Pharmacological DVT Prophylaxis Does Not Lead to Hematoma Expansion in Intracerebral Hemorrhage with Intraventricular Extension Tzu-Ching Wu, MD, Mallik Kasam, PhD, Nusrat Harun, MS, Hen Hallevi, MD, Hesna Bektas, MD, Indrani Acosta, MD, Vivek Misra, MD, Andrew D. Barreto, MD, Nicole R. Gonzales, MD, George A. Lopez, MD, James C. Grotta, MD, and Sean I. Savitz, MD Department of Neurology, University of Texas-Houston Medical School Houston, TX, USA. Abstract Background and Objective—Patients with intracerebral hemorrhage (ICH) are at high risk for development of deep venous thrombosis (DVT). Current guidelines state that low dose subcutaneous (SQ) low-molecular weight heparin (LMWH) or unfractionated heparin (UH) may be considered at 3 to 4 days from onset. However, insufficient data exists on hematoma volume (HV) in patients with ICH before and after pharmacological DVT prophylaxis, leaving physicians with uncertainty regarding the safety of this practice. Methods—We identified patients from our stroke registry (6/03 to 12/07) who presented with ICH only or ICH + intraventricular hemorrhage (IVH) and received either LMWH SQ or UH within 7 days of admission and had a repeat CT scan performed within 4 days of starting DVT prophylaxis. We calculated the change in hematoma volume (Δvol) from the admission and post treatment CTs. HV was calculated using the (ABC/2) method and IVH volumes were calculated using a published method of hand drawn regions of interest (ROI) Results—We identified 73 patients with a mean age of 63 yo and median NIHSS 11.5. The mean baseline total HV was 25.8ml ± 23.2ml. There was an absolute Δvol from pre and posttreatment CT of −4.3ml ± 11.0ml. Two patients developed hematoma growth. Repeat analysis of patients given pharmacological DVT prophylaxis within 2 or 4 days after ICH found no increase in hematoma size. Conclusion—Pharmacological DVT prophylaxis given SQ in patients with ICH and/or IVH in the subacute period is generally not associated with hematoma growth. Keywords Intracerebral Hemorrhage; Anticoagulants Corresponding Author: Sean I. Savitz, MD Department of Neurology The University of Texas-Houston Medical School 6431 Fannin Street Suite Houston, TX 77030, USA Phone number: + 1713 500 7092 Fax number: +1 713 500 0692 [email protected]. Conflicts of interest Authors have no conflicts of interest to disclose This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain. NIH Public Access Author Manuscript Stroke. Author manuscript; available in PMC 2012 August 07. Published in final edited form as: Stroke. 2011 March ; 42(3): 705–709. doi:10.1161/STROKEAHA.110.600593. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Pharmacological DVT Prophylaxis Does Not Lead to HematomaExpansion in Intracerebral Hemorrhage with IntraventricularExtension
Tzu-Ching Wu, MD, Mallik Kasam, PhD, Nusrat Harun, MS, Hen Hallevi, MD, Hesna Bektas,MD, Indrani Acosta, MD, Vivek Misra, MD, Andrew D. Barreto, MD, Nicole R. Gonzales, MD,George A. Lopez, MD, James C. Grotta, MD, and Sean I. Savitz, MDDepartment of Neurology, University of Texas-Houston Medical School Houston, TX, USA.
AbstractBackground and Objective—Patients with intracerebral hemorrhage (ICH) are at high risk fordevelopment of deep venous thrombosis (DVT). Current guidelines state that low dosesubcutaneous (SQ) low-molecular weight heparin (LMWH) or unfractionated heparin (UH) maybe considered at 3 to 4 days from onset. However, insufficient data exists on hematoma volume(HV) in patients with ICH before and after pharmacological DVT prophylaxis, leaving physicianswith uncertainty regarding the safety of this practice.
Methods—We identified patients from our stroke registry (6/03 to 12/07) who presented withICH only or ICH + intraventricular hemorrhage (IVH) and received either LMWH SQ or UHwithin 7 days of admission and had a repeat CT scan performed within 4 days of starting DVTprophylaxis. We calculated the change in hematoma volume (Δvol) from the admission and posttreatment CTs. HV was calculated using the (ABC/2) method and IVH volumes were calculatedusing a published method of hand drawn regions of interest (ROI)
Results—We identified 73 patients with a mean age of 63 yo and median NIHSS 11.5. The meanbaseline total HV was 25.8ml ± 23.2ml. There was an absolute Δvol from pre and posttreatmentCT of −4.3ml ± 11.0ml. Two patients developed hematoma growth. Repeat analysis of patientsgiven pharmacological DVT prophylaxis within 2 or 4 days after ICH found no increase inhematoma size.
Conclusion—Pharmacological DVT prophylaxis given SQ in patients with ICH and/or IVH inthe subacute period is generally not associated with hematoma growth.
