Pharmacy Practice Innovations: Best Practices in Care Transitions Michelle Cudnik, PharmD John Moorman, PharmD, BCPS June 27 th , 2013

Pharmacy Practice Innovations: Best Practices in Care Transitions Michelle Cudnik, PharmD John Moorman, PharmD, BCPS June 27 th, 2013.
Dec 17, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Pharmacy Practice Innovations:
Best Practices in Care Transitions
Michelle Cudnik, PharmD
John Moorman, PharmD, BCPS
June 27th, 2013
Michelle Cudnik, PharmDClinical Ambulatory Care Lead
Pharmacist, Summa Health System
Associate Professor of Pharmacy Practice, NEOMED
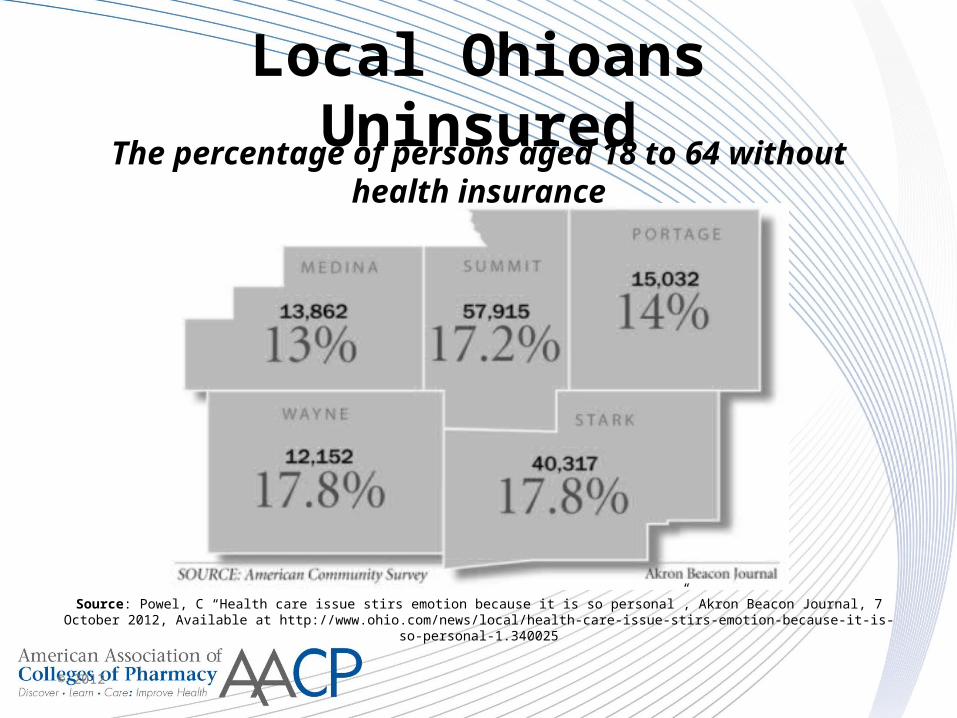
Local Ohioans Uninsured
© 2012
Source: Powel, C “Health care issue stirs emotion because it is so personal”, Akron Beacon Journal, 7 October 2012, Available at http://www.ohio.com/news/local/health-care-issue-stirs-emotion-because-it-is-so-personal-1.340025
The percentage of persons aged 18 to 64 without health insurance
What is the highest percentage of admission rates seen in the country
that are due to 30-day readmissions?
