© 2003 Blackwell Science Ltd Br J Clin Pharmacol , 55 , 115–125 115 Blackwell Science, Ltd Oxford, UK BCPBritish Journal of Clinical Pharmacology 0306-5251Blackwell Publishing 2002 54Original Article Once-daily nelfinavir/ritonavirR. E. Aarnoutse et al. Correspondence: Rob E. Aarnoutse, Department of Clinical Pharmacy, Univer- sity Medical Centre Nijmegen, PO Box 9101, 533 KF, 6500 HB, Nijmegen, The Netherlands. Tel.: + 31 24 361 6405; Fax: + 31 24 354 0331; E-mail: [email protected]. Received 19 February 2002, accepted 17 September 2002. Pharmacokinetics, food intake requirements and tolerability of once- daily combinations of nelfinavir and low-dose ritonavir in healthy volunteers R. E. Aarnoutse, J. A. H. Droste, J. J. G. van Oosterhout, P. P. Koopmans, M. Popescu, 1 P. Reiss, 2 Y. A. Hekster & D. M. Burger Departments of Clinical Pharmacy & General Internal Medicine, University Medical Centre Nijmegen, Nijmegen, The Netherlands, 1 F. Hoffmann- La Roche Ltd, Basel, Switzerland, and 2 Department of Infectious Diseases, Tropical Medicine and AIDS, and National AIDS Therapy Evaluation Centre, Academic Medical Centre, Amsterdam, The Netherlands Aims This study was performed to evaluate the steady-state pharmacokinetics, food intake requirements and short-term tolerability of once-daily combinations of nelfi- navir and low-dose ritonavir. Methods Twenty-seven healthy volunteers were randomized over three groups to receive a once-daily regimen of nelfinavir/ritonavir 2000/200 mg (group 1), 2000/ 400 mg (group 2) or 2500/200 mg (group 3) with food for 14 days. Pharmacoki- netic parameters for nelfinavir and its active metabolite M8 were assessed on study days 15 and 16, after administration of the regimens with a full (610 kcal) or light (271 kcal) breakfast, respectively. Results Pharmacokinetic data were evaluable for eight volunteers in group 1, eight in group 2 and four in group 3. Administration of nelfinavir/ritonavir with a full breakfast resulted in geometric mean (GM) nelfinavir AUC 24h values of 76.8, 51.3, and 61.9 h*mg/l in group 1, 2 and 3, respectively. GM 24-h C min concentrations of nelfinavir were 0.76 mg l - 1 , 0.43 mg l - 1 and 0.47 mg l - 1 , respectively. Co- administration of ritonavir increased M8 concentrations more than nelfinavir con- centrations, resulting in GM AUC 24h and C min values for nelfinavir plus M8 that were higher than or comparable to reference values for the approved regimen of nelfinavir (1250 mg BID without ritonavir). In the 2000/200 mg group, seven out of eight subjects had a C min value of nelfinavir plus M8 above a threshold of 1.0 mg l - 1 . Administration of the combinations with a light breakfast resulted in significant decreases in the AUC 24h and C min of nelfinavir and nelfinavir plus M8, compared with intake with a full breakfast. For the C min of nelfinavir plus M8, the GM ratio (light/full breakfast) was 0.76 (90% confidence interval 0.67–0.86, participants from all groups combined) . Short-term tolerability was satisfactory, apart from a higher than expected incidence of mild rash (12%). Conclusions Administration of nelfinavir in a once-daily regimen appears feasible. A nelfinavir/ritonavir 2000/200 mg combination appears appropriate for further evaluation. Once-daily nelfinavir/ritonavir should be taken with a meal containing at least 600 kcal. Keywords: nelfinavir, once daily, pharmacokinetics, ritonavir Introduction The availability of highly active antiretroviral therapy (HAART) has dramatically decreased mortality and mor- bidity in HIV infection [1]. However, up to 50% of treatment-naive patients do not have sustained antiviral response after 1 year of therapy [2, 3]. To a considerable extent this can be ascribed to difficulties in achieving

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

© 2003 Blackwell Science Ltd
Br J Clin Pharmacol
,
55
, 115–125
115
Blackwell Science, Ltd
Oxford, UK
BCPBritish Journal of Clinical Pharmacology
0306-5251Blackwell Publishing 2002
54Original Article
Once-daily nelfinavir/ritonavirR. E. Aarnoutse
et al.
Correspondence:
Rob E. Aarnoutse, Department of Clinical Pharmacy, Univer-sity Medical Centre Nijmegen, PO Box 9101, 533 KF, 6500 HB, Nijmegen,The Netherlands. Tel.:
+
31 24 361 6405; Fax:
+
31 24 354 0331; E-mail:[email protected].
Received 19 February 2002, accepted 17 September 2002.
Pharmacokinetics, food intake requirements and tolerability of once-daily combinations of nelfinavir and low-dose ritonavir in healthy volunteers
R. E. Aarnoutse, J. A. H. Droste, J. J. G. van Oosterhout, P. P. Koopmans, M. Popescu,
1
P. Reiss,
2
Y. A. Hekster & D. M. Burger
Departments of Clinical Pharmacy & General Internal Medicine, University Medical Centre Nijmegen, Nijmegen, The Netherlands,
1
F. Hoffmann-La Roche Ltd, Basel, Switzerland, and
2
Department of Infectious Diseases, Tropical Medicine and AIDS, and National AIDS Therapy Evaluation Centre, Academic Medical Centre, Amsterdam, The Netherlands
Aims
This study was performed to evaluate the steady-state pharmacokinetics, foodintake requirements and short-term tolerability of once-daily combinations of nelfi-navir and low-dose ritonavir.
Methods
Twenty-seven healthy volunteers were randomized over three groups toreceive a once-daily regimen of nelfinavir/ritonavir 2000/200 mg (group 1), 2000/400 mg (group 2) or 2500/200 mg (group 3) with food for 14 days. Pharmacoki-netic parameters for nelfinavir and its active metabolite M8 were assessed on studydays 15 and 16, after administration of the regimens with a full (610 kcal) or light(271 kcal) breakfast, respectively.
Results
Pharmacokinetic data were evaluable for eight volunteers in group 1, eightin group 2 and four in group 3. Administration of nelfinavir/ritonavir with a fullbreakfast resulted in geometric mean (GM) nelfinavir
AUC
24h
values of 76.8, 51.3,and 61.9 h*mg/l in group 1, 2 and 3, respectively. GM 24-h
C
min
concentrationsof nelfinavir were 0.76 mg l
-
1
, 0.43 mg l
-
1
and 0.47 mg l
-
1
, respectively. Co-administration of ritonavir increased M8 concentrations more than nelfinavir con-centrations, resulting in GM
AUC
24h
and
C
min
values for nelfinavir plus M8 thatwere higher than or comparable to reference values for the approved regimen ofnelfinavir (1250 mg BID without ritonavir). In the 2000/200 mg group, seven outof eight subjects had a
C
min
value of nelfinavir plus M8 above a threshold of 1.0 mgl
-
1
. Administration of the combinations with a light breakfast resulted in significantdecreases in the
AUC
24h
and
C
min
of nelfinavir and nelfinavir plus M8, comparedwith intake with a full breakfast. For the
C
min
of nelfinavir plus M8, the GM ratio(light/full breakfast) was 0.76 (90% confidence interval 0.67–0.86, participants fromall groups combined)
.
Short-term tolerability was satisfactory, apart from a higherthan expected incidence of mild rash (12%).
Conclusions
Administration of nelfinavir in a once-daily regimen appears feasible.A nelfinavir/ritonavir 2000/200 mg combination appears appropriate for furtherevaluation. Once-daily nelfinavir/ritonavir should be taken with a meal containingat least 600 kcal.
Keywords:
nelfinavir, once daily, pharmacokinetics, ritonavir
Introduction
The availability of highly active antiretroviral therapy(HAART) has dramatically decreased mortality and mor-bidity in HIV infection [1]. However, up to 50% oftreatment-naive patients do not have sustained antiviralresponse after 1 year of therapy [2, 3]. To a considerableextent this can be ascribed to difficulties in achieving

R. E. Aarnoutse
et al
.
116
© 2003 Blackwell Science Ltd
Br J Clin Pharmacol
,
55
, 115–125
adequate adherence to the complex HAART regimens[4, 5]. Simpler dosing regimens are associated with betteradherence [6–8], and there is a move to decrease thefrequency of HAART dosing to a once-daily regimen.