KeywordsIntracerebral Hemorrhage; Anticoagulants
Corresponding Author: Sean I. Savitz, MD Department of Neurology The University of Texas-Houston Medical School 6431 FanninStreet Suite Houston, TX 77030, USA Phone number: + 1713 500 7092 Fax number: +1 713 500 0692 [email protected].
Conflicts of interest Authors have no conflicts of interest to disclose
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providingthis early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before itis published in its final citable form. Please note that during the production process errors may be discovered which could affect thecontent, and all legal disclaimers that apply to the journal pertain.
NIH Public AccessAuthor ManuscriptStroke. Author manuscript; available in PMC 2012 August 07.
Published in final edited form as:Stroke. 2011 March ; 42(3): 705–709. doi:10.1161/STROKEAHA.110.600593.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
IntroductionPatients with intracerebral hemorrhage (ICH) or ischemic stroke are at high risk fordevelopment of venous thromboembolism (VTE) (1). In comparison to patients withischemic stroke, the risk for VTE is higher in the hemorrhagic stroke population (2). VTErisk is also enhanced by immobilization and paresis of the lower extremities and laterecognition of subclinical thrombotic events. Without preventative measures, 53% and 16%of immobilized patients develop deep venous thrombosis (DVT) or pulmonary embolism(PE), respectively, in this population (3). One study detected DVT in 40% of ICH patientswithin two weeks and 1.9% of those patients had a PE (4). Development of VTE in the ICHpatient adds further detrimental complications to an already lethal disease with a 1 monthcase fatality rate of 35-52% (5). DVT also prolongs the length of hospital stays, delaysrehabilitation programs, and introduces a potential risk for PE (6).
Current AHA/ASA guidelines for acute ischemic stroke recommend the administration ofsubcutaneous (SQ) anticoagulants such as unfractionated heparin (UH) or low-molecularweight heparin (LMWH) to prevent DVT in immobilized patients (1). On the other hand,AHA/ASA guidelines for hemorrhagic stroke are less clear stating that subcutaneousanticoagulants may be considered at 3 to 4 days from onset, after documentation of cessationof bleeding (5). This tepid recommendation stems from the fact that there is a lack of largerandomized controlled trials addressing VTE prevention in the ICH population and even lessdata are available for patients with intraventricular hemorrhage (IVH). As a consequence,there is no consensus on how and when to start DVT prophylaxis to prevent VTEcomplications in the ICH and/or IVH population.
Much hesitation arises from the concern that anticoagulants may increase hematoma sizeand cause neurological worsening (7). There have been 2 small prospective randomizedtrials published on early heparin use in ICH both showing no increased risk of bleeding (8,9). One recent published prospective randomized trial compared early use LMWH andcompression stockings in ICH patients also found no increase risk of hematoma enlargementin both groups (6). However the number of patients was small in these studies andsubsequent CTs were not always routinely performed to document rebleeding. With the lackof data and concerns about hematoma expansion, physicians are left with uncertaintyregarding the safety of this practice (10, 11).
This retrospective study aimed to assess the safety of subcutaneous anticoagulants in theICH and/or IVH population and its association with hematoma growth.
MethodsStudy Design and Population
A retrospective search from our prospectively gathered stroke registry from June 2003 toDecember 2007 identified all patients with the diagnosis of ICH. Patients were excludedwho had an ICH etiology of mass lesion, AVM, aneurysm, or undetermined. HypertensiveICH was diagnosed if patients had history of hypertension with typical hemorrhage locationon imaging. Amyloid bleeds were diagnosed using clinical information including history ofhypertension, blood pressure on presentation and through-out the hospitalization stay andsupportive imaging. Coagulopathy associated bleeds were diagnosed if patients had ICH inthe setting of elevated INRs on admission. Patients were categorized as having anundetermined etiology if it was unclear whether the etiology was hypertension, amyloid orboth based on the clinical and radiological data.
Wu et al. Page 2
Stroke. Author manuscript; available in PMC 2012 August 07.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Patients were included after chart reviews confirmed ICH and/or IVH on admission andreceived either LMWH SQ or UH SQ within 7 days of admission and had a subsequent CTscan performed within 4 days of starting DVT prophylaxis. Treatment within 7 days ofadmission was chosen since the guidelines for DVT prophylaxis initiation is unclear and toalso capture prescribing trends at our institution. CT scans within 4 days of starting DVTprophylaxis was chosen to allow for variability in post treatment scanning since this is aretrospective analysis. Separate analysis was performed on patients that received eitherLMWH SQ or UH SQ within 2 and 4 days of admission and by diagnosis (ICH only, ICH+IVH). Chart review was performed on patients that fit the study criteria (figure 1) to gatherbaseline demographics and clinical information including admission NIHSS and dischargemodified Rankin score.