1. 15%
2. 17%
3. 19%
4. 21%
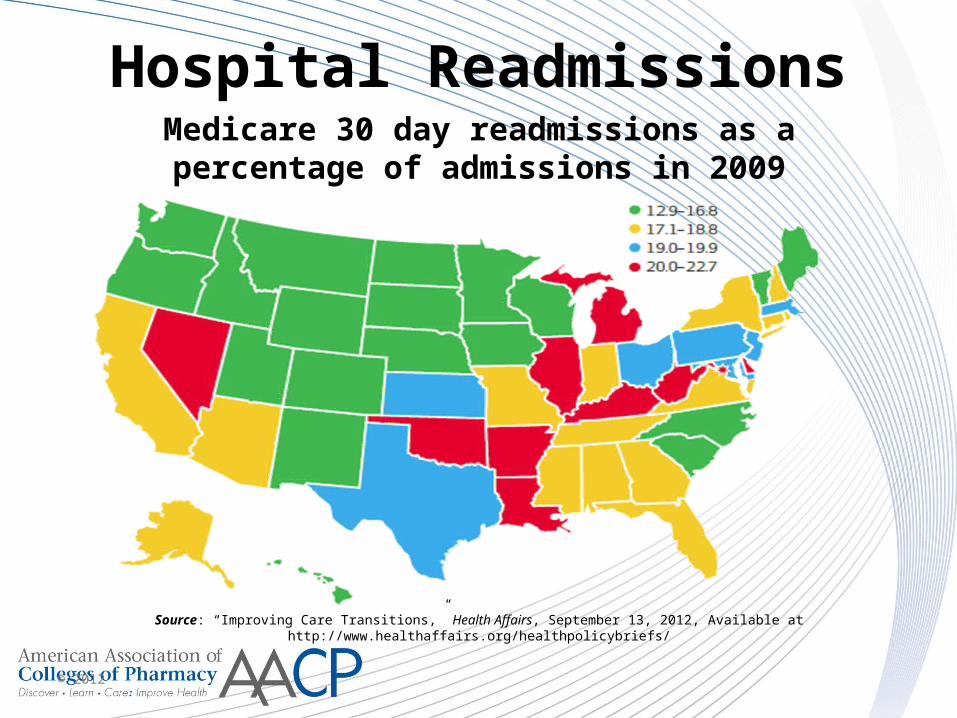
Hospital Readmissions
© 2012
Source: “Improving Care Transitions,” Health Affairs, September 13, 2012, Available at http://www.healthaffairs.org/healthpolicybriefs/
Medicare 30 day readmissions as a percentage of admissions in 2009
Why a new model?
• Institute of Medicine Report 2001, “Crossing the Quality Chasm”– Less than 50% of patients with major chronic
illness receive accepted treatments– Less than 50% have satisfactory disease control– Focus on episodic and not continuous care– Little attention given to the patient’s knowledge,
skills, behavior in managing their own illnessInstitute of Medicine. Crossing the Quality Chasm: A New Health System
for the 21st Century. Washington DC. National Academy Press; 2001
A tested Model: PCMH• Patient-centered (using patient goals)• Physician-guided (EBM, directs the team)• Cost-efficient• Reimbursable (sustainable)• Longitudinal, (goals persist through many
contacts over time)• A continuous healing relationship (not just
services)• Care provided in a variety of settings-Transitions are Key!• “Medical Home” refers to primary responsibility to assemble and interpret
data and assist patient with self care of diseaseThe Advanced Medical Home. American College of Physicians Policy Monograph, 2006
•
National and Regional Relevance
• Model is centerpiece of Affordable Care Act, 2009
• Meaningful Use (15 required core objectives; 5 menu objectives)
• Accountable Care Organization: (89 nationally under Center for Medicare and Medicaid services)
• NCQA (National Committee for Quality Assurance) Patient Centered Medical Home certification
www.cms.gov for meaningful use
www.innovation.cms.gov for accountable care organizations
They all require:
•A new practice focus on quality outcomes.
•Exchange level data systems to track and report outcomes.
•Care delivery systems require team-based care to achieve outcomes.
They all require:
•A new practice focus on quality outcomes.
•Exchange level data systems to track and report outcomes.
•Care delivery systems require team-based care to achieve outcomes.
