Coverage may depend on previous use or trial of another drug. Step Therapy Medication Name Medication Class Preferred Products ANDRODERM Androgens Must try Androgel TESTIM Androgens Must try Androgel Axiron Androgens Must try Androgel Fortesta Androgens Must try Androgel Striant Androgens Must try Androgel Lamisil Antifungal If patient has HIV, Cancer, or Diabetes Tier 2, all other Tier 3 Sporanox Antifungal If patient has HIV, Cancer, or Diabetes Tier 2, all other Tier 3 ABILIFY Antipsychotics Must try 2 of the following: risperidone, Geodon, Seroquel/-XR, Zyprexa ABILIFY Antipsychotics Must try 2 of the following: risperidone, Geodon, Seroquel/-XR, Zyprexa FANAPT Antipsychotics Must try 2 of the following: risperidone, Geodon, Seroquel/-XR, Zyprexa INVEGA Antipsychotics Must try 2 of the following: risperidone, Geodon, Seroquel/-XR, Zyprexa SAPHRIS Antipsychotics Must try 2 of the following: risperidone, Geodon, Seroquel/-XR, Zyprexa Atacand/-HCT ARB Must try 2 of the following: generics, Diovan/-HCT, Micardis/-HCT, losartan/-HCT Benicar/-HCT ARB Must try 2 of the following: generics, Diovan/-HCT, Micardis/-HCT, losartan/-HCT Teveten/-HCT ARB Must try 2 of the following: generics, Diovan/-HCT, Micardis/-HCT, losartan/-HCT Edarbi/Edarbyclor ARB Must try 2 of the following: generics, Diovan/-HCT, Micardis/-HCT, losartan/-HCT Actonel Bisphosphonates Must try one of the following: alendronate or ibandronate Atelvia Bisphosphonates Must try one of the following: alendronate or ibandronate Altoprev Cholesterol Generic Statin and then Crestor Lescol XL Cholesterol Generic Statin and then Crestor Vytorin Cholesterol Generic Statin and then Crestor Byetta Diabetes Requires trial of metformin, sulfonylurea, or TZD prior to approval Symlin Diabetes Requires usage of another insulin Antara Fenofibrates Generic fenofibrates or gemfibrozil Fenoglide Fenofibrates Generic fenofibrates or gemfibrozil Fibricor Fenofibrates Generic fenofibrates or gemfibrozil Lipofen Fenofibrates Generic fenofibrates or gemfibrozil THINKING HEALTH FORWARD Pharmacy Benefit Limitations List Welcome to Cox HealthPlans! We appreciate the opportunity to provide health care coverage to the members of your plan. This list of medications is provided for your review and for review with your physician. These medications may require additional information or assistance from your physician prior to your first fill under your new benefits. Please review this list for any medications plan members are taking. These medications may require additional medical information, may require the use of a lower cost alternative before your current medication may be covered, or may be limited in quantity for coverage under your health plan. If you need assistance transitioning to a formulary medication, please contact your physician or complete the Self-Referral Case Management form for assistance from our medical staff in our Welcome Aboard program. Please note: Medications prescribed by your physician may be filled with the medication and dosage indicated. However, certain medications may not be covered in full or in part by your health insurance coverage. This medication list and the full formulary list do not imply all medications listed are covered benefits. Please consult your Schedule of Benefits for coverage information. Full formulary and additional information regarding each medication may be obtained at www.coxhealthplans.com or by contacting Catamaran at 888.341.8578.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Coverage may depend on previous use or trial of another drug. Step TherapyMedication Name Medication Class Preferred ProductsANDRODERM Androgens Must try Androgel
TESTIM Androgens Must try Androgel
Axiron Androgens Must try Androgel
Fortesta Androgens Must try Androgel
Striant Androgens Must try Androgel
Lamisil Antifungal If patient has HIV, Cancer, or Diabetes Tier 2, all other Tier 3
Sporanox Antifungal If patient has HIV, Cancer, or Diabetes Tier 2, all other Tier 3
ABILIFY Antipsychotics Must try 2 of the following: risperidone, Geodon, Seroquel/-XR, Zyprexa
ABILIFY Antipsychotics Must try 2 of the following: risperidone, Geodon, Seroquel/-XR, Zyprexa
FANAPT Antipsychotics Must try 2 of the following: risperidone, Geodon, Seroquel/-XR, Zyprexa
INVEGA Antipsychotics Must try 2 of the following: risperidone, Geodon, Seroquel/-XR, Zyprexa
SAPHRIS Antipsychotics Must try 2 of the following: risperidone, Geodon, Seroquel/-XR, Zyprexa
Atacand/-HCT ARB Must try 2 of the following: generics, Diovan/-HCT, Micardis/-HCT, losartan/-HCT
Benicar/-HCT ARB Must try 2 of the following: generics, Diovan/-HCT, Micardis/-HCT, losartan/-HCT
Teveten/-HCT ARB Must try 2 of the following: generics, Diovan/-HCT, Micardis/-HCT, losartan/-HCT
Edarbi/Edarbyclor ARB Must try 2 of the following: generics, Diovan/-HCT, Micardis/-HCT, losartan/-HCT
Actonel Bisphosphonates Must try one of the following: alendronate or ibandronate
Atelvia Bisphosphonates Must try one of the following: alendronate or ibandronate
Altoprev Cholesterol Generic Statin and then Crestor
Lescol XL Cholesterol Generic Statin and then Crestor
Vytorin Cholesterol Generic Statin and then Crestor
Byetta Diabetes Requires trial of metformin, sulfonylurea, or TZD prior to approval
Symlin Diabetes Requires usage of another insulin
Antara Fenofibrates Generic fenofibrates or gemfibrozil
Fenoglide Fenofibrates Generic fenofibrates or gemfibrozil
Fibricor Fenofibrates Generic fenofibrates or gemfibrozil
Lipofen Fenofibrates Generic fenofibrates or gemfibrozil
THINKING HEALTH FORWARD
Pharmacy Benefit Limitations ListWelcome to Cox HealthPlans! We appreciate the opportunity to provide health care coverage to the members of your plan.