ManagementPatients with ICH and/or IVH were treated according to AHA/ASA guidelines (5) and werenot treated with Factor VII or received intraventricular tPA; however, blood pressures in theacute post-bleed period were not strictly protocolized. In patients that demonstratedobstructive hydrocephalus, an external ventricular drain was placed. Two forms of SQanticoagulants (LMWH=enoxaparin 40mg or dalteparin 5000 Units SQ once daily,UH=heparin 5000 units SQ twice to three times a day) were employed at our institutionduring this period. Medication preference and timing of administration were left up to thediscretion of the attending physician. Intermittent compression devices were used on allpatients.
RadiologicalAll CT scans were performed using identical technique (slice thickness 5mm, gantry tilt—16). Admission CT scans was reviewed by the authors to confirm ICH and/or IVH. Allhematoma volume calculations were performed by a single author blinded to the treatmentand outcome of the study. ICH volume within the parenchyma was calculated using the(ABC/2) method (12). IVH volume was calculated using a published method of hand drawnregions of interest (ROI) around each area of intraventricular blood in every slice, multipliedby the slice thickness and added together to obtain the total IVH volume (13). The sum ofthe ICH volume and IVH volume was considered the total hematoma volume (HV). Thechange in hematoma volume (Δvol) defined as the difference between the total HV of thefirst post treatment CT scan and the total HV of the admission CT scan. Hematoma site wasclassified into deep (thalamus, putamen, caudate), lobar, and other (primary IVH, cerebellar,brainstem).
Hematoma GrowthWe chose absolute hematoma growth as our primary outcome and significant hematomagrowth as our secondary outcome. Significant hematoma growth was defined as change inhematoma volume >33% and an absolute change in volume ≥ 5ml. We chose a change involume of >33% since it corresponds to a 10% increase in diameter in a sphere and it hadbeen used in prior hematoma growth studies (14). An absolute Δvol of 5ml was chosen asthe cutoff because the authors felt that a Δvol ≤ 5ml was unlikely to cause clinicaldeterioration and it also accounts for imprecise hematoma volume calculation using CT.
Statistical AnalysisUsing the cutoff of 5ml and the SD of our data (25ml), sample size/power calculations wereperformed and it showed that with a correlation of 0.85, it would require 61 patients for 80%power in detecting a Δvol of 5ml. Means with standard deviations or medians forcontinuous variables were used. The differences were assessed using t-tests, chi-square tests,
Wu et al. Page 3
Stroke. Author manuscript; available in PMC 2012 August 07.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Fisher exact test or Mann-Whitney U test. A significance level of 0.05 was used to assessstatistical difference. The statistical analysis was performed using SAS 9.
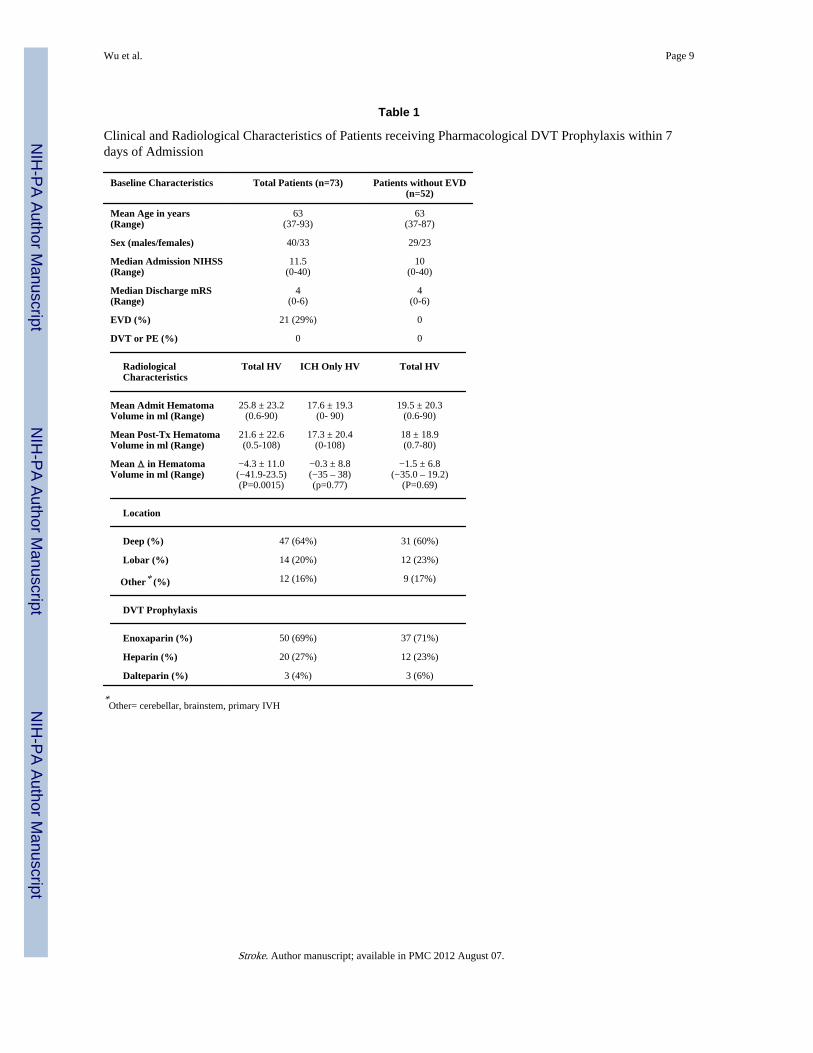
ResultsWe identified 73 patients who met study criteria. Baseline clinical and radiologicalcharacteristics are shown in table 1. The mean age was 63 and the median NIHSS onadmission was 11.5. Fifty patients (69%) received enoxaparin, 20 patients (27%) receivedunfractionated heparin, and 3 patients (4%) received dalteparin. The time from ICHadmission to DVT prophylaxis administration also varied; the majority of DVT prophylaxiswas administered between days 2-5 (Figure 2). Overall, there was an absolute Δvol from preand post-treatment CT of −4.3ml ± 11.0ml (p=0.0015). Analyzing only the ICH portion ofthe hematoma in all 73 patients showed absolute Δvol of −0.3ml ± 8.8ml (p=0.77). Inpatients without EVD placement, the absolute Δvol was −1.5ml ± 6.8ml (p=0.69).
