Persistent Atrial Standstill—Clinical, Electrophysiological, and Morphological Study K.K. TALWAR, V. DEV, P. CHOPRA, T.H. DAVE, and S. RADHAKRISHNAN From the Department of Cardiology. Cardiothoracic Centre. All India Institute of Medical Sciences. New Delhi, India TALWAR, K.K., ET AL.: Persistent Atrial Standstill—Clinical, Electrophysiological, and Morphological Study. Persistent atrial standstiJJ (PAS) is a rare disorder characterized by absence of alrial activity on the surface and intracavity electrograms, absence of atrial mechanical activity, and inabi/i(y to electri- cally stimuJale (he atria. Four patients (ages 18-60 years) with PAS were evaJuated. One of these (no. 3} only had right atrial (RAJ standstill, whereas left atrium (LA) showed spontaneous activity and could be stimulated eJectricaily. As RA biapsy is not possible, right ventricular (flV) endomyocardiaJ biopsy (EMB) was obtained to identify possible atrial pathology that revealed in/lanima(ory myocarditis, 2; amyloidosis. 1; and myocardial hypertrophy with fibrosis, 1. Three patients were given permanent pace- makers. One of these with amyloidosis died suddenly. One is lost to follow-up. The others cases are persisting with PAS. (PACE, Vol. 14, August 1991) persistent atrial standstill, intracavity electrograms Introduction Persistent atrial standstill (PAS) is a rare dis- order characterized by absence of atrial activity on tbe surface and intracavity electrograms. absence of atrial mechanical activity, and inability to elec- trically stimulate tbe atria. This appears to be an arrhythmia that develops because of extensive dis- ruption of the atrial myocardium. After the initial report by Chavez et al.,' nearly 100 such patients bave been described.^"" The PAS has been iden- tified to occur in three clinical settings: (1) long- standing progressive cardiac disease; (2) patients with neuromuscular diseases; and (3) isolated PAS without identifiable disease of the rest of the heart or any systemic disease. We describe here in clinical, bemodynamic, and electropbysiolog- ical data of four patients of this entity along with tbeir myocardial histology obtained by endomy- ocardial biopsy [EMB). Tbe long-term follow-up is presented. Address for reprints: K.K. Talwar, D.M., Department of Car- diology, Cardiolhoracic Centre, All India Institute of Mediual Sciences, Ansari Nagar. New Delhi-110029, India. Received |anuary 22, 1991; revision April 18, 1991; accepted April 28, 1991. Material and Methods Over the last 3 years we bave encountered four patients witb PAS. One of them (case 1) has been reported by us earlier.^ Tboy were all sub- jected to a detailed physical examination and in- vestigations including a 12-lead electrocardi- ogram (ECG), cross-sectional and Doppler echo- cardiograpby. detailed rigbt and left heart catheterization, angiocardiography, detailed elec- trophysioiogical study, and EMB, Echocardiog- raphy was performed on an ATL ultramark-8 ma- chine (Advanced Technology Laboratories, Botb- ell, WA, USA) with combined Doppler and cross- sectional studies. Cardiac catbeterization was per- formed in fasting, supine, resting state after an in- formed consent. Right and left heart pressures were measured using fluid filled transducer sys- tem and recorded on Mingograph 8 (Siemens- Elema, Solna. Sweden). Left ventricular (LV) an- giograms were done in all. In one patient (with suspected endomyocardial fibrosis lEMF]) a right ventricular (RV) cineangiogram was also per- formed. EMB was performed using a Cordis biop- tome (Cordis Corp.. Miami, FL. USA) introduced into the RV from the femora! vein using a long sheatb. On an average 3-5 pieces of tissue from 1274 August 1991 PACE, Vol. 14

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Persistent Atrial Standstill—Clinical,Electrophysiological, and Morphological Study
K.K. TALWAR, V. DEV, P. CHOPRA, T.H. DAVE, and S. RADHAKRISHNAN
From the Department of Cardiology. Cardiothoracic Centre. All India Institute of MedicalSciences. New Delhi, India
