Original Research Pharmacists’ counseling on oral contraceptives: A theory informed analysis Mohamed E.K. Amin, Ph.D. a, * , Betty Chewning, Ph.D., F.A.Ph.A. b a Faculty of Pharmacy, Beirut Arab University, Room 102 Hariri Building, Tareek El Jadida, Beirut, Lebanon b Sonderegger Research Center, School of Pharmacy, University of Wisconsin–Madison, Madison, WI 53705-2222, USA Abstract Background: Providing correct and complete counseling on the use of oral contraceptives (OCs) is central to securing the autonomy of women in child-bearing age and is a powerful, proven tool of social change. Pharmacists in many developing countries such as Egypt are involved in dispensing and at times prescribing pharmaceuticals, including oral contraceptives that are readily available without a prescription. Objectives: To predict Egyptian community pharmacists’ counseling on oral contraceptives while utilizing a theoretical framework guided by the Theory of Planned Behavior (TPB). Methods: A cross-sectional, self-administered survey was completed by a random sample of community pharmacists in Alexandria, Egypt to determine their attitudes and behaviors regarding counseling on OCs. Multiple regression was used to predict self-reported counseling on oral contraceptives as a function of the TPB-related constructs and six other factors – “perceived importance of profit from dispensing OCs on pharmacy revenue,” “number of hours worked,” “age,” “gender,” “pharmacy practice degree” and “marital status” of the pharmacist. Results: Of the 181 pharmacists invited to complete the survey, 168 (93%) participated. Pharmacists indicated they talked to a slightly higher proportion of women about the importance of taking OCs at the same time daily than about topics such as which day to start taking OCs, side effects and what to do when a dose of OCs was missed. Pharmacists’ reported counseling on oral contraceptives was positively associated with their perception that women welcomed pharmacist initiated OC counseling (b ¼ 0.315, P ! 0.001), perceived adequacy of time available to counsel women on OCs (b ¼ 0.290, P ¼ 0.003) and the perceived number of women who asked for their help in selecting an OC without providing a pre- scription in the past week (b ¼ 0.160, P ¼ 0.018). Pharmacists reported that women’s welcoming phar- macists initiating OC counseling was associated with the pharmacists’ reported percent who asked pharmacists for OC advice out of the last 5 women seeking OC (r ¼ 0.45; P ! 0.0001). Male pharmacists were less likely than female pharmacists to report that women welcomed pharmacist initiated OC coun- seling (r ¼0.27; P ¼ 0.0005). Conclusions: The TPB appears to help predict pharmacists’ OC counseling. There is a need to prepare pharmacists who are frequently requested to assist women with the selection of an oral contraceptive. Interventions that would facilitate women’s requests for information may be valuable to increase pharmacists’ counseling on oral contraceptives. Future qualitative and observational studies are needed * Corresponding author. E-mail address: [email protected] (M.E.K. Amin). 1551-7411/$ - see front matter Ó 2015 Elsevier Inc. All rights reserved. http://dx.doi.org/10.1016/j.sapharm.2015.08.009 Research in Social and Administrative Pharmacy j (2015) j–j

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Research in Social and
Administrative Pharmacy j (2015) j–j
Original Research
Pharmacists’ counseling on oral contraceptives:A theory informed analysis
Mohamed E.K. Amin, Ph.D.a,*, Betty Chewning, Ph.D., F.A.Ph.A.baFaculty of Pharmacy, Beirut Arab University, Room 102 Hariri Building, Tareek El Jadida, Beirut, Lebanon
bSonderegger Research Center, School of Pharmacy, University of Wisconsin–Madison, Madison, WI 53705-2222, USA
Abstract
Background: Providing correct and complete counseling on the use of oral contraceptives (OCs) iscentral to securing the autonomy of women in child-bearing age and is a powerful, proven tool of
social change. Pharmacists in many developing countries such as Egypt are involved in dispensing andat times prescribing pharmaceuticals, including oral contraceptives that are readily available without aprescription.
Objectives: To predict Egyptian community pharmacists’ counseling on oral contraceptives while utilizinga theoretical framework guided by the Theory of Planned Behavior (TPB).Methods: A cross-sectional, self-administered survey was completed by a random sample of communitypharmacists in Alexandria, Egypt to determine their attitudes and behaviors regarding counseling on OCs.
Multiple regression was used to predict self-reported counseling on oral contraceptives as a function of theTPB-related constructs and six other factors – “perceived importance of profit from dispensing OCs onpharmacy revenue,” “number of hours worked,” “age,” “gender,” “pharmacy practice degree” and
“marital status” of the pharmacist.Results: Of the 181 pharmacists invited to complete the survey, 168 (93%) participated. Pharmacistsindicated they talked to a slightly higher proportion of women about the importance of taking OCs at the
same time daily than about topics such as which day to start taking OCs, side effects and what to dowhen a dose of OCs was missed. Pharmacists’ reported counseling on oral contraceptives was positivelyassociated with their perception that women welcomed pharmacist initiated OC counseling (b ¼ 0.315,P ! 0.001), perceived adequacy of time available to counsel women on OCs (b ¼ 0.290, P ¼ 0.003) and
the perceived number of women who asked for their help in selecting an OC without providing a pre-scription in the past week (b ¼ 0.160, P ¼ 0.018). Pharmacists reported that women’s welcoming phar-macists initiating OC counseling was associated with the pharmacists’ reported percent who asked
pharmacists for OC advice out of the last 5 women seeking OC (r ¼ 0.45; P ! 0.0001). Male pharmacistswere less likely than female pharmacists to report that women welcomed pharmacist initiated OC coun-seling (r ¼ �0.27; P ¼ 0.0005).
Conclusions: The TPB appears to help predict pharmacists’ OC counseling. There is a need to preparepharmacists who are frequently requested to assist women with the selection of an oral contraceptive.Interventions that would facilitate women’s requests for information may be valuable to increase
pharmacists’ counseling on oral contraceptives. Future qualitative and observational studies are needed
* Corresponding author.
E-mail address: [email protected] (M.E.K. Amin).
1551-7411/$ - see front matter � 2015 Elsevier Inc. All rights reserved.
http://dx.doi.org/10.1016/j.sapharm.2015.08.009
2 Amin & Chewning / Research in Social and Administrative Pharmacy j (2015) 1–13
to assess complexities in counseling on oral contraceptives in developing countries.� 2015 Elsevier Inc. All rights reserved.
Keywords: Oral contraceptives; Family planning; Contraception; Egypt; Theory of planned behavior; Pharmacist
Introduction
Background
Oral contraceptives (OCs) are highly effectivewhen used properly. Providing correct and
complete counseling on the use of oral contra-ceptives is central to securing the autonomy ofwomen in child-bearing age and has been
proven to be a powerful tool of social change.In recent decades, Egypt, the most populouscountry in the Middle East and the third most
populous country in Africa, has witnessed aconsiderable expansion of family planning usethat was associated with an increased awareness
of family planning methods.1
Pharmacists in many developing countries suchas Egypt dispense, select and at times prescribepharmaceuticals including OCs, which are readily
available without a prescription. They have asignificant potential to ensure the safe use ofOCs where family planning is a national priority.
The 2014 Egypt Demographic and Health Survey(EDHS), the latest in a series of nationallyrepresentative population and health surveys con-
ducted in Egypt, shows that pharmacies were theprincipal source for OCs.1 However, it also showsthat women obtaining their OCs from pharmacieswere much less likely than women obtaining their
OCs from other health facilities to have receivedinformation, especially about side effects, neces-sary to make an informed choice.1
While most of the literature focused on phar-macists’ attitudes and practices related to emer-gency contraception,2–9 a few studies examined
community pharmacists’ counseling on the morecommonly used low dose OCs.7,10–12 Studies thatused simulated patrons to evaluate the quality of
counseling provided to patrons indicate that asmall percentage of pharmacists provided coun-seling on OCs and that even when counselingwas provided, it was missing key information.7,12
Sattari et al’s findings indicate that at times phar-macists were not providing information to pa-trons even when pharmacists possessed the
correct knowledge.10 While these few studies sug-gest pharmacists’ counseling behavior is limited,there is little information on factors associated
with the provision of counseling to women onOCs.
