International Journal of Play Therapy, 12(1), pp. 47- 65 Copyright 2003, APT, Inc. PERSON-CENTERED PLAY THERAPY FOR ADULTS WITH DEVELOPMENTAL DISABILITIES Stephen P. Demanchick University of Rochester Nancy H. Cochran JeffL. Cochran State University of New York College Abstract: Due to problems in communicating with psychologists, counselors, and other daily helpers, adults with developmental disabilities may experience a lifetime of daily routines that involve few if any opportunities for emotional expression, validation, and growth. This paper presents two case studies that utilize an adapted form of Child-Centered Play Therapy in working with adults with developmental disabilities. Person-Centered Play Therapy is used to help two adults with developmental disabilities overcome behavioral and emotional difficulties. Results indicate positive growth and changes in self-expression, self- direction, self-efficacy, and emotional well-being. Changes are indicated both within sessions, and outside of sessions in a residential day treatment program. Possibilities for future work with this population are discussed. Meeting the behavioral and emotional needs of adults with developmental disabilities can be challenging for mental health professionals. Traditional methods of psychotherapy are rarely used due to clients' impairments in cognitive and verbal functioning (Walker, 1983). Because of the decreased usefulness of traditional methods of psychotherapy, adults with developmental disabilities may experience a lifetime of daily routines that involve few if any opportunities for Stephen P. Demanchick is a doctoral student at the University of Rochester in the Counselor Education and Human Development Program. Correspondence regarding this article should be addressed to: Stephen Demanchick, c/o Jeff L. Cochran, Department of Counselor Education, SUNY Brockport, 350 New Campus Drive, Brockport, NY 14420. Nancy H. Cochran is an adjunct instructor of Counselor Education at the State University of New York College at Brockport. Jeff L. Cochran is an assistant professor of Counselor Education at the State University of New York College at Brockport.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
International Journal of Play Therapy, 12(1), pp. 47- 65 Copyright 2003, APT, Inc.
PERSON-CENTERED PLAY THERAPY FORADULTS WITH DEVELOPMENTAL
DISABILITIES
Stephen P. DemanchickUniversity of Rochester
Nancy H. CochranJeffL. Cochran
State University of New York College
Abstract: Due to problems in communicating with psychologists, counselors,and other daily helpers, adults with developmental disabilities may experience alifetime of daily routines that involve few if any opportunities for emotionalexpression, validation, and growth. This paper presents two case studies thatutilize an adapted form of Child-Centered Play Therapy in working with adultswith developmental disabilities. Person-Centered Play Therapy is used to helptwo adults with developmental disabilities overcome behavioral and emotionaldifficulties. Results indicate positive growth and changes in self-expression, self-direction, self-efficacy, and emotional well-being. Changes are indicated bothwithin sessions, and outside of sessions in a residential day treatment program.Possibilities for future work with this population are discussed.
Meeting the behavioral and emotional needs of adults withdevelopmental disabilities can be challenging for mental healthprofessionals. Traditional methods of psychotherapy are rarely used dueto clients' impairments in cognitive and verbal functioning (Walker,1983). Because of the decreased usefulness of traditional methods ofpsychotherapy, adults with developmental disabilities may experience alifetime of daily routines that involve few if any opportunities for
Stephen P. Demanchick is a doctoral student at the University of Rochester in theCounselor Education and Human Development Program. Correspondence regarding thisarticle should be addressed to: Stephen Demanchick, c/o Jeff L. Cochran, Department ofCounselor Education, SUNY Brockport, 350 New Campus Drive, Brockport, NY 14420.Nancy H. Cochran is an adjunct instructor of Counselor Education at the State Universityof New York College at Brockport. Jeff L. Cochran is an assistant professor of CounselorEducation at the State University of New York College at Brockport.

48 Demanchick, Cochran, & Cochran
emotional expression, validation, and growth. As a result, many exhibitsymptomatic behaviors such as physical and verbal acting out, self-injury, withdrawal, disruptive verbal outbreaks and tantrums. Thisarticle presents the results of a study that used a person-centeredapproach to play therapy in working with young adults withdevelopmental disabilities, and explores possibilities for future workwith this population.
Mental retardation can be defined as "a) significant limitations ingeneral intellectual functioning; b) significant limitations in adaptivefunctioning, which exist concurrently; and c) the onset of intellectual andadaptive limitations before the age of 22 years" (Jacobson & Mulick, 1996p.13). In this article, the authors use the term developmentally disabledinstead of mentally retarded to reflect the current terminology beingused in the field.
