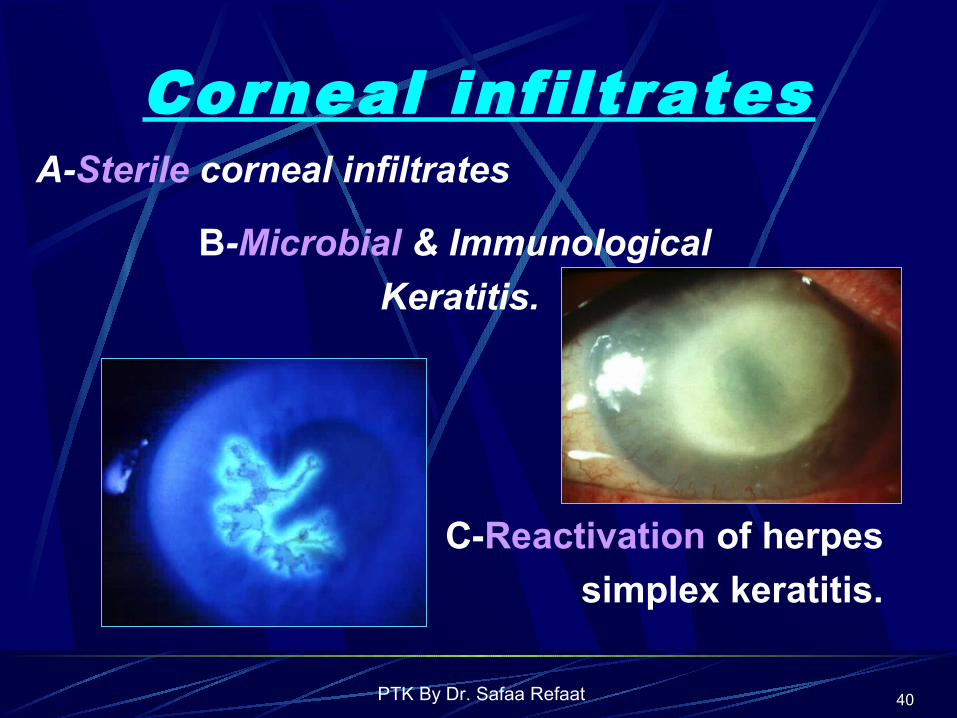
PTK By Dr. Safaa Refaat 4040
Corneal infiltratesA-Sterile corneal infiltrates
B-Microbial & Immunological
Keratitis.
C-Reactivation of herpes
simplex keratitis.

PTK By Dr. Safaa Refaat 4141
Stromal haze
Activated keratocytes new collagen and proteoglycan matrix haze formation

PTK By Dr. Safaa Refaat 4242
Grading of corneal haze:Grade 0 Totally clear cornea.
Grade0.5 Barely perceptible haze, (seen only against the red reflex).Grade 1 Trace haze (of minimal density seen with direct and diffuse illumination).
Grade 2 Mild haze, (easily visible with direct focal slit illumination).
Grade 3 Moderate haze, (partially obscures iris details).
Grade 4 Severe haze, (that completely obscures iris details).

PTK By Dr. Safaa Refaat 4343
Visual disorders of night glare and halos
Optical zone must be greater than the pupil
to avoid foveal & para foveal glare or ghosting

PTK By Dr. Safaa Refaat 4444
Hyperopic shift:
It is one of the most commonly seen side effect.
Measures to reduce the hyperopic shift: Shallow ablations.Transition zone settings. Skillful use of masking agents.

PTK By Dr. Safaa Refaat 4545
Other Complications
• Corneal graft rejection.• Keratectasia.• Limbal stem cell deficiency. • Elevation of the intraocular pressure .• Cataract. • Rare reported complications:
Ptosis Intracorneal granulomatous inflammation .

PTK By Dr. Safaa Refaat 4646

PTK By Dr. Safaa Refaat 4747
Aim Of The WorkTo evaluate the safety
and efficacy of PTK in improving vision in patients with poor
functional visual acuity due to superficial corneal opacities.

PTK By Dr. Safaa Refaat 4848
Materials
We performed a non-randomized prospective clinical study on 10 eyes of 10 patients with defective vision due to central or para central superficial corneal opacities.