Theoretical framework
The Theory of Planned Behavior (TPB) implies
that individuals carefully consider the availableinformation before acting.13 According to TPB,attitudes (feelings about a behavior), subjective
norms (perception of whether important peopleperform and approve the behavior or not) andperceived behavioral control (perception of thedifficulty of performing a behavior) determine
the individual’s behavioral intention (plan toperform behavior) and consequently determinethe likelihood of the individual carrying out that
specific behavior. A measure of perceived moralobligation (personal feelings of responsibility toperform, or refuse to perform, a certain
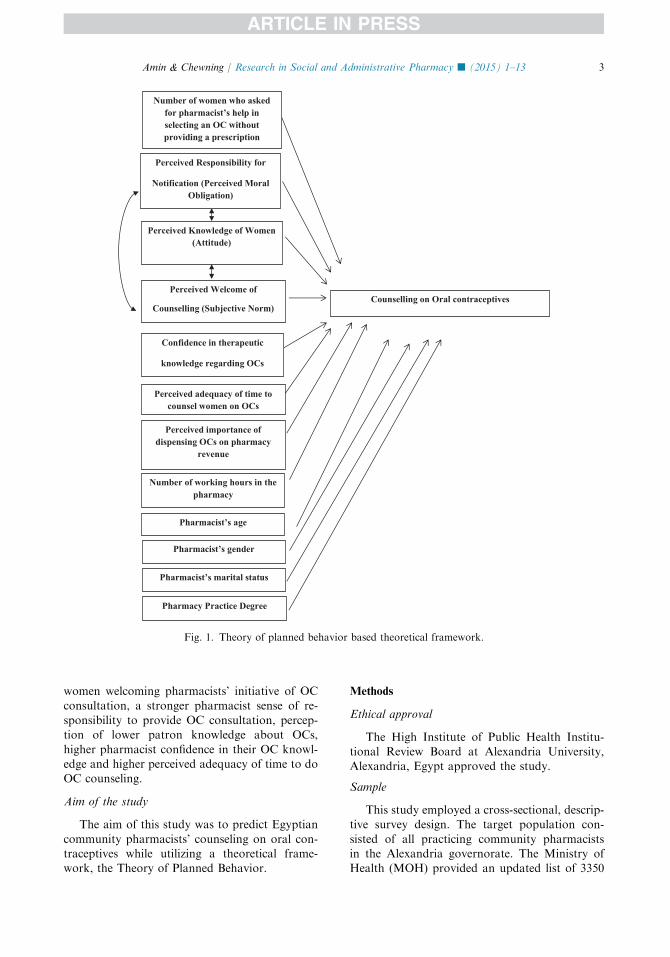
behavior)14 could add predictive power to themodels predicting pharmacists’ intentions to carryout behaviors.15,16 As seen in Fig. 1, this study
uses constructs derived from TPB and adaptedto the research question following pre-testing.Consistent with TPB, pharmacists’ counseling isassumed to be under their volitional control.
Perceived Welcome of Counseling (PWC), derivedfrom the subjective norm construct, is defined asthe pharmacist’s perception of the proportion of
women who would welcome the pharmacist initi-ation of a conversation on topics related to oralcontraceptive use. The Perceived Knowledge of
Women (PKW), derived from the attitudeconstruct, is defined as a pharmacist’s perceptionof the proportion of women who possess adequate
knowledge regarding OCs. Perceived Responsibil-ity for Notification (PRN), derived from theperceived moral obligation construct, is definedas the pharmacist’s perception of responsibility
to notify women about four key topics related toOCs. Finally, two measures related to theperceived behavioral control construct were
used. These included the level of confidence inone’s therapeutic knowledge regarding OCs andperceived adequacy of time available to counsel
women on OCs.Consistent with TPB higher rates of counseling
on OCs should be associated with higher rates of
Perceived Knowledge of Women(Attitude)
Perceived Welcome of
Counselling (Subjective Norm)
Perceived Responsibility for
Notification (Perceived Moral Obligation)
Confidence in therapeutic
knowledge regarding OCs
Perceived adequacy of time to counsel women on OCs
Perceived importance of dispensing OCs on pharmacy
revenue
Number of working hours in the pharmacy
Counselling on Oral contraceptives
Pharmacist’s age
Pharmacist’s gender
Pharmacist’s marital status
Pharmacy Practice Degree
Number of women who asked for pharmacist’s help in selecting an OC without providing a prescription
Fig. 1. Theory of planned behavior based theoretical framework.
3Amin & Chewning / Research in Social and Administrative Pharmacy j (2015) 1–13
women welcoming pharmacists’ initiative of OC
consultation, a stronger pharmacist sense of re-sponsibility to provide OC consultation, percep-tion of lower patron knowledge about OCs,
higher pharmacist confidence in their OC knowl-edge and higher perceived adequacy of time to doOC counseling.
Aim of the study
The aim of this study was to predict Egyptian
community pharmacists’ counseling on oral con-traceptives while utilizing a theoretical frame-work, the Theory of Planned Behavior.
Methods
Ethical approval
The High Institute of Public Health Institu-tional Review Board at Alexandria University,Alexandria, Egypt approved the study.
Sample
This study employed a cross-sectional, descrip-tive survey design. The target population con-
sisted of all practicing community pharmacistsin the Alexandria governorate. The Ministry ofHealth (MOH) provided an updated list of 3350
4 Amin & Chewning / Research in Social and Administrative Pharmacy j (2015) 1–13
potentially open community pharmacies as thesampling frame. To determine sample size it wasassumed that predictors will explain at least 15%
of the variance in the dependent variable. Analpha of 0.01, power ¼ 0.90 with 13 predictorvariables in the model was specified. Resultsindicated that 138 pharmacists would be needed.
Substantial planning went into identifying andenrolling the sample. To achieve a target sampleof at least 138 pharmacists, consideration was
given to potential pharmacist refusals, closedpharmacies, pharmacies that cannot be located,and absenteeism pharmacies where a non-
pharmacist served patrons.17 Thus, of the 3309community pharmacies in the sampling frame,230 pharmacies were selected using a randomnumber generator. One pharmacist per commu-
nity pharmacy was asked to complete the surveyforms. When more than one pharmacist was inthe pharmacy at the time of the visit, the data col-
lector asked the staff pharmacist who was aboutto interact with the next patron to fill the survey.Pharmacy students, pharmacy interns and non-
pharmacist attendants were excluded.
Study measures
Dependent variableA pharmacist’s reported amount of OC coun-
seling was measured using four items on the
following topics (1) the importance of takingOCs at the same time every day, (2) the appro-priate day to start taking OCs, (3) how to act ifone or more pills are missed and (4) OC side
effects. Pharmacists were asked to recall the lastfive women to whom they dispensed OCs andindicate the number they counseled on each of
these four topics. This included women who didor did not present a prescription for OCs to thepharmacist. A 6-point scale ranging from 0 to 5
was used. To construct the dependent measure,the four numbers reported by pharmacists wereaveraged. This average generated an overall indi-
cator of the proportion of women to which thetotal array of OC consulting topics were coveredby pharmacists (see Table 1).
Independent variablesThe Perceived Responsibility for Notification
(PRN) predictor variable was operationalized asthe pharmacist perception of their responsibilityfor notifying women about OC using the four items
and a 5-point scale ranging from “not at all respon-sible to extremely responsible” The average scorefor the four items was used in calculating the
pharmacist’s mean PRN in the analysis (seeTable 1). The Perceived Knowledge of Women(PKW) predictor variable was operationalized as
a pharmacist’s perception of the proportion ofwomen who possess adequate knowledge regardingthe same four OC topics using a 5-point scaleranging from 0 to 100%. The average score for
the four items was used in calculating the pharma-cist’s mean PKW in the analysis (see Table 1). Simi-larly, pharmacists’ perception of how much women
welcomed pharmacist initiating OC consultation,the Perceived Welcome of Counseling (PWC) wasoperationalized as the pharmacist’s perception of
the proportion of women who would welcome thepharmacist initiation of a conversation about eachof the same four topics and a 5-point scale rangingfrom 0 to 100%. The average score for the four
items was used in calculating the pharmacist’smean PWC in the analysis (see Table 1). Like thedependent variable, these three TPB measures
included women who did or did not present a pre-scription for OCs to the pharmacist.
