Pharmaceutical marketing From Wikipedia, the free encyclopedia The examples and perspective in this article deal primarily with the United States and do not represent a worldwide view of the subject. Please improve this article and discuss the issue on the talk page . (June 2011) An advertisement, c. 1885, promoting the medicinal use of a cocaine based product. Pharmaceutical marketing, sometimes called medico-marketing or pharma marketing in some countries, is the business of advertising or otherwise promoting the sale of pharmaceuticals or drugs . Many countries have measures in place to limit advertising by pharmaceutical companies . Pharmaceutical company spending on marketing far exceeds that spent on research. [1] [2] In Canada, $1.7 billion was spent in 2004 to market drugs to physicians; in the United States, $21 billion was spent in 2002. [3] In 2005 money spent on pharmaceutical marketing in the US was estimated at $29.9 billion with one estimate as high as $57 billion. [2] When the US numbers are broken down, 56% was free samples , 25% was pharmaceutical sales representative "detailing" (promoting drugs directly to) physicians, 12.5% was direct to user advertising, 4% on detailing to hospitals, and 2% on journal ads. [3] There is some evidence that marketing practices can

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Pharmaceutical marketingFrom Wikipedia, the free encyclopedia
The examples and perspective in this article deal primarily with the United States and do not represent a worldwide view of the subject. Please improve this article and discuss the issue on the talk page. (June 2011)
An advertisement, c. 1885, promoting the medicinal use of a cocaine based product.
Pharmaceutical marketing, sometimes called medico-marketing or pharma marketing in some countries, is the business of advertising or otherwise promoting the sale of pharmaceuticals or drugs.
Many countries have measures in place to limit advertising by pharmaceutical companies.
Pharmaceutical company spending on marketing far exceeds that spent on research.[1][2] In Canada, $1.7 billion was spent in 2004 to market drugs to physicians; in the United States, $21 billion was spent in 2002.[3] In 2005 money spenton pharmaceutical marketing in the US was estimated at $29.9billion with one estimate as high as $57 billion.[2] When theUS numbers are broken down, 56% was free samples, 25% was pharmaceutical sales representative "detailing" (promoting drugs directly to) physicians, 12.5% was direct to user advertising, 4% on detailing to hospitals, and 2% on journalads.[3] There is some evidence that marketing practices can
negatively affect both patients and the health care profession.[4]
Contents 1 History 2 To health care providers
o 2.1 New pharma code & guidelines o 2.2 Free samples o 2.3 Continuing medical education o 2.4 Pharmaceutical representatives o 2.5 Peer influence o 2.6 Journal articles o 2.7 Private and public insurers
3 To users o 3.1 Drug coupons
4 Economics 5 Regulation and fraud 6 Evolution of marketing 7 See also 8 References 9 Further reading
HistoryThe marketing of medication has a long history. The sale of miracle cures, many with little real potency, has always been common. Marketing of legitimate non-prescription medications, such as pain relievers or allergy medicine, hasalso long been practiced, although, until recently, mass marketing of prescription medications has been rare. It was long believed that since doctors made the selection of drugs, mass marketing was a waste of resources; specific adstargeting the medical profession were thought to be cheaper and just as effective.[citation needed] This would involve ads in professional journals and visits by sales staff to doctor’s offices and hospitals. An important part of these efforts was marketing to medical students.[citation needed]
To health care providersMarketing to health care providers takes four main forms: gifting, activity by pharmaceutical sales representatives, provision of drug samples, and sponsoring continuing medicaleducation (CME).[2] Of the 237,000 medical sites representing680,000 physicians surveyed in SK&A's 2010 Physician Access survey, half said they prefer or require an appointment to see a rep (up from 38.5% preferring or requiring an appointment in 2008), while 23% won't see reps at all, according to the survey data. Practices owned by hospitals or health systems are tougher to get into than private practices, since appointments have to go through headquarters, the survey found. 13.3% of offices with just one or two doctors won't see reps, compared with a no-see rate of 42% at offices with 10 or more docs The most accessible physicians for promotional purposes are allergists/immunologists – only 4.2% won't see reps at all –followed by orthopedic specialists (5.1%) and diabetes specialists (7.6%). Diagnostic radiologists are the most rigid about allowing details – 92.1% won't see reps – followed by pathologists and neuroradiologists, at 92.1% and91.8%, respectively.[5]
E-detailing is widely used to reach "no see physicians"; approximately 23% of primary care physicians and 28% of specialists prefer computer-based edetailing, according to survey findings reported in the April 25, 2011, edition of American Medical News (AMNews), published by the American Medical Association (AMA).[6]
New pharma code & guidelines
The Pharmaceutical Research and Manufacturers of America (PhRMA) released updates to its voluntary Code on Interactions with Healthcare Professionals on July 10. The new guidelines take effect January 2009."[7]
In addition to prohibiting small gifts and reminder items such as pens, notepads, staplers, clipboards, pill boxes, etc.,[7] the revised Code:
1. Prohibits company sales representatives from providing restaurant meals to healthcare professionals, but allows them to provide occasional meals in healthcare professionals’ offices in conjunction with informational presentations"[7]
2. Includes new provisions requiring companies to ensure their representatives are sufficiently trained about applicable laws, regulations, and industry codes of practice and ethics.[7]
3. Provides that each company will state its intentions toabide by the Code and that company CEOs and compliance officers will certify each year that they have processes in place to comply.[7]
4. Includes more detailed standards regarding the independence of continuing medical education.[7]
5. Provides additional guidance and restrictions for speaking and consulting arrangements with healthcare professionals.[7]
However, the Good Works Health government-approved platform offers physicians and other health care professionals the opportunity to direct donations to charities of their choicein exchange for participation in pharmaceutical promotional/educational programs. [8]
Free samples
Free samples have been shown to affect physician prescribingbehaviour. Physicians with access to free samples are more likely to prescribe brand name medication over equivalent generic medications.[2] Other studies found that free samplesdecreased the likelihood that physicians would follow standard of care practices.[2]
Receiving pharmaceutical samples does not reduce prescription costs. Even after receiving samples, sample
recipients remain disproportionately burdened by prescription costs.[9]
It is argued that a benefit to free samples is the “try it before you buy it” approach. Free Samples give immediate access to the medication and the patient can begin treatmentright away. Also, it saves time from going to a pharmacy to get it filled before treatment begins. Since not all medications work for everyone, and many do not work the sameway for each person, free samples allow patients to find which dose and brand of medication works best before having to spend money on a filled prescription at a pharmacy.[9]
Continuing medical education
Hours spent by physicians in industry-supported CME is greater than that from either medical schools or professional societies.[2]
Pharmaceutical representatives
Currently, there are approximately 81,000 pharmaceutical sales representatives in the United States[10] pursuing some 830,000 pharmaceutical prescribers. A pharmaceutical representative will often try to see a given physician everyfew weeks. Representatives often have a call list of about 200-300 physicians with 120-180 targets that should be visited in 1-2 or 3 week cycle.
Because of the large size of the pharmaceutical sales force,the organization, management, and measurement of effectiveness of the sales force are significant business challenges. Management tasks are usually broken down into the areas of physician targeting, sales force size and structure, sales force optimization, call planning, and sales forces effectiveness. A few pharmaceutical companies have realized that training sales representatives on high science alone is not enough, especially when most products are similar in quality. Thus, training sales representativeson relationship selling techniques in addition to medical
science and product knowledge, can make a difference in sales force effectiveness. Specialist physicians are relyingmore and more on specialty sales reps for product information, because they are more knowledgeable than primary care reps.
The United States has 81,000 pharmaceutical representatives or 1 for every 7.9 physicians.[2] The number and persistence of pharmaceutical representatives has placed a burden on thetime of physicians.[11] "As the number of reps went up, the amount of time an average rep spent with doctors went down—so far down, that tactical scaling has spawned a strategic crisis. Physicians no longer spend much time with sales reps, nor do they see this as a serious problem."
Marketers must decide on the appropriate size of a sales force needed to sell a particular portfolio of drugs to the target market. Factors influencing this decision are the optimal reach (how many physicians to see) and frequency (how often to see them) for each individual physician, how many patients suffer from that disease state, how many salesrepresentatives to devote to office and group practice and how many to devote to hospital accounts if needed. To aid this decision, customers are broken down into different classes according to their prescription behavior, patient population, and of course, their business potential.
Marketers attempt to identify the set of physicians most likely to prescribe a given drug. Historically, this was done by measuring the number of total prescriptions (TRx) and new prescriptions (NRx) per week that each physician writes. This information is collected by commercial vendors.The physicians are then "deciled" into ten groups based on their writing patterns. Higher deciles are more aggressivelytargeted. Some pharmaceutical companies use additional information such as:
profitability of a prescription (script), accessibility of the physician,
tendency of the physician to use the pharmaceutical company's drugs,
effect of managed care formularies on the ability of the physician to prescribe a drug,
the adoption sequence of the physician (that is, how readily the physician adopts new drugs in place of older treatments), and
the tendency of the physician to use a wide palette of drugs
influence that physicians have on their colleagues.
Data for drugs prescribed in a hospital are not usually available at the physician level. Advanced analytic techniques are used to value physicians in a hospital setting.[citation needed]
Physicians are perhaps the most important component in sales. They write the prescriptions that determine which drugs will be used by people. Influencing the physician is the key to pharmaceutical sales. Historically, this was doneby a large pharmaceutical sales force. A medium-sized pharmaceutical company might have a sales force of 1000 representatives.[citation needed] The largest companies have tens of thousands of representatives around the world. Sales representatives called upon physicians regularly, providing clinical information, approved journal articles, and free drug samples. This is still the approach today; however, economic pressures on the industry are causing pharmaceutical companies to rethink the traditional sales process to physicians. The industry has seen a large scale adoption of Pharma CRM systems that works on laptops and more recently tablets. The new age pharmaceutical representative is armed with key data at his fingertips and tools to maximize the time spent with physicians.
Peer influence
Key opinion leaders
Key opinion leaders (KOL), or "thought leaders", are respected individuals, such as prominent medical school faculty, who influence physicians through their professionalstatus. Pharmaceutical companies generally engage key opinion leaders early in the drug development process to provide advocacy and key marketing feedback.[12] Some pharmaceutical companies identify key opinion leaders through direct inquiry of physicians (primary research). Recently, pharmaceutical companies have begun to use social network analysis to uncover thought leaders; because it doesnot introduce respondent bias, which is commonly found in primary research; it can identify and map out the entire scientific community for a disease state; and it has greatercompliance with state and federal regulations; because physician prescribing patterns are not used to create the social network.[13]
Alternatives to segmenting physicians purely on the basis ofprescribing do exist, and marketers can call upon strategic partners who specialize in delineating which characteristicsof true opinion leadership, a physician does or does not possess. Such analyses can help guide marketers in how to optimize KOL engagements as bona fide advisors to a brand, and can help shape clinical development and clinical data publication plans for instance, ultimately advancing patientcare.
Colleagues
Physicians acquire information through informal contacts with their colleagues, including social events, professionalaffiliations, common hospital affiliations, and common medical school affiliations. Some pharmaceutical companies identify influential colleagues through commercially available prescription writing and patient level data.[14] Doctor dinner meetings are an effective way for physicians to acquire educational information from respected peers. These meetings are sponsored by some pharmaceutical companies.
Journal articles
See also: Medical ghostwriter
Recent legal cases and US congressional hearings have provided access to pharmaceutical industry documents revealing new marketing strategies for drugs.[15] Activities once considered independent of promotional intent, includingcontinuing medical education and medical research, are used,including paying to publish articles about promoted drugs for the medical literature, and alleged suppression of unfavorable study results.[16]
Private and public insurers
Public and private insurers affect the writing of prescriptions by physicians through formularies that restrict the number and types of drugs that the insurer willcover. Not only can the insurer affect drug sales by including or excluding a particular drug from a formulary, they can affect sales by tiering, or placing bureaucratic hurdles to prescribing certain drugs. In January 2006, the U.S. instituted a new public prescription drug plan through its Medicare program. Known as Medicare Part D, this programengages private insurers to negotiate with pharmaceutical companies for the placement of drugs on tiered formularies.
To usersOnly two countries as of 2008 allow direct to users advertising (DTCA): the United States and New Zealand.[2] Since the late 1970s, DTCA of prescription drugs has become important in the United States. It takes two main forms: thepromotion or creation of a disease out of a non-pathologic physical condition or the promotion of a medication.[2] Many people will inquire about, or even demand a medication they have seen advertised on television.[who?] In the United States, recent years have seen an increase in mass media advertisements for pharmaceuticals. Expenditures on direct-
to-users advertising have more than quintupled in the seven years between 1997 and 2005 since the FDA changed the guidelines, from $1.1 billion in 1997 to more than $4.2 billion in 2005, a 19.6% annual increase, according to the United States GAO (Government Accountability Office, 2006).[2]
The mass marketing to users of pharmaceuticals is banned in over 30 industrialized nations, but not in the US and New Zealand, which is considering a ban.[17] Some feel it is better to leave the decision wholly in the hands of medical professionals; others feel that users education and participation in health is useful, but users need independent, comparative information about drugs (not promotional information).[17] For these reasons, most countries impose limits on pharmaceutical mass marketing that are not placed on the marketing of other products. In some areas it is required that ads for drugs include a list of possible side effects, so that users are informed of bothfacets of a medicine. Canada's limitations on pharmaceuticaladvertising ensure that commercials that mention the name ofa product cannot in any way describe what it does. Commercials that mention a medical problem cannot also mention the name of the product for sale; at most, they can direct the viewer to a website or telephone number operated by the pharmaceutical company.
Drug coupons
In the United States, pharmaceutical companies often providedrug coupons to consumers to help offset the copayments charged by health insurers for prescription medication. These coupons are generally used to promote medications thatcompete with non-preferred products and cheaper, generic alternatives by reducing or eliminating the extra out-of-pocket costs that an insurers typically charge a patient fora non-preferred drug product.[18]
Economics
Pharmaceutical company spending on marketing exceeds that spent on research.[1][2] In 2004 in Canada $1.7 billion a yearwas spent marketing drugs to physicians and in the United States $21 billion were spent in 2002.[3] In 2005 money spenton pharmaceutical marketing in the US was estimated at $29.9billion with one estimate as high as $57 billion.[2] When theUS number are broken down 56% was free samples, 25% was detailing of physicians, 12.5% was direct to users advertising, 4% on hospital detailing, and 2% on journal ads.[3] In the United States approximately $20 billion could be saved if generics were used instead of equivalent brand name products.[2]
Although pharmaceutical companies have made large investments in marketing their products, overall promotionalspending has been decreasing over the last few years, and declined by 10 percent from 2009 to 2010. Pharmaceutical companies are cutting back mostly in detailing and sampling,while spending in mailings and print advertising grew since last year.[19]
Regulation and fraudSee also: List of Largest Pharmaceutical SettlementsSee also: List of off-label promotion pharmaceutical settlements
In the United States, marketing and distribution of pharmaceuticals is regulated by the Federal Food, Drug, and Cosmetic Act and the Prescription Drug Marketing Act, respectively. Food and Drug Administration (FDA) regulationsrequire all prescription drug promotion to be truthful and not misleading, based on "substantial evidence or substantial clinical experience", to provide a "fair balance" between the risks and benefits of the promoted drug, and to maintain consistency with labeling approved by the FDA. The FDA Office of Prescription Drug Promotion enforces these requirements.
Antipsychotic drugs are now the top-selling class of pharmaceuticals in America, generating annual revenue of about $14.6 billion. Large pharmaceutical companies got behind the development of the drugs in the 1990s, when they were "still seen as treatments for the most serious mental illnesses, like hallucinatory schizophrenia, and recast themfor much broader uses". Drugs such as Abilify and Geodon were given to a broad range of patients, from preschoolers to octogenarians. In 2010, more than a half-million youths took antipsychotic drugs, and one-quarter of nursing-home residents have used them. Yet the government warns that the drugs may be fatal to some older patients and have unknown effects on children.[20]
Every major company selling the drugs — Bristol-Myers Squibb, Eli Lilly, Pfizer, AstraZeneca and Johnson & Johnson— has either settled recent government cases, under the False Claims Act, for hundreds of millions of dollars or is currently under investigation for possible health care fraud. Following charges of illegal marketing, two of the settlements set records last year for the largest criminal fines ever imposed on corporations. One involved Eli Lilly’santipsychotic Zyprexa, and the other involved Bextra. In theBextra case, the government also charged Pfizer with illegally marketing another antipsychotic, Geodon; Pfizer settled that part of the claim for $301 million, without admitting any wrongdoing.[20]
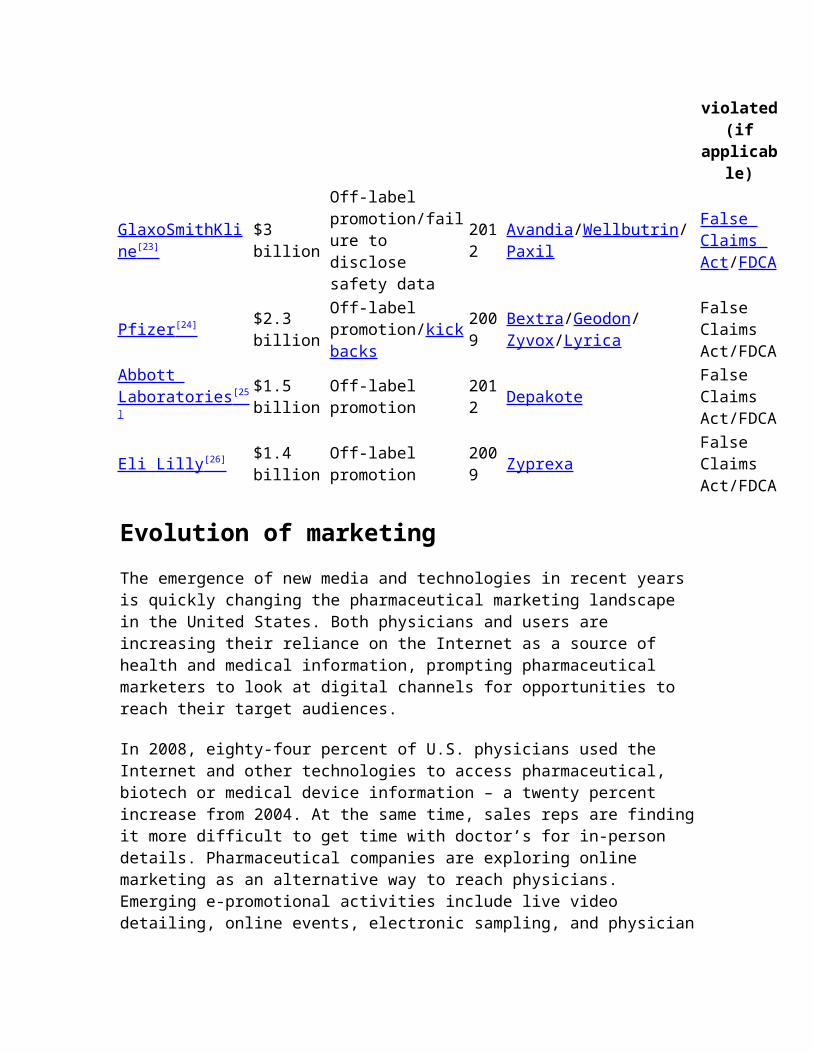
The following is a list of the four largest settlements reached with pharmaceutical companies from 1991 to 2012, rank ordered by the size of the total settlement. Legal claims against the pharmaceutical industry have varied widely over the past two decades, including Medicare and Medicaid fraud, off-label promotion, and inadequate manufacturing practices.[21][22]
Company Settlement
Violation(s) Year
Product(s) Lawsallegedl
y
violated(if
applicable)
GlaxoSmithKline [23]
$3 billion
Off-label promotion/failure to disclose safety data
2012
Avandia/Wellbutrin/Paxil
False Claims Act/FDCA
Pfizer [24] $2.3 billion
Off-label promotion/kickbacks
2009
Bextra/Geodon/Zyvox/Lyrica
False Claims Act/FDCA
Abbott Laboratories [25 ]
$1.5 billion
Off-label promotion
2012 Depakote
False Claims Act/FDCA
Eli Lilly [26] $1.4 billion
Off-label promotion
2009 Zyprexa
False Claims Act/FDCA
Evolution of marketingThe emergence of new media and technologies in recent years is quickly changing the pharmaceutical marketing landscape in the United States. Both physicians and users are increasing their reliance on the Internet as a source of health and medical information, prompting pharmaceutical marketers to look at digital channels for opportunities to reach their target audiences.
In 2008, eighty-four percent of U.S. physicians used the Internet and other technologies to access pharmaceutical, biotech or medical device information – a twenty percent increase from 2004. At the same time, sales reps are findingit more difficult to get time with doctor’s for in-person details. Pharmaceutical companies are exploring online marketing as an alternative way to reach physicians. Emerging e-promotional activities include live video detailing, online events, electronic sampling, and physician
customer service portals such as PV Updates, MDLinx, Physicians Interactive and Epocrates.
Direct-to-users marketers are also recognizing the need to shift to digital channels as audiences become more fragmented and the number of access points for news, entertainment and information multiplies. Standard television, radio and print direct-to-users (DTC) advertisements are less relevant than in the past, and companies are beginning to focus more on digital marketing efforts like product websites, online display advertising, search engine marketing, social media campaigns, and mobile advertising to reach the over 145 million U.S. adults onlinefor health information.
