1 Center of Strategic Health Studies CSHS Dissertation Uncontrolled prices & profit margins of pharmaceutical products at Syria. Health Economics, Policy & Finance Maher ALAREF

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

1
Center of Strategic Health Studies CSHS
Dissertation
Uncontrolled prices & profit margins of pharmaceutical
products at Syria.
Health Economics, Policy & Finance
Maher ALAREF

2
This dissertation submitted to Liverpool University, Faculty of Health and Life Science
at December 2011 and accredited a Mater Degree of Health Economics, Policy and
Finance.
3
Acknowledgments
All through the hard road of this Master , many great people and true supports were an
essential tool of my life and study . Unforgettable names by heart and mind added lots of
special moments and enormous help to me :
Prof. Roy CarrHill , my great master and friend , (Cheers !)
Miss Dima Alrashee , the hard worker tutor that handled most of our irrational
attitude as big students .
Dr. Raghad Taqieldien , her continuous support and understands finally brought
us to where we should be.
Dr. Orwa Alabdullah , the friend indeed whom his contribution to this work was
more than a need .
My father , father in low and big brother their financial support made this master.
My mother and mother in low , your brays and tears weeded this work to tree.
My first princes Lolita (Leen) , her sweet words and talk meant to me all the
energy was needed.
And last but not least , our great teachers whom their knowledge and experience
were beyond our expectations :Talaium Jebara, Peter Cosgrove, Detlef Schwefel,
Peter West, Alan Maynard, Cor Jonker and many other great names , we had an
endless benefit for our country and mind out of your words.
4
Table of contents:
1- Introduction 6
2- Importance of research 10
3- Literature Review 12
4- Aim and Objectives 20
5- The framework of research design 20
6- Methodology and Methods 22
I. Research Methodology 22
II. Research Setting 23
III. Research Sampling 24
IV. Research Methods 25
7- Research Procedures 26
8- Data Analysis 27
9- Results 27
10- Discussion 31
11- Conclusion 32
12- Recommendations 35
13- Limitations 37
14- Appendixes 38
15- References 43
5
Abstract
Introduction: The Syrian pharmaceutical market is considered to have a valuable
and supportive effect on the overall Syrian National economics. The Syrian
pharmaceutical market is regulated by MoH. However, there are several factors which
affect the competition between the pharmaceutical firms such as bonuses which also
affect the profit size of these firms. Moreover, these factors could affect the people
demand and the quality of the pharmaceutical products.
Aim of the Research: This research aimed to identify the role of bonuses and their
effectives on the Syrian pharmaceutical market. Moreover, this inquiry aimed to identify
and study the factors which support these incentives.
Methods: This inquiry was considered as a case study which was conducted in
order to study a single and unique case of the pharmaceutical sector. In this inquiry,
both qualitative and quantitative methodologies were used by preparing questionnaire
to be fulfilled by targeted pharmacists, in addition to semi-structure interviews with
public and private stakeholders.
Results: Bonuses size showed significant relationships with several factors such as
buying rate, therapeutic category, pharmacist’s price. However, there was no
relationship between bonuses size and quality of the pharmaceutical products.
Conclusion: The current feature of the pharmaceutical market in Syria as a vicious
circle of several overlapped factors which are combined together to form the series of
the overall Syrian pharmaceutical market picture. The pharmacists’ behavior in selling
the pharmaceutical products as OTC or ethical, along with his ethics, is key factor to
start any solutions of controls.
6
1- Introduction:
Pharmaceutical expenditures are witnessing a rapid increase in many countries
which result in additional concerns in the pricing sector of pharmaceuticals. Therefore,
many countries have been creating and developing some form of expenditure regulation.
Actually many countries worldwide are, nowadays, applying the pharmaceutical
regulations in order to limit the cost of the pharmaceutical bills. The pharmaceutical
marketplace creates several forms of competitive market wherein each firm seeks to
achieve a fast product manufacturing and selling by spending billions of dollars on
marketing activities to maximize overall revenue (Bhatia et al, 2006, p.3).
Comparing the pharmaceutical market to the normal competitive market is irrational
and illogical. Consumers among normal market are to a certain extent able to ensure
that they get value for money. However, it is completely unavailable within the
pharmaceutical market where the individuals are unable to ensure the value of the
pharmaceutical product by themselves. Moreover, the intervening role of governments
in the pharmaceutical market could lead to distortion of the competitive market
operation. Actually the current regulations of the countries were introduced from the
perspective of people protection. These regulations are concerning the intrinsic efficacy,
safety and quality of pharmaceuticals, as well measures to raise the standard of
prescribing and promote the appropriate use of medicines (Capri, S. & Levaggi, R, p.2).
Pharmaceutical expenditure and drug procurements, in developing countries, account
for 20 to 50 % of public health budgets. The key condition for improving national health
indicators is making essential drugs available for everyone at affordable prices.
Moreover, the role of corruption in pharmaceutical and medical supplies procurement
and distribution result in reducing the access to essential medicines, particularly for the
most vulnerable groups. In addition, the performance of the health system in any
country is affected by the inadequate provision of drug and medical supplies (U4
partner agencies).
Prices as it is considered to be the means for regulating access in free markets, is a
method by which goods are distributed depending on private desires. Therefore,
governments should create the optimal incorporation of the pharmaceutical market
among the overall policy to achieve the objectives of the health sector. The regulating
role of government regarding pharmaceutical pricing is to ensure affordability and
equitable access, and to rationalize drug consumption and control price growth in order
to avoid excessive costs resulting in additional societal burdens. Therefore, governments
are seeking for the uniformity of the similar pharmaceutical products’ across the
country. In low-income developing nations, the focus is on improving access, while in
developed countries, the challenge is on cost control. However, several mid-income
developing nations face both challenges. Therefore, as there are market imperfections,
7
there are imperfections associated with government criteria of pricing. The process can
be difficult and prone to political manipulations. Indeed, there are several alternatives
by which the governments can achieve the same goals such as price control. By applying
financing methods, governments might guarantee the access to health care system by
individuals such as the expansion of insurance coverage. Moreover, expand the basic
information in order to enhance the price competition, limit the competition between
pharmaceutical firms by the use of compulsory licensing for products and the use of
generic forms in prescribing and labeling. Government can make a control on drug
expenditure through different ways such as prescribing control and incentives margins
such as bonuses which are frequently overlooked. Distribution margins also contribute
directly to pharmaceutical costs, and can affect products categorization and total
pharmaceutical consumption (WHO, 1998).
The pharmaceutical industry is relatively young in Syria. A little over 20 years ago, Syria
had to import over 82% of its drug requirements, and there were only two state-owned
factories supplying the bulk of the country’s pharmaceutical products. That is now a
thing of the past. Since then, dozens of companies have been established and local
production is estimated to cover around 90% of demand. Nowadays, capacity is
estimated to be twice the local market demand, which in turn is estimated at around
US$750 million per year. Despite having grown exponentially in the last five years,
pharmaceutical exports are still modest. According to the statistics of the Scientific
Council for National Pharmaceutical Industries
In the eighties, Syria imported medicine with a cost of around USD 600 million
each year, and now Syria ranks second among Arab countries after Egypt in covering
local needs, and also ranks second among Arab countries after Jordan in export. The
Syrian pharmaceutical industry ranks first among the country's industries, and is
considered the primary resource for supporting national economy.
The Syrian pharmaceutical industry has developed during the past years to
become one of the main industries that support national economy through export,
which amounts to over USD 120 million. According to the statistics of the Scientific
Council for National Pharmaceutical Industries, this industry provides 25,000 job
opportunities, 25% of which are university graduates.
Pharmaceutical products, which amount to USD 500 million, provide more than
92% of the local market's needs, lowering the amount of imports to less than 10%. The
public sector produces 7% of the overall Syrian production; with the private sector
producing the rest. The yearly production size is approximately 500 million dollars, 350
million of which is for the local market while the rest are exported worldwide. Syria
exports pharmaceutical products to 56 countries, mostly Arab and African countries and
8
some Asian countries, with exports to European countries beginning recently.(AMS
DATA)
According to a public stockholder Strict control is exercised by the ministry of
Health (MOH) over the industry. The MoH which established a Good Manufacturing
Practice guideline in conjunction with the World Health Organization enforces strong
quality controls and has the capacity to close outright any plant that does not abide by
its standards. The MOH also sets the price of any drug that is produced and sold in Syria
with the aim of making medicines available to all segments of society. MOH also
controls the price of any drug that is produced and sold in Syria.
According to Syrian MoH, currently, there are 66 licensed firms producing
pharmaceutical products in the country. Fifty-four have acquired ISO 9001 certification,
while 49 are ISO 14001 certified and 28 are ISO 18001 certified, in addition to
compliance with the international Good Manufacturing Practices GMP specifications.
Syria has the largest number of pharmaceutical companies compared with any other
Arab market, even though its domestic market size is smaller than many others. Private
capital inflows have increased significantly in the last decade thanks to the involvement
of several major industrial and trading groups in the drug industry.
The MoH sets prices according to a formula that includes all production and marketing
costs, plus a 20 percent profit margin for the manufacturer, see appendix 2 (MoH,
2009). Prices of Licensed products are usually set at around a 50 percent premium. The
strong price controls exercised by the Ministry have two negative consequences: first is
psychological as many patients are often reluctant to buy cheap medicines that they
associate with poor quality; the other is that the downward pressure on prices is forcing
some manufacturers to limit costs and research and development.
9
2- Importance of research :
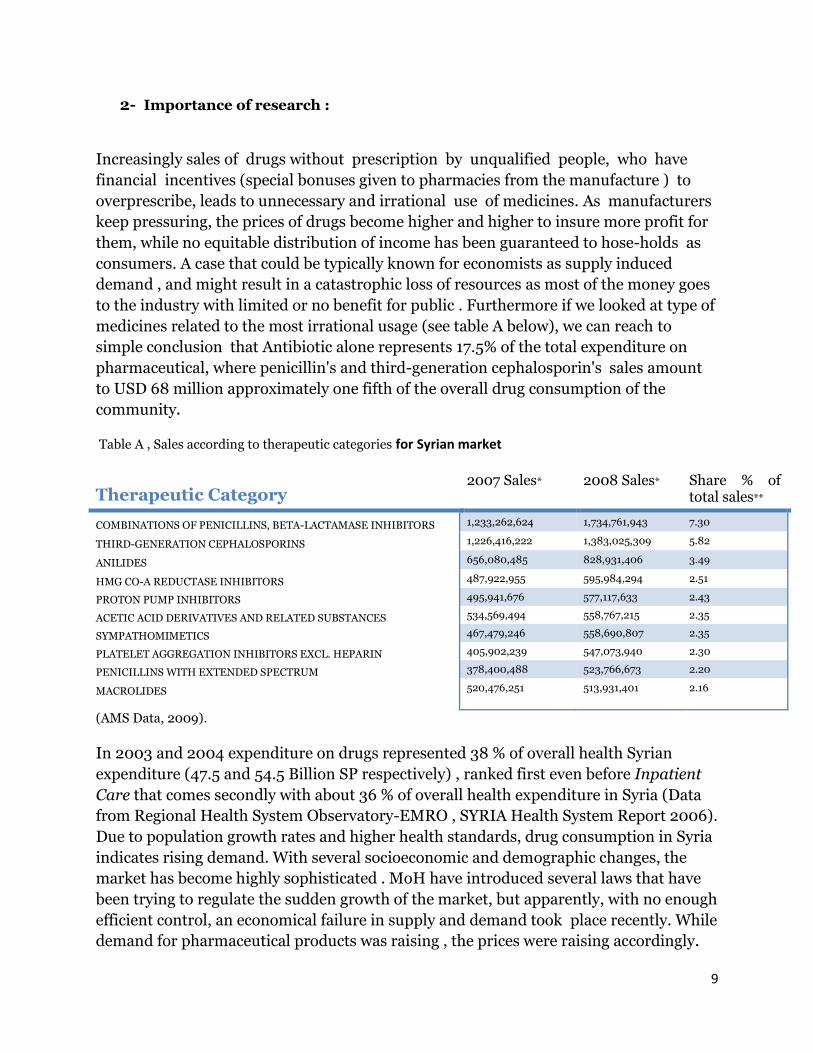
Increasingly sales of drugs without prescription by unqualified people, who have
financial incentives (special bonuses given to pharmacies from the manufacture ) to
overprescribe, leads to unnecessary and irrational use of medicines. As manufacturers
keep pressuring, the prices of drugs become higher and higher to insure more profit for
them, while no equitable distribution of income has been guaranteed to hose-holds as
consumers. A case that could be typically known for economists as supply induced
demand , and might result in a catastrophic loss of resources as most of the money goes
to the industry with limited or no benefit for public . Furthermore if we looked at type of
medicines related to the most irrational usage (see table A below), we can reach to
simple conclusion that Antibiotic alone represents 17.5% of the total expenditure on
pharmaceutical, where penicillin's and third-generation cephalosporin's sales amount
to USD 68 million approximately one fifth of the overall drug consumption of the
community.
Table A , Sales according to therapeutic categories for Syrian market
(AMS Data, 2009).
