Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18 Chapter 48: Drugs Affecting Corticosteroid Levels: I. Definitions Related to Corticosteroids: a. Corticosteroids are used in replacement therapy to maintain adequate levels of hormones in patients with inadequate adrenal function and diminished natural corticosteroid production i. Also used as: anti-inflammatory : reducing swelling and irritation; antiallergenic : minimizing and or preventing body’s response to allergens; and immunosuppressive: decreasing the body’s harmful response to diseases that affect the immune system ii. Have to taper off of medication; cannot abruptly stop **Where are the Adrenal Glands located: top of the kidneys** II. Physiology: a. Adrenal Glands: i. Two adrenal glands: one above each kidney: each consisting of medulla and cortex ii. Medulla and cortex crucial to metabolism, stress response, fluid and electrolyte balance iii. Adrenal medulla synthesis and secretes catecholoamines (epinephrine and norepinephrine) iv. Adrenal cortex: synthesis and secretion of the glucocorticoid and mineralocorticoid supply b. Adrenal Corticosteroids: i. Effect on almost every organ in the body ii. Primary actions: metabolism, carbohydrates, protein, fats, electrolytes, and water iii. Also role in cardiovascular function and immune effects iv. Zona Reticularis region of adrenal cortex important in production and secretion of other steroid hormones 1. Adrenal androgens 2. Progesterone 3. Estrogens c. Glucocorticoids: (acquired name from their role in glucose metabolism) Adrenal Glands Adrenal Medulla catecholoamin es: epinephrine and norepinephrin e Adrenal Cortex glucocortico ids mineralcorti coids 1

Pharmacology Notes Test 3 New
Dec 23, 2015
Pharmacology Notes Test 3; Pharmacology pharmacokinetics, pharmacodynamics, pharmacotherapeutics
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
Chapter 48: Drugs Affecting Corticosteroid Levels:
I. Definitions Related to Corticosteroids: a. Corticosteroids are used in replacement therapy to maintain adequate levels of hormones in patients
with inadequate adrenal function and diminished natural corticosteroid production i. Also used as: anti-inflammatory: reducing swelling and irritation; antiallergenic: minimizing and
or preventing body’s response to allergens; and immunosuppressive: decreasing the body’s harmful response to diseases that affect the immune system
ii. Have to taper off of medication; cannot abruptly stop **Where are the Adrenal Glands located: top of the kidneys**
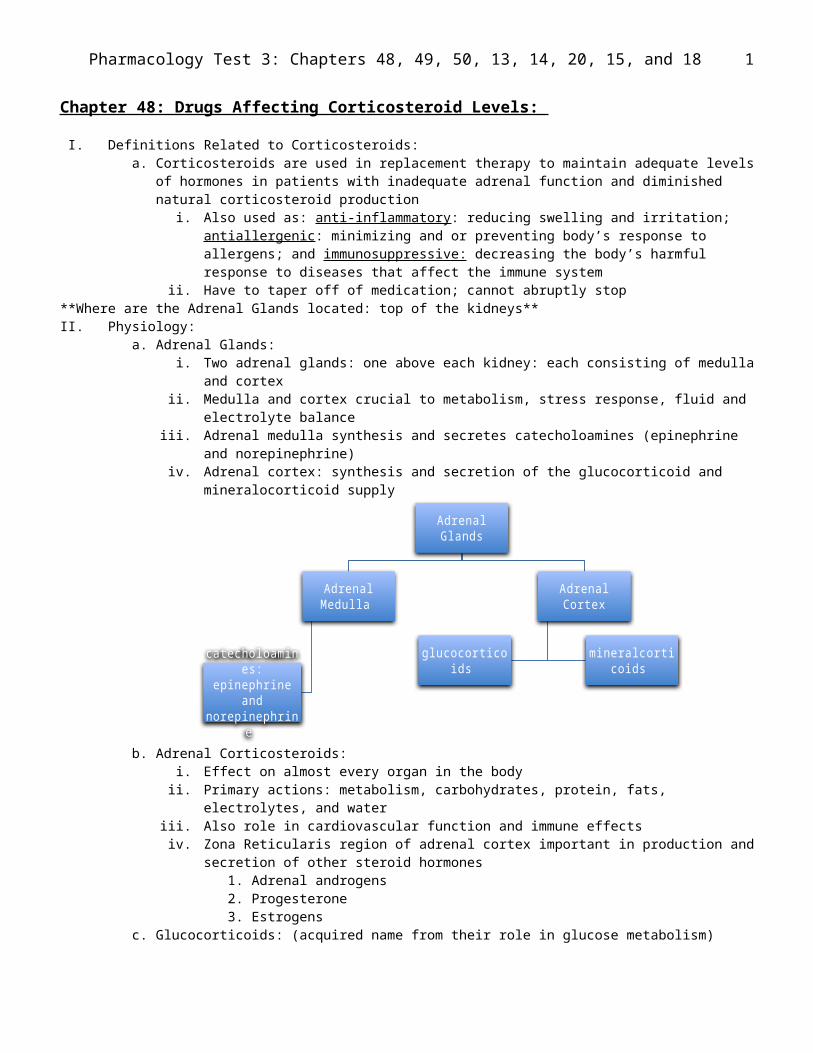
II. Physiology: a. Adrenal Glands:
i. Two adrenal glands: one above each kidney: each consisting of medulla and cortex ii. Medulla and cortex crucial to metabolism, stress response, fluid and electrolyte balance
iii. Adrenal medulla synthesis and secretes catecholoamines (epinephrine and norepinephrine) iv. Adrenal cortex: synthesis and secretion of the glucocorticoid and mineralocorticoid supply
b. Adrenal Corticosteroids: i. Effect on almost every organ in the body
ii. Primary actions: metabolism, carbohydrates, protein, fats, electrolytes, and water iii. Also role in cardiovascular function and immune effects iv. Zona Reticularis region of adrenal cortex important in production and secretion of other steroid
hormones 1. Adrenal androgens 2. Progesterone 3. Estrogens
c. Glucocorticoids: (acquired name from their role in glucose metabolism) i. Role in glucose metabolism:
1. Increase blood glucose concentrations and glucose secretion by the liver 2. Increase hepatic sensitivity to the gluconeogenic actions of glucagon and
catecholamines 3. Decrease glucose uptake and utilization by peripheral tissue 4. Increasing proteolysis 5. Decreasing protein synthesis in muscles
ii. Metabolic Effects 1. Gluconeogenesis 2. Mobilization of amino acids from protein in striated muscle 3. Protein catabolism 4. Fat synthesis and lipolysis 5. Hepatic enzymatic activities that convert amino acids to glucose
Adrenal Glands
Adrenal Medulla
catecholoamines: epinephrine and norepinephrine
Adrenal Cortex
glucocorticoids mineralcorticoids
1
Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
iii. Exert potent and diverse actions on glucose, protein, and bone metabolism and possess anti-inflammatory, antiallergenic, and immunosuppressant actions
iv. Metabolic effects of the glucocorticoids result in the following: 1. An increase in circulating amino acid levels 2. An overall depletion of muscle protein 3. A negative nitrogen balance 4. A mobilization of fatty acids, converting cell metabolism from using glucose for energy
to using fatty acids for energy 5. An antagonistic effect on antidiuretic hormones to maintain water balance 6. A lowering of the threshold for electrical excitation in the brain 7. A reduction in the amount of new bone synthesis
v. Hypothalamic cortocotrophin-releasing factor (CRF) stimulates the release of pituitary adrenocorticotropic hormone (ACTH)
vi. This hypothalamic-pituitary-adrenal (HPA) axis regulates and stimulates cortisol synthesis release by the adrenal cortex
vii. Three factors important in regulating ACTH secretion: 1. Circulating Cortisol Levels 2. Stress Levels 3. Circadian (diurnal) Rhythm
viii. Symptoms related to glucocorticoid deficiency: 1. Hypoglycemia2. Anorexia3. Nausea and vomiting 4. Flatulence 5. Diarrhea6. Hyper-pigmentation of the skin 7. Anxiety 8. Depression and loss of mental activity
d. Mineralocorticoids: i. Most prevalent naturally occurring aldosterone
1. Production occurring the outer layer of the cells of adrenal cortex 2. Regulation of potassium, sodium, and water balance 3. Aldosterone: role in promoting the reabsorption of sodium into the blood in exchange
for potassium secreted into the renal tubules for urinary excretion 4. Angiotensin II: impact on synthesis and secretion of aldosterone 5. Mechanisms controlling aldosterone levels:
a. Renal renin release—a reduction in renal blood flow increases aldosterone levels by the renin-angiotensin-aldosterone system
b. Pituitary adrenocorticotropic hormone (ACTH)c. When sodium level low/ K level high/ aldosterone will increase
6. Symptoms related to mineralocorticoid deficiency: a. Fluid and electrolyte imbalance b. Orthostatic hypotension c. Hyponatremiad. Hyperkalemia e. General malaise f. Muscle weaknessg. Muscle pain h. Cardiac arrhythmias
e. Sex steroids: i. Amount of sex steroids and some weak anabolic androgens produced in adrenal cortex
insignificant compared to hormone secretions by gonads ii. A substantial endocrine imbalance possible with certain conditions
III. Pathophysiology: a. Adrenal Insufficiency:
2

Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
i. Primary (Addison Disease): due to destruction of adrenal cortex by infection or hemorrhage 1. Resulting in hyposecretion of all adrenocortical hormones2. Characteristics of Addison Disease 3. Major Complications: sudden life threatening exacerbation called addisonian crisis—
(extremes of hypotension, hyponatremia, dehydration, hyperkalemia, and hyperthermia)
4. Characteristics related to glucocorticoid deficiency: hypoglycemia, anorexia, nausea, vomiting, flatulence, diarrhea, hyperpigmentation, anxiety, depression, loss of mental acuity
