Pe u tz-Jeg h ers Syndrome with Feminizing Sertoli Cell Tumor JOSE MARIA CANTU, MD, HORACIO RIVERA, MD, RENE OCAMPO-CAMPOS, MD, NORMA BEDOLLA, MSC, VINCENTE CORTES-GALLEGOS, MD, AMADO GONZALEZ-MENDOZA, MD, MIGUEL DfAZ, MD, AND ALEJANDRO HERNANDEZ, MD A case involving a 6-year-old boy with Peutz-Jeghers syndrome and an unilateral feminizing Sertoli cell tumor is described. Endocrinologic studies revealed consistently high plasma and urine levels of estrogens and normal levels of testosterone and dihydrotestosterone. The increased levels of estrogens did not show changes that could be correlated with exogenous gonadotropin administration, thus in- dicating an autonomous nature. The histopathologic studies of nontumorous testicular tissue revealed changes in the seminiferoustubules which suggested that estrogens, directly or indirectly, may have had both stimulating and atrophying effects. It is concluded that gonadal tumors are an additional mani- festation of the Peutz-Jeghers syndrome gene in both male and female patients. Cancer 46:223-228, 1980. N 1921, P E U T Z ~ ~ observed oral melanosis associated I with nasal and intestinal polyps in several members of a Dutch family. In 1949, Jeghers et al.I3 described additional cases and provided evidence of autosomal dominant inheritance. Since then, there have been reports of many other cases of this disorder, which is currently known as Peutz-Jeghers syndrome. The in- testinal polyps are of an hamartomatous nature1*z’fi,29,30 whose propensity for malignancy is still uncer- tain.6Jfi~17~z0~2Y Ovarian tumors are more common in women with Peutz-Jeghers syndrome than in the general female p ~ p u l a t i o n ; ~ ~ ~ * ~ ~ ~ ~ ~ however, no associ- ation between Peutz-Jeghers syndrome and gonadal tumors has been reported in the male patient. The pur- pose of this report is to describe for the first time, the association of Peutz-Jeghers syndrome with a Sertoli cell tumor, to emphasize the variable expres- sivity and pleiotropism of the causal gene, and to cor- relate the testicular histopathologic findings with the tumoral endocrine dysfunction. From the Divisiones deGenetica y Hematologia, Patologia Experimental y Biologia de la Reproduccion (CMN), Subjefatura de Investigacion Cientifica, Unidad de Investigacion Biomedica, y Hospitales de Pediatria y Gineco-Obstetricia, Centro Medico de Occidente, Instituto Mexican0 del Seguro Social, Guadalajara, Jalisco, Mexico. Supported in part by a grant from the Ford Foundation. Address for reprints: J. M. Cantu, MD, Apartado Postal 1-3838, Guadalajara, Jalisco, Mexico. The authors thank Drs. Gregorio Perez-Palacios and Tomas Morato for LH and FSH determinations and Dr. Enrique Corona-Rivera for his help in the clinical studies. Accepted for publication July 6, 1979. Case Report Clinical and Familial Data The 6-year-old patient was the second child of noncon- sanguineous parents; aged 27 (father) and 28 (mother) years at his birth. The pregnancy, delivery, and psychomotor development were normal. An urethral meatotomy was per- formed when he was four years old because of congenital stenosis. At five years of age, medical consultation was sought for bilateral gynecomastia with an evolution of about two years; it was progressive, painless, without galactorrea, with slight predominance on the right side and associated with a rapid increase in stature. He also had numerous small (1-4mm) blackish macules on the lips and the buccal mucous membranes, without any additional symptoms. Upon physi- cal examination at five years; seven months of age, the fol- lowing somatometric data were found: height, 119 cm (above the 97th percentile corresponding to about the 50th percentile for seven and a half years); weight, 24 kg; arm span, 119 cm; upper to lower segment ratio, 1.05; and cephalic, thoracic and abdominal circumferences of 52, 68, and 59 cm respec- tively. The clinical features included melanosis oris (Fig. l), severe bilateral gynecomastia (Tanner’s Stage 111) with im- mature nipples, and large testes for his age (Tanner’s Stage 11-111) measuring 3.5 x 2.0 cm, but with normal morphology and consistency. The penis was normal without evidence of precocious virilization. Ophthalmologically , the pro- positus showed nonaccomodative alternate esotropia. Laboratory Studies Laboratory studies including urinalysis, blood cell count, plasma glucose, urea and creatinine, liver and thyroid function tests, screening tests for metabolic defects 0008-543X/80/0701/0223 $0.80 0 American Cancer Society 223

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Pe u tz- Jeg h ers Syndrome with Feminizing Sertoli Cell Tumor
JOSE MARIA CANTU, MD, HORACIO RIVERA, MD, RENE OCAMPO-CAMPOS, MD, NORMA BEDOLLA, MSC, VINCENTE CORTES-GALLEGOS, MD, AMADO GONZALEZ-MENDOZA, MD, MIGUEL DfAZ, MD,
AND ALEJANDRO HERNANDEZ, MD
A case involving a 6-year-old boy with Peutz-Jeghers syndrome and an unilateral feminizing Sertoli cell tumor is described. Endocrinologic studies revealed consistently high plasma and urine levels of estrogens and normal levels of testosterone and dihydrotestosterone. The increased levels of estrogens did not show changes that could be correlated with exogenous gonadotropin administration, thus in- dicating an autonomous nature. The histopathologic studies of nontumorous testicular tissue revealed changes in the seminiferous tubules which suggested that estrogens, directly or indirectly, may have had both stimulating and atrophying effects. It is concluded that gonadal tumors are an additional mani- festation of the Peutz-Jeghers syndrome gene in both male and female patients.