This list of medications is provided for your review and for review with your physician. These medications may require additional information or assistance from your physician prior to your first fill under your new benefits.
Please review this list for any medications plan members are taking. These medications may require additional medical information, may require the use of a lower cost alternative before your current medication may be covered, or may be limited in quantity for coverage under your health plan.
If you need assistance transitioning to a formulary medication, please contact your physician or complete the Self-Referral Case Management form for assistance from our medical staff in our Welcome Aboard program.
Please note: Medications prescribed by your physician may be filled with the medication and dosage indicated. However, certain medications may not be covered in full or in part by your health insurance coverage. This medication list and the full formulary list do not imply all medications listed are covered benefits. Please consult your Schedule of Benefits for coverage information. Full formulary and additional information regarding each medication may be obtained at www.coxhealthplans.com or by contacting Catamaran at 888.341.8578.
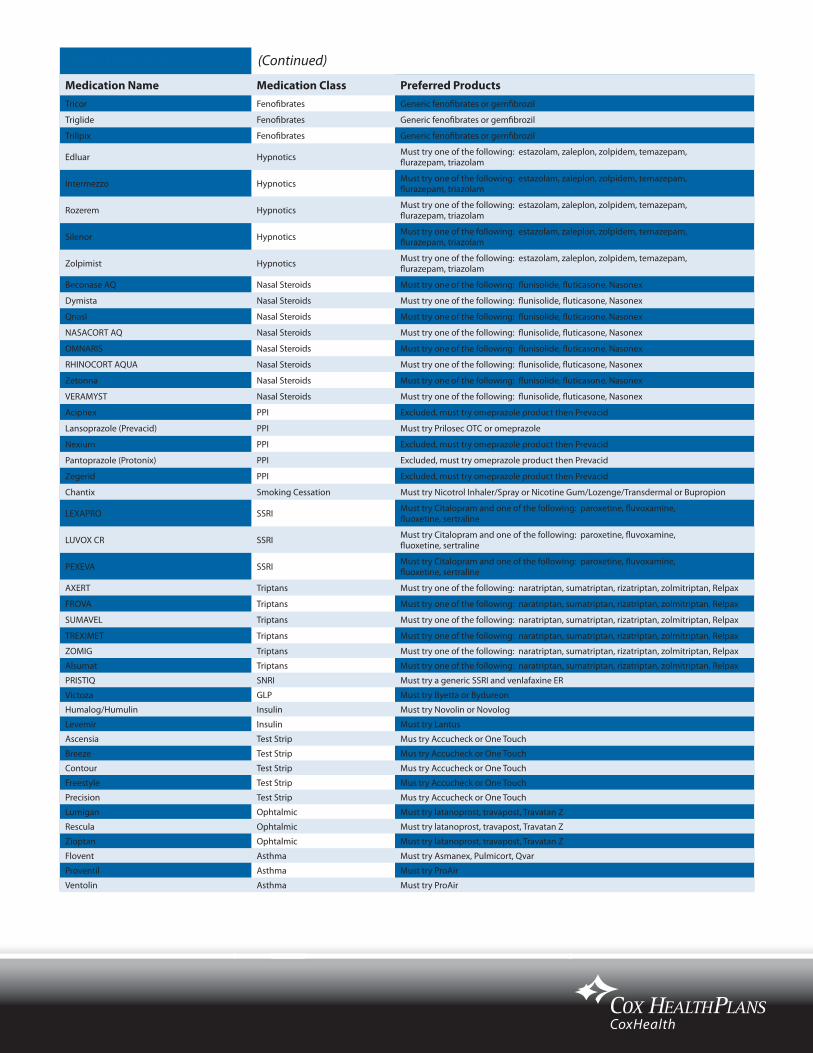
Medication Name Medication Class Preferred ProductsTricor Fenofibrates Generic fenofibrates or gemfibrozil
Triglide Fenofibrates Generic fenofibrates or gemfibrozil
Trilipix Fenofibrates Generic fenofibrates or gemfibrozil
Edluar Hypnotics Must try one of the following: estazolam, zaleplon, zolpidem, temazepam, flurazepam, triazolam
Intermezzo Hypnotics Must try one of the following: estazolam, zaleplon, zolpidem, temazepam, flurazepam, triazolam
Rozerem Hypnotics Must try one of the following: estazolam, zaleplon, zolpidem, temazepam, flurazepam, triazolam
Silenor Hypnotics Must try one of the following: estazolam, zaleplon, zolpidem, temazepam, flurazepam, triazolam
Zolpimist Hypnotics Must try one of the following: estazolam, zaleplon, zolpidem, temazepam, flurazepam, triazolam
Beconase AQ Nasal Steroids Must try one of the following: flunisolide, fluticasone, Nasonex
Dymista Nasal Steroids Must try one of the following: flunisolide, fluticasone, Nasonex
Qnasl Nasal Steroids Must try one of the following: flunisolide, fluticasone, Nasonex
NASACORT AQ Nasal Steroids Must try one of the following: flunisolide, fluticasone, Nasonex
OMNARIS Nasal Steroids Must try one of the following: flunisolide, fluticasone, Nasonex
RHINOCORT AQUA Nasal Steroids Must try one of the following: flunisolide, fluticasone, Nasonex
Zetonna Nasal Steroids Must try one of the following: flunisolide, fluticasone, Nasonex
VERAMYST Nasal Steroids Must try one of the following: flunisolide, fluticasone, Nasonex
Aciphex PPI Excluded, must try omeprazole product then Prevacid
Lansoprazole (Prevacid) PPI Must try Prilosec OTC or omeprazole
Nexium PPI Excluded, must try omeprazole product then Prevacid
Pantoprazole (Protonix) PPI Excluded, must try omeprazole product then Prevacid
Zegerid PPI Excluded, must try omeprazole product then Prevacid
Chantix Smoking Cessation Must try Nicotrol Inhaler/Spray or Nicotine Gum/Lozenge/Transdermal or Bupropion
LEXAPRO SSRI Must try Citalopram and one of the following: paroxetine, fluvoxamine, fluoxetine, sertraline
LUVOX CR SSRI Must try Citalopram and one of the following: paroxetine, fluvoxamine, fluoxetine, sertraline