These individuals often "suffer from social isolation asevidenced by withdrawal, depression, confusion, poor verbal skills, poorinteraction with peers and overdependence on authority figures" (Davis& Shapiro, 1983 p.147). Davis and Shapiro also suggest that negative self-esteem issues that result from social isolation of these individuals oftencauses them to appear unfit for psychotherapy. For individuals tofacilitate personal growth, independence, self-direction, and self-actualization, however, they need an opportunity to accept themselvescompletely while experiencing the acceptance of others (Guerney, 1983).In order to facilitate personal growth of persons with developmentaldisabilities, it is essential for the therapist to be able and willing to enterand experience their world, as unapproachable and incomprehensible asit might appear (Portner, 2001). Therefore, it seems imperative that thisbasic principle of person-centered psychotherapy be taken into account,and that empathy, acceptance, and positive regard be considered asessential in providing this opportunity for growth to all persons,including those with developmental disabilities.
Today there are programs and interventions available tofacilitate the positive participation of children and adults withdevelopmental disabilities in the life of their communities and families.Yet, the struggle to meet the mental health needs of children and adultswith developmental disabilities continues. Person-Centered PlayTherapy is an adapted form of Child-Centered Play Therapy (Guerney,2001; Nordling & Cochran, 1999) that may help persons of this

Person-Centerted Play Therapy 49
population overcome behavioral and emotional difficulties and exceedfunctional limitations in several major life activities.
According to Morrison and Newcomer (1975), play therapy canpositively impact the behavior and cognition of mentally retardedchildren. Play is a child's way to explore, learn and grow. Children usetheir actions in play as adults use their more highly developed verbaland abstract thinking skills (Axline, 1969). Kielhofner & Miyake (1981)suggest that a foundational element to individual development withinsociety is play. "Play is part and parcel human experience, its absencesignals a lesser quality of life" (Kielhofner & Mikaye, 1981, p.375).
During play, one may say that the "total child is present"(Landreth, 2002, p.16). Therefore, with a trained therapist, the child isable to fully express and explore feelings, thoughts, behaviors, andexperiences in a safe environment (Landreth, 2002). Axline (1969)outlined eight basic principles of play therapy that are essential for thesuccess of the child. Axline's principles emphasize empathy, rapport,and respect while allowing the child to test limits, fully express feelings,and gain autonomy through self-direction (Axline, 1969). Faith,acceptance, and respect are core attitudes in child-centered work(Moustakas, 1953).
Much like Axline's eight principles for play therapy, Desnoyers-Hurley and Hurley (1987) suggest nine principles for establishingrelationships with developmentally disabled clients. These nineprinciples are "accept the client as he is, understand reality as the clientsees it, accept the client's life circumstances, be consistent, separatetherapy from other aspects of life, keep the relationship totally devotedto the client, draw the client out, express genuine interest in the person,and be a real person" (p. 15-19). Rogers (1957) stated that a minimaltherapeutic relationship must occur and without it all other conditionshave no meaning.
Rogers (1957) went on to describe three essential conditions tofoster a therapeutic relationship: acceptance, unconditional positiveregard, and genuineness. The principles of psychotherapy are essentiallythe same for the developmentally disabled population as they are for thegeneral population. Adaptations must be made, however, to fit thespecific needs and developmental skills of the individual.
Adults with developmental disabilities experience differences infunctioning based on chronological age vs. mental age. Although adults

50 Demanchick, Cochran, & Cochran
with developmental disabilities have chronological ages of 22 or above,the authors' experience has shown that most of these individualsfunction cognitively, emotionally, and socially between the ages of 3 and13 years. Therefore, for this study, the authors adapted the model ofChild-Centered Play Therapy (CCPT) as developed by the NationalInstitute for Relationship Enhancement (NIRE) (Guerney, 2001; Nordling& Cochran, 1999) for adults with developmental disabilities. The modelwas renamed Person-Centered Play Therapy (PCPT) because theparticipants were adults. The purpose of this case study report is toinvestigate the process and outcomes of adapting a model of CCPT tomeet the mental health needs of adults with developmental disabilities.
METHODParticipants
The names and identifying information for these two casestudies have been changed to preserve client privacy and anonymity.One male, Mark, age 24, and one female, Melissa, age 22, participated.Permission for their participation was given by their guardians and bythe agency that provides residential and day services for them. Both arediagnosed as having moderate mental retardation with limited receptiveand expressive verbal ability. Melissa was diagnosed as autistic,whereas, Mark showed "autistic-like" features. Both exhibited behavioraldifficulties of concern to their day treatment providers (day programmanagers, behavior specialists, recreational therapists, and life skillsmanagers). Mark was referred for treatment due to frequent difficultieswith transitions, inability to get along without teasing, pinching orotherwise annoying others, and behaviors such as crying spells andgenerally depressed mood. Melissa was referred for difficulties withtransitions and adjusting to change, tantrums, and self-injuriousbehaviors (SIB). Mark's and Melissa's behavioral and emotionaldifficulties were of great concern to staff, and had not corrected throughusual measures such as behavior management plans, medications, and astructured environment in a day treatment facility.