Cancer 46:223-228, 1980.
N 1921, P E U T Z ~ ~ observed oral melanosis associated I with nasal and intestinal polyps in several members of a Dutch family. In 1949, Jeghers et al.I3 described additional cases and provided evidence of autosomal dominant inheritance. Since then, there have been reports of many other cases of this disorder, which is currently known as Peutz-Jeghers syndrome. The in- testinal polyps are of an hamartomatous nature1*z’fi,29,30 whose propensity for malignancy is still uncer- tain.6Jfi~17~z0~2Y Ovarian tumors are more common in women with Peutz-Jeghers syndrome than in the general female p ~ p u l a t i o n ; ~ ~ ~ * ~ ~ ~ ~ ~ however, no associ- ation between Peutz-Jeghers syndrome and gonadal tumors has been reported in the male patient. The pur- pose of this report is to describe for the first time, the association of Peutz-Jeghers syndrome with a Sertoli cell tumor, to emphasize the variable expres- sivity and pleiotropism of the causal gene, and to cor- relate the testicular histopathologic findings with the tumoral endocrine dysfunction.
From the Divisiones deGenetica y Hematologia, Patologia Experimental y Biologia de la Reproduccion (CMN), Subjefatura de Investigacion Cientifica, Unidad de Investigacion Biomedica, y Hospitales de Pediatria y Gineco-Obstetricia, Centro Medico de Occidente, Instituto Mexican0 del Seguro Social, Guadalajara, Jalisco, Mexico.
Supported in part by a grant from the Ford Foundation. Address for reprints: J. M. Cantu, MD, Apartado Postal 1-3838,
Guadalajara, Jalisco, Mexico. The authors thank Drs. Gregorio Perez-Palacios and Tomas Morato
for LH and FSH determinations and Dr. Enrique Corona-Rivera for his help in the clinical studies.
Accepted for publication July 6, 1979.
Case Report
Clinical and Familial Data
The 6-year-old patient was the second child of noncon- sanguineous parents; aged 27 (father) and 28 (mother) years at his birth. The pregnancy, delivery, and psychomotor development were normal. An urethral meatotomy was per- formed when he was four years old because of congenital stenosis. At five years of age, medical consultation was sought for bilateral gynecomastia with an evolution of about two years; it was progressive, painless, without galactorrea, with slight predominance on the right side and associated with a rapid increase in stature. He also had numerous small (1-4mm) blackish macules on the lips and the buccal mucous membranes, without any additional symptoms. Upon physi- cal examination at five years; seven months of age, the fol- lowing somatometric data were found: height, 119 cm (above the 97th percentile corresponding to about the 50th percentile for seven and a half years); weight, 24 kg; arm span, 119 cm; upper to lower segment ratio, 1.05; and cephalic, thoracic and abdominal circumferences of 5 2 , 68, and 59 cm respec- tively. The clinical features included melanosis oris (Fig. l) , severe bilateral gynecomastia (Tanner’s Stage 111) with im- mature nipples, and large testes for his age (Tanner’s Stage 11-111) measuring 3.5 x 2.0 cm, but with normal morphology and consistency. The penis was normal without evidence of precocious virilization. Ophthalmologically , the pro- positus showed nonaccomodative alternate esotropia.
Laboratory Studies
Laboratory studies including urinalysis, blood cell count, plasma glucose, urea and creatinine, liver and thyroid function tests, screening tests for metabolic defects
0008-543X/80/0701/0223 $0.80 0 American Cancer Society
223
224 CANCER July 1 1980 Vol. 46
TABLE 1. Urinary Excretion (24 Hours) of Total Estrogens (EJ, 17-Ketosteroids (17-0), 17-Hydroxysteroids (17-OH),
and Creatinine
17-0 17-OH E, Creatinine Volumen Sample (mg) (mg) (PSI (g) (ml)
1. Basal 2.5 3.0 15.3 0.85 978.0 2. Basal 2.2 0.7 14.03 0.5 635.0 3. DST 0.8 13.3 0.54 630.0 4. DST 0.4 18.6 0.65 750.0 5 . DST ND 11.7 0.59 640.0
DST = dexamethasone suppression test; ND = not detectable.