Pharmacokinetic interactions between protease inhib-itors (PIs) can be exploited as a means of decreasing thedosing frequency of these antiretroviral drugs. More spe-cifically, exposure to PIs can be raised, and their half-lives can be prolonged, by coadministration of low-doseritonavir [9]. The latter impairs the metabolism of otherPIs by potent inhibition of cytochrome (CYP) 3A4. Datafrom recent studies suggest that ritonavir can adequatelyboost concentrations of amprenavir, indinavir andsaquinavir, to allow for once-daily dosing of these PIs[10–15].
Nelfinavir is another PI that is widely used for treat-ment of HIV infection. It is approved for twice-dailydosing (1250 mg BID), and should be taken with food[16].
In vitro
studies revealed that nelfinavir is metabolizedby at least five different pathways, catalysed by severalCYP isoenzymes (CYP3A4, CYP2C19, CYP2D6 andCYP2C9 [17]). CYP3A4 and CYP2C19 are the pre-dominant contributors to nelfinavir metabolism.CYP2C19 catalyses exclusively the conversion of nelfi-navir to an active metabolite termed M8, which in turnis metabolized by CYP3A4 [18]. Plasma concentrationsof M8 are about 30% of those of nelfinavir after BIDdosing of the latter [19]. M8 has equipotent activity tonelfinavir
in vitro
, binds to plasma protein
in vivo
to asimilar extent to nelfinavir (
≥
98%), and has an almostidentical molar weight [20]. Assuming additive virologicalefficacy, this suggests that the sum nelfinavir and M8plasma concentrations may represent all active drug afteradministration of the parent drug.
Nelfinavir appears to be an appropriate PI for once-daily administration, because of its pharmacokineticproperties and its good tolerability. Nelfinavir shows sloworal absorption and an elimination half-life that is rela-tively long (3.5–5 h) compared with most other PIs [16].In addition, previous pharmacokinetic studies have dem-onstrated that exposure to nelfinavir can be increased bycoadministration of low-dose ritonavir (100–400 mgBID) [21, 22]. In these studies, ritonavir also increasedM8 concentrations, as well as the M8:nelfinavir ratio,enhancing the relative contribution of M8 to the antiviralefficacy of nelfinavir. Thus, it appeared feasible that ther-apeutic plasma concentrations of nelfinavir plus M8could be maintained over 24 h after once-daily adminis-tration of nelfinavir and ritonavir.
With respect to the tolerability of such a once-dailyregimen, it appeared advantageous that no clear relation-ship has been demonstrated between the adverse effectsof nelfinavir and its plasma concentration, particularly
C
max
[23, 24].
Therefore this study was performed to characterize thesteady-state pharmacokinetics and short-term tolerabilityof possible once-daily nelfinavir/ritonavir combinations.We also evaluated whether ingestion with a light mealwould permit adequate absorption of these combinations.
Methods
Subjects
Male or female healthy volunteers, aged 18–65 years,were eligible for enrolment. Subjects were excluded ifthey were hepatitis B- or C-seropositive, pregnant,hypersensitive to PIs or loperamide, if they had positiveserology for HIV infection or prespecified abnormal lab-oratory parameters, and if they were taking any medica-tion or illicit drugs.
All subjects gave written informed consent after fullexplanation of the study details. The study was approvedby the Institutional Review Board of University MedicalCentre Nijmegen, The Netherlands.
Study design and procedures
This study had an open-label, randomized, multiple-dose, parallel-group design. Twenty-seven volunteerswere randomized (stratified by gender) to three dosagegroups.
Participants took once-daily doses of either 2000 mgnelfinavir plus 200 mg ritonavir (group 1), 2000 mgnelfinavir plus 400 mg ritonavir (group 2), or2500 mg nelfinavir plus 200 mg ritonavir (group 3).Nelfinavir (Viracept
®
) was administered as film-coatedtablets, each containing 250 mg. Ritonavir (Norvir
®
) wasgiven as capsules containing 100 mg.
Nelfinavir and ritonavir in all three combinations wereingested concomitantly with food (at least two slices ofbread) at 24-h intervals and for 14 days.
Participants in the 2000/400 mg group (group 2)started with a 4-day lead-in period of 300 mg (insteadof 400 mg) ritonavir combined with nelfinavir in orderto attenuate possible ritonavir-associated adverse eventsin the initial period of the study [9].
Blood samples for two consecutive 24-h pharmacoki-netic profiles were collected on study days 15 and 16.Participants attended in the morning after an overnightfast and a predose blood sample was drawn. On day 15they ingested nelfinavir and ritonavir with a standardized,full breakfast, which consisted of 130 ml water and fourslices of bread, filled with butter plus cheese, ham, pasteor jam (610 kcal: 33% fat, 16% proteins and 51% carbo-hydrates). Blood samples were drawn at 0.5, 1.0, 1.5, 2.0,2.5, 3.0, 4.0, 5.0, 6.0, 7.0, 8.0, 10.0, 12.0, 16.0 and24.0 h postdose. Plasma was isolated by centrifugation

Once-daily nelfinavir/ritonavir
© 2003 Blackwell Science Ltd
Br J Clin Pharmacol
,
55
, 115–125
117
within 12 h of sampling and was stored at
-
20
∞
C untilanalysis.
After an overnight fast, the same procedure wasrepeated on day 16. However, the drugs were ingestedwith a light instead of a full breakfast. This comprisedone slice of bread with butter and cheese and 130 ml ofsemiskimmed milk (271 kcal: 37% fat, 24% proteins, 39%carbohydrates).
The study was conducted on an outpatient basis. Sub-jects received their study medication in a vial that con-tained sealed plastic sachets, each holding the appropriatenumber of tablets and capsules for 1 day. Drug adminis-tration was witnessed on days 1, 4, 11, 15 and 16.Compliance with study medication at home was verifiedat every study visit by inspection of drug-taking diaries,counting of sachets, measurement of plasma drug con-centrations, and electronic monitoring of opening ofvials, using the Medication Event Monitoring System(MEMS
®
) [25].
Drug analysis
Nelfinavir and ritonavir concentrations were assayedusing a previously described validated reversed-phaseHPLC method with u.v. detection [26]. M8 concentra-tions were determined simultaneously using the samemethod without modifications. The retention time ofM8 was 12.7 min. The accuracy of the method for nelfi-navir ranged from 96% to 100%, depending on the con-centration. Those for ritonavir and M8 were 102–108%and 93–108%, respectively. Intra-day precision andbetween-day precision were 2.1–7.5% and 0.4–3.5% fornelfinavir, 2.0–8.1% and 0–2.4% for ritonavir, and 2.8–4.3% and 2.0–3.0% for M8. The limit of determinationwas 0.04 mg l
-
1
for nelfinavir, ritonavir and M8.
Pharmacokinetic analysis
Pharmacokinetic parameters for nelfinavir, ritonavir andM8 were obtained by noncompartmental methods [27].The highest observed plasma concentration was definedas
C
max
, with the corresponding sampling time as
t
max
.
C
min
was the concentration at 24 h after ingestion of thedrugs. The terminal, log-linear period (log
C vs t
) wasdefined by visual inspection of the last data points (
n
≥
3).The value of the slope (–
b
/2.303) was calculated by least-squares linear regression analysis, where
b
is the first-order elimination rate constant. The elimination half life(
t
1/2
) was calculated from the expression 0.693/
b
.The area under the concentration
vs
time curve(
AUC
24h
) was calculated using the trapezoidal rule from0 to 24 h. The time of ingestion of nelfinavir/ritonaviron day 14 (the day preceding pharmacokinetic assess-ments) varied among participants, resulting in different
contributions of this dose to the
AUC
24h
on day 15.Therefore
AUC
24h
values for study day 15 were correctedfor the contribution of the previous dose by subtractionof
C
0
/
b
(where
C
0
is the concentration just before inges-tion of nelfinavir/ritonavir at
t
=
0), and area under thecurve was extrapolated to infinity by adding
C
min
/
b
.Accordingly, the corrected
AUC
24h
value (
AUC
24h,corr
) forday 15 was obtained from the equation:
AUC
24h,corr
=
AUC
24h
-
C
0
/
b
day15
+
C
min
/
b
day15
.
The
AUC
24h
for day 16 was corrected in the same way,but the contribution of the predose AUC was calculatedusing the elimination rate constant
b
determined on day15:
AUC
24h,corr
=
AUC
24h
-
C
0
/
b
day15 + Cmin/bday16.