PEXEVA SSRI Must try Citalopram and one of the following: paroxetine, fluvoxamine, fluoxetine, sertraline
AXERT Triptans Must try one of the following: naratriptan, sumatriptan, rizatriptan, zolmitriptan, Relpax
FROVA Triptans Must try one of the following: naratriptan, sumatriptan, rizatriptan, zolmitriptan, Relpax
SUMAVEL Triptans Must try one of the following: naratriptan, sumatriptan, rizatriptan, zolmitriptan, Relpax
TREXIMET Triptans Must try one of the following: naratriptan, sumatriptan, rizatriptan, zolmitriptan, Relpax
ZOMIG Triptans Must try one of the following: naratriptan, sumatriptan, rizatriptan, zolmitriptan, Relpax
Alsumat Triptans Must try one of the following: naratriptan, sumatriptan, rizatriptan, zolmitriptan, Relpax
PRISTIQ SNRI Must try a generic SSRI and venlafaxine ER
Victoza GLP Must try Byetta or Bydureon
Humalog/Humulin Insulin Must try Novolin or Novolog
Levemir Insulin Must try Lantus
Ascensia Test Strip Mus try Accucheck or One Touch
Breeze Test Strip Mus try Accucheck or One Touch
Contour Test Strip Mus try Accucheck or One Touch
Freestyle Test Strip Mus try Accucheck or One Touch
Precision Test Strip Mus try Accucheck or One Touch
Lumigan Ophtalmic Must try latanoprost, travapost, Travatan Z
Rescula Ophtalmic Must try latanoprost, travapost, Travatan Z
Zioptan Ophtalmic Must try latanoprost, travapost, Travatan Z
Flovent Asthma Must try Asmanex, Pulmicort, Qvar
Proventil Asthma Must try ProAir
Ventolin Asthma Must try ProAir
(Continued)Step Therapy

Medication Name Medication Class Quantity Limit Time FrameBupropion (Wellbutrin 100mg) Antidepressant 90 Every 30 days
Bupropion (Wellbutrin 75mg) Antidepressant 120 Every 30 days
Bupropion (Wellbutrin SR) Antidepressant 60 Every 30 days
Bupropion (Wellbutrin XL) Antidepressant 30 Every 30 days
Citalopram (Celexa) Antidepressant 30 Every 30 days
Cymbalta Antidepressant 60 Every 30 days
Fluoxetine (Sarafem) Antidepressant 30 Every 30 days
Lexapro Antidepressant 30 Every 30 days
Paroxetine (Paxil) Antidepressant 30 Every 30 days
Paroxetine CR (Paxil CR) Antidepressant 30 Every 30 days
Sertraline (Zoloft) Antidepressant 30 Every 30 days
fluconazole (Diflucan) Antifungal 4 Every 30 days
Actonel 35mg Bisphosphonate 4 Every 30 days
Actonel 5/30mg Bisphosphonate 30 Every 30 days
Actonel with Calcium Bisphosphonate 28 Every 30 days
Boniva 150mg Bisphosphonate 1 Every 30 days
Boniva 2.5mg Bisphosphonate 30 Every 30 days
Fosamax 35/70mg Bisphosphonate 4 Every 30 days
Fosamax 5/10/40mg Bisphosphonate 30 Every 30 days
Fosamax Plus D Bisphosphonate 4 Every 30 days
Fosamax Solution Bisphosphonate 300 Every 30 days
Advicor Cholesterol 30 Every 30 days
Altocor Cholesterol 30 Every 30 days
Crestor Cholesterol 30 Every 30 days
Lescol Cholesterol 30 Every 30 days
Lescol XL Cholesterol 30 Every 30 days
Lipitor Cholesterol 30 Every 30 days
lovastatin (Mevacor) Cholesterol 30 Every 30 days
pravastatin (Pravachol) Cholesterol 30 Every 30 days
simvastatin (Zocor) Cholesterol 30 Every 30 days
Vytorin Cholesterol 30 Every 30 days
Zetia Cholesterol 30 Every 30 days
Tussionex Cough and Cold 120 Every 30 days
Glucagon, Glucagen Diabetes 2 Every 365 days
Insulin Injecting Devices Diabetes 2 Every 365 days
Cialis Eryctile Dysfunction 6 Every 30 days
Levitra Eryctile Dysfunction 6 Every 30 days
Muse/Edex/Caverject Eryctile Dysfunction 6 Every 30 days
Viagra Eryctile Dysfunction 6 Every 30 days
Depo Provera Family Planning/Hormone Replacement 1 Every 90 days
Estring Family Planning/Hormone Replacement 1 Every 90 days