5. Characteristics related to mineralocorticoid deficiency: fluid/electrolyte imbalance, orthostatic hypotension, hyponatremia, hyperkalemia, general malaise, muscle weakness, muscle pain, cardiac arrhythmias
ii. Secondary adrenal insufficiency: due to insufficient secretion of ACTH by anterior pituitary; little or no alteration in aldosterone secretion—therefore there is glucocorticoid insufficiency with no effect on mineralocorticoid
1. Most common cause: long term tx of nonendocrine disorders with pharmacologic doses of glucocorticoid drugs
b. Cushing Syndrome: rare disorder resulting from increased adrenocortical secretion of cortisol, resulting in chronic elevation in glucocorticoid and adrenal androgen hormones
i. Mineralcorticoid levels usually not affected ii. Causes: ACTH-dependent adrenocortical hyperplasia; tumor; ACTH secreting tumor; long-term
administration of large doses of glucocorticoids iii. Characteristics: moon face, glaucoma, hirsutism and masculinization, cervicodorsal fat (buffalo
hump), extremity thinning/atrophy, abdominal straie, protuberant abdomen, truncal obesity, swelling, brittle bones
c. Salt-Losing Adrenogenital Syndrome; i. Congenital condition: inherited enzymatic interference with normal biosynthesis of
glucocorticoids and mineralcorticoids ii. Low levels of corticosteroids stimulate production of large amounts of corticotropin (ACTH)
iii. Adrenal glands respond to increased ACTH by increasing production of adrenal androgens leading to abnormally high testosterone levels resulting in masculinization
d. Hyperaldosteronism: i. Production of excessive aldosterone by some tumors of adrenal cortex impacting hormone action
in the distal renal tubule 1. Hypertension secondary to sodium and water retention 2. Hypokalaemia: induced muscle weakness
ii. Surgical removal of tumor necessary IV. Steroid Hormone Agonists:
a. Glucocorticoids: i. The primary endogenous glucocorticoids produced by the adrenal gland are cortisol
(hydrocortisone) and cortisone ii. They have no role in any systemic anti-inflammatory therapeutic regimen because of their high
mineralcorticoid activity relative to their anti-inflammatory activity iii. All natural and synthetic glucocorticoids act by binding to a specific cytoplasmic glucocorticoid
receptor iv. Used mainly as anti-inflammatory agents, immunosuppressive agents, replacement therapy for
individuals with adrenal insufficiency, and adjunctive treatment in selected malignant disorders v. A common adverse effect of synthetic glucocorticoids administered in high doses for anti-
inflammatory and immunosuppressant effects (combined or separately) is suppression of the HPA Axis and may lead to secondary adrenal insufficiency
vi. Abrupt discontinuation of a glucocorticoid following prolonged administration may result in acute adrenal insufficiency; to prevent this the drug must be tapered
vii. Prototype Drug: prednisone (Deltasone, Prednicot) four times more potent than naturally occurring cortisol resulting in longer acting and a more potent anti-inflammatory response
3
Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
1. Most often used for treatment of inflammatory conditions and autoimmune diseases viii. Drugs Closely Related to Prednisone:
1. Hydrocortisone: Solu-Cortef (rectal preparations are absorbed as much as 50%) a. Structurally identical to cortisolb. Treatment of choice: adrenal insufficiency replacement therapy c. Rectal preparations used for ulcerative colitis
2. Methylprednisone: Medrol (potent anti-inflammatory and immunosuppressive effects) 3. Dexamethasone: Decadron
a. No mineralocorticoid activity with maximum anti-inflammatory activity b. Used in short term situations requiring the max anti-inflammatory (cerebral
edema and septic shock), or replacement therapy, or antiemetic c. Used to diagnose Cushing Diease
4. Betamethasone: Celestone a. Produces anti-inflammatory and immunosuppressive effects b. Uses similar to those of dexamethasone and methylprednisolone c. Also used to prevent respiratory distress syndrome in premature infants
5. Inhaled glucocorticoids: a. Metabolized in lung—therefore reducing systematic effects b. Can develop dysphonia & oropharyngeal Candida albicans infection)
6. Topical glucocorticoids: a. Non-specific anti-inflammatory activity leading to decrease in edema, erythema,
and pruritus 7. Intra-articular injection (injected glucocorticoids)
a. Produce local effects for symptomatic relief of joint pain and increased joint mobility
b. Allow treated area sufficient time to heal 24-48 hours b. Mineralocorticoids
i. Aldosterone, the naturally occurring mineralocorticoid, is expensive and requires parenteral administration
ii. Therefore, fludrocortisone is prototype iii. This adrenal corticosteroid has both high mineralocorticoid and glucocorticoid activity
1. Its glucocorticoid potency is 15 times greater than that of hydrocortisone iv. However, when used as replacement therapy in adrenocortical deficiency, its therapeutic effect
is mineralocorticoid activity v. Prototype Drug: fludrocortisone (Florinef Acetate)
V. Steroid Hormone Antagonists: a. Steroid hormone antagonists act to inhibit or suppress the adrenal cortex, thus controlling the symptoms
of Cushing syndrome (adrenocortical hormone excess) i. Prototype Drug: aminoglutethimide (Cytadren)
4
Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
Chapter 49: Drugs Affecting Blood Glucose Levels I. Diabetes Mellitus:
a. Although an estimated 23.6 million people are diagnosed with diabetes, 5.7 million are unaware they have the disease
b. Approximately 5% to 10% of Americans diagnosed with diabetes have type 1, whereas 90%-95% have type 2
c. People with diabetes are at increased risk for cardiovascular disease, kidney failure, blindness, nervous system disease, extremity amputations, dental disease, and complications of pregnancy
d. In 2007, the total annual economic cost of diabetes was estimated to be $174 billion e. Exogenous insulin’s are used to replicate deficient intrinsic insulins prototype drug is regular insulinf. Other types of insulin: oral antidiabetic drugs—two groups: sulfonylureas and nonsulfonylureas
i. Prototype of sulfonylureas (antiglycemics) is glyburide ii. Prototype of nonsulfonylureas (antihyperglycemics) is metformin
II. Physiology: a. Glucose is made available to the body from food that is ingested and from the production of glucose by
the liver b. Unable to store or synthesize glucose, the brain depends on a steady supply of glucose from the
circulation and extracts its energy on a nearly continuous basis c. Three body systems are involved in the regulation and use of glucose—the liver, pancreas, and skeletal
muscle tissue d. The liver synthesizes its own glucose supply (a process called gluconeogenesis) in addition to storing the
releasing glucose e. The pancreas is both an exocrine and an endocrine gland
i. Endocrine function is to synthesize and secrete peptide hormones (insulin, glucagon, and somatostatin) by the islets of Langerhans