Apparent clearance (CL/F, where F is bioavailability) wascalculated by dividing dose (D) by AUC24h,corr, and appar-ent volume of distribution (Vd/F) was obtained by divid-ing CL/F by b. Both were corrected for weight.
Safety and tolerability
Safety and tolerability were assessed by a questionnairethat described 15 possible adverse events that could occurduring treatment with nelfinavir or ritonavir. The ques-tionnaire was completed four times each, on study days4, 8, 11 and 15. Participants were asked to grade everyevent as mild (symptoms do not interfere with dailyactivities), moderate (symptoms interfere with daily activ-ities) or severe (symptoms markedly interrupt daily activ-ities). An extensive blood chemistry and haematologyscreen and urinalysis were performed on the same fourstudy days. If WHO grade 2 diarrhoea occurred, use ofloperamide was allowed.
Data analysis
The study was not powered to enable formal statisticalcomparisons of pharmacokinetic parameters between thestudy groups. Therefore pharmacokinetic parameters arepresented descriptively for each study group.
To assess the effect of the composition of the concur-rent meal on the pharmacokinetics of nelfinavir, M8,nelfinavir plus M8, and ritonavir, a two-way mixedanalysis of variance (ANOVA) was performed on the log-arithmically transformed values of AUC24h,corr, Cmax andCmin. Absence of an effect of the meal composition onAUC24h,corr, Cmax or Cmin was concluded if the 90% CIfor a geometric mean ratio was contained within 80–125% limits [28]. Tmax values were not log-transformedand were compared using the Wilcoxon signed-rankstest.
The incidence of adverse events was expressed as the
R. E. Aarnoutse et al.
118 © 2003 Blackwell Science Ltd Br J Clin Pharmacol, 55, 115–125
percentage of participants who reported a particular eventat least once. Consequently every reported mild, moder-ate or severe adverse event was assigned a severity scoreof 1, 2 or 3 points, respectively. Scores were added upfor each participant and were divided by the number ofeach subject. In this way mean toxicity scores over thestudy period were obtained.
All statistical evaluations were performed with SPSSfor Windows, version 10.0 (SPSS Inc., Chicago, IL,USA).
Results
Twenty-seven volunteers were enrolled into the study.Five male and four female subjects were included in eachgroup. Median ages were 28, 23 and 25 years in groups1, 2, and 3, respectively, and median weights were 71,73 and 71 kg. All subjects were Caucasians.
Twenty-one volunteers completed the study and data
for 20 volunteers were evaluated (eight in group 1, eightin group 2 and four in group 3).
One subject in group 1, one in group 2 and three ingroup 3 were withdrawn because of toxicity concerns.An additional volunteer in group 3 withdrew hisinformed consent. One subject in group 3 did not con-vert nelfinavir to M8, probably because of CYP2C19poor metabolizer genotype status, which occurs in 3–5%of Caucasian subjects [18]. Because of this, pharmacok-inetic data for this volunteer were not analysed, whichreduced the number of evaluable participants in group 3to four.
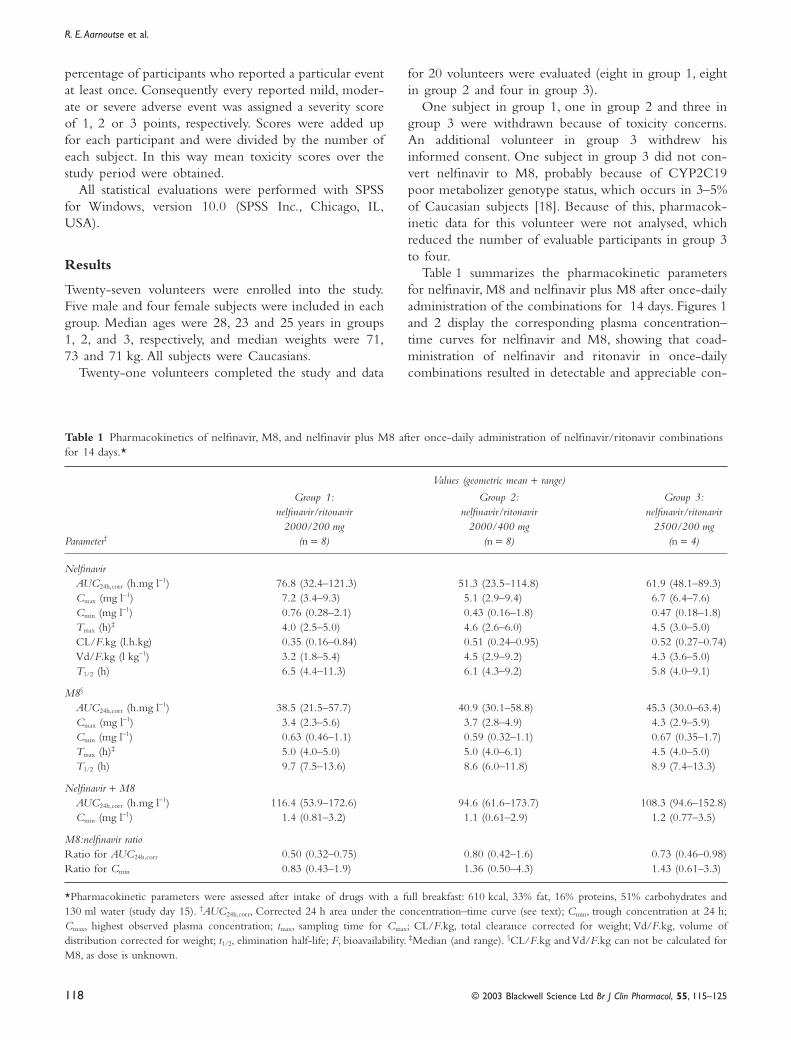
Table 1 summarizes the pharmacokinetic parametersfor nelfinavir, M8 and nelfinavir plus M8 after once-dailyadministration of the combinations for 14 days. Figures 1and 2 display the corresponding plasma concentration–time curves for nelfinavir and M8, showing that coad-ministration of nelfinavir and ritonavir in once-dailycombinations resulted in detectable and appreciable con-
Table 1 Pharmacokinetics of nelfinavir, M8, and nelfinavir plus M8 after once-daily administration of nelfinavir/ritonavir combinations for 14 days.*
Parameter†
Values (geometric mean + range)
Group 1:nelfinavir/ritonavir
2000/200 mg(n = 8)
Group 2:nelfinavir/ritonavir
2000/400 mg(n = 8)
Group 3:nelfinavir/ritonavir
2500/200 mg(n = 4)
NelfinavirAUC24h,corr (h.mg l-1) 76.8 (32.4–121.3) 51.3 (23.5–114.8) 61.9 (48.1–89.3)Cmax (mg l-1) 7.2 (3.4–9.3) 5.1 (2.9–9.4) 6.7 (6.4–7.6)Cmin (mg l-1) 0.76 (0.28–2.1) 0.43 (0.16–1.8) 0.47 (0.18–1.8)Tmax (h)‡ 4.0 (2.5–5.0) 4.6 (2.6–6.0) 4.5 (3.0–5.0)CL/F.kg (l.h.kg) 0.35 (0.16–0.84) 0.51 (0.24–0.95) 0.52 (0.27–0.74)Vd/F.kg (l kg-1) 3.2 (1.8–5.4) 4.5 (2.9–9.2) 4.3 (3.6–5.0)T1/2 (h) 6.5 (4.4–11.3) 6.1 (4.3–9.2) 5.8 (4.0–9.1)
M8§
AUC24h,corr (h.mg l-1) 38.5 (21.5–57.7) 40.9 (30.1–58.8) 45.3 (30.0–63.4)Cmax (mg l-1) 3.4 (2.3–5.6) 3.7 (2.8–4.9) 4.3 (2.9–5.9)Cmin (mg l-1) 0.63 (0.46–1.1) 0.59 (0.32–1.1) 0.67 (0.35–1.7)Tmax (h)‡ 5.0 (4.0–5.0) 5.0 (4.0–6.1) 4.5 (4.0–5.0)T1/2 (h) 9.7 (7.5–13.6) 8.6 (6.0–11.8) 8.9 (7.4–13.3)
Nelfinavir + M8AUC24h,corr (h.mg l-1) 116.4 (53.9–172.6) 94.6 (61.6–173.7) 108.3 (94.6–152.8)Cmin (mg l-1) 1.4 (0.81–3.2) 1.1 (0.61–2.9) 1.2 (0.77–3.5)
M8:nelfinavir ratioRatio for AUC24h,corr 0.50 (0.32–0.75) 0.80 (0.42–1.6) 0.73 (0.46–0.98)Ratio for Cmin 0.83 (0.43–1.9) 1.36 (0.50–4.3) 1.43 (0.61–3.3)
*Pharmacokinetic parameters were assessed after intake of drugs with a full breakfast: 610 kcal, 33% fat, 16% proteins, 51% carbohydrates and130 ml water (study day 15). †AUC24h,corr, Corrected 24 h area under the concentration–time curve (see text); Cmin, trough concentration at 24 h;Cmax, highest observed plasma concentration; tmax, sampling time for Cmax; CL/F.kg, total clearance corrected for weight; Vd/F.kg, volume ofdistribution corrected for weight; t1/2, elimination half-life; F, bioavailability. ‡Median (and range). §CL/F.kg and Vd/F.kg can not be calculated forM8, as dose is unknown.