Femring Family Planning/Hormone Replacement 1 Every 90 days
Lunelle Family Planning/Hormone Replacement 1 Every 30 days
Nuvaring Family Planning/Hormone Replacement 1 Every 30 days
Amerge Migraine 18 Per month (Whole Class)
Axert Migraine 18 Per month (Whole Class)
Frova Migraine 18 Per month (Whole Class)
Maxalt/-MLT Migraine 18 Per month (Whole Class)
Relpax Migraine 18 Per month (Whole Class)
Sumatriptan (Imitrex) Migraine 18 Per month (Whole Class)
Zomig/-ZMT Migraine 18 Per month (Whole Class)
Coverage may be limited to specific quantities per prescription and for time period. Quantity Limited

Medication Name Medication Class Quantity Limit Time FrameAllegra D 12hr Non Sedating Antihistamines 60 Every 30 days
Allegra D 24 hr Non Sedating Antihistamines 30 Every 30 days
Cetirizine (Zyrtec) Non Sedating Antihistamines 30 Every 30 days
Cetirizine /-D (Zyrtec/-D) Non Sedating Antihistamines 60 Every 30 days
Clarinex/-D Non Sedating Antihistamines 30 Every 30 days
Fexofenadine 180mg (Allegra) Non Sedating Antihistamines 30 Every 30 days
Fexofenadine 30mg/60mg (Allegra) Non Sedating Antihistamines 60 Every 30 days
Xyzal Non Sedating Antihistamines 30 Every 30 days
Celebrex 100/200mg NSAID 60 Every 30 days
Celebrex 400mg NSAID 30 Every 30 days
Lansoprazole (Prevacid) PPI 30 Every 30 days
Omeprazole 40mg (Prilosec) PPI 30 Every 30 days
Adcirca Pulmonary Arterial Hypertension 90 Every 30 days
Revatio Pulmonary Arterial Hypertension 90 Every 30 days
Advair Respiratory 60 Every 30 days
Aerobid Respiratory 14 Every 30 days
Aerochamber, Inspirease Respiratory 1 Every 365 days
Alupent Respiratory 28 Every 30 days
Atrovent Respiratory 30 Every 30 days
Atrovent HFA Respiratory 26 Every 30 days
Azmacort Respiratory 41 Every 30 days
Combivent Respiratory 30 Every 30 days
Epi-Pen, Epi-Pen JR Respiratory 2 Every 365 days
Flovent HFA Respiratory 26 Every 30 days
Flovent Rotadisk Respiratory 120 Every 30 days
Intal Respiratory 30 Every 30 days
Maxair Autohaler Respiratory 28 Every 30 days
Proventil HFA/Ventolin HFA Respiratory 18 Every 30 days
Proventil/Ventolin Respiratory 51 Every 30 days
Pulmicort Respules Respiratory 140 Every 30 days
Pulmicort Turbohaler Respiratory 2 Every 30 days
Qvar Respiratory 16 Every 30 days
Serevent Diskus Respiratory 120 Every 30 days
Tilade Respiratory 34 Every 30 days
Twinject Respiratory 2 Every 365 days
Ambien CR Sleep Aid 15 Every 30 days for all sleep aids combined
Lunesta Sleep Aid 15 Every 30 days for all sleep aids combined
Rozerem Sleep Aid 15 Every 30 days for all sleep aids combined
Zaleplon (Sonata) Sleep Aid 15 Every 30 days for all sleep aids combined
Zolpidem (Ambien) Sleep Aid 15 Every 30 days for all sleep aids combined
Chantix Smoking Cessation 2 Cycles 6 months total
(Continued)Quantity Limited

Medication Name Medication Class RationaleADHD Stimulant Class (Ritalin, Adderall, etc) ADHD Stimulant Class Require PA for members 19 and older
Bupropion (Wellbutrin) Antidepression Not for use in smoking cessation or weight loss
Nuvigil Antinarcolepsy Approved for FDA Indications of: Narcolepsy, Idiopathic Hypersomnia, OSAHS, SWSD, Fatigue due to MS.
Provigil/Modafanil AntinarcolepsyApproved for FDA Indications of: Narcolepsy, Idiopathic Hypersomnia, OSAHS, SWSD, Fatigue due to MS. Also requires trial of Nuvigil prior to approval.
Abilify Antipsychotic Requires trial of 2 antidepressants prior to approval for depression. For use in Autisim, requires trial of risperidone.