See also Big Pharma: How the World's Biggest Drug Companies Control Illness
(2006) by Jacky Law Side Effects (2008) by Alison Bass Bad Pharma (2012) by Ben Goldacre Biotechnology Disease mongering Ethics in pharmaceutical sales Food and Drug Administration Inverse benefit law List of pharmaceutical companies Medicare (United States) Medicare Part D Medicare Prescription Drug, Improvement, and
Modernization Act National pharmaceuticals policy Pharmaceutical company Pharmacology Predictive analytics Prescription Drug Marketing Act (PDMA) Prescription drug prices in the United States
References
1. ^ Jump up to: a b Brezis M (2008). "Big pharma andhealth care: unsolvable conflict of interests between private enterprise and public health". Isr J Psychiatry Relat Sci 45 (2): 83–9; discussion 90–4. PMID 18982834.
2. ^ Jump up to: a b c d e f g h i j k l m Sufrin CB, Ross JS (September 2008). "Pharmaceutical industry marketing: understanding its impact on women's health".Obstet Gynecol Surv 63 (9): 585–96. doi:10.1097/OGX.0b013e31817f1585. PMID 18713478.
3. ^ Jump up to: a b c d "www.medicine.mcgill.ca".4. Jump up ̂ Landefeld CS, Steinman MA (January
2009). "The Neurontin legacy--marketing through misinformation and manipulation". N. Engl. J. Med. 360 (2):103–6. doi:10.1056/NEJMp0808659. PMID 19129523.
5. Jump up ̂ "SK&A's 2010 Physician Access Survey".6. Jump up ̂ "Less than 30% of doctors prefer
edetailing, according to surveys -- doctor emails are primary promotional method".
7. ^ Jump up to: a b c d e f g "PhRMA Code's revised guidelines take effect January 2009".
8. Jump up ̂ Good Works Health9. ^ Jump up to: a b Alexander GC, Zhang J, Basu A.
Characteristics of patients receiving pharmaceutical samples and association between sample receipt and out-of-pocket prescription costs. Medical Care. 2008;46:394-402. [1]
10. Jump up ̂ "ZS Associates; Pharmaceutical".11. Jump up ̂ "www.pharmexec.com".12. Jump up ̂ "Glossary Term: Key Opinion Leader".13. Jump up ̂
http://www.lnxpharma.com/images/pages/Lnx_Whitepaper_1.pdf
14. Jump up ̂ "www.pharmexec.com".15. Jump up ̂ "Narrative Review: The Promotion of
Gabapentin: An Analysis of Internal Industry Documents -- Steinman et al. 145 (4): 284 -- Annals of Internal Medicine".
16. Jump up ̂ "Safeguarding Patient Welfare: Who's In Charge? -- Henney 145 (4): 305 -- Annals of Internal Medicine".
17. ^ Jump up to: a b "www.chmeds.ac.nz".18. Jump up ̂ Lunzer Kritz, Francesca (3 December
2007). "Check out drug coupons, then check bottom line". Los Angeles Times. Retrieved 20 November 2011.
19. Jump up ̂ "The ax comes out for pharma promotionalspending".
20. ^ Jump up to: a b Duff Wilson (October 2, 2010). "Side Effects May Include Lawsuits". New York Times.
21. Jump up ̂ Sammy Almashat, M.D., M.P.H., Charles Preston, M.D., M.P.H., Timothy Waterman, B.S., Sidney Wolfe, M.D., Rapidly Increasing Criminal and Civil Monetary Penalties Against the Pharmaceutical Industry:1991 – 2010, Public Citizen’s Health Research Group, December 16, 2010
22. Jump up ̂ http://www.nytimes.com/2012/07/03/business/glaxosmithkline-agrees-to-pay-3-billion-in-fraud-settlement.html?pagewanted=all
23. Jump up ̂ http://www.justice.gov/opa/pr/2012/July/12-civ-842.html
24. Jump up ̂ http://www.justice.gov/usao/ma/news/Pfizer/Pfizer%20-%20PR%20(Final).pdf
25. Jump up ̂ http://www.justice.gov/opa/pr/2012/May/12-civ-585.html
26. Jump up ̂ http://www.justice.gov/opa/pr/2009/January/09-civ-038.html
Further reading Insider's Guide to the World of Pharmaceutical Sales,
Seventh Edition (Paperback) (ISBN 0-9704153-6-2) Merrill Goozner: The $800 million pill. University of
California Press, Berkeley 2004, 297 S., ISBN 0-520-23945-8
Ray Moynihan, Alan Cassels: Selling sickness: How the world's biggest pharmaceutical companies are turning usall into patients. Nation Books, New York 2005
Be Brief, Be Bright, Be Gone: Career Essentials for Pharmaceutical Representatives (Paperback) (ISBN 0-595-17418-3)
PharmRepSelect-Your Complete Guide to Getting a Pharmaceutical Sales Job (Pharmrepselect, 1) (Paperback) (ISBN 0-9724675-1-3)
The Rx Factor : Strategic Creativity in Pharmaceutical Marketing (Response Book) (Hardcover) (ISBN 0-8039-9378-1)
Pharmaceutical Marketing: Principles, Environment, and Practice (Hardcover) (ISBN 0-7890-1582-X)
Presentation Planning and Media Relations for the Pharmaceutical Industry
Lynn Payer: Disease-Mongers. John Wiley, 1992 Little Black Book of Pharmaceutical Marketing [2] How To Conduct Doctor Dinner Meetings (Paperback) (ISBN
0-9656231-1-4) Drugs, Doctors and Dinners: How drug companies
influence health in the developing world. users International, London 2007 (ISBN 1-902391-59-4)[3]
360 Degree Selling - How To Sell Biotechnology Products(Paperback) (ISBN 0-9656231-3-0)
Selling To Specialist Physicians (Paperback) (ISBN 0-9656231-5-7)
Conroy, M.S., The Cosmetics Baron You've Never Heard Of: E. Virgil Neal and Tokalon, Altus History LLC, (Englewood), 2009. ISBN 0-615-27278-9
Conroy, M.S., The Soviet Pharmaceutical Business During the First Two Decades (1917-1937), Peter Lang, (New York), 2006. ISBN0-8204-7899-7
Alexander GC, Zhang J, Basu A. Characteristics of patients receiving pharmaceutical samples and association between sample receipt and out-of-pocket prescription costs Medical Care. 2008;46:394-402.
Categories:
Marketing Pharmaceutical industry Pharmaceuticals policy Pharmacy
Navigation menu Create account Log in
Article Talk
Read Edit View history
Main page Contents Featured content Current events Random article Donate to Wikipedia Wikimedia Shop
Interaction
Help About Wikipedia Community portal Recent changes Contact page
Tools
Print/export
Languages
ارسی ف�� Edit links
This page was last modified on 28 January 2014 at 10:07.
Text is available under the Creative Commons Attribution-ShareAlike License; additional terms may apply. By using this site, you agree to the Terms of Use and Privacy Policy. Wikipedia® is a registered trademark of the Wikimedia Foundation, Inc., a non-profit organization.
Privacy policy About Wikipedia Disclaimers Contact Wikipedia Developers Mobile view
Pharmaceutical marketingPharmaceutical marketing, sometimes called medico-marketing or pharma marketing in some countries, is the business of advertising or otherwise promoting the sale of pharmaceuticals or drugs.
Many countries have measures in place to limit advertising by pharmaceutical companies.
Pharmaceutical company spending on marketing far exceeds that spent on research.[1][2] In Canada, $1.7 billion was spent in 2004 to market drugs to physicians; in the United States, $21 billion was spent in 2002.[3] In 2005 money spenton pharmaceutical marketing in the US was estimated at $29.9billion with one estimate as high as $57 billion.[2] When theUS numbers are broken down, 56% was free samples, 25% was pharmaceutical sales representative "detailing" (promoting drugs directly to) physicians, 12.5% was direct to user advertising, 4% on detailing to hospitals, and 2% on journalads.[3] There is some evidence that marketing practices can negatively affect both patients and the health care profession.[4]
Contents 1 History 2 To health care providers
o 2.1 New pharma code & guidelines o 2.2 Free samples o 2.3 Continuing medical education o 2.4 Pharmaceutical representatives o 2.5 Peer influence o 2.6 Journal articles o 2.7 Private and public insurers
3 To users o 3.1 Drug coupons
4 Economics 5 Regulation and fraud 6 Evolution of marketing 7 See also 8 References 9 Further reading
HistoryThe marketing of medication has a long history. The sale of miracle cures, many with little real potency, has always been common. Marketing of legitimate non-prescription
medications, such as pain relievers or allergy medicine, hasalso long been practiced, although, until recently, mass marketing of prescription medications has been rare. It was long believed that since doctors made the selection of drugs, mass marketing was a waste of resources; specific adstargeting the medical profession were thought to be cheaper and just as effective.[citation needed] This would involve ads in professional journals and visits by sales staff to doctor’s offices and hospitals. An important part of these efforts was marketing to medical students.[citation needed]
To health care providersMarketing to health care providers takes four main forms: gifting, activity by pharmaceutical sales representatives, provision of drug samples, and sponsoring continuing medicaleducation (CME).[2] Of the 237,000 medical sites representing680,000 physicians surveyed in SK&A's 2010 Physician Access survey, half said they prefer or require an appointment to see a rep (up from 38.5% preferring or requiring an appointment in 2008), while 23% won't see reps at all, according to the survey data. Practices owned by hospitals or health systems are tougher to get into than private practices, since appointments have to go through headquarters, the survey found. 13.3% of offices with just one or two doctors won't see reps, compared with a no-see rate of 42% at offices with 10 or more docs The most accessible physicians for promotional purposes are allergists/immunologists – only 4.2% won't see reps at all –followed by orthopedic specialists (5.1%) and diabetes specialists (7.6%). Diagnostic radiologists are the most rigid about allowing details – 92.1% won't see reps – followed by pathologists and neuroradiologists, at 92.1% and91.8%, respectively.[5]
E-detailing is widely used to reach "no see physicians"; approximately 23% of primary care physicians and 28% of specialists prefer computer-based edetailing, according to survey findings reported in the April 25, 2011, edition of
American Medical News (AMNews), published by the American Medical Association (AMA).[6]
New pharma code & guidelines
The Pharmaceutical Research and Manufacturers of America (PhRMA) released updates to its voluntary Code on Interactions with Healthcare Professionals on July 10. The new guidelines take effect January 2009."[7]
In addition to prohibiting small gifts and reminder items such as pens, notepads, staplers, clipboards, pill boxes, etc.,[7] the revised Code:
1. Prohibits company sales representatives from providing restaurant meals to healthcare professionals, but allows them to provide occasional meals in healthcare professionals’ offices in conjunction with informational presentations"[7]
2. Includes new provisions requiring companies to ensure their representatives are sufficiently trained about applicable laws, regulations, and industry codes of practice and ethics.[7]
3. Provides that each company will state its intentions toabide by the Code and that company CEOs and compliance officers will certify each year that they have processes in place to comply.[7]
4. Includes more detailed standards regarding the independence of continuing medical education.[7]
5. Provides additional guidance and restrictions for speaking and consulting arrangements with healthcare professionals.[7]
However, the Good Works Health government-approved platform offers physicians and other health care professionals the opportunity to direct donations to charities of their choicein exchange for participation in pharmaceutical promotional/educational programs. [8]
Free samples
Free samples have been shown to affect physician prescribingbehaviour. Physicians with access to free samples are more likely to prescribe brand name medication over equivalent generic medications.[2] Other studies found that free samplesdecreased the likelihood that physicians would follow standard of care practices.[2]
Receiving pharmaceutical samples does not reduce prescription costs. Even after receiving samples, sample recipients remain disproportionately burdened by prescription costs.[9]
It is argued that a benefit to free samples is the “try it before you buy it” approach. Free Samples give immediate access to the medication and the patient can begin treatmentright away. Also, it saves time from going to a pharmacy to get it filled before treatment begins. Since not all medications work for everyone, and many do not work the sameway for each person, free samples allow patients to find which dose and brand of medication works best before having to spend money on a filled prescription at a pharmacy.[9]
Continuing medical education
Hours spent by physicians in industry-supported CME is greater than that from either medical schools or professional societies.[2]
Pharmaceutical representatives
Currently, there are approximately 81,000 pharmaceutical sales representatives in the United States[10] pursuing some 830,000 pharmaceutical prescribers. A pharmaceutical representative will often try to see a given physician everyfew weeks. Representatives often have a call list of about 200-300 physicians with 120-180 targets that should be visited in 1-2 or 3 week cycle.
Because of the large size of the pharmaceutical sales force,the organization, management, and measurement of
effectiveness of the sales force are significant business challenges. Management tasks are usually broken down into the areas of physician targeting, sales force size and structure, sales force optimization, call planning, and sales forces effectiveness. A few pharmaceutical companies have realized that training sales representatives on high science alone is not enough, especially when most products are similar in quality. Thus, training sales representativeson relationship selling techniques in addition to medical science and product knowledge, can make a difference in sales force effectiveness. Specialist physicians are relyingmore and more on specialty sales reps for product information, because they are more knowledgeable than primary care reps.
The United States has 81,000 pharmaceutical representatives or 1 for every 7.9 physicians.[2] The number and persistence of pharmaceutical representatives has placed a burden on thetime of physicians.[11] "As the number of reps went up, the amount of time an average rep spent with doctors went down—so far down, that tactical scaling has spawned a strategic crisis. Physicians no longer spend much time with sales reps, nor do they see this as a serious problem."
Marketers must decide on the appropriate size of a sales force needed to sell a particular portfolio of drugs to the target market. Factors influencing this decision are the optimal reach (how many physicians to see) and frequency (how often to see them) for each individual physician, how many patients suffer from that disease state, how many salesrepresentatives to devote to office and group practice and how many to devote to hospital accounts if needed. To aid this decision, customers are broken down into different classes according to their prescription behavior, patient population, and of course, their business potential.
Marketers attempt to identify the set of physicians most likely to prescribe a given drug. Historically, this was done by measuring the number of total prescriptions (TRx) and new prescriptions (NRx) per week that each physician
writes. This information is collected by commercial vendors.The physicians are then "deciled" into ten groups based on their writing patterns. Higher deciles are more aggressivelytargeted. Some pharmaceutical companies use additional information such as:
profitability of a prescription (script), accessibility of the physician, tendency of the physician to use the pharmaceutical
company's drugs, effect of managed care formularies on the ability of
the physician to prescribe a drug, the adoption sequence of the physician (that is, how
readily the physician adopts new drugs in place of older treatments), and
the tendency of the physician to use a wide palette of drugs
influence that physicians have on their colleagues.
Data for drugs prescribed in a hospital are not usually available at the physician level. Advanced analytic techniques are used to value physicians in a hospital setting.[citation needed]
Physicians are perhaps the most important component in sales. They write the prescriptions that determine which drugs will be used by people. Influencing the physician is the key to pharmaceutical sales. Historically, this was doneby a large pharmaceutical sales force. A medium-sized pharmaceutical company might have a sales force of 1000 representatives.[citation needed] The largest companies have tens of thousands of representatives around the world. Sales representatives called upon physicians regularly, providing clinical information, approved journal articles, and free drug samples. This is still the approach today; however, economic pressures on the industry are causing pharmaceutical companies to rethink the traditional sales process to physicians. The industry has seen a large scale adoption of Pharma CRM systems that works on laptops and more recently tablets. The new age pharmaceutical
representative is armed with key data at his fingertips and tools to maximize the time spent with physicians.
Peer influence
Key opinion leaders
Key opinion leaders (KOL), or "thought leaders", are respected individuals, such as prominent medical school faculty, who influence physicians through their professionalstatus. Pharmaceutical companies generally engage key opinion leaders early in the drug development process to provide advocacy and key marketing feedback.[12] Some pharmaceutical companies identify key opinion leaders through direct inquiry of physicians (primary research). Recently, pharmaceutical companies have begun to use social network analysis to uncover thought leaders; because it doesnot introduce respondent bias, which is commonly found in primary research; it can identify and map out the entire scientific community for a disease state; and it has greatercompliance with state and federal regulations; because physician prescribing patterns are not used to create the social network.[13]
Alternatives to segmenting physicians purely on the basis ofprescribing do exist, and marketers can call upon strategic partners who specialize in delineating which characteristicsof true opinion leadership, a physician does or does not possess. Such analyses can help guide marketers in how to optimize KOL engagements as bona fide advisors to a brand, and can help shape clinical development and clinical data publication plans for instance, ultimately advancing patientcare.
Colleagues
Physicians acquire information through informal contacts with their colleagues, including social events, professionalaffiliations, common hospital affiliations, and common medical school affiliations. Some pharmaceutical companies
identify influential colleagues through commercially available prescription writing and patient level data.[14] Doctor dinner meetings are an effective way for physicians to acquire educational information from respected peers. These meetings are sponsored by some pharmaceutical companies.
Journal articles
See also: Medical ghostwriter
Recent legal cases and US congressional hearings have provided access to pharmaceutical industry documents revealing new marketing strategies for drugs.[15] Activities once considered independent of promotional intent, includingcontinuing medical education and medical research, are used,including paying to publish articles about promoted drugs for the medical literature, and alleged suppression of unfavorable study results.[16]
Private and public insurers
Public and private insurers affect the writing of prescriptions by physicians through formularies that restrict the number and types of drugs that the insurer willcover. Not only can the insurer affect drug sales by including or excluding a particular drug from a formulary, they can affect sales by tiering, or placing bureaucratic hurdles to prescribing certain drugs. In January 2006, the U.S. instituted a new public prescription drug plan through its Medicare program. Known as Medicare Part D, this programengages private insurers to negotiate with pharmaceutical companies for the placement of drugs on tiered formularies.
To usersOnly two countries as of 2008 allow direct to users advertising (DTCA): the United States and New Zealand.[2] Since the late 1970s, DTCA of prescription drugs has become
important in the United States. It takes two main forms: thepromotion or creation of a disease out of a non-pathologic physical condition or the promotion of a medication.[2] Many people will inquire about, or even demand a medication they have seen advertised on television.[who?] In the United States, recent years have seen an increase in mass media advertisements for pharmaceuticals. Expenditures on direct-to-users advertising have more than quintupled in the seven years between 1997 and 2005 since the FDA changed the guidelines, from $1.1 billion in 1997 to more than $4.2 billion in 2005, a 19.6% annual increase, according to the United States GAO (Government Accountability Office, 2006).[2]
The mass marketing to users of pharmaceuticals is banned in over 30 industrialized nations, but not in the US and New Zealand, which is considering a ban.[17] Some feel it is better to leave the decision wholly in the hands of medical professionals; others feel that users education and participation in health is useful, but users need independent, comparative information about drugs (not promotional information).[17] For these reasons, most countries impose limits on pharmaceutical mass marketing that are not placed on the marketing of other products. In some areas it is required that ads for drugs include a list of possible side effects, so that users are informed of bothfacets of a medicine. Canada's limitations on pharmaceuticaladvertising ensure that commercials that mention the name ofa product cannot in any way describe what it does. Commercials that mention a medical problem cannot also mention the name of the product for sale; at most, they can direct the viewer to a website or telephone number operated by the pharmaceutical company.
Drug coupons
In the United States, pharmaceutical companies often providedrug coupons to consumers to help offset the copayments charged by health insurers for prescription medication.
These coupons are generally used to promote medications thatcompete with non-preferred products and cheaper, generic alternatives by reducing or eliminating the extra out-of-pocket costs that an insurers typically charge a patient fora non-preferred drug product.[18]
EconomicsPharmaceutical company spending on marketing exceeds that spent on research.[1][2] In 2004 in Canada $1.7 billion a yearwas spent marketing drugs to physicians and in the United States $21 billion were spent in 2002.[3] In 2005 money spenton pharmaceutical marketing in the US was estimated at $29.9billion with one estimate as high as $57 billion.[2] When theUS number are broken down 56% was free samples, 25% was detailing of physicians, 12.5% was direct to users advertising, 4% on hospital detailing, and 2% on journal ads.[3] In the United States approximately $20 billion could be saved if generics were used instead of equivalent brand name products.[2]
Although pharmaceutical companies have made large investments in marketing their products, overall promotionalspending has been decreasing over the last few years, and declined by 10 percent from 2009 to 2010. Pharmaceutical companies are cutting back mostly in detailing and sampling,while spending in mailings and print advertising grew since last year.[19]
Regulation and fraudSee also: List of Largest Pharmaceutical SettlementsSee also: List of off-label promotion pharmaceutical settlements
In the United States, marketing and distribution of pharmaceuticals is regulated by the Federal Food, Drug, and Cosmetic Act and the Prescription Drug Marketing Act, respectively. Food and Drug Administration (FDA) regulations
require all prescription drug promotion to be truthful and not misleading, based on "substantial evidence or substantial clinical experience", to provide a "fair balance" between the risks and benefits of the promoted drug, and to maintain consistency with labeling approved by the FDA. The FDA Office of Prescription Drug Promotion enforces these requirements.