Two patients (2.7%) showed significant hematoma growth within the study period. Onepatient received LMWH and one received UH, with hypertension as the etiology of thebleed in both patients. No pattern was indentified in regards to clinical and radiologicalcharacteristics for these two patients that had significant hematoma growth.
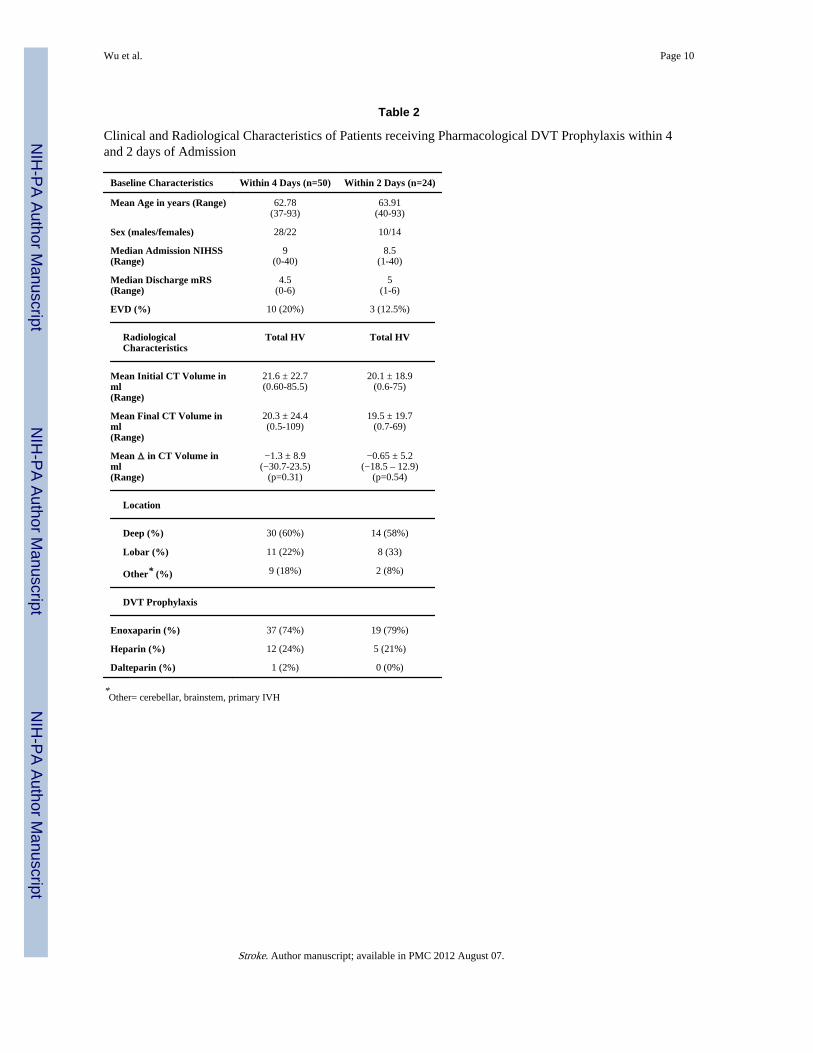
We analyzed separately patients that received DVT prophylaxis within 4 days of admissionand results revealed an absolute Δvol from pre and post-treatment CT of −1.3ml ± 8.9ml(P=0.31) (Table 2). For patients that received DVT prophylaxis within 2 days of admission,data showed an absolute Δvol from pre and post-treatment CT of −0.65ml ± 5.2ml (P=0.54)(Table 2).