Once-daily nelfinavir/ritonavir
© 2003 Blackwell Science Ltd Br J Clin Pharmacol, 55, 115–125 119
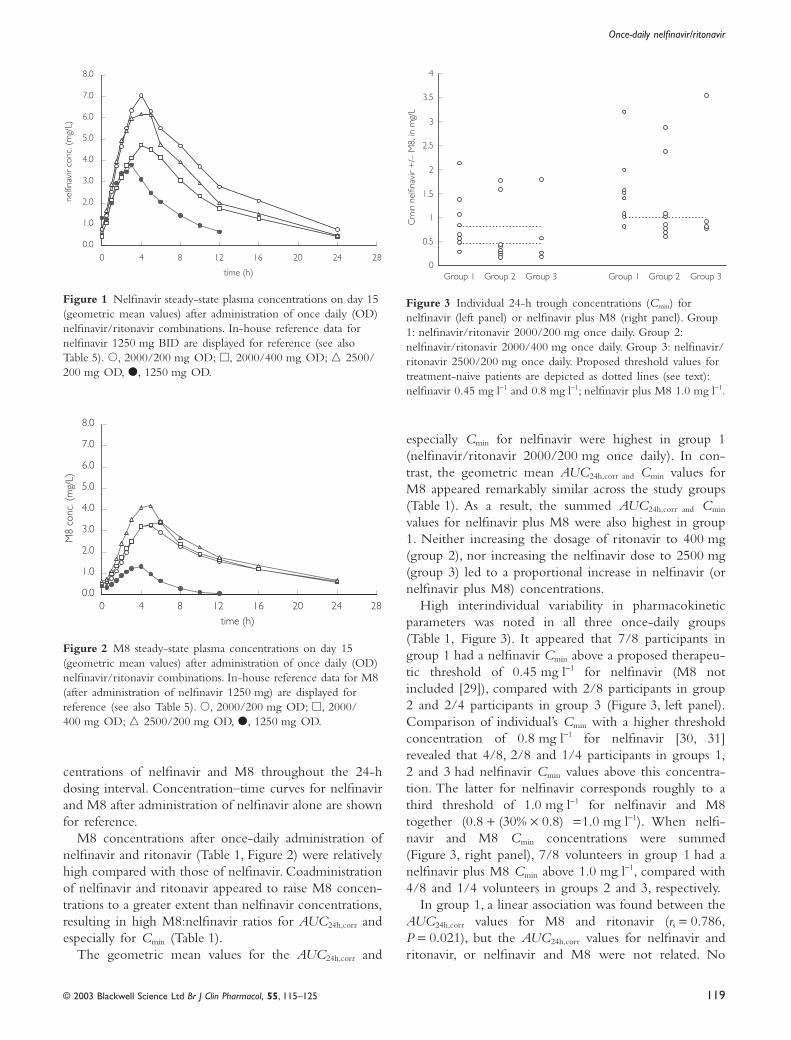
Figure 3 Individual 24-h trough concentrations (Cmin) for nelfinavir (left panel) or nelfinavir plus M8 (right panel). Group 1: nelfinavir/ritonavir 2000/200 mg once daily. Group 2: nelfinavir/ritonavir 2000/400 mg once daily. Group 3: nelfinavir/ritonavir 2500/200 mg once daily. Proposed threshold values for treatment-naive patients are depicted as dotted lines (see text): nelfinavir 0.45 mg l-1 and 0.8 mg l-1; nelfinavir plus M8 1.0 mg l-1.
Group 1 Group 2
Cm
in n
elfin
avir
+/–
M8,
in m
g/L
Group 3 Group 1 Group 2 Group 30
0.5
1
1.5
2
2.5
3
3.5
4
Figure 1 Nelfinavir steady-state plasma concentrations on day 15 (geometric mean values) after administration of once daily (OD) nelfinavir/ritonavir combinations. In-house reference data for nelfinavir 1250 mg BID are displayed for reference (see also Table 5). �, 2000/200 mg OD; �, 2000/400 mg OD; � 2500/200 mg OD, �, 1250 mg OD.
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
0 4 8 12 16 20 24 28
time (h)
nelfi
navi
r co
nc. (
mg/
L)
centrations of nelfinavir and M8 throughout the 24-hdosing interval. Concentration–time curves for nelfinavirand M8 after administration of nelfinavir alone are shownfor reference.
M8 concentrations after once-daily administration ofnelfinavir and ritonavir (Table 1, Figure 2) were relativelyhigh compared with those of nelfinavir. Coadministrationof nelfinavir and ritonavir appeared to raise M8 concen-trations to a greater extent than nelfinavir concentrations,resulting in high M8:nelfinavir ratios for AUC24h,corr andespecially for Cmin (Table 1).
The geometric mean values for the AUC24h,corr and
especially Cmin for nelfinavir were highest in group 1(nelfinavir/ritonavir 2000/200 mg once daily). In con-trast, the geometric mean AUC24h,corr and Cmin values forM8 appeared remarkably similar across the study groups(Table 1). As a result, the summed AUC24h,corr and Cmin
values for nelfinavir plus M8 were also highest in group1. Neither increasing the dosage of ritonavir to 400 mg(group 2), nor increasing the nelfinavir dose to 2500 mg(group 3) led to a proportional increase in nelfinavir (ornelfinavir plus M8) concentrations.
High interindividual variability in pharmacokineticparameters was noted in all three once-daily groups(Table 1, Figure 3). It appeared that 7/8 participants ingroup 1 had a nelfinavir Cmin above a proposed therapeu-tic threshold of 0.45 mg l-1 for nelfinavir (M8 notincluded [29]), compared with 2/8 participants in group2 and 2/4 participants in group 3 (Figure 3, left panel).Comparison of individual’s Cmin with a higher thresholdconcentration of 0.8 mg l-1 for nelfinavir [30, 31]revealed that 4/8, 2/8 and 1/4 participants in groups 1,2 and 3 had nelfinavir Cmin values above this concentra-tion. The latter for nelfinavir corresponds roughly to athird threshold of 1.0 mg l-1 for nelfinavir and M8together (0.8 + (30% ¥ 0.8) =1.0 mg l-1). When nelfi-navir and M8 Cmin concentrations were summed(Figure 3, right panel), 7/8 volunteers in group 1 had anelfinavir plus M8 Cmin above 1.0 mg l-1, compared with4/8 and 1/4 volunteers in groups 2 and 3, respectively.
In group 1, a linear association was found between theAUC24h,corr values for M8 and ritonavir (rs = 0.786,P = 0.021), but the AUC24h,corr values for nelfinavir andritonavir, or nelfinavir and M8 were not related. No
Figure 2 M8 steady-state plasma concentrations on day 15 (geometric mean values) after administration of once daily (OD) nelfinavir/ritonavir combinations. In-house reference data for M8 (after administration of nelfinavir 1250 mg) are displayed for reference (see also Table 5). �, 2000/200 mg OD; �, 2000/400 mg OD; � 2500/200 mg OD, �, 1250 mg OD.
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
8.0
0 4 8 12 16 20 24 28time (h)
M8
conc
. (m
g/L)

R. E. Aarnoutse et al.
120 © 2003 Blackwell Science Ltd Br J Clin Pharmacol, 55, 115–125
corresponding associations were found in group 2. Cor-relation analyses were not performed for group 3,because of the small number of participants.