f. These three hormones regulate and maintain homeostasis of blood glucose—islets of Langerhans contain the following types of cells:
i. Beta Cells: secrete hypoglycemic hormone insulin ii. Alpha Cells: secrete hyperglycemic hormone glucagon
iii. Delta Cells: release somatostatin, hormone that inhibits both glucagon and insulin secretion iv. F Cells: synthesize and secrete pancreatic polypeptides used in digestion
g. Insulin regulates carbohydrate metabolism and blood glucose levels i. Functions of Insulin: regulates carbohydrate metabolism but also plays important role in
metabolizing fats and proteins 1. Lowers blood glucose levels by stimulating peripheral glucose uptake 2. Specific Receptor sites allow the glucose to enter the cells 3. Insulin resistance: inappropriately elevated hepatic glucose output and impaired
glucose uptake by the muscle tissue 4. In the liver, insulin: promotes the uptake and storage of glucose in the form of glycogen,
promotes the conversion of excess glucose into fat, and suppresses hepatic gluconeogenesis and glycogenolysis
5. All tissues in body need insulin for glucose to enter cells: except brain, nerves, intestine, liver, retina, erythrocytes, and renal tubules
ii. Insulin synthesis and release: 1. Plasma glucose level single most important factor in controlling rate of insulin synthesis
and release 2. Other factors that influence release: blood levels of sugars, levels of free fatty acids,
growth hormone, thyroid-stimulating hormone, glucagon, sympathetic and parasympathetic stimulation, adrenocorticotropic hormone, and cortisol
iii. Any of the following can affect blood glucose levels: 1. Stress or illness 2. Secretion of insulin-antagonistic hormones that affect glucose metabolism 3. Rates of hepatic synthesis of glucose or conversion of glycogen to yield glucose 4. Presence and levels of insulin antibodies 5. Use of glucose by peripheral cells or tissues
5
Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
6. Number of cellular insulin receptors iv. In response to postprandial levels: insulin is released into bloodstream by the beta cells v. When serum glucose decreases, the alpha cells release glucagon into the bloodstream,
stimulating release of glycogen from hepatic storage sitesvi. Hepatic glycogen stores are depleted 6 hours after a meal
vii. Muscles begin to release amino acids that are converted to glucose; free fatty acids broken down from adipose tissue converted in to glucose by the muscle and liver cells
h. Glucagon: i. Declining blood glucose levels stimulate the release from pancreatic islet alpha cells
ii. Sympathetic nerve impulses, exercise, infection, and trauma also stimulate release iii. In the liver, it stimulates glycogenolysis and gluconeogenesis resulting in a release of glucose into
the blood III. Pathophysiology:
a. Diabetes mellitus is a serious chronic disease that affects people of all ages and ethnic groups b. Type 1 diabetes is an autoimmune disorder characterized by the destruction of the insulin-secreting
beta cells, in the pancreas, leading to absolute insulin deficiency i. Hyperglycemia—circulating blood glucose is not acceptable to cells, so body mistakenly
interprets this to mean that there is not enough glucose and thus initiates two other processes to gain energy Breaking down lipids and proteins
c. Type 2 diabetes is the result of insulin resistance by tissues and usually a decrease in insulin production i. Abnormalities of carbohydrate, fat, and protein metabolism
ii. No appreciable loss of pancreatic beta cells or cellular activity from the islets occurs in type 2 diabetes
iii. Pancreas tries to overcome resistance by producing insulin; because peripheral tissue is resistant to insulin, it does not enter the cells but stays in the bloodstream
iv. Metabolic syndrome is a precursor to type 2 diabetes d. Gestational diabetes mellitus (GDM) occurs when a woman’s pancreatic function is not sufficient to
overcome the insulin resistance created by the anti-insulin hormones secreted by the placenta e. Criteria for Diabetes Mellitus Diagnosis:
i. Plasma glucose=126mg/dL after fasting for 8 hours or ii. Plasma glucose=200mg/dL during and oral glucose tolerance test (OGTT) or
iii. An A1C level of 6.5% or higher or iv. Symptoms of diabetes and hyperglycemia or hyperglycemic crisis (plasma glucose greater than
200mg/dL anytime throughout the day) IV. Insulins:
a. Synthetic insulin (exogenous) acts in the same manner as endogenously produced insulin i. Sources of exogenous insulin, historically included pork and beef pancreas, but not only
recombinant DNA technology or genetic engineering is used to create human-like insulin ii. Modifying the amino acid sequence of the human insulin molecule has resulted in new, rapid-
acting insulin analogues, such as aspart, lispro, or gluisine (produce by rDNA technology) iii. Human –sourced insulin is considered the standard therapy iv. The potency of insulin is expressed in the United States Pharmacopeia (USP) or international
unitsb. Drugs Closely Related to Regular Insulin: Rapid Acting Insulins
i. Rapid acting insulin: that are analogues of rapid-acting regular insulin are now available: aspart (NovaLog), lispro (Humalog), and glulisine (Apidra)
1. Administer within 15 minutes of start of the meal 2. Can be used in insulin pumps
c. Drugs Different from Regular Insulin: Long-Acting Insulini. NPH: (intermediate) protamine is added to insulin to create NPH
1. Humulin N 2. Onset: 1-1.5 hours 3. Peak: 4-12 hours 4. Duration: up to 24 hours 5. Considered intermediate acting
6
Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
6. Cloudy (suspension must be rolled gently) 7. Given SC (NEVER IV) 8. Observe for hypoglycemia in mid to late afternoon
ii. Detemir: long acting insulin 1. Administered once or twice daily only SC not IV or pump2. Cannot be mixed with any other insulins 3. Less weight gain and lower risk for nocturnal hypoglycemia than NPH
iii. Glargine:1. Administered once daily at bedtime 2. Duration: 24 hours (no peak)
iv. Exubera: 1. Onset: 10-20 minutes 2. Inhaled insulin
V. Noninsulin Antidiabetic Medications a. Until the mid-1990’s, the sulfonylurea drugs were the only class of oral antidiabetic agents available to
manage type 2 diabetes b. Currently five chemical classes of oral antidiabetic agents are available c. Sulfonylureas
i. First and second generation drugs (same class but developed at different times and have some different characteristic)
ii. Glyburide is the prototype and is a second generation drug iii. Prototype Drug: glyburide (DiaBeta)
d. Nonsulfonylureas: i. The nonsulfonylurea antidiabetics compromise three different classes grouped by their chemical
structure: 1. Biguanides 2. Thiazolidinediones 3. Alpha-glucosidase inhibitors
ii. These drugs are considered by their mode of action: 1. Improving insulin action 2. Delaying the digestion of carbohydrates
iii. Prototype Drug: metformin (Fortamet, Glucophage) VI. Glucose-Elevating Agents
a. Glucagon is a hyperglycemic polypeptide hormone produced by the alpha cells of the pancreatic islets of Langerhans