(Phenistix, glucose oxidase, Millon, anthrone, ferric chloride, DNPH, nitrosonaphthol, acid albumin turbidity, CTA, methylmalonic acid, Benedict, and cyanide nitroprusside), brain gammagram, urocystogram, and x-chromatin and karyo- type, all yielded normal results. Determinations of total estrogens (EJ, 17-ketosteroids (17 = 0) and 17-hydroxy- steroids (17-OH) in 24-hour urine studies, basal as well as after adrenocortical inhibition with dexamethasone (500 mg every 6 hours for four days), showed consistently high levels of estrogens and a normal decrease in the levels of 17-OH (Table 1).
Radiologic Studies
Results of a barium-meal examination, barium-enema studies, and intravenous pyelography with retroperitoneal insufflation were normal. The radiologic bone age was increased by about two years.
Familial Data
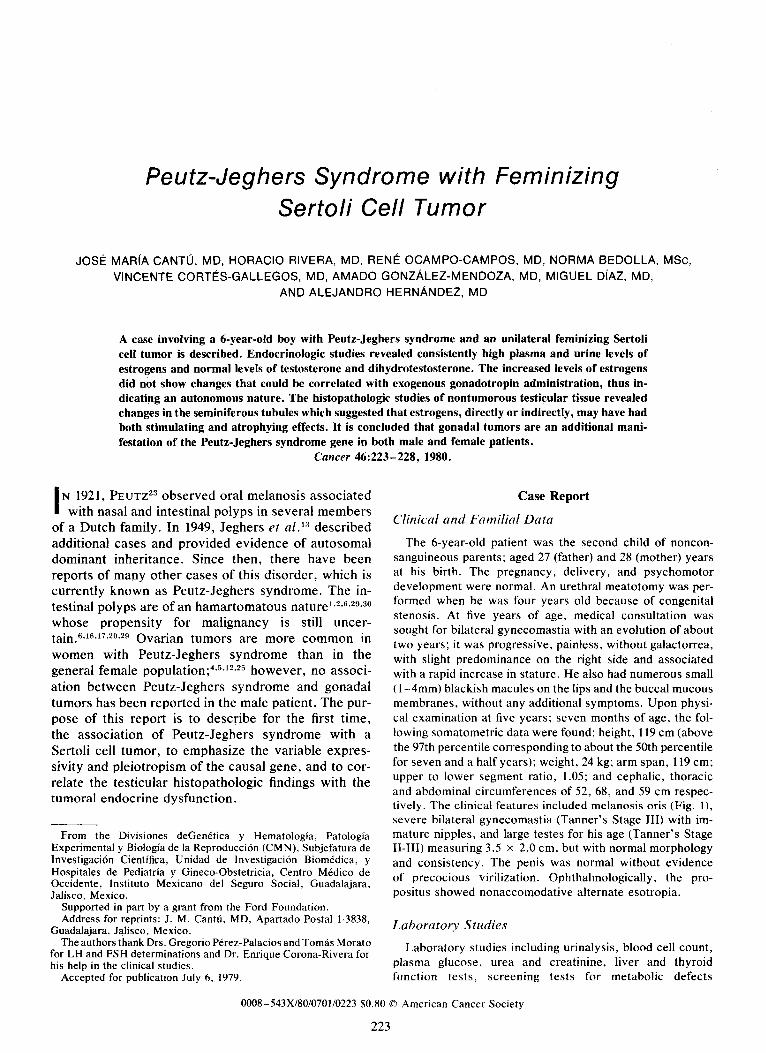
Familial studies revealed that the propositus' 7-year-old only brother had melanosis oris. The mother, born to a 38- year-old father, also showed melanosis oris as well as blackish macules on the palms (Fig. 1). None of the patients presented symptoms or radiologic evidence of polyposis.
FIG. 1. Melanosis oris in the propositus (top left) and in his mother (bottom left ). Melanosis of the palmar side of the mother's thumb is also shown (right).
No other relative had antecedents of mucocutaneous melanosis or gastrointestinal disorders suggestive of polyposis.
Materials and Methods
Plasma luteinizing hormone (LH) and follicle stimu- lating hormone (FSH) were measured by means of a double-antibody radioimmunoassay;** samples were assayed in duplicate at two different dilutions in order to ascertain parallelism with the standard curves. Results were expressed as ImU/ml of the second IRP- HMG preparation. Plasma testosterone (T), dihydro- testosterone (DHT), estradiol (E2), and Et deter- minations were carried out by means of radioim- m u n o a s ~ a y ~ , ~ ~ and the results expressed as pglml.