The geometric mean AUC24h,corr, Cmin and Cmax forritonavir in groups 1 and 3 (200 mg of ritonavir oncedaily) were comparable (Table 2). Increasing the dose ofritonavir from 200 mg to 400 mg (group 2) resulted ina more than proportional increase in the AUC24h,corr forritonavir. The latter in group 2 was significantly higherthan that in groups 1 and 3 (P £ 0.001).
A significant effect of meal composition on theAUC24h,corr and Cmin values for nelfinavir and nelfinavirplus M8 was found. No significant differences betweenstudy groups could be demonstrated for these parametersand the interaction between study group and meal com-position was never significant.
The geometric mean ratios (light/full breakfast) and90% CI were 0.70 (0.62–0.78) and 0.76 (0.68–0.85) fornelfinavir AUC24h,corr and Cmin, respectively, and 0.71(0.63–0.81) and 0.76 (0.67–0.86) for the AUC24h,corr andCmin of nelfinavir plus M8 (data from all three groupscombined).
As the lack of significant between-group differencesand the lack of an group-by-period interaction could beattributable to the small number of participants in eachgroup, Table 3 shows geometric mean ratios and CIs foreach of the study groups separately. The statistical powerto detect a relevant food effect was low (about 0.5) ingroup 3, due to the small number of participants. Thisimplies that the absence of a significant food effect forsome pharmacokinetic parameters in this group (seeTable 3) does not exclude the existence of such an effect.
With respect to ritonavir, it appeared that theAUC24h,corr in group 2 (400 mg of ritonavir) was not
significantly affected by the composition of the breakfast,in contrast to the findings in groups 1 and 3 (200 mg ofritonavir).
Safety and tolerability
Five volunteers were withdrawn because of concernsover toxicity. Three of these (one in each study group)suffered a mild rash. A second subject in group 3 waswithdrawn as a precautionary measure, as he complainedof, for example, localized itch, feeling of thick lips, butshowed no objective sign of toxicity. A third subject ingroup 3 was withdrawn because of severe fatigue (WHOgrade 3 toxicity) after 11 days of nelfinavir/ritonavir.One day after stopping the medication, increased livertransaminases were found in this subject (AST grade 2,ALT grade 3 toxicities), but these readings normalized inthe next 3 weeks.
Apart from these events, the nelfinavir/ritonavir regi-mens were tolerated reasonably well. The most commonadverse reactions are shown in Table 4.
Median toxicity scores were 1.5, 2.5 and 3.1 in studygroups 1, 2 and 3, respectively. This means that subjectsin group 1 had an average of 1.5 mild adverse events. Nosignificant correlations were found between the toxicityscores and the AUC24h,corr, Cmax or Cmin of nelfinavir,nelfinavir plus M8, or ritonavir.
Small increases in fasting cholesterol were observed inthe majority of participants who completed the study (6/8, 6/8 and 2/4 participants in groups 1, 2 and 3, respec-tively). Median changes in cholesterol were +0.50, +0.25and 0.0 mmol l-1 in groups 1, 2 and 3, whereas medianchanges in triglycerides were negligible (+0.04, +0.04and +0.16 mmol l-1 in groups 1, 2 and 3). The study
Table 2 Pharmacokinetics of ritonavir after once daily administration of nelfinavir/ritonavir combinations for 14 days.*
Values (geometric mean + range)
Parameter†
Group 1:nelfinavir/ritonavir
2000/200 mg(n = 8)
Group 2:nelfinavir/ritonavir
2000/400 mg(n = 8)
Group 3: nelfinavir/ritonavir
2500/200 mg (n = 4)
RitonavirAUC24h,corr (h.mg l-1) 12.2 (8.2–18.3) 32.4 (14.0–53.7) 11.8 (7.9–23.4)Cmax (mg l-1) 1.7 (1.1–2.9) 4.0 (2.3–5.7) 1.8 (1.2–3.9)Cmin (mg l-1) 0.04 (0.00–0.12) 0.15 (0.06–0.24) 0.04 (0.02–0.13)tmax (h)‡ 4.0 (2.0–5.0) 4.1 (1.0–6.0) 5.0 (1.5–5.0)CL/F.kg (l.h.kg) 0.22 (0.16–0.35) 0.15 (0.06–0.30) 0.22 (0.12–0.37)Vd/F.kg (l kg-1) 1.1 (0.58–1.5) 0.95 (0.32–2.2) 1.3 (0.62–2.6)t1/2 (h) 3.4 (2.4–5.7) 4.4 (3.7–7.0) 4.1 (2.7–5.4)
*Pharmacokinetic parameters were assessed after intake of drugs with a full breakfast: 610 kcal, 33% fat, 16% proteins, 51% carbohydrates and130 ml water (study day 15). †Abbreviations of pharmacokinetic parameters: see Table 1. ‡Median (and range).
Once-daily nelfinavir/ritonavir
© 2003 Blackwell Science Ltd Br J Clin Pharmacol, 55, 115–125 121
medication had no material effect on other laboratoryparameters.
Discussion
The results of this study suggest it is possible to achieveeffective exposure to nelfinavir and M8 after once-dailydosing of nelfinavir in combination with low-doseritonavir. These data are in agreement with results froma similar study, presented in abstract [32]. A nelfinavir-based HAART regimen with once-daily dosing for alldrugs is simple and also facilitates witnessed therapy ofHAART. Both these advantages may result in improvedlong-term adherence [6–8], which is associated withimproved efficacy of HAART [4, 5]. Once-daily admin-istration of HAART may be particularly useful for asubgroup of patients who cannot adhere to more com-plex drug regimens, due to unstable lifestyles, imprison-ment, or injectable drug misuse.
Whereas once-daily administration of nelfinavir may
prove more convenient, the number of tablets that needto be taken and food restrictions still make a once-dailyregimen quite complex. The proposed development of625-mg tablets of nelfinavir will enable further simplifi-cation of the regimen. With respect to food restrictions,once-daily administration offers patients the flexibility toadapt dosing to their dietary habits, assuming that thepharmacokinetics of nelfinavir/ritonavir do not changewith the time of dosing.
It is important not to over-interpret the apparent phar-macokinetic differences or similarities between the threenelfinavir/ritonavir regimens in this exploratory study.Each study group comprised a relatively small number ofparticipants, and considerable interindividual variabilitywas observed for all pharmacokinetic parameters. Thenumber of participants who completed group 3 of thestudy was particularly small (n = 4). Therefore, no firmconclusions can be drawn with regard to the nelfinavir/ritonavir 2500/200 mg combination.
Comparison of Table 1 and Table 5 reveals that the
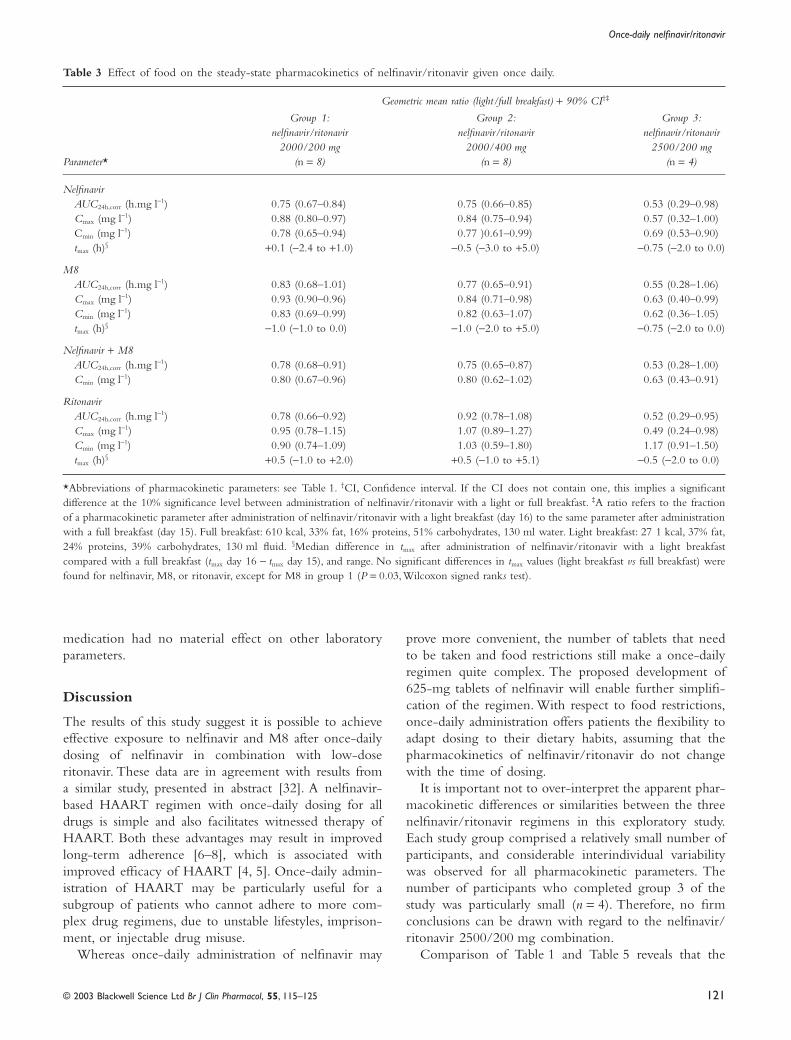
Table 3 Effect of food on the steady-state pharmacokinetics of nelfinavir/ritonavir given once daily.