In addition to the above-mentioned variables
derived from the perception and subjective norm,the following independent variables were includedto represent perceived behavioral control. Phar-
macists were asked about their level of confidencein their therapeutic knowledge regarding OCs andperceived adequacy of time available to counselwomen on OCs. Similar to PRN, 5-point scales
ranging from “not ———— at all” to “extremely—————”
The full adapted TPB framework is shown in
Fig. 1.
Other variablesIn relation to the extent to which pharmacists
believed women welcomed pharmacists’ raising
OC topics, pharmacists were asked about thenumber of women who solicited advice frompharmacists on any topic related to OCs. Other
variables included importance of profit fromdispensing OCs for pharmacy revenue, and de-mographic variables such as pharmacists’ age,gender, marital status, pharmacy practice degree,
and the average number of hours the pharmacistworked every day. In terms of the prescriptionstatus of requests, pharmacists were asked about
the average number of women in the past weekwho requested an OC who had an OC prescrip-tion and the average number of women who did
not have a prescription. They were also asked forthe average number of women who requested helpin selecting an OC product without providing a
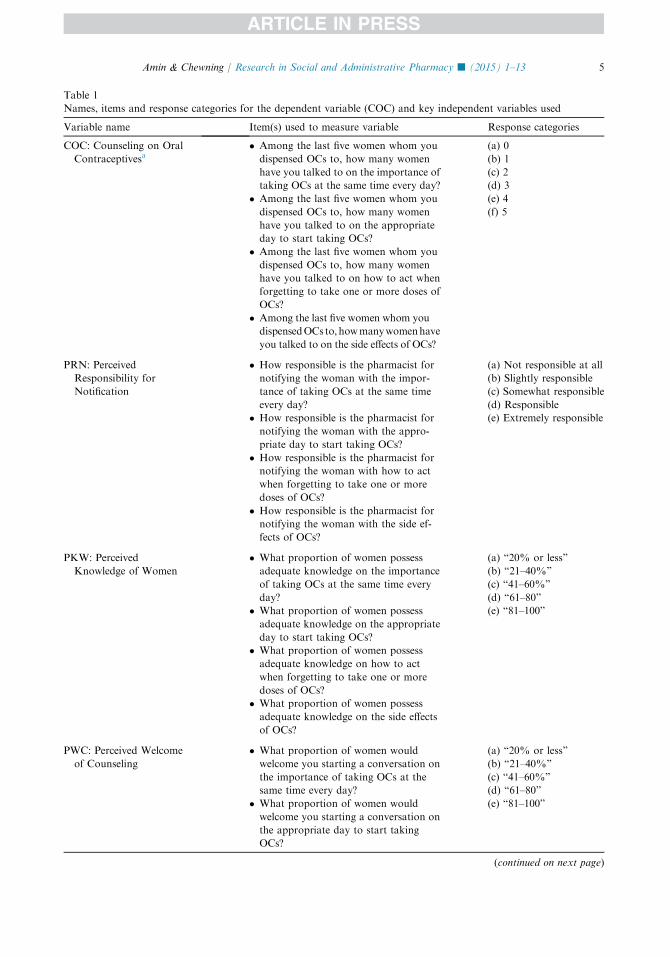
Table 1
Names, items and response categories for the dependent variable (COC) and key independent variables used
Variable name Item(s) used to measure variable Response categories
COC: Counseling on Oral
Contraceptivesa� Among the last five women whom you
dispensed OCs to, how many women
have you talked to on the importance of
taking OCs at the same time every day?
� Among the last five women whom you
dispensed OCs to, how many women
have you talked to on the appropriate
day to start taking OCs?
� Among the last five women whom you
dispensed OCs to, how many women
have you talked to on how to act when
forgetting to take one or more doses of
OCs?
� Among the last five women whom you
dispensedOCs to, howmanywomenhave
you talked to on the side effects of OCs?
(a) 0
(b) 1
(c) 2
(d) 3
(e) 4
(f) 5
PRN: Perceived
Responsibility for
Notification
� How responsible is the pharmacist for
notifying the woman with the impor-
tance of taking OCs at the same time
every day?
� How responsible is the pharmacist for
notifying the woman with the appro-
priate day to start taking OCs?
� How responsible is the pharmacist for
notifying the woman with how to act
when forgetting to take one or more
doses of OCs?
� How responsible is the pharmacist for
notifying the woman with the side ef-
fects of OCs?
(a) Not responsible at all
(b) Slightly responsible
(c) Somewhat responsible
(d) Responsible
(e) Extremely responsible
PKW: Perceived
Knowledge of Women
� What proportion of women possess
adequate knowledge on the importance
of taking OCs at the same time every
day?
� What proportion of women possess
adequate knowledge on the appropriate
day to start taking OCs?
� What proportion of women possess
adequate knowledge on how to act
when forgetting to take one or more
doses of OCs?
� What proportion of women possess
adequate knowledge on the side effects
of OCs?
(a) “20% or less”
(b) “21–40%”
(c) “41–60%”
(d) “61–80”
(e) “81–100”
PWC: Perceived Welcome
of Counseling
� What proportion of women would
welcome you starting a conversation on
the importance of taking OCs at the
same time every day?
� What proportion of women would
welcome you starting a conversation on
the appropriate day to start taking
OCs?
(a) “20% or less”
(b) “21–40%”
(c) “41–60%”
(d) “61–80”
(e) “81–100”
(continued on next page)
5Amin & Chewning / Research in Social and Administrative Pharmacy j (2015) 1–13
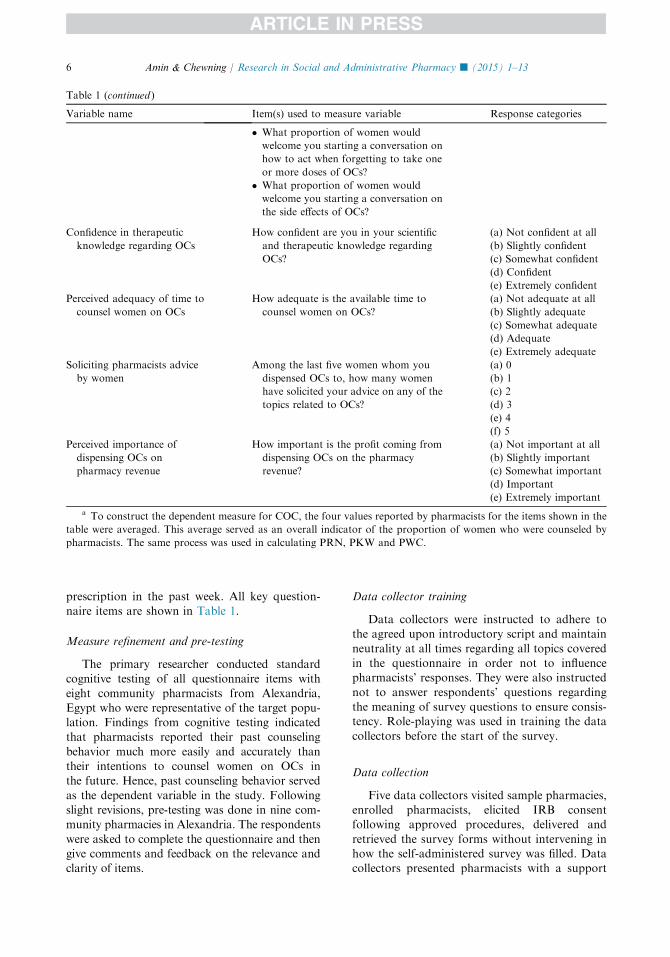
Table 1 (continued )
Variable name Item(s) used to measure variable Response categories
� What proportion of women would
welcome you starting a conversation on
how to act when forgetting to take one
or more doses of OCs?
� What proportion of women would
welcome you starting a conversation on
the side effects of OCs?
Confidence in therapeutic
knowledge regarding OCs
How confident are you in your scientific
and therapeutic knowledge regarding
OCs?
(a) Not confident at all
(b) Slightly confident
(c) Somewhat confident
(d) Confident
(e) Extremely confident
Perceived adequacy of time to
counsel women on OCs
How adequate is the available time to
counsel women on OCs?