Hypothalamic Pituitary Studies
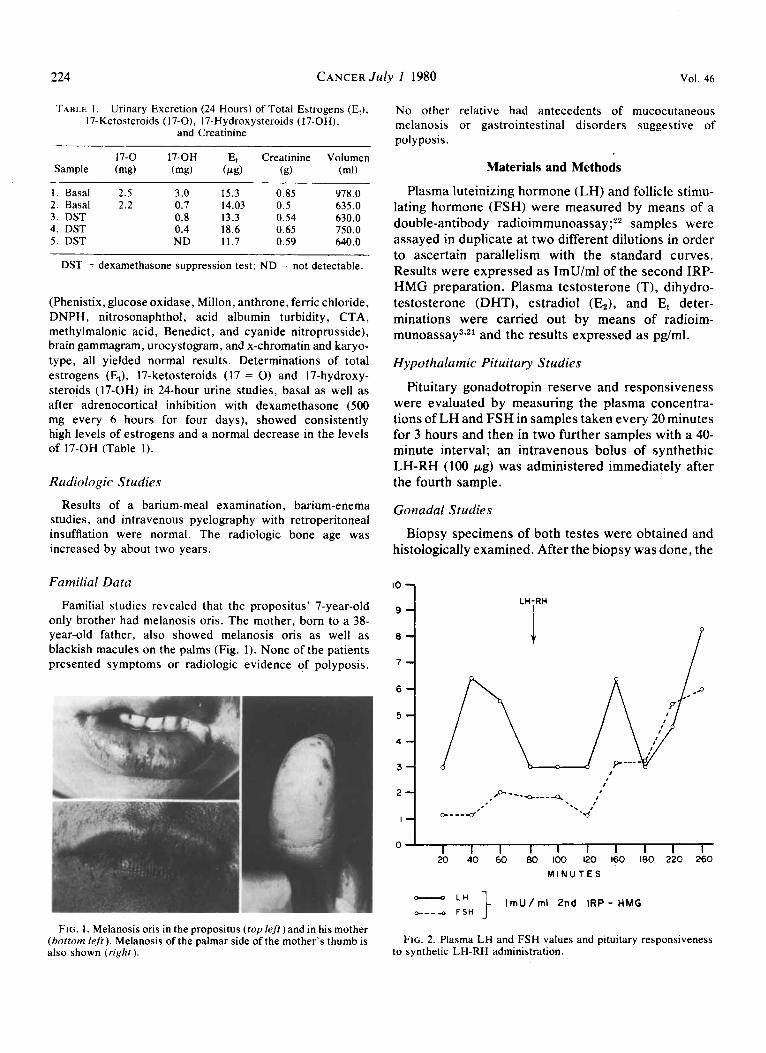
Pituitary gonadotropin reserve and responsiveness were evaluated by measuring the plasma concentra- tions of LH and FSH in samples taken every 20 minutes for 3 hours and then in two further samples with a 40- minute interval; an intravenous bolus of synthethic LH-RH (100 pg) was administered immediately after the fourth sample.
Gonadal Studies
Biopsy specimens of both testes were obtained and histologically examined. After the biopsy was done, the
10
8 g1 7
LH-RH
i
0 ' I I I I I I I I I 1 20 40 60 80 100 120 160 180 220 260
M I N U T E S - L H } I m U / m l 2nd I R P - H M G o----o F S H
FIG. 2. Plasma LH and FSH values and pituitary responsiveness to synthetic LH-RH administration.
No. 1 PEUTZ- JEGHERS SYNDROME .
HCG 2500 IU F$ ,&ol,!,u m n
Cantu et a1
f
225
2 4 92 199 250 279 501 342 412 3 5 ' 7 9 162330343g 38 132 251 272 2O6 328 380 454
1 D A Y
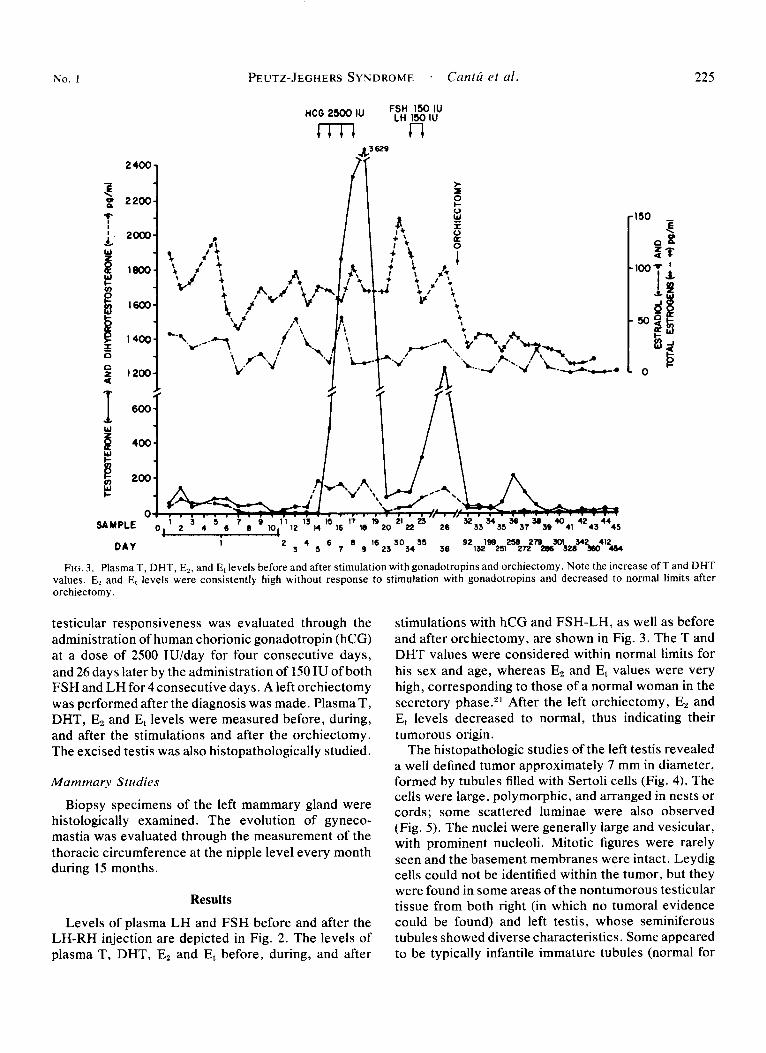
FIG. 3. Plasma T, DHT, E,, and Et levels before and after stimulation with gonadotropins and orchiectomy. Note the increase of T and DHT values. E2 and Et levels were consistently high without response to stimulation with gonadotropins and decreased to normal limits after orchiectomy.