TALWAR, K.K., ET AL.: Persistent Atrial Standstill—Clinical, Electrophysiological, and MorphologicalStudy. Persistent atrial standstiJJ (PAS) is a rare disorder characterized by absence of alrial activity onthe surface and intracavity electrograms, absence of atrial mechanical activity, and inabi/i(y to electri-cally stimuJale (he atria. Four patients (ages 18-60 years) with PAS were evaJuated. One of these (no.3} only had right atrial (RAJ standstill, whereas left atrium (LA) showed spontaneous activity and couldbe stimulated eJectricaily. As RA biapsy is not possible, right ventricular (flV) endomyocardiaJ biopsy(EMB) was obtained to identify possible atrial pathology that revealed in/lanima(ory myocarditis, 2;amyloidosis. 1; and myocardial hypertrophy with fibrosis, 1. Three patients were given permanent pace-makers. One of these with amyloidosis died suddenly. One is lost to follow-up. The others cases arepersisting with PAS. (PACE, Vol. 14, August 1991)
persistent atrial standstill, intracavity electrograms
Introduction
Persistent atrial standstill (PAS) is a rare dis-order characterized by absence of atrial activity ontbe surface and intracavity electrograms. absenceof atrial mechanical activity, and inability to elec-trically stimulate tbe atria. This appears to be anarrhythmia that develops because of extensive dis-ruption of the atrial myocardium. After the initialreport by Chavez et al.,' nearly 100 such patientsbave been described.^"" The PAS has been iden-tified to occur in three clinical settings: (1) long-standing progressive cardiac disease; (2) patientswith neuromuscular diseases; and (3) isolatedPAS without identifiable disease of the rest of theheart or any systemic disease. We describe herein clinical, bemodynamic, and electropbysiolog-ical data of four patients of this entity along withtbeir myocardial histology obtained by endomy-ocardial biopsy [EMB). Tbe long-term follow-upis presented.
Address for reprints: K.K. Talwar, D.M., Department of Car-diology, Cardiolhoracic Centre, All India Institute of MediualSciences, Ansari Nagar. New Delhi-110029, India.Received |anuary 22, 1991; revision April 18, 1991; acceptedApril 28, 1991.
Material and Methods
Over the last 3 years we bave encounteredfour patients witb PAS. One of them (case 1) hasbeen reported by us earlier.^ Tboy were all sub-jected to a detailed physical examination and in-vestigations including a 12-lead electrocardi-ogram (ECG), cross-sectional and Doppler echo-cardiograpby. detailed rigbt and left heartcatheterization, angiocardiography, detailed elec-trophysioiogical study, and EMB, Echocardiog-raphy was performed on an ATL ultramark-8 ma-chine (Advanced Technology Laboratories, Botb-ell, WA, USA) with combined Doppler and cross-sectional studies. Cardiac catbeterization was per-formed in fasting, supine, resting state after an in-formed consent. Right and left heart pressureswere measured using fluid filled transducer sys-tem and recorded on Mingograph 8 (Siemens-Elema, Solna. Sweden). Left ventricular (LV) an-giograms were done in all. In one patient (withsuspected endomyocardial fibrosis lEMF]) a rightventricular (RV) cineangiogram was also per-formed. EMB was performed using a Cordis biop-tome (Cordis Corp.. Miami, FL. USA) introducedinto the RV from the femora! vein using a longsheatb. On an average 3-5 pieces of tissue from
1274 August 1991 PACE, Vol. 14
ATRIAL STANDSTILL
the right side of the ventricular septum were takenand were sent for histopathological examination.Hematoxylin eosin stain was used for the paraffinsections (4-5 \x. thick slices) and in one patientwith suspected amyloid congo red staining wasused. The electrophysiology study was performedby introducing electrode catheters through thefemoral vein and placing one at RV apex, one forHis-bundle recording (HBE), and the third, a quad-ripolar catheter in the right atrium (RA) for pacingand recording purposes. The same catheter wasmanipulated into coronary sinus for recording andpacing left atrium. Intraatrial recordings weretaken from multiple sites in RA and in two pa-tients from the coronary sinus. In two patients cor-onary sinus could not he entered hecause of mark-edly dilated RA. In them, a lubricated bipolar per-manent pacing electrode was introduced into theesophagus from the nose for recording left atrial(LA) activity. Pacing was performed from multiplesites with increasing current strength up to a max-imum of 25 mA using a programmed stimulator(Medtronics-5325; Medtronic, Inc., Minneapolis.MN, USA).
Case Reports
Case One
This patient has been reported earlier^ andonly a brief description is included here.