PTK By Dr. Safaa Refaat 4949
Inclusion criteria
Superficial corneal scars or opacities limited to the anterior one third of the stroma.
PTK By Dr. Safaa Refaat 5050
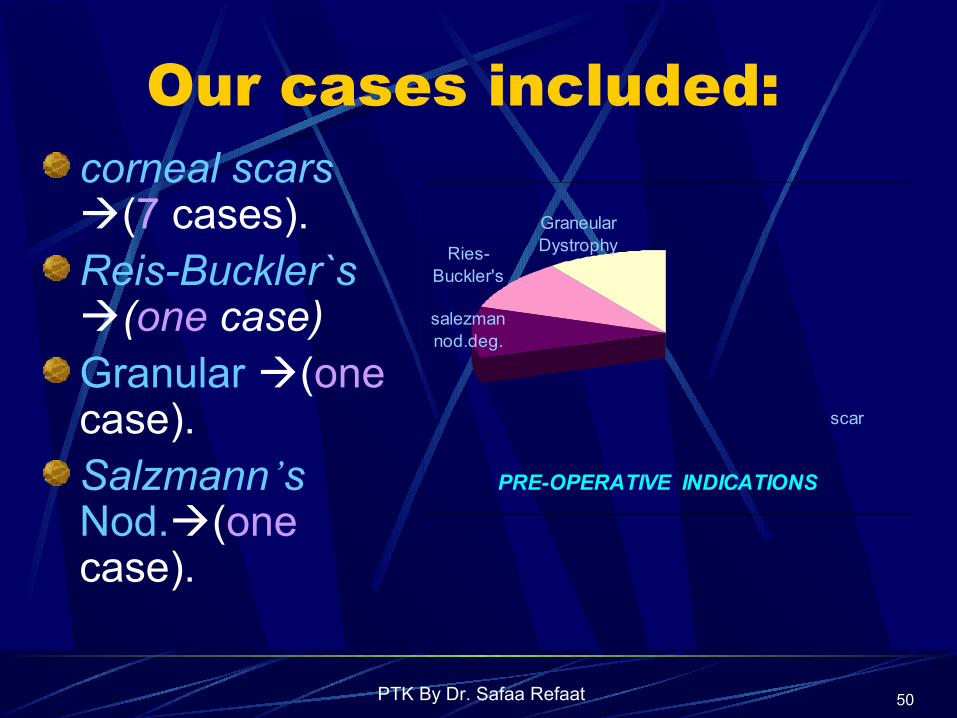
Our cases included:corneal scars (7 cases).Reis-Buckler`s (one case)Granular (one case). Salzmann’s Nod.(one case).
PRE-OPERATIVE INDICATIONS
scar
Graneular DystrophyRies-
Buckler's
salezman nod.deg.

PTK By Dr. Safaa Refaat 5151
Exclusion criteria Ocular exclusion criteria included:Ocular surface disorders & infection.Uveitis .Corneal neovascularization. Recently active Herpetic scars. Corneal thinning.Glaucoma or suspected glaucoma.

PTK By Dr. Safaa Refaat 5252
Systemic exclusion criteria included:
Generalized debilitating diseasesAutoimmune diseases.Uncontrolled DM.Collagen vascular diseases .Pregnant and lactating women .
PTK By Dr. Safaa Refaat 5353
Pre operative preparations History. Examination :Unaided and BCVA..Refraction. Pupillary light reflex, and pupil size Fluorescine BUT. Corneal pathology. IOP, Dilated fundus examination Ultrasound pachmetry

PTK By Dr. Safaa Refaat 5454
The Main Preoperative Data.
PTK By Dr. Safaa Refaat 5555
Pre-operative medication:
Prophylactic antibiotic(Ciprofloxacin ED) two days before the procedure.
Mild pre operative Sedation.

PTK By Dr. Safaa Refaat 5656
Technique
Technolas 117, 193 nm excimer laser system.Fluence setting used was 160mJ/cm2
Pulse frequency of 50 Hz.

PTK By Dr. Safaa Refaat 5757
Surgical Steps:Topical aneasthesia.Mechanical epithelial debridment.Setting of the ablation depth and diameter..Stromal ablation. Irrigation with BSS.Soft C.L.