(a) Not adequate at all
(b) Slightly adequate
(c) Somewhat adequate
(d) Adequate
(e) Extremely adequate
Soliciting pharmacists advice
by women
Among the last five women whom you
dispensed OCs to, how many women
have solicited your advice on any of the
topics related to OCs?
(a) 0
(b) 1
(c) 2
(d) 3
(e) 4
(f) 5
Perceived importance of
dispensing OCs on
pharmacy revenue
How important is the profit coming from
dispensing OCs on the pharmacy
revenue?
(a) Not important at all
(b) Slightly important
(c) Somewhat important
(d) Important
(e) Extremely important
a To construct the dependent measure for COC, the four values reported by pharmacists for the items shown in the
table were averaged. This average served as an overall indicator of the proportion of women who were counseled by
pharmacists. The same process was used in calculating PRN, PKW and PWC.
6 Amin & Chewning / Research in Social and Administrative Pharmacy j (2015) 1–13
prescription in the past week. All key question-naire items are shown in Table 1.
Measure refinement and pre-testing
The primary researcher conducted standardcognitive testing of all questionnaire items with
eight community pharmacists from Alexandria,Egypt who were representative of the target popu-lation. Findings from cognitive testing indicatedthat pharmacists reported their past counseling
behavior much more easily and accurately thantheir intentions to counsel women on OCs inthe future. Hence, past counseling behavior served
as the dependent variable in the study. Followingslight revisions, pre-testing was done in nine com-munity pharmacies in Alexandria. The respondents
were asked to complete the questionnaire and thengive comments and feedback on the relevance andclarity of items.
Data collector training
Data collectors were instructed to adhere tothe agreed upon introductory script and maintain
neutrality at all times regarding all topics coveredin the questionnaire in order not to influencepharmacists’ responses. They were also instructed
not to answer respondents’ questions regardingthe meaning of survey questions to ensure consis-tency. Role-playing was used in training the data
collectors before the start of the survey.
Data collection
Five data collectors visited sample pharmacies,enrolled pharmacists, elicited IRB consentfollowing approved procedures, delivered and
retrieved the survey forms without intervening inhow the self-administered survey was filled. Datacollectors presented pharmacists with a support
7Amin & Chewning / Research in Social and Administrative Pharmacy j (2015) 1–13
letter from the Dean of the High Institute ofPublic Health in Alexandria University thatvalidated the identity of the primary researcher,explained the purpose of the study and encour-
aged cooperation from pharmacists. The phar-macy was visited up to two additional times tomake sure the pharmacist was located. If the
pharmacist was not found after a total of threevisits, the pharmacist was considered absent. Datawere collected in the period from the December
2014 to January 2015.
Data analysis
Data were analyzed using STATA (Version 12).
Descriptive analysesDescriptive statistics were used to describe the
characteristics of the sample as well the dependent
and independent variables. Descriptive analysesgenerated frequencies, as well as means, ranges orstandard deviations as relevant.
Bivariate and psychometric analysesScale scores were calculated by summing the
items and dividing by the number of items in thescale. Average scores were created for PWC,PKW, RRN and COC. Higher scores signified
pharmacists’ higher perceived (1) patron welcomeof pharmacist initiated OC counseling, (2) patronknowledge of OCs, (3) pharmacist responsibility
to educate women about OCs and (4) a largerpercent of the last five women they dispensed OCsto who they also counseled on OC topics.
Bivariate analyses of the independent and
dependent variables were conducted. A correlationmatrix was created to examine the relationshipsbetween different variables. Cronbach’s alpha was
used to analyze internal consistency of PWC,PKW, RRN and COC behavior scales.
RegressionIn addition to TPB predictors, the regression
model included sociocognitive or pharmacistcharacteristic variables that were hypothesized tobe theoretically associated with pharmacist coun-seling behavior. The goal was to achieve the most
parsimonious model that explains the most vari-ance in the dependent variable.
Before insertion into the regression model, the
four items of the PWC and PKW variables wereeach coded as 0–4 for the following responsecategories: “20% or less,” “21–40%,” “41–60%,”
“61–80” “81–100.” The four items of the PRNvariable were coded 0–4 for the followingresponse categories: “Not responsible at all,”