b. Its physiologic effect is generally the opposite of that of insulin c. Glucagon is the body’s first line of defense against hypoglycemia d. The main stimulus to glucagon secretion to decrease in intracellular glucose concentrations that usually
occurs as a result of a drop in serum blood sugar i. Prototype Drug: Glucogon (GlucaGen)
1. Used in unconscious patients to reverse insulin overdose a. Drugs Different:
i. Diazoxide:1. Hyperglycemic effects 2. Inhibits insulin release from the pancreas
7
Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
Chapter 50: Drugs Affecting Pituitary, Thyroid, Parathyroid, and Hypothalamic Function: I. Physiology
a. Pituitary Gland Function i. Anterior lobe of the pituitary gland: it controls the function of glucocorticoid hormone levels
(ACTH), body growth and metabolism (GH), function of the thyroid gland (TSH), gonadal function (FSH and LH), milk production and breast growth (prolactin)
ii. Posterior lobe of the pituitary gland: it stores and secretes two effector hormones (hormones that produce an effect when stimulated): oxytocin and vasopressin (also known as antidiuretic hormone [ADH])
b. Thyroid gland function: i. It controls cellular metabolism and promotes normal growth and development
ii. 100-200mcg of iodide is adequate for thyroid gland to make normal hormones iii. controls celllar metabolism and promotes normal growth and development: regulate
heat/energy productin, blood volume, cardiac output, oxygen consumption, and metabolism of fats, carbs, and proteins
iv. produces calcitonin c. Parathyroid gland function
i. PTH affects three target organs: bone, kidneys, and GI tract ii. The major controlling factor for PTH secretion is serum calcium
II. Pathophysiology a. Anterior pituitary gland dysfunction: it includes growth hormone deficiency and excess
i. Deficiency: 1. In children—idiopathic (most common—inadequate GHRH) or congenital (decreased
growth rate within first years of life) 2. Adults—GH deficiency as children or develop it in adulthood secondary to a pituitary
tumor or its treatment ii. Excess:
1. Gigantism: uncommon condition in children—caused by excessive secretion of GH by somatrope adenomas (7ft or taller)
2. Acromegaly—in adults: after puberty and the closure of the epiphyseal plate closes—very uncommon
a. Enlarged heart, hypertension, accelerated atherosclerosis, peripheral neuropathies, and muscle weakness
b. Posterior pituitary gland dysfunction: major disorders are diabetes insipidus (DI) and syndrome of inappropriate antidiuretic hormone (SIADH)
i. DI—caused by either a deficiency in or decreased response to ADH ii. SIADH—excessive ADH secretion secondary to failure of the negative feedback system
responsible for its release and inhibition c. Thyroid Gland Dysfunction: hyperfunctioning or hypofunctioning gland, malfunctions that may be
caused by either a congenital defect of by a problem that occurs later in life i. Dramatic changes in patterns of growth and development, functions of the cardiovascular,
respiratory, GI, neuromusclular, skeletal, and reproductive systems can result ii. Increase in the size of the thyroid—goiter
iii. Congenital Hypothyroidism: occurs from abnormal synthesis of of hormone, deficient TSH, or absence of thyroid gland (Hashimotos)
iv. Drop of blood taken from heel to measure newborns thyroid hormone levelsv. Hyperthyroidism (thyrotoxicosis)—Graves Disease is the most common cause
d. Parathyroid Gland Dysfunction: PTH is a major regulator of serum calcium and phosphate i. A decrease in serum calcium concentration is the dominant regulator of PTH, with a response of
just a few seconds ii. A decrease in phosphate causes an indirect effect on PTH by combining with calcium and
decreasing serum calcium concentrations III. Growth Hormones:
8

Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
a. GH deficiency, leading to short stature, was initially treated with GH injections extracted from the pituitary glands of cadavers
b. Presently, synthetic human GH (rhGH), produced from recombinant DNA, is available c. rhGH is very expensive d. Prototype Drug: somatropin e. **Patients taking somatropin should have which lab values monitored on a routine basis due to adverse
effects of drug therapy—TSH and Glucose Level f. Drugs Different from Somatrophin:
i. GH antagonists decrease GH secretion ii. Almost all are conditions caused by pituitary tumor and require surgery or radiation
iii. Octreotide Acetate (sandostatin) 1. Potent inhibitor of GH secretion 2. Long acting antagonistic analogues3. Treatment for acromegaly
IV. Posterior Pituitary Hormone Regulators: a. The posterior pituitary stores two hormones that are produced in the hypothalamus
i. Vasopressin ii. Oxytocin
b. Desmopressin and vasopressin are synthetic analogues of the naturally occurring posterior pituitary hormone
c. Prototype Drug: desmopressin d. **Desmopressin is used to treat—central DI, primary nocturnal enuresis, hemophilia A**
V. Thyroid Drugsa. Thyroid hormones influence essentially every organ system in the body b. Thyroid disorders involve an alteration in the quantity of thyroid hormone secretion, enlargement of the
thyroid gland (goiter), or both and are classified as either hyperthyroidism or hypothyroidism c. Hypothyroidism may be mistaken for the normal aging process d. The only treatment for hypothyroidism is lifelong replacement of thyroid hormones that are adequate to
meet the individuals metabolic needs e. Prototype Drug: levothyroxine ( T 4; Levothroid, Synthroid)
VI. Antithyroid Compounds: a. Hyperthyroidism is treated with thyroid-hormone antagonist drugs, surgery, or radioactive iodine b. The purpose of treatment is to reduce the amount of functional thyroid tissue c. Prototype Drug: methimazole (MMI )
VII. Parathyroid Drugs a. Antihypercalcemia, Calcium-Regulator Drugs
i. Antihypercalcemic drugs do not directly affect the parathyroid gland or PTH but rather inhibit bone reabsorption of calcium
ii. These agents are frequently used in the treatment of Paget disease—bone inflammation that results in thickening, softening, and bowing of the affect bones
iii. Individuals with symptomatic disease experience bone pain and deformity, fractures, spinal cord compression, or cranial and spinal cord entrapment
iv. Prototype Drug: calcitonin, salmon b. Antihypocalcemic Drugs:
i. Vitamin D compounds regulate absorption of calcium and phosphate ii. Vitamin D is considered a hormone although it is not a natural human hormone
iii. Vitamin D metabolites: 1. Control intestinal absorption of dietary calcium 2. Tubular reabsorption of calcium by the kidney 3. Mobilization of calcium from the skeleton, in conjunction with PTH
iv. Vitamin D is also involved in magnesium metabolism v. Vitamin D works together with PTH and calcitonin to regulate calcium homeostasis
9

Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
vi. Vitamin D stimulates calcium absorption from the intestine and restores the serum calcium to normal level
vii. Prototype Drug: calcitriol (1,25—dihydroxyvitamin D3, Rocaltrol [capsules, solution], Calcijex [parenteral])
Chapter 15: Drugs Relieving Anxiety and Promoting Sleep: **What system in the brain is responsible for emotion?—limbic system