In 2003 and 2004 expenditure on drugs represented 38 % of overall health Syrian
expenditure (47.5 and 54.5 Billion SP respectively) , ranked first even before Inpatient
Care that comes secondly with about 36 % of overall health expenditure in Syria (Data
from Regional Health System Observatory-EMRO , SYRIA Health System Report 2006).
Due to population growth rates and higher health standards, drug consumption in Syria
indicates rising demand. With several socioeconomic and demographic changes, the
market has become highly sophisticated . MoH have introduced several laws that have
been trying to regulate the sudden growth of the market, but apparently, with no enough
efficient control, an economical failure in supply and demand took place recently. While
demand for pharmaceutical products was raising , the prices were raising accordingly.
Therapeutic Category 2007 Sales* 2008 Sales* Share % of
total sales**
COMBINATIONS OF PENICILLINS, BETA-LACTAMASE INHIBITORS 1,233,262,624 1,734,761,943 7.30
THIRD-GENERATION CEPHALOSPORINS 1,226,416,222 1,383,025,309 5.82
ANILIDES 656,080,485 828,931,406 3.49
HMG CO-A REDUCTASE INHIBITORS 487,922,955 595,984,294 2.51
PROTON PUMP INHIBITORS 495,941,676 577,117,633 2.43
ACETIC ACID DERIVATIVES AND RELATED SUBSTANCES 534,569,494 558,767,215 2.35
SYMPATHOMIMETICS 467,479,246 558,690,807 2.35
PLATELET AGGREGATION INHIBITORS EXCL. HEPARIN 405,902,239 547,073,940 2.30
PENICILLINS WITH EXTENDED SPECTRUM 378,400,488 523,766,673 2.20
MACROLIDES 520,476,251 513,931,401 2.16

10
Pharmaceutical industry should be powerful partners of the MOH as it constitutes
a back bone of the health care system and expenditure .
Recently issued law by the MoH that stated a 20% deduction on price for almost 70% of
the products existing in the market ( see appendix 3) clearly demonstrate the big effort
of the ministry to overcome the same problem this research is trying to highlight. While
the previously mentioned law was enforced immediately, no available data were found
later to evaluate wither it achieved its purpose or not. This research might help in one of
its objectives to investigate more about the results of this law .

11
3- Literature Review:
Expenditures on prescribed drugs account for a remarkable large size share of total
health care expenditures these days compared with 10 years ago. In addition, the
gradual increasing in the costs of prescribed drug affect consumers along with health
plans. Consumers struggle with financially managing their prescription drug regimens
while health plans attempt to provide comprehensive benefits at affordable prices (Scott
et all, 2007).
Unfortunately, the available researches regarding physicians’ prescribing behavior are
inadequate. Several studies in France have shown that physicians remain rather
insensitive to economic determinants as long as they do not bear the cost. The main
factors contributing to doctor prescribing behaviour are the doctor age (and the role of
patient’s age). Other studies have also shown that the doctor’s risk aversion might also
affect the prescribing behaviour (S. Jacobzone., 2000).
Figures which might give us a clue for what Pharmaceutical industry spend to market its
product can be obtained from published reports of IMS*, Verispan, CAM or Angell. But
as the method of calculations differ, the figures become vague, here are some recent
estimates from different recourses :
$20.4 billion in 2007
$29.8 billion in 2005
$57.5 billion in 2004
$54 billion in 2001 * IMS and Verispan are companies which initiate their researches regarding pharmaceutical marketing after
collecting data from industry. However, CAM collects industry marketing data directly from doctors. Angell
estimation was based on Novartis annual reports which distinguish marketing from adminstiration.
According to (S. Jacobzone., 2000), in the United States, the marketing variables for the
pharmaceutical firms include direct sales calls, advertising directly to consumers,
advertising in medical journals and advertising at various physician meetings. Actually
it is very important for pharmaceutical firms to estimate the increase in the number of
new prescriptions written for the particular drug.
It is assumed that the structure for the industry should be concluded through research
and developing in order to create patented drugs in addition to marketing and
competition. Although many countries negotiate prices product-by-product, a few
regulate the profits of pharmaceutical firms. Product-by-product price fixing has been
chosen when a universal health-care system prescribes pharmaceuticals products, and
to improve the patient access without financial determinants, and when public funds are
limited. Product-by-product price fixing may involve distortions and it is complicated to
review since it can bias statistical instruments such as price index. Additionally, in order
to control health expenditure, governments need to control volumes of consumption
12
through worldwide budgets. When countries have faced financial restrictions, especially
in Europe, attempts to stabilize expenditure have involved price cuts, or lower
compensations. This may result in short-term securing and has generally, however, left
the essential rate of growth of expenditure on pharmaceuticals unchanged.
Reforms of pharmaceutical policies need to promote efficiency and preserve equity. This
can be approached through increased market pressure to create competitive prices for
non-patented pharmaceutical products while allowing higher prices for those still on
patent. Actually the recent experience from OECD countries (Organization for Economic
Co-operation and Development) indicate a remarkable success in this sector. Nowadays,
several countries and health systems are using the reference pricing system for non-
patented products and the use of generic pharmaceutical products has been increased in
many countries. A few countries have produced additional plans regarding
pharmaceutical products pricing. They introduced a test of cost effectiveness before new
drugs will be accepted. In order to improve the cost-effectiveness of prescribing, an
advanced management methods were derived from controlled and managed care
settings and tools. These methods are also influential measures to assess the best value
for money (S. Jacobzone., 2000, p.3-4)
Actually the main goal of the pharmaceutical firms is to market and get rid of their
goods in a rapid manner and best values. Therefore, these firms are in a continuous
developing in of a new method to market and sell the pharmaceutical products. The
“detailing” process is one of the most important and expensive marketing method, it
involves a medical representative from the company to visit Doctors clinic and promote
a product or more by giving specific encouragement details. “Detailers” precise
information about what each physician prescribes by collecting data about purchased
drugs from retail pharmacies.
The use of pharmaceutical “detailing” is on the rise. As the method becomes more
frequent, it becomes increasingly competitive and sometimes on illegal manner.
Industry sales reps have a harder time keeping a doctor’s attention or even getting
through the office door.
“Gifts” and offer meals are ways to make friends with office staff and get time with
doctors (Horner, et al, 2006).
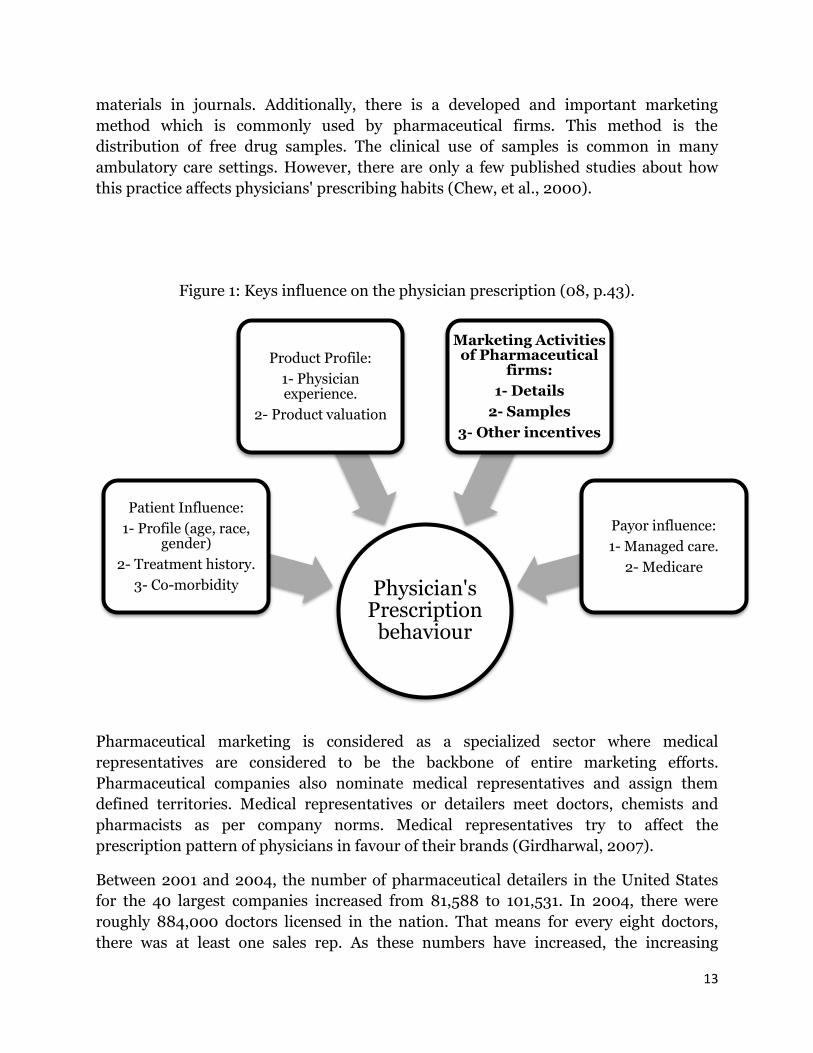
There are several factors which are considered to influence the physician’s prescription
behavior. Although these factors vary between countries and prescribers, the main
factors are clarified in this figure (Bhatia et al, 2006).
In U.S.A, drug advertising and marketing process have been shown to affect physicians'
prescribing behaviors, with an estimated $12 billion a year spent on drug advertising
and marketing (Humaidi, 2008). Nowadays, pharmaceutical companies use several
approaches to advertise and market their pharmaceutical products. They developed
techniques such as hospital and office detailing by pharmaceutical representatives,
direct-to-consumer advertising television advertisement, magazines, and printed
13
materials in journals. Additionally, there is a developed and important marketing
method which is commonly used by pharmaceutical firms. This method is the
distribution of free drug samples. The clinical use of samples is common in many
ambulatory care settings. However, there are only a few published studies about how
this practice affects physicians' prescribing habits (Chew, et al., 2000).
Figure 1: Keys influence on the physician prescription (08, p.43).
Pharmaceutical marketing is considered as a specialized sector where medical
representatives are considered to be the backbone of entire marketing efforts.
Pharmaceutical companies also nominate medical representatives and assign them
defined territories. Medical representatives or detailers meet doctors, chemists and
pharmacists as per company norms. Medical representatives try to affect the
prescription pattern of physicians in favour of their brands (Girdharwal, 2007).
Between 2001 and 2004, the number of pharmaceutical detailers in the United States
for the 40 largest companies increased from 81,588 to 101,531. In 2004, there were
roughly 884,000 doctors licensed in the nation. That means for every eight doctors,
there was at least one sales rep. As these numbers have increased, the increasing
Physician's Prescription
behaviour
Patient Influence:
1- Profile (age, race, gender)
2- Treatment history.
3- Co-morbidity
Product Profile:
1- Physician experience.
2- Product valuation
Marketing Activities of Pharmaceutical
firms:
1- Details
2- Samples
3- Other incentives
Payor influence:
1- Managed care.
2- Medicare
14
competition has resulted in the pharmaceutical industry pushing their products ever
more aggressively (Horner et al., 2006).
In 2007, and according to estimation, there were slightly less than 95,000 reps, up from
88,000 in 2001. In other words, this is about 1 rep for every 7 doctors (based on
95,000/663,000). However, many physicians are in non-clinical roles, in rarely visited
rural practices, or refuse to see representative (Pharmaceutical Industry Marketing,
2009).
As mentioned, individual pharmaceutical firms representatives meet with doctors and
pharmacists to promote specific prescription in a marketing method called ‘detailing’.
Each detail consists of the sales representative sharing information regarding the
medications, efficacy and side effects of the drug in clinical studies. Most currently
literature found a significant effect of detailing on physicians prescribing and find
physicians to be unrelenting in their prescription patterns (Bhatia et al., 2006, p.4)
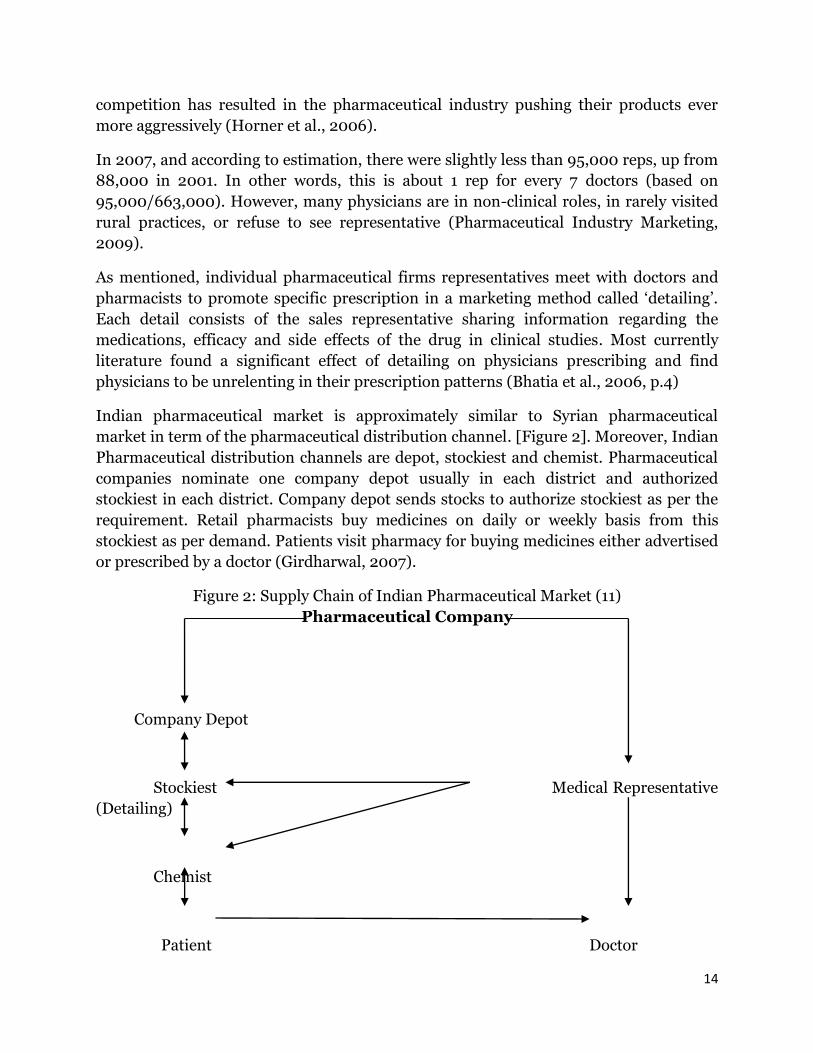
Indian pharmaceutical market is approximately similar to Syrian pharmaceutical
market in term of the pharmaceutical distribution channel. [Figure 2]. Moreover, Indian
Pharmaceutical distribution channels are depot, stockiest and chemist. Pharmaceutical
companies nominate one company depot usually in each district and authorized
stockiest in each district. Company depot sends stocks to authorize stockiest as per the
requirement. Retail pharmacists buy medicines on daily or weekly basis from this
stockiest as per demand. Patients visit pharmacy for buying medicines either advertised
or prescribed by a doctor (Girdharwal, 2007).