DiscussionTo our knowledge, this study is the first to report hematoma growth with regards to the useof SQ anticoagulants for DVT prevention in the ICH and IVH population. In the studyrecently published by Orken et al, they studied the safety of LMWH and compressionstocking for DVT prophylaxis and its effects on hematoma enlargement in ICH patients.They found that treatment with LMWH (n=39) and compression stocking (n=36) for DVT/PE prevention was not associated with hematoma enlargement, but did not report thefrequency of IVH in their study population nor commented on time to medicationadministration, only that it was given after 48 hours (6). In comparison, the majority of ourpatients were started on anticoagulants within 2-5 days of their hemorrhage with 28%(n=20) patients receiving anticoagulants within 48 hrs of admission. In general we foundthat the administration of pharmacological DVT prophylaxis SQ in the acute (2-4 days) tosubacute period (≤7days) was not associated with hematoma growth. Our patients in thisstudy had variable sizes of hematoma from 0.5 cc to 90 cc. In the subacute period, however,two patients did develop significant hematoma expansion but no pattern or factors could befound that were associated with hematoma growth. Hematoma growth was also not observedwhen the patient population was partitioned by diagnosis (ICH only and ICH + IVH) and bythe presence of an EVD. However, the difference in Δvol in the ICH only group was muchsmaller than the ICH +IVH group confirming that IVH plays a role in hematoma resolution.Of the 36 ICH +IVH patients, 21 of them had an EVD placed and we only identified onepatient that developed bleeding around the catheter. Therefore, starting SQ anticoagulants inpatients with EVDs may be safe with low rates of complications. Our data, however, doesindicate that patients that were treated in the acute period had lower median admissionNIHSS scores (9 within day 4, 8.5 within day 2) compared to a median NIHSS of 11.5 forthose treated within day 7 of admission. This may indicate that there is a tendency to delaySQ anticoagulation in the sicker ICH patients or possibly those patients with higher
Wu et al. Page 4
Stroke. Author manuscript; available in PMC 2012 August 07.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

admission NIHSS tend to have early rebleeding leading to later SQ anticoagulationadministration.
Current guidelines for ICH management recommend intermittent pneumatic compression forprevention of VTE, and its use has been demonstrated to be effective (15). Even though norandomized data exist, the addition of SQ anticoagulants to intermittent pneumaticcompression devices should provide added protection against the development VTE. Thewidespread availability, low cost and proven efficacy of SQ anticoagulants for VTEprevention can potentially reduce VTE complications in the highly vulnerable ICH/IVHpopulation. Our study adds to the existing limited literature and further supports the safety ofanticoagulants in the acute and subacute period after ICH.
Our study is limited, however, by its retrospective nature, small sample size and the inherentinaccuracy of measuring hematoma volume on CT scan. With the small sample, we werealso unable to assess the efficacy of SQ LMWH or SQ UH in preventing DVT or PE,however, there were no PE or DVT observed in the study population. The observed overallhematoma reduction may be largely contributed by ventriculostomy drainage and/or naturalhematoma regression; however, when looking at the ICH portion of all 73 study patients,hematoma growth was not observed. Another major confounder may be blood pressurecontrol, as some have postulated that hematoma growth is associated with the degree ofhypertension control in ICH patients (16).
The inclusion criteria of the study may have also affected our data and results. First, we onlyincluded patients that received DVT prophylaxis. This selection bias may have excludedpatients that had more severe hemorrhages, with the potential for early hematoma growth inwhich the attending physician may have chosen to withhold anticoagulants. Conversely, byonly including patients that had follow up imaging, we may also have neglected a populationof stable patients that received SQ anticoagulants and were clinically stable, hence notnecessitating follow up CT scans. This may have over-represented patients with hematomaenlargements in this study since those that clinically deteriorate are more likely to havefollow-up imaging. Lastly, by choosing to only analyze the hematoma volume of the firstpost-treatment CT scan, we were limited in our ability to detect delayed hematomaexpansion.
In conclusion, data from this study suggest that administration of SQ LMWH or UH inpatients with ICH and/or IVH for DVT prophylaxis in the acute to subacute period isgenerally safe. A prospective safety and efficacy study of SQ anticoagulants in ICH patientsis warranted.
AcknowledgmentsThis study was funded by NIH Training Grant: 5 T32 NS007412-12, SPOTRIAS Grant: P50 NS 044227, theHoward Hughes Medical Institute, and the American Heart Association 0475008N.