I. Emotions and Neurotransmitters a. The limbic system in the brain is known to be primarily responsible for emotions b. The amygdala receives incoming sensory signals and then communicates with the frontal lobes of the
brain c. The amygdala can signal the brain that a threat is present and set off a fear response or anxiety d. Another part of the brain, the hippocampus is responsible for processing threatening or traumatic stimuli e. The brain sends its messages to the body by way of the nervous system f. Neuroplasticity: structures of the brain undergo frequent refinement in response to the internal and
external environment g. GABA: gamma aminobutyric acid is a neurotransmitter that either inhibits or excites receptors
II. Sleep: a. Sleep is a time of bodily rest, although the brain remains active b. There are two phases:
i. Rapid Eye movements (REM) ii. Non-rapid eye movement (NREM)
1. Stage 1—light sleep; muscles relax; brain waves are irregular and rapid 2. Stage 2—brain waves are larger than in stage 1, with bursts of electrical activity 3. Stages 3 and 4—deep sleep, with even larger, slower brain waves called delta waves
c. A number of physiologic changes occur during sleep d. The amount of sleep needed by a person varies throughout the life span, with infants requiring the most
sleep and adults requiring the leastIII. Anxiety:
a. A feeling of unease that something bad or undesirable may happen b. Some anxiety is normal; it is a protective mechanism c. Anxiety becomes pathologic when it is severe and chronic and interferes with a person’s ability to
function in normal life d. Anxiety disorders can become progressively worse if they are untreated e. Anxiety commonly occurs in combination with other mental or physical illness ting f. Types of anxiety disorders:
i. Panic disorder: sudden feelings of terror that come on suddenly or repeatedly without warning ii. Phobic Disorders: persistent, unrealistic fears of situations or objects that do not realistically
pose a significant threat or danger 1. Social Phobia (Social anxiety disorder) 2. Specific Phobia: intense, irrational fear of a particular thing or situation that poses little
or no actual danger 3. Obsessive Compulsive Disorder (OCD)—recurrent, unwelcome thoughts with rituals
attempting to control the anxiety resulting from these thoughts 4. Post Traumatic Stress Disorder—PTSD5. Generalized Anxiety Disorder—(GAD) chronic anxiety lasting longer than 6 months and
can cause the person to have exaggerated worry and tension every day IV. Sleep Disorders:
a. Between 50-70 million Americans have a sleep disorder b. These disorders are many and may include the following problems:
i. Narcolepsy: sudden irresistible sleep attacks of unknown origin lasting from seconds to minutes, two to six times a day
ii. Sleep apnea: a group of disorders characterized by cessation of breathing during sleep iii. Sleepwalking: getting up and walking about while still asleep
10

Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
c. These disorders are many and may include the following problems: i. Night terrors: occur only in children, with period of fright, crying, moaning, or screaming after a
brief time asleep ii. Excessive daytime sedation
iii. Insomnia: difficulty falling asleep or staying asleep, waking up too early in the morning without being able to return to sleep, waking up frequently during the night with difficulty returning to sleep, not sleeping long enough, feeling that sleep was not restful, sleeping poorly
V. Drugs to Relieve Anxiety: a. Selective Serotonin Reuptake Inhibitors:
i. Selective serotonin reuptake inhibitors (SSRIs) are a class of antidepressant drugs, some of which are now considered first-line therapy for anxiety disorders
ii. Low serotonin levels are known to be present in severe stress and in many mood and anxiety-related disorders
iii. SSRIs indirectly increase the amount of the neurotransmitter serotonin available in the synapses iv. SSRIs are generally well tolerated with few adverse effects v. Must be taken for a few weeks for their full anti-anxiety effect to take place
vi. Prototype drug is sertraline b. Tricylcic Antidepressants:
i. TCA’s are another class of antidepressants ii. TCA’s are as effective as the SSRI’s in treating most anxiety disorders
iii. TCAs work by affecting the regulation of serotonin or norepinephrine in the brain iv. TCAs have a higher adverse effect profile than SSRI’s, which limits their use as antidepressants—
dizziness, drowsiness, dry mouth, weight gain v. Prototype drug: nortriptyline
c. Monoamine Oxidase Inhibitors i. MAOI’s are the oldest class of antidepressants
ii. Used to treat anxiety disorders are phenelzine, tranylchpromine, and isocarboxazid iii. These drugs are occasionally prescribed for panic disorder and social phobia iv. Monoamine oxidase is the enzyme that degrades serotonin in the synapse v. By inhibiting the enzyme, higher levels of serotonin can remain in the synapse and be active
vi. The MAOIs are associated with significant risk for serious drug-food interactions vii. Prototype drug is phenelzine
d. Beta-Blockers: i. Adrenergic drugs most frequently used for a wide variety of cardiac conditions
ii. Among other actions, they slow heart rate iii. This helps the patient with some types of anxiety who may be uncomfortable and highly aware of
the tachycardia and palpitations iv. Prototype drug: propranolol
e. Benzodiazepines: i. Used for a number of therapeutic effects
ii. As a class, they appear to potentiate the effects of GABA iii. The result is more CNS depression than would normally be found iv. Benzodiazepines bind to specific receptor sites to produce their effects v. As a drug class, they have high margin of safety
vi. Prototype Drug: Lorazepam **Benzodiazepines are used to treat—anxiety, seizures, and alcohol withdrawal****Benzodiazepines has a short duration of action**VI. Nonbenzodiazepines:
a. Buspirone i. Azaspirodecanedione that is not chemically or pharmacologically related to benzodiasepines
ii. It is used to treat the symptoms of anxiety although exactly how it works is unknown iii. Optimum relief of anxiety usually occurs after 3-4 weeks of treatment
11

Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
iv. Buspirone is intended for short-term therapy; patients who have been treated with buspirone for up to 1 year have not required a dosage increase to maintain therapeutic effect and withdrawal symptoms did not occur when the drug was stopped
b. Hydroxyzine: i. Hydroxyzine is a miscellaneous antianxiety drug
ii. It exerts CNS depressant activity in subcortical areas iii. It rapidly produces a feeling of calm and relieves anxiety without impairing mental alertness iv. It may be coadministered with a narcotic to control pain while minimizing the nausea that may
be an adverse effect from the narcotic c. Meprobamate:
i. Used for short-term management of anxiety symptoms ii. Has selective effects at multiple sites within the CNS, including the thalamus and the limbic
system iii. It may also inhibit multineuronal spinal reflexes iv. It has mild tranquilizing properties and some anticonvulsant and muscle-relaxant properties v. Meprobamate can produce several CNS adverse effects