S.K., an 18-year-oId boy presented with oneepisode of syncope a week prior to admission. Ex-amination revealed cardiomegaly and a LV thirdheart sound. Electrocardiogram revealed a narrowQRS tachycardia (166/min) with absent P waves.A bolus of verapamii (10 mg intravenously] pro-duced no benefit. Following direct current (DC)cardioversion the rhythm reverted to a slow junc-tional escape at a rate of 45/minute. No P waveswere seen. His bundle showed presence of junc-tional rhythm with a preceding bundle of His ac-tivity and prolonged HV interval (90 msec). Noatrial activity was seen. Attempts at stimulatingthe RA from various sites were unsuccessful withstimuli up to 25 mA. RV EMB was obtained. Thisrevealed the presence of focal lymphocytic infil-trates. A diagnosis of myocarditis was made andthe patient was treated with immunosuppressivetherapy (azathioprine 2 mg/kg per day and pred-
nisolone 1.25 mg/kg per day). In the next 1 week,the patient showed few episodes of airial flutterwith varying block and one episode of sinusrhythm. But after this his ECC showed PAS. Inview of symptomatic severe hradycardia a per-manent multiprogrammable pacemaker was im-planted. Immunosuppressive therapy wasstopped after 3 months. Up to a follow-up of 48months now, the patient still continues to have noatrial activity on surface electrogram.
Case Two
M.P., a 25-year-old male presented with re-current episodes of syncope in tho preceding 4years. At admission he was detected to have a slowpulse rate (30/min) and an ejection systolic mur-mur (grade III/VI) at the left sternal border. TheECC showed slow junctional rhythm (rate 30/min)with right bundle branch block. There was noatrial activity. Chest skiagram and echocardio-gram were normal. Cardiac catheterization re-vealed normal hemodynamic data. Fluoroscopyshowed lack of atrial contractility. At electrophy-siology study, no left or right atrial activity couldbe recorded. The infranodal conduction (HV) wasnormal—^45 msec. Atrial pacing with stimuli upto 25 mA failed to stimulate either the right or leftatria. RV EMB was performed. This showed onlya mild myocellular hypertrophy (Figs. lA and lB)and focal aggregate of lymphomononuclear cellsaround myofibers and focal fibrocollagen thick-ening of endocardium—features consistent withmild focal myocarditis. A permanent pacemakerImplantation was done. The patient has continuedto remain in atrial standstill over a follow-up of1V2 years and has no cardiomegaly or congestiveheart failure (CHF).
Case Three
D.R., an 18-year-old male presented with pro-gressive dyspnea, pedal edema, abdominal dis-tension, and slow heart rate of 1-year duration. Onexamination he was found to have gross CHF anda systolic murmur of tricuspid regurgitation. TheECC revealed a slow junctional rhythm (rate of 54/min) with absent P waves. Intravenous atropineincreased the rate of junctional focus to 64/minutewithout any apparent atrial activity on the ECG.Cross-sectional echocardiography showed normal
PACE, Vol. 14 August 1991 1275
TALWAR. ET AL.
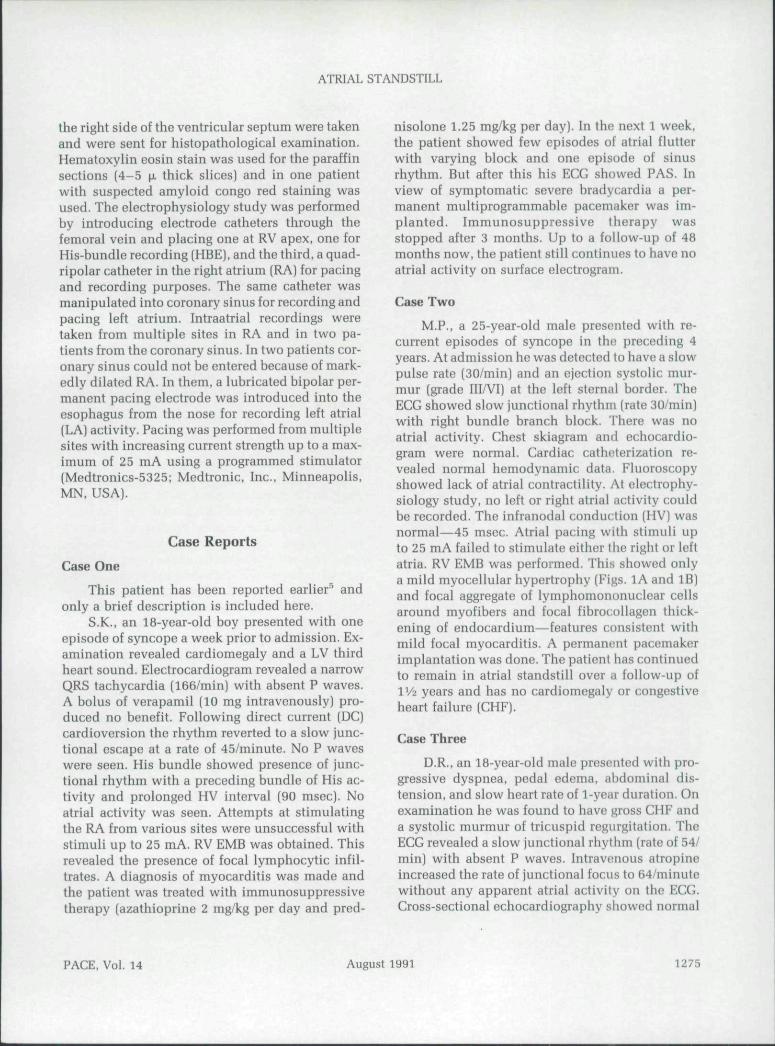
Figure IA. EMB to show mild hypertro/ifiy of (he my-ofibers and focal aggregate of lymphomononuciearceJJs farrowj around myofibers. G and E x 250.