TreatmentTreatment was provided at the participants' day program
treatment facility. Treatment was based on the training model of CCPTdeveloped by NIRE (Guerney, 1983; Nordling & Cochran, 1999). CCPT is

Person-Centerted Play Therapy 51
a method of play therapy developed by Virginia Axline, an associate ofCarl Rogers. It follows the principles of a person-centered approach totherapy of creating a non-judgmental, emotionally supportivetherapeutic atmosphere, but with clear boundaries that provide the childclient with psychological safety to permit the learning of emotional andbehavioral self-regulation. The child client is free to play and self-expresswithout evaluation, direction, or interference from the therapist. Limitsare provided as the need arises, and for realistic purposes of structuring(time limits) and child and therapist safety. Additionally, limits areexpressed in a therapeutic manner wherein the child client's desire to actor express is acknowledged with empathy. The CCPT training modeldeveloped by NIRE is skill-based and provides the therapist with amethod that allows for the child's optimal free expression, self-direction,and self-regulation. PCPT is an adapted form of this model of CCPT.
Direct supervision of the treatment was provided by the secondauthor, who is a certified supervisor of CCPT by NIRE, in order tosupport the treatment and ensure adherence to the NIRE CCPT model.This supervision was face-to-face for one hour each week, after thesupervisor had reviewed the session tapes from the previous week. Thetreatment was provided by the first author twice weekly for the first sixweeks, and once weekly for the remaining eleven weeks, for a total of 23sessions for Mark, and 23 sessions for Melissa. The sessions were 40minutes each. There were some weekly sessions missed in Mark'streatment, due to his opportunities to participate in field trips and specialevents. Missed sessions were made up by adding weekly sessions toequal the number missed.
DataThe data fall into three sets: qualities of client changes observed
in session, quantified observations of client changes outside sessions, andqualities of change observed outside sessions. Qualities of change insessions were defined through reviewing video recordings of sessions,discussing, and reaching consensus on change definitions. In definingand judging the data, the authors used their expertise in the areas ofCCPT, CCPT supervision, CCPT work experience with children andadults with developmental disabilities, general research methods, surveyand qualitative research.

52 Demanchick, Cochran, & Cochran
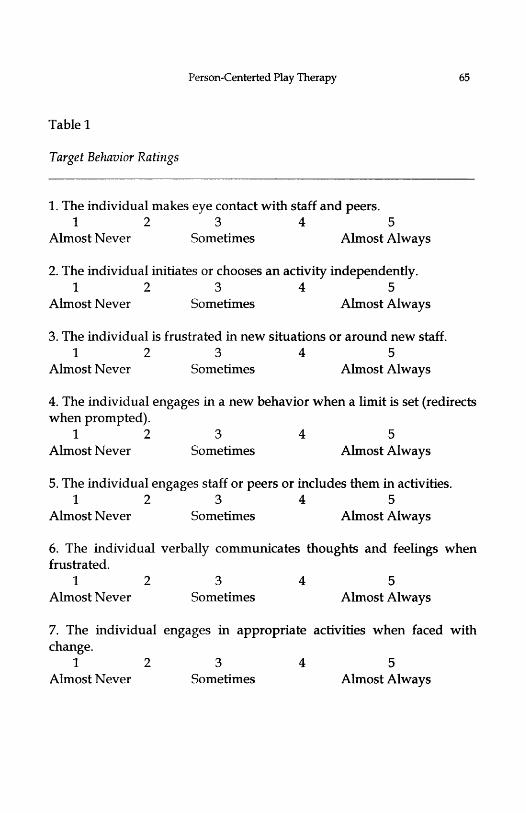
Quantified observations of participant changes outside sessionswere collected from participants' Me skills managers whose knowledgeof participant behavior stemmed from their training and expertise, aswell as daily observations of the participants and their peers duringgroup day treatment activities. Mark's life skills manager changed in theninth week of treatment, when Mark was moved to a different daytreatment group for reasons unrelated to treatment. For the quantifiedobservations, the first author established seven target behaviorsmeasuring potential change during treatment, in consultation with eachparticipant's day program treatment providers (day program managers,behavior specialists, recreational therapists, and life skills managers).Behavior ratings of these target behaviors were recorded on a five pointLikert scale. The target behaviors tend to emphasize such areas ofprogress as reduction of self injurious behavior resulting fromfrustration, expression of needs in appropriate ways instead of havingemotional outbursts, moving smoothly through transitions in groupactivities, and other evidences of improved independence and overallemotional well-being. The target behaviors were rated by eachparticipant's life skills manager twice monthly. The items for ratingtarget behaviors are listed in Table 1.