Parameter*
Geometric mean ratio (light/full breakfast) + 90% CI†‡
Group 1:nelfinavir/ritonavir
2000/200 mg(n = 8)
Group 2:nelfinavir/ritonavir
2000/400 mg(n = 8)
Group 3: nelfinavir/ritonavir
2500/200 mg (n = 4)
NelfinavirAUC24h,corr (h.mg l-1) 0.75 (0.67–0.84) 0.75 (0.66–0.85) 0.53 (0.29–0.98)Cmax (mg l-1) 0.88 (0.80–0.97) 0.84 (0.75–0.94) 0.57 (0.32–1.00)Cmin (mg l-1) 0.78 (0.65–0.94) 0.77 )0.61–0.99) 0.69 (0.53–0.90)tmax (h)§ +0.1 (-2.4 to +1.0) -0.5 (-3.0 to +5.0) -0.75 (-2.0 to 0.0)
M8AUC24h,corr (h.mg l-1) 0.83 (0.68–1.01) 0.77 (0.65–0.91) 0.55 (0.28–1.06)Cmax (mg l-1) 0.93 (0.90–0.96) 0.84 (0.71–0.98) 0.63 (0.40–0.99)Cmin (mg l-1) 0.83 (0.69–0.99) 0.82 (0.63–1.07) 0.62 (0.36–1.05)tmax (h)§ -1.0 (-1.0 to 0.0) -1.0 (-2.0 to +5.0) -0.75 (-2.0 to 0.0)
Nelfinavir + M8AUC24h,corr (h.mg l-1) 0.78 (0.68–0.91) 0.75 (0.65–0.87) 0.53 (0.28–1.00)Cmin (mg l-1) 0.80 (0.67–0.96) 0.80 (0.62–1.02) 0.63 (0.43–0.91)
RitonavirAUC24h,corr (h.mg l-1) 0.78 (0.66–0.92) 0.92 (0.78–1.08) 0.52 (0.29–0.95)Cmax (mg l-1) 0.95 (0.78–1.15) 1.07 (0.89–1.27) 0.49 (0.24–0.98)Cmin (mg l-1) 0.90 (0.74–1.09) 1.03 (0.59–1.80) 1.17 (0.91–1.50)tmax (h)§ +0.5 (-1.0 to +2.0) +0.5 (-1.0 to +5.1) -0.5 (-2.0 to 0.0)
*Abbreviations of pharmacokinetic parameters: see Table 1. †CI, Confidence interval. If the CI does not contain one, this implies a significantdifference at the 10% significance level between administration of nelfinavir/ritonavir with a light or full breakfast. ‡A ratio refers to the fractionof a pharmacokinetic parameter after administration of nelfinavir/ritonavir with a light breakfast (day 16) to the same parameter after administrationwith a full breakfast (day 15). Full breakfast: 610 kcal, 33% fat, 16% proteins, 51% carbohydrates, 130 ml water. Light breakfast: 27 1 kcal, 37% fat,24% proteins, 39% carbohydrates, 130 ml fluid. §Median difference in tmax after administration of nelfinavir/ritonavir with a light breakfastcompared with a full breakfast (tmax day 16 - tmax day 15), and range. No significant differences in tmax values (light breakfast vs full breakfast) werefound for nelfinavir, M8, or ritonavir, except for M8 in group 1 (P = 0.03, Wilcoxon signed ranks test).

R. E. Aarnoutse et al.
122 © 2003 Blackwell Science Ltd Br J Clin Pharmacol, 55, 115–125
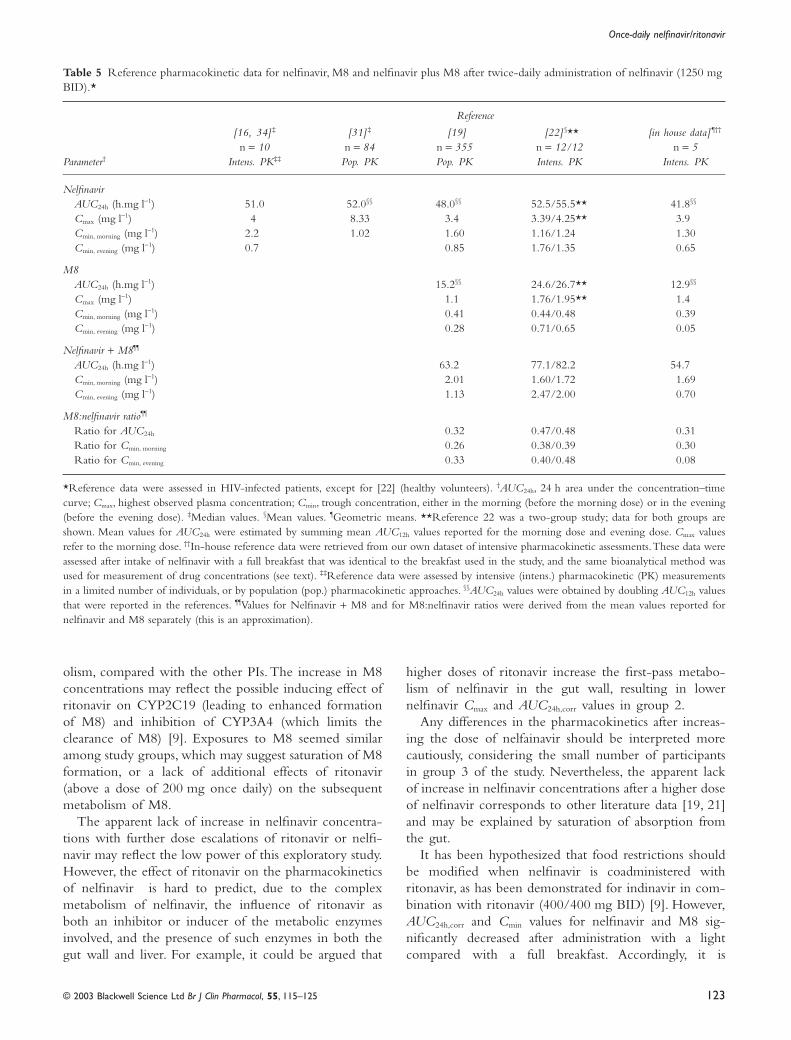
geometric mean AUC24h,corr values for once-daily nelfi-navir are similar to values reported for the approved BIDregimen, and are considerably higher when the contri-bution of M8 is included. Therefore efficacy is predictedfor all three once-daily regimens. In contrast, only group1 (nelfinavir/ritonavir 2000/200 mg once daily) yieldeda geometric mean 24-h Cmin value for nelfinavir that wascomparable to the lowest 12-h Cmin values reported forthe BID regimen. When M8 concentrations are takeninto consideration, the mean 24-h Cmin values in allgroups are comparable to reference data, with group 1showing the most favourable results.
Comparing experimental data to reference data couldbe confounded by differences across studies. The currentstudy was performed in healthy volunteers, whereas mostreference data are from HIV-infected patients. No sub-stantial differences in nelfinavir pharmacokinetics havebeen observed between these two groups [16], but theycan not be excluded. Differences in the composition ofmeals taken with nelfinavir as well as different analyticalmethods could also confound interpretation of its phar-macokinetic parameters. Our in-house reference data(Table 5) were obtained using the same breakfast contentand the same bioanalytical method as in the currentstudy. Thirdly, some reference AUC12h values reported for
the BID regimen were doubled to enable comparisonwith once-daily AUC24h,corr values. However, this neglectsrelatively modest circadian variations that occur in thepharmacokinetics of nelfinavir.