Figure IB. Photomicrograph of EMB to illustrate focal/ibrocoliagen thickening of the endocardium. H and EX 250.
Figure lC. Fhnloiiiicrogmpii of EMB shows fidema of(h(! inlerstifium ivith stray IymphGrnononuciearcei/.s mthe intersfitium. The endocardium is withm r\ormallimits. HematoxyJin and eosin (H &• E) x lOO.
Figure ID. Photomicrograph of EMB shows extensivedeposition of homogenous material around the myofi-bers seen as light gray in the picture (arroivsj. The my-ofiber which are dark in color are otrophic. The mo-terial was characterized as amyJoid by special stains.H and E x 250.
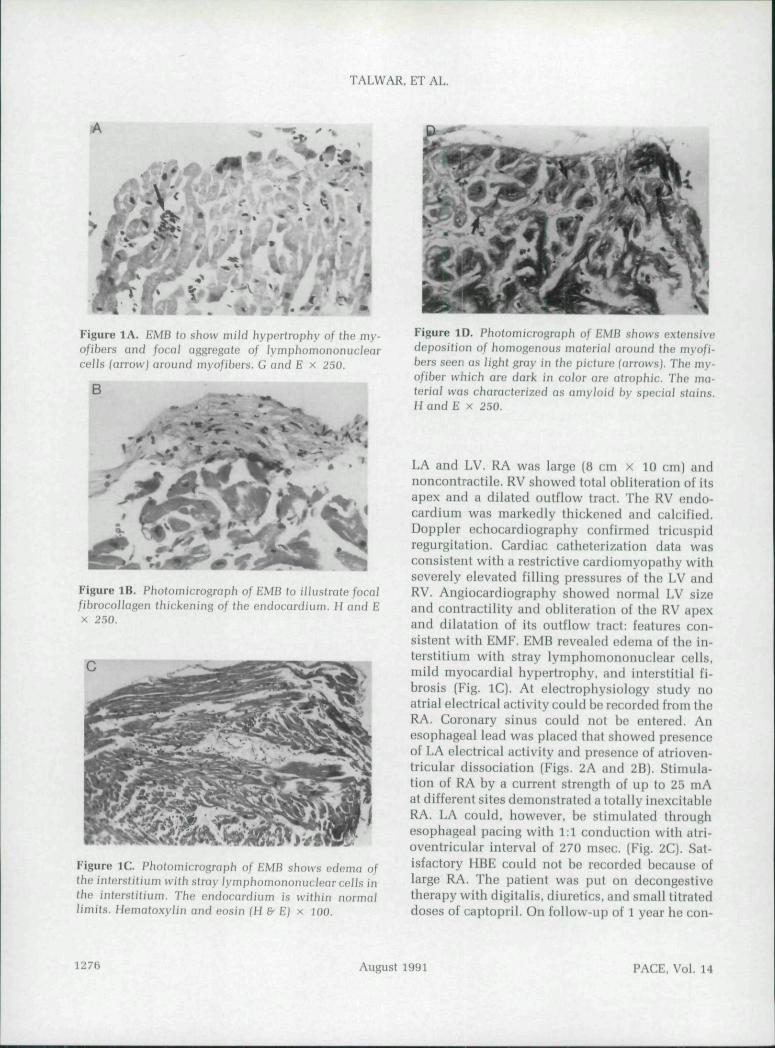
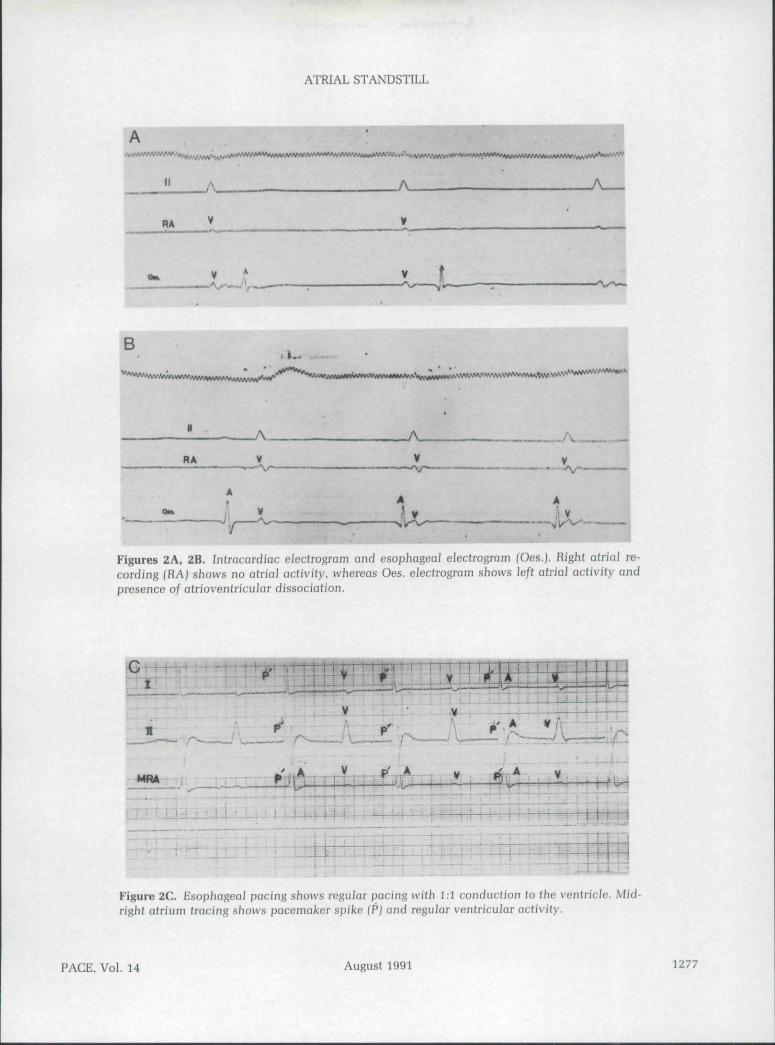
LA and LV. RA was large (B cm x 10 cm) andnoncontractile. RV showed total obliteration of itsapex and a dilated outflow tract. The RV endo-cardium was markedly thickened and calcified.Doppler echocardiography confirmed tricuspidregurgitation. Cardiac catheterization data wasconsistent with a restrictive cardiomyopathy withseverely elevated filling pressures of the LV andRV. Angiocardiography showed normal LV sizeand contractility and obliteration of the RV apexand dilatation of its outflow tract: features con-sistent with EMF. EMB revealed edema of the in-terstitium with stray lymphomononuclear cells,mild myocardial hypertrophy, and interstitial fi-brosis (Fig. lC). At electrophysiology study noatrial electrical activity could be recorded from theRA. Coronary sinus could not bo entered. Anesophageal lead was placed that showed presenceof LA electrical activity and presence of atrioven-tricular dissociation (Figs. 2A and 2B). Stimula-tion of RA by a current strength of up to 25 mAat different sites demonstrated a totally inexcitableRA. LA could, however, be stimulated throughesophageal pacing with 1:1 conduction with atri-oventricular interval of 270 msec. (Fig. 2C). Sat-isfactory HBE could not be recorded because oflarge RA. The patient was put on decongestivetherapy with digitalis, diuretics, and small titrateddoses of captopril. On follow-up of 1 year he con-
1276 August 1991 PACE, Vol. 14
ATRIAL STANDSTILL
. ''-v
./v
B
A.V
^.