Qualities of participant changes outside sessions were observedby each participant's day program treatment providers. The first authorinterviewed this group prior to treatment, at mid point in treatment, andjust after the conclusion of treatment, in order to gather their impressionsof changes, progress, or difficulties being experienced by the participantsthat may have been related to treatment. Consistent with qualitativeresearch methodology, the questioning was open-ended and semi-structured. McCracken (1988) described this format as having specificquestions or sub-topics to be covered, but covering the topics bybeginning with a broad opening question, and then eliciting moreinformation with the use of "floating prompts". An example of anopening question would be, "Tell me how Mark may have changed sincewe last met." "Floating prompts" refer to such actions as asking the staffto elaborate vague suggestions of change, to give specifics when onlygeneral change is described, or to define the general quality of changewhen only specific examples are given. This questioning formatachieved a balance that controlled the content and flow of the
Person-Centerted Play Therapy 53
information in interviews, yet allowed the interviewees to respond intheir own words.
RESULTS
Qualities of Change Within SessionsBeginning treatment - changes observed within sessions 1-6.
Qualities of change within sessions as well as within the relationshipbetween therapist and client were noticeable from the beginning stagesof PCPT. Noticeable qualities of change for both Mark and Melissaincluded a quick development of rapport with and trust of the therapist,and physical changes indicating more relaxation and sense of ease andcomfort. Both Mark and Melissa began in therapy (sessions 1-3) withfairly typical expressions indicating anxiety and tentativeness (rigidposture, little eye contact, and nervous habits like staring off in anopposite direction and intense repetitive rocking). During the first twosessions, both Mark and Melissa showed little interest in the toys, andresponse to the therapist was tentative. The therapist was careful toexpress warmth and interest through his facial expressions, bodyposture, and tone of voice, and in no way attempt to direct the sessions.The therapist was also careful to attend to even the smallest nuances ofcommunication from Mark and Melissa while offering a safe space wherethey were encouraged to try out their own impulses and make their owndecisions. With each new session (sessions 3-6) both Mark and Melissashowed small signs of increased ease and comfort, and of a developingsense of trust and rapport. For instance, both began exploring the roomand toys visually first, and then by slowly touching, and briefly pickingup different toys. Both clients continued to increase eye contact, andthere was a marked decrease in rigid, anxious posture (arms held stifflyat sides) and anxious behaviors such as staring off and mouthing words(Mark) and intense repetitive rocking (Melissa).
Of particular interest and surprise to staff were the initialreactions to the therapist by both Mark and Melissa who ordinarily haddifficulties with new people and situations. For example, staff hadpredicted that Melissa would likely last in session for no more than 20minutes in the session without acting out or engaging in self-injuriousbehavior. During her initial and all subsequent sessions, however,Melissa chose to stay with the therapist for the full forty minutes. She

54 Demanchick, Cochran, & Cochran
never showed self-injurious behavior during any of her PCPT sessions.After the initial PCPT session, both Mark and Melissa approached thetherapist readily, with interest, and without need for staff assistance ofany sort. Mark showed an enthusiasm and readiness to go to his thirdPCPT session by joyfully hugging the therapist upon being picked up togo to the therapy room. Melissa increased eye contact with the therapist,and walked closer to the therapist on the way to the therapy room.
Both clients became initially interested in toys of preferencewithin the first 6 sessions, and made some verbalizations, and attemptsto reach out to the therapist. For example, Mark would often repeatwords and phrases that the therapist had said. While doing this, Markwould also quickly reach out and touch the therapist's arm. While therepetition of words was due in part to Marks' echolalia (repetition of lastwords spoken by another), with each session he seemed to want to let thetherapist know that he was listening, and was aware of the therapyprocess. While this repetition of words initially seemed a nervousresponse, it became more of a way for Mark to look expectantly towardthe therapist, engage in eye contact, and share a "knowing" interchange.Because the therapist used tracking statements (stating Mark's actionsout loud) to show warmth, empathy, and acceptance of Marks' decisionsand actions, this repetition, and ability to repeat some of what thetherapist had said became playful in quality. Mark seemed to enjoy thesense of acknowledgment and acceptance for just being himself, as wellas the comfort of tracking statements that the therapist used to, in a senseconvey, "I'm right here with you, buddy, and I prize you."