PTK By Dr. Safaa Refaat 5858
A 47 yrs. old female with para central corneal scar.
PTK By Dr. Safaa Refaat 5959
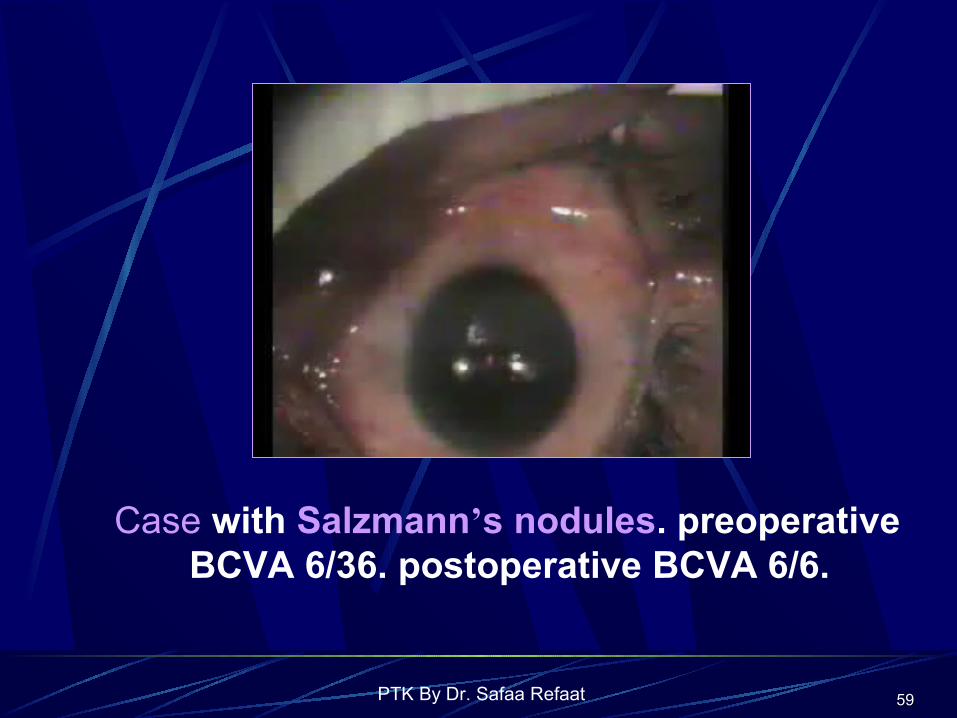
Case with Salzmann’s nodules. preoperative BCVA 6/36. postoperative BCVA 6/6.

PTK By Dr. Safaa Refaat 6060
Aphakic patient with central superficial corneal opacity.

PTK By Dr. Safaa Refaat 6161
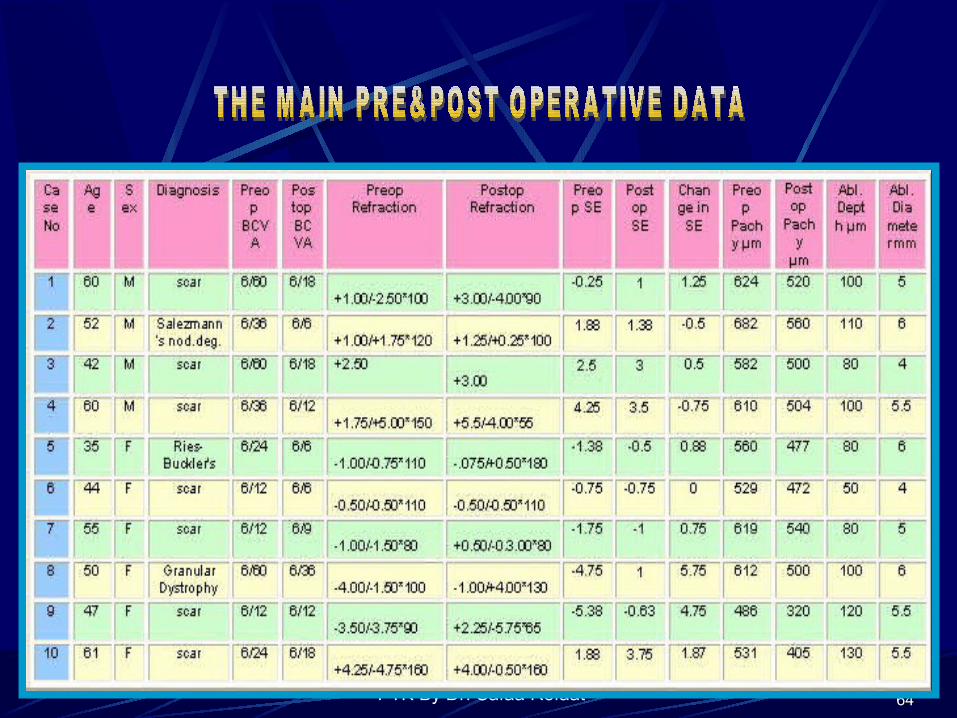
The Main Operative Data
PTK By Dr. Safaa Refaat 6262
Post operative care
Strong pain killer.
Tobramycin with 0.1%dexamethazone combination eye drops .
Preservative free artificial tears.
When the epithelial healing was complete flurometholone 0.1% for 2-4 months.