2011 Patient-Centered Medical Home Standards
• Enhance Access and Continuity• Identify and Manage Patient Populations• Plan and Manage Care• Provide Self-care and Community Support• Track and Coordinate Care• Measure and Improve Performance
National Committee for Quality Assurance 2011
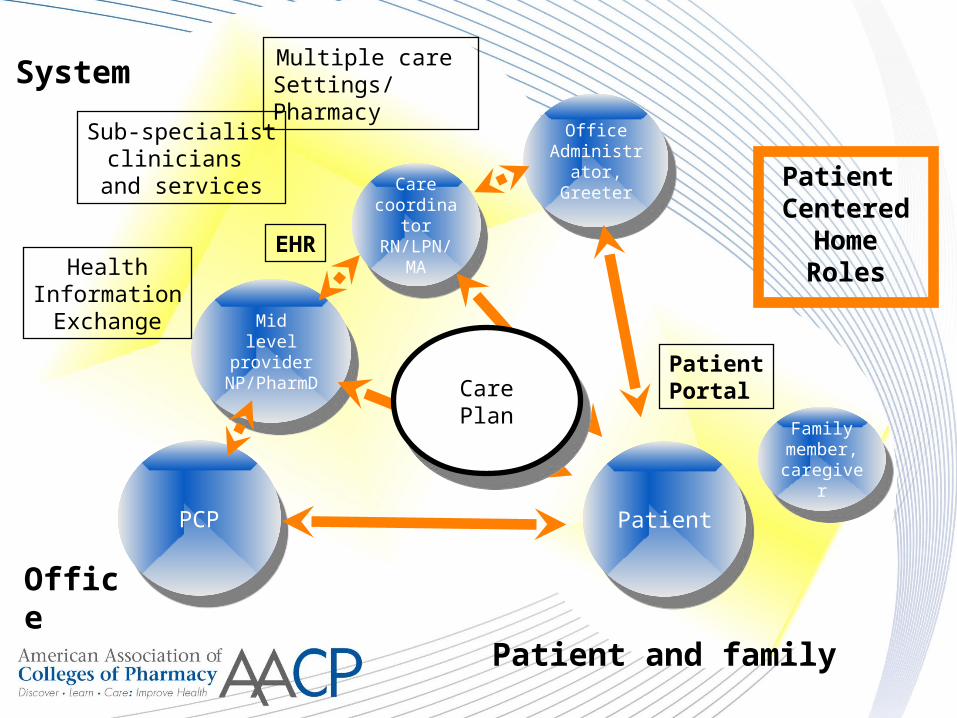
Familymember,caregiver
Familymember,caregiver
PCPPCP
Midlevel providerNP/PharmD
Midlevel providerNP/PharmD
Care coordinatorRN/LPN/
MA
Care coordinatorRN/LPN/
MA
OfficeAdministrator
, Greeter
OfficeAdministrator
, Greeter
PatientPatient
HealthInformationExchange
Sub-specialistclinicians
and services
Multiple care Settings/Pharmacy
System
Office
Patient and family
EHR
PatientPortal
Patient Centered
HomeRoles
CarePlan
CarePlan
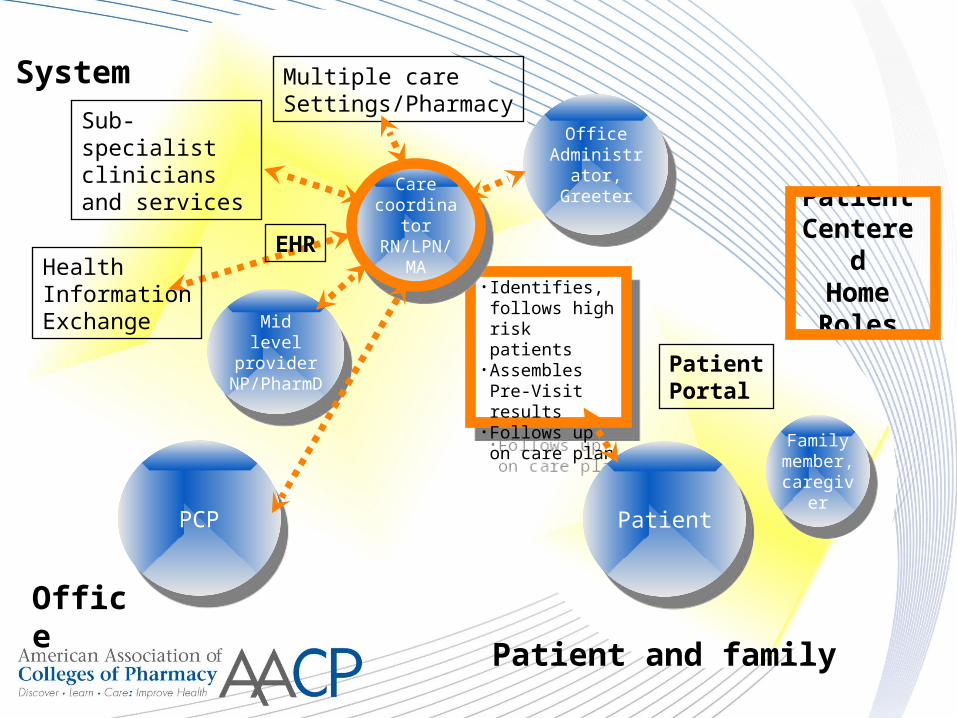
• Identifies, follows high risk patients
•Assembles Pre-Visit results
•Follows up on care plan
• Identifies, follows high risk patients
•Assembles Pre-Visit results
•Follows up on care plan
Familymember,caregiver
Familymember,caregiver
PCPPCP
Midlevel
providerNP/PharmD
Midlevel
providerNP/PharmD
Care coordinatorRN/LPN/
MA
Care coordinatorRN/LPN/
MA
OfficeAdministrator
, Greeter
OfficeAdministrator
, Greeter
PatientPatient
HealthInformationExchange
Sub-specialistclinicians and services
Multiple care Settings/Pharmacy
System
OfficePatient and family
EHR
PatientPortal
Patient Centered
HomeRoles
Summa Health System• 8 hospitals and centers representing over
2,000 inpatient beds• Summit County’s largest employer with over