testicular responsiveness was evaluated through the administration of human chorionic gonadotropin (hCG) at a dose of 2500 IU/day for four consecutive days, and 26 days later by the administration of 150 IU of both FSH and LH for 4 consecutive days. A left orchiectomy was performed after the diagnosis was made. Plasma T, DHT, E, and E, levels were measured before, during, and after the stimulations and after the orchiectomy. The excised testis was also histopathologically studied.
Mammary Studies
Biopsy specimens of the left mammary gland were histologically examined. The evolution of gyneco- mastia was evaluated through the measurement of the thoracic circumference at the nipple level every month during 15 months.
Results
Levels of plasma LH and FSH before and after the LH-RH injection are depicted in Fig. 2 . The levels of plasma T, DHT, E2 and E, before, during, and after
stimulations with hCG and FSH-LH, as well as before and after orchiectomy, are shown in Fig. 3 . The T and DHT values were considered within normal limits for his sex and age, whereas E, and E, values were very high, corresponding to those of a normal woman in the secretory phase.21 After the left orchiectomy, E, and E, levels decreased to normal, thus indicating their tumorous origin.
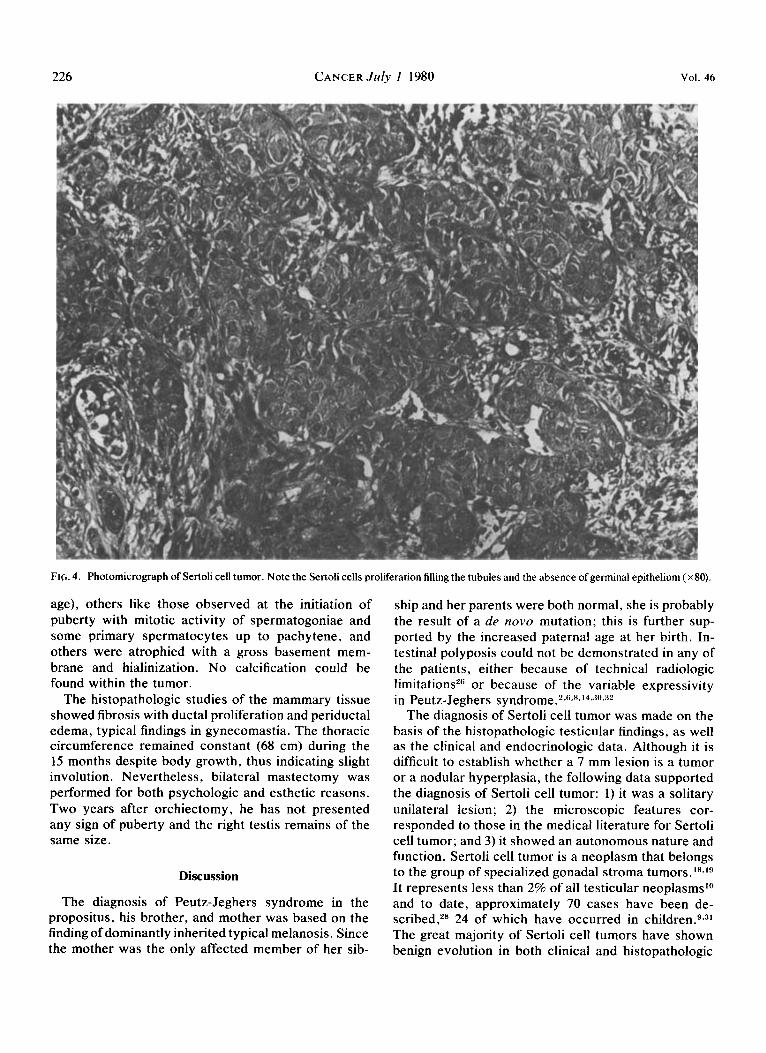
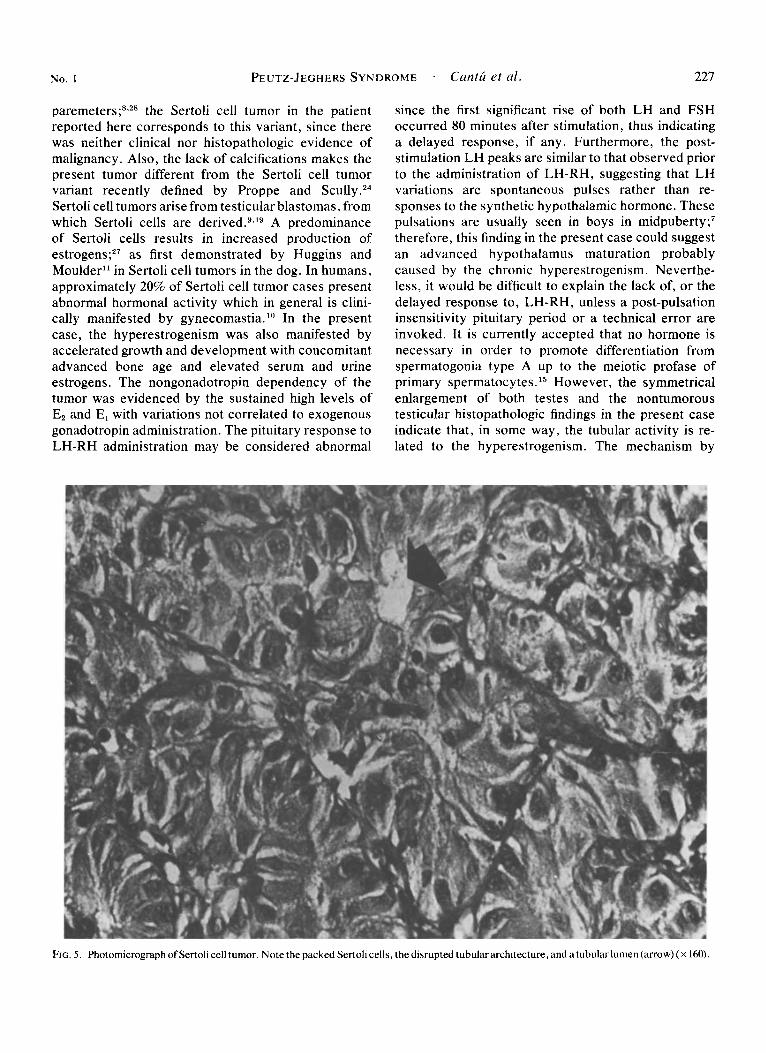