Mid-treatment - changes observed within sessions 7 -15.Within sessions 7-15 much better eye contact, relaxed posture, and self-directedness occurred. There was an observed reduction in self-stimulatory behaviors. For example, Melissa's repetitive rocking reducedin frequency and intensity, and she began spending more time playingwith toys of preference (toy foods, art supplies, toy phones). Mark'secholalia decreased, and he turned his face and full attention increasinglytoward the therapist, often smiling and reaching out to touch him. BothMark and Melissa walked into the therapy room confidently, andbecame immediately self-directed in choosing toys and activities. Markappeared to be more animated, relaxed, and happy. He especiallyenjoyed the play telephones that made musical sounds, and a stuffed toythat spoke in three predictable, sequenced sentences when thrown down
Person-Centerted Play Therapy 55
three times. Mark used these toys to engage the therapist, and seemed toderive great pleasure in the predictability of the last sentence, "How doyou do it?" that would result from the third toss of the stuffed toy. Eachtime he heard this phrase, this brought on shared expressions of laughterand joy with the therapist. While Mark's play was highly repetitive, heseemed to derive great joy in choosing the same toys (toy phones andstuffed toy) and engaging in the same pattern of interactive playfulnesswith the therapist. Melissa showed and seemed to enjoy more symbolicplay (cooking and making plates of toy food) and free, independentdrawing with provided mediums. Her sessions also involvedintermittent times between play activities when she would put her headdown, and at times suck her thumb or sing softly to herself. Duringthumb sucking, the therapist noted that it often seemed as if she wereplaying a peek-a-boo type game with him by looking at him, smiling,and looking away.
Ending Sessions - Changes Observed Within Sessions 15-23.During the last 15-23 sessions, Mark and Melissa continued to exhibitrelaxed posture, steady eye contact, spontaneity, and playfulness in theirindividual PCPT sessions. They made independent choices regardingplay materials and activities, and found unique ways to engage thetherapist. Mark would engage the therapist by playing a familiar game(tossing his favorite stuffed toy, and laughing joyously with thetherapist), lining up and naming out loud types of toy foods, andbanging loudly on the table and laughing, while directing the therapist tojoin in by picking up the therapist's hand and dropping it. Melissa oftensang loudly in session, and whereas she previously had not movedaround the room, she began to leave her seat and walk around. Shewould at times get up and begin jumping up and down while laughingand singing.
The therapy sessions with Mark and Melissa differed in the needfor therapeutic limit setting. During PCPT sessions, the therapistfollowed the NIRE CCPT model of therapeutic limit setting. In CCPT,limit setting allows the child and therapist to remain physically safeduring the play sessions. While the therapist shows acceptance of thedesire or determination to cross the limit, the responsibility to control theimpulse to hurt self or others (or purposely destroy materials) is given tothe child. This allows the child to experience greater control and a senseof self-efficacy. An important component of the limit setting procedure in
56 Demanchick, Cochran, & Cochran
CCPT is that the therapist never sets limits ahead of time, but only whennecessary. When limits are needed, the therapist pairs them withempathy, and always enforces them by first stating and accepting theclient's desire to engage in the act that crosses a limit. Mark neverengaged in behaviors that required the therapist to set a limit. Melissa,however, engaged in behaviors that required limit setting such asattempting to eat paints, to put toy food in her mouth, and to turn on thefaucet and play with hot water. The therapist showed acceptance forMelissa's desire to do these activities, and set these limits with empathy.Melissa accepted these limits, stopped or adjusted the behavior, andexperienced acceptance for the desire and determination to act or do thisparticular behavior. The therapist also accepted Melissa's resultingfrustration or irritation with empathy. For example the therapist noticedthat when a limit was set, Melissa would sometimes put her head downand turn from him. To acknowledge and accept this, the therapist wouldrespond, "you really wanted to put the toy grapes in your mouth...that'show you want to play...you'll just put your head down and stopplaying...that's what you'll do." We believe that Melissa often repeatedthe testing of some limits as her unique way to engage the therapist andrelate to him. For example, after the initial limit was set about putting toyfood in her mouth, Melissa continued in future sessions to put the toyfood almost in her mouth. She would place the toy food near her mouth,look at the therapist, and then smile or laugh.