References1). Adams HP Jr, del Zoppo G, Alberts MJ, Bhatt DL, Brass L, Furlan A, Grubb RL, Higashida RT,
Jauch EC, Kidwell C, Lyden PD, Morgenstern LB, Qureshi AI, Rosenwasser RH, Scott PA,Wijdicks EF. Guidelines for the early management of adults with ischemic stroke: A Guidelinefrom the American Heart Association/American Stroke Association Stroke Council, ClinicalCardiology Council, Cardiovascular Radiology and Intervention Council, and the AtheroscleroticPeripheral Vascular Disease and Quality of Care Outcomes in Research Interdisciplinary.Working Groups: the American Academy of Neurology affirms the value of this guideline as aneducational tool for neurologists. Stroke. 2007; 38:1655–1711. [PubMed: 17431204]
Wu et al. Page 5
Stroke. Author manuscript; available in PMC 2012 August 07.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
2). Skaf E, Stein PD, Beemath A, Sanchez J, Bustamante MA, Olson RE. Venous Thromboembolismin Patients with Ischemic and Hemorrhagic Stroke. The American Journal of Cardiology.96:1731–1733. [PubMed: 16360366]
3). Warlow C, Ogston D, Douglas AS. Deep venous thrombosis of legs after strokes: Part I – Incidenceand predisposing factors. Part II – Natural history. Br Med J. 1976:1178–83. [PubMed: 1268614]
4). Ogata T, Yasaka M, Wakugawa Y, Inoue T, Ibayashi S, Okada Y. Deep Venous Thrombosis AfterAcute Intracerebral Hemorrhage. Journal of the Neurological Sciences. 2008; 272:83–86.[PubMed: 18555486]
5). Broderick J, Connolly S, Feldmann E, Hanley D, Kase C, Krieger D, Mayberg M, Morgenstern L,Ogilvy CS, Vespa P, Zuccarello M. Guidelines for the Management of Spontaneous IntracerebralHemorrhage in Adults 2007 Update: A Guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and theQuality of Care and Outcomes in Research Interdisciplinary Working Group. Stroke. 2007;38:2001–2023. [PubMed: 17478736]
6). Orken DN, Kenangil G Gulay, Ozkurt H, Guner C, Gundogdu L, Basak M, Forta H. Prevention ofDeep Venous Thrombosis and Pulmonary Embolism in Patients with Acute IntracerebralHemorrhage. The Neurologist. 2009; 15:329–331. [PubMed: 19901711]
7). Kiphuth IC, Staykov D, Kohrmann M, Struffert T, Ricter G, Bardutzky J, Kollmar R, Maurer M,Schellinger PD, Hilz MJ, Doerfler A, Schwab S, Huttner HB. Early Administration of LowMolecular Weight Heparin after Spontaneous Intracerebral Hemorrhage–A Safety Analysis.Cerebrovascular Diseases. 2009; 27:146–150. [PubMed: 19039218]