“slightly responsible,” “somewhat responsible,”“responsible” and “extremely responsible.” Foreach of these variables, the average of the scoresfrom their respective four items was inserted in the
regression model. Statistical tests were two-sidedwith alpha set at P ! 0.05.
Results
Sample identification and response
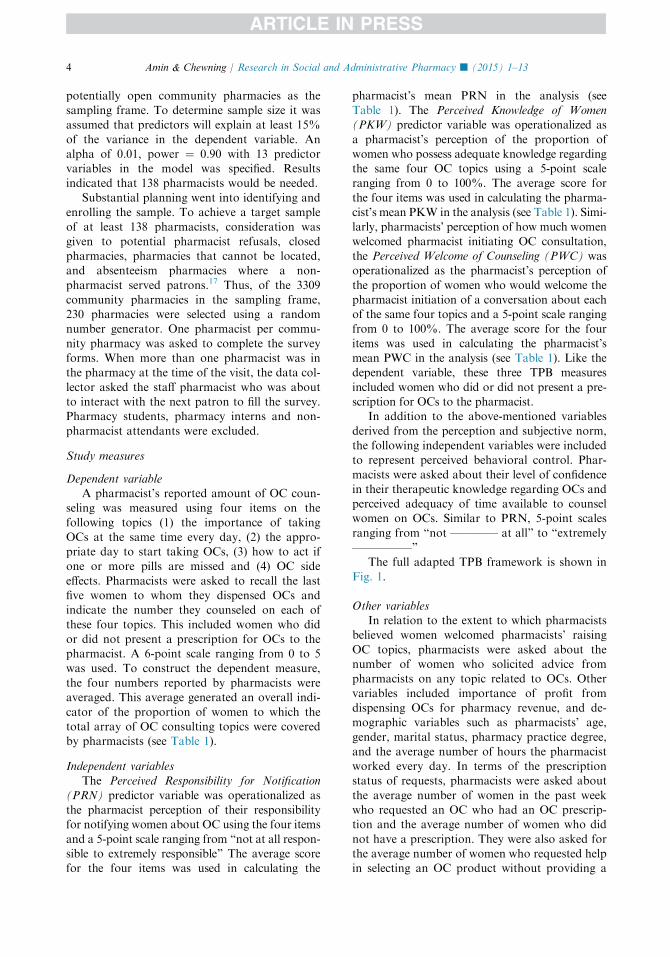
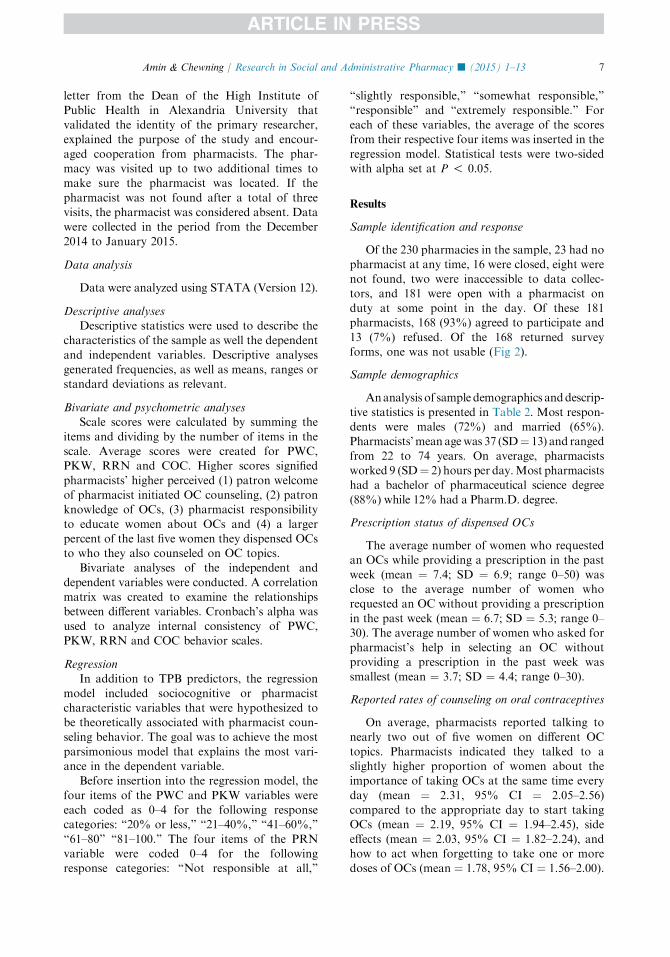
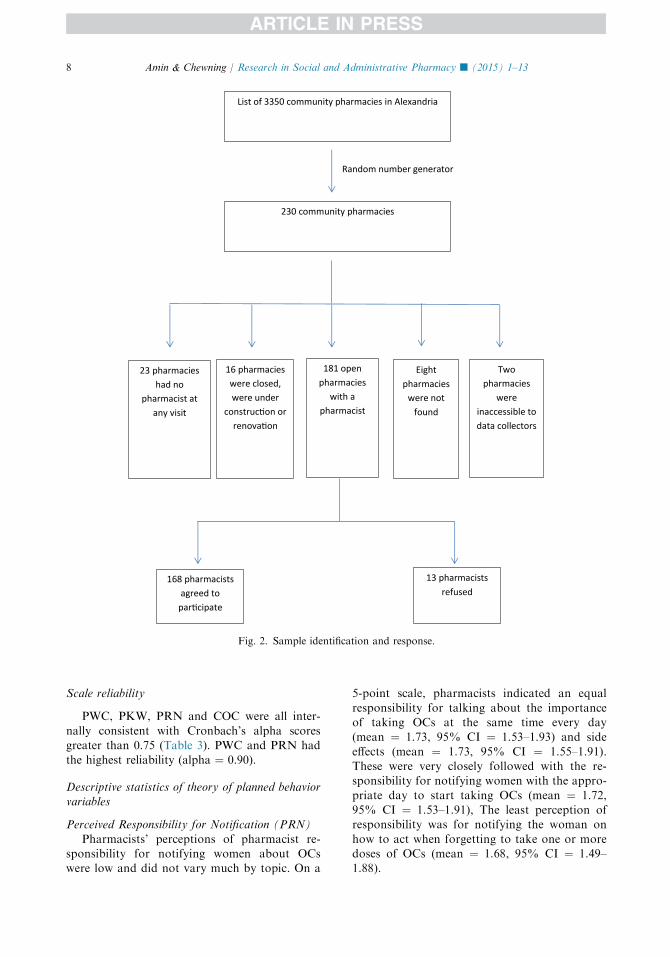
Of the 230 pharmacies in the sample, 23 had nopharmacist at any time, 16 were closed, eight were
not found, two were inaccessible to data collec-tors, and 181 were open with a pharmacist onduty at some point in the day. Of these 181pharmacists, 168 (93%) agreed to participate and
13 (7%) refused. Of the 168 returned surveyforms, one was not usable (Fig 2).
Sample demographics
Ananalysis of sample demographics anddescrip-
tive statistics is presented in Table 2. Most respon-dents were males (72%) and married (65%).Pharmacists’mean agewas 37 (SD¼ 13) and ranged
from 22 to 74 years. On average, pharmacistsworked 9 (SD¼ 2) hours per day.Most pharmacistshad a bachelor of pharmaceutical science degree
(88%) while 12% had a Pharm.D. degree.
Prescription status of dispensed OCs
The average number of women who requestedan OCs while providing a prescription in the past
week (mean ¼ 7.4; SD ¼ 6.9; range 0–50) wasclose to the average number of women whorequested an OC without providing a prescription
in the past week (mean ¼ 6.7; SD ¼ 5.3; range 0–30). The average number of women who asked forpharmacist’s help in selecting an OC withoutproviding a prescription in the past week was
smallest (mean ¼ 3.7; SD ¼ 4.4; range 0–30).
Reported rates of counseling on oral contraceptives
On average, pharmacists reported talking tonearly two out of five women on different OC
topics. Pharmacists indicated they talked to aslightly higher proportion of women about theimportance of taking OCs at the same time every
day (mean ¼ 2.31, 95% CI ¼ 2.05–2.56)compared to the appropriate day to start takingOCs (mean ¼ 2.19, 95% CI ¼ 1.94–2.45), side
effects (mean ¼ 2.03, 95% CI ¼ 1.82–2.24), andhow to act when forgetting to take one or moredoses of OCs (mean ¼ 1.78, 95% CI ¼ 1.56–2.00).
List of 3350 community pharmacies in Alexandria
230 community pharmacies
Random number generator
23 pharmacies had no
pharmacist at any visit
16 pharmacies were closed, were under
construc on or renova on
181 open pharmacies
with apharmacist
Eight pharmacies
were not found
Twopharmacies
wereinaccessible to data collectors
168 pharmacists agreed to
par cipate
13 pharmacists refused
Fig. 2. Sample identification and response.
8 Amin & Chewning / Research in Social and Administrative Pharmacy j (2015) 1–13
Scale reliability
PWC, PKW, PRN and COC were all inter-
nally consistent with Cronbach’s alpha scoresgreater than 0.75 (Table 3). PWC and PRN hadthe highest reliability (alpha ¼ 0.90).
Descriptive statistics of theory of planned behaviorvariables
Perceived Responsibility for Notification (PRN)
Pharmacists’ perceptions of pharmacist re-sponsibility for notifying women about OCswere low and did not vary much by topic. On a
5-point scale, pharmacists indicated an equal
responsibility for talking about the importanceof taking OCs at the same time every day(mean ¼ 1.73, 95% CI ¼ 1.53–1.93) and side
effects (mean ¼ 1.73, 95% CI ¼ 1.55–1.91).These were very closely followed with the re-sponsibility for notifying women with the appro-
priate day to start taking OCs (mean ¼ 1.72,95% CI ¼ 1.53–1.91), The least perception ofresponsibility was for notifying the woman on
how to act when forgetting to take one or moredoses of OCs (mean ¼ 1.68, 95% CI ¼ 1.49–1.88).
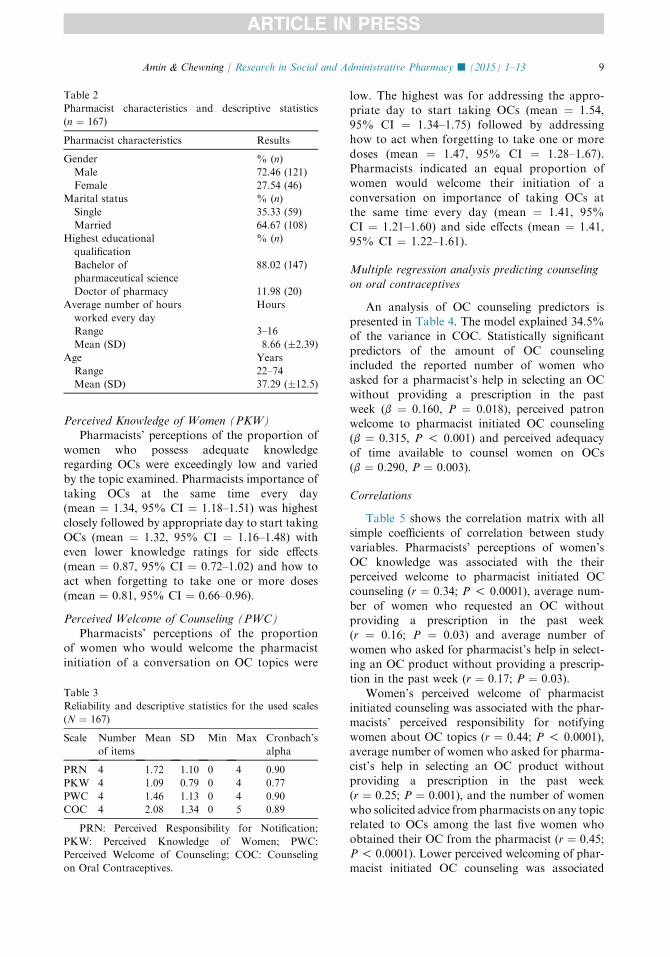
Table 2
Pharmacist characteristics and descriptive statistics
(n ¼ 167)
Pharmacist characteristics Results
Gender % (n)
Male 72.46 (121)
Female 27.54 (46)
Marital status % (n)
Single 35.33 (59)
Married 64.67 (108)
Highest educational
qualification
% (n)
Bachelor of
pharmaceutical science
88.02 (147)
Doctor of pharmacy 11.98 (20)
Average number of hours
worked every day
Hours
Range 3–16
Mean (SD) 8.66 (�2.39)
Age Years
Range 22–74
Mean (SD) 37.29 (�12.5)
9Amin & Chewning / Research in Social and Administrative Pharmacy j (2015) 1–13
Perceived Knowledge of Women (PKW)Pharmacists’ perceptions of the proportion of
women who possess adequate knowledgeregarding OCs were exceedingly low and varied
by the topic examined. Pharmacists importance oftaking OCs at the same time every day(mean ¼ 1.34, 95% CI ¼ 1.18–1.51) was highest
closely followed by appropriate day to start takingOCs (mean ¼ 1.32, 95% CI ¼ 1.16–1.48) witheven lower knowledge ratings for side effects
(mean ¼ 0.87, 95% CI ¼ 0.72–1.02) and how toact when forgetting to take one or more doses(mean ¼ 0.81, 95% CI ¼ 0.66–0.96).