Antipsychotic drugs are now the top-selling class of pharmaceuticals in America, generating annual revenue of about $14.6 billion. Large pharmaceutical companies got behind the development of the drugs in the 1990s, when they were "still seen as treatments for the most serious mental illnesses, like hallucinatory schizophrenia, and recast themfor much broader uses". Drugs such as Abilify and Geodon were given to a broad range of patients, from preschoolers to octogenarians. In 2010, more than a half-million youths took antipsychotic drugs, and one-quarter of nursing-home residents have used them. Yet the government warns that the drugs may be fatal to some older patients and have unknown effects on children.[20]
Every major company selling the drugs — Bristol-Myers Squibb, Eli Lilly, Pfizer, AstraZeneca and Johnson & Johnson— has either settled recent government cases, under the False Claims Act, for hundreds of millions of dollars or is currently under investigation for possible health care fraud. Following charges of illegal marketing, two of the settlements set records last year for the largest criminal fines ever imposed on corporations. One involved Eli Lilly’santipsychotic Zyprexa, and the other involved Bextra. In theBextra case, the government also charged Pfizer with illegally marketing another antipsychotic, Geodon; Pfizer settled that part of the claim for $301 million, without admitting any wrongdoing.[20]
The following is a list of the four largest settlements reached with pharmaceutical companies from 1991 to 2012, rank ordered by the size of the total settlement. Legal claims against the pharmaceutical industry have varied
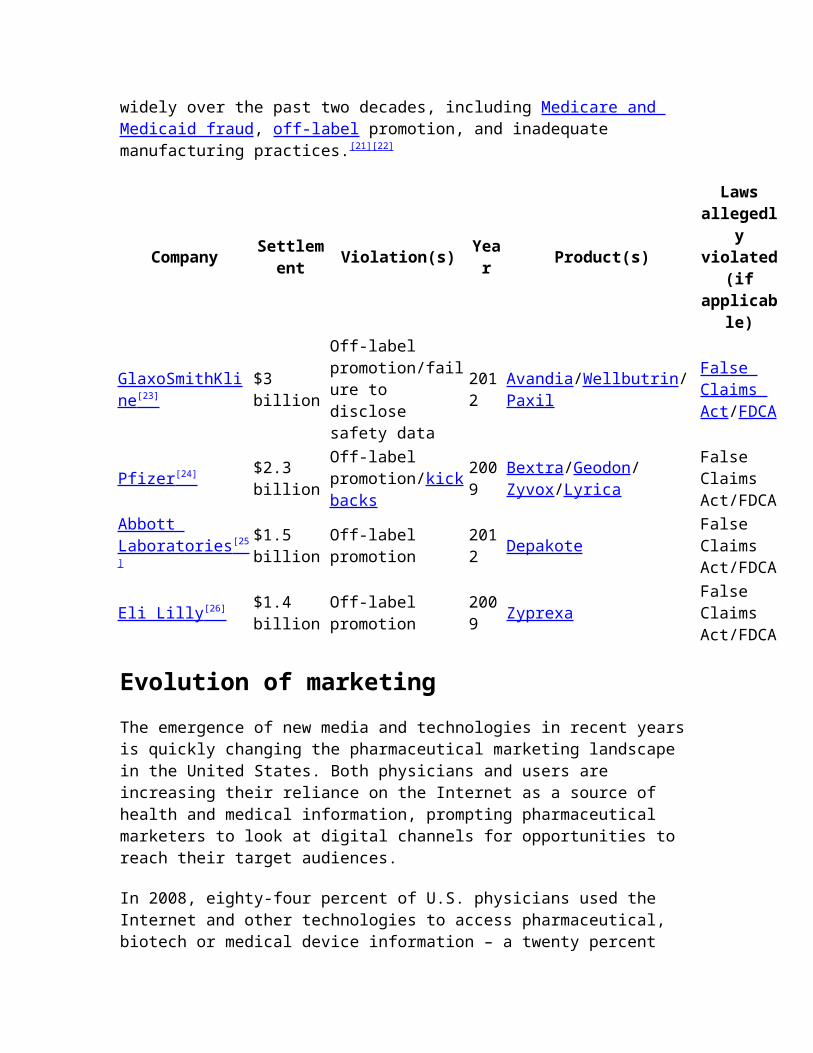
widely over the past two decades, including Medicare and Medicaid fraud, off-label promotion, and inadequate manufacturing practices.[21][22]
Company Settlement Violation(s) Yea
r Product(s)
Lawsallegedl
yviolated
(ifapplicab
le)
GlaxoSmithKline [23]
$3 billion
Off-label promotion/failure to disclose safety data
2012
Avandia/Wellbutrin/Paxil
False Claims Act/FDCA
Pfizer [24] $2.3 billion
Off-label promotion/kickbacks
2009
Bextra/Geodon/Zyvox/Lyrica
False Claims Act/FDCA
Abbott Laboratories [25 ]
$1.5 billion
Off-label promotion
2012 Depakote
False Claims Act/FDCA
Eli Lilly [26] $1.4 billion
Off-label promotion
2009 Zyprexa
False Claims Act/FDCA
Evolution of marketingThe emergence of new media and technologies in recent years is quickly changing the pharmaceutical marketing landscape in the United States. Both physicians and users are increasing their reliance on the Internet as a source of health and medical information, prompting pharmaceutical marketers to look at digital channels for opportunities to reach their target audiences.
In 2008, eighty-four percent of U.S. physicians used the Internet and other technologies to access pharmaceutical, biotech or medical device information – a twenty percent
increase from 2004. At the same time, sales reps are findingit more difficult to get time with doctor’s for in-person details. Pharmaceutical companies are exploring online marketing as an alternative way to reach physicians. Emerging e-promotional activities include live video detailing, online events, electronic sampling, and physiciancustomer service portals such as PV Updates, MDLinx, Physicians Interactive and Epocrates.
Direct-to-users marketers are also recognizing the need to shift to digital channels as audiences become more fragmented and the number of access points for news, entertainment and information multiplies. Standard television, radio and print direct-to-users (DTC) advertisements are less relevant than in the past, and companies are beginning to focus more on digital marketing efforts like product websites, online display advertising, search engine marketing, social media campaigns, and mobile advertising to reach the over 145 million U.S. adults onlinefor health information.
See also Big Pharma: How the World's Biggest Drug Companies Control Illness
(2006) by Jacky Law Side Effects (2008) by Alison Bass Bad Pharma (2012) by Ben Goldacre Biotechnology Disease mongering Ethics in pharmaceutical sales Food and Drug Administration Inverse benefit law List of pharmaceutical companies Medicare (United States) Medicare Part D Medicare Prescription Drug, Improvement, and
Modernization Act National pharmaceuticals policy Pharmaceutical company
Pharmacology Predictive analytics Prescription Drug Marketing Act (PDMA) Prescription drug prices in the United States
References1. ^ Jump up to: a b Brezis M (2008). "Big pharma and
health care: unsolvable conflict of interests between private enterprise and public health". Isr J Psychiatry Relat Sci 45 (2): 83–9; discussion 90–4. PMID 18982834.
2. ^ Jump up to: a b c d e f g h i j k l m Sufrin CB, Ross JS (September 2008). "Pharmaceutical industry marketing: understanding its impact on women's health".Obstet Gynecol Surv 63 (9): 585–96. doi:10.1097/OGX.0b013e31817f1585. PMID 18713478.
3. ^ Jump up to: a b c d "www.medicine.mcgill.ca".4. Jump up ̂ Landefeld CS, Steinman MA (January
2009). "The Neurontin legacy--marketing through misinformation and manipulation". N. Engl. J. Med. 360 (2):103–6. doi:10.1056/NEJMp0808659. PMID 19129523.
5. Jump up ̂ "SK&A's 2010 Physician Access Survey".6. Jump up ̂ "Less than 30% of doctors prefer
edetailing, according to surveys -- doctor emails are primary promotional method".
7. ^ Jump up to: a b c d e f g "PhRMA Code's revised guidelines take effect January 2009".
8. Jump up ̂ Good Works Health9. ^ Jump up to: a b Alexander GC, Zhang J, Basu A.
Characteristics of patients receiving pharmaceutical samples and association between sample receipt and out-of-pocket prescription costs. Medical Care. 2008;46:394-402. [1]
10. Jump up ̂ "ZS Associates; Pharmaceutical".11. Jump up ̂ "www.pharmexec.com".12. Jump up ̂ "Glossary Term: Key Opinion Leader".13. Jump up ̂
http://www.lnxpharma.com/images/pages/Lnx_Whitepaper_1.pdf
14. Jump up ̂ "www.pharmexec.com".15. Jump up ̂ "Narrative Review: The Promotion of
Gabapentin: An Analysis of Internal Industry Documents -- Steinman et al. 145 (4): 284 -- Annals of Internal Medicine".
16. Jump up ̂ "Safeguarding Patient Welfare: Who's In Charge? -- Henney 145 (4): 305 -- Annals of Internal Medicine".
17. ^ Jump up to: a b "www.chmeds.ac.nz".18. Jump up ̂ Lunzer Kritz, Francesca (3 December
2007). "Check out drug coupons, then check bottom line". Los Angeles Times. Retrieved 20 November 2011.
19. Jump up ̂ "The ax comes out for pharma promotionalspending".
20. ^ Jump up to: a b Duff Wilson (October 2, 2010). "Side Effects May Include Lawsuits". New York Times.
21. Jump up ̂ Sammy Almashat, M.D., M.P.H., Charles Preston, M.D., M.P.H., Timothy Waterman, B.S., Sidney Wolfe, M.D., Rapidly Increasing Criminal and Civil Monetary Penalties Against the Pharmaceutical Industry:1991 – 2010, Public Citizen’s Health Research Group, December 16, 2010
22. Jump up ̂ http://www.nytimes.com/2012/07/03/business/glaxosmithkline-agrees-to-pay-3-billion-in-fraud-settlement.html?pagewanted=all
23. Jump up ̂ http://www.justice.gov/opa/pr/2012/July/12-civ-842.html
24. Jump up ̂ http://www.justice.gov/usao/ma/news/Pfizer/Pfizer%20-%20PR%20(Final).pdf
25. Jump up ̂ http://www.justice.gov/opa/pr/2012/May/12-civ-585.html
26. Jump up ̂ http://www.justice.gov/opa/pr/2009/January/09-civ-038.html
Further reading
Insider's Guide to the World of Pharmaceutical Sales, Seventh Edition (Paperback) (ISBN 0-9704153-6-2)
Merrill Goozner: The $800 million pill. University of California Press, Berkeley 2004, 297 S., ISBN 0-520-23945-8
Ray Moynihan, Alan Cassels: Selling sickness: How the world's biggest pharmaceutical companies are turning usall into patients. Nation Books, New York 2005
Be Brief, Be Bright, Be Gone: Career Essentials for Pharmaceutical Representatives (Paperback) (ISBN 0-595-17418-3)
PharmRepSelect-Your Complete Guide to Getting a Pharmaceutical Sales Job (Pharmrepselect, 1) (Paperback) (ISBN 0-9724675-1-3)
The Rx Factor : Strategic Creativity in Pharmaceutical Marketing (Response Book) (Hardcover) (ISBN 0-8039-9378-1)
Pharmaceutical Marketing: Principles, Environment, and Practice (Hardcover) (ISBN 0-7890-1582-X)
Presentation Planning and Media Relations for the Pharmaceutical Industry
Lynn Payer: Disease-Mongers. John Wiley, 1992 Little Black Book of Pharmaceutical Marketing [2] How To Conduct Doctor Dinner Meetings (Paperback) (ISBN
0-9656231-1-4) Drugs, Doctors and Dinners: How drug companies
influence health in the developing world. users International, London 2007 (ISBN 1-902391-59-4)[3]
360 Degree Selling - How To Sell Biotechnology Products(Paperback) (ISBN 0-9656231-3-0)
Selling To Specialist Physicians (Paperback) (ISBN 0-9656231-5-7)
Conroy, M.S., The Cosmetics Baron You've Never Heard Of: E. Virgil Neal and Tokalon, Altus History LLC, (Englewood), 2009. ISBN 0-615-27278-9
Conroy, M.S., The Soviet Pharmaceutical Business During the First Two Decades (1917-1937), Peter Lang, (New York), 2006. ISBN0-8204-7899-7
Alexander GC, Zhang J, Basu A. Characteristics of patients receiving pharmaceutical samples and association between sample receipt and out-of-pocket prescription costs Medical Care. 2008;46:394-402.
Categories: Marketing Pharmaceutical industry Pharmaceuticals policy Pharmacy
Navigation menu Create account Log in
Article Talk
Read Edit View history
Main page Contents Featured content Current events Random article Donate to Wikipedia Wikimedia Shop
Interaction
Help About Wikipedia Community portal Recent changes Contact page
Tools
Print/export
Languages
ارسی ف�� Edit links
This page was last modified on 28 January 2014 at 10:07.
Text is available under the Creative Commons Attribution-ShareAlike License; additional terms may apply. By using this site, you agree to the Terms of Use and Privacy Policy. Wikipedia® is a registered trademark of the Wikimedia Foundation, Inc., a non-profit organization.
Privacy policy About Wikipedia Disclaimers Contact Wikipedia Developers Mobile view
ijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 5 6MARCH 2012VOL 3, NO 11ETHICAL AND NON-ETHICAL PHARMACEUTICAL MARKETINGPRACTICES: CASE STUDY OF KARACHI CITYRizwan Rahim Ahmed,Research Scholar (PH.D)Hamdard Institute of Education and Social Sciences (HIESS)
Hamdard University, Karachi - PakistanDR. AHMED SAEEDResearch SupervisorAbstractUnethical marketing practices has become an essential part of the pharmaceuticalindustry in Pakistan and it roots is so strong that it may not be possible to reverse thesame. However previous study has a limitation and was a casestudy on pharmaceuticalindustry only in Hyderabad. In view of the findings of previous study there was a needto carry out the same on Pakistan basis. Thus this research has been undertaken withthis objective in mind. The focus of the subject study was to identify the intensity andtrends of unethical drug promotion practices in Pakistan. Ascertaining the contributionof the doctors, health related institutions and the pharmaceutical industry in promotingsuch practices.Keywords: Ethical pharmaceutical marketing practices, non-ethical pharmaceuticalmarketing practices, marketing practices1. IntroductionUnethical marketing practices has become an essential part of the pharmaceutical industry inPakistan and it roots is so strong that it may not be possible to reverse the same (Parmar &Jalees, 2004). However this previous study has a limitation.It was a case study onpharmaceutical industry in Hyderabad. In view of the findings of this study there was a needto carry out the same on Pakistan basis. Thus this research has been undertaken with thisobjective in mind.The phenomenon of the unethical drug practices is common worldwide but its severity ismore deep rooted in developing countries. Unethical drug practices have two dimensions.
One is drug related, and other is drug promotion related. Extensive research on drug relatedunethical practices has been carried out internationally. However, the author was not able tofind any empirical study on unethical drug promotion practices except the one that wascarried out by (Parmar, Jalees, 2004). Parmar and Jalees (2004) in their study observed thatpharmaceutical industry spends a substantial portion of its budget on market research but donot carry out the research on unethical drug promotion practices. One of the reasons is thatthe industry itself is indulged in this practice therefore it does not find any need to carry outthe research on this issue.ijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 5 7MARCH 2012VOL 3, NO 11Lack of research on the subject does not mean that unethicaldrug promotion practices do notexist. The pre-survey and focus groups discussions indicate that unethical pharmaceuticalmarketing practices have become an acceptable norm of the pharmaceutical industry, andalmost all the pharmaceutical companies patronized these unethical practices in collaborationwith doctors, government and private hospitals, health related agencies and pharmacies at thecost of patients’ well being. All the entities as discussed above appears to be corrupted,therefore, it may not be fair to blame any one of them, including pharmaceutical industry.Doctors and other entities as discussed above have become greedy, therefore, are vulnerableto Pharmaceutical industry unethical drug promotion practices. Most of the conferences and
academic activities of doctors are sponsored by the Pharmaceutical Industry; therefore, theindustry uses the forum to pursue its goals which at times may not be the same as the purposeand objective of the conferences. Pakistan Medical Journalists Association (PMJA) haspublished a few articles on this issue. But this has not affected the prevailing unethical drugpromotion practices (Zaidi et.al, 1995).The focus of the subject study was to identify the intensityand trends of unethical drugpromotion practices in Pakistan. Ascertaining the contribution of the doctors, health relatedinstitutions and the pharmaceutical industry in promoting such practices. Unethical marketingpractices have now an integral part of drug promotion. Unethical practices could be classifiedinto two segments. One is related to the medical side of thedrug i.e. the trial of the drug bothon animals and the human, and registration of indications and patent period in differentcountries.According to the prominent scholar and eminent physician of the country, Dr Sania Nishtar(2007), the anecdotal reports of corruption in the pharmaceutical sector must receive carefuland objective analysis. Corruption in this domain has a direct bearing on the performance ofthe health system. This practice can involve both the regulators and the private sector andmay involve any step along the drug supply chain, starting from registration, licensing andaccreditation to the setting of prices, marketing of drugs and sale and procurements.Corruption in this sector has its roots in the commercial interests of the non-bonafidepharmaceutical companies, who find compliance with regulations costly and try to bypass
procedures to get their product registered, speed up the approval process, and get favorableprices or to have their drugs included on the essential druglist in order to increase theirmarket share.The contracting process for the purchase of drugs offers a lucrative source of returns forcorrupt officials and suppliers through kickbacks, over-invoicing, and outright graft. There isanecdotal evidence for the same in Pakistan from several public hospitals; however this needsto be assessed carefully and its magnitude quantified.In a nutshell therefore, healthcare provision depends on a system which efficiently combinesfinancial and human resources and supplies to deliver services; good governance andtransparency are critical factors in making such a system function. However on the otherhand, both poor governance and corruption in the health system are manifestations of abroader systems phenomenon in a country. Addressing these issues requires mandates andprerogatives both within but also outside of the health sector, which is why ideally, ananticorruption drive in health must ride a much larger wave (Sania, 2007).ijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 5 8MARCH 2012VOL 3, NO 112. Previous ResearchThere are about 650 leading Nationals and Multinational pharmaceutical companies operatingin Pakistan. Of this total 23 are multinationals and rests of companies are local companies.The local companies could be classified into three categories which are (1) Manufacturing
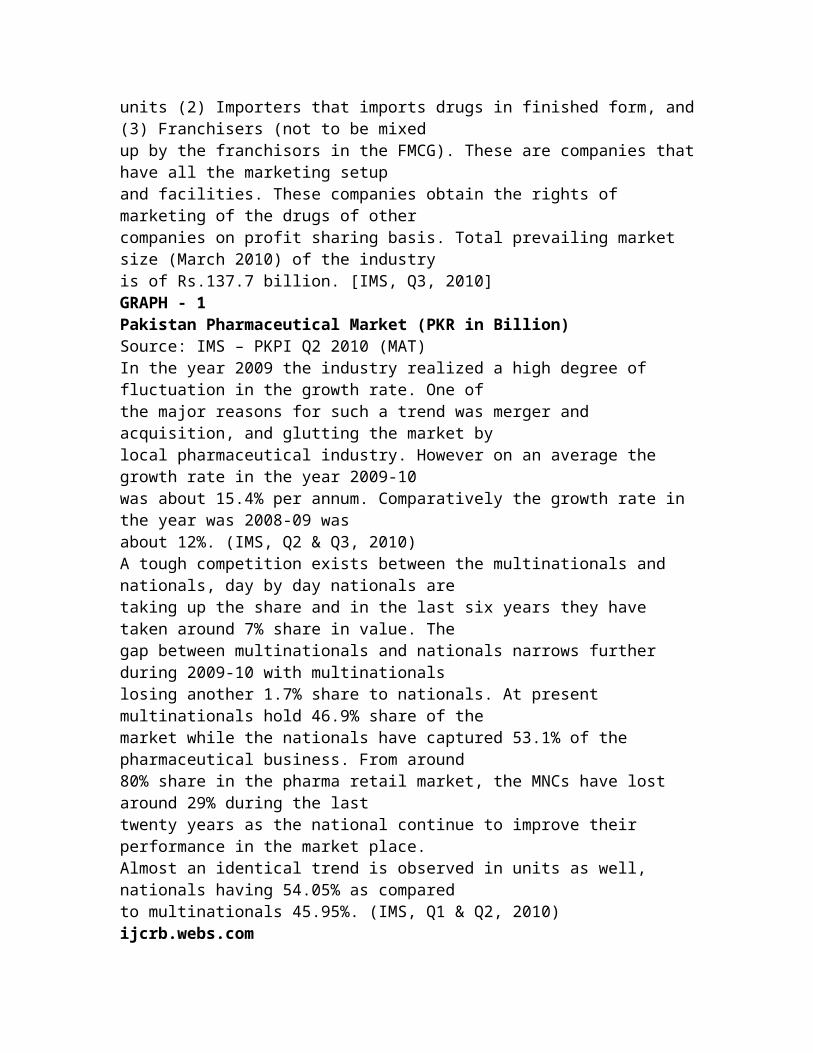
units (2) Importers that imports drugs in finished form, and(3) Franchisers (not to be mixedup by the franchisors in the FMCG). These are companies thathave all the marketing setupand facilities. These companies obtain the rights of marketing of the drugs of othercompanies on profit sharing basis. Total prevailing market size (March 2010) of the industryis of Rs.137.7 billion. [IMS, Q3, 2010]GRAPH - 1Pakistan Pharmaceutical Market (PKR in Billion)Source: IMS – PKPI Q2 2010 (MAT)In the year 2009 the industry realized a high degree of fluctuation in the growth rate. One ofthe major reasons for such a trend was merger and acquisition, and glutting the market bylocal pharmaceutical industry. However on an average the growth rate in the year 2009-10was about 15.4% per annum. Comparatively the growth rate in the year was 2008-09 wasabout 12%. (IMS, Q2 & Q3, 2010)A tough competition exists between the multinationals and nationals, day by day nationals aretaking up the share and in the last six years they have taken around 7% share in value. Thegap between multinationals and nationals narrows further during 2009-10 with multinationalslosing another 1.7% share to nationals. At present multinationals hold 46.9% share of themarket while the nationals have captured 53.1% of the pharmaceutical business. From around80% share in the pharma retail market, the MNCs have lost around 29% during the lasttwenty years as the national continue to improve their performance in the market place.Almost an identical trend is observed in units as well, nationals having 54.05% as comparedto multinationals 45.95%. (IMS, Q1 & Q2, 2010)ijcrb.webs.com
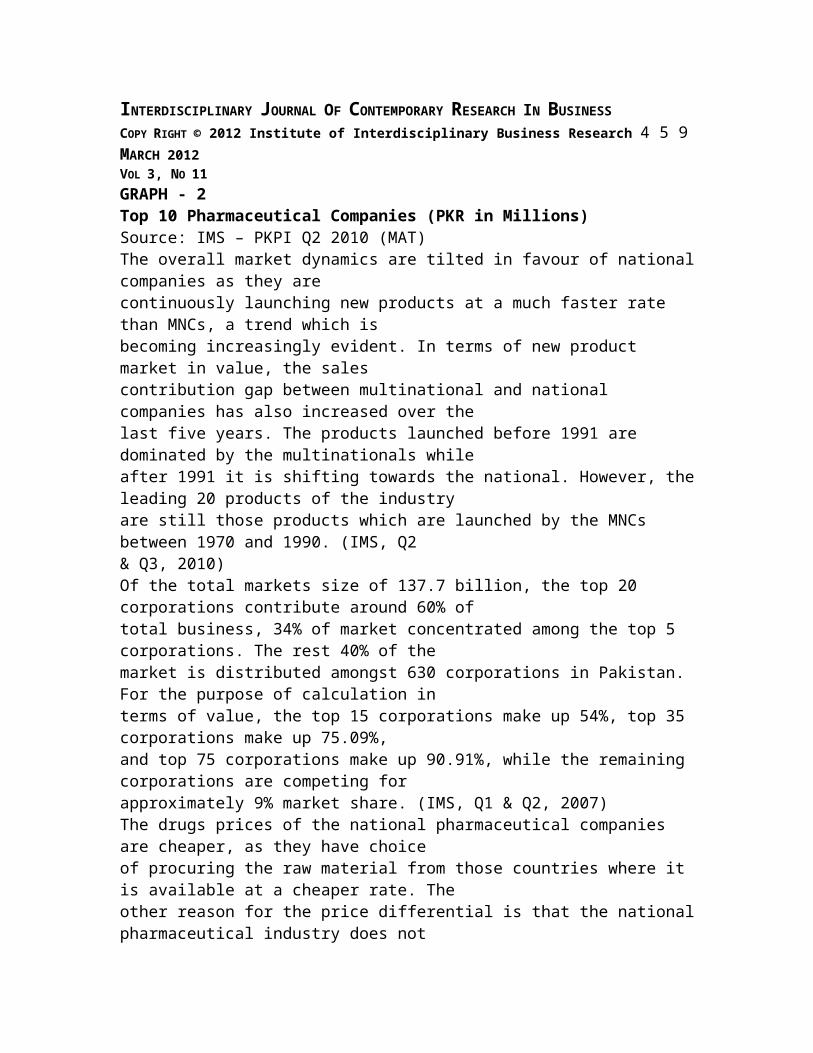
INTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 5 9MARCH 2012VOL 3, NO 11GRAPH - 2Top 10 Pharmaceutical Companies (PKR in Millions)Source: IMS – PKPI Q2 2010 (MAT)The overall market dynamics are tilted in favour of nationalcompanies as they arecontinuously launching new products at a much faster rate than MNCs, a trend which isbecoming increasingly evident. In terms of new product market in value, the salescontribution gap between multinational and national companies has also increased over thelast five years. The products launched before 1991 are dominated by the multinationals whileafter 1991 it is shifting towards the national. However, theleading 20 products of the industryare still those products which are launched by the MNCs between 1970 and 1990. (IMS, Q2& Q3, 2010)Of the total markets size of 137.7 billion, the top 20 corporations contribute around 60% oftotal business, 34% of market concentrated among the top 5 corporations. The rest 40% of themarket is distributed amongst 630 corporations in Pakistan. For the purpose of calculation interms of value, the top 15 corporations make up 54%, top 35 corporations make up 75.09%,and top 75 corporations make up 90.91%, while the remaining corporations are competing forapproximately 9% market share. (IMS, Q1 & Q2, 2007)The drugs prices of the national pharmaceutical companies are cheaper, as they have choiceof procuring the raw material from those countries where it is available at a cheaper rate. Theother reason for the price differential is that the nationalpharmaceutical industry does not
invest in research and development compare to multinationals. Multinational companiesinvest a huge amount of their net profit in R & D, therefore, when they introduce a newmolecule into the market they have already invested billionsof dollars for a new product,therefore, the price of the new product keeps high in order to meet the total cost of the drug ina certain time period because after patent period any company can make its Me too orimitation at cheaper rate. So, the national companies have twice leverage to set their prices atthe lower lever i.e. first they did not invest a single penny on Research & Development andsecondly they are having cheaper raw material resources (Parmar & Jalees, 2004).Another, important point in price difference is that national companies are not bound to paycertain amount of profit to any other body, whereas, multinational companies are payingcertain percentage of profit to their parent companies. Moreover, national companies do nothave huge overhead expenses; in contrast, multinational companies allocate huge overheadexpenses in different fields at the beginning of every fiscal year for every product in a certainratio, therefore, the cost of goods (COG) are different in national and multinationalijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 6 0MARCH 2012VOL 3, NO 11companies. In order to maintain all these costs they are bound to set a high price, otherwisebottom line will be very low and business would not be feasible any more.One of the reasons why the sector is vulnerable to corruption is that it is heavily regulated.