Viracept HIV Cannot be pregnant
Viagra, Cialis, Levitra, Muse Erectile Dysfunction Requires diagnosis
Solodyn Acne Products Requires trial of minocycline
Doryx Acne Products Requires trial of doxycycline
Medication Name Medication Class Medication Name Medication Class Medication Name Medication Class
5-FLUOROURACIL Specialty ARANESP ALBUMIN FREE SURECLICK Specialty CALCIUM FOLINATE Specialty
8-MOP Specialty ARCALYST Specialty CALCIUM LEVULINATE Specialty
ABRAXANE Specialty AREDIA Specialty CALOMEL Specialty
ACTEMRA Specialty ARIXTRA Specialty CAMPATH Specialty
ACTHAR HP Specialty ASTAGRAF XL Specialty CAMPTOSAR Specialty
ACTIMMUNE Specialty ATROPINE METHONITRATE Specialty CAPRELSA Specialty
ADCETRIS Specialty AUBAGIO Specialty CARBAGLU Specialty
ADCIRCA Specialty AUTOPLEX T Specialty CARBOPLATIN Specialty
ADEFOVIR DIPIVOXIL Specialty AVASTIN Specialty CARIMUNE Specialty
ADEMPAS Specialty AVONEX Specialty CARIMUNE NANOFILTERED Specialty
ADRIAMYCIN Specialty AVONEX PEN Specialty CAYSTON Specialty
ADRUCIL Specialty AZACITIDINE Specialty CEFOTAXIME SODIUM Specialty
ADVATE Specialty BARACLUDE Specialty CEREDASE Specialty
AFINITOR Specialty BAYGAM Specialty CEREZYME SpecialtyALCLOMETASONE DIPROPIONATE Specialty BAYRHO-D Specialty CERIUM OXALATE Specialty
ALDURAZYME Specialty BEBULIN Specialty CETROTIDE Specialty
ALFERON N Specialty BEBULIN VH Specialty CETYLPYRIDINIUM CHLORIDE Specialty
ALIMTA Specialty BENEFIX Specialty CHLOROTHYMOL Specialty
ALKERAN Specialty BENLYSTA Specialty CHLORPROMAZINE Specialty
ALOXI Specialty BERINERT Specialty CHLORPROPAMIDE Specialty
ALPHANATE Specialty BETASERON Specialty CHOREX-10 SpecialtyALPHANATE/VON WILLEBRAND FACTOR COMPLEX/HUMAN
Specialty BETHKIS Specialty CHORIONIC GONADOTROPIN Specialty
ALPHANINE SD Specialty BICNU Specialty CHORIONIC GONADOTROPIN (HUMAN) Specialty
AMEVIVE Specialty BIVIGAM Specialty CHORIONIC GONADOTROPIN W/DILUENT Specialty
AMIFOSTINE Specialty BLENOXANE Specialty CIDOFOVIR Specialty
AMPYRA Specialty BLEOMYCIN SULFATE Specialty CIMZIA Specialty
ANZEMET Specialty BONIVA Specialty CIMZIA STARTER KIT Specialty
APOKYN Specialty BOSULIF Specialty CINRYZE Specialty
ARALAST Specialty BOTOX Specialty CISPLATIN Specialty
ARALAST NP Specialty BRAVELLE Specialty CLADRIBINE Specialty
ARANESP ALBUMIN FREE Specialty BUSULFEX Specialty COLISTIMETHATE SODIUM Specialty
Requires specific physician request process.
Requiring prior authorization.
Prior Authorization
Specialty Medications
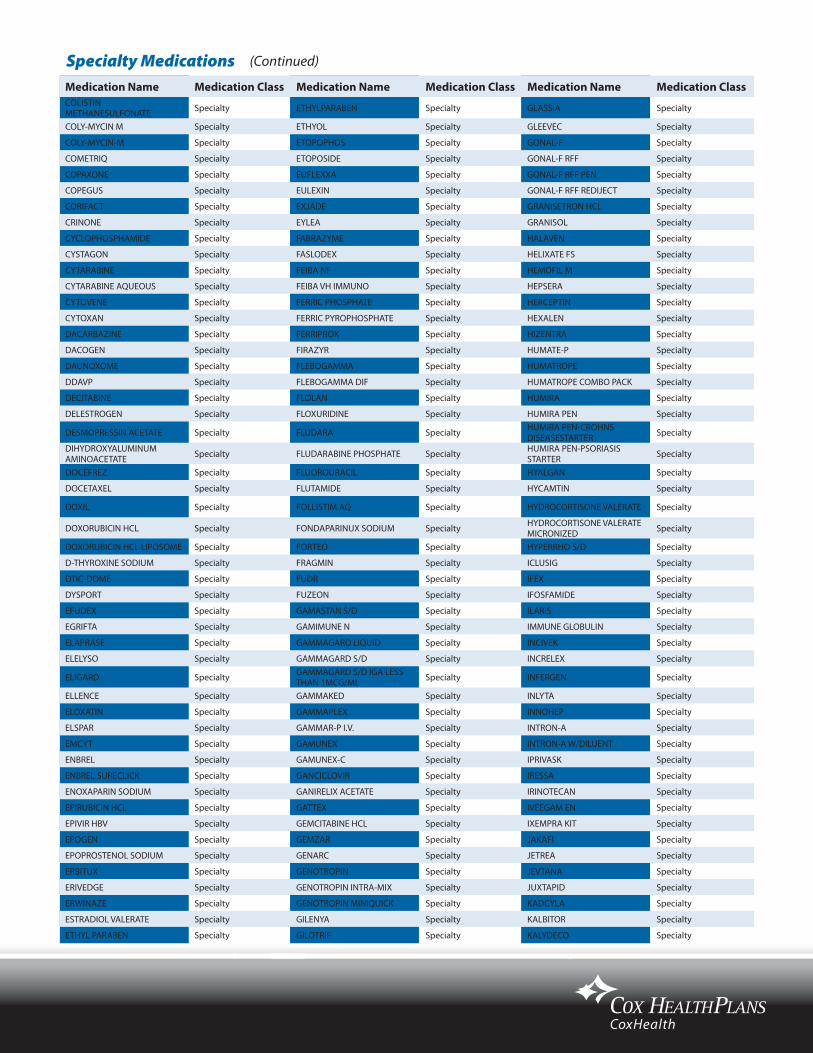
Medication Name Medication Class Medication Name Medication Class Medication Name Medication ClassCOLISTIN METHANESULFONATE Specialty ETHYLPARABEN Specialty GLASSIA Specialty
COLY-MYCIN M Specialty ETHYOL Specialty GLEEVEC Specialty
COLY-MYCIN-M Specialty ETOPOPHOS Specialty GONAL-F Specialty
COMETRIQ Specialty ETOPOSIDE Specialty GONAL-F RFF Specialty
COPAXONE Specialty EUFLEXXA Specialty GONAL-F RFF PEN Specialty
COPEGUS Specialty EULEXIN Specialty GONAL-F RFF REDIJECT Specialty
CORIFACT Specialty EXJADE Specialty GRANISETRON HCL Specialty
CRINONE Specialty EYLEA Specialty GRANISOL Specialty
CYCLOPHOSPHAMIDE Specialty FABRAZYME Specialty HALAVEN Specialty