The histopathologic studies of the left testis revealed a well defined tumor approximately 7 mm in diameter, formed by tubules filled with Sertoli cells (Fig. 4). The cells were large, polymorphic, and arranged in nests or cords; some scattered luminae were also observed (Fig. 5 ) . The nuclei were generally large and vesicular, with prominent nucleoli. Mitotic figures were rarely seen and the basement membranes were intact. Leydig cells could not be identified within the tumor, but they were found in some areas of the nontumorous testicular tissue from both right (in which no tumoral evidence could be found) and left testis, whose seminiferous tubules showed diverse characteristics. Some appeared to be typically infantile immature tubules (normal for
226 CANCER July 1 1980 Vol. 46
Frp. 4. Photomicrograph of Sertoli cell tumor. Note the Sertoli cells proliferation filling the tubules and the absence of germinal epithelium ( ~ 8 0 ) .
age), others like those observed at the initiation of puberty with mitotic activity of spermatogoniae and some primary spermatocytes up to pachytene, and others were atrophied with a gross basement mem- brane and hialinization. No calcification could be found within the tumor.
The histopathologic studies of the mammary tissue showed fibrosis with ductal proliferation and periductal edema, typical findings in gynecomastia. The thoracic circumference remained constant (68 cm) during the 15 months despite body growth, thus indicating slight involution. Nevertheless, bilateral mastectomy was performed for both psychologic and esthetic reasons. Two years after orchiectomy, he has not presented any sign of puberty and the right testis remains of the same size.