The 0.45 mg l-1 (800 nM) threshold for nelfinavir isbased upon in vitro 95% effective concentrations againstHIV, with adjustment for in vivo protein binding and theelevated concentrations of a1-acid glycoprotein in HIV-infected patients [29]. Thresholds derived from in vivopatient response data may be more relevant, and the0.8 mg l-1 value defined for wild-type HIV-1 (ie intreatment-naive patients) has been independently assessedin two patient cohorts [30, 31]. This threshold corre-sponds to about 1.0 mg l-1 when the Cmin values of nelfi-navir and M8 are summed. Regardless of the thresholdchosen and the inclusion or exclusion of M8 concentra-tions, the 2000/200 mg regimen (group 1) appeared tobe the most favourable. As this combination was alsoassociated with the lowest toxicity score, it appears to bean appropriate regimen for further evaluation.
The boosting effect of ritonavir on nelfinavirAUC24h,corr values appears less pronounced than thoseseen after addition of ritonavir to indinavir and especiallysaquinavir therapy. This could be explained by the rela-tively small contribution of CYP3A to nelfinavir metab-
Table 4 Adverse events: incidence and toxicity scores.*
Adverse event
Study group
Group 1:nelfinavir/ritonavir
2000/200 mg (n = 9)
Group 2:nelfinavir/ritonavir
2000/400 mg(n = 9)
Group 3: nelfinavir/ritonavir
2500/200 mg(n = 8)*
All groups:(n = 26)
Incidence (any severity)†
Diarrhoea 100 78 50 77Flatulence 56 78 38 58Nausea 11 56 25 31Vomiting 0 11 25 12Abdominal pain 22 44 50 38Asthenia 11 22 38 23Fatigue/somnolence 22 56 75 50Fever 0 0 13 4Headache 56 33 25 38Skin reaction or rash 22 33 63 38Taste perversion 11 11 25 15Peroral paraesthesia 33 11 13 19Peripheral paraesthesia 22 22 13 19Arthralgia 22 22 25 23Myalgia 11 22 13 15
Median severity score‡ 1.5 2.5 3.1 2.4
*Data are from all participants, including those who withdrew. One participant in group 3 withdrew informed consent before taking the drugs andbefore the first evaluation of adverse events. †Incidence expressed as the percentage of participants who reported a particular adverse event at leastonce. ‡A severity score of 3.0 represents three mild adverse events, or one moderate adverse event (2 points) plus a mild one, or one severe adverseevent (3 points).
Once-daily nelfinavir/ritonavir
© 2003 Blackwell Science Ltd Br J Clin Pharmacol, 55, 115–125 123
olism, compared with the other PIs. The increase in M8concentrations may reflect the possible inducing effect ofritonavir on CYP2C19 (leading to enhanced formationof M8) and inhibition of CYP3A4 (which limits theclearance of M8) [9]. Exposures to M8 seemed similaramong study groups, which may suggest saturation of M8formation, or a lack of additional effects of ritonavir(above a dose of 200 mg once daily) on the subsequentmetabolism of M8.
The apparent lack of increase in nelfinavir concentra-tions with further dose escalations of ritonavir or nelfi-navir may reflect the low power of this exploratory study.However, the effect of ritonavir on the pharmacokineticsof nelfinavir is hard to predict, due to the complexmetabolism of nelfinavir, the influence of ritonavir asboth an inhibitor or inducer of the metabolic enzymesinvolved, and the presence of such enzymes in both thegut wall and liver. For example, it could be argued that
higher doses of ritonavir increase the first-pass metabo-lism of nelfinavir in the gut wall, resulting in lowernelfinavir Cmax and AUC24h,corr values in group 2.
Any differences in the pharmacokinetics after increas-ing the dose of nelfainavir should be interpreted morecautiously, considering the small number of participantsin group 3 of the study. Nevertheless, the apparent lackof increase in nelfinavir concentrations after a higher doseof nelfinavir corresponds to other literature data [19, 21]and may be explained by saturation of absorption fromthe gut.
It has been hypothesized that food restrictions shouldbe modified when nelfinavir is coadministered withritonavir, as has been demonstrated for indinavir in com-bination with ritonavir (400/400 mg BID) [9]. However,AUC24h,corr and Cmin values for nelfinavir and M8 sig-nificantly decreased after administration with a lightcompared with a full breakfast. Accordingly, it is
Table 5 Reference pharmacokinetic data for nelfinavir, M8 and nelfinavir plus M8 after twice-daily administration of nelfinavir (1250 mg BID).*
Parameter†
Reference
[16, 34] ‡
n = 10Intens. PK‡‡
[31] ‡
n = 84Pop. PK
[19]n = 355Pop. PK
[22] §**n = 12/12Intens. PK
[in house data] ¶†† n = 5
Intens. PK
NelfinavirAUC24h (h.mg l-1) 51.0 52.0§§ 48.0§§ 52.5/55.5** 41.8§§
Cmax (mg l-1) 4 8.33 3.4 3.39/4.25** 3.9Cmin, morning (mg l-1) 2.2 1.02 1.60 1.16/1.24 1.30Cmin, evening (mg l-1) 0.7 0.85 1.76/1.35 0.65
M8AUC24h (h.mg l-1) 15.2§§ 24.6/26.7** 12.9§§
Cmax (mg l-1) 1.1 1.76/1.95** 1.4Cmin, morning (mg l-1) 0.41 0.44/0.48 0.39Cmin, evening (mg l-1) 0.28 0.71/0.65 0.05
Nelfinavir + M8¶¶
AUC24h (h.mg l-1) 63.2 77.1/82.2 54.7Cmin, morning (mg l-1) 2.01 1.60/1.72 1.69Cmin, evening (mg l-1) 1.13 2.47/2.00 0.70
M8:nelfinavir ratio¶¶
Ratio for AUC24h 0.32 0.47/0.48 0.31Ratio for Cmin, morning 0.26 0.38/0.39 0.30Ratio for Cmin, evening 0.33 0.40/0.48 0.08
*Reference data were assessed in HIV-infected patients, except for [22] (healthy volunteers). †AUC24h, 24 h area under the concentration–timecurve; Cmax, highest observed plasma concentration; Cmin, trough concentration, either in the morning (before the morning dose) or in the evening(before the evening dose). ‡Median values. §Mean values. ¶Geometric means. **Reference 22 was a two-group study; data for both groups areshown. Mean values for AUC24h were estimated by summing mean AUC12h values reported for the morning dose and evening dose. Cmax valuesrefer to the morning dose. ††In-house reference data were retrieved from our own dataset of intensive pharmacokinetic assessments. These data wereassessed after intake of nelfinavir with a full breakfast that was identical to the breakfast used in the study, and the same bioanalytical method wasused for measurement of drug concentrations (see text). ‡‡Reference data were assessed by intensive (intens.) pharmacokinetic (PK) measurementsin a limited number of individuals, or by population (pop.) pharmacokinetic approaches. §§AUC24h values were obtained by doubling AUC12h valuesthat were reported in the references. ¶¶Values for Nelfinavir + M8 and for M8:nelfinavir ratios were derived from the mean values reported fornelfinavir and M8 separately (this is an approximation).

R. E. Aarnoutse et al.
124 © 2003 Blackwell Science Ltd Br J Clin Pharmacol, 55, 115–125
recommended that once-daily regimens of nelfinavir/ritonavir are administered with a meal comparable incalories (~600 kcal) and fat content (~33%) to the fullbreakfast used in this study.
The spectrum of adverse events was as expected. Milddiarrhoea is a common adverse effect of both nelfinavirand ritonavir. The incidence of rash in this study (11%)was higher than the 3% value reported for phase IIIstudies in which nelfinavir was administered withoutritonavir [29]. The occurrence requires close study whenonce-daily nelfinavir/ritonavir regimens are tested inHIV-infected patients.
The observed increases in cholesterol values warrantclose monitoring of blood lipids when the nelfinavir/ritonavir regimen is used in HIV-infected patients, espe-cially if combined with other antiretroviral agents withknown lipid-elevating effects.
In conclusion, data from this study demonstrate thatcoadministration of nelfinavir and low-dose ritonaviroffers the potential for once-daily administration of nelfi-navir. A once-daily regimen of 2000 mg nelfinavir and200 mg ritonavir seems appropriate for further evalua-tion. This regimen should be taken with a meal con-taining at least 600 kcal. Short-term tolerability wassatisfactory, apart from a higher than expected incidenceof rash. Follow-up pharmacokinetic and tolerabilityassessments in HIV-infected patients are warranted toconfirm the findings of this study in healthy volunteers.