Figure 2: Supply Chain of Indian Pharmaceutical Market (11)
Pharmaceutical Company
Company Depot
Stockiest Medical Representative
(Detailing)
Chemist
Patient Doctor
15
In a study conducted in India in order to illustrate the most important factors
influencing prescription behavior of physicians has found that the regular visit of
medical representative of pharmaceutical companies was the fifth factor followed by the
personality of medical representative as the eighth factor. However, the price of product
was the second factor while prescribing a medicine. The study has indicated according
to physicians’ comment that the best tool of promotion for the pharmaceutical industry
is the regular visit by a smart, experienced, skilled and well trained representative. The
role of this representative is considered as an influencing factor by which the
pharmaceutical company has its effect on physician prescription behavior when the
representative presents a well prepared presentation explaining about the product. In
addition, the representatives may offer additional informal incentives such as a
sponsorship for conferences or personal visit to a medical event. These incentives are
considered to be very effective tools used by the pharmaceutical companies by which the
stimulate physicians to prescribe their products. Furthermore, several pharmaceutical
companies use the personal gifts and free drug samples as other incentives for
physicians. Regarding to factors which help in product recalling by physicians,
physicians have to remember several brands or products of several pharmaceutical
companies. The study has concluded that advertising pictures which are gifted by the
pharmaceutical company play an effective role in brand recalling. The competition
status between the pharmaceutical companies is obvious by their pressure on physicians
to shift from one brand to their own brand in same therapeutic category. According to
the same study, which involved 100 physicians; 86% of them has been shifting their
prescription from one brand to another because of several influenced factors. Among
the influenced factors, the regular visits and persistence of the pharmaceutical industry
representative in addition to the promotional efforts of the pharmaceutical company
were the third and forth factors respectively (Girdharwal, 2007).
Sporling et al have carried out an analysis of 58 studies in order to explain the effect/
role of detailing on physician behaviour. The results have indicated that 38 studies
confirmed the statement that physicians who are detailed by pharmaceutical
representative tend to prescribe the brands of these firms more than other brands.
Furthermore, Sporling has found that this behavior lead to more expenditure by
patients for drugs which are not the best for patients’ health status (SANA, 2010).
Generic drugs are drugs with the same chemical compound, including the same
International Common Denomination. However, differ on their trade names. Products
which are off-patent can be sold as generic drugs at a much lower price. Recently, with
the time limit on patents expiring for an increasing number of products, and the need to
save generate, the concern in generic drugs has grown. (S. Jacobzone, 2000, p.21).
Pharmaceutical companies use their medical representatives to update physicians’
knowledge as a source of information about their brands. Medical representatives and
mailers from pharmaceutical companies were the third and forth source of information

16
respectively by which physicians update their knowledge about generic drugs. The role
of pharmaceutical companies is to update physicians’ knowledge using their own brand
instead of generic drug. Nowadays, pharmaceutical companies are trying to develop
other incentives in order to stimulate physicians to prescribe their products. Several
companies have developed relationship marketing by which they use the regular events
related to physician as way to produce their incentives and gifts such as birthdays and
undertaking high positions such a director or dean of medicine. The study has resulted
that 42% of physicians are influenced by these relationship (Girdharwal, 2007).
These results are meeting with those concluded from an economic conducted survey
which states that consumers’ demand for drugs tends to be sensitive to price, but the
sensitivity varies across different groups of patients in term of socioeconomic level.
However, physicians' prescribing behavior seems to show little sensitivity to economic
factors. (S. Jacobzone, 2000, p.5).
Pharmaceutical firms have contracted with many hundreds of physicians to serve on
their advisory boards for which they are well compensated. These firms have additional
affective incentive such as offering the continuing Medical Education (CME) which
physicians are required to earn free of charge their speciality certification. Moreover,
these firms produce payment for attending “scientific” conferences and scholarship,
pharmaceutical samples, and grants for research projects (Horner, et al, 2006).
Although, pharmaceutical firms’ marketing plans are directed toward physicians,
medical students are involved in these plans as well. Regarding to this issue, a study has
conducted in Canadian academic centre (University of Western Ontario) in order to
assess the attitudes of medical students regarding to pharmaceutical promotion
including the gifts, free drug samples, and incentives. 202 first, second and fourth-year
medical students were involved in this study. 59% of students did not agree with the
statement that medical students should not have any interaction with pharmaceutical
firms’ marketing. Furthermore, 49% of students agreed with the statement that it is
acceptable for medical students to receive gifts and incentives from a pharmaceutical
firm. In term of prescriptions, 17% of participants indicated that they will prescribe the
drug brands from the pharmaceutical firms that provided them with gifts or incentives
rather than brands from drug firms that did not interact with them through incentives,
gifts, and free samples. 81% of students stated that pharmaceutical industries are
primary interested in profits beside the interests of physicians and patients. Moreover,
while 24% of students believed that information relevant to drug effectiveness from
pharmaceutical firms is undependable, about 39% of students believed that this
information is trustworthy. 36% of them were neutral regarding to this issue (Barfett et
al., 2004).
Free samples are one of the most marketable ways to make advertising about any
product. However, in term of pharmaceutical sales, this issue will raise a lot of questions
17
to minds. Pharmaceutical companies offer huge amounts of incentives as free samples to
physicians and healthcare facilities. Although these companies have the right to market
their products in a way which is considered to be the proper way, the marketing
procedures should be restricted by certain criteria relevant to the pharmaceutical
products’ quality regardless of other incentives which are sometimes considered to be
informal method of pharmaceutical marketing. The potential problem in this way of
marketing is the probability of this method to develop to a competition by which the
national and foreign pharmaceutical companies will launch their products using this
“informal” method to increase sales regardless to the safety and rational
recommendations of drug consumption. Moreover, from the patients’ perspective, there
are several effects on patients which are resulted by this method. This competition, in
addition to the wide prevalence of the same pharmaceutical product with several trade
names besides the point of product quality will result in the “informal incentives” way
amongst physicians and pharmacists in order to guarantee better sales and revenues
(Humaidi, 2008).
According to (Bhatia et al, 2006) the optimal distribution of detailing depending on
response parameters assessed by using a surrogate allocation mechanism by allocating
detailing using the data on the percentage of new patients for each doctor along with the
prescription cost information.
The three specific allocations tested here are:
Same detailing to each physician (base case)
Prescription cost based allocation (current industry practice)
Prescription cost and percentage of new patients based allocation (our
recommendation)
Regarding this issue, a study was conducted to study the role of detailing on doctors’
prescribing behaviors. The found that allocating more detailing resources (as currently
used by the industries) works better than allocating the same detailing per physician.
Moreover, the study also found that the prescription costs and percentage of new
patients based allocation performs much better than the allocation based just on the
prescription volume (Bhatia et al, 2006, p.29-31).
Samples are always welcomed by patients and physicians. In addition to former drug
salesmen, some doctors and public health stakeholders and advocates suggest the free
pills are part of a developed marketing technique to encourage patients to buy costly
brand-name drugs. Free samples and bonuses also bypass pharmacists, who can give
these incentives to the patient (Favole, 2010).
A study conducted on free samples effectiveness found that patients who receive free
prescription samples spent approximately 40 percent more for medication during the

18
six months they got samples, and nearly 20 percent more in the six months afterward,
than those who didn’t.
“The notion that people have is that if you receive samples, it helps with out-of-pocket
costs because you don’t have to go out and buy the drugs,” said Anirban Basu, one of the
study authors and an assistant professor of medicine at the University of Chicago. He
added; “What we found, actually, was that their out-of-pocket expenditures increased.
Most surprising was that those out-of-pocket expenditures continued even after the
samples stopped.”
The study refreshes the debate regarding the role of more than $18 billion in free
pharmaceutical samples distributed each year, which drug firms’ representatives have
described as a cost-saving safety net for the poor.
“This builds on a growing body of literature that shows that samples are not aimed to
help the uninsured and the poor, but to increase the sales of the branded drugs,” said
Dr. William Shrank, an instructor at Harvard Medical School, who has studied the issue.
“However, Reason for higher costs isn't clear. Exactly why the costs rose wasn’t clear”,
said Alexander, who added that the study wasn’t designed to answer that question.
“Patients who received samples may have been sicker than those who didn’t, which
would explain the higher costs. But analysis showed that illness played a small part, at
most, in the higher expenses”, Alexander said. “Or, patients may have received higher-
priced brand-name drugs — those ones most often given as samples — and then
continued with the same pricey prescriptions”, Alexander added.
“We have known for a while that sample use increases health care costs,” said Leuchter.
“But the new study provides first details of out-of-pocket costs, including the fact that
the medication expenses remained high even after the samples were finished” (Aleccia,
2011).
When physicians listen to the detailers’ information, and have been the beneficiary of
free samples, gifts and others perks, it is not simply a matter for patients’ checkbooks.
While industry maintains that detailer reps produce the “education” for doctors about
important new drug forms. In addition, the message delivered by this detailer may not
be based on academic rules. Indeed, research stated that physicians are heavily relying
on detailers’ information and that the more doctors rely on commercial sources of
information, the less likely they are to prescribe drugs in a pattern consistent with
patient needs. Actually the information provided by detailers is often biased, and
sometimes seriously misleading.
According to the Food and Drug Administration, inaccurate information of
pharmaceutical sales detailers during their meetings with doctors were the fourth most
common source of false or misleading drug information observed in pharmaceutical
marketing. Studies show that many doctors ignored even the most serious safety
warnings required on prescriber information by the FDA (Horner, et al, 2006).
19
4- Aim & Objectives:
This research aims to suggest research-based recommendations regarding the current
situation of pharmaceutical market in Syria to form an optimal support regarding the
national economy, medical sector, and public demands.
1- To describe the current situation of Syrian pharmaceutical market and its
relationship with the overall Syrian economical market.
2- To asses if the Bonuses could be an indicator to what known as a Market Failure
between supply and demand, and to identify which major variables had lead to
this current situation.
3- To identify the possible solutions in order to deal with this imperfection.
5- The framework for research design:
The main purpose of this inquiry is to define the reason of pharmaceutical market
imperfection and clarify the reasons which lead to the current situation of informal
competition between pharmaceutical industries, which in turn could lead to inequality
in the gain amounts, in addition to its reflection on overall Syrian market and Syrian
economy as the pharmaceutical market considered as a backbone of Syrian economy.
Furthermore, by clarifying the current defect in the pharmaceutical market, we will be
able to establish the most suitable criteria and principles to be followed in order to reach
an optimal fairly status of the Syrian pharmaceutical industry. The theory of this study is
focused about the reality of the existence of serious imperfection in the Syrian
pharmaceutical market and illegal competition between Syrian pharmaceutical firms.
This failure is a result of unorganized relationship between the Syrian pharmaceutical
market control on one hand and illegal forms of pharmaceutical marketing. This
initiative theory of the research was based on in order to clarify the aim and objectives of
this research. Furthermore, this research will suggest research-based recommendation
in order to develop the current situation of Syrian pharmaceutical market to support in
an optimal way the Syrian economical market.
There are several questions which are going to be answered throughout this research
linked in with the based theory of the research; “The existence of a imperfection in
Syrian pharmaceutical market and illegal competition between Syrian pharmaceutical
firms using several informal ways”. Using this theory and in combination with the
gained data of this research and results, we tried to find logical answers of several
questions; what is the reality of the failure in Syrian pharmaceutical market, and what
are the most important factors which create the appropriate environment for Syrian
pharmaceutical firms to use their own illegal forms of competition to reach their annual
gains? Furthermore, what are the optimal solutions for this imperfection and how could
it be used in order to accommodate the Syrian pharmaceutical market with the overall
20
Syrian economical market? However, this enquiry will clarify other relevant theories
which will be needed to tackle through other researches.