vi. Pregnancy category C drug VII. Nonbenzodiapines to Promote Sleep:
a. Eszopiclone i. Lunesta: nonbenzodiazepine hypnotic
ii. The drug induces sleep quickly, prevents waking during the night iii. Believed to achieve its therapeutic effect from interaction with GABA-receptor/benzodiazepine-
receptor complexes iv. It is the only drug for insomnia that is approved for long-term use (up to 6 months) v. Rapid onset: within 1 hour and is metabolized in the liver and excreted in the urine
vi. The most common adverse effects after 6 weeks of use were headache, prolonged drowsiness, and an unpleasant taste
b. Zaleplon: i. Sonata is a sedative for short-term use (up to 28 days)
ii. Although a nonbenzodiazepine and not chemically related to the benzodiazepines, it does interact with GABA-benzadiazepines (BZ) complex
iii. The most common adverse effects are drowsiness, dizziness, light-headedness, and difficulty with coordination
iv. Pregnancy category C drug v. May lead to dependency and rebound insomnia is possible
c. Zolpidem: i. Ambien: used for short term treatment of insomnia—generally not for more than 7-10days
ii. It induces sleep rapidly and should be taken immediately before going to bed iii. Although it is not chemically related to the benzodiazepines iv. Generally preserves all of the sleep stages and has only minor effects on REM sleep v. The most common adverse effecs from zolpidem are headache, prolonged drowsiness, and
dizziness d. Ramelteon
i. Melatonin receptor agonists stimulate the same receptor sites as endogenous melatonin ii. Ramelteon is used in the treatment of insomnia when the patient has difficulty falling asleep
iii. Ramelteon has high affinity at two specific melatonin receptors iv. Common adverse effects of ramelteon include headache, daytime sleepiness, dizziness, tiredness,
nausea, worsening insomnia, and colds VIII. Drugs that Promote Sleep from Other Classes:
a. Trazodone: i. Trazodone (Desyrel) is an atypical antidepressant
ii. This drug causes significant sedation as an adverse effect iii. Trazodone is most commonly used to promote sleep
12
Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
b. Chloral Hydrate: i. Chloral hydrate is a non-barbiturate hypnotic used to induce sleep and to cause preoperative
sedation ii. It can be used as an adjunct to opiates and analgesics in pain control
iii. In therapeutic doses, chloral hydrate has little effect on respirations, blood pressure, or relflexes iv. It does produce numerous adverse effects in CNS
IX. Barbituates: a. Such as phenobarbital, secobarbital, and pentobarbital were used to treat insomnia before the availability
of benzodiazepines.b. Although they are effective short-term treatment of insomnia, they are also highly habit forming c. Patients can develop tolerance and physical and psychological dependence on the drugs
13

Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
Chapter 18: Drugs Treating Seizure Disorders: I. Epilepsy: a brain disorder
a. Seizures are loss of consciousness with generalized muscle twitching or mild alterations in consciousness with repetitive blinking
b. Patients with patterns of seizures who are diagnosed with epilepsy are treated with antiepileptic drugs c. The three main ways that antiepileptic drugs work are—
i. Decreasing the rate at which sodium flows into the cell ii. Inhibiting calcium flow rate into the cell through specific channels
iii. Increasing the effect of the neuroinhibitor gama aminobutyric acid (GABA) II. Physiology:
a. Action potentials within neurons are initiated by an influx of sodium into the cell b. Influx of calcium through specialized voltage-dependent channels also plays a role in creating an action
potentialc. When the cell fires, there is a release of neurotransmitters into the synaptic cleft d. The neurotransmitter glutamate produces excitation e. GABA normally acts as a counterbalance to glutamate, preventing hyperexcitation
III. Pathophysiology: a. When a group of neurons exhibits coordinated, high-frequency discharge, it is termed a focus b. The causes of a focus include head trauma, tumor growth, hypoxia, and inherited birth defects c. When the activity from a focus spreads to other areas of the brain, causing other neurons to join in the
hyperactivity, seizures result d. Seizures may result from either high levels of glutamate or low levels of GABA e. Partial seizures occur when focus activity is limited to an area of the brain
i. Simple: twitching a particular muscle group ii. Complex: involve some involuntary muscle twitching or movement also, but the patient seems
confused or exhibits odd behavior (loss of consciousness) f. When the focus activity is within both hemispheres, generalized seizure symptoms occur
i. Tonic-clonic: entire cerebral cortex is altered by hyperexcited neurons ii. Absence seizure: very brief loss of consciousness, lasting several seconds but less than 1 minute
iii. Atonic seizure: a sudden loss of muscle tone—head drop or drop attack iv. Myoclonic seizure: sudden rapid muscle contractions v. Status epilepticus: one seizure follows another without recovery of consciousness between
events or return baseline clinical state, or lasts longer than 5 minutes IV. Antiepileptic Drugs that Decrease Sodium Influx
a. Control seizures by decreasing sodium influx into the cells b. Sodium influx causes an action potential c. Phenytoin is a representative of a class of drugs called hyandoins d. Prototype Drug: phenytoin (Dilantin) e. **What condition places the patient at greater risk for toxicity to phenytoin—Malnutrition (affects
protein albumin that will be available for binding)** V. Antiepileptic Drugs that Decrease Calcium Influx
a. Prototype Drug: ethosuximide (Zarontin) b. **Ethosuximide is used to treat absence seizures**
VI. Drugs used in Seizures related to pre-eclampsia and eclampsia: a. Magnesium sulfate—completely different from others—also used to control preterm labor
i. Depresses CNS—blocks neuromuscular transmission of acetycholine and decreasing amount neurotransmitter liberated at the end plate by motor nerve impulses
14
Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
Chapter 20: Drugs Affecting Muscle Spasm and Spasticity:I. Chapter summary:
a. Spasmolytics:i. Treats spasticity: involuntary muscle contraction that is not coordinated with other muscles and
is associated with upper motor neuron syndromesii. Centrally acting or peripherally acting
b. Skeletal muscle relaxants:i. Used in combination with physical therapy and anti-inflammatory agents to treat muscle sapsms
II. Physiology: a. The human body contains approximately 600 skeletal muscles b. Skeletal muscles movement is voluntary c. Striated muscle is composed of two contractile proteins d. Muscle contraction is triggered by a sudden inflow of calcium ions (Ca2+)e. In the resting state, the protein tropomyosin winds around actin and covers the myosin-binding sites f. Muscle contraction stops when Ca2+ is removed from the immediate environment of the myofilaments
III. Pathophysiology: a. Muscle Spasm