V
Figures 2A, 2B. Intracardiac eiectrogram and esophageal eiectrogram (Oes.J. Righl atrial re-cording (RAJ shows no atrial activity, whereas Oes. elecfrogram shows left atrial aclivity andpresence of atrioventricular dissociation.
i C : 1 llm
p ,
: i j i i -•"• i ±t
~-v I 1
! - • ' " 1
Figure 2C. Esophageal pacing shows regular pacing with 1:1 conduction to the ventricle. Mid-right afrium (racing shows pacemaker spike fPJ and regular ventricular activity.
PACE, Vol. 14 August 1991 1277
TALWAR, ET AL.
tinues to be in PAS and CHF. Repeat echocardio-gram revealed a large thrombus in RA.
Case Four
S.P., a 60-year-old male presented with a 1-year history of progressive dyspnea and one epi-sode of transient right hemiparesis. He was foundto have elevated jugular venous pressure, a loudventricular gallop, and a grade III/Vl systolic mur-mur at left sternal border. The ECG revealed sinusrhythni, prolonged PR interval, and ST segmentdepression in the inferolateral leads. The echo-cardiogram revealed thickened hypokinetic inter-ventricular septum (IVS) and thick posterior LVwall with no systolic anterior motion of the mitralvalve or mid-systolic closure of the aortic valve.Doppler echocardiography did not reveal any in-traventricular gradient. A diagnosis of nonob-structive hypertrophic cardiomyopathy was madeand the patient was put on verapamil 80 mg threetimes a day. Two hours after the first dose of ver-apamil, the patient was giddy and his heart ratefell to 40/minute. ECG showed junctional rhythm(40/min) with no P waves. A temporary pacemakerwas implanted. Echocardiographic reviewshowed sparking granular appearance of the IVSand a thickened intoratrial septum suggestive ofamyloidosis. Hemodynamic data showed a pat-tern consistent with restrictive myocardial diseasewith elevated filling pressures in the RV and LV.EMB showed dense amyloid deposit (Fig. ID) withcharacteristic apple-green birerefringent on pola-roid light with congo-red staining. Electrophysi-ological study revealed absent atrial activity andcompletely inexcitable RA up to a stimulusstrength of 25 niA. The infranodal conductiontime was normal—50 msec. The atrial standstillpersisted and the patient remained dependentupon a temporary pacemaker despite being off ver-apamil and administration of repeated intrave-nous doses of atropine. A permanent pacemakerwas implanted after 4 weeks. The patient sud-denly expired in the hospital just prior to dis-charge.
Discussion
Clinical and Electrophysiological ProfileThe four patients presented in this report be-
long to different clinical subgroups of PAS. Two
patients presented with syncope and were de-tected to have PAS. The other two presented withsymptoms suggestive of progressively increasingCHF related to the underlying disease (amyloi-dosis and idiopathic restrictive heart disease inone patient each). Also, in two patients, some evi-dence of atrial activity was present before goinginto PAS. Electrophysiologically all four patientssatisfied criteria for the diagnosis of PAS. Threepatients had total PAS while in one patient (case3) atrial activity (spontaneous as well as induci-ble) involving LA was present. Such cases of par-tial PAS have also been described previously.'-^Additionally, one patient had prolonged infran-odal conduction. The rate of the escape focus inthree of our patients was low. necessitating pace-maker implantation. This may also indicate con-comitant involvement of the AV node in PAS. AVnode and SA node involvement in PAS is alsodocumented.^"
Pathologically, the inexcitability of the atriaitissue even at high stimulus strength suggests dis-ruption of the atrial myocardium and its replace-ment with inexcitable tissue. In the literature,pathological studies of atrial tissues suggest twopathological changes: replacement of muscle tis-sue by fibrous tissue or by amyloid.^••' Amyloidreplacement of atrial muscle mass occurs in gen-eralized cardiac amyloidosis.' in some patientswith familial PAS and in some; patients with is-olated PAS.'*'' Fibrosis of the atrial musculature isidentified in patients with PAS who have familialor acquired cardiomyopathy,^ '" muscular dystro-phy/'^^ other progressive cardiac disorders.'' '^ orsome cases with isolated PAS.'-' In our patientsatrial tissue was not available for analysis. How-ever RV endomyocardial tissue was obtained atbiopsy to identify the possible atrial pathology.Amyloid deposit in case 4. fibrosis in case 3. andatrial myocarditis (or subsequent fibrosis) in cases1 and 2 could possibly constitute the pathologicalsubstrate of PAS in our patients. Amyloid depositsand fibrosis in the atrial musculature have beenreported in patients with isolated PAS and couldwell be the case in our patient too.'*''^
Two of our patients (cases 2 and 3) are unu-sual. Myocarditis as a cause of PAS is reported butrare. Rosonbaum et al..^' Benchimol et al.,"* andWohlgelernter et al.'^ have each described a caseof PAS caused by rheumatic myocarditis, Chagas'
1278 August 1991 PACE, Vol. 14
ATRIAL STANDSTILL
SubjectNo.