As this inquiry is considered as a case study (the inquiry discussed the case of Syrian
pharmaceutical market and its assumed imperfection). Therefore, the study discussed in
general several points regarding the contribution of case study. According to (Singh,
2006, p.148) the points which should have discussed are:
The inclusion of this particular case under a specific category: this case is
categorized under an economical sector as the pharmaceutical market is
considered as a backbone for the overall Syrian economy.
The evaluation of this inquiry: by studying the case after the recommendations of
the inquiry take place.
The findings of the research depending on the statistical analysis and results will
be evaluated and analyzed critically. Moreover, these findings should have been
discussed in term of current pharmaceutical market, and will be compared with
the suggested or recommended market for Syrian pharmaceutical manufacturing.
The research will suggest the possible topics which may discussed as new
researches among pharmaceutical sector.
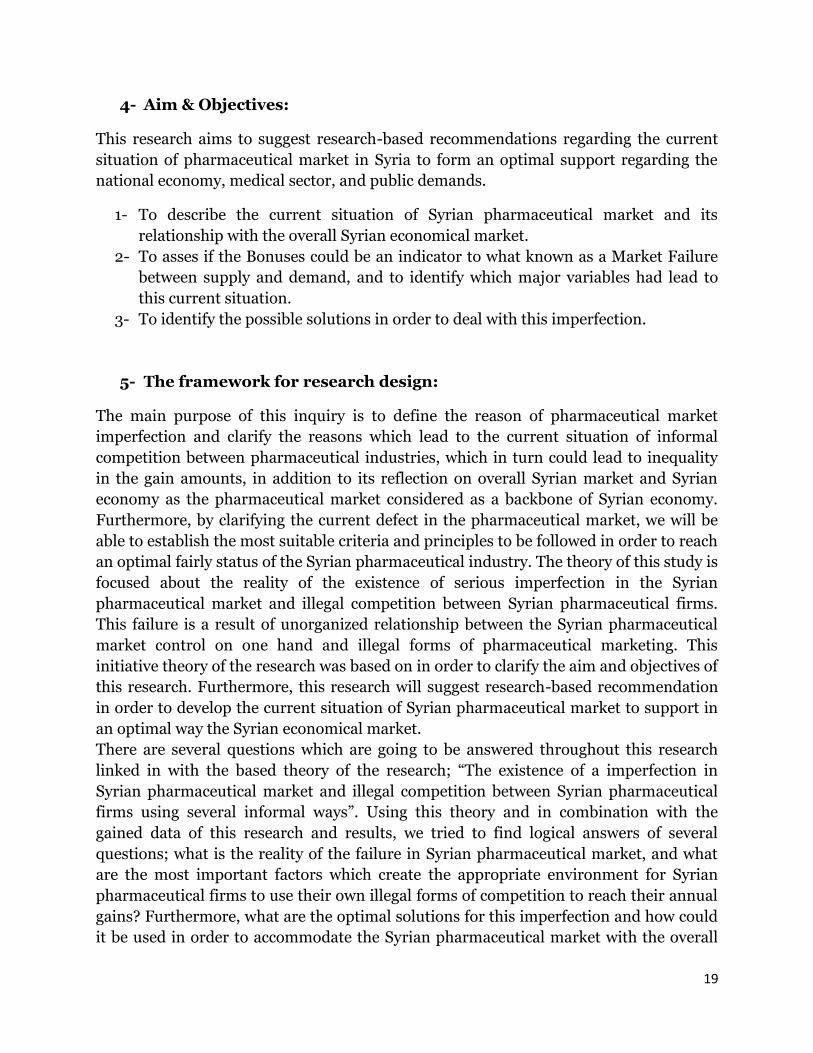
The logical studying of the Syrian pharmaceutical market as a specific case based on a
specific set of criteria in order to reach a logical findings and conclusion. According to
(Mohd Noor, 2008), the research was undertaken by discussing the following steps:
21
According to (Singh, 2006, p.292), the research was conducted following three main
phases:
Retrospective phase: the study discussed the pharmaceutical market in Syria in
term of history, recent development, and recent legislations regarding the
pharmaceutical market in Syria.
Prospective phase: the study analysed the current pharmaceutical market in Syria
in order to approach better understanding of the case. Thereupon, we can suggest
the optimal recommendations.
Conspective phase: depending on the interviews, questionnaires, and our
comprehension to the topic, and depending on our recommendations, the
researcher discussed the expectation of Syrian pharmaceutical market.
6- Methodology and Methods:
I. Research Methodology:
The research was conducted in order to assess the imperfection in the pharmaceutical
market in Syria. In addition, it was initiated in order to identify the main reasons behind
this assumed failure and conclude the available recommendations regarding this
imperfection to create the fairly situation regarding the relationship between the Syrian
pharmaceutical firms and the overall Syrian economical market. The researcher has
discussed aspects which can be quantified or expressed in term of quantity. In addition,
the research contains semi-structured interviews. The data collected through the
research explores the relation between specific variables expressed in quantitative terms
However, as this study is a unique study regarding the pharmaceutical market in Syria,
and there are no previous study regarding this issue, we used qualitative data to support
our results as a descriptive analysis in linked with pharmaceutical market in Syria and
the possible solutions. Therefore, this research is considered as quantitative-qualitative
mixed research.
As this research involves testing of our hypothesis, the underlying reasons which are
making the relationship with the hypothesis should first be confirmed and
operationalized, and then the deductive method will be followed (Gray, 2004, p.6).
Therefore, the issue regarding an existence of a failure in Syrian pharmaceutical market
was confirmed, and after confirming the underlying variables which are assumed to be
in relationships with the failure in pharmaceutical market and its effect on overall
economical market, we used a deductive process in order to test our hypothesis to
ensure the reality about the existence of this imperfection. Thereupon, and before
starting the interviews and collecting data, we operationalized some of our underlying
variables in order to make them measurable and we created some indicators to measure
collected data and make the desired comparison between the hypothesis and gained
data in one hand, and among the entire data themselves on another hand. These
22
procedures will be explained later throughout the progress of the research and will be
clarified on the whole.
This study was conducted in order to describe the current situation of Syrian
pharmaceutical market and its relationship with the overall Syrian economical market.
Therefore, this study is considered as descriptive enquiry. Furthermore, as we used the
already available facts regarding Syrian pharmaceutical market depending on several
interviews with public and private sector stakeholders, this study included an analytical
support to our data and results (Robson, 2002, p.292).
The suggested variables of this inquiry are related to the theory regarding the existence
of failure in pharmaceutical market. These variables are out of researcher’s control and
actually they are closely related to the theory. Therefore, the main design of this inquiry
is non experimental. Moreover, as this research deal with a particular situation or case
and involve an in-depth examination of a this single case to provide an accurate,
description, and complete analysis of this case to expand the knowledge and clarify the
current blurry situation of pharmaceutical market. Therefore, this study is considered as
non experimental case study (Marczyk et al, 2005, p.147-148). This case study research
attempted to capture as many variables as possible to identify how the complex set of
regulations, attitudes, facts and behaviors come together to produce the current
pharmaceutical market status in Syria (Hancock, 2002, p.6-7).
There was a close collaboration between the researcher and practitioners which was
done through the interviews with public and private stakeholders to collect information
on their attitudes and perspectives in pharmaceutical field. Moreover, our findings were
based on data which were collected by self administered questionnaire to pharmacists;
these findings leaded to clarify the reality of the pharmaceutical failure and identified
the main reasons behind this failure. In addition, the main aim of this research is to
create a change in the current situation of pharmaceutical market by research-based
recommendations. There upon and depending on previous facts, this research is
considered as an action research (Gray, 2004).
II. Research Setting:
The research procedures took place in several cities in Syria. The selection of these cities
was depending on the average of drug consumption for each city in Syria, and the total
average of drug consumption among these three cities was 72%. Of total consumption in
Syria of which 35% was in Damascus Meanwhile, the total consumption of
pharmaceutical products was 25% in Aleppo as the second ranked, and 12% for Homs as
the third ranked (according to Pharmex, the governmental pharmaceutical distribution
company).

23
III. Research Sampling:
There are several points should be taken in consideration in order to develop an
appropriate sample design:
Type of pharmacist sample: there are two types of samples in our research. The
first one is considered as human samples. The public and private stakeholders in
addition to the pharmacists are considered as human samples. Whereas, the
pharmaceutical products are considered as the second type of the sample.
Size of samples: the total numbers of pharmacists who were asked to be involved
in the research is 30.
Sampling frame: basing on the average of drug consumption among the
mentioned three cities, we decided to distribute our questionnaire to be filled out
by pharmacists among these three cities in a manner by which we accord the
average of total consumption for each of these three cities and the number of
targeted subjects (pharmacists) in each city. Of the total drug consumption in the
three cities 49% (of the 72%) was in Damascus 35% was in Aleppo and 16% in
Homs. Given these proportions, then the 30 questionnaires will distributed on 15,
11, and 4 in Damascus, Aleppo, and Homs respectively..
Sampling method: Actually the majority of pharmacists have the same
background regarding to the pharmaceutical marketing which is applied by
pharmaceutical companies in Syria. Therefore, we could rely on a convenience
sampling method in order to distribute the questionnaires.
On the other hand, regarding the pharmaceutical products, the sampling method
will be completely different from the previous one. In this part of the research
sampling, basing on the researcher’s practical knowledge of the research area
(pharmaceutical marketing) in an intellectual manner, the researcher chose the
most productive pharmaceutical products to answer the researcher question.
Therefore, and after taking on consideration that this research is directed in
order to explain a case study, this part of sampling was considered to be a
judgment (purposeful) sampling method. This study is considered to be a unique
study in Syria in term of its purpose. Therefore, an in-depth comprehension was
required to interpret our findings and relate them with the pharmaceutical
market situation in Syria. As the stakeholders (public and private) have the most
interaction with this situation, it was suggested to conduct self interviews with
them. The interviewees were suggested by the researcher and were considered as
additional targeted sampling units by interviews in order to make a descriptive
analysis for their interviews to support our findings. The method by which the
additional sample units were defined is a purposeful sampling method (Marshall,
1996).
24
IV. Research Methods:
This research was aimed to study the current situation of the pharmaceutical market in
Syria. Several variables were involved in the analysis in order to attain a holistic
comprehension for this case. A prepared list of the most 100 pharmaceutical product
was prepared by the researcher depending on the suggested factors by which the
pharmaceutical market is affected. This rating was according to AMS Data .Moreover, a
prepared questionnaire was set by the researcher to be self administered by 30
pharmacists. This questionnaire was directed to collect additional information for
several variables which are suggested to have a significant role in the pharmaceutical
marketing in Syria.
4-1- Pharmaceutical product variables according to AMS:
4-1-1- Pharmaceutical form: by which the product was manufactured.
4-1-2- Pharmaceutical company: which the pharmaceutical product is belonged
to. However, and for ethical and confidential purpose, during the analysis,
pharmaceutical companies’ names in addition to products’ names were ignored
and not mentioned in the results and replaced by numbers.
4-1-3- Pharmacist’s price: the estimation cost for each selected form unit which
was paid by the pharmacist to the pharmaceutical firm.
4-1-4- Pharmaceutical product’s classification according to MoH: OTC products
were classified as 1 and ethical products by 2. This classification was according to
the minister of health deputy for pharmaceutical affaires.
4-1-5- Therapeutic categories: depending on the products’ indications. Moreover,
the pharmaceutical forms were categorized among two main categories 1-
antibiotics: the most frequent therapeutic category. 2- other categories.
4-1-6- Units: number of the sold units by pharmaceutical firms for each product.
4-1-7- product manufacturing in term of its source whether it was imported,
under licensed(Brand), or locally manufactured(Generic) .
4-1-8- Product categorization depending on MoH definition whether it was
classified as Over The Counter (OTC) drug (purchased without medical
prescription), or as Ethical drug (dispensed only with prescription).
4-2- Pharmaceutical product variables among the pharmacists’ questionnaire:
4-2-1- Bonus: (informal incentive pharmaceutical products which are given to
pharmacists). This variable contained the number of free units given for every 10
or 100 buy units. Moreover, the total size of bonuses for each selected
pharmaceutical form was calculated by multiplying the total number of sold units
by the number of bonuses units divided by 10 or 100. Additionally, the total
25
market size for the total size of bonuses for each selected form was calculated by
multiplying the last variable by pharmacist’s price.
4-2-2- Discount: certain deducted percentage of the sold pharmaceutical product
bill value. This variable has a one-way reciprocal direct relationship with net
price variable.
The two previous variables are considered to be a significant part of the heart of
the pharmaceutical marketing matter in Syria.
4-2-3- Quality: each pharmaceutical product was rated according to the
pharmacists’ viewpoint by one of 3 main values; 1- good, 2- accepted, 3- ok.