8). Boeer A, Voth E, Henze TH, Prange HW. Early Heparin Therapy in Patients with SpontaneousIntracerebral Haemorrhage. Journal of Neurology, Neurosurgery, and Psychiatry. 1991; 54:466–467.
9). Dickman U, Voth E, Schicha H, Henze TH, Prange HW, Emrich D. Heparin Therapy, Deep-VeinThrombosis and Pulmonary Embolism after Intracerebral Hemorrhage. Klinische Wochenschrift.1988:1182–1183. [PubMed: 3062268]
10). Kazui S, Naritomi H, Yamamoto H, Sawada T, Yamaguchi T. Enlargement of SpontaneousIntracerebral hemorrhage: incidence and time course. Stroke. 1996; 27:1783–1787. [PubMed:8841330]
11). Lim JK, Hwang HS, Cho BM, Lee HK, Ahn SK, Oh SM, Choi SK. Multivariate analysis of riskfactors of hematoma expansion in spontaneous intracerebral hemorrhage. Surg Neurol. 2008;69:40–45. [PubMed: 18054613]
12). Huttner HB, Steiner T, Hartmann M, Köhrmann M, Juettler E, Mueller S, Wikner J, Meyding-Lamade U, Schramm P, Schwab S, Schellinger PD. Comparison of ABC/2 Estimation Techniqueto Computer-assisted Planimetric Analysis in Warfarin-related Intracerebral ParenchymalHemorrhage. Stroke. 2006; 37:404–408. [PubMed: 16373654]
13). Zimmerman RD, Maldjian JA, Brun NC, Horvath B, Skolnick BE. Radiologic Estimation ofHematoma Volume in Intracerebral Hemorrhage Trial by CT Scan. AJNR. 2006; 27:666–670.[PubMed: 16552014]
14). Brott T, Broderick J, Kothari R, Barsan W, Tomsick T, Sauerbeck L, Spilker J, Duldner J, KhouryJ. Early hemorrhage growth in patients with intracerebral hemorrhage. Stroke. 1997; 28:1–5.[PubMed: 8996478]
15). Lacut K, Bressollette L, Le Gal G, Etienne E, De Tinteniac A, Renault A, Rouhard F, Besson G,Garcia JF, Mottier D, Oger E. Prevention of Venous Thrombosis in Patients with AcuteIntracerebral Hemorrhage. Neurology. 2005; 65:865–869. [PubMed: 16186525]
16). Kazui SMK, Sawada T, Yamaguchi T. Predisposing factors to enlargement of spontaneousintracerebral hematoma. Stroke. 1997; 28:2370–75. [PubMed: 9412616]
Wu et al. Page 6
Stroke. Author manuscript; available in PMC 2012 August 07.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
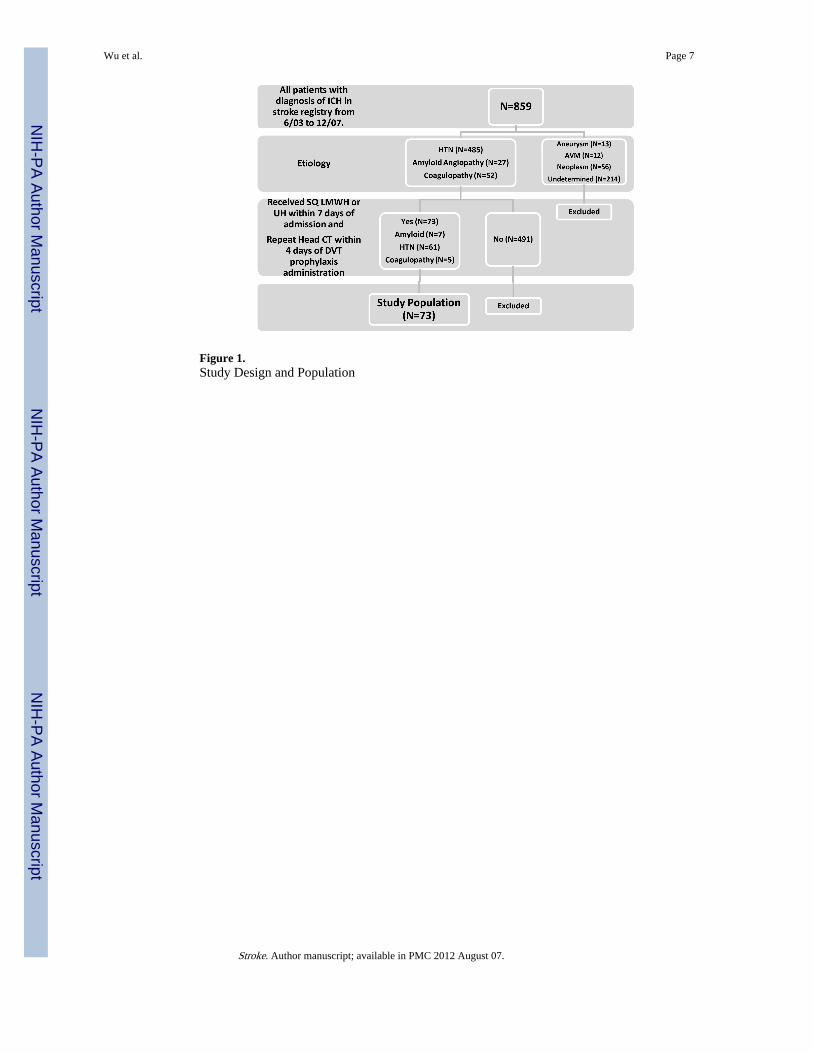
Figure 1.Study Design and Population
Wu et al. Page 7
Stroke. Author manuscript; available in PMC 2012 August 07.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
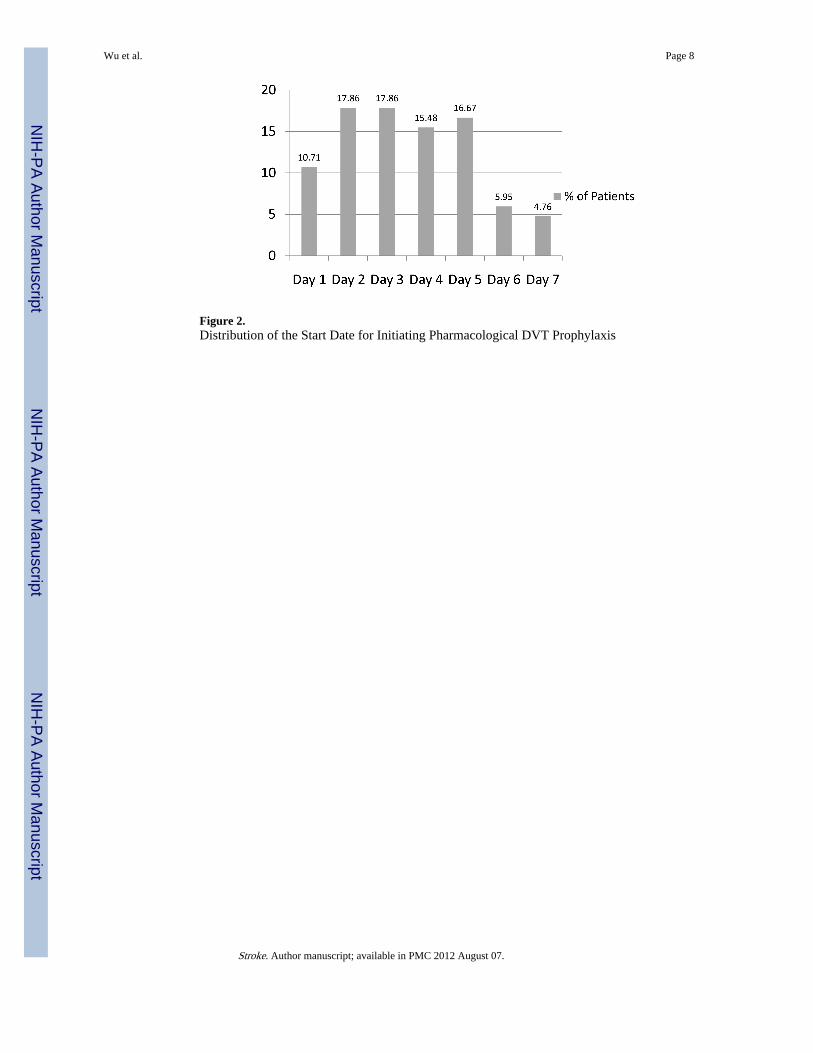
Figure 2.Distribution of the Start Date for Initiating Pharmacological DVT Prophylaxis