The healthy volunteers are thanked for their participation. H. terHofstede, D. Telgt, A. Bergshoeff, C. la Porte and M. de Graaffare acknowledged for their assistance during the study. The tech-nicians of the Department of Clinical Pharmacy are thanked foranalysis of the plasma samples. This study was funded by an unre-stricted grant from F. Hoffmann-La Roche Ltd.
References
1 Palella FJ Jr, Delaney KM, Moorman AC et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. N Engl J Med 1998; 338: 853–860.
2 Wit FW, van Leeuwen R, Weverling GJ et al. Outcome and predictors of failure of highly active antiretroviral therapy: one year follow-up of a cohort of human immunodeficiency type-1-infected persons. J Infect Dis 1999; 179: 790–798.
3 Deeks SG, Hecht FM, Swanson M et al. HIV RNA and CD4 cell count response to protease inhibitor therapy in an urban AIDS clinic: response to both initial and salvage therapy. AIDS 1999; 13: F35–F43.
4 Paterson DL, Swindells S, Mohr J et al. Adherence to protease inhibitor therapy and outcomes in patients with HIV infection. Ann Intern Med 2000; 133: 21–30.
5 Nieuwkerk PT, Sprangers MA, Burger DM et al. Limited patient adherence to highly active antiretroviral therapy for HIV-1 infection in an observational cohort study. Arch Intern Med 2001; 161: 1962–1968.
6 Tseng AL. Compliance issues in the treatment of HIV infection. Am J Health Syst Pharm 1998; 55: 1817–1824.
7 Stone VE, Hogan JW, Schuman P et al. Antiretroviral regimen complexity, self-reported adherence, and HIV patients’ understanding of their regimens: a survey of women in the HER study. J Acquir Immune Def Syndr 2001; 28: 124–131.
8 Stone VE. Strategies for optimizing adherence to highly active antiretroviral therapy: lessons from research and clinical practice. Clin Infect Dis 2001; 33: 865–872.
9 Hsu A, Granneman GR, Bertz RJ. Ritonavir. Clinical pharmacokinetics and interactions with other anti-HIV agents. Clin Pharmacokinet 1998; 35: 275–291.
10 Sale M, Sadler BM, Stein DS. Pharmacokinetic modeling and simulations of interaction of amprenavir and ritonavir. Antimicrob Agents Chemother 2002; 46: 746–754.
11 Burger DM, Hugen PWH, van der Ende ME et al. Once-daily indinavir plus ritonavir: preliminary results of the PIPO study. AIDS 2000; 14: 2621–2623.
12 Mole L, Schmidgall D, Holodniy M. A pilot trial of indinavir, ritonavir, didanosine, and lamivudine in a once-daily four-drug regimen for HIV-infection. J Acquir Immune Defic Syndr 2001; 27: 260–265.
13 Heeswijk van RPG, Veldkamp AI, Mulder JW et al. Once daily dosing of saquinavir and low-dose ritonavir in HIV-1-infected individuals. A pharmacokinetic pilot study. AIDS 2000; 14: F95–F99.
14 Kilby JM, Sfakianos G, Gizzi N et al. Safety and pharmacokinetics of once-daily regimens of soft-gel capsule saquinavir plus minidose ritonavir in human immunodeficiency virus-negative adults. Antimicrob Agents Chemother 2000; 44: 2672–2678.
15 Cardiello PG, van Heeswijk RP, Hassink EA et al. Simplifying protease inhibitor therapy with once-daily dosing of saquinavir soft-gelatin capsules/ritonavir (1600/100 mg): HIVNAT 001.3 study. J Acquir Immune Defic Syndr 2002; 29: 464–470.
16 Bardsley-Elliott A, Plosker GL. Nelfinavir, an update of its use in HIV infection. Drugs 2000; 59: 581–620.
17 Sandoval TM, Grettenberger HM, Zhang KE et al. Metabolism of nelfinavir mesylate, an HIV-1 protease inhibitor, by human liver microsomes and recombinant human isoforms [Abstract 1096]. 12th Annual Meeting and Exposition of the American Association of Pharmaceutical Scientists. San Francisco: , November 1998.
18 Lillibridge JH, Lee CA, Pithavala YK et al. The role of polymorphic CYP2C19 in the metabolism of nelfinavir mesylate. 12th Annual Meeting and Exposition of the American Association of Pharmaceutical Scientists. San Francisco: , November 1998 [Abstract 3035].
19 Baede-van Dijk PA, Hugen PWH, Verweij-van Wissen CPWGM et al. Analysis of variation in plasma concentrations of nelfinavir and its active metabolite M8 in HIV-positive patients. AIDS 2001; 15: 991–998.
20 Zhang KE, Wu E, Patick AK et al. Circulating metabolites of the human immunodeficiency virus protease inhibitor nelfinavir in humans: structural identification, levels in plasma, and antiviral activities. Antimicrob Agents Chemother 2001; 45: 1086–1093.
21 Flexner C. Steady–state pharmacokinetic interactions between ritonavir (RTV), nelfinavir (NFV) and the nelfinavir
Once-daily nelfinavir/ritonavir
© 2003 Blackwell Science Ltd Br J Clin Pharmacol, 55, 115–125 125
active metabolite M8 (AG1402). 12th World AIDS Conference, Geneva, 28 June to 3 July, 1998 [Abstract 42265].
22 Kurowski M, Kaeser B, Sawyer A et al. Low-dose ritonavir moderately enhances nelfinavir exposure. Clin Pharmacol Ther 2002; 72: 123–132.
23 Reijers MH, Weigel HM, Hart AA et al. Toxicity and drug exposure in a quadruple drug regimen in HIV-1 infected patients participating in the ADAM study. AIDS 2000; 14: 59–67.
24 Hsyu P, Flexner C, Chu A et al. Correlation of efficacy, nelfinavir pharmacokinetics, and diarrhea in treatment-naive HIV positive patients receiving nelfinavir, zidovudine and lamivudine. 2nd International Workshop on Clinical Pharmacology of HIV Therapy. Noordwijk: April 2–4, 2001 [Abstract 4.4].
25 Urquhart J. The electronic medication event monitor. Lessons for pharmacotherapy. Clin Pharmacokinet 1997; 32: 345–356.
26 Hugen PWH, Verweij-van Wissen CPWGM, Burger DM et al. Simultaneous determination of the HIV-protease inhibitors indinavir, nelfinavir, saquinavir and ritonavir by reversed-phase high-performance liquid chromatography. J Chrom B Biomed Sci Appl 1999; 727: 139–149.
27 Compartmental and noncompartmental pharmacokinetics. In Biopharmaceutics and Clinical Pharmacokinetics, Ed Gibaldi M. Philadelphia and London: Lea and Febiger, 1991: 14–23.
28 US Department of Health and Human Services. Food and Drug Administration. Center for Drug Evaluation and
Research. Guidance for Industry. Food-Effect Bioavailability and Fed Bioequivalence Studies: Study Design, Data Analysis, and Labeling (Draft Guidance) URL: http://www.fda.gov, accessed 2002, July 3.
29 Viraceptâ Product Monograph. Basel: Hoffmann-La Roche Ltd,
30 Burger DM, Hugen PWH, Aarnoutse RE et al. Treatment failure of nelfinavir-containing triple therapy can largely be explained by low nelfinavir plasma concentrations. AIDS 2000; 14 (S4): 258.
31 Pellegrin I, Breilh D, Montestruc F et al. Virologic response to nelfinavir-based regimens: pharmacokinetics and drug resistance mutations (VIRAPHAR study). AIDS 2002; 16: 1331–1340.
32 Hsyu PH, Lewis RH, Tran JQ et al. Pharmacokinetics (PK) of nelfinavir (NFV) after once daily dosing in combination with mini-doses of ritonavir (RTV) in healthy volunteers. XIII International AIDS Conference, Durban: July 9–14, 2000.
33 Acosta EP, Kakuda TN, Brundage RC et al. Pharmacodynamics of human immunodeficiency virus type 1 protease inhibitors. Clin Infect Dis 2000; 30 (Suppl. 2): S151–S159.
34 Johnson M, Petersen A, Johnson M et al. Comparison of BID and TID dosing of Viracept (nelfinavir, NFV) in combination with stavudine (d4T) and lamivudine (3TC). Fifth Conference on Retroviruses and Opportunistic Infections. Chicago: February 1998 [Abstract 373].
Related Documents