Heavily regulation is essential to safeguard the population against sub-standard drugs andunfairly priced goods. But there is a second central reason why governments regulate thepharmaceutical market: to ensure that industrial policies strengthen economiccompetitiveness of the pharmaceutical sector and improve innovation and efficiency. Thesetwo objectives can sometimes lie at cross-purposes. If regulators are subject to pressure fromcommercial groups, health objectives can be compromised. Generous political campaigndonations and lobbying expenditures by pharmaceutical companies are examples of suchpressures.The relationship between drugs companies and physicians is also vulnerable to corruption.Doctors may be offered commissions for prescribing a particular drug or a drug from aparticular company. Because this practice is illegal in mostcountries, companies may employunderhand methods to disguise such kickbacks. The aggressivepromotion of medicines, thesheer volume of information that is received in its many forms by prescribers and the use ofpatient groups through which to generate demand for prescription drugs, all contribute to theinappropriate prescription of medicines. In the United States some US$ 16 billion is spentannually by pharmaceutical, device and biotechnology industries on marketing to physicians.The issue of unethical pharmaceutical marketing practice hasreceived a great deal ofattention in recent years, prompting many doctors associations, pharmaceutical industryassociations and individual corporations to engage with the issue. Many have passed codes ofconduct and ethical guidelines for the marketing of pharmaceuticals; but if not monitored and
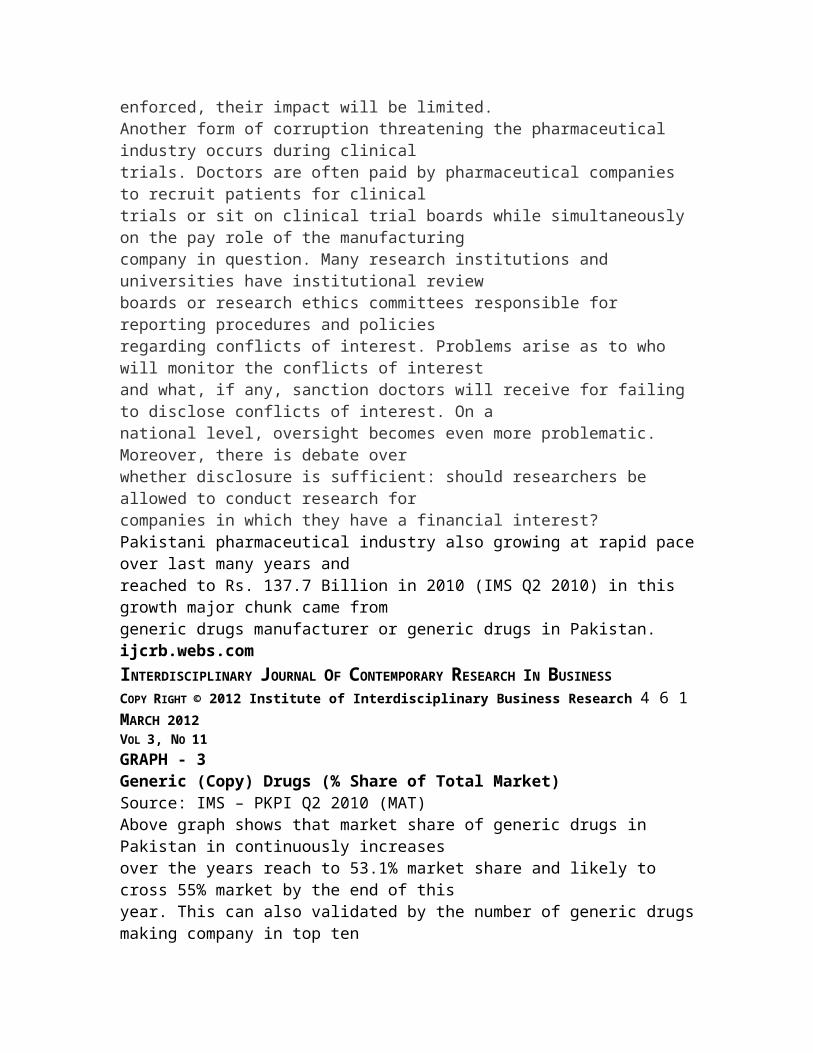
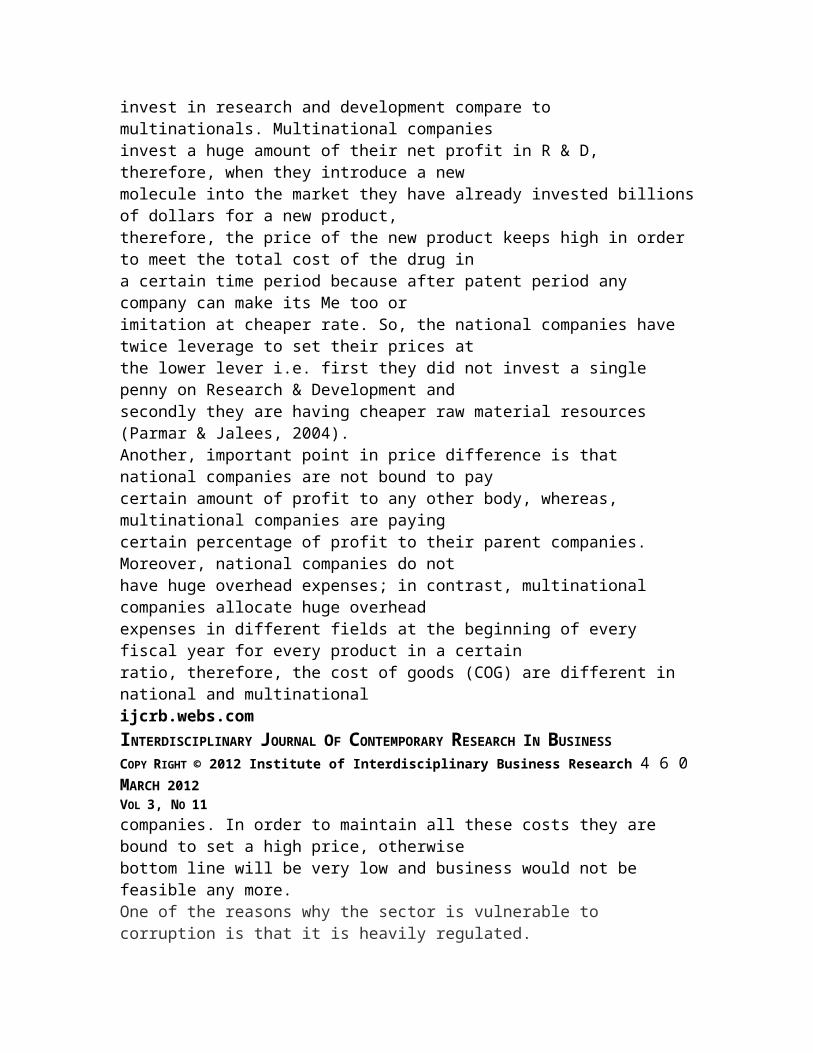
enforced, their impact will be limited.Another form of corruption threatening the pharmaceutical industry occurs during clinicaltrials. Doctors are often paid by pharmaceutical companies to recruit patients for clinicaltrials or sit on clinical trial boards while simultaneously on the pay role of the manufacturingcompany in question. Many research institutions and universities have institutional reviewboards or research ethics committees responsible for reporting procedures and policiesregarding conflicts of interest. Problems arise as to who will monitor the conflicts of interestand what, if any, sanction doctors will receive for failing to disclose conflicts of interest. On anational level, oversight becomes even more problematic. Moreover, there is debate overwhether disclosure is sufficient: should researchers be allowed to conduct research forcompanies in which they have a financial interest?Pakistani pharmaceutical industry also growing at rapid paceover last many years andreached to Rs. 137.7 Billion in 2010 (IMS Q2 2010) in this growth major chunk came fromgeneric drugs manufacturer or generic drugs in Pakistan.ijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 6 1MARCH 2012VOL 3, NO 11GRAPH - 3Generic (Copy) Drugs (% Share of Total Market)Source: IMS – PKPI Q2 2010 (MAT)Above graph shows that market share of generic drugs in Pakistan in continuously increasesover the years reach to 53.1% market share and likely to cross 55% market by the end of thisyear. This can also validated by the number of generic drugsmaking company in top ten
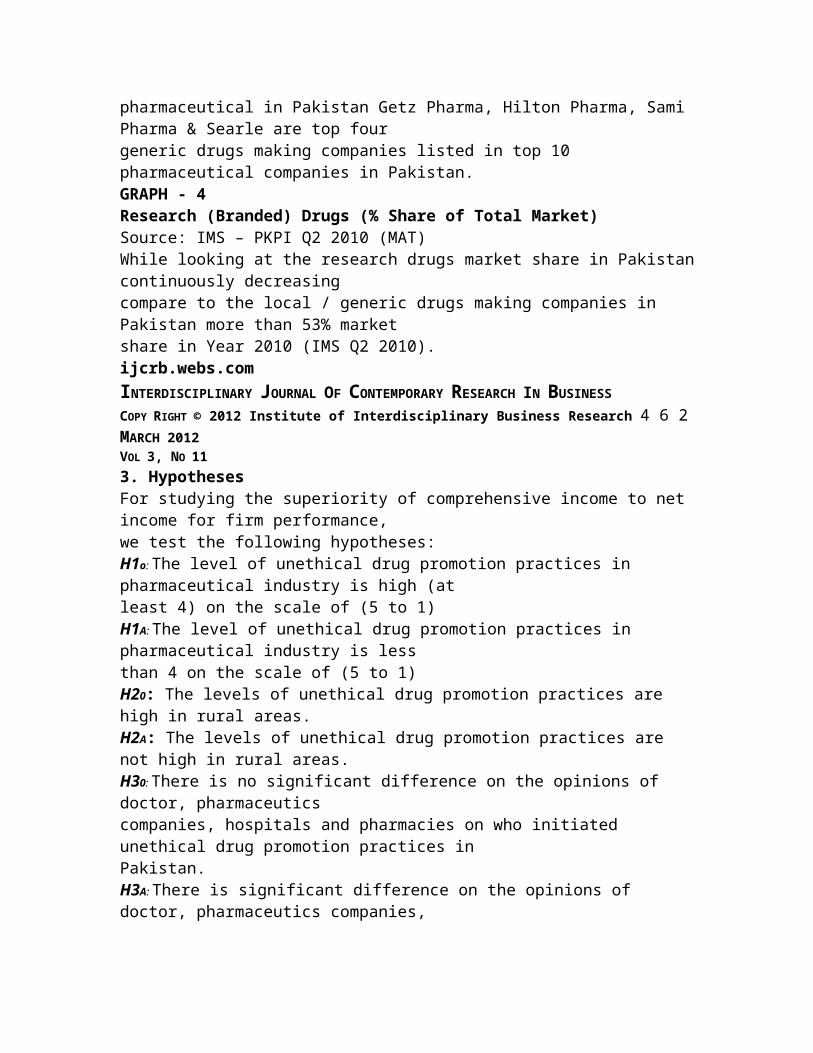
pharmaceutical in Pakistan Getz Pharma, Hilton Pharma, Sami Pharma & Searle are top fourgeneric drugs making companies listed in top 10 pharmaceutical companies in Pakistan.GRAPH - 4Research (Branded) Drugs (% Share of Total Market)Source: IMS – PKPI Q2 2010 (MAT)While looking at the research drugs market share in Pakistancontinuously decreasingcompare to the local / generic drugs making companies in Pakistan more than 53% marketshare in Year 2010 (IMS Q2 2010).ijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 6 2MARCH 2012VOL 3, NO 113. HypothesesFor studying the superiority of comprehensive income to net income for firm performance,we test the following hypotheses:H1o: The level of unethical drug promotion practices in pharmaceutical industry is high (atleast 4) on the scale of (5 to 1)H1A: The level of unethical drug promotion practices in pharmaceutical industry is lessthan 4 on the scale of (5 to 1)H20: The levels of unethical drug promotion practices are high in rural areas.H2A: The levels of unethical drug promotion practices are not high in rural areas.H30: There is no significant difference on the opinions of doctor, pharmaceuticscompanies, hospitals and pharmacies on who initiated unethical drug promotion practices inPakistan.H3A: There is significant difference on the opinions of doctor, pharmaceutics companies,
hospitals and pharmacies on who initiated unethical drug promotion practices in Pakistan.H40: The contribution of the pharmaceutical industry in continuation of unethical drugpromotion practices is higher than the doctors.H4A: The contribution of the pharmaceutical industry in continuation of unethical drugpromotion practices is higher than the doctors.4. Research MethodThe total population, and targeted population has been givenas under and on the basis oftargeted population we have selected our sample size which has also been elaborated asunder, moreover, following research methodology will be adopted in order to conduct ourresearch study.The total population of undertaken study consist of all Sales & Marketing Personnel of allPharmaceutical Companies which are operating in Pakistan including Multinational &National Companies, all the doctor community whether they are General practitioner in ruralor urban area or Medical Officers & Resident Medical Officers of Government & Privatehospitals or the Consultants of all specialties whether theyare working in Government orPrivate Hospitals, all the Retail Pharmacies' of the Country, all the whole sales pharmacies ofthe Country, all the Public & Private Hospitals of the Country, all the indoor & outdoorpatients & their attendants' during the data collection timeperiod and Government Offices &Officials which are directly or indirectly involved in orderto implement & ensure the lawenforcement which are related to the subject matter of undertaken study.Whereas the targeted population of undertaken study are Sales & Marketing Personnel of top
10 (according to IMS) Pharmaceutical Companies which are operating in Pakistan includingMultinational & National Companies. These top 10 players have more than 80% share oftotal pharmaceutical volume, which include GSK, Abbott, Sanofi-Avantis, Novartis, Pfizer,Merck-Serrano, Buyer-Schering, Getz, Hilton, and Bosch Pharmaceuticals, peripheral andurban areas of Karachi City, general practitioner in rural (peripheral) and urban areas,medical officers & Resident Medical Officers of Government &Private hospitals or theConsultants of all specialties whether they are working in Government or Private Hospitalshave been taken for this study.Probability sampling technique will be used because the research study based on quantitativeanalysis. For the sampling purpose the Cluster sampling technique will be used, anotherreason to use this sampling technique is, the overall population is very much scattered andspread in a larger geographical area of the city, moreover, the overall population isheterogeneous. Therefore, for sampling purpose different clusters will be collected fromdifferent areas of Karachi city. Researcher has used following six variables in order toijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 6 3MARCH 2012VOL 3, NO 11conduct the undertaken study and to draw statistical analysis & conclusions. The total sampleof 300 has been extracted from following six different variables.- Multinational / national pharmaceutical's personnel- General practitioners (both rural & urban)
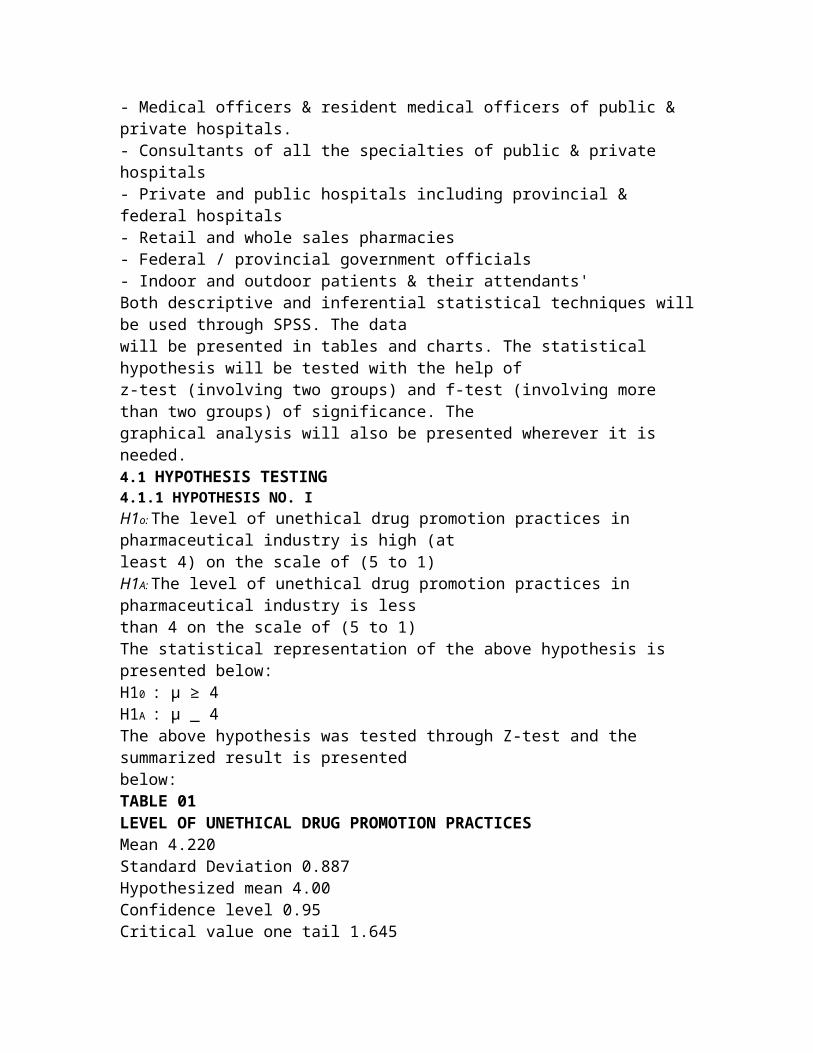
- Medical officers & resident medical officers of public & private hospitals.- Consultants of all the specialties of public & private hospitals- Private and public hospitals including provincial & federal hospitals- Retail and whole sales pharmacies- Federal / provincial government officials- Indoor and outdoor patients & their attendants'Both descriptive and inferential statistical techniques willbe used through SPSS. The datawill be presented in tables and charts. The statistical hypothesis will be tested with the help ofz-test (involving two groups) and f-test (involving more than two groups) of significance. Thegraphical analysis will also be presented wherever it is needed.4.1 HYPOTHESIS TESTING4.1.1 HYPOTHESIS NO. IH1o: The level of unethical drug promotion practices in pharmaceutical industry is high (atleast 4) on the scale of (5 to 1)H1A: The level of unethical drug promotion practices in pharmaceutical industry is lessthan 4 on the scale of (5 to 1)The statistical representation of the above hypothesis is presented below:H10 : μ ≥ 4H1A : μ _ 4The above hypothesis was tested through Z-test and the summarized result is presentedbelow:TABLE 01LEVEL OF UNETHICAL DRUG PROMOTION PRACTICESMean 4.220Standard Deviation 0.887Hypothesized mean 4.00Confidence level 0.95Critical value one tail 1.645