During the last nine sessions, Mark and Melissa were madeaware that a countdown phase of therapy was occurring. The therapistreminded each client at the beginning of the session, and at the end of thesession of the number of sessions left until he would be saying good-byeto them. Both clients indicated an understanding of saying, "good-bye"to the therapist. During his last three sessions, Mark would linger nearthe end of his special play time, and would seem to want to stay longerby remaining seated. He would listen intently with a sad expressionwhen the therapist would let him know how many sessions were left.Melissa revisited some limit testing behaviors in more of an engagingmanner, than a limit testing manner. She would sometimes place theother toys near her mouth, but refrain from actually putting them inwhile smiling at the therapist. This was done in a playful manner, andseemed to communicate to the therapist, "remember when I did this?"Interestingly, Melissa also seemed, at times, to use limit testing to

Person-Centerted Play Therapy 57
communicate a disagreement with, or dislike of the sessions coming to anend. For instance, during the last five sessions, when told by the therapistthat she had "five minutes (or one minute) left of special play time,"Melissa would often immediately start testing the limit of playing withthe hot water faucet.
During the third to last session, Melissa sang out in a sad tone,"goooood-byyyye" in response to the therapist saying to her that therewere three sessions left. During the final sessions, Melissa also began tomove in very close to the therapist, as if to study his face intently. Duringthe final session, Melissa stood up, walked over, and began leaningagainst the therapist. This had never happened before in sessions. Thetherapist accepted this, and acknowledged her need to be near him.Because of her size, however, the therapist had to limit her leaning, sothat she could remain close to him, but also lean on the therapist's chairfor support. The intention was clear that Melissa wanted to be physicallyclose to the therapist.
Behavior Ratings Observed in Day Treatment ProgramFor both Mark and Melissa, there were areas of change, and
sometimes lack of change, that will be useful to consider in discussion.The rating scale for each behavior ranged from one, indicating "almostnever," to five, indicating "almost always." Regarding the behavior ofverbally communicating thoughts and feelings when frustrated, Mark'srating was never improved beyond one. However, Melissa's ratingimproved from one to two during the first month of treatment, then fromtwo to four during the final two weeks of treatment.
In the areas of managing frustration and change, there wereseveral noteworthy changes in Mark's ratings. Regarding engaging inappropriate activities when frustrated and prompted by caregiver,Mark's ratings improved from one, during the early weeks of treatmentto five, during the late weeks. Similarly, regarding his engaging inappropriate activities, when faced with change, Mark's ratings improvedfrom a steady two, during the first half of treatment, to a steady climb tofive, during the second half of treatment. Similarly, regarding hisgeneral frustration with new situations and staff, his ratings improvedfrom four, early in treatment, to two, later in treatment. Regardingchoosing alternative behaviors, instead of yelling or engaging inoutbursts when frustrated, his ratings dropped from two at the
58 Demanchick, Cochran, & Cochran
beginning of treatment, to one, during a mid-treatment week, thenimproved to a steady four, during the last three weeks of treatment.
Regarding initiating activities independently, Mark's ratingsimproved from one, at beginning of treatment, to three, consistent mostweeks of treatment through the end. Neither Mark's nor Melissa'sratings regarding making eye contact with staff and peers improvedmore than one point throughout treatment. Regarding items notnarrated above, there was no change in ratings.
Qualities of Change Observed in Day Treatment ProgramStaff observed changes in both Mark's and Melissa's behaviors
outside of the play therapy sessions. Mark's life skills assistant reportedthat his "playful spirit" returned. She characterized Mark as morerelaxed, fun, and happy. She reflected on his renewed smile and calmnature. Mark also reportedly showed changes in being more cooperativeduring exercise taken with his walking group. His occupational therapistnoted that he became more self-directed and self-reliant. During the lastfew weeks of play therapy, Mark prepared himself for walking groupmore quickly. He began to choose to change his shirt, gather his things,and be on time without dawdling or need for staff reminders andassistance.
Melissa experienced an increase in self-expression. During a busride to day treatment, she told the driver that she had an upset stomach.Although Melissa has the ability to communicate verbally, she rarely did.Her ability to communicate this information was a first for Melissa. Shealso began to use more two-word phrases. Staff also noted that she beganto ask for help with unit activities. As her verbal communicationincreased in sessions, so did her verbal communication outside of thesessions.
Outside of the sessions, Melissa and Mark initially experiencedsome difficulty adjusting to the transition back to class after the sessions.Behaviors included agitation, sleeping, lack of motivation and some SIB.Reports from staff concluded that these transition problems rapidlydecreased over time to the point that any acting out behavior could be re-directed within five minutes. Mark experienced marked improvement inmood after sessions. He was characterized as being happy and pleasant.Mark began to have an easier time with day treatment activities, oftentaking pride in his work, according to day treatment staff.
Person-Centerted Play Therapy 59
The authors noted that each client began to anticipate and planfor sessions. For example, one morning the therapist went to Melissa'sclass to change the time of her session. Melissa saw him and mistakenlyassumed that her therapist had come to get her, but then changed hismind and left the room. Upon returning to the room at the later time, hefound Melissa acting out and engaged in tearing up paper. Staffcommented that she had become very upset when she was not picked upfor therapy. When the therapist asked Melissa if she was ready andwould like to go, she stood up, smiled, and left. She immediatelydisengaged from all acting out behavior.