i. Muscle spasm is a sudden, violent involuntary contraction of a muscle or group of muscles resulting from an imbalance of excitatory and inhibitory input from descending motor pathways
ii. Spasms are related to a localized skeletal muscle injury or an imbalance in electrolytes iii. Tonic spasm is characterized by an unusually prolonged and strong muscular contraction, with
relaxation occurring slowly iv. Clonic: contractions of the affected muscles occur repeatedly, forcibly, and in quick succession,
with equally sudden and frequent relaxations b. Spasticity
i. Spasticity is a condition in which certain muscles are continuously ii. Motor disorder of involuntary velocity-dependent increased muscle tone that is associated with
neurologic conditions or trauma to CNS iii. This contraction causes stiffness or tightness of the muscles iv. Spasticity may be associated with spinal cord injury
IV. Centrally Acting Muscle Relaxants: a. They act in the central nervous system (CNS) b. Prototype Drug: cyclobenzaprine (Flexeril) c. **Cyclobenzaprine is chemically similar to which of the following drugs?—
V. Centrally Acting Spasmolytics a. The centrally acting spasmolytics work in the CNS to reduce excessive reflex activity and to allow muscle
relaxation b. Used to alleviate musculoskeletal pain and spasms and reduce spasticity in a variety of neurologic
disorders c. Prototype Drug: baclofen (Lioresal) d. **Baclofen therapy is effective at treating muscle spasms due to cerebral vascular accident—false
VI. Peripherally Acting Spasmolytics a. Peripherally acting spasmolytics relax muscles through direct action on the skeletal muscle fibers b. They do not interfere with neuromuscular communication c. They have NO CNS effects d. Prototype Drug: dantrolene (Dantrium) e. **Dantrolene is used to treat which of the following conditions?--
15
Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
Chapter 13: Drugs Affecting Adrenergic Function: **The sympathetic nervous system produces what type of response?—fight or flight
I. Chapter Summary: a. The nervous system is divided into two main branches, the central nervous system (CNS) and the
peripheral nervous system (PNS) b. The efferent division has neurons that carry signals away from the brain and spinal cord to the periphery
i. Divided into the autonomic and somatic nervous system (works on skeletal muscle and voluntary movement)
c. Afferent divisions carry impulses from the periphery to the CNSd. The autonomic nervous system (ANS) is in turn subdivided into the sympathetic nervous system (SNS)
—adrenergic—and the parasympathetic nervous system (PSNS)—cholinergic i. Involuntary system responsible for control of smooth muscle, cardiac muscle, and exocrine
glands ii. Sympathetic nervous system is responsible for the fight or flight response
1. Increase our heart rate, dilate our pupils, mobilize our energy, and redirect our blood flow from non-essential organs to skeletal muscles
II. Function of the Autonomic Nervous System: a. The ANS has been identified as an involuntary system responsible for control of smooth muscle b. The actual connection between neurons and effector organs and tissues relies on neurotransmitters and
synaptic transmission c. Neurotransmitters in the ANS include acetylcholine (Ach), norepinephrine (NE), and epinephrine (Epi) d. Synaptic transmission initially involves the synthesis of neurotransmitters in the nerve terminal e. In the SNS, preganglionic transmission is mediated by ACh, whereas prostganglionic transmission is
mediated by NE III. Neurotransmitters:
a. Acetylcholine: preganglionic neurotransmitter in the SNS and both preganglionic and postganglionic in the PSNS
b. Norepinephrine: postganglionic neurotransmitter in the SNS and thus responsible for stimulation of various organs under control of SNS
c. Epinephrine: adrenalin—stored in adrenal medulla—responds to action potential however it is a hormone
d. Dopamine: precursor to NE—capable of stimulating all adrenergic receptors IV. Adrenergic Receptors:
a. In the SNS, there are several types of adrenergic receptors, including alpha-adrenergic and beta-adrenergic receptors
b. Another type of receptor, the dopaminergic receptor, is related to adrenergic receptors in that dopamine is the precursor to NE
c. Alpha and beta receptors are located throughout the body d. Alpha-1 and beta-1 receptors respond to Epi, dopamine, and NE e. Beta-2 receptors respond only to blank f. Beta-2 and alpha-2 respond to NE and Epi
V. Pathophysiology: a. The therapeutic uses of sympathetic drugs are related to providing extra-adrenergic stimulation or
blockade of normal ANS functioning b. One of the most frequent indications for adrenergic agonist drugs is shock c. Shock is the result of inadequate tissue perfusion, leaving the cells without the oxygen and nutrients they
need to function normally and survived. Drugs create therapeutic effect on the postganglionic side
VI. Adrenergic Agonists: a. Drugs that mimic the action of the SNS b. They exert their effects by direct or indirect stimulation of adrenergic receptors
i. Indirect—increasing transmission of NE, inhibiting NE reuptake, and inhibiting MAOI or COMT c. These drugs are generally divided into two groups—catecholamines and noncatecholamines
16

Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
i. Catecholamines: must be given IV infusion, do not cross blood brain barrier, short duration of action—noncatecholamines are completely opposite
d. Adrenergic agonists are also classified according to their selectivity e. Nonselective adrenergic agonists stimulate both alpha and beta receptors f. Prototype Drug nonselective adrenergic agonist: Epinephrine g. **Which of the following receptors is stimulated by epinephrine? Alpha 1, alpha 2, beta 1, beta 2
VII. Alpha-1 Adrenergic Agonists a. The alpha-1 adrenergic agonist are drugs that stimulate the alpha-1 receptor directly b. Prototype drug: Phenylephrine (Allerest)
VIII. Alpha-2 and Beta-Adrenergic Agonists: a. Alpha-2 adrenergic agonists:
i. Stimulation of alpha-2 receptors in the CNS decreases sympathetic outflow by inhibiting the release of norepinephrine
ii. Prototype Drug: Clonidine (Catapres) 1. Narrow range of specific clinical indications and has fallen out of practice 2. Pharmacotherapeutics: treatment of hypertension—decreased HR, BP, vasoconstriction,
and renal vascular resistance 3. Renal blood flow and glomerular filtration rate remain unchanged 4. Off-Label: symptoms of alcohol, methadone, or opiate withdrawal during detoxification;
reduction of allergen-induced inflammatory reactions in patients with extrinsic asthma; smoking cessation, and ulcerative colitis
5. Can also be administered via epidural line to control pain 6. Orally, parenterally, or most frequently transdermally 7. Adverse effects: dry mouth, drowsiness, dizziness, sedation, and constipation—and
rebound hypertension and erythema is common 8. Black market exists due to narcotic withdrawal properties
b. Beta-adrenergic agonists: i. Also mimic the action of the SNS and classified as either catecholamines or noncatecholamines
ii. Also labeled according to their selectivity iii. Prototype Drug: Dopamine (Intropin) iv. What route is dopamine administered by?