4-2-4- Buying rate for each product: which referred the rating value of buying
average for each pharmaceutical product in the list. The variable was categorized
as following: 1- high-average of buying which pharmacist might buy on a weekly
bases , 2- Moderate-average of buying which pharmacist might buy on a monthly
bases, 3-low-average of buying as more than a month bases of buying .
4-2-5- Pharmaceutical product classification according to the pharmacist’s
behavior: the subject had asked to classify each of the 100 products according to
the way by which each product was sold. OTC products were classified by 1, and
the ethical products were classified by 2.
Bonus was categorized among new variable depending on bonus size:
0: No bonuses, 1: low bonus (1-2) units, 2: medium bonus (3-5) units, 3: high bonus
more than 5 units.
7- Research Procedures:
We were provided with AMS data by PharmaWare using a software programme.
According to this software, we chose the top 100 selling pharmaceutical product in
Syria. The list contained 562 entries of all forms and packaging sizes (1 product may give
11 different forms). Therefore, we took the most selling form as a percentage of overall
money selling size to make the data collection by the questionnaire is manageable.
Data were collected within a period of time from the 1st of December 2010 to 25th of
January 2011. The pharmaceutical drugs list was obtained from AMS data. A descending
sort was applied on the list depending on sells volumes by U.S dollars to draw out a list
of 100 pharmaceutical products. A self-administered questionnaire was designed and
distributed among the targeted pharmacists. The purpose of the research was orally
explained for each targeted pharmacist beside the written explanation. The
questionnaire was submitted to the pharmacist after an oral consent. The time of
submission was determined by the pharmacist. At the same time, a set of several
questions was prepared in order to be asked as a semi-structure interview. Questions for
each interview were selected according to the interviewee specialty (specialty based
semi-structure interview). The interview’s time was determined after a call contact
between Centre for Strategic Health Studies CSHS, Damascus and the targeted

26
stakeholder. The interviews were conducted, analysed, and the requested statements
were selected to support our findings by them.
8- Data Analysis:
Data analysis was performed using SPSS v.18 and Excel Microsoft.
The bonus values for every 100 product were transformed to represent every 10 product
units. After that, the mode for each product variables was identified and recorded as the
value for the variable. Actually there were no remarkable gaps regarding the values
which were filled out by pharmacists as they share same backgrounds in term of
pharmaceutical marketing methods.
9- Results:
Depending on AMS data, several analysis were performed in order to present the
current situation of pharmaceutical market in Syria.
According to AMS database, the market share of the 100 pharmaceutical products was
36.8% of the total pharmaceutical market size in Syria. Furthermore, the total market
size of the 100 product was 228,026,282 U.S dollars. However, the market size of the
selected top selling presentational form for each product was 141,964,182 U.S dollars.
From our Data and calculations explained above the total market size for bonuses of the
100 top selling product was 23,395,852 U.S dollars which forms 16.5% of the total
pharmaceutical size in Syria.
Local manufacturing was the prominent sector among the 100 products. While as 90
products were locally manufactured (26 were under licensed(Brands), and 64
locally(Generics), 10 products were imported.
Descriptive analysis was performed by studying the values which were provided by the
pharmacists. 58 products were sold by the pharmaceutical firms with informal
incentives (bonus). While among the 100 pharmaceutical products there was a single
case which had 15 bonus units , there were 2 different products which had 12 bonus
units. The most frequent number of bonuses was 2 which were presented with 11
different products. Table 1 expresses the frequency of pharmaceutical products
according to the bonus categories.
27
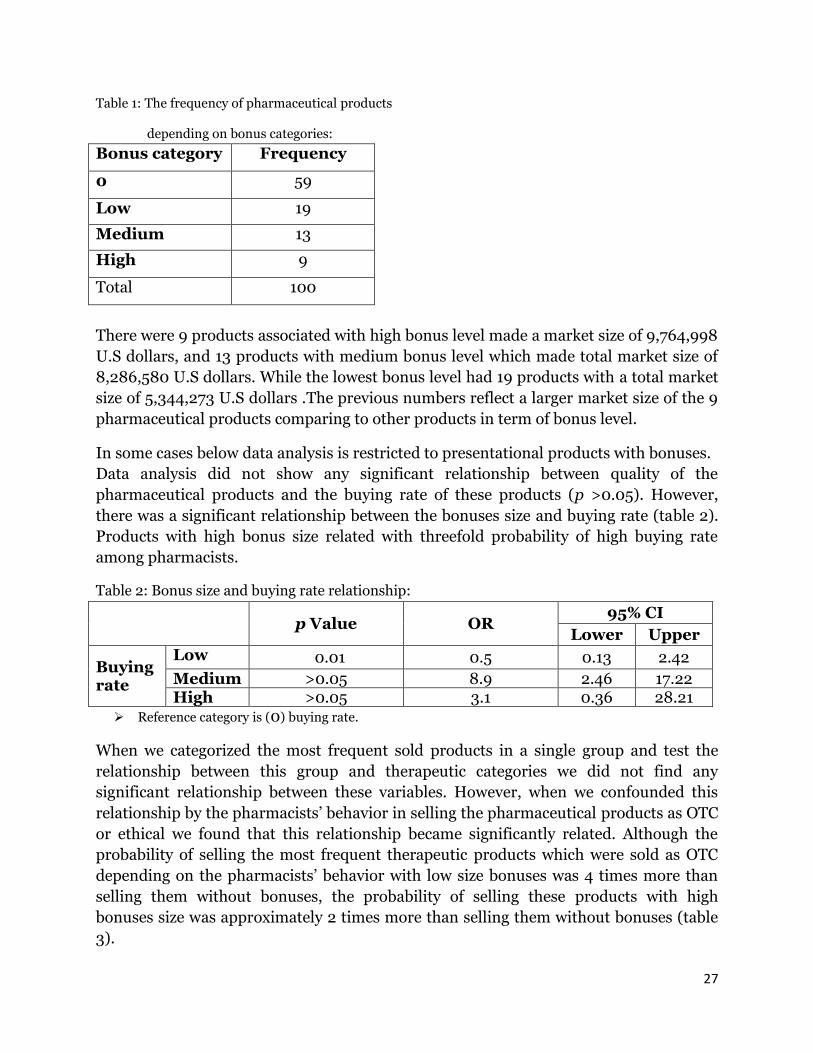
Table 1: The frequency of pharmaceutical products
depending on bonus categories:
Bonus category Frequency
0 59
Low 19
Medium 13
High 9
Total 100
There were 9 products associated with high bonus level made a market size of 9,764,998
U.S dollars, and 13 products with medium bonus level which made total market size of
8,286,580 U.S dollars. While the lowest bonus level had 19 products with a total market
size of 5,344,273 U.S dollars .The previous numbers reflect a larger market size of the 9
pharmaceutical products comparing to other products in term of bonus level.
In some cases below data analysis is restricted to presentational products with bonuses.
Data analysis did not show any significant relationship between quality of the
pharmaceutical products and the buying rate of these products (p >0.05). However,
there was a significant relationship between the bonuses size and buying rate (table 2).
Products with high bonus size related with threefold probability of high buying rate
among pharmacists.
Table 2: Bonus size and buying rate relationship:
p Value OR
95% CI
Lower Upper
Buying rate
Low 0.01 0.5 0.13 2.42
Medium >0.05 8.9 2.46 17.22 High >0.05 3.1 0.36 28.21
Reference category is (0) buying rate.
When we categorized the most frequent sold products in a single group and test the
relationship between this group and therapeutic categories we did not find any
significant relationship between these variables. However, when we confounded this
relationship by the pharmacists’ behavior in selling the pharmaceutical products as OTC
or ethical we found that this relationship became significantly related. Although the
probability of selling the most frequent therapeutic products which were sold as OTC
depending on the pharmacists’ behavior with low size bonuses was 4 times more than
selling them without bonuses, the probability of selling these products with high
bonuses size was approximately 2 times more than selling them without bonuses (table
3).
28
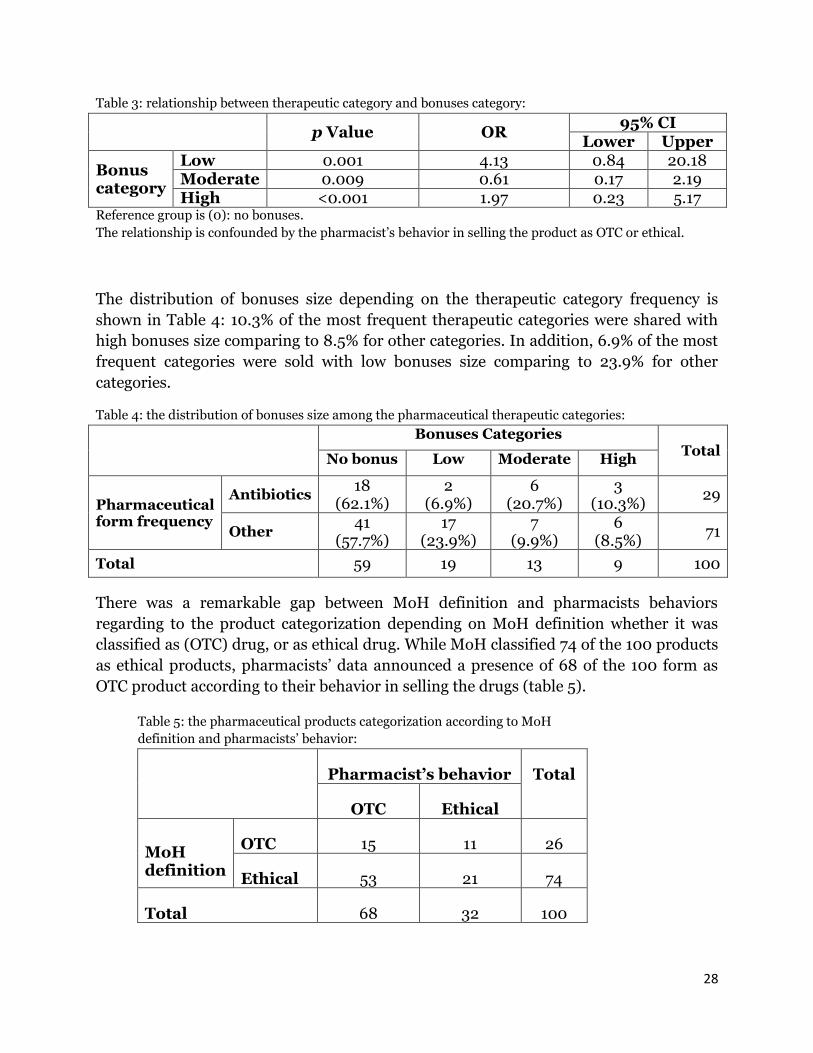
Table 3: relationship between therapeutic category and bonuses category:
p Value OR
95% CI Lower Upper
Bonus category
Low 0.001 4.13 0.84 20.18 Moderate 0.009 0.61 0.17 2.19 High <0.001 1.97 0.23 5.17
Reference group is (0): no bonuses.
The relationship is confounded by the pharmacist’s behavior in selling the product as OTC or ethical.
The distribution of bonuses size depending on the therapeutic category frequency is
shown in Table 4: 10.3% of the most frequent therapeutic categories were shared with
high bonuses size comparing to 8.5% for other categories. In addition, 6.9% of the most
frequent categories were sold with low bonuses size comparing to 23.9% for other
categories.
Table 4: the distribution of bonuses size among the pharmaceutical therapeutic categories:
Bonuses Categories Total
No bonus Low Moderate High
Pharmaceutical form frequency
Antibiotics 18
(62.1%) 2
(6.9%) 6
(20.7%) 3
(10.3%) 29
Other 41
(57.7%) 17
(23.9%) 7
(9.9%) 6
(8.5%) 71
Total 59 19 13 9 100
There was a remarkable gap between MoH definition and pharmacists behaviors
regarding to the product categorization depending on MoH definition whether it was
classified as (OTC) drug, or as ethical drug. While MoH classified 74 of the 100 products
as ethical products, pharmacists’ data announced a presence of 68 of the 100 form as
OTC product according to their behavior in selling the drugs (table 5).