CYSTAGON Specialty FASLODEX Specialty HELIXATE FS Specialty
CYTARABINE Specialty FEIBA NF Specialty HEMOFIL M Specialty
CYTARABINE AQUEOUS Specialty FEIBA VH IMMUNO Specialty HEPSERA Specialty
CYTOVENE Specialty FERRIC PHOSPHATE Specialty HERCEPTIN Specialty
CYTOXAN Specialty FERRIC PYROPHOSPHATE Specialty HEXALEN Specialty
DACARBAZINE Specialty FERRIPROX Specialty HIZENTRA Specialty
DACOGEN Specialty FIRAZYR Specialty HUMATE-P Specialty
DAUNOXOME Specialty FLEBOGAMMA Specialty HUMATROPE Specialty
DDAVP Specialty FLEBOGAMMA DIF Specialty HUMATROPE COMBO PACK Specialty
DECITABINE Specialty FLOLAN Specialty HUMIRA Specialty
DELESTROGEN Specialty FLOXURIDINE Specialty HUMIRA PEN Specialty
DESMOPRESSIN ACETATE Specialty FLUDARA Specialty HUMIRA PEN-CROHNS DISEASESTARTER Specialty
DIHYDROXYALUMINUM AMINOACETATE Specialty FLUDARABINE PHOSPHATE Specialty HUMIRA PEN-PSORIASIS
STARTER Specialty
DOCEFREZ Specialty FLUOROURACIL Specialty HYALGAN Specialty
DOCETAXEL Specialty FLUTAMIDE Specialty HYCAMTIN Specialty
DOXIL Specialty FOLLISTIM AQ Specialty HYDROCORTISONE VALERATE Specialty
DOXORUBICIN HCL Specialty FONDAPARINUX SODIUM Specialty HYDROCORTISONE VALERATE MICRONIZED Specialty
DOXORUBICIN HCL LIPOSOME Specialty FORTEO Specialty HYPERRHO S/D Specialty
D-THYROXINE SODIUM Specialty FRAGMIN Specialty ICLUSIG Specialty
DTIC-DOME Specialty FUDR Specialty IFEX Specialty
DYSPORT Specialty FUZEON Specialty IFOSFAMIDE Specialty
EFUDEX Specialty GAMASTAN S/D Specialty ILARIS Specialty
EGRIFTA Specialty GAMIMUNE N Specialty IMMUNE GLOBULIN Specialty
ELAPRASE Specialty GAMMAGARD LIQUID Specialty INCIVEK Specialty
ELELYSO Specialty GAMMAGARD S/D Specialty INCRELEX Specialty
ELIGARD Specialty GAMMAGARD S/D IGA LESS THAN 1MCG/ML Specialty INFERGEN Specialty
ELLENCE Specialty GAMMAKED Specialty INLYTA Specialty
ELOXATIN Specialty GAMMAPLEX Specialty INNOHEP Specialty
ELSPAR Specialty GAMMAR-P I.V. Specialty INTRON-A Specialty
EMCYT Specialty GAMUNEX Specialty INTRON-A W/DILUENT Specialty
ENBREL Specialty GAMUNEX-C Specialty IPRIVASK Specialty
ENBREL SURECLICK Specialty GANCICLOVIR Specialty IRESSA Specialty
ENOXAPARIN SODIUM Specialty GANIRELIX ACETATE Specialty IRINOTECAN Specialty
EPIRUBICIN HCL Specialty GATTEX Specialty IVEEGAM EN Specialty
EPIVIR HBV Specialty GEMCITABINE HCL Specialty IXEMPRA KIT Specialty
EPOGEN Specialty GEMZAR Specialty JAKAFI Specialty
EPOPROSTENOL SODIUM Specialty GENARC Specialty JETREA Specialty
ERBITUX Specialty GENOTROPIN Specialty JEVTANA Specialty
ERIVEDGE Specialty GENOTROPIN INTRA-MIX Specialty JUXTAPID Specialty
ERWINAZE Specialty GENOTROPIN MINIQUICK Specialty KADCYLA Specialty
ESTRADIOL VALERATE Specialty GILENYA Specialty KALBITOR Specialty
ETHYL PARABEN Specialty GILOTRIF Specialty KALYDECO Specialty
(Continued)Specialty Medications
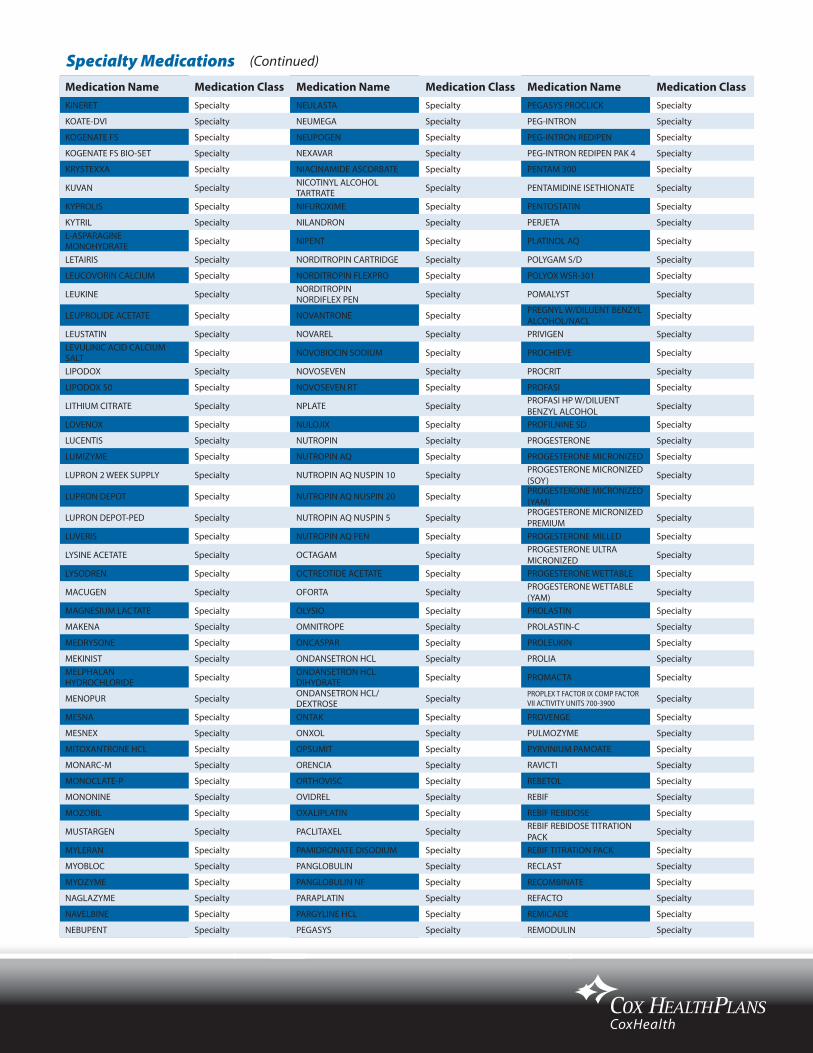
Medication Name Medication Class Medication Name Medication Class Medication Name Medication ClassKINERET Specialty NEULASTA Specialty PEGASYS PROCLICK Specialty
KOATE-DVI Specialty NEUMEGA Specialty PEG-INTRON Specialty
KOGENATE FS Specialty NEUPOGEN Specialty PEG-INTRON REDIPEN Specialty