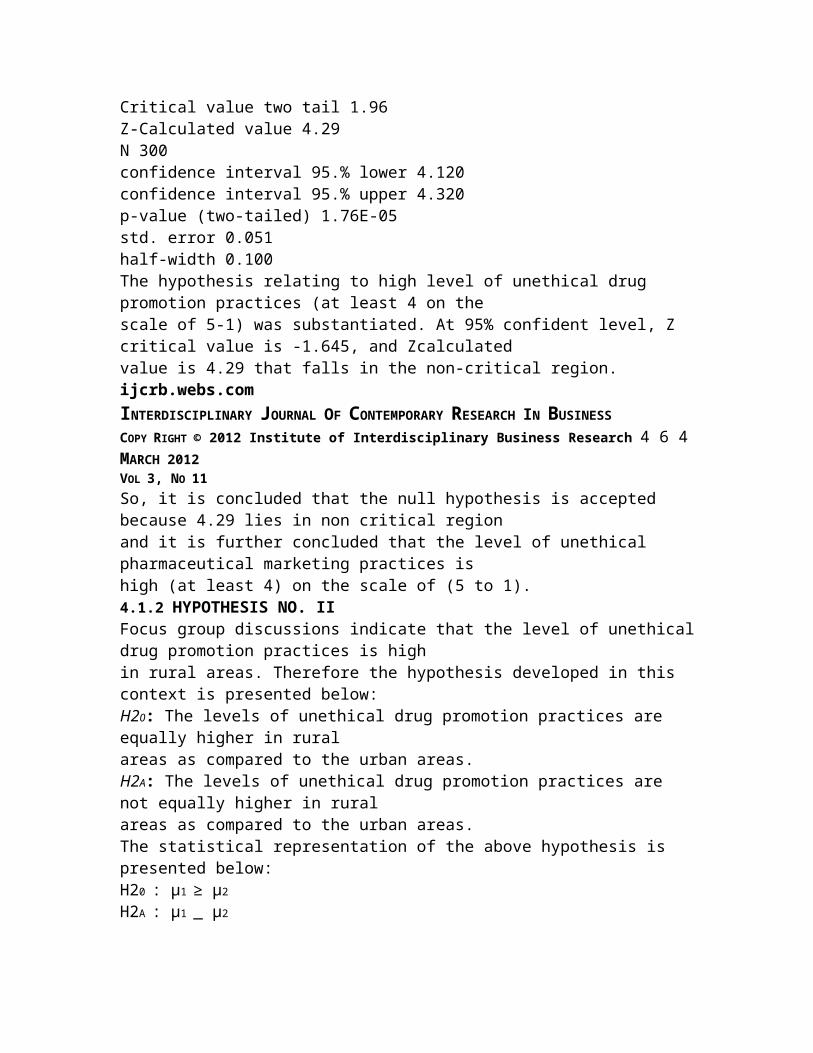
Critical value two tail 1.96Z-Calculated value 4.29N 300confidence interval 95.% lower 4.120confidence interval 95.% upper 4.320p-value (two-tailed) 1.76E-05std. error 0.051half-width 0.100The hypothesis relating to high level of unethical drug promotion practices (at least 4 on thescale of 5-1) was substantiated. At 95% confident level, Z critical value is -1.645, and Zcalculatedvalue is 4.29 that falls in the non-critical region.ijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 6 4MARCH 2012VOL 3, NO 11So, it is concluded that the null hypothesis is accepted because 4.29 lies in non critical regionand it is further concluded that the level of unethical pharmaceutical marketing practices ishigh (at least 4) on the scale of (5 to 1).4.1.2 HYPOTHESIS NO. IIFocus group discussions indicate that the level of unethicaldrug promotion practices is highin rural areas. Therefore the hypothesis developed in this context is presented below:H20: The levels of unethical drug promotion practices are equally higher in ruralareas as compared to the urban areas.H2A: The levels of unethical drug promotion practices are not equally higher in ruralareas as compared to the urban areas.The statistical representation of the above hypothesis is presented below:H20 : μ1 ≥ μ2H2A : μ1 _ μ2
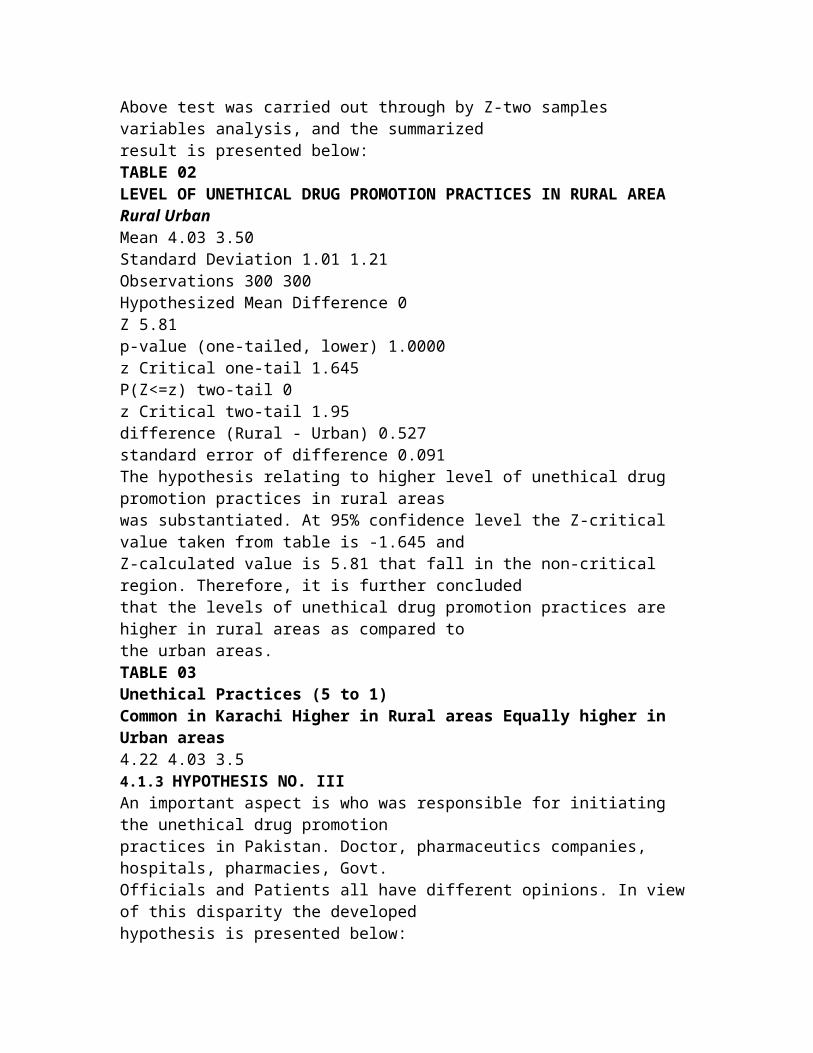
Above test was carried out through by Z-two samples variables analysis, and the summarizedresult is presented below:TABLE 02LEVEL OF UNETHICAL DRUG PROMOTION PRACTICES IN RURAL AREARural UrbanMean 4.03 3.50Standard Deviation 1.01 1.21Observations 300 300Hypothesized Mean Difference 0Z 5.81p-value (one-tailed, lower) 1.0000z Critical one-tail 1.645P(Z<=z) two-tail 0z Critical two-tail 1.95difference (Rural - Urban) 0.527standard error of difference 0.091The hypothesis relating to higher level of unethical drug promotion practices in rural areaswas substantiated. At 95% confidence level the Z-critical value taken from table is -1.645 andZ-calculated value is 5.81 that fall in the non-critical region. Therefore, it is further concludedthat the levels of unethical drug promotion practices are higher in rural areas as compared tothe urban areas.TABLE 03Unethical Practices (5 to 1)Common in Karachi Higher in Rural areas Equally higher in Urban areas4.22 4.03 3.54.1.3 HYPOTHESIS NO. IIIAn important aspect is who was responsible for initiating the unethical drug promotionpractices in Pakistan. Doctor, pharmaceutics companies, hospitals, pharmacies, Govt.Officials and Patients all have different opinions. In view of this disparity the developedhypothesis is presented below:
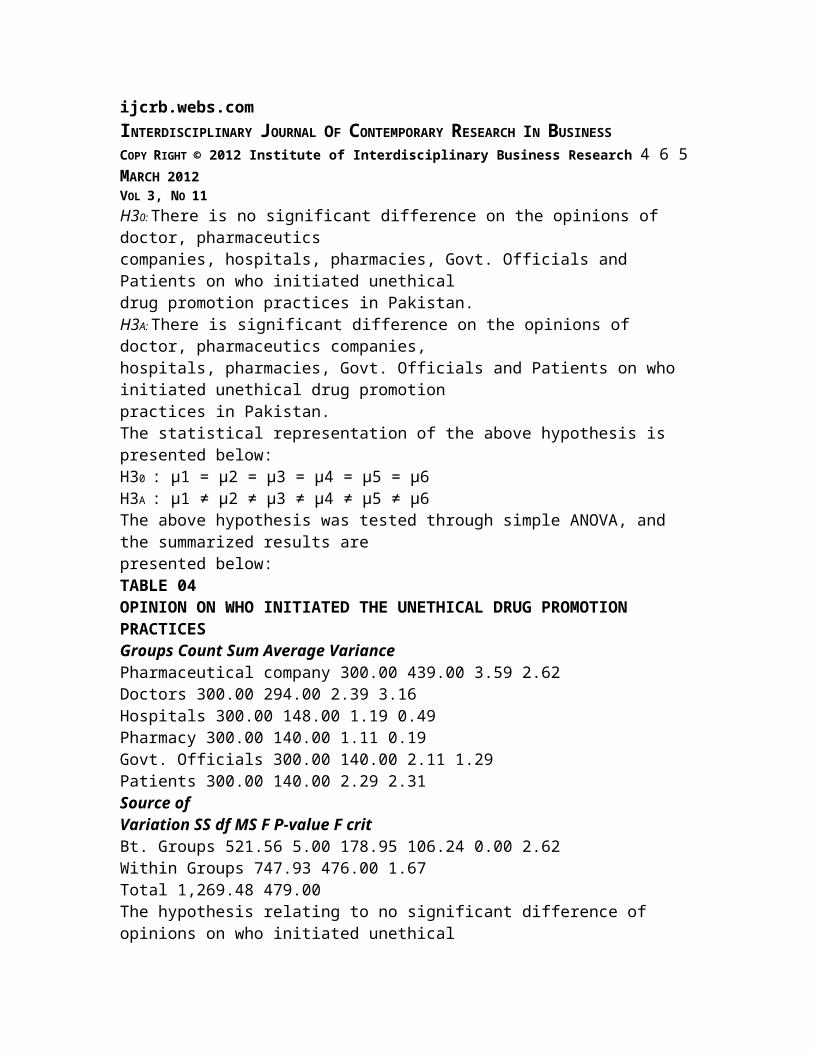
ijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 6 5MARCH 2012VOL 3, NO 11H30: There is no significant difference on the opinions of doctor, pharmaceuticscompanies, hospitals, pharmacies, Govt. Officials and Patients on who initiated unethicaldrug promotion practices in Pakistan.H3A: There is significant difference on the opinions of doctor, pharmaceutics companies,hospitals, pharmacies, Govt. Officials and Patients on who initiated unethical drug promotionpractices in Pakistan.The statistical representation of the above hypothesis is presented below:H30 : μ1 = μ2 = μ3 = μ4 = μ5 = μ6H3A : μ1 ≠ μ2 ≠ μ3 ≠ μ4 ≠ μ5 ≠ μ6The above hypothesis was tested through simple ANOVA, and the summarized results arepresented below:TABLE 04OPINION ON WHO INITIATED THE UNETHICAL DRUG PROMOTIONPRACTICESGroups Count Sum Average VariancePharmaceutical company 300.00 439.00 3.59 2.62Doctors 300.00 294.00 2.39 3.16Hospitals 300.00 148.00 1.19 0.49Pharmacy 300.00 140.00 1.11 0.19Govt. Officials 300.00 140.00 2.11 1.29Patients 300.00 140.00 2.29 2.31Source ofVariation SS df MS F P-value F critBt. Groups 521.56 5.00 178.95 106.24 0.00 2.62Within Groups 747.93 476.00 1.67Total 1,269.48 479.00The hypothesis relating to no significant difference of opinions on who initiated unethical
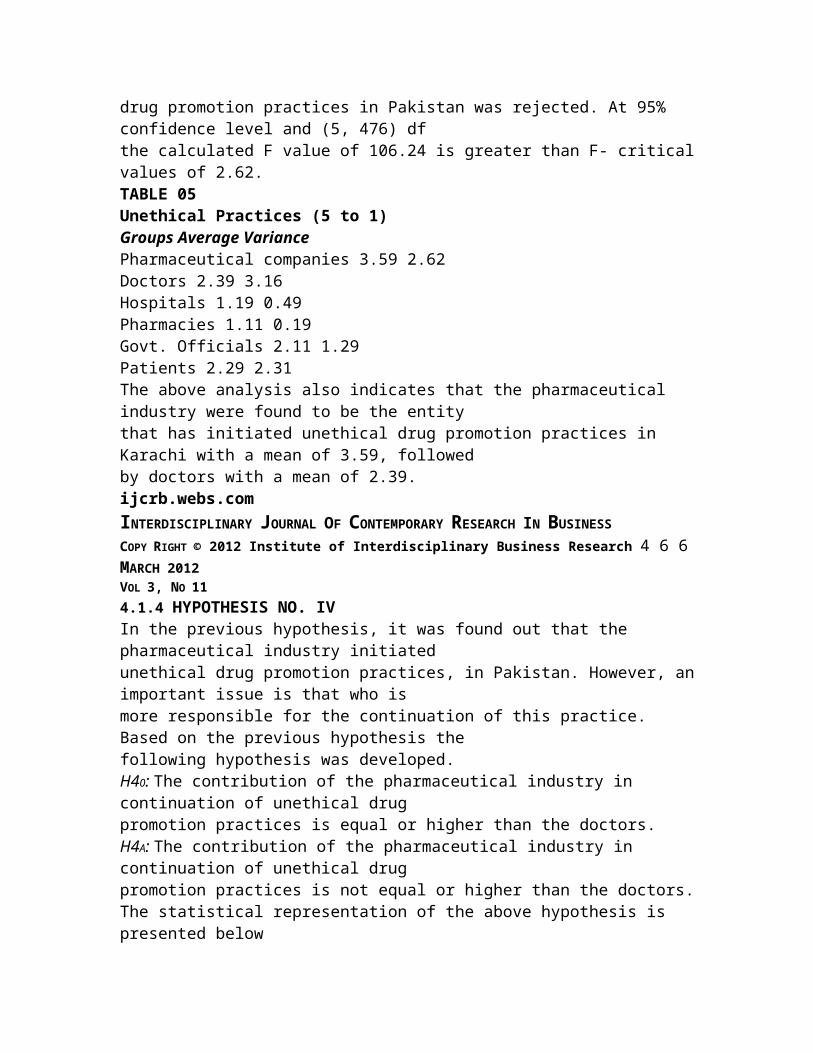
drug promotion practices in Pakistan was rejected. At 95% confidence level and (5, 476) dfthe calculated F value of 106.24 is greater than F- criticalvalues of 2.62.TABLE 05Unethical Practices (5 to 1)Groups Average VariancePharmaceutical companies 3.59 2.62Doctors 2.39 3.16Hospitals 1.19 0.49Pharmacies 1.11 0.19Govt. Officials 2.11 1.29Patients 2.29 2.31The above analysis also indicates that the pharmaceutical industry were found to be the entitythat has initiated unethical drug promotion practices in Karachi with a mean of 3.59, followedby doctors with a mean of 2.39.ijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 6 6MARCH 2012VOL 3, NO 114.1.4 HYPOTHESIS NO. IVIn the previous hypothesis, it was found out that the pharmaceutical industry initiatedunethical drug promotion practices, in Pakistan. However, animportant issue is that who ismore responsible for the continuation of this practice. Based on the previous hypothesis thefollowing hypothesis was developed.H40: The contribution of the pharmaceutical industry in continuation of unethical drugpromotion practices is equal or higher than the doctors.H4A: The contribution of the pharmaceutical industry in continuation of unethical drugpromotion practices is not equal or higher than the doctors.The statistical representation of the above hypothesis is presented below
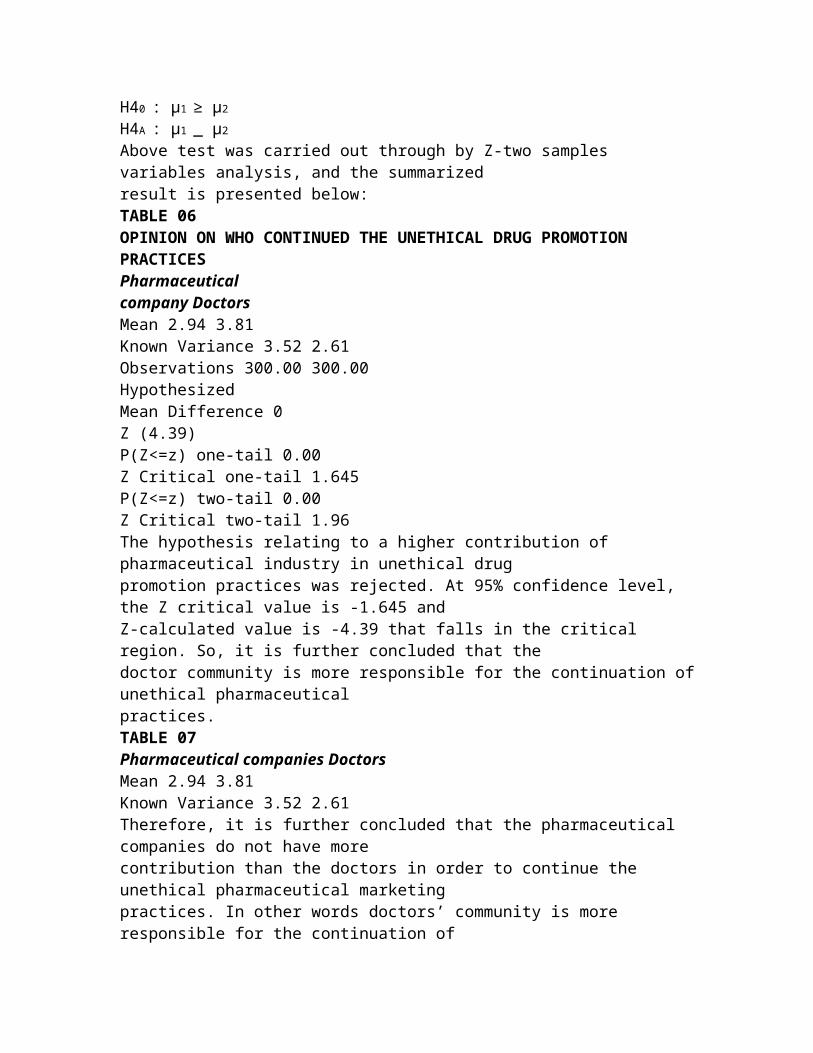
H40 : μ1 ≥ μ2H4A : μ1 _ μ2Above test was carried out through by Z-two samples variables analysis, and the summarizedresult is presented below:TABLE 06OPINION ON WHO CONTINUED THE UNETHICAL DRUG PROMOTIONPRACTICESPharmaceuticalcompany DoctorsMean 2.94 3.81Known Variance 3.52 2.61Observations 300.00 300.00HypothesizedMean Difference 0Z (4.39)P(Z<=z) one-tail 0.00Z Critical one-tail 1.645P(Z<=z) two-tail 0.00Z Critical two-tail 1.96The hypothesis relating to a higher contribution of pharmaceutical industry in unethical drugpromotion practices was rejected. At 95% confidence level, the Z critical value is -1.645 andZ-calculated value is -4.39 that falls in the critical region. So, it is further concluded that thedoctor community is more responsible for the continuation ofunethical pharmaceuticalpractices.TABLE 07Pharmaceutical companies DoctorsMean 2.94 3.81Known Variance 3.52 2.61Therefore, it is further concluded that the pharmaceutical companies do not have morecontribution than the doctors in order to continue the unethical pharmaceutical marketingpractices. In other words doctors’ community is more responsible for the continuation of
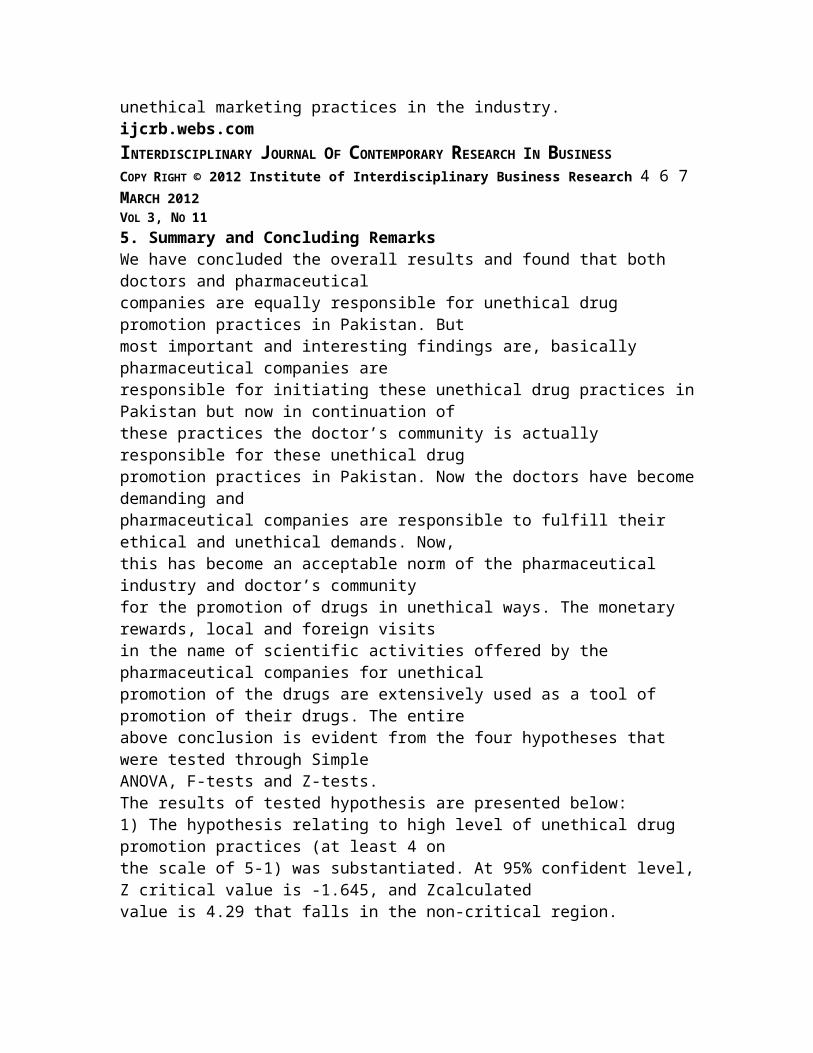
unethical marketing practices in the industry.ijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 6 7MARCH 2012VOL 3, NO 115. Summary and Concluding RemarksWe have concluded the overall results and found that both doctors and pharmaceuticalcompanies are equally responsible for unethical drug promotion practices in Pakistan. Butmost important and interesting findings are, basically pharmaceutical companies areresponsible for initiating these unethical drug practices inPakistan but now in continuation ofthese practices the doctor’s community is actually responsible for these unethical drugpromotion practices in Pakistan. Now the doctors have becomedemanding andpharmaceutical companies are responsible to fulfill their ethical and unethical demands. Now,this has become an acceptable norm of the pharmaceutical industry and doctor’s communityfor the promotion of drugs in unethical ways. The monetary rewards, local and foreign visitsin the name of scientific activities offered by the pharmaceutical companies for unethicalpromotion of the drugs are extensively used as a tool of promotion of their drugs. The entireabove conclusion is evident from the four hypotheses that were tested through SimpleANOVA, F-tests and Z-tests.The results of tested hypothesis are presented below:1) The hypothesis relating to high level of unethical drug promotion practices (at least 4 onthe scale of 5-1) was substantiated. At 95% confident level,Z critical value is -1.645, and Zcalculatedvalue is 4.29 that falls in the non-critical region.