Discussion
The diagnosis of Peutz-Jeghers syndrome in the propositus, his brother, and mother was based on the finding of dominantly inherited typical melanosis. Since the mother was the only affected member of her sib-
ship and her parents were both normal, she is probably the result of a de n o w mutation; this is further sup- ported by the increased paternal age at her birth. In- testinal polyposis could not be demonstrated in any of the patients, either because of technical radiologic limitations2'j or because of the variable expressivity in Peutz-Jeghers s y n d r ~ r n e . * ~ ~ ~ * ~ ~ ~ ~ ~ ~ ~ ~ ~
The diagnosis of Sertoli cell tumor was made on the basis of the histopathologic testicular findings, as well as the clinical and endocrinologic data. Although it is difficult to establish whether a 7 mm lesion is a tumor or a nodular hyperplasia, the following data supported the diagnosis of Sertoli cell tumor: 1) it was a solitary unilateral lesion; 2) the microscopic features cor- responded to those in the medical literature for Sertoli cell tumor; and 3) it showed an autonomous nature and function. Sertoli cell tumor is a neoplasm that belongs to the group of specialized gonadal stroma tumors. 18319
It represents less than 2% of all testicular neoplasmsl0 and to date, approximately 70 cases have been de- scribed,28 24 of which have occurred in ~ h i l d r e n . ~ ~ ~ ~ The great majority of Sertoli cell tumors have shown benign evolution in both clinical and histopathologic
No. 1 PEUTZ-JEGHERS SYNDROME . Cantu et al. 227
paremeters;8,28 the Sertoli cell tumor in the patient reported here corresponds to this variant, since there was neither clinical nor histopathologic evidence of malignancy. Also, the lack of calcifications makes the present tumor different from the Sertoli cell tumor variant recently defined by Proppe and S c ~ l l y . ~ ~ Sertoli cell tumors arise from testicular blastomas, from which Sertoli cells are derived."I9 A predominance of Sertoli cells results in increased production of
as first demonstrated by Huggins and Moulder" in Sertoli cell tumors in the dog. In humans, approximately 20% of Sertoli cell tumor cases present abnormal hormonal activity which in general is clini- cally manifested by gynec0mastia.l" In the present case, the hyperestrogenism was also manifested by accelerated growth and development with Concomitant advanced bone age and elevated serum and urine estrogens. The nongonadotropin dependency of the tumor was evidenced by the sustained high levels of E2 and E, with variations not correlated to exogenous gonadotropin administration. The pituitary response to LH-RH administration may be considered abnormal
since the first significant rise of both LH and FSH occurred 80 minutes after stimulation, thus indicating a delayed response, if any. Furthermore, the post- stimulation LH peaks are similar to that observed prior to the administration of LH-RH, suggesting that LH variations are spontaneous pulses rather than re- sponses to the synthetic hypothalamic hormone. These pulsations are usually seen in boys in midpuberty;' therefore, this finding in the present case could suggest an advanced hypothalamus maturation probably caused by the chronic hyperestrogenism. Neverthe- less, it would be difficult to explain the lack of, or the delayed response to, LH-RH, unless a post-pulsation insensitivity pituitary period or a technical error are invoked. It is currently accepted that no hormone is necessary in order to promote differentiation from spermatogonia type A up to the meiotic profase of primary ~permatocytes . '~ However, the symmetrical enlargement of both testes and the nontumorous testicular histopathologic findings in the present case indicate that, in some way, the tubular activity is re- lated to the hyperestrogenism. The mechanism by
FIG. 5. Photomicrograph of Sertoli cell tumor. Note the packed Sertoli cells, the disrupted tubular architecture, and a tubular lumen (arrow) ( X 160).
228 CANCER July I 1980 Vol. 46
which estrogens induced these changes can not be definitely established with the present data. Never- theless, an early maturation of the gonadostat or a direct effect of estrogens on germinal epithelium (or both), could be speculated.
Oncologically , an association between ovarian neo- plasms and Peutz-Jeghers syndrome of about 14% has been found.5 Some of them are granulosa cell tumors5 whose embriologic origin is identical to that of Sertoli cell tumors. Furthermore, the ovarian neoplasm which Scully termed “sexual cordon tumor with annular tubule^''^^ probably originated in the granulosa cells, shows a growth pattern very similar to that of Sertoli cell tumors. Of the 13 cases reported by this investigation, 6 patients were women with corrobora- ted Peutz-Jeghers syndrome.25
The association in Peutz-Jeghers syndrome of polyp- osis and ovarian tumors or Sertoli cell tumors could be explained on the basis of the defective action of a single gene during differentiation of the corresponding mesodermal and endodermal derivates. It may be con- cluded that gonadal tumors in Peutz-Jeghers syndrome have the same biologic significance in male and female patients and are additional evidence of pleiotropism.
REFERENCES
1 . Bartholomew LG, Dahlin DC, Waugh JM. Intestinal poly- posis associated with mucocutaneous melanin pigmentation: Peutz-Jeghers syndrome. Review of literature and report of six cases with special reference to pathological findings. Gastro- enterology 1957; 32:434-451.
2. Bartholomew LG, Moore CE, Dahlin DC, Waugh JM. In- testinal polyposis associated with mucocutaneous pigmentation. Surg Gynecol Obstet 1962; 115:l-11.
3 . Castaneda-Peiia G, Arellano H, Alonso-Uriarte R, Bedolla- Tovar N, Cortes-Gallegos V. Analisis de Androstendiona (A), Dihidrotestosterona (DHT) y Testosterona (T) en sujetos normales y sujetos intoxicados con Dibromocloropropano (DBCP). Proc XVIII Reun Annu Soc Mex Nut y Endocrinol Dec 6- 10, 1978.
4. Christian CD, McLoughlin TG, Cathcart ER, Eisenberg MM. Peutz-Jeghers syndrome associated with functioning ovarian tumor. JAMA 1964; 190: 157-160.
5. Dozois RR, Kempers RD, Dahlin DC, Bartholomew LG. Ovarian tumors associated with the Peutz-Jeghers syndrome. Ann Surg 1970; 172:233-238.
6. Erbe RW. Inherited gastrointestinal-polyposis syndromes. N Engl J Med 1976; 294:llOl-1104.
7. Faiman C, Winter JSD. Gonadotropins and sex hormones patterns in puberty: clinical data. In Grumbach MM, Grave GD, Mayer FE, eds. Control of Onset of Puberty. New York: John Wiley, 1974:32-61.