Perceived Welcome of Counseling (PWC)Pharmacists’ perceptions of the proportion
of women who would welcome the pharmacist
initiation of a conversation on OC topics were
Table 3
Reliability and descriptive statistics for the used scales
(N ¼ 167)
Scale Number
of items
Mean SD Min Max Cronbach’s
alpha
PRN 4 1.72 1.10 0 4 0.90
PKW 4 1.09 0.79 0 4 0.77
PWC 4 1.46 1.13 0 4 0.90
COC 4 2.08 1.34 0 5 0.89
PRN: Perceived Responsibility for Notification;
PKW: Perceived Knowledge of Women; PWC:
Perceived Welcome of Counseling; COC: Counseling
on Oral Contraceptives.
low. The highest was for addressing the appro-priate day to start taking OCs (mean ¼ 1.54,95% CI ¼ 1.34–1.75) followed by addressinghow to act when forgetting to take one or more
doses (mean ¼ 1.47, 95% CI ¼ 1.28–1.67).Pharmacists indicated an equal proportion ofwomen would welcome their initiation of a
conversation on importance of taking OCs atthe same time every day (mean ¼ 1.41, 95%CI ¼ 1.21–1.60) and side effects (mean ¼ 1.41,
95% CI ¼ 1.22–1.61).
Multiple regression analysis predicting counseling
on oral contraceptives
An analysis of OC counseling predictors ispresented in Table 4. The model explained 34.5%of the variance in COC. Statistically significant
predictors of the amount of OC counselingincluded the reported number of women whoasked for a pharmacist’s help in selecting an OC
without providing a prescription in the pastweek (b ¼ 0.160, P ¼ 0.018), perceived patronwelcome to pharmacist initiated OC counseling(b ¼ 0.315, P ! 0.001) and perceived adequacy
of time available to counsel women on OCs(b ¼ 0.290, P ¼ 0.003).
Correlations
Table 5 shows the correlation matrix with allsimple coefficients of correlation between studyvariables. Pharmacists’ perceptions of women’s
OC knowledge was associated with the theirperceived welcome to pharmacist initiated OCcounseling (r ¼ 0.34; P ! 0.0001), average num-
ber of women who requested an OC withoutproviding a prescription in the past week(r ¼ 0.16; P ¼ 0.03) and average number of
women who asked for pharmacist’s help in select-ing an OC product without providing a prescrip-tion in the past week (r ¼ 0.17; P ¼ 0.03).
Women’s perceived welcome of pharmacistinitiated counseling was associated with the phar-macists’ perceived responsibility for notifyingwomen about OC topics (r ¼ 0.44; P ! 0.0001),
average number of women who asked for pharma-cist’s help in selecting an OC product withoutproviding a prescription in the past week
(r ¼ 0.25; P ¼ 0.001), and the number of womenwho solicited advice from pharmacists on any topicrelated to OCs among the last five women who
obtained their OC from the pharmacist (r ¼ 0.45;P ! 0.0001). Lower perceived welcoming of phar-macist initiated OC counseling was associated
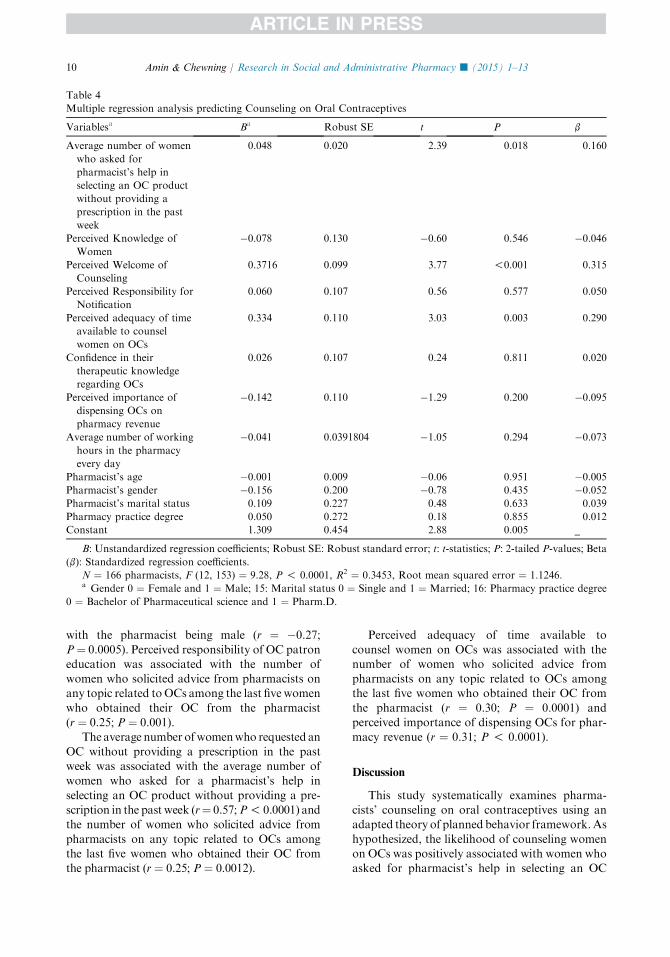
Table 4
Multiple regression analysis predicting Counseling on Oral Contraceptives
Variablesa Ba Robust SE t P b
Average number of women
who asked for
pharmacist’s help in
selecting an OC product
without providing a
prescription in the past
week
0.048 0.020 2.39 0.018 0.160
Perceived Knowledge of
Women
�0.078 0.130 �0.60 0.546 �0.046
Perceived Welcome of
Counseling
0.3716 0.099 3.77 !0.001 0.315
Perceived Responsibility for
Notification
0.060 0.107 0.56 0.577 0.050
Perceived adequacy of time
available to counsel
women on OCs
0.334 0.110 3.03 0.003 0.290
Confidence in their
therapeutic knowledge
regarding OCs
0.026 0.107 0.24 0.811 0.020
Perceived importance of
dispensing OCs on
pharmacy revenue
�0.142 0.110 �1.29 0.200 �0.095
Average number of working
hours in the pharmacy
every day
�0.041 0.0391804 �1.05 0.294 �0.073
Pharmacist’s age �0.001 0.009 �0.06 0.951 �0.005
Pharmacist’s gender �0.156 0.200 �0.78 0.435 �0.052
Pharmacist’s marital status 0.109 0.227 0.48 0.633 0.039
Pharmacy practice degree 0.050 0.272 0.18 0.855 0.012
Constant 1.309 0.454 2.88 0.005 _
B: Unstandardized regression coefficients; Robust SE: Robust standard error; t: t-statistics; P: 2-tailed P-values; Beta
(b): Standardized regression coefficients.
N ¼ 166 pharmacists, F (12, 153) ¼ 9.28, P ! 0.0001, R2 ¼ 0.3453, Root mean squared error ¼ 1.1246.a Gender 0 ¼ Female and 1 ¼ Male; 15: Marital status 0 ¼ Single and 1 ¼ Married; 16: Pharmacy practice degree
0 ¼ Bachelor of Pharmaceutical science and 1 ¼ Pharm.D.