So, it is concluded that the null hypothesis is accepted because 4.29 lies in non critical regionand it is further concluded that the level of unethical pharmaceutical marketing practices ishigh (at least 4) on the scale of (5 to 1).It may be pointed that the level of unethical drug promotionpractices as was ascertained by(Parmar and Jalees, 2004) in their research was 3.56. The reason could be that the study of(Parmar and Jalees) was case study of Hyderabad, where as this study is Karachi based, andthe sample drawn was a more representative sample.2) The hypothesis relating to higher level of unethical drugpromotion practices in ruralareas was substantiated. At 95% confidence level the Z-critical value taken from table is -1.645 and Z-calculated value is 5.81 that fall in the non-critical region. Therefore, it is furtherconcluded that the levels of unethical drug promotion practices are higher in rural areas ascompared to the urban areas.An important aspect is who was responsible for initiating the unethical drug promotionpractices in Pakistan. Doctor, pharmaceutics companies, hospitals and pharmacies all havedifferent opinions. In view of this disparity the developed hypothesis is presented below:3) The hypothesis relating to no significant difference of opinions on who initiatedunethical drug promotion practices in Pakistan was rejected.At 95% confidence level and (5,476) df the calculated F value of 106.24 is greater than F- critical values of 2.62.The above analysis also indicates that the pharmaceutical industry were found to be the entitythat has initiated unethical drug promotion practices in Pakistan with a mean of 3.59,followed by doctors with a mean of 2.39.ijcrb.webs.com
INTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 6 8MARCH 2012VOL 3, NO 11In the previous hypothesis, it was found out that the pharmaceutical industry initiatedunethical drug promotion practices, in Pakistan. However, animportant issue is that who ismore responsible for the continuation of this practice.4) The hypothesis relating to a higher contribution of pharmaceutical industry inunethical drug promotion practices was rejected. At 95% confidence level, the Z criticalvalue is -1.645 and Z-calculated value is -4.39 that falls in the critical region.Therefore, it is further concluded that the pharmaceutical companies do not have morecontribution than the doctors in order to continue the unethical pharmaceutical marketingpractices. In other words doctors’ community is more responsible for the continuationunethical marketing practices in the industry.The qualitative analyses of determinants such as (a) tools of unethical drug promotionpractices (b) drug promotion to the non-qualified doctors (c) Legislation for unethical drugpromotion (d) eradication of unethical drug promotion is given as below:a) As was discussed in the literature survey that the commonly used tools for unethical drugpractices were, monetary rewards, local visits, and foreign visits etc. The summarized resultsare presented below:It was discussed in earlier section that the doctors are theones that are responsible for thecontinuation of unethical drug promotion practices. The Qualitative analysis shows thatforeign visits with a mean of 4.59 are more in demand and local visits being the second. The
reasons for high preferences for local visits and foreign visits are that pharmaceutical industrycould justify these expenses by linking it with the conference.b) Opinions on drug promotion to non qualified doctors were obtained. Ethically, the firmsshould not promote their drugs through them. The respondents’ opinions are presented below:The Qualitative analysis shows that the majority of respondents’ of all the segments such asdoctors, Pharmaceutical companies, hospitals, pharmacies, govt. officials or Patients werestrongly against drug promotion to the non-qualified doctors. However, despite their opinionsit is a fact that the drugs are being promoted through non-qualified doctors.c) Respondents’ opinions were obtained on the prospects of strong legislation againstunethical drug promotion practices. The respondents’ opinions are presented below:Inference could be drawn from the Qualitative analysis that the majority of respondents arestrongly in the favor of making some strong legislation against the unethical drugpromotional practices in Pakistan. Although some legislationis already available but thisresearch showed there is no implementation of that legislation, therefore, majority ofrespondent demanded that there must be strong legislation tostop this unethical drugpromotion in Pakistan.d) Opinions on eradication of drug promotion in Pakistan were obtained from therespondents’. The respondents’ opinions are presented below:ijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 6 9MARCH 2012VOL 3, NO 11
The Qualitative analysis shows that the majority of the respondents’ i.e. doctors,pharmaceutical personnel, hospitals, pharmacies, govt. officials and Patients stronglydisagree about the opinion that the unethical drug promotionpractices cannot be stoppednow. Majority of respondents’ agreed upon that these unethical practices can still be stopped.5.1 RecommendationsThe focus groups discussions and survey findings suggest that strong legislation must bedeveloped, implemented and enforced by the government. However, the regulations andlegislation actually works when they are supported by the norms and values of the society.In this particular case, these unethical practices are considered as the norms of thepharmaceutical industry and the doctor’s community; therefore, it could only be addressed byeducating both the segments for realizing their social responsibilities with the focus on thepatients’ well being.Furthermore, there must be strong check and monitoring by the Ministry of Health and othermonitoring agencies both on pharmaceutical industry and the doctors.It is also strongly recommended that there should be strong legislation by the healthcareauthorities and government agencies to stop or at least minimize these unethicalpharmaceutical marketing practices both by the doctor community and the pharmaceuticalindustry.There must be strong enforcement of existing rules and regulations by the relevantgovernment departments and autonomous bodies who responsibleto implement and ensurethese rules and regulations both on pharmaceutical industry and the doctors’ community.
We also recommend to the doctors’ community that this is also their prime and ethicalresponsibility to avoid getting unethical benefits from pharmaceutical companies while theyare prescribing their products.The pharmaceutical industry should also restrict itself up to ethical marketing offers anddiscourage healthcare professionals if they would ask any thing which is unethical accordingto the ethical pharmaceutical practices guidelines.Since the under taken study was a case study of Karachi Cityonly, therefore, it could not beconcluded that the result of the study if which would be conducted on country-wide would bethe same as, therefore, further research can be conducted onPan-Pakistan basis for morerepresentative sample. Another dimension is to segregate thespecialties and then could beconducted the study in order to analyze whether the results of different specialties are same ordifferent. Since in this study only promotional or the marketing aspect of pharmaceuticalindustry is been covered, other areas of pharmaceutical industry like medical, production andprocurement could also be covered. In this study few variables have been incorporatedwhereas, in further research more variables can be incorporated in order to have more clearand accurate results.ijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 7 0MARCH 2012VOL 3, NO 11ReferencesA. Berenson & A. Pollack, Doctors Reap Millions for Anemia Drugs, N.Y. TIMES (May 9,2007);
A. Catlin et al., National Health Spending in 2005, 26 HEALTH AFFAIRS 142 (2007).Aaker, J. L., Williams, P. (1998). Empathy versus pride: Theinfluence of emotional appealsacross cultures. Journal of Consumer Research. 25(3), 241-261.Aday, L. A. (1996). Designing and conducting health surveys (2nd ed.).San Francisco:Jossey-Bass. American College of Physicians. (1990). Physicians and the pharmaceuticalindustry. Annals of Internal Medicine, 112, 392-394.Ahmed R.R & Jalees T, (2008), "Pharmaceutical Industry in Pakistan: UnethicalPharmaceutical Marketing Practices" (Eds) Market Forces, Karachi, Pakistan.American Medical Association. (1991). Council on Ethical andJudicial Affairs. Gifts tophysicians from the industry. JAMA, 265, 501.American Medical Association. (1995-2002). Council on Ethical and Judicial Affairs. Ethicalguidelines for gifts to physicians from the industry. Retrieved February 13, 2002 from:http://www.ama-assn.org/ama/pub/printcat/5689.htmlAshley Wazana, M.D., Physicians and the Pharmaceutical Industry: Is a GiftEver Just aGift?, 283 JAMA 373 (Jan. 19, 2000).Avorn, J., Chen, M., & Hartley, R. (1982). Scientific versuscommercial sources of influenceon prescribing behaviors of physicians. American Journal of Medicine, 73(1), 4-8.Bar-On, R., Parker, J. D. (Ed.). (2000). The handbook of emotional intelligence. SanFrancisco: Jossey-Bass.Bishnu P. Ravi S. (2005), “An educational initiative looks critically at the drug industry'spromotional tactics” (Eds), 10.1371/journal.pmed.0020256, August 30.Bodenheimer T. Uneasy alliance: clinical investigators and the pharmaceutical industry. NEngl J Med 2000; 342: 1539-1544.
Boseley, S. (2006) Drug firms a danger to health – report. The Guardian, 26th JuneBowman, M. A., & Pearle, D. L. (1988). Changes in drug prescribing patterns related tocommercial company funding of continuing medical education. Journal of ContinuingEducation Health Professions, 8(1), 13-20.Brennan, TA, Rothman, DJ, Blank, L, Blumenthal, Chimonas, S,Cohen, J.J., Goldman,J,Kassirer, JP, Kimball, H, Naughton, J, Smelser, N (2006). Health industry practices thatcreate conflicts of interest, Journal of the American Medical Association, 295 (4); 429-433.ijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 7 1MARCH 2012VOL 3, NO 11Campbell, E., Gruen, R., Mountford, J., Miller, L., Cleary, P., & Blumentahl, M., A NationalSurvey of Physician –Industry Relationships, N. ENGL. J. MED. 356:17 (Apr. 26, 2007).Chew, L. D., O’Young, T.S., Hazlet, T. K., Bradley, K. A., Maynard, C., & Lessler, D. S.(2000). A Physician Survey of the Effect of Drug Sample availability on Physicians'Behavior. Journal of General Internal Medicine, 15, 478-483.Coleman, J., Katz, E., Menzel, H. (1968). Doctors and new drugs. New York: The Free Pressof Glencoe.Coyle, S. L. (2002a). Ethics and Human Rights Committee, American College of Physicians-American Society of Internal Medicine. Position Paper: Physician-industry relations. Part 1:Individual physicians. Annals of Internal Medicine, 136 (5),396-402.Coyle, S. L. (2002b). Ethics and Human Rights Committee, American College of Physicians-
American Society of Internal Medicine. Position Paper: Physician-industry relations. Part 2:Organizational issues. Annals of Internal Medicine, 136 (5),403-406.Curcura, P. J. (1999). Stop saying “dinner meetings” it’s peer selling and it’s a science.Medical Marketing and Media, 34(12), 92-100.Daniella. A and Michael. A (2005), “Interactions between Pharmaceutical Representativesand Doctors in Training”, J Gen Intern Med. August; 20(8): 777–786.E. Hemminki, Review of Literature on the Factors Affecting Drug Prescribing, 9 SOC. SCI.& MED. 111 (1975).Fisher S, Bryant SG, Kent TA (1993), “Post marketing surveillance by patient selfmonitoring:trazodone versus fluoxetine”, J Clin Psychopharmacology; 13:235-242.Frederick Sierles et al., Medical Students’ Exposure to and Attitudes About Drug CompanyInteractions, 294 JAMA 1034 (Sept. 7, 2005).Gibbons, R. V., Landry, F. J., Blouch, D. L., Jones, D. L., Williams, F. K., Lucey, C. R. et al.(1998). A comparison of physicians' and patients' attitudes toward pharmaceutical industrygifts. J Gen Intern Medicine, 13, 151-154.Gonul, F. F., Carter, F., Petrova, E., & Srinivasan, K. (2001). Promotion of prescription drugsand its impact on physician’s choice behaviors. Journal of Marketing, 65, 79-90.Greene, J. (1999). Concern raised over increasing role of nonphysicians. American MedicalNews (December 6). Retrieved January 21, 2002 from: http://www.ama-assn.org .Greene, J. (2000). Drug reps targeting non physicians. American Medical News (March 27).Retrieved January 21, 2002 from: http://www.ama-assn.org .ijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESS
COPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 7 2MARCH 2012VOL 3, NO 11Harris, G. (2004). As doctors write prescriptions, drug company writes a check. New YorkTimes, June 27, 2004. Retrieved July 2, 2004 from:http://www.nytimes.com/2004/06/27/business/27DRUG.final.html?ex=1089337894&ei=1&en=c0877fb1c152b62Haxby, D. G., Rodriguez, G. S., Zenchnich, A. D., Schuff, R.A., Tanigawa, J. S. (1995).Manufacturers’ distribution of drug samples to a family medicine clinic. American Journal ofHealth Systems Pharmacology, 52, 496-499.Healthy Skepticism (2002). About Healthy Skepticism Inc. Retrieved June 21, 2002 from:http://www.healthyskepticism.org/index.htm .Hodges, B. (1995). Interactions with the pharmaceutical industry: Experiences and attitudesof psychiatry interns, residents and clerks. Canadian Medical Association Journal, 153, 553-559.Holmer, A. F. (1999). Direct-to-consumer prescription drug advertising builds bridgesbetween patients and physicians. JAMA, 281(3), 380-382.Holmes, D.R., Firth, B.G., James, A., Winslow, R., Hodgson, P.K., Gamble G.,IMS Health. (2002). Free pharmaceutical sample distribution.Retrieved June 24, 2002 from:http://www.ims-global.com/cgi .Ingelfinger, F. J. (1972). Advertising: informational but not educational. New EnglandJournal of Medicine, 286, 1318-1319.Kessenich, C. R., Westbrook, M. H. (1999). Pharmaceutical companies and the prescriptivepractices of nurse practitioners. Journal of the American Academy of Nurse Practitioners, 11(12), 533-538.
Lane, R. D. (2000). Levels of emotional awareness. In R. Bar-On & J. D. A. Parker.(Ed.),The handbook of emotional intelligence (pp. 171-191). San Francisco: Jossey-Bass.Lexchin J. (1992), “Pharmaceutical promotion in the third world”, Journal of Drug Issues;22(2):417-422.Lexchin J. (1995), “Deception by design: pharmaceutical promotion in the third world”,Consumers International, Malaysia.Lidstone, J. MacLennan, J. Marketing Planning for the Pharmaceutical Industry, 2nd ed.Gower PublishingLurie, N., Rich, E. C., & Simpson, D. E. (1990). Pharmaceutical representatives in academicmedical centers: Interaction with faculty and housestaff. Journal of General InternalMedicine, 5, 240-243.Manning, R. & Keith, A. (2001). The economics of direct-to-consumer advertising ofprescription drugs. In Manning, R. L. & Masia, N. A. (Eds.) Economic Realities in Healthijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 7 3MARCH 2012VOL 3, NO 11Care Policy, 2 (1), 10-15. Retrieved May 13, 2002 from:http://www.Pfizer.com/pfizerinc/policy/Erhealthcare.pdf .Manning, R. L. & Masia, N. A. (Eds.) (2001). Economic Realities in Health Care Policy, 2(1), 10-15. Retrieved May 13, 2002 from:http://www.Pfizer.com/pfizerinc/policy/Erhealthcare.pdf .Mathieu MP, editor. Parexel’s pharmaceutical R & D statistical sourcebook 1998. Waltham,Massachusetts: Parexel International Corporation, 1999.Mintzes, B. (1998). Blurring the boundaries: new trends in drug promotion. Amsterdam:HAI-Europe. Retrieved February 1, 2003 from:
http://www.haiweb.org/pubs/blurring/blurring.intro.html .Mintzes, B., Barer, M. L., Kravitz, R. L., Kazanjian, A., Bassett, K., Lexchin, J. et al. (2002).Influence of direct to consumer pharmaceutical advertising and patients’ requests onprescribing decisions: two sites cross sectional survey. British Medical Journal, 324, 278-279.Mixed Reaction to Consumer Advertising. (2003, March). Clinician News, 7(2), 13.Murray, D. (2002, October 11). Gifts what’s all the fuss about? Medical Economics, 79 (9),119-120.National Institute for Health Care Management. (2001, November). Advertised prescriptiondrugs are the hottest sellers. Washington, DC: Mahoney, A., Findlay, S.Retrieved February15, 2003 from: http://nihcm.org/DTC2001PR.html .National Institute for Health Care Management. (2002, May). Prescription drug expendituresin 2001: Another year of escalating costs. Washington, DC: Research and EducationalFoundation. Available from: http://www.nihcm.org/spending2001.pdf .No Free Lunch (2002a). About Us. Retrieved September 15, 2002 from:http://www.nofreelunch.org/aboutus.htm .Parmar & Jalees (2004), “Pharmaceutical Industry in Hyderabad, Unethical Practices in DrugPromotion”, Independent Study for MS, Shaheed Zulfiqar Ali Bhutto Institute of Science &Technology, Karachi, May.Paul Komesaroff and Ian Kerridge, “Ethical issues concerningthe relationships betweenmedical practitioners and the pharmaceutical industry”, MJA 2002; Vol. 176: P. 118-121Phatak A (1998), “The pharmaceutical industry and the medical profession”, Indian Journalof Medical Ethics, Oct-Dec, 6 (4).