1
2
3
4
NameAge/Sex
SK. 18,'M
MP, 25/M
DR, 18/M
SP, 60/M
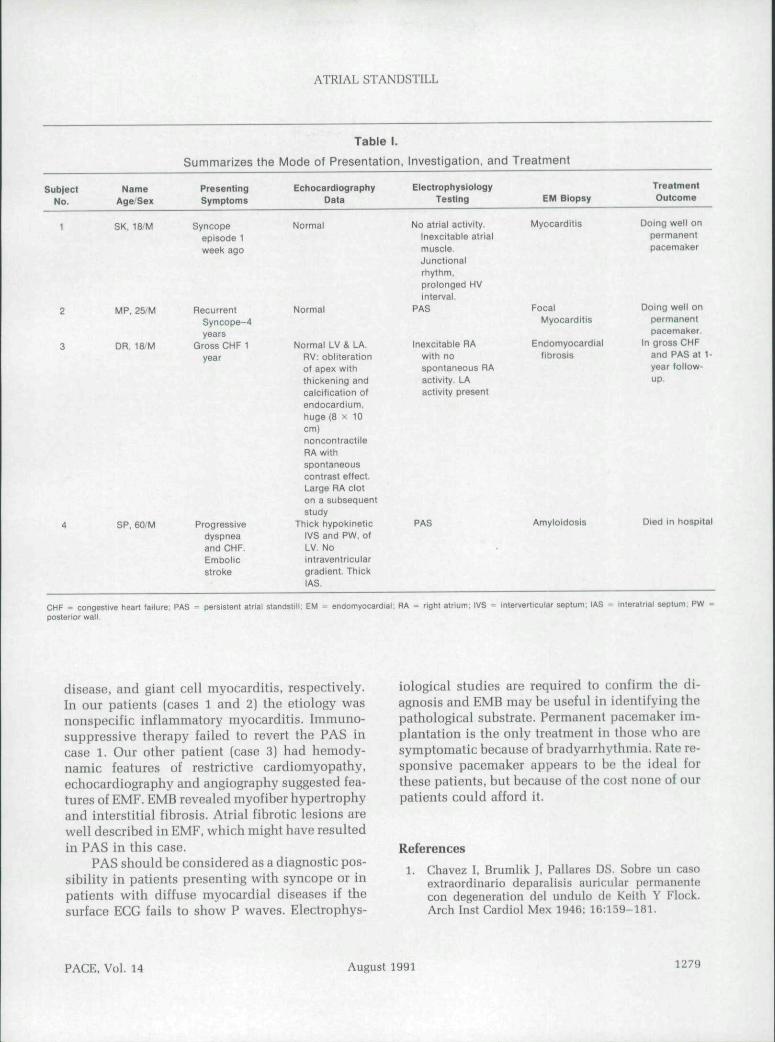
Summarizes the
PresentingSymptoms
Syncopeepisode 1week ago
RecurrentSyncope-4years
Gross CHF 1year
Progressivedyspneaand CHF.EmboiicStroke
Table 1.
Mode of Presentation,
EctiocardlographyData
Normal
Normal
Normal LV & LA.RV; obliterationof apex withthickening andcalcification ofendocardium.huge { 8 x 1 0cm)noncontractileRA withspontaneouscontrast effect.Large RA cloton a subsequent
studyThick hypokinetic
lVS and PW, ofLV, Nointraventriculargradient. ThickIAS,
Investigation, and
ElectrophysiologyTesting
No atrial activity.Inexcitable atrialmuscle.Junctionalrhythm,prolonged HVinterval.
PAS
Inexcitable RAwith nospontaneous RAactivity, LAactivity present
PAS
Treatment
EM Biopsy
Myocarditis
FocalMyocarditis
Endomyocardialfibrosis
Amyloidosis
Treatment
Outcome
Doing well onpermanentpacemaker
Doing well onpermaneritpacemaker.