Table 5: the pharmaceutical products categorization according to MoH
definition and pharmacists’ behavior:
Pharmacist’s behavior Total
OTC Ethical
MoH definition
OTC 15 11 26
Ethical 53 21 74
Total 68 32 100
29
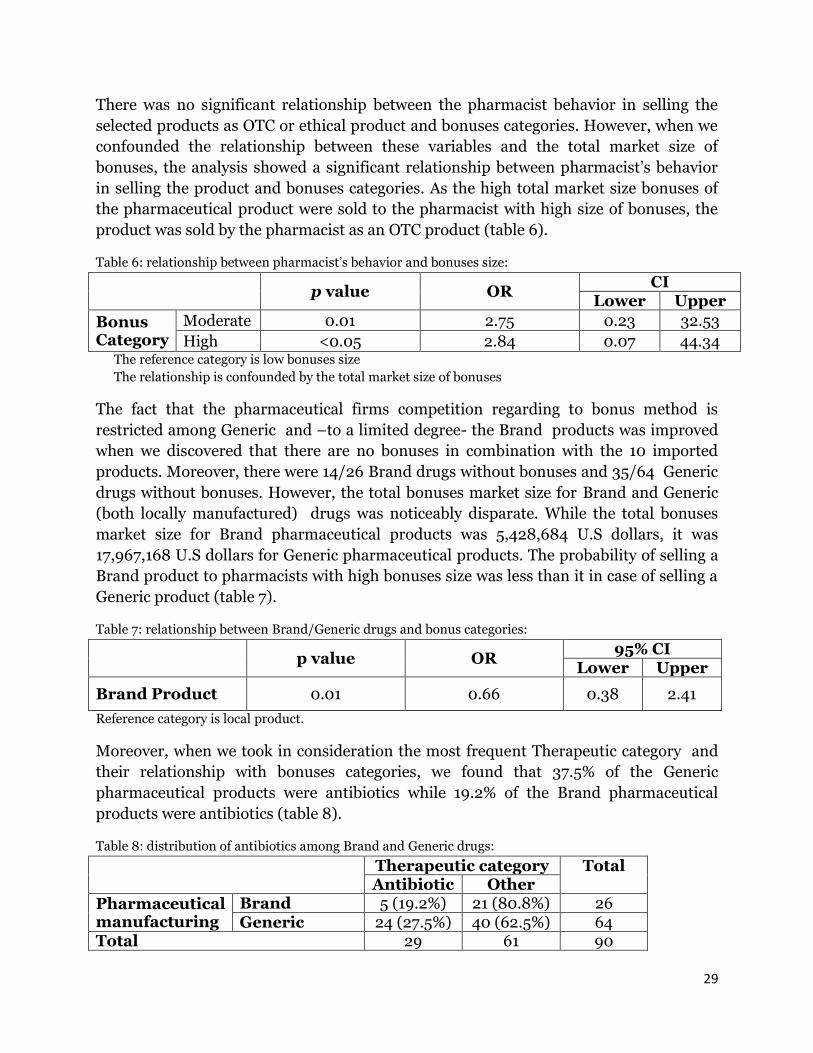
There was no significant relationship between the pharmacist behavior in selling the
selected products as OTC or ethical product and bonuses categories. However, when we
confounded the relationship between these variables and the total market size of
bonuses, the analysis showed a significant relationship between pharmacist’s behavior
in selling the product and bonuses categories. As the high total market size bonuses of
the pharmaceutical product were sold to the pharmacist with high size of bonuses, the
product was sold by the pharmacist as an OTC product (table 6).
Table 6: relationship between pharmacist’s behavior and bonuses size:
p value OR
CI Lower Upper
Bonus Category
Moderate 0.01 2.75 0.23 32.53
High <0.05 2.84 0.07 44.34 The reference category is low bonuses size
The relationship is confounded by the total market size of bonuses
The fact that the pharmaceutical firms competition regarding to bonus method is
restricted among Generic and –to a limited degree- the Brand products was improved
when we discovered that there are no bonuses in combination with the 10 imported
products. Moreover, there were 14/26 Brand drugs without bonuses and 35/64 Generic
drugs without bonuses. However, the total bonuses market size for Brand and Generic
(both locally manufactured) drugs was noticeably disparate. While the total bonuses
market size for Brand pharmaceutical products was 5,428,684 U.S dollars, it was
17,967,168 U.S dollars for Generic pharmaceutical products. The probability of selling a
Brand product to pharmacists with high bonuses size was less than it in case of selling a
Generic product (table 7).
Table 7: relationship between Brand/Generic drugs and bonus categories:
p value OR
95% CI Lower Upper
Brand Product 0.01 0.66 0.38 2.41
Reference category is local product.
Moreover, when we took in consideration the most frequent Therapeutic category and
their relationship with bonuses categories, we found that 37.5% of the Generic
pharmaceutical products were antibiotics while 19.2% of the Brand pharmaceutical
products were antibiotics (table 8).
Table 8: distribution of antibiotics among Brand and Generic drugs:
Therapeutic category Total Antibiotic Other
Pharmaceutical manufacturing
Brand 5 (19.2%) 21 (80.8%) 26 Generic 24 (27.5%) 40 (62.5%) 64
Total 29 61 90

30
10- Discussion:
“The pharmaceutical market in Syria is considered to form a remarkable sector of the
Syrian economic” a public stakeholder stated Syrian regulations impose the supervision
and control of MoH on the pharmaceutical industry and the selling mechanisms bother
between pharmaceutical firms and pharmacists, and between pharmacists and people.
However, some informal methods such as bonuses are present in the reciprocal
transaction between pharmaceutical firms and pharmacists. This research was aimed to
clarify the real role of bonuses as informal method of competition and its mechanisms
among the reciprocal transaction between pharmaceutical firms and pharmacists in
addition to the reason of the current tendency among pharmaceutical firms and
pharmacists to use bonuses among their trade relations.
Our data showed a non significant relationship between the pharmaceutical product’s
quality and buying rate, which reflect an absence in quality-based choice among
pharmacists in their selling behaviors which negatively reflects on population demands.
“Bonus is a trivial trade method was created in order to increase the selling mechanism
in a rapid manner” a private stakeholder stated. Therefore, based on what was found we
can state that the bonuses trade is a competing tool in the market which attain the
demands of both pharmaceutical firms and pharmacists, however, not people’s demand
because of the quality absence.
The bonuses sizes lead to an increase in: high bonuses products (more bonuses to be
induced) and higher buying rate. Although the products which were indicated to be sold
with high bonuses amounts were the smallest count (9/100), they presented the largest
share of total pharmaceutical market size. Pharmaceutical sold procedures should be
based on ethical aspects taking in consideration the population demand. However, this
procedure is affected in the first degree by bonuses size not by people demands. A public
stakeholder stated: “Bonuses mechanism is one of the most important factors which
lead to a defect in the Syrian pharmaceutical market”.
The relationship between therapeutic categories and bonuses size was not significant
unless it was confounded by the pharmacist’s behavior in selling the pharmaceutical
product as OTC or ethical. Therefore, we can say that the firms sell the most frequent
pharmaceutical products with high bonuses size basing on the illegal behavior of the
pharmacist in selling the pharmaceutical products regardless to the MoH definition of
each product (OTC or ethical). Moreover, the total bonuses market size showed a
significant role in confounding the relationship between pharmacists’ behavior in selling
the pharmaceutical products as OTC or ethical and bonuses categories. Pharmacists
tend to sell the pharmaceutical products without prescription if they were introduced
with higher bonuses.
This finding was expressed by a public stakeholder: “Bonuses mechanism has a great
effect on the pharmacist’s behavior; it leads to illegal behaviors by the pharmacist and

31
lead to an absence of self discipline”. Actually the: MoH defined 74 forms as ethical
products and not permitted to be sold without a prescription, whilst the data showed
only 32 forms as ethical products. Indeed 53 forms were sold by the pharmacists as OTC
forms while they were defined as ethical products by MoH. This illegal behavior is
affected by the bonuses size and total bonuses’ market size. Moreover, this table
reflected the absence of regulation or procedures of selling from pharmacists to people:
some pharmacists who were aware of the most recent MoH categorisation of
pharmaceutical products and there are several forms which are frequently re-
categorized. In other words, the pharmaceutical deals without any concern to the
academic aspect and the ethical rules of this carrier. A public stakeholder talked about
this updating by MoH; “There are several pharmaceutical categories which were re-
categorized from OTC to ethical by MoH because of their side effects in addition to the
applying of drug consumption rationalization policy”. Moreover, bonus mechanism and
the profit procedures which share it affect the quality of sold forms. Although physicians
are often affected by the pharmaceutical marketing methods and they tend to prescribe
certain forms, pharmacists change the prescribed forms to sell high bonus size forms.
Regarding this illegal method in selling certain forms, a public stakeholder stated: “The
worst items in the Syrian healthcare system are pharmacist and physician. Pharmacists
could change the prescriptions in order to sell certain forms, and even could sell an
ethical form without a prescription”.
11- Conclusion:
The overall statistical findings in addition to the interviews remarkably indicated to a
presence of bonuses size as illegal method among the pharmaceutical marketing
procedures. Although this method was considered as a legal method in pharmaceutical
marketing by some stakeholders, they assured that this method, nowadays, changed to
illegal method; “The bonus method is a legal pharmaceutical marketing unless it was
uncontrolled and without a specific margin”. Depending on our data, there were several
products which their sold units were shared with the same number of bonuses. In other
words, the number of sold units is equal to the number of shared bonuses. Moreover, a
few products were sold with bonuses more than the number of sold units. Actually 5
products were sold with bonuses equaled or exceeded the number of sold units. . These
findings reflected the illegal method by which both pharmaceutical firms and
pharmacists are marketing their pharmaceutical goods. Given that the Syrian
pharmaceutical market is regulated and controlled by MoH, what is the role of MoH in
the current policy of pharmaceutical firms and pharmacists regarding to bonus method?
How MoH can control and restrict the illegal profit manners taking in consideration the
effected quality of sold products because of pharmacists’ behaviors? A public
stakeholder stated; “It is very complicated to control bonus method because the

32
pharmacists, nowadays, consider the bonuses as a legal and acquired right and became
an inclusive demand”.
In this inquiry, the common factor among all the analysis and interviews was the
pharmacist and the pharmacist’s behavior. However, the unscientific role of the
pharmaceutical firms by which they are marketing their products should be taken in
consideration in affecting the pharmacist’s behavior. Moreover, the people demand has
its uncontrolled role regardless of the low level of healthcare awareness and edification
of the individuals. During an interview, when a public stakeholder was asked where the
changing should be started from, the answer was focused on the pharmacist’s behavior
and attitudes towards bonus method. The public stakeholder considered the
pharmacists’ ethical behaviors (which is almost missing among all new pharmacist,
according to the resource) as a safety valve in the Syrian pharmaceutical system. It is
important to create more criterions and obligations for the pharmacists’ behavior
regarding bonus method which is considered to be one of the most important defects
among the Syrian health system. However, what is the reason lying behind this method?
To which degree can the reason affect the bonus method and who is the initiative? A
private stakeholder mentioned; “There are several technical criteria and procedures
should be followed in order to include the pharmaceutical product among the national
drugs list. These procedures and criteria are controlled by the technical opinion and
experience of special national centers”. The private stakeholder added; “These criteria
and procedures are affected by the individual’s opinion and relationships which is a
weak point among the pricing procedure” The stakeholder wondered why we do not
depend on FDA criteria during the pricing procedures.
Regardless to stakeholders’ different opinions about free pharmaceutical market
in Syria as a satisfactory solution, they agreed about the necessity of developing pricing
criteria. Several suggestions about the absence of the experience and the weak role of
MoH in pricing procedures were mentioned in addition to depending on global pricing
criteria. The question is; what is the basis MoH have used to suggest these criteria?
Another weak point in the pricing procedure was mentioned by a private stakeholder;
“MoH create these base. However, does not reach them by research and developing.
There is a noticeable absence in the international conventions, experts, and training
programs”, the stakeholder added; “Pricing procedure should be based on the national
demands”.
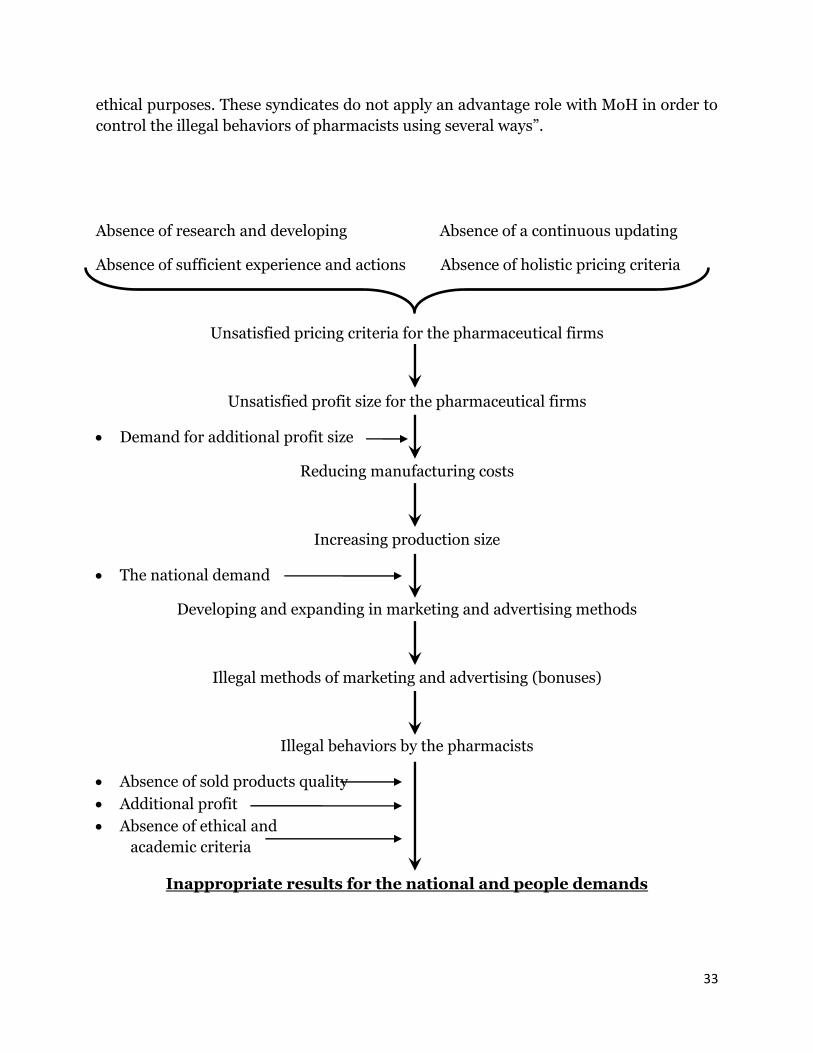
Based on what we found we can express the current feature of the pharmaceutical
market in Syria as a vicious circle of several overlapped factors which are combined
together to form the series of the overall Syrian pharmaceutical market picture.