KOGENATE FS BIO-SET Specialty NEXAVAR Specialty PEG-INTRON REDIPEN PAK 4 Specialty
KRYSTEXXA Specialty NIACINAMIDE ASCORBATE Specialty PENTAM 300 Specialty
KUVAN Specialty NICOTINYL ALCOHOL TARTRATE Specialty PENTAMIDINE ISETHIONATE Specialty
KYPROLIS Specialty NIFUROXIME Specialty PENTOSTATIN Specialty
KYTRIL Specialty NILANDRON Specialty PERJETA SpecialtyL-ASPARAGINE MONOHYDRATE Specialty NIPENT Specialty PLATINOL AQ Specialty
LETAIRIS Specialty NORDITROPIN CARTRIDGE Specialty POLYGAM S/D Specialty
LEUCOVORIN CALCIUM Specialty NORDITROPIN FLEXPRO Specialty POLYOX WSR-301 Specialty
LEUKINE Specialty NORDITROPIN NORDIFLEX PEN Specialty POMALYST Specialty
LEUPROLIDE ACETATE Specialty NOVANTRONE Specialty PREGNYL W/DILUENT BENZYL ALCOHOL/NACL Specialty
LEUSTATIN Specialty NOVAREL Specialty PRIVIGEN SpecialtyLEVULINIC ACID CALCIUM SALT Specialty NOVOBIOCIN SODIUM Specialty PROCHIEVE Specialty
LIPODOX Specialty NOVOSEVEN Specialty PROCRIT Specialty
LIPODOX 50 Specialty NOVOSEVEN RT Specialty PROFASI Specialty
LITHIUM CITRATE Specialty NPLATE Specialty PROFASI HP W/DILUENT BENZYL ALCOHOL Specialty
LOVENOX Specialty NULOJIX Specialty PROFILNINE SD Specialty
LUCENTIS Specialty NUTROPIN Specialty PROGESTERONE Specialty
LUMIZYME Specialty NUTROPIN AQ Specialty PROGESTERONE MICRONIZED Specialty
LUPRON 2 WEEK SUPPLY Specialty NUTROPIN AQ NUSPIN 10 Specialty PROGESTERONE MICRONIZED (SOY) Specialty
LUPRON DEPOT Specialty NUTROPIN AQ NUSPIN 20 Specialty PROGESTERONE MICRONIZED (YAM) Specialty
LUPRON DEPOT-PED Specialty NUTROPIN AQ NUSPIN 5 Specialty PROGESTERONE MICRONIZED PREMIUM Specialty
LUVERIS Specialty NUTROPIN AQ PEN Specialty PROGESTERONE MILLED Specialty
LYSINE ACETATE Specialty OCTAGAM Specialty PROGESTERONE ULTRA MICRONIZED Specialty
LYSODREN Specialty OCTREOTIDE ACETATE Specialty PROGESTERONE WETTABLE Specialty
MACUGEN Specialty OFORTA Specialty PROGESTERONE WETTABLE (YAM) Specialty
MAGNESIUM LACTATE Specialty OLYSIO Specialty PROLASTIN Specialty
MAKENA Specialty OMNITROPE Specialty PROLASTIN-C Specialty
MEDRYSONE Specialty ONCASPAR Specialty PROLEUKIN Specialty
MEKINIST Specialty ONDANSETRON HCL Specialty PROLIA SpecialtyMELPHALAN HYDROCHLORIDE Specialty ONDANSETRON HCL
DIHYDRATE Specialty PROMACTA Specialty
MENOPUR Specialty ONDANSETRON HCL/DEXTROSE Specialty PROPLEX T FACTOR IX COMP FACTOR
VII ACTIVITY UNITS 700-3900 Specialty
MESNA Specialty ONTAK Specialty PROVENGE Specialty
MESNEX Specialty ONXOL Specialty PULMOZYME Specialty
MITOXANTRONE HCL Specialty OPSUMIT Specialty PYRVINIUM PAMOATE Specialty
MONARC-M Specialty ORENCIA Specialty RAVICTI Specialty
MONOCLATE-P Specialty ORTHOVISC Specialty REBETOL Specialty
MONONINE Specialty OVIDREL Specialty REBIF Specialty
MOZOBIL Specialty OXALIPLATIN Specialty REBIF REBIDOSE Specialty
MUSTARGEN Specialty PACLITAXEL Specialty REBIF REBIDOSE TITRATION PACK Specialty
MYLERAN Specialty PAMIDRONATE DISODIUM Specialty REBIF TITRATION PACK Specialty
MYOBLOC Specialty PANGLOBULIN Specialty RECLAST Specialty
MYOZYME Specialty PANGLOBULIN NF Specialty RECOMBINATE Specialty
NAGLAZYME Specialty PARAPLATIN Specialty REFACTO Specialty
NAVELBINE Specialty PARGYLINE HCL Specialty REMICADE Specialty