8. Farmer RG, Hawk WA, Turnbull RB. The sprectrum of the Peutz-Jeghers syndrome. Report of 3 cases. A m J Dig Dis 1965; 8:953-961.
9. Fligiel 2, Kaneko M, Leiter E. Bilateral Sertoli cell tumor of testes with feminizing and masculinizing activity occurring in a child. Cancer 38:1853-1858, 1976.
10. Goellner JR, Myers RP. Sertoli cell tumor. Case Report with ultrastructural findings. Mayo Clinic Proc 1975; 50:459-463.
11. Huggins C, Moulder PV. Estrogen production by Sertoli cell tumors of testis. Cancer Res 1945; 5:510-514.
12. Humphries AL, Jr, Shepherd MH, Peters HJ. Peutz-Jeghers syndrome with colonic adenocarcinoma and ovarian tumor. JAMA 1966; 197:296-298.
13. Jeghers H, McKusick VA, Katz KH. Generalized intestinal polyposis and melanin spots of the oral mucosa, lips, and digits: syndrome of diagnostic significance. N Engl J Med 1949; 241: 993-1005.
14. Kieselstein M, Herman G, Wahrman J, et al . Mucocutaneous pigmentation and intestinal polyposis (Peutz-Jeghers syndrome) in a family of Iraqui Jews with polycystic kidney disease. With a Chromosome Study. Israel J Med Sci 1969; 5:81-90.
15. Lostroh AJ. Hormonal control of spermatogenesis. In: Spilman CH. et a / . , eds. Regulatory Mechanisms of Male Repro- ductive Physiology. Amsterdam: Excerpta Medica 1976: 13-23.
16. McAllister AJ, Hicken NF, Latimer RG, Condon VR. Seventeen patients with Peutz-Jeghers syndrome in four genera- tions. Am J Surg 1967; l14:839-843.
17. McKittrick JE, Lewis WM, Doane WA, Gerwig WH. The Peutz-Jeghers syndrome. Report of two cases, one with 30-year follow-up. Arch Surg 1971; 103:57-62.
18. Mostofi FK. Infantile testicular tumors. Bull NY Acad Med 1952; 28:684-687.
19. Mostofi FK, Theiss EA, Ashley DJB. Tumors of specialized gonadal stroma in human male patients; androblastoma, Sertoli cell tumor, granulosa-theca cell tumor of the testis, and gonadal stroma tumor. Cancer 1959; 12t944-957.
20. Papaioannou A, Critselis A. Malignant changes in Peutz- Jeghers syndrome. N Engl J Med 298:694, 1973.
21. Perez-Angeles N, Valenzuela-Duriet P, Yanez-Aguilar V, Andrade-Vargas A, Cones-Gallegos V. Fisiologia Ovarica IV. Indices directos e indirectos de actividad estrogenica. Arch Invest Med (h4e.r) 1973; 4: 175- 190.
22. Perez-Palacios G, Iramain CA, et al. Plasma profile of pituitary gonadotropins and ovarian steroids in the normal menstrual cycle. Rev Invest Clin 1973; 25:305-313.
23. Peutz JLA. Over een zeer Merkwaardige, gecombineerde familiaire polyposis van de slijmvliezen van den tractus intestinalis met die van de neuskeelholte en gepaard met eigenaardige pig- mentaties van huid en slijmvliesen. Nederl Tijdschr Geneesk 1921; 10:134-146.
24. Proppe KH, Scully RE. Calcifying Sertoli cell tumor of testis: a study of nine cases of a distinctive tumor. Lab Invest 1978; 38:361.
25. Scully RE. Sex cord tumor with annular tubules. A distinc- tive ovarian tumor of the Peutz-Jeghers syndrome. Cancer 1970; 25: 1107- 1121.
26. Sheward JD. Peutz-Jeghers syndrome in childhood: unusual radiological features. Brit Med J 1962; 1:921-923.
27. Shiffman MA. Androblastoma(Serto1i cell tumor): case report. J Urol 1967; 98:493-496.
28. Talerman A. Malignant Sertoli cell tumor of the testis. Cancer 1971 ; 28:446-455.
29. Wennstrom J , Pierce ER, McKusick VA. Hereditary benign and malignant lesions of the large bowel. Cancer 1974; 34:850-857.
30. Wenzl JE, Bartholomew LG, Hallenbeck GA, Stickler GB. Gastrointestinal polyposis with mucocutaneous pigmentation in children. (Peutz-Jeghers syndrome). Pediatrics 1961; 28:655-661.
31. Wetzneir S, Gropp A. Sertoli cell tumor of testis in child- hood. Am J Dis Child 1974; 128:541-543.
32. Yosowitz P, Hobson R, Ruyman F. Sporadic Peutz-Jeghers syndrome in early childhood. A diagnostic dilemma. Am J Dis Child 1974; 128: 709-712.
Related Documents