DISCUSSION
Although cognitively and developmentally deficient, these twoindividuals experienced growth during a series of sessions in which thecore conditions of empathy, genuineness and unconditional positiveregard were present. These two adults with developmental disabilitiesflourished when given the opportunity to experience Person-CenteredPlay Therapy. Mark and Melissa were able to experience greaterautonomy, environmental and self-control, confidence and self-expression.
As noted earlier, Day Treatment Specialists regarded verbalexpression of thoughts and feeling as an important goal for bothindividuals. Although some verbal ability was tracked and noted, theseindividuals may not possess the cognitive ability to express themselvesfully in that way. However, self-expression often materialized otherways, through facial expressions, increased playfulness, independentchoice, drawing, laughing, singing, and self-direction. An importantobservation is that expression may be very subtle at times with thispopulation. It was beneficial and necessary for the therapist to meetMark at his own level, and Melissa at her own level. This means that thetherapist accepted and recognized the individual abilities and modes ofcommunication that Mark and Melissa naturally brought to the session.This was done, not to draw attention to possible cognitive deficiency, butto allow them the opportunity to feel safe, trusted, in-control, andaccepted.
It may be summarized that for these particular individuals"negative" emotions are present but the various outlets for these

60 Demanchick, Cochran, & Cochran
emotions are inhibited. The use of the PCPT approach supplied onepossible outlet for these individuals to feel in control, accepted, valuedand worthwhile. While their needs may not be verbally expressed, thistherapy allows them to experience fulfillment and expression of theseinherent human needs. The authors believe that in an atmosphere wherethe core conditions (Rogers, 1957) are present, these individuals did nothave to rely on acting out behavior to feel noticed and understood.
The therapist's attitude during session was critical in the successof this project. We believe that the therapist's genuineness, acceptance,and unconditional positive regard towards these clients helped tofacilitate an atmosphere in which they could feel safe, comfortable,worthwhile, and trusted. Thus, they quickly came to trust their therapistand participate freely in PCPT sessions. Contrary to the expectations ofthe day treatment staff, both Mark and Melissa were able to accomplishthis transition and adjustment to change, and to someone new, withoutextreme distress and acting out.
The PCPT model allowed the therapist to facilitate each client'sself-directedness, autonomy and sense of self. For adults withdevelopmental disabilities, the vast majority of their day is controlled sothat their safety and well-being can be effectively managed. Duringtherapy, control and a sense of self-efficacy was shifted to Mark andMelissa. Each client had the opportunity to decide and choose what toplay with, in which manner they would like to communicate or notcommunicate, and at what points to take a break. The therapist's rolewas not to direct, but to be with both clients on their level, at their ownpace, and to notice and respond to the unique and individual forms ofcommunication present in his relationship with them. It is importantwhen counseling non-verbal clients or clients with limited verbal abilitythat the therapist be aware of the various forms of communication.Through CCPT with children, and the adapted PCPT with adults such asMark and Melissa, clients may become free to explore all the possibleways of relating and communicating.
The authors were interested in Mark's and Melissa's initialdifficulty in transitioning back to their units. As the difficulty decreased,it appeared as if the rest of their days were getting better. This initialdifficulty is attributed to the fact that they had begun to experienceincreased self-direction, independent choice, empathy, and acceptance oftheir choices. Through the PCPT model, individuals become empowered,
Person-Centerted Play Therapy 61
confident and autonomous. It was suspected that they might declineparticipation in activities that they had not chosen. As the therapycontinued, however, both individuals were able to adapt to transitionsmore quickly, and exert greater levels of self-control.
Some of the changes described in this article seem quitesignificant. However, the term significant is defined as havingsignificant importance to the clients, their caregivers, and loved ones.Statistical significance or generalizations are not concluded from the twocase studies. Further, having studied the possible benefits of PCPT foronly two persons in a non-empirical design does not provide certaintythat progress made by Mark and Melissa is attributed to theirexperiences in PCPT.
Suggestions for Further Study and ApplicationA larger sample would prove more effective in determining
possible meanings and generalizations from this work. Additionally, theauthors experienced difficulty receiving qualitative and quantitative dataon time and completed. In future work, it may be helpful to train staff onqualities of change that might be expected from therapy. For example,qualities might include increased autonomy, self-direction, self-expression, and self-confidence. It would be helpful to train staff on howto notice eye contact, and more subtle forms of verbal and non-verbalcommunication. Additionally, in this study, staff were presented with allthe materials at the beginning of the study. In future work, it would behelpful to collect measures, record comments, answer questions, anddispense new forms weekly so that staff would not have to beresponsible for keeping an entire volume of records. This would reduceany materials that may become lost, misplaced or forgotten.