IX. Dopaminergic Agonists a. There are 5 types of dopamine receptors; only dopamine-1 (DA1) and dopamine-2 (DA2) receptors
mediate responses in the adrenergic nervous system b. Stimulation of DA1 and DA2 receptors results in peripheral vasodilation c. Stimulating both receptors may have either complementary or opposing effects d. Prototype Drug: Fenoldopam (Corlopam)
X. Alpha-Adrenergic Antagonists: a. Alpha-adrenergic antagonists blank the stimulation of the alpha receptors b. Alpha-1a receptors mediate human prostatic smooth muscle contraction c. Alpha-1b and alpha-1d receptors are involved in vascular smooth muscle contraction d. Prototype Drug: Prazosin (Minipress)
XI. Beta-Adrenergic Antagonists: BETA-BLOCKERS a. Grouped according to their specificity of action at the beta-1 and beta-2 receptors b. Stimulation of beta-1 only (tachycardia, increased lipolysis, inotropy) c. Stimulation of both beta-1 and beta-2 receptors (vasodilation, decreased peripheral resistance,
bronchodilaiton) d. Prototype Drug: Metoprolol (Lopressor, Toprol XL)
17
Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
Chapter 14: Drugs Affecting Cholinergic Function: I. Chapter Summary:
a. Autonomic Nervous System: divided into sympathetic and pararsympathetic nervous systems—woprk in combination or opposition to maintain homeostasis within the body
i. Because a receptor is stimulated by Ach—it is referred to as cholinergic receptor b. Drugs categorized into:
i. Cholinergic agonists: stimulate cholinergic receptors ii. Cholinergic antagonists: block cholinergic receptor and prevent Ach from attaching to the
receptor II. Function of the Autonomic Nervous System
a. The autonomic nervous system (ANS) is an involuntary system responsible for the control of smooth muscle, cardiac muscle, and exocrine glands
b. The sympathetic (SNS) and parasympathetic (PSNS) nervous systems work either as complementary or oppositional systems to maintain involuntary functions of the body
c. Parasympathetic system: “rest and digest system” i. Increased salivation
ii. Increased GI tone and motilityiii. Increased gastric secretions iv. SLUDD: salivation, lacrimation, urination, digestion, defecation
III. Cholinergic Neurotransmitters: a. Cholinergic drugs act on the parasympathetic nervous system b. Acetycholine (Ach) is the presynaptic and postsynaptic neurotransmitter in the parasympathetic nervous
system c. Ach is released in response to an action potential, diffuses across the synaptic cleft, and binds to
cholinergic receptors on the target organs or tissues d. After dissociation, Ach is degraded into two inactive products, acetate, and choline by
acetylcholinesteraseIV. Cholinergic Receptors: three types—nicotinic-N, nicotinic-M, and muscarinic
a. Nicotine receptors—i. Activation of NicotineN receptors in the adrenal medulla results in the release of epinephrine
ii. Stimulation of nicotinicM receptors results in skeletal muscle contraction b. Muscarinic Receptors—
i. Stimulation of the receptors results in the pharmacologic response of the vasodilation, resulting in decreasing blood pressure
V. Pathophysiology: a. The therapeutic uses of parasympathetic drugs are related to providing extra cholinergic
stimulation or blockade normal ANS functioning b. Disorders of the bronchi, cardiovascular system, GI or GU tract, skeletal muscle, eyes, and various
glands may respond to cholinergic stimulation Cholinergic Agonists
VI. Direct-Acting Muscarinic Agonists: a. Drugs that bind to the muscarinic receptors located in various tissues and organs throughout the body b. Their activation elicits a response that resembles the action of the parasympathetic nervous system c. Prototype Drug: Pilocarpine (Akarpine) d. What is the antidote for Pilocarpine overdosage—atropine
VII. Direct-Acting Nicotinic Agonists: a. The direct acting-nicotinic are also called ganglionic stimulating agents b. These drugs stimulate nicotininc receptors directly c. The two significant classes of nicotinic stimulants are—
i. Ganglionic stimulants ii. The neurotransmitter nicotinic stimulants
d. Prototype Drug: Nicotine e. Monotherapy use of nicotine replacement is the preferred treatment for smoking cessation—False
i. Rationale: nicotine is considered an adjunct of smoking cessation
18
Pharmacology Test 3: Chapters 48, 49, 50, 13, 14, 20, 15, and 18
VIII. Indirect-Acting Cholinergic Agonists: a. After the neurotransmitter crosses the synaptic gap and binds to a receptor, the neurotransmitter is
cleared from the synaptic gap b. Acetycholine is cleared from the synaptic gap by acetycholinesterase c. Any drug that inhibits cholinesterase will be functional equivalent of a cholinergic receptor d. Reversible cholinesterase inhibitor e. Prototype Drug: neostigmine (Prostigmin) f. Neostigmine is absorbed well when given orally—False
i. Rationale: 2-4 hours orally and 10-30 minutes parenterallyIX. Cholinergic Antagonists:
a. The cholinergic antagonists are drugs that antagonize, or block, muscarinic or nicotinic receptors directly b. The clinical importance is in decreasing blood pressure c. Include: antinicotinic ganglionic blockers, antinicotinic neuromuscular blockers, and
antimuscinaric/anticholinergic Drugs d. Prototype Drug: atropine— anticholinergic drugs specifically targeting muscarinic cholinergic receptors e. Atropine causes which of the following adverse effects
i. Urinary retention ii. Dry mouth
iii. Mydriasisiv. All of the above
f. Summary of Cholinergic Antagonists: TABLE 14.7 i. Atropine
ii. Benztropine—extrapyramidal symptoms, akathisia, dystonic rxn, haloperidol, parkinsonian, drooling, myoclonus, priapism
iii. Darifenacin—overactive bladderiv. Dicyclomine--IBSv. Flavoxate hydrochloride—overactive bladder
vi. Glycopyrrolate—inhibit salivation and excessive respiratory tract secretions vii. Hyosyamine—abd cramps, colic, dysentery, IBS, parkinsons, PUD, spastic colon, pancreatitis,
rhinitis viii. Ipratropium—asthma, chronic bronchitis, COPD, rhinorrhea
ix. Oxybutynin—overactive bladder x. Propantheline—duodenal ulcer, GI spasmolytic, hyperhidrosis, sialorrhea, urinary incontinence
xi. Scopolamine—motion sickness, preanesthesia, antidelirium, obstetric amnesia, glaucoma, opthlamology, uveitis
19
Related Documents