In gross CHFand PAS at 1-year follow-up.
Died in hospital
CHF - congestive heart failure; PAS = persistent atrial standstill; EM = endomyocardial; RA = right alnurn; IVS = mterverticular septum, IASposterior wall.
Interatrlal septum, PW =
disease, and giant cell myocarditis, respectively.In our patients (cases 1 and 2) the etiology wasnonspecific inflammatory myocarditis. Immuno-suppressive therapy failed to revert the PAS incase 1. Our other patient (case 3) had hemody-namic features of restrictive cardiomyopathy,echocardiograpliy and angiography suggested fea-tures of EMF. EMB revealed myofiber hypertrophyand interstitial fibrosis. Atrial fibrotic lesions arewell described in EMF, which might have resultedin PAS in this case.
PAS should be considered as a diagnostic pos-sibility in patients presenting with syncope or inpatients with diffuse myocardial diseases if thesurface ECG fails to show P waves. Electrophys-
iological studies are required to confirm the di-agnosis and EMB may be useful in identifying thepathological substrate. Permanent pacemaker im-plantation is the only treatment in those who aresymptomatic because of bradyarrhythmia. Rate re-sponsive pacemaker appears to bo the ideal forthese patients, but because of the cost none of ourpatients could afford it.
References1. Chavez I, Brumlik J, Pallares DS. Sobre un casn
extraordinario deparalisis auricular permanentecon degeneration del undulo de Keith Y Flock.Arch Inst Cardiol Mex 1946; 16:159-181.
PACE, Vol. 14 August 1991 1279
TALWAR. ET AL.
Ward DE, Yen Ho S, Shinebourne EA. Familial 9.atrial standstill and in excitably in childhood. AmJ Cardiol 1984; 53:965-967.Woolliscroft J, Tuna N. Permanent atrial standstill: 10.The clinical spectrum. Am J Cardiol 1982;49:2037-2041.Benchimol CIB, Schlesinger P, Ginefra P, et al. Per- 11.sistent atrial standstill. Acta Cardiologica 1975;30;313-322.Taiwar KK. Radhakrishnan S, Chopra P. Myocar-ditis presenting as persistent atrial standstill a case 12.report. Int J Cardiol 1988; 20:283-285.Levy S, Pouget B. Lacaze JC. et al, Partial atrialstandstill; Report of three cases and review of clin- 13.ical and electrophysiological features. Eur Heart J1980; 17;107-116.Rosen KM, Rahimtolla S. Gunnar RM, et al, Tran-sient and persistent atrial standstill with His bun- 14.die lesions. Circulation 1971; 44:220-236.Williams DO. Jones EL. Nagle RE. et al. Familial 15.atrial cardiomyopathy with heart block. Q J Med1972; 41;491-508.
Maeda S, Tanka T, Hayashi T. Familial atrialstandstill caused bv amyloidosis. Br Heart J 1988;39:498-500,AUensworth DC, Rice GJ, Lowe GW. Persistentatrial standstill in a family with myocardial di-sease. Am J Med 1969; 47:775-784.Caponnetto S. Pastorini C. Tirelli G. Persistentatrial standstill in a patient affected with fascios-capulohumeral distrophy. Cardiologia 1968;53;341-350.Khan AH, Haider R. Boughner DR. et al. Sinusrhythm with absent P waves in advanced rheu-matic heart disease. Am J Cardiol 1973; 32:93-97.Tanaka H. Atsuchi Y. Tanaka N, et al. Persistentatrial standstill due to atrial inexcitability; Anelectropbysiological and bistological study. JpnHeart J 1975; 16:639-653.Rosenbaum FF. Levine SA. Auricular standstill.Am I Med Sci 1939; 198:774-778.Wohlgelernter DC, Otis CN. Batisford WP. et al.Myocarditis presenting with silent atrium and leftatrial thrombus. Am Heart J1984; 108:1557-1558.
1280 August 1991 PACE, Vol. 14

Related Documents







![Dysrhythmias (002) [Read-Only] - Aventri · Atrial AV node Ventricular Classification of Rhythm Abnormalities Supraventricular Atrial origin Atrial fibrillation Atrial flutter Atrial](https://static.cupdf.com/doc/110x72/5f024baa7e708231d4038f22/dysrhythmias-002-read-only-aventri-atrial-av-node-ventricular-classification.jpg)