The pharmacists’ behavior in selling the pharmaceutical products as OTC or ethical is
the responsibility of the pharmacist syndicates. However, the role of these syndicates at
this point is usually ignored and not applied. A public stakeholders stated; “the real
monitoring is MoH responsibility. However, pharmacist syndicates were involved for
33
ethical purposes. These syndicates do not apply an advantage role with MoH in order to
control the illegal behaviors of pharmacists using several ways”.
Absence of research and developing Absence of a continuous updating
Absence of sufficient experience and actions Absence of holistic pricing criteria
Unsatisfied pricing criteria for the pharmaceutical firms
Unsatisfied profit size for the pharmaceutical firms
Demand for additional profit size
Reducing manufacturing costs
Increasing production size
The national demand
Developing and expanding in marketing and advertising methods
Illegal methods of marketing and advertising (bonuses)
Illegal behaviors by the pharmacists
Absence of sold products quality
Additional profit
Absence of ethical and
academic criteria
Inappropriate results for the national and people demands
34
12-Recommendations:
The Syrian health system urgently needs more analysis and in-depth by experts of
health economics, as Syria economy is entering a new era. Additional efforts and
time are need to apply the rules of social market economy among Syrian health
system. Social health insurance is a major step towered the success of all aims and
objectives of our optimal health system.
The current regulation criteria of the pharmaceutical market in Syria that exist at
MoH need to be enforced to ensure best results. At the same time, any new
regulations are to be added should also be piloted and analyzed before applying
nationally.
It is critical and at the same time beneficial to study - and disseminate the findings
of such studies - to policy and decision makers of regulations and methods for
pharmaceutical industries among other and neighborhood countries which are
similar to Syria in term of the health indicators and socioeconomics
Applying and activating regulations are much more likely to succeed if they are
were made in cooperation of all involved states. The role of the pharmacists
syndicate also needs to be clarified: a clear and transparence description of its
responsibilities and accountabilities should be issued and followed continuously.
It is vital by MoH to support the social health insurance plans in order to provide
low socioeconomic individuals with appropriate drugs instead of pressuring on the
pharmaceutical firms to control their products’ prices which lead to a quality
reduction of the pharmaceutical drugs.
There are important implications about stability: given the presence of multiple
factors and complexity that affect this market, an independent director should be
established under the MoH pharmaceutical affairs department. This directorate
should be involved in all researches, regulations, follow up or procedures related
especially to the pharmaceutical market. With a sufficient and well trained human
resources along with appropriate tools, this directorate will be the link point of all
efforts of different stakeholders involved among the Syrian pharmaceutical market
such as:
The supervision on the Scientific Council for Pharmaceutical Industry that
represents manufacturers ensuring the scope of local manufacturers
representing and all council recommendations or regulations are in
adherence to the optimal future of the pharmaceutical industry.
Supervision of pharmacist syndicates and health directorates among
Syrian governorates regarding to organizational pharmacy regulations.
such as OTC - Ethical selling pharmaceutical products by pharmacists.
To be involved in market researchers that should protect and guarantee
the beneficiary of public sector in the first place, along with other involved
parts like manufacturers.

35
To be involved in continuous training and updating of information for all
stakeholders and policy makers for this market.
The pharmaceutical industry is an important part of the country economy; the
government has to take a dominant role in controlling the health care market in general
and the pharmaceutical catastrophic expenditure in particular. The author believes that
lots can be done along with the country development plans in the field of Health
Systems, with the association of the EU projects and the WHO supports. One is to
implement financial penalties on pharmacies' that encourages unethical consumptions
for drugs without appropriate prescription. Another is that health care regulations and
committees must get closer to the community based pharmacies and try to get involved
on the sales processes that exist. Government should regulate the pharmaceutical
industry, not in order to suppress it, but in order to ensure more adequate control for
profits and pricing. Or it might benefit from earmarked taxes comes from that industry
to reallocate those resources in such a way to ensure equity and efficiency. At last but
not least it crucial to build well educated society in terms of health care, with good
knowledge about basics of health maintenance and protection, such programs can be
delivered early starting at school age, or can be advocated to the public generally.
Obtaining equivalent and sufficient amount of information through wide scope of the
society regarding their health protects us from further economical failures that might be
hiding in the future.
36
13- Limitations:
1- As the topic of this research was discussing an extremely sensitive points
(bonuses, profit margins, and amount of sells), the author faced a lot of
limitations and obstacles. With the targeted pharmacists, unexpectedly, lots had
refuses to participate in data collection, no matter the author emphasized on
anonymous and confidentiality. Lots of the sample that accepted to give data
delayed for several weeks after the submission date.
2- One of the main public stakeholders were in a long vacation that the author could
not perform the interview, while his assistants did not cooperate enough or give
any useful data.
3- The author did not found by any mean any documentations in the
pharmaceutical regulation departments that could support his literature review
or the research in general.
4- As all the interviews were conducted in Arabic language, the translation of their
statements might be slightly different of what they originally meant to say.
5- The limited time given for this research affected its quality by several means.
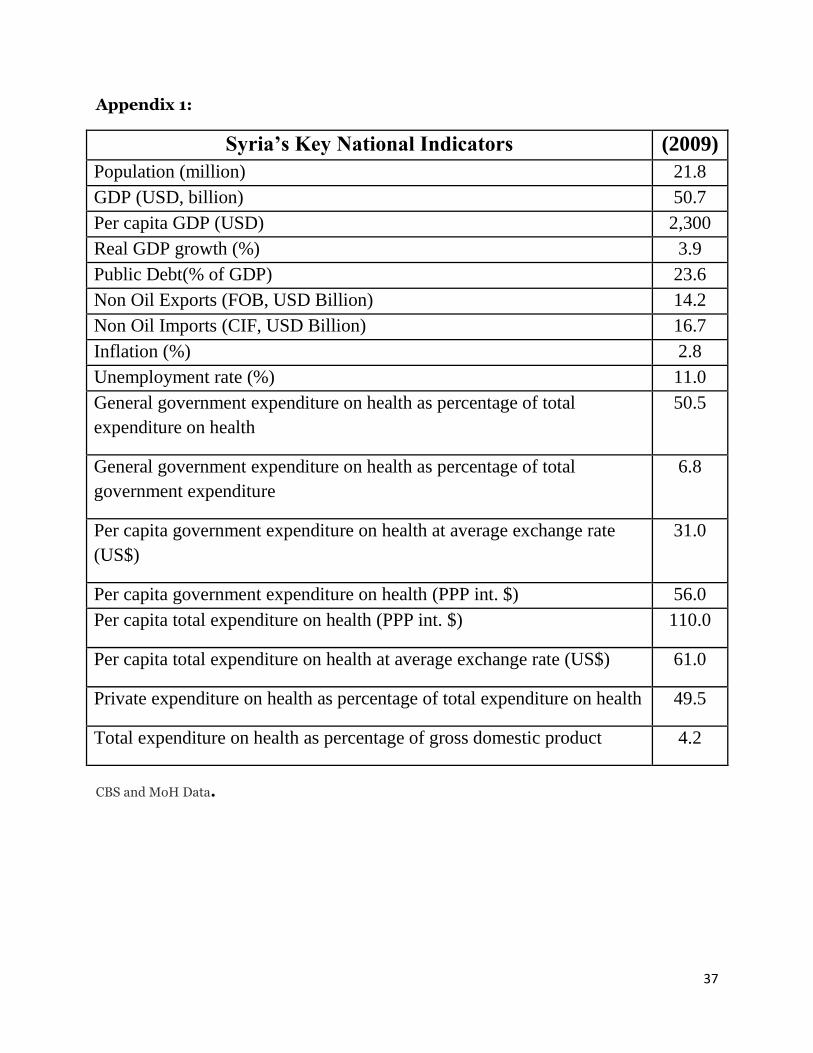
37
Appendix 1:
(2009) Syria’s Key National Indicators
21.8 Population (million)
50.7 GDP (USD, billion)
2,300 Per capita GDP (USD)
3.9 Real GDP growth (%)
23.6 Public Debt(% of GDP)
14.2 Non Oil Exports (FOB, USD Billion)
16.7 Non Oil Imports (CIF, USD Billion)
2.8 Inflation (%)
11.0 Unemployment rate (%)
50.5 General government expenditure on health as percentage of total
expenditure on health
6.8 General government expenditure on health as percentage of total
government expenditure
31.0 Per capita government expenditure on health at average exchange rate
(US$)
56.0 Per capita government expenditure on health (PPP int. $)
110.0 Per capita total expenditure on health (PPP int. $)
61.0 Per capita total expenditure on health at average exchange rate (US$)
49.5 Private expenditure on health as percentage of total expenditure on health
4.2 Total expenditure on health as percentage of gross domestic product
CBS and MoH Data.
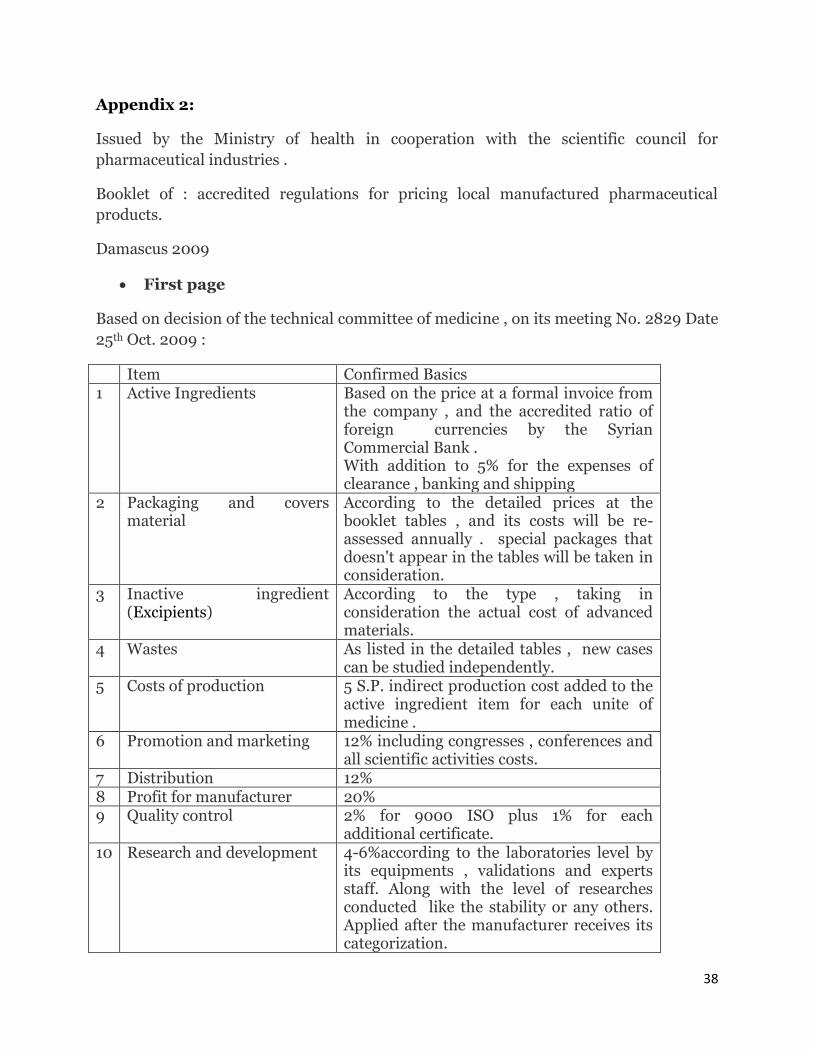
38
Appendix 2:
Issued by the Ministry of health in cooperation with the scientific council for
pharmaceutical industries .
Booklet of : accredited regulations for pricing local manufactured pharmaceutical
products.
Damascus 2009
First page
Based on decision of the technical committee of medicine , on its meeting No. 2829 Date
25th Oct. 2009 :
Item Confirmed Basics 1 Active Ingredients Based on the price at a formal invoice from
the company , and the accredited ratio of foreign currencies by the Syrian Commercial Bank . With addition to 5% for the expenses of clearance , banking and shipping
2 Packaging and covers material
According to the detailed prices at the booklet tables , and its costs will be re-assessed annually . special packages that doesn't appear in the tables will be taken in consideration.
3 Inactive ingredient (Excipients)
According to the type , taking in consideration the actual cost of advanced materials.
4 Wastes As listed in the detailed tables , new cases can be studied independently.
5 Costs of production 5 S.P. indirect production cost added to the active ingredient item for each unite of medicine .
6 Promotion and marketing 12% including congresses , conferences and all scientific activities costs.
7 Distribution 12% 8 Profit for manufacturer 20% 9 Quality control 2% for 9000 ISO plus 1% for each
additional certificate. 10 Research and development 4-6%according to the laboratories level by
its equipments , validations and experts staff. Along with the level of researches conducted like the stability or any others. Applied after the manufacturer receives its categorization.