PTK By Dr. Safaa Refaat 6363
Postoperative examination:
Epithelial healing.BCVA. Refraction.Symptoms corneal light scattering. Anterior stromal haze.
PTK By Dr. Safaa Refaat 6464

PTK By Dr. Safaa Refaat 6565
Results:Epithelial healing: Complete in 72hours
Visual outcome: All eyes showed improved BCVA except one.The improvement in BCVA was statistically
highly significant (P< 0.001 ) (P =0.00647) The mean preop. BCVA was 6/24 (+/- 2 lines). The mean postop. BCVA is 6/12 (+/- one line).

PTK By Dr. Safaa Refaat 6666
GAINED SNELLEN’S LINES GAINED S. LINES
no lines
1 line
2 lines
3 lines
4 lines
5 lines

PTK By Dr. Safaa Refaat 6767

PTK By Dr. Safaa Refaat 6868
Refractive out comes Two eyes showed a myopic shift.
one eye showed no change in SE.
7 eyes showed a hyperopic shift.
Change in SE statistically insignificant. (P =0.22).
The mean preoperative SE was –0.3750 D(+/-3.1) The mean postoperative SE was+1.075 D(+/-1.8)
The mean change in SE was +1.45 D (+/- 2.16)

PTK By Dr. Safaa Refaat 6969
CHANGE IN REFRACTION.

PTK By Dr. Safaa Refaat 7070
One eye with combined PTK and PRK developed postoperative astigmatism -5.75D compared to – 3.75D preoperative.
Symptomatic outcome
All patients experienced improvement in their quality of vision and decreased symptoms of eye fatigue and irritation.

PTK By Dr. Safaa Refaat 7171
CHANGE IN SE

PTK By Dr. Safaa Refaat 7272
Discussion
Compared to lamellar and PKP, excimer laser PTK is the:Safest & Least aggressive Faster visual recovery.Lower incidence of astigmatism. Could be repeatedLower cost.

PTK By Dr. Safaa Refaat 7373
Szentmáry et al (2004) found that PTK does not appear to impair the outcome of subsequent PKP.
Koreishi et al (2003) in a comparative study bet. primary treatment of lattice dystrophy with PTK versus PKP, they found that PTK alone give equal or better V.A.

PTK By Dr. Safaa Refaat 7474
Stewart et al (2002) had found that 93% of PTK treated cases with corneal dystrophies maintained or improved their BCVA. All were free of symptoms of REETrend towards a hyperopic shift. % 17 showed recurrence of the dystrophy.

PTK By Dr. Safaa Refaat 7575
Dorgu et al (2000) reported the findings of 14 PTK for mid stromal corneal scars:
They noticed that corneal sensitivity, tear film BUT & tear film lipid layer interferometry grades improved gradually and significantly after PTK.

PTK By Dr. Safaa Refaat 7676
In our work, we aimed to study visual and symptomatic outcome of PTK in 10 eyes with superficial corneal opacities.
We attained visual improvement in 9 eyes (90%) and saw that PTK could obviate the need for PKP.
THERE WERE NO SERIOUS COMPLICATION .

PTK By Dr. Safaa Refaat 7777
One patient with combined PTK and PRK no change in the BCVA. Our experience from this case will not encourage combined refractive correction with primary PTK. This could be due to:Unreliable refractionScar induced astigmatismDifferential ablation rate.

PTK By Dr. Safaa Refaat 7878
Conclusion:PTK improves both quality and quantity of vision.PTK can alleviate the need for PKP. The recent advances in PTK techniques:New, ideal modulators. Real time corneal topography feedback.Wave front analysis.
Will allow for reshaping every corneal surface to achieve the optimal corneal contour.

PTK By Dr. Safaa Refaat 7979
THANK YOUTHANK YOU
Related Documents