10 Amin & Chewning / Research in Social and Administrative Pharmacy j (2015) 1–13
with the pharmacist being male (r ¼ �0.27;
P¼ 0.0005). Perceived responsibility of OC patroneducation was associated with the number ofwomen who solicited advice from pharmacists onany topic related toOCs among the last five women
who obtained their OC from the pharmacist(r ¼ 0.25; P ¼ 0.001).
The average number ofwomenwho requested an
OC without providing a prescription in the pastweek was associated with the average number ofwomen who asked for a pharmacist’s help in
selecting an OC product without providing a pre-scription in the past week (r¼ 0.57;P! 0.0001) andthe number of women who solicited advice from
pharmacists on any topic related to OCs amongthe last five women who obtained their OC fromthe pharmacist (r ¼ 0.25; P ¼ 0.0012).
Perceived adequacy of time available to
counsel women on OCs was associated with thenumber of women who solicited advice frompharmacists on any topic related to OCs amongthe last five women who obtained their OC from
the pharmacist (r ¼ 0.30; P ¼ 0.0001) andperceived importance of dispensing OCs for phar-macy revenue (r ¼ 0.31; P ! 0.0001).
Discussion
This study systematically examines pharma-cists’ counseling on oral contraceptives using anadapted theory of planned behavior framework.As
hypothesized, the likelihood of counseling womenon OCs was positively associated with women whoasked for pharmacist’s help in selecting an OC

Table 5
Correlation matrix for study variables (The number of observations used in estimating correlations ranged from 166
to 167)
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
1 1.00
2 0.17* 1.00
3 0.49* 0.34* 1.00
4 0.32* 0.07 0.44* 1.00
5 0.28* 0.16* 0.06 0.09 1.00
6 0.10 0.14 0.12 �0.11 0.21* 1.00
7 0.29* 0.17* 0.25* 0.03 0.57* 0.43* 1.00
8 0.49* 0.10 0.45* 0.25* 0.25* 0.06 0.31* 1.00
9 0.46* 0.25* 0.46* 0.48* 0.14 0.07 0.23* 0.30* 1.00
10 0.24* 0.25* 0.33* 0.25* 0.12 0.00 0.07 0.25* 0.47* 1.00
11 0.12 0.08 0.29* 0.26* �0.00 0.05 0.02 0.04 0.31* 0.28* 1.00
12�0.00 0.05 0.05 0.01 0.25* 0.13 0.11 0.11 0.12 0.14 �0.05 1.00
13 0.04 0.14 0.00 0.12 0.12 �0.09 �0.04 �0.03 0.17* 0.23*�0.00 0.18* 1.00
14�0.18*�0.07 �0.27*�0.13 �0.07 �0.06 �0.13 �0.06 �0.13 �0.01 �0.14 0.06 0.26* 1.00
15 0.05 0.13 0.08 0.08 0.12 �0.10 �0.08 �0.03 0.17* 0.17* 0.12 0.16* 0.60* 0.33* 1.00
16�0.02 0.16* 0.02 �0.25* �0.07 0.05 0.01 0.09 �0.09 0.07 �0.01�0.10 �0.05 �0.06 �0.11 1.00
*Significant at P ! 0.05.
1: Counseling on Oral Contraceptives (COC); 2: Perceived Knowledge of Women (PKW); 3: Perceived Welcome of
Counseling (PWC); 4: Perceived Responsibility for Notification (PRN); 5: Average number of women who requested an
OC without providing a prescription in the past week; 6: Average number of women who requested an OCs while
providing a prescription in the past week; 7: Average number of women who asked for pharmacist’s help in selecting
an OC product without providing a prescription in the past week; 8: The number of women who solicited advice
from pharmacists on any topic related to OCs among the last five women who obtained their OC from the pharmacist;
9: Perceived adequacy of time available to counsel women on OCs; 10: Confidence in their therapeutic knowledge
regarding OCs; 11: Perceived importance of dispensing OCs on pharmacy revenue; 12: Average number of working
hours the pharmacy every day; 13: Pharmacist’s age; 14: Gender 0 ¼ Female and 1 ¼ Male; 15: Marital status
0 ¼ Single and 1 ¼ Married; 16: Pharmacy practice degree 0 ¼ Bachelor of Pharmaceutical science and 1 ¼ Pharm.D.
11Amin & Chewning / Research in Social and Administrative Pharmacy j (2015) 1–13
without providing a prescription, the pharmacist’sperception of the proportion of women who wouldwelcome the pharmacist initiation of a conversa-tion onCOC topics and perceived adequacy of time
available to counsel women on OCs. However, apharmacist’s perception of the proportion ofwomenwho possess adequate knowledge regarding
OCs and a pharmacist’s perception of responsibil-ity for notifying women with information on topicsrelated to OCs were not significantly associated
with counseling on OCs. One, two or all three TPBconstructs have been found to be significant pre-dictors of other types of pharmacist behaviors in
previous studies.18–20
Compared to other topics, pharmacists re-ported they were less likely to counsel women onside effects and how to act when forgetting to take
one or more doses of OCs. Pharmacists in thisstudy had the perception that women in generalwould not prefer to listen to possible side effects
before they start taking OCs. It may also beexplained by a classical case where the principle ofbeneficence and autonomy collide as a pharmacist
would fear that the women would not take herOCs if she is informed about the OC side effects.This may explain the demographic health surveyfinding of women not receiving adequate infor-
mation on side effects from pharmacies, necessaryto make an informed choice and manage sideeffects should they occur.1 Providing information
on how to act when forgetting to take one ormore doses of OCs is time demanding and wouldneed a certain competency in therapeutic knowl-
edge that most Egyptian pharmacists may nothave acquired in their training.
Pharmacists’ perception of having adequate
time to counsel women was associated with coun-seling more women on OCs. This should come asno surprise since pharmacist busyness is commonlycited as a barrier for providing information to
patrons in different studies addressing counselingprovided by community pharmacists. Amount ofinformation provided to patrons was affected by
the level of pharmacy busyness.21–23 Interventionsaddressing pharmacist counseling on OCs andother topics should use strategies that address

12 Amin & Chewning / Research in Social and Administrative Pharmacy j (2015) 1–13
organizational factors such as time constraints,complementary to concerns about the training pro-vided to pharmacists and/or patrons.24
The pharmacist’s perception of the proportionof women who would welcome the pharmacistinitiation of a conversation on OCs was thestrongest predictor of counseling on OCs after
controlling for other predictors. Further, thisperception was associated with the number ofwomen who were perceived to have solicited OC
advice from pharmacists. This gives insight onhow pharmacists perceive whether their consultswould be welcomed by women. A woman who is
willing to ask questions is seen as more likely towelcome the pharmacist’s initiating a conversa-tion on a topic related to OCs. While pharmacist’sgender was not a significant predictor of coun-
seling but was associated with perceived patronwelcome of OC counseling. Female pharmacistsfelt that their advice would be better received by
women than their male counterparts did.In Egypt as in many developing countries, most
medicines are routinely supplied without a prescrip-
tion. In some cases where a medication is dispensedwithout a prescription, a pharmacist is assumingprescribing duties.25,26 In this study, pharmacists
were more likely to provide information to womenwho are considering using a contraceptive whenthey prescribed OCs. There is a special need toensure that pharmacists who are serving women
withoutOCprescriptionshave the adequate trainingto carry out this role or to refer women to physicianswho are adequately trained to do so.
Perception of responsibility to counsel on OCswas particularly low for the majority of pharma-cists. It is possible that pharmacists view this as
part of the gynecologist’s responsibility ratherthan theirs. It was alarming to see the perceptionof the proportion of women who possess adequateknowledge was not a significant predictor. Ideally,
a pharmacist would provide counseling to some-one who lacks therapeutic information.
Strengths and limitations
As with all studies, this research had both
strengths and weaknesses. The probability samplewith high response rate reduced nonresponse biasand improved the generalizability of the study. The
study uses scales that employ item specific re-sponses to questions rather than agree/disagreeanswer options which strengthens it further. The
questionnaire was provided to pharmacists in theirnative language improving the comprehension ofquestionnaire items and ultimately improving the
quality of data. Theory based a priori hypothesesdrove the analyses.