10,000 employees• 1,200 credentialed physicians and 280
resident physicians• One of top 3 largest integrated healthcare
delivery systems in Ohio • Health Plan (SummaCare)• Affiliated with NEOMED University
Summa Health System Payer Mix
• Commercial/Managed Care: 30%• Self-Pay: 7% (27% in Internal Medicine Center)
• Medicaid: 15%
• Medicare: 47%
My Practice • Akron City Hospital- Internal Medicine Clinic
• Shared Faculty with
NEOMED
• 12,000 patients
(mostly indigent)
• Certified Patient-
Centered Medical
Home
A Day in the Life…
• Collaborative Practice Agreement
• Daily Huddles- identify high-risk patients
• Diabetic Planned visits 3 days per week
• Hypertension Clinic visits 1 day per week
• Medication Therapy Management visits each day
A Day in the Life…
• Key member of the Patient-centered medical home!
• Plan and manage care, coordinate follow-up visits, interface with community pharmacies and focus on continuity of care.
• Facility fee billing
Successes
• Continued improvement in clinical outcome measurements in our diabetic patients
• Improved education to medication residents, faculty and staff in the Internal medicine center
• Comprehensive medication reconciliation completed at all visits
Barriers
• Initial delay in collaborative practice agreement
• Knowledge by healthcare providers of what a pharmacist can offer to patients
• Financial reimbursement for services
Next Steps
• Pilot study of a pharmacist in various primary care clinics within our healthcare system- different days of week (Resources by ACO?)