Wu et al. Page 8
Stroke. Author manuscript; available in PMC 2012 August 07.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Wu et al. Page 9
Table 1
Clinical and Radiological Characteristics of Patients receiving Pharmacological DVT Prophylaxis within 7days of Admission
Baseline Characteristics Total Patients (n=73) Patients without EVD(n=52)
Mean Age in years(Range)
63(37-93)
63(37-87)
Sex (males/females) 40/33 29/23
Median Admission NIHSS(Range)
11.5(0-40)
10(0-40)
Median Discharge mRS(Range)
4(0-6)
4(0-6)
EVD (%) 21 (29%) 0
DVT or PE (%) 0 0
Radiological Characteristics
Total HV ICH Only HV Total HV
Mean Admit HematomaVolume in ml (Range)
25.8 ± 23.2(0.6-90)
17.6 ± 19.3(0- 90)
19.5 ± 20.3(0.6-90)
Mean Post-Tx HematomaVolume in ml (Range)
21.6 ± 22.6(0.5-108)
17.3 ± 20.4(0-108)
18 ± 18.9(0.7-80)
Mean Δ in HematomaVolume in ml (Range)
−4.3 ± 11.0(−41.9-23.5)(P=0.0015)
−0.3 ± 8.8(−35 – 38)(p=0.77)
−1.5 ± 6.8(−35.0 – 19.2)
(P=0.69)
Location
Deep (%) 47 (64%) 31 (60%)
Lobar (%) 14 (20%) 12 (23%)
Other* (%) 12 (16%) 9 (17%)
DVT Prophylaxis
Enoxaparin (%) 50 (69%) 37 (71%)
Heparin (%) 20 (27%) 12 (23%)
Dalteparin (%) 3 (4%) 3 (6%)
*Other= cerebellar, brainstem, primary IVH
Stroke. Author manuscript; available in PMC 2012 August 07.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Wu et al. Page 10
Table 2
Clinical and Radiological Characteristics of Patients receiving Pharmacological DVT Prophylaxis within 4and 2 days of Admission
Baseline Characteristics Within 4 Days (n=50) Within 2 Days (n=24)
Mean Age in years (Range) 62.78(37-93)
63.91(40-93)
Sex (males/females) 28/22 10/14
Median Admission NIHSS(Range)
9(0-40)
8.5(1-40)
Median Discharge mRS(Range)
4.5(0-6)
5(1-6)
EVD (%) 10 (20%) 3 (12.5%)
Radiological Characteristics
Total HV Total HV
Mean Initial CT Volume inml(Range)
21.6 ± 22.7(0.60-85.5)
20.1 ± 18.9(0.6-75)
Mean Final CT Volume inml(Range)
20.3 ± 24.4(0.5-109)
19.5 ± 19.7(0.7-69)
Mean Δ in CT Volume inml(Range)
−1.3 ± 8.9(−30.7-23.5)
(p=0.31)
−0.65 ± 5.2(−18.5 – 12.9)
(p=0.54)
Location
Deep (%) 30 (60%) 14 (58%)
Lobar (%) 11 (22%) 8 (33)
Other* (%) 9 (18%) 2 (8%)
DVT Prophylaxis
Enoxaparin (%) 37 (74%) 19 (79%)
Heparin (%) 12 (24%) 5 (21%)
Dalteparin (%) 1 (2%) 0 (0%)
*Other= cerebellar, brainstem, primary IVH
Stroke. Author manuscript; available in PMC 2012 August 07.
Related Documents