Limitations of this project merit discussion. Self-
report measures are more likely to result in theoverestimation of counseling, a socially desirablebehavior. In an attempt to reduce this bias, thesurvey was self-administered and no identifying
information was collected from pharmacists. Thestudy did not include a measure that addressesopportunity for privacy which could have been a
predictor of counseling on oral contraceptives.However, it is unlikely that pharmacies vary in thisregard since counseling spaces are rarely provided in
Egyptian pharmacies. Finally, itwas not possible forpharmacists to discriminate between first time re-quests vs refill requests for OCs from patorns. Thisdistinction was not possible since patrons routinely
obtain medications without a prescription fromEgyptian pharmacies, which are not routinelyequipped with electronic patron medical records.
Need for further research
Qualitative research with pharmacists would
be beneficial for a more in-depth understanding ofthe relationship between the different variablesand counseling on OCs. It would be interesting to
see how useful the PWC is in predicting coun-seling on other medication classes. It would alsobe interesting to know what proportion of women
actually welcome a pharmacist initiating a con-versation on OCs. This would be important sinceearlier research has indicated that pharmacistsand patrons do not necessarily follow the same
“relationship script.”27
Conclusion
The Theory of Planned Behavior appears tohelp predict pharmacists’ OC counseling. There isa need to prepare pharmacists who are frequentlyrequested to assist women with the selection of an
oral contraceptive. Interventions that would facil-itate women’s requests for information may bevaluable to increase pharmacists’ counseling on
oral contraceptives. Future qualitative and obser-vational studies are needed to assess complexitiesin counseling patrons on oral contraceptives.
Acknowledgments
The authors would like to thank Dr. AshrafWahdan at the High Institute of Public Health,
Alexandria University for assisting the researchteam with the project logistics including datacollection and entry.
13Amin & Chewning / Research in Social and Administrative Pharmacy j (2015) 1–13
References
1. Ministry of Health and Population [Egypt], El-
Zanaty and Associates [Egypt], and ICF Interna-
tional. Egypt Demographic and Health Survey 2014.
Cairo, Egypt and Rockville, Maryland, USA: Minis-
try of Health and Population and ICF International;
2015. Available at: http://dhsprogram.com/pubs/
pdf/fr302/fr302.pdf. Accessed 10.06.15.
2. Bennett W, Petraitis C, D’Anella A, Marcella S.
Pharmacists’ knowledge and the difficulty of obtain-
ing emergency contraception.Contraception 2003;68:
261–267.
3. Fuentes EC, Azize-Vargas Y. Knowledge, attitudes
and practices in a group of pharmacists in Puerto
Rico regarding emergency contraception. P RHealth
Sci J 2007;26:191–197.
4. BorregoME, Short J, HouseN,GupchupG,NaikR,
Cuellar D. New Mexico pharmacists’ knowledge,
attitudes, and beliefs toward prescribing oral emer-
gency contraception. J Am Pharm Assoc (2003)
2006;46:33–43.
5. Whelan AM, Langille DB, Hurst E. Nova Scotia
pharmacists’ knowledge of, experiences with and
perception of factors interfering with their ability to
provide emergency contraceptive pill consultations.
Int J Pharm Pract 2013;21:314–321.
6. Shaaban OM, Fathalla MM, Shahin AY, Nasr A.
Emergency contraception in the context of marriage in
Upper Egypt. Int J Gynaecol Obstet 2011;112:195–199.
7. Ratanajamit C, Chongsuvivatwong V. Survey of
knowledge and practice on oral contraceptive and
emergency contraceptive pills of drugstore personnel
in Hat Yai, Thailand. Pharmacoepidemiol Drug Saf
2001;10:149–156.
8. Minh PD, Huong DT, Byrkit R, Murray M.
Strengthening pharmacy practice in Vietnam: find-
ings of a training intervention study. Trop Med Int
Health 2013;18:426–434.
9. Hellerstedt WL, Van Riper KK. Emergency contra-
ceptive pills: dispensing practices, knowledge and at-
titudes of South Dakota pharmacists. Perspect Sex
Reprod Health 2005;37:19–24.
10. Sattari M, Mokhtari Z, Jabari H, Mashayekhi SO.
Knowledge, attitude and practice of pharmacists
and health-care workers regarding oral contracep-
tives correct usage, side-effects and contraindica-
tions. East Mediterr Health J 2013;19:547–554.
11. Sarino LV, Dang KH, Dianat N, et al. Drug interac-
tion between oral contraceptives and St. John’s
Wort: appropriateness of advice received from com-
munity pharmacists and health food store clerks.
J Am Pharm Assoc 2007;47:42–47.
12. Obreli-Neto PR, Pereira LR, Guidoni CM, et al. Use
of simulated patrons to evaluate combined oral con-
traceptive dispensing practices of community phar-
macists. PLoS One 2013;8:e79875.
13. Ajzen I. The theory of planned behavior. In: Van
Lange PAM, Kruglanski AW, Higgins ET, eds.
Handbook of theories of Social psychology, vol. 1. Thou-
sandOaks,CA:SagePublicationsLtd;2012.p.438–459.
14. Ajzen I. The theory of planned behavior. Organ
Behav Hum Dec 1991;50:179–211.
15. FlemingML, Barner JC, Brown CM, ShepherdMD,
Strassels S, Novak S. Using the theory of planned
behavior to examine pharmacists’ intention to utilize
a prescription drug monitoring program database.
Res Social Adm Pharm 2014;10:285–296.
16. Gavaza P, Fleming M, Barner JC. Examination of
psychosocial predictors of Virginia pharmacists’
intention to utilize a prescription drug monitoring
program using the theory of planned behavior. Res
Social Adm Pharm 2014;10:448–458.
17. Amin ME, Chewning B. Predicting pharmacists’
adjustment of medication regimens in Ramadan us-
ing the Theory of Planned Behavior. Res Social
Adm Pharm 2015;11:e1–e15.
18. Herbert KE, Urmie JM, Newland BA, Farris KB.
Prediction of pharmacist intention to provide Medi-
care medication therapy management services using
the theory of planned behavior. Res Social Adm
Pharm 2006;2:299–314.
19. Gavaza P, Brown CM, Lawson KA, Rascati KL,
Wilson JP, Steinhardt M. Examination of pharma-
cists’ intention to report serious adverse drug events
(ADEs) to the FDA using the theory of planned
behavior. Res Social Adm Pharm 2011;7:369–382.
20. Walker A, Watson M, Grimshaw J, Bond C.
Applying the theory of planned behaviour to phar-
macists’ beliefs and intentions about the treatment
of vaginal candidiasis with non-prescription medi-
cines. Fam Pract 2004;21:670–676.
21. Pradel FG, Obeidat NA, Tsoukleris MG. Factors
affecting pharmacists’ pediatric asthma counseling.
J Am Pharm Assoc 2007;47:737–746.
22. Witry MJ, Doucette WR. Community pharmacists,
medicationmonitoring, and the routine nature of refills:
aqualitative study.JAmPharmAssoc2014;54:594–603.
23. Odukoya OK, Chui MA, Pu J. Factors influencing
quality of patron interaction at community phar-
macy drive-through and walk-in counseling areas.
Int J Pharm Pract 2014;22:246–256.
24. Patwardhan PD,AminME, Chewning BA. Interven-
tion research to enhance community pharmacists’
cognitive services: a systematic review. Res Social
Adm Pharm 2014;10:475–493.
25. Goel P, Ross-Degnan D, Berman P, Soumerai S.
Retail pharmacies in developing countries: a
behavior and intervention framework. Soc Sci Med
1996;42:1155–1161.
26. Smith F. The quality of private pharmacy services in
low and middle-income countries: a systematic re-
view. Pharm World Sci 2009;31:351–361.
27. Worley MM, Schommer JC, Brown LM, et al. Phar-
macists’ and patrons’ roles in the pharmacist-patron
relationship: are pharmacists and patrons reading
from the same relationship script? Res Social Adm
Pharm 2007;3:47–69.
Related Documents