• Focus on transitions of care for highest-risk patients
• Reimbursement for Transitions of Care visits
John Moorman, PharmD, BCPSPharmacotherapy Specialist,
Endocrinology, Akron General Medical Center
Assistant Professor of Pharmacy Practice, NEOMED
“The scenario in which a patient moves from one care setting to
another”
Cost of poor care transition
34,500 patients discharged and readmitted on the same day in 1996-1997
Cost = $226 million
J. Gibbs Brown, personal communication, February 11, 2000
Cost of poor care transition
20% of Medicare hospitalizations followed by readmission within 30 days in 2003-2004
~50% had no physician visit before readmission
N Engl J Med 2009;360:1418-28
Cost of poor care transition
19% of Medicare discharges followed by adverse event within 30 days
66% were drug-related
Ann Intern Med 2003;138:161-7
Cost of poor care transition
Potential for cost savings by preventing unplanned readmissions
$17.4 billion
N Engl J Med 2009;360:1418-28
Cost of poor care transition
A decrease in diabetes medication adherence results in a 58% increase in
hospitalizations
…and an 81% increase in all-cause mortality
Arch Intern Med 2006;166:1836-41
National Transitions of Care Coalition (NTOCC)
• Implementation and evaluation outline
• Multiple resources developed:– TOC checklist– Interventions for low health literacy– Standardized forms– Metrics for tracking outcomes
General recommendations
• Improve communication
• Implement electronic medical records
• Establish points of accountability
• Increase use of case management
• Expand role of pharmacist in TOC
• Implement payment systems
• Develop performance measures
When implementing a new TOC service, when should one decide which
metrics to track?
1. Once management has been approached
2. Once personnel have been hired
3. Once a gap in care has been identified
4. Once a service has been implemented
Akron General Medical Center• 511 adult-bed
teaching hospital– Affiliated with
Northeast Ohio Medical University
• Significant proportion of admissions for underserved patients
Personal experiences with TOC
A day in the life…
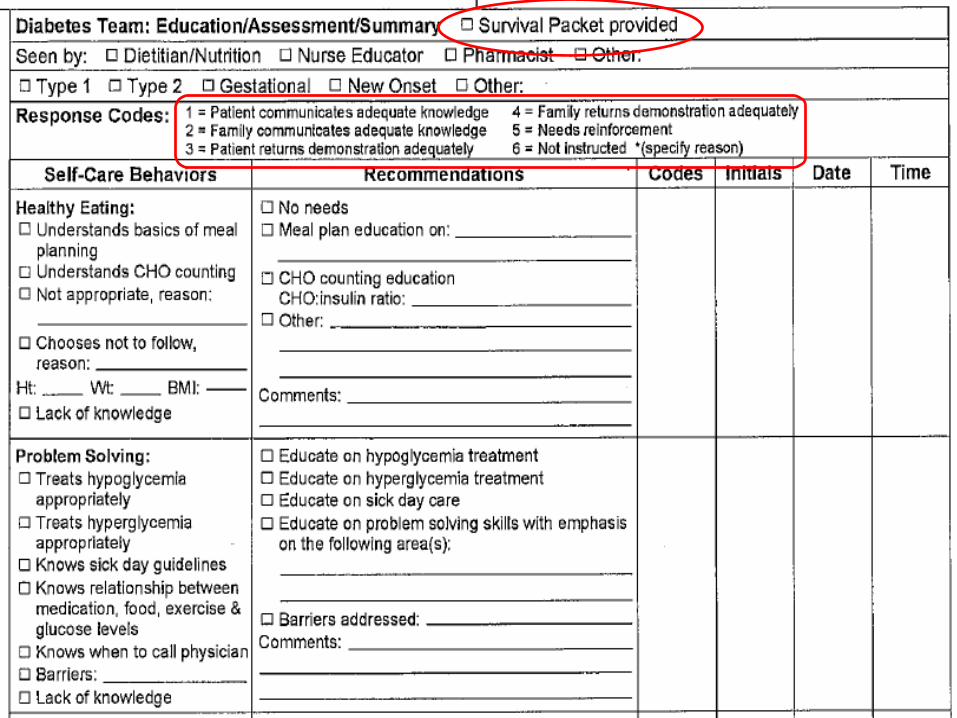
• Inpatient diabetes management team– Endocrinologist– Pharmacist– Diabetes educators (RN, CDE)– Dieticians
• Outpatient transitional care clinic– “Bridge” clinic– Private endocrinology practice
Interventions
• Inpatient education
• Medication reconciliation
• Involve social work/care management
• Plan development– Medication regimen– Goals of therapy– Follow-up
Follow-up structure
• Follow-up plan established– Discharge location– Need for transitional care visit?