PhRMA (2002b). PhRMA Code on Interactions with Healthcare Professionals. Washington,D.C.: Authors.ijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 7 4MARCH 2012VOL 3, NO 11PhRMA. (2002a). Media Room Press Release, April 19, 2002. PhRMA adopts newmarketing code. Retrieved October 16, 2002 from:http://www.phrma.org/mediaroom/press/releases/19.04.2002.390.cfm .Poor judgment in spite of high intellect: Neurological evidence for emotional intelligence. InBar-On, R., Parker, J. D. (Ed.). (2000). The handbook of emotional intelligence. SanFrancisco: Jossey-Bass.Popp, R.L., Harrington. R.A. (2004). Conflict of interest, American Heart Journal, 147(2);228-237.Sandberg, W. S., Carlos, R., Sandberg, E. H., Roizen, M. F. (1997). The effect of educationalgifts from pharmaceutical firms on medical students’ recall of company names and products.Academic Medicine, 72, 916-918.Sharpe, V.A. (2002). Science, bioethics, and the public trust, Hastings Center Report, 32(3);23-26.Sibbald H. (2004) Legal Action against GSK over SSRI data CMAJ. July 6; 171(1): 23.doi:10.1503/cmaj.1040982Socolar, D., Sager, A. (2001, October). Pharmaceutical marketing and research spending: Theevidence does not support PhRMA’s claims. Paper presented atAmerican Public HealthAssociation Annual Meeting (session 2018.0), Atlanta, GA.Steinman, M. A., Shlipak, M. G., & McPhee, S. J. (2001). Of principles and pens: Attitudes
and practices of medical house staff toward pharmaceutical industry promotions. TheAmerican Journal of Medicine, 110, 551-557.Stolberg, S. G., & Gerth, J. (2000, November 16). High tech stealth being used to swaydoctor prescriptions. New York Times. Fromhttp://nytimes.com/2000/11/16/science/16PRES.html .T. Brennan et al., Health Industry Practices That Create Conflicts of Interest, 295 JAMA 429(Jan. 25, 2006).Tomlinson H (2004) AstraZeneca sued for ulcer drug profits. The Guardian, 24 NovemberTutor2u. (2004). Buyer Behavior - Stimulus-Response Model. Retived June 25, 2004 from:http://www.tutor2u.net/business/marketing/buying_stimulus_model.asp.Wang, T. J., Ausiello, J. C., & Stafford, R. S. (1999). Trends in antihypertensive drugadvertising, 1985-1996. Circulation, 99(15), 2055-2057.Waud, D. R. (1992). Pharmaceutical promotions-a free lunch? New England Journal ofMedicine, 327, 351-353.Wazana, A. (2000). Physicians and the pharmaceutical industry: is a gift ever just a gift?JAMA, 283(3), 373-80.ijcrb.webs.comINTERDISCIPLINARY JOURNAL OF CONTEMPORARY RESEARCH IN BUSINESSCOPY RIGHT © 2012 Institute of Interdisciplinary Business Research 4 7 5MARCH 2012VOL 3, NO 11Westfall, J. M., McCabe, H., & Nicholas, R. A. (1997). Personal use of drug samples byphysicians and office staff. JAMA, 278:141-143.Westfall, J. M., McCabe, H., & Nicholas, R. A. (1998). Replyto Drug samples: Benefit orbait? JAMA, 279(21), 169-1699.Willimack, D. K., Schuman, H., Pennell, B. E., & Lepkowski, J. M. (1995). Effects of prepaidnon-monetary incentive on response rates and response quality in a face-to-face survey.
Public Opinion Quarterly, 59, 78-92.Wolf, B. (1998). Drug samples: Benefit or bait? JAMA, 279(21), 1698-1699.Wolfe, S. M. (2002). Direct-to-consumer advertising – Education or emotion promotion?New England Journal of Medicine, 346(7), 524-526.Zaidi SH, Niaz U, Jafary MH & Jawaid SA, (1995), "Medical Ethics in the ContemporaryEra" (Eds) Pakistan Medical Journalists Association, Karachi, Pakistan.Ziegler, M. G., Lew, P., & Singer, B. C. (1995). The accuracy of drug information frompharmaceutical sales representatives. JAMA, 27, 1296-1298.
The International Code of Marketing ofBreastmilk Substitutes: A Model forAssuring Children’s Nutrition Rights
Under the Law
Leah Margulies*July 21, 1998
This article argues that the International Code of Marketing of Breastmilk Substitutes, adopted by the World Health Assembly in 1981, is part of the body of human rights instruments that have been developed under the auspices of the United Nationssince the Universal Declaration of Human Rights was proclaimed in 1948. The human rights that the Code attempts to protect arethe rights to health and life, the rights to food and nutrition, and the right of women to full and accurate information on which to base decisions affecting their children’s health. Because national laws based on the Code are being adopted by a growing number of countries, the Codeprovides a useful model for transforming "soft"
international law, which enumerates and defines rights, into"hard" national law that protects and enforces rights.
The adoption of a Code outlining minimum standards for the marketing of lucrative products manufactured and distributedby a small number of powerful transnational companies was, at its heart, a political process. Similarly, adopting national laws which can enforce the rights that the Code protects, requires a confluence of political forces committed policy makers, informed and engaged health professionals, and citizen advocates active in non-governmental organizations.
Protecting human rights through international negotiation and cooperation is a drama that is continuously unfolding. This story is an unusually clear example of how international action can be taken to restrict marketing and promotion practices having specific harmful effects.
BACKGROUND: BREASTFEEDING IS BEST
Breastfeeding is the unequaled way of providing the ideal food for infants. Breastmilk is an infant’s first "immunization". The dangers associated with not breastfeeding -- that is bottle feeding with a breastmilk substitute -- are well known. Since breastmilk is a live substance, containing immunological and anti-infective properties, bottle-fed babies have more severe and greater numbers of infections, diarrhea and diseases which can lead to malnutrition and even death. As pointed out in Lancet:
In countries with a moderate or high infant mortality rate, artificially fed infants are at least 14 times more likely to die from diarrhea than are breastfed children, and 4 times more likely to die from pneumonia. Evenin countries where infant mortality is low, artificially fed infants require hospital
treatment up to 5 times more often than thosewho are fully or partly breastfed.
The United Nations Children’s Fund (UNICEF) and the World Health Organization (WHO) estimate that more than 1 million infant lives could be saved each year through effective breastfeeding.
By the late 1970’s it became clear to UNICEF, WHO, and a small group of dedicated health professionals who were leading the way, that breastfeeding was declining precipitously on a global scale, and that the aggressive marketing and promotion of breastmilk substitutes was seriously exacerbating the trend. Promotion of breastmilk substitutes was inducing mothers, medical personnel and health institutions to abandon breastfeeding. Breastfeeding was "old fashioned", while substitutes were modern and "Western". Meanwhile, bottle feeding, particularly for thosein poverty, posed predictable risks. Infants were frequentlyfed diluted or contaminated food without any of the anti-infective benefits of breastmilk. This was and remains a public health disaster, having especially negative economic results for poor countries. While scarce capital pays for unnecessary imported commercial baby food products, high levels of infant mortality and morbidity result in higher health care costs.
In 1981, after two years of intense and often fractious negotiations, the World Health Assembly (WHA), the governingbody of the World Health Organization, adopted the International Code of Marketing of Breastmilk Substitutes. The Code protects breastfeeding by restricting certain marketing practices for breastmilk substitutes. Every section of the Code was a reaction to marketing and promotion practices which exploit the uncertainties of new mothers. The Code’s position is that commercial products should be available when needed, but should not be promoted.
The Code, like the United Nation’s Universal Declaration on Human Rights, is not a treaty, but an intergovernmental resolution.Thus, while not legally binding, it establishes
internationally recognized minimum standards that Member States are urged to incorporate into national law. Today, more than fifteen years after it was adopted, more than halfof the world’s population live in countries where the Code has been adopted, fully or partially, as national law. To achieve these results has been a struggle of enormous proportions.
HIGHLIGHTS OF THE INTERNATIONAL CODE
The Code consists of a preamble and 11 articles, most with several subparagraphs detailing specific requirements. Its features include the following:
o The Code applies to a relatively broad scope of products all breastmilk substitute products and other products which are used as a partial or total replacement of breastmilk, bottles and teats.
o All advertising and promotion to the general public is banned. This includes forbidding the distribution of free samples, gifts and other promotional materials, and eliminating direct or indirect contact between marketing personnel and pregnant women and mothers.
o Promotion is banned in health care facilities. This includes banning displays of products, placards and the use of "mothercraft nurses" to promote products. "Mothercraft nurses" are nurses or sales people dressed as nurses who are hired topromote products.
o Informational and educational materials about breastmilk substitutes are permitted. However, thematerials must be scientific and factual, and mustinclude information on all of ten points listed inthe Code, including, for example, the superiority of breastfeeding, the difficulty of reversing the decision not to breastfeed, the financial implications of buying commercial substitutes, and
the health hazards of improper use. No pictures ortext may idealize the use of breast-milk substitutes, or imply equivalency with breastmilk.
o To discourage the routine use of formula in hospitals, the Code restricts "donations" (free supplies) and low-cost supplies of breastmilk substitutes only to charity cases where a breastmilk substitute is deemed necessary.
o The Code designates a specific list of label requirements. Labels must, among other things, include the message that the product only be used on the advice of a health worker who can instruct on the proper method of use. Also, labels may not show pictures of babies or idealize, through either words or images, the use of infant formula.
o The Code assigns implementation and monitoring responsibilities among the various parties: governments, manufacturers and distributors, non-governmental organizations and professional groups. Governments are urged to "adopt national legislation, regulation or other suitable measure"to implement the Code. Manufacturers and distributors, "independently of any other measures" are instructed (in Article 11.3) "to ensure that their conduct at every level" conformsto the Code. Non-governmental organizations, professional groups, institutions and individuals are to draw the attention of manufacturers and governments to activities which are incompatible with the Code.
PROBLEMATIC MARKETING AND PROMOTION PRACTICES
Before the adoption of the Code, egregious marketing and promotion practices were rampant. Companies sponsored "pretty baby" shows and hired "mothercraft nurses" to visit homes and maternity wards. Radio jingles and print ads led to widespread consumer recognition of the products. The medical profession was targeted as a promotional ally free

samples at the health clinic and supplies from the maternityward meant, to mothers, that the product was medically endorsed. Doctors and health facilities received various material benefits, everything from pens and key chains to cash payments and trips abroad, for their implied or explicit endorsement.
While some of these practices continue today, promotion has generally taken more subtle forms, with companies frequently"misinterpreting" the Code to justify their actions. For example, the companies will not concede that the Code is intended to be applied universally, and not just to developing countries. Under this cover, hospitals in industrialized countries receive large cash grants (sometimes in the millions of dollars) in exchange for usingand distributing particular brands of infant formula. Some companies, in direct violation of the Code, have establishedtoll-free "hot lines" to give mothers "infant feeding advice" from company personnel.
Some companies argue that the Code only applies to "infant formula", one type of breastmilk substitute, to justify their continued promotion of other types, such as "follow-upformulas" and other complementary foods which are used to replace breastmilk. Some manufacturers have developed generic beautiful baby posters with the company name and logo, as a way to get around the provision banning posters promoting products. Almost all companies ignore most of the requirements for informational and educational materials. And there have been numerous debates over many years about how to interpret the ban on free and low-cost supplies, leading the World Health Assembly to declare unambiguously that governments should "ensure that there are no free or subsidized supplies of breastmilk substitutes or other products covered by the [Code] in any part of the health care system."
These problems can be effectively dealt with at the nationallevel by drafting comprehensive and specific national rules.Indeed, some countries have established committees
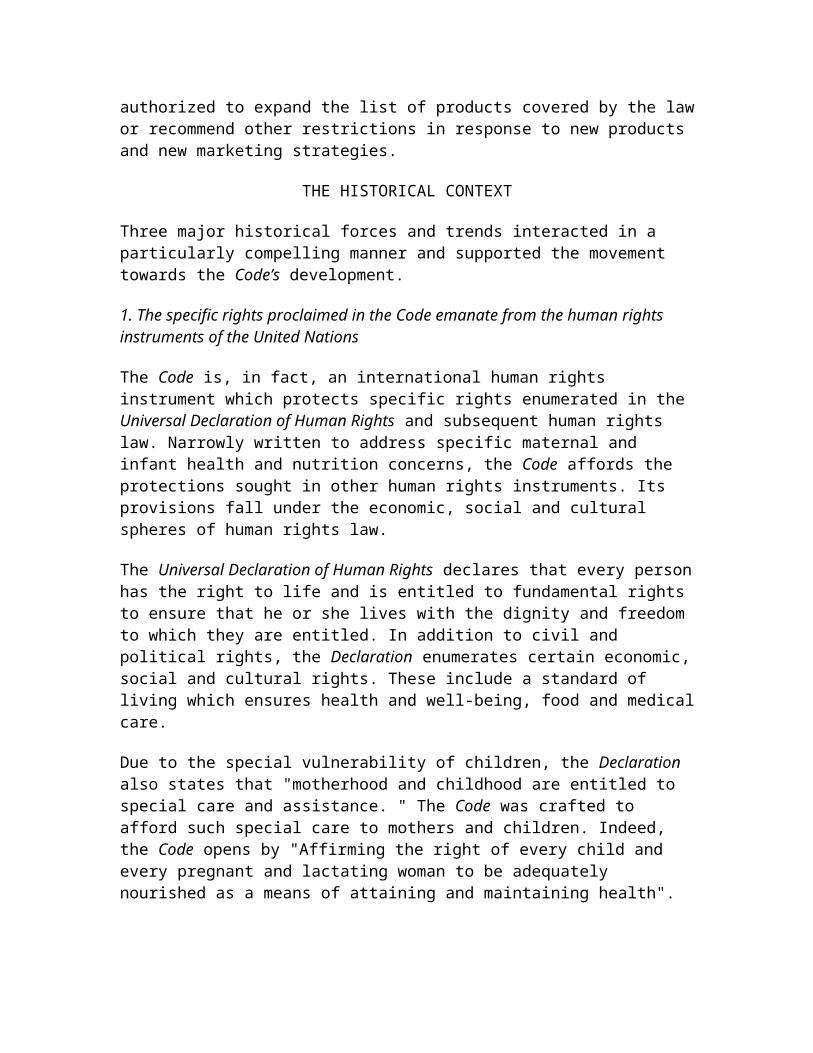
authorized to expand the list of products covered by the lawor recommend other restrictions in response to new products and new marketing strategies.
THE HISTORICAL CONTEXT
Three major historical forces and trends interacted in a particularly compelling manner and supported the movement towards the Code’s development.
1. The specific rights proclaimed in the Code emanate from the human rights instruments of the United Nations
The Code is, in fact, an international human rights instrument which protects specific rights enumerated in the Universal Declaration of Human Rights and subsequent human rights law. Narrowly written to address specific maternal and infant health and nutrition concerns, the Code affords the protections sought in other human rights instruments. Its provisions fall under the economic, social and cultural spheres of human rights law.
The Universal Declaration of Human Rights declares that every personhas the right to life and is entitled to fundamental rights to ensure that he or she lives with the dignity and freedom to which they are entitled. In addition to civil and political rights, the Declaration enumerates certain economic,social and cultural rights. These include a standard of living which ensures health and well-being, food and medicalcare.
Due to the special vulnerability of children, the Declaration also states that "motherhood and childhood are entitled to special care and assistance. " The Code was crafted to afford such special care to mothers and children. Indeed, the Code opens by "Affirming the right of every child and every pregnant and lactating woman to be adequately nourished as a means of attaining and maintaining health".

The late 1970’s and early 1980’s were a very fruitful time for the development of human rights law within the intergovernmental organizations. Nations emerging out of colonial status became members in their own right of the General Assembly and the other decision making bodies of theUnited Nations organizations. Establishing international human rights standards through intergovernmental negotiated legal instruments was an important step in giving legal standing to the rights proclaimed in the Universal Declaration of Human Rights for all the Member States of the United Nations,and especially for the new nations of the South.
Although the Universal Declaration of Human Rights was adopted as a non-binding resolution by the General Assembly, its definitions and descriptions of the rights to which all persons are entitled have become accepted as authoritative. In addition, in 1976 the two treaties designed to guarantee the rights enumerated in the Declaration, the International Covenant on Civil and Political Rights, and the International Covenant on Economic, Social and Cultural Rights entered into force.
The International Covenant on Economic, Social and Cultural Rights recognizes the right to enjoy "the highest attainable standard of physical and mental health", including the reduction of infant mortality and the healthy development ofthe child. This is elaborated upon in the Preamble of the Code: "inappropriate feeding practices lead to infant malnutrition, morbidity and mortality in all countries, and improper practices in the marketing of breastmilk substitutes and related products can contribute to these major public health problems."
Just prior to the decision by the World Health Assembly to develop the Code, the General Assembly adopted the Convention on the Elimination of All Forms of Discrimination against Women. Article 10of the Convention protects access to information to ensure the health and well-being of families; Article 11 confers the right to health "including the safeguarding of the function of reproduction" and Article 12 assures "adequate nutrition during pregnancy and lactation, " thus recognizing
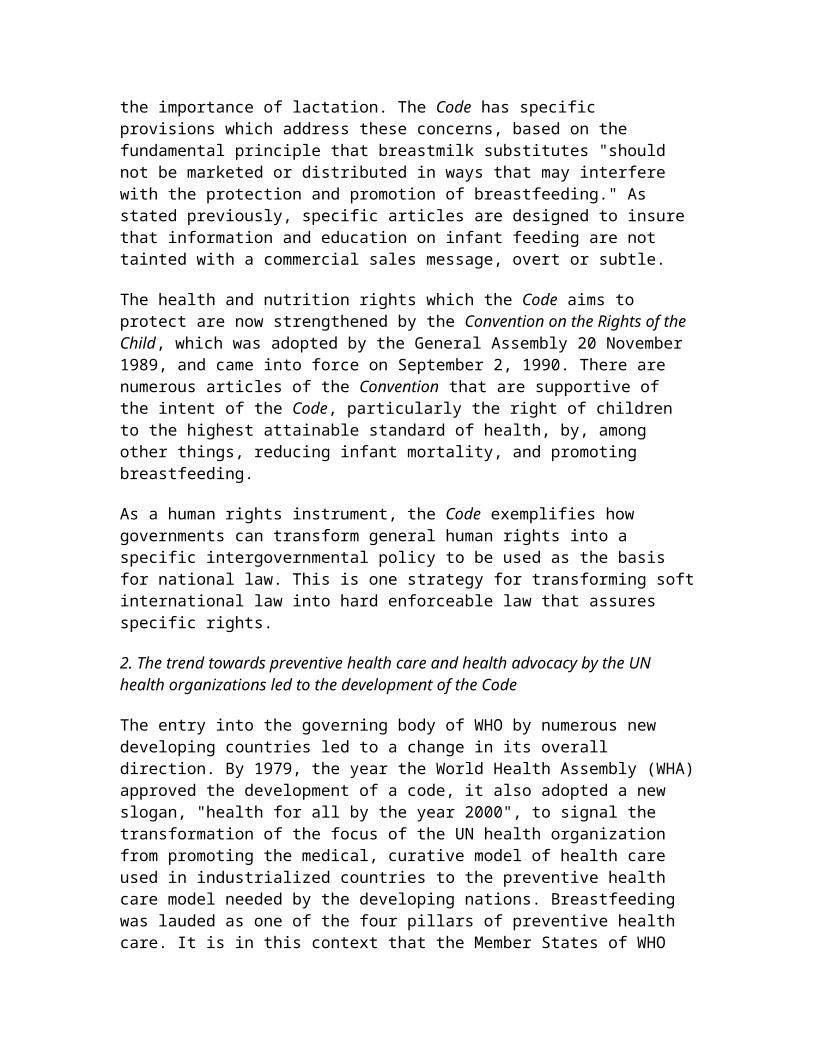
the importance of lactation. The Code has specific provisions which address these concerns, based on the fundamental principle that breastmilk substitutes "should not be marketed or distributed in ways that may interfere with the protection and promotion of breastfeeding." As stated previously, specific articles are designed to insure that information and education on infant feeding are not tainted with a commercial sales message, overt or subtle.
The health and nutrition rights which the Code aims to protect are now strengthened by the Convention on the Rights of the Child, which was adopted by the General Assembly 20 November 1989, and came into force on September 2, 1990. There are numerous articles of the Convention that are supportive of the intent of the Code, particularly the right of children to the highest attainable standard of health, by, among other things, reducing infant mortality, and promoting breastfeeding.
As a human rights instrument, the Code exemplifies how governments can transform general human rights into a specific intergovernmental policy to be used as the basis for national law. This is one strategy for transforming softinternational law into hard enforceable law that assures specific rights.
2. The trend towards preventive health care and health advocacy by the UN health organizations led to the development of the Code
The entry into the governing body of WHO by numerous new developing countries led to a change in its overall direction. By 1979, the year the World Health Assembly (WHA)approved the development of a code, it also adopted a new slogan, "health for all by the year 2000", to signal the transformation of the focus of the UN health organization from promoting the medical, curative model of health care used in industrialized countries to the preventive health care model needed by the developing nations. Breastfeeding was lauded as one of the four pillars of preventive health care. It is in this context that the Member States of WHO
and UNICEF began formally criticizing the inappropriate promotion practices for breastmilk substitutes which competed with breastfeeding.
In 1970, the Pan American Health Organization (PAHO), a regional arm of WHO, anticipated the Code in adopting guidelines to prevent advertising of commercial milk, accessto health care facilities by "commercial milk" nurses, and acceptance of "free" milk samples.
In 1974, the Twenty-Seventh World Health Assembly adopted a resolution criticizing sales promotion practices which persuade mothers that breastfeeding is inferior to manufactured breastmilk substitutes, and urging countries toreview promotional activities on baby foods and introduce appropriate remedial measures, including advertising codes and legislation where necessary. Then, in 1978 (one year before the WHO/UNICEF sponsored meeting which recommended the development of a code of marketing) the Assembly adopteda resolution recommending that member states, to prevent malnutrition in pregnant and lactating women, infants and young children, support and promote breastfeeding and regulate inappropriate sales promotion of infant foods that can be used to replace breastmilk.