NEBUPENT Specialty PEGASYS Specialty REMODULIN Specialty
Specialty Medications (Continued)

Medication Name Medication Class Medication Name Medication Class Medication Name Medication ClassREPRONEX Specialty SYNVISC Specialty VENTAVIS Specialty
RESORCINOL MONOACETATE Specialty SYNVISC ONE Specialty VEPESID Specialty
REVATIO Specialty TABLOID Specialty VESANOID Specialty
REVLIMID Specialty TAFINLAR Specialty VICTRELIS Specialty
RHOGAM HUMAN Specialty TARCEVA Specialty VIDAZA SpecialtyRHOGAM ULTRA-FILTERED PLUS Specialty TARGRETIN Specialty VINBLASTINE SULFATE Specialty
RHOPHYLAC Specialty TASIGNA Specialty VINCASAR PFS Specialty
RIASTAP Specialty TAXOL Specialty VINCRISTINE SULFATE Specialty
RIBAPAK Specialty TAXOTERE Specialty VINORELBINE TARTRATE Specialty
RIBASPHERE Specialty TECFIDERA Specialty VISTIDE Specialty
RIBATAB Specialty TECFIDERA STARTER PACK Specialty VISUDYNE Specialty
RIBAVIRIN Specialty TEMODAR Specialty VIVAGLOBIN Specialty
RITUXAN Specialty TEMOZOLOMIDE Specialty VIVITROL Specialty
RIXUBIS Specialty TEV-TROPIN Specialty VOTRIENT Specialty
ROFERON-A Specialty THALOMID Specialty VPRIV Specialty
SABRIL Specialty THROMBATE III W/10 ML STERILE WATER Specialty WILATE Specialty
SAIZEN Specialty THROMBATE III W/20 ML STERILE WATER Specialty WINRHO SDF Specialty
SAIZEN CLICK.EASY Specialty THYROGEN Specialty XALKORI Specialty
SANDOSTATIN Specialty TIVICAY Specialty XELJANZ Specialty
SANDOSTATIN LAR DEPOT Specialty TOBI Specialty XELODA Specialty
SENNA LEAF Specialty TOBRAMYCIN Specialty XENAZINE Specialty
SENSIPAR Specialty TOPOSAR Specialty XEOMIN Specialty
SEROSTIM Specialty TOPOTECAN HCL Specialty XGEVA Specialty
SILDENAFIL CITRATE Specialty TORISEL Specialty XIAFLEX Specialty
SIMPONI Specialty TRACLEER Specialty XOFIGO Specialty
SIMPONI ARIA Specialty TREANDA Specialty XOLAIR Specialty
SODIUM GLYCEROPHOSPHATE Specialty TRELSTAR DEPOT Specialty XTANDI SpecialtySODIUM PYROPHOSPHATE ANHYDROUS Specialty TRELSTAR DEPOT MIXJECT Specialty XYNTHA Specialty
SOLIRIS Specialty TRELSTAR LA Specialty XYNTHA SOLOFUSE Specialty
SOMATULINE DEPOT Specialty TRELSTAR LA MIXJECT Specialty XYREM Specialty
SOMAVERT Specialty TRELSTAR MIXJECT Specialty YERVOY Specialty
SPRYCEL Specialty TRETINOIN Specialty ZALTRAP Specialty
STELARA Specialty TYKERB Specialty ZANOSAR Specialty
STIMATE Specialty TYSABRI Specialty ZAVESCA Specialty
STIVARGA Specialty TYVASO Specialty ZELBORAF Specialty
STRIBILD Specialty TYVASO REFILL Specialty ZEMAIRA Specialty
SUCRAID Specialty TYVASO STARTER Specialty ZEVALIN IN-111 Specialty
SULFACHLORPYRIDAZINE Specialty TYZEKA Specialty ZEVALIN Y-90 SpecialtySULFACHLORPYRIDAZINE SODIUM Specialty VALCHLOR Specialty ZOFRAN Specialty
SUPARTZ Specialty VALCYTE Specialty ZOLADEX Specialty
SUPPRELIN LA Specialty VANDETANIB Specialty ZOLEDRONIC ACID Specialty
SUTENT Specialty VANTAS Specialty ZOLINZA Specialty
SYLATRON Specialty VECTIBIX Specialty ZOMETA Specialty
SYNAGIS Specialty VELCADE Specialty ZORBTIVE Specialty
SYNAREL Specialty VELETRI Specialty ZORTRESS Specialty
SYNRIBO Specialty VENOGLOBULIN-S Specialty ZYTIGA Specialty
Specialty Medications (Continued)
Related Documents