• “Bridge” clinic appointments set as inpatient– Not intended as chronic management– Communicated to primary care physician
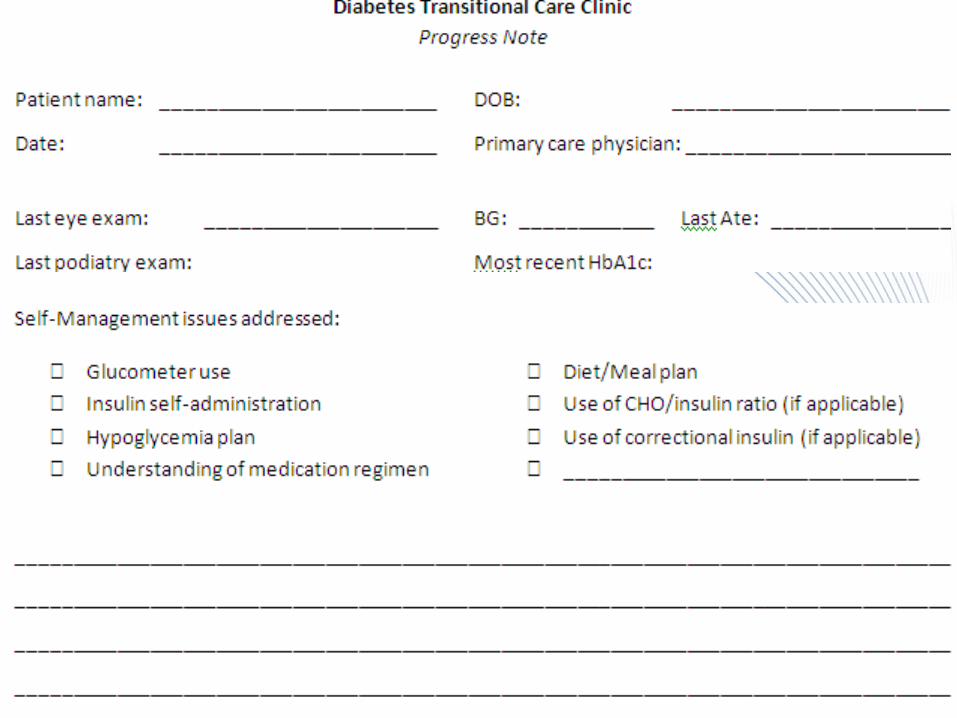
“Bridge” clinic
• Review of discharge medication list
• Goals of therapy reviewed
• Education/Literature provided
• Medication therapy performed if needed– Collaborative practice agreement
• Follow-up plan established
• All information sent to primary care

Successes
• Initially, patients instructed to call for appointment– Scheduling while inpatient improved show rate
• As “Bridge” appointments increased, readmission rates decreased– Significantly lower than general readmission rate
• Increased consultations by hospitalist groups/attending physicians
Barriers
• Private practice vs. health system– Inability to bill for services– Use of EMR limited
• Limited to patients seen on inpatient service– Collaborative practice agreement– Concern over number of consults per physician
• Length of stay
Next steps• Diabetes Needs Assessment
– Diabetic patients admitted to hospital prompts immediate referral
– Triage based on need for education/management• Increase exposure to at-risk population
• Intention to begin education on day 1– Potential for decreased length of stay
• Avoids “last-hour” consultations
– Identify barriers earlier in hospital stay
Conclusions
• Established role for pharmacists in TOC– Diabetes vs. other disease states– Role needs to be expanded
• Multiple interventions shown to be beneficial– Discharge counseling/med rec.
• Implementing programs may be challenging– Requires focused approach with proper personnel– Know metrics before implementing
Conclusions
• These are just 2 models that focus on pharmacists involvement in transitions of care/continuity of care
• These models can be adapted to other settings to provide innovative pharmacy services!

Thank you for your attention!
Questions?
Related Documents