Similarly, the 1978 UNICEF report "Trends in Breastfeeding and Their Impact on Child Health" stated:
Breast milk meets all the nutritional needs of the young infant. No other known food preparation does so as effectively…Through advertising of breastmilk substitutes, mothers are told and consistently reminded ofproducts that are held up to be equal if not better than breast milk.
The fact that these policy commitments had been accepted by the Member States of WHO and UNICEF for more than a decade was an important element in overcoming the political resistance to the Code. This lay the groundwork for the concluding words of the Code’s Preamble, that "the marketing

of breastmilk substitutes requires special treatment, which makes usual marketing practices unsuitable for these products."
3. The political forces which affected the Code’s development
Before the debt crisis and structural adjustment demands effectively stopped it, the new nations of the South attempted to rectify the imbalances in the legacy of Colonialism by joining together to call for a New International Economic Order which was to have assured a greater degree of national control over the direction of andthe fruits of development. This struggle for control over development was being acted out in various UN fora. Under the auspices of the United Nations Centre on Transnational Corporations (created, in part, to assist developing countries in negotiating fair investment contracts with transnational companies), the General Assembly was considering the terms of a code of conduct to govern relations between governments and transnational companies, many of which had economies far larger than that of the states themselves. At the United Nations Conference on Tradeand Development (UNCTAD), a highly politicized debate was underway on how to transfer technology from industrialized to developing nations.
In the World Health Organization, industrialized and developing countries were battling over whether and how to rein in the vast numbers of pharmaceutical products that were now entering the markets of developing countries without any controls, endangering health and overwhelming fledgling domestic industries. For the most part, industrialized countries, home to the corporate headquartersof the largest transnational companies, found themselves representing the companies’ needs and demands. The call for a New International Economic Order (NIEO), while receiving ahostile response from the governments of most industrializednations, was gaining support among a wide range of non-governmental organizations. These groups, throughout the industrialized countries, generally supported the concept of
the NIEO, and considered poverty and lack of development as the main barriers to creating strong countries capable of extending democratic principles. Newly emerging nations needed to control the pace and direction of development to lift their citizens from poverty and enjoy the rights envisioned in the UN Charter and Universal Declaration of Human Rights.
By the mid-1970’s, non-governmental advocacy groups in the United States and Europe were campaigning to stop the promotion of breastmilk substitutes using a wide variety of tactics, including exposés, boycotts, shareholder campaigns,and lawsuits. At issue was the transfer of two inappropriatetechnologies to developing countries. First, there was the questionable use of bottle feeding, whose safe use requires literacy, knowledge of sterilization techniques, access to clean water, and money to buy enough of a breastmilk substitute. Second, sophisticated marketing and promotion practices aimed at creating the need for these Western middle-class products were seen as potentially harmful when targeted to the Third World poor.
At informational hearings in the US Senate in 1978, corporate executives testified that they were unwilling to substantially change their marketing practices since they were not responsible for the conditions—contaminated water, illiteracy, and the lack of resources to purchase enough of the product—that led to the predictable harms to infant health from using breastmilk substitutes. Following this, Senator Edward Kennedy, along with thousands of advocates, sought action by the World Health Organization. An expert group meeting in 1979 recommended the development of a code,and the idea was authorized by the 1980 World Health Assembly.
The parties to the Code negotiations included representatives of Member States of the World Health Assembly; officials of the World Health Organization, UNICEF, and other intergovernmental bodies; representatives of the major international producers of breastmilk

substitutes; and leaders of the non-governmental organizations who were campaigning to end promotion of breastmilk substitutes. This was the first time NGOs participated to this degree in intergovernmental negotiations. In the WHA, an alliance grew between the Northern advocacy groups and the Southern governmental representatives, buttressed by the several Northern Europeangovernments who tended to be sympathetic to developing country demands and who, in addition, didn’t have a strong domestic breastmilk-substitutes industry.
The NGOs brought to the WHA a team of advocates from North and South countries, armed with the latest scientific research on the benefits of breastfeeding and examples of egregious promotional practices from around the world. Even though the NGOs couldn’t participate in the formal debate, their presence and the issues they were presenting had an electrifying affect on the normally more stolid proceedings.For the first time in history, international standards, sanctioned by the UN, were established to control the excesses of a large multinational industry.
ELEMENTS OF THE CODE STRUGGLE ADAPTABLE TO OTHER ISSUES
A crucial feature in any attempt to create an international intergovernmental instrument implementing human rights standards is the necessity of bringing about a working alliance between the sympathetic governments -- usually those most affected by the problem -- and the advocacy NGOs.In this partnership, it is the job of the NGOs to insure theaccessibility and accuracy of the latest relevant scientificinformation and data. Reliable research and data proving or demonstrating harm are necessary to challenge economically profitable practices of major industries. Government officials will rely on this information to strengthen their negotiating positions on behalf of reform. In 1980-81 it wasinnovative for NGOs to be present at intergovernmental negotiations. Now it is common--the debate being to what degree and when rather than whether. The effect on any
intergovernmental meeting of the active presence of advocacyNGOs is likely to be enormous.
If the issue in question involves a particular corporate sector, which is often the case for specific problems relating to nutrition, health safety, or the environment, the language of the intergovernmental instrument must specifically address the obligations and responsibilities ofthat sector. The Code broke new ground in this regard and addressed the responsibilities not only of government, but the responsibilities of manufacturers and distributors of breastmilk substitutes, as well as those of health workers, non-governmental organizations, professional groups and consumer organizations. Specifying the responsibilities of non-governmental actors in the intergovernmental instrument will make easier the task of translating the instrument intonational law.
At the time of the Code’s adoption, its status as a non-binding resolution was a disappointment to the NGOs who wereadvocating for a regulation, a more binding instrument underthe WHO Constitution. But, like the Universal Declaration of HumanRights, this "expression of the collective will of the membership of the World Health Assembly" carries a moral force and power in the world at large far beyond the Assembly’s Constitutional right to make recommendations to its membership. It establishes internationally agreed upon minimum standards for all countries regardless of their economic status. Companies feel obligated to profess adherence to it. However, no formula company, in fact, fullyfollows the Code. Companies that state that the Code is their policy actually only claim to apply it in developing countries.
Since the Code was adopted as a "minimum requirement", it sets the floor for acceptable standards rather than the ceiling. This is particularly important for policies that deal with marketing practices and products. Since marketing practices and product lines change in response to market conditions, establishing minimum standards allows for

flexibility in standard setting. Indeed, a number of national laws implementing the Code have provisions setting forth the procedures for revising the law and expanding the scope of covered products in response to changes in marketing and promotion strategies.
Another element to be included when developing similar humanrights instruments is the requirement that the issue appear regularly on the forum’s agenda. The resolution authorizing the Code’s development and the resolution adopting the Code both require biannual reports on the promotion of breastfeeding and the status of implementation of the Code. By keeping the issue alive on the organization’s agenda, governments will have up-to-date information, and the debatebetween NGOs and companies will be held in the public intergovernmental arena.
Moreover, appearing regularly and predictably on the agenda has meant an opportunity every two years to adopt resolutions which further clarify and strengthen the Code. To date, three subsequent resolutions have adopted clarifications and additional recommendations vis-à-vis the Code. As a result, the World Health Assembly often refers toits adopted policies in this area collectively as "the International Code and subsequent relevant resolutions". All parties understand the significance of this requirement, andover the years, there have been several attempts (led by governments that are the home countries for the corporationsaffected) to remove the issue from the WHA agenda.
Since the Code was adopted as a non-binding resolution, the WHA took particular care to urge all Member States "to translate the International Code into national legislation, regulations and other suitable measures." Because the Code envisions that governments will translate it into legislation, enforcement should become a function of the national regulatory structures. However, translating the Code into national law, and then monitoring and enforcing that law is a process that takes years.
Unfortunately, one area where the Code is weak is its failure to establish at the World Health Organization, or other intergovernmental body such as UNICEF, a Secretariat to fully monitor not only national law development, but whether the practices of specific manufacturers and distributors conform to the Code. Such a Secretariat was envisioned in various drafts of the Code, but was defeated during the negotiation process. This is an important elementto incorporate into a similar human rights instrument.
THE GROWTH OF IBFAN
The International Baby Food Action Network (IBFAN) was born when NGOs from both North and South countries met in Geneva at the WHO to strategize how best to influence the expert meeting they were attending to support the development of a Code. From the outset, they understood the necessity of publicizing up-to-date information and examples of the ongoing promotional practices of the industry. Since 1980 IBFAN has biannually produced an in-depth compendium of company promotion practices and violations of the Code. Overthe last 17 years, IBFAN has grown from a handful of people to a world-wide network of groups in over 90 countries. IBFAN’s International Code Documentation Centre in Penang has trained approximately 200 government officials from 80 countries on Code development and implementation. The effortand commitment of IBFANers has been key in keeping breastfeeding and the Code on the international agenda, and in moving the Code from a set of recommendations on paper toenforceable national law. This unique achievement has inspired the creation of other international NGO advocacy efforts, such as the Pesticides Action Network (PAN) and Health Action International (HAI).
THE BABY FRIENDLY HOSPITAL INITIATIVE
In 1992, UNICEF and WHO launched the Baby Friendly Hospital Initiative (BFHI). This was the first time since the Code’s adoption that significant international resources and
personnel would be devoted to promoting breastfeeding and urging governments to act to restrict promotion of breastmilk substitutes. BFHI has two complementary goals. The first asks hospitals to transform their practices to actively support rather than discourage breastfeeding by following the Ten Steps to Successful Breast-Feeding. The second asks governments to enact policies or laws stopping companies from distributing free or low-cost supplies of breastmilk substitutes to health care facilities. Health systems which have to purchase breastmilk substitutes are more likely to use them only when needed for a specific child, rather than to routinely feed all infants in the facility.
UNICEF and WHO relied on the promise made by the trade association of breastmilk manufacturers that its members would stop giving free supplies in developing countries onlyso long as governments adopted policies that would make thisa requirement for all companies. From the outset, there weresignificant differences between what the companies were prepared to do and the policies that the intergovernmental bodies were urging governments to adopt, since these had to be consistent with the Code and subsequent resolutions. As stated previously, in 1994 the WHA attempted to resolve any future disputes by supporting a total ban on donations of free and low-cost supplies to the whole health care system. Today, as a result of the BFHI, there are more than 7,000 hospitals that have been designated "Baby Friendly". All butone or two of the developing countries where free supplies were distributed have adopted policies, regulations or laws banning such donations.
Adopting a policy, however, doesn’t necessarily mean enforcing a policy. Therefore, monitoring and enforcement remain ongoing issues. BFHI’s focus on a regulatory instrument to control marketing stimulated renewed interest in the Code aswhole, and the transformation of the Code into national law has greatly accelerated as a result.

DEVELOPMENT OF NATIONAL LAW
Nearly 30 countries have adopted the Code as law, and othersare in various stages of law development. Still others have adopted the Code with weaker legal status and various degrees of comprehensives. Thus, it is now possible to review the benefits and pitfalls of different experiences. As indicated in the following brief accounts, some countries, like India and Zimbabwe, developed their laws with active NGO participation. In China the law was developed by government without strong NGO involvement. In Guatemala, the law was challenged as violating free trade rules.
India
In 1992, after ten years of intense negotiations and lobbying, India adopted the Infant Milk Substitutes, Feeding Bottles andInfant Foods Bill. By 1993, the government introduced regulations for implementation, including very specific label requirements. National consumer advocacy groups, breastfeeding promotion groups, and pediatrics and child care associations, lobbied for the bill’s adoption. The mostunique and innovative aspect of the bill is its authorizing of voluntary organizations to bring criminal complaints for violations of the act for prosecution by an Assistant PublicProsecutor. Complaints have now been brought by voluntary organizations against Johnson & Johnson, Nestlé and a local manufacturer. In November 1995 Johnson & Johnson announced it was ending marketing baby bottles in India. The complaintagainst Nestlé concerns its failure to translate important warnings on baby milk tins into Hindi. (India has a population of 900 million, of which half are literate in Hindi and less than 4% read English). Nestlé failed to appear on two court dates, and is challenging the act as arbitrary and unconstitutional. The case is currently under consideration by the New Delhi High Court. The enforcement role given to voluntary, non-governmental organizations is effective and crucial. This procedure should be followed in other countries, particularly where government resources for
health inspectors and consumer protection agencies is limited.
Zimbabwe
In Zimbabwe, as in several other smaller countries, there isa useful overlap of membership between women’s health and breastfeeding promotion organizations and government agencies. This overlap has influenced the high degree of government commitment to the Code and breastfeeding promotion. From 1981 on, the Government of Zimbabwe has beenactively involved in educating health personal and circulating rules to health facilities restricting promotion. By 1984, a code was adopted, which was incorporated into the national Public Health Act in 1986. Zimbabwe’s law has a broad scope. It applies not only to infant formula but to follow-up formulas and other foods foruse by infants and young children up to three years of age.
Until the trade liberalization policies of the last few years, Nestlé had a virtual monopoly of the market, and thusfaced little competitive pressure. Now, with more products available, increased competition can result in more promotion. Therefore, there is a greater need for monitoringand enforcement. A government survey in 1994 found that exclusive breastfeeding is uncommon and early supplementation is a significant problem, although 95% of the babies are breastfed at 10 -11 months of age. In addition, Zimbabwean families are too poor to spend preciousresources on commercial breastmilk substitutes. The cost of purchasing enough of a commercial product for a one month period ranges from 78% to 140% of the monthly minimum wage. For these reasons, Zimbabwe is now in the process of revising its 1986 regulations, with the involvement of both non-governmental organizations and industry representatives.The non-governmental organizations are seeking the regularization of monitoring to ensure that marketing practices conform to the national law and the International Code. As leaders of IBFAN Africa, they are also working

towards a coordinated, regional effort for law development and monitoring in Sub-Saharan Africa.
China
It appears that China’s Ministry of Health became committed to drafting a national law based on the Code as a result of its involvement with the Baby Friendly Hospital Initiative. In 1992, as part of BFHI, it issued an administrative notification to stop permitting free supplies of breastmilk substitutes in health care facilities. The notification alsobanned advertising, promotion and financial support from companies. Thereafter, it began in earnest to draft a law. For public health officials, fast action was imperative since the opening of the Chinese market would be accompaniedby aggressive competition among companies, to the detriment of breastfeeding.
China’s law took effect October 1, 1995. However, comprehensive monitoring and enforcement is probably years away. In many countries, monitoring has been largely conducted by NGOs involved in breast-feeding advocacy, oftenwith government approval and sometimes support. China, however, lacks this kind of local NGO involvement. An unusual situation has developed in China because the internationally respected children’s aid society, Save the Children, began to monitor company practices. It has now asked the Chinese Government to investigate its findings that Nestlé "has made Lactogen [infant formula] widely available in six hospitals in Kunming, where it has targetedhealth professionals with both free and discounted supplies of the formula." This public airing of their complaint of violations came after a year of private effort by Save the Children to prod Nestlé’s chairman to take action against the abuses. Nestlé repeatedly denied the allegations, and conducted, according to Save the Children, an inadequate investigation of the situation.
The Chinese law, which came into force during this controversy has a number of provisions that are stronger
than the Code, including ending gifts and donations to academic bodies. Sanctions against violators can include fines and orders to stop marketing. However, China is a verylarge country with little ability to monitor and enforce thelaw, particularly without an aggressive NGO movement. Enforcement may depend on the good-will of aid organizationssuch as Save the Children. Hopefully, country-based offices of international agencies such as UNICEF will assist the government in monitoring adherence to its law.
Guatemala and Costa Rica
Using the Code as a "minimum requirement", Guatemala included all complementary foods--not just bottle-fed ones--in its 1983 law. But in 1992, the Gerber Company began a campaign to pressure the Guatemalan government to exempt Gerber from the law because it was introducing a new productline of complementary foods into Guatemala and other countries in the region. Gerber began advertising on TV, andinsisted that its labels continue to depict the Gerber baby,both in clear violation of the national law and the International Code. After the Ministry of Health refused to exempt Gerber, Gerber brought numerous legal actions and enlisted the United States State Department and Central American economic ministers to its cause. At stake was Guatemala’s trade status with the US and a threatened ban ofimports under the regional free trade agreement. After threeyears of pressure, Guatemala caved in and its Supreme Court exempted imported baby foods from the scope of the national law. The anomalous effect is that Guatemala may now be in violation of the regional and GATT free trade regimes since imported products are given preferential treatment under national law. Unfortunately, only the government has standing under World Trade Organization rules to challenge this preference, which, under the circumstances, will surelynever happen.
A similar campaign is under way in Costa Rica, where industry is alleging that Costa Rica’s new national law implementing the Code imposes non-tariff barriers to trade.

MONITORING THE INTERNATIONAL CODE
While the Code tells governments to give effect to the Code,as appropriate to each government’s social and legislative framework, through the adoption of "national legislation, regulations or other suitable measures," it also instructs companies that "independently of any other measures taken for implementation," they should monitor their marketing practices and take steps to ensure that their conduct at every level conforms to the Code.
Although industry consistently argues in favor of voluntary compliance with the International Code, and voluntary national codes in lieu of law, the companies individually, or collectively through their industry association, have failed to monitor their compliance with the Code provisions.To date, most Code monitoring has been undertaken by groups associated with IBFAN. In 1994, IBFAN coordinated a monitoring exercise involving country level monitoring projects in 23 countries, and their report, Breaking the Rules 1994, included information received from 62 countries.
Companies have gone to great lengths to deny what is in the IBFAN reports. As a result, there has been a great deal of confusion and disagreement about company compliance with theCode. Seeking the truth, a consortium of children’s aid, academic and church organizations called the Interagency Group on Breastfeeding Monitoring (IGBM) commissioned research in 1996 to obtain objective evidence of violations of the Code. While it solicited reactions to its research protocol from the industry and IBFAN, it conducted its research independently of both groups.
The IGBM study was carried out in Poland, Bangladesh, Thailand and South Africa. The research design randomly selected pregnant women, mothers of infants and health workers for interviews, with a target sample size in each country of 120 health workers and 800 mothers and mothers-to-be at 40 health facilities. The results, published in a
report entitled Cracking the Code, proved, again, that companies "are taking action which violates the Code, and ina systematic rather than one-off manner."
In all four countries, company information not in compliancewith the Code was given to mothers and health facilities; mothers and health workers received free samples; company personnel visited health facilities in ways that contravenedCode restrictions; and, posters and products were improperlydisplayed. The findings created headlines throughout Europe,and calls for increased pressure on the companies to conformto the Code. The report indeed confirms that monitoring, whether of the Code or of national law implementing the Code, must be undertaken independent of the manufacturers and distributors of breastmilk substitutes. Most importantly, though, the report underscores the need to moveexpeditiously towards national law implementation, coupled with the political will to monitor and enforce the law. Thisis clearly the only way to assure that mothers and children will have the rights the Code seeks to protect.
CONCLUSION
In 1996, after defeating an attempt to remove the issue of the Code from the regular agenda, the World Health Assembly adopted a new resolution urging Member States to ensure thatCode monitoring is "carried out in a transparent, independent manner, free from commercial influence". This isan issue of increasing importance, as demonstrated by the independent IGBM research revealing violations of the Code. Indeed, in recent years companies have been trying to influence various monitoring projects by shaping the research protocols or donating large sums of money.
The resolution also appears to clarify other disputed areas of the Code by explicitly asking states to protect the full breastfeeding period. While there have been various interpretations of the language describing which complementary foods are covered under the Code’s scope, this
resolution takes a more inclusive approach by ensuring that all "complementary foods are not marketed for or used in waysthat undermine exclusive and sustained breastfeeding." (Emphasis added) In the past, although there is nothing in the Code to support this contention, companies have argued that the Code was intended to apply only to products used inthe first six months of life. This alleged six-month cut-offhas now clearly been rejected by the WHA.
Significantly, this resolution also addresses the conflict of interest which may arise as a result of financial supportprovided to health professionals by companies. Again, this is an area of long-simmering dispute, and its inclusion in the 1996 resolution is a notable achievement.
The Code and the three substantive clarifying resolutions clearly demonstrate that only through joint and sustained efforts by non-governmental organizations working with nation-states can transnational companies be restrained. By their very nature, transnational companies are able to operate in ways that transcend national controls. Indeed, many transnational companies have economies far larger than the countries in which they market and invest. The politicalinfluence of this kind of economic might is incalculable. The Code establishes minimum standards at the intergovernmental level which companies are expected to follow even if a government has not adopted a national law. In addition, governments are called upon to translate the Code into enforceable national law. Since the Code operates on these two levels, it represents a potent strategy for gaining some control over transnational corporate policies that directly impact citizens who have no other effective means of protection.
The UN and its associated bodies are more accessible to non-governmental organizations than other intergovernmental and multilateral fora, and it is the accepted arena for the development of international human rights law. Therefore, the UN remains the best available arena for developing legalinstruments such as the Code for holding transnational
corporations accountable for practices which clearly violateinternationally recognized human rights. The Code experiencedemonstrates a practical and effective way to implement specific provisions in a variety of human rights instruments. By specifically addressing the responsibilitiesof corporations and other non-state actors, the Code expandsthe reach of human rights law. It establishes one of the fewarenas in which transnational companies can legitimately be called to account as potential violators of human rights under international law.
Return to Special Issue Contents Page
Related Documents