Considerations for future study and application of this PCPTmodel might include using PCPT with adults with developmentaldisabilities that are more verbal, and have overall higher functioninglevels than the clients in this study. The clients in this study were largelynon-verbal, and had cognitive and adaptive functioning levels thatmeasure in the 2-6 year old range. A larger sample of the populationmight include adults with developmental disabilities whose cognitiveand adaptive functioning levels measure more consistently in the 6-13year old range.

62 Demanchick, Cochran, & Cochran
In addition, further applications of this study might includeusing the results to help in trainings for day treatment providers. Forthose who work with, and wish to enhance communication andrelationships with adults with developmental disabilities, the basic tenetsof a person-centered approach may prove to be beneficial for allconcerned. Through the core conditions of empathy, genuineness, andunconditional positive regard, progress and emotional growth may bepossible for persons previously underserved by counseling andpsychotherapy.

Person-Centerted Play Therapy 63
REFERENCES
Axline, V. (1969) Play therapy (Rev. ed.). Cambridge, MA: RiversidePress.
Davis, K.R. & Shapiro, L.J. (1983) Exploring group process as a means ofreaching the mentally retarded. In L. Wikler & M.P. Keenan(Eds.), Developmental disabilities: No longer a private tragedy(pp.147-154). Silver Spring, MD: National Association of SocialWorkers.
Desnoyers-Hurley, A. & Hurley, F.J. (1987). Psychotherapy andcounseling II: Establishing a therapeutic relationship. PsychiatricAspects of Mental Retardation Reviews, 4(4), 15-20.
Guerney, L. (1983). Client-centered (nondirective) play therapy. In C. E.Schaefer & K.J. O'Connor (Eds.), Handbook of play therapy (pp. 21-64). NY: John Wiley & Sons.
Guerney, L. (2001). Child-centered play therapy. International Journal ofPlay Therapy, 10(2), 13-31.
Jacobson, J.W., & Mulick, J.A. (Eds.). (1996). Manual of diagnosis andprofessional practice in mental retardation. Washington, DC:American Psychological Association.
Kielhofner, G. & Miyake, S. (1981). The therapeutic use of games withmentally retarded adults. The American Journal of OccupationalTherapy, 35(6), 375-382.
Landreth, G. (2002). Play therapy: The art of the relationship (2nd ed.). NewYork: Brunner-Routledge.
McCracken, G. (1988). The long interview. Newbury Park, CA: SagePublications.
Morrison, T.L. & Newcomer, B.L. (1975). Effects of directive vs. non-directive play therapy with institutionalized mentally retardedchildren. American Journal of Mental Deficiency, 79(6), 666-669.
Moustakas, C. (1953). Children in play therapy. NY: Ballantine Books.Nordling, W. & Cochran, N. H. (1999, April). Child-centered play therapy.
Workshop series sponsored by the National Institute forRelationship Enhancement (NIRE), Savannah, GA.
Portner, M. (2001). The person-centered approach in working withpeople with special needs. Person-Centered Practice, 9(1), 18-30.
Rogers, C. (1957). The necessary and sufficient conditions of therapeuticpersonality change. Journal of Counseling Psychology, 21(2), 95-103.

64 Demanchick, Cochran, & Cochran
Walker, P.W. (1983) The developmentally disabled: A social workchallenge. In L. Wikler & M.P. Keenan (Eds.), DevelopmentalDisabilities: No longer a private tragedy (pp.55-61). Silver Spring,MD: National Association of Social Workers.
Person-Centerted Play Therapy 65
Table 1
Target Behavior Ratings
1. The individual makes eye contact with staff and peers.1 2 3 4 5
Almost Never Sometimes Almost Always
2. The individual initiates or chooses an activity independently.1 2 3 4 5
Almost Never Sometimes Almost Always
3. The individual is frustrated in new situations or around new staff.1 2 3 4 5
Almost Never Sometimes Almost Always
4. The individual engages in a new behavior when a limit is set (redirectswhen prompted).
1 2 3 4 5Almost Never Sometimes Almost Always
5. The individual engages staff or peers or includes them in activities.1 2 3 4 5
Almost Never Sometimes Almost Always
6. The individual verbally communicates thoughts and feelings whenfrustrated.
1 2 3 4 5Almost Never Sometimes Almost Always
7. The individual engages in appropriate activities when faced withchange.
1 2 3 4 5Almost Never Sometimes Almost Always
Related Documents