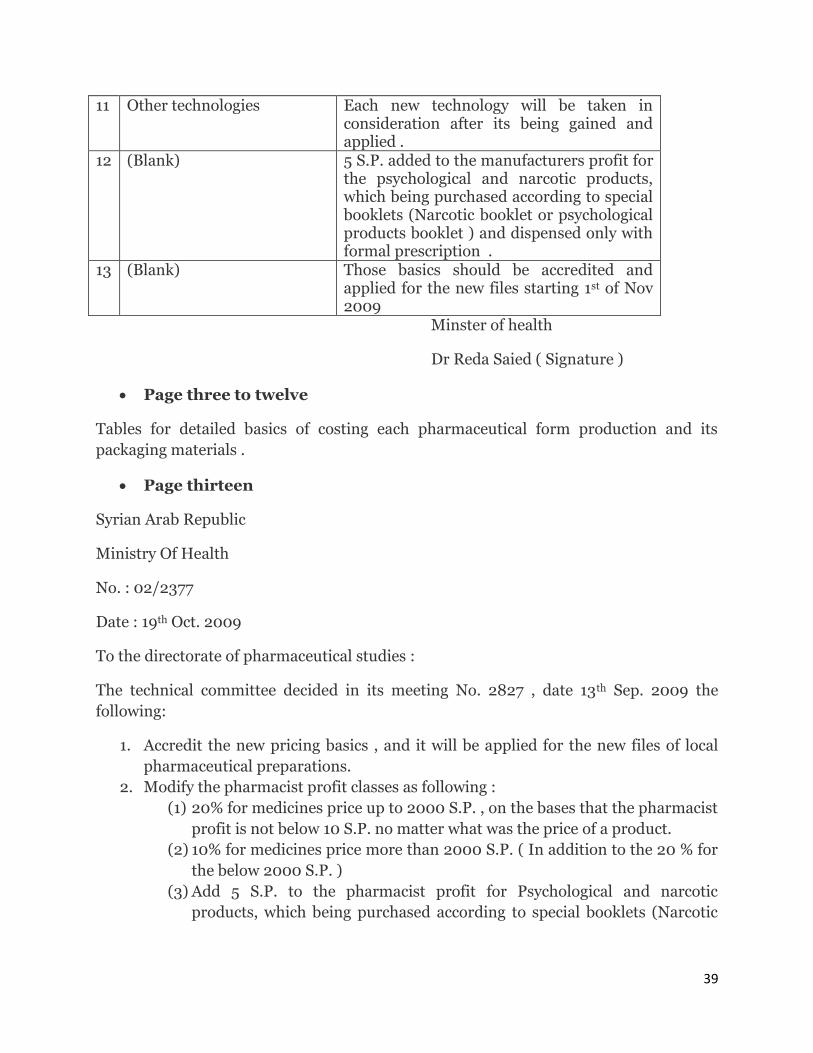
39
11 Other technologies Each new technology will be taken in consideration after its being gained and applied .
12 (Blank) 5 S.P. added to the manufacturers profit for the psychological and narcotic products, which being purchased according to special booklets (Narcotic booklet or psychological products booklet ) and dispensed only with formal prescription .
13 (Blank) Those basics should be accredited and applied for the new files starting 1st of Nov 2009
Minster of health
Dr Reda Saied ( Signature )
Page three to twelve
Tables for detailed basics of costing each pharmaceutical form production and its
packaging materials .
Page thirteen
Syrian Arab Republic
Ministry Of Health
No. : 02/2377
Date : 19th Oct. 2009
To the directorate of pharmaceutical studies :
The technical committee decided in its meeting No. 2827 , date 13th Sep. 2009 the
following:
1. Accredit the new pricing basics , and it will be applied for the new files of local
pharmaceutical preparations.
2. Modify the pharmacist profit classes as following :
(1) 20% for medicines price up to 2000 S.P. , on the bases that the pharmacist
profit is not below 10 S.P. no matter what was the price of a product.
(2) 10% for medicines price more than 2000 S.P. ( In addition to the 20 % for
the below 2000 S.P. )
(3) Add 5 S.P. to the pharmacist profit for Psychological and narcotic
products, which being purchased according to special booklets (Narcotic
40
booklet or psychological products booklet ) and dispensed only with
formal prescription .
3. The price for public is calculated after transferring the approximate value of
Syrian pound to one full unite.
4. Applied and approved from the date of this issue .
Damascus 19th Oct. 2009
Ministry of Health
Dr Reda Saied ( Signature )
Copy to :
-pricing committee at the MOH .
- Ministry of economics and foreign trades (pricing directorate )
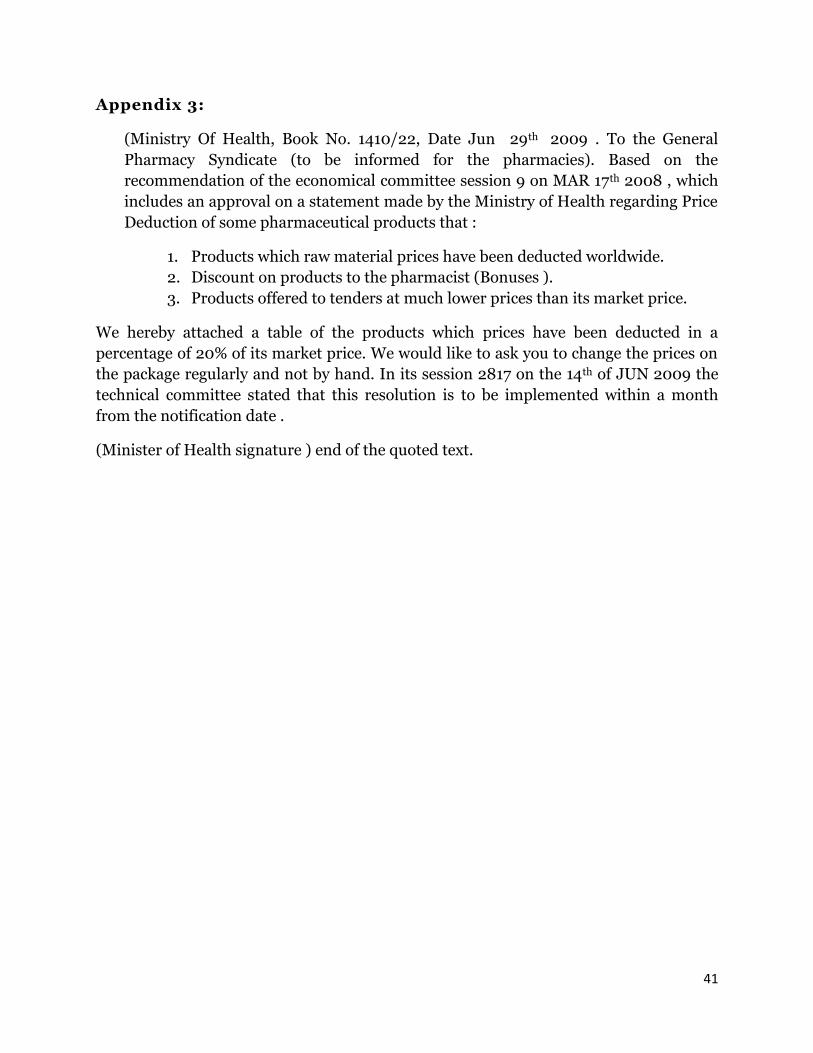
41
Appendix 3:
(Ministry Of Health, Book No. 1410/22, Date Jun 29th 2009 . To the General
Pharmacy Syndicate (to be informed for the pharmacies). Based on the
recommendation of the economical committee session 9 on MAR 17th 2008 , which
includes an approval on a statement made by the Ministry of Health regarding Price
Deduction of some pharmaceutical products that :
1. Products which raw material prices have been deducted worldwide.
2. Discount on products to the pharmacist (Bonuses ).
3. Products offered to tenders at much lower prices than its market price.
We hereby attached a table of the products which prices have been deducted in a
percentage of 20% of its market price. We would like to ask you to change the prices on
the package regularly and not by hand. In its session 2817 on the 14th of JUN 2009 the
technical committee stated that this resolution is to be implemented within a month
from the notification date .
(Minister of Health signature ) end of the quoted text.
42
References:
1- Aleccia, J., 2011, Free drug samples cost more in the long run. MSNBC. [Website] Available at: http://www.msnbc.msn.com/id/23783105/ns/health-health_care/ [Accessed 9.January.2011].
2- AMS Data, 2009 , Software for pharmaceutical sales monitor system, Global Market Research company, L.T.D.
3- Author, Fact Sheet, Pharmaceutical Industry Marketing., 2009, Boston, Available at: http://www.prescriptionproject.org/tools/sunshine_docs/files/0004.pdf
4- Author, Corruption in health sector. U4 partner agencies [Website]., Available at: http://www.u4.no/themes/health/main.cfm [Accessed: 21. Novenber. 2010].
5- Barfett, J., Lanting, B., Lee, J., Lee, M., Victor. Ng, & Simkhovitch, P., 2004, Pharmaceutical Marketing to Medical Students: The Student Perspective. MJM, Vol.8, No.1, p.21-27.
6- Bhatia, T., Hansen, K., Krishnamurthi, L., 2006, Modeling Key Drivers of Physician’s Choice Of Prescription Drugs: An Integrated View Incorporating Patient and Physician Heterogeneity, Pennsylvania, The Pennsylvania State University.
7- Capri, S. & Levaggi, R,. Pricing drugs in a regulated market: a bargaining approach. Italy, Dipartimento di Scienze Economiche, Facoltà di Economia.
8- Chew, L.D, et al., 2000, A Physician Survey of the Effect of Drug Sample Availability on Physicians’ Behavior. Journal of General Internal Medicine. Vol.15, Issue.7, p.478-483.
9- Favole, J.A., 2010, Drug Industry Spends Billions On Free Samples Of Popular Meds. NASDAQ. [Website]. Available at: http://search.nasdaq.com/search?q=Drug%20Industry%20Spends%20Billions%20On%20Free%20Samples%20Of%20Popular%20Meds&site=dotcom_collection&client=default_frontend&proxystylesheet=default_frontend&output=xml_no_dtd&proxyreload=1
10- Girdharwal, N., 2007, A Study of Physicians Behavior Toward Marketing of Pharmaceutical Products (A Case Study of Indian Market). Pharmainfo [Website]., Available at: http://www.pharmainfo.net/reviews/study-physicians-behaviour-toward-marketing-pharmaceutical-products-case-study-indian-market [Accessed 11. October. 2010].
11- Gray, D.E., 2004, Doing Research in The Real World. London, SAGE. 12- Hancock, B., 2002, An Introduction to Qualitative Research., Trent Focus
Group. 13- Horner, B., Hartwell, M., Levin, A., 2006, The Pharmaceutical Companies’
Direct Marketing to Doctors and the Impact on Health Care Costs and Patient Safety. Washington, NYPIRG
14- Humaidi, T., 2008, Free drug samples, a legal marketing or implicit bribe. Menbar Al-Rai [Website]., Available at: http://manbaralrai.com/?q=taxonomy/term/33 [Accessed 25.October.2010]
15- Marczyk, G., DeMatteo, D. & Festinger, D., 2005, Essential of Research Design and Methodology. New Jersey, John Wiley & Sons, Inc.
43
16- Marshall, N.M., 1996, Sampling for Qualitative Research., Family Practice., Vol.13, No.6, p.522-525.
17- MoH, 2009, Accredited regulations for pricing local manufactured pharmaceutical products. Syria, Damascus. MoH, Scientific Council for Pharmaceutical Industry.
18- Mohd Noor, Kh. B., 2008, Case Study: A Strategic Research Methodology, American Journal of Applied Science. Vol.5, No. 11. p.1602-1604
19- Robson, C., 2002. Real World Research. 2nd ed. Massachusetts: Blackwell. p.80-81
20- S. Jacobzone., 2000, Pharmaceutical Policies in OECD Countries, Reconciling Social and Industrial Goals. Paris, OECD.
21- SANA, Physicians tend to prescribe drugs which were marketing to them by pharmaceutical firms. 2010 .األطباء يميلون لوصف أدوية تروجها لهم شركات األدوية, Syrian Arab New Agency, SANA., [Website]. Available at: http://www.sana.sy/ara/18/2010/10/20/314373.htm [Accessed at: 13.December.2010]
22- Scott, A.B., Culley, E.J., O'Donnell, J., 2007, Effects of a Physician Office Generic Drug Sampling System on Generic Dispensing Ratios and Drug Costs in a Large Managed Care Organization. Journal of Managed Care Pharmacy., Vol.13, No.5
23- Singh, Y.K., 2006, Fundamental of Research Methodology and Statistics. New Delhi, Bangalore, Mumbai, New Age International (P) Limited.
24-WHO., 1998, Pharmaceuticals and Health Sector Reform in the Americas: An Economic Perspective. Geneva. Available at: http:// aaps.who.int/medicinedocs/es/d/jh2926e
Related Documents











