eripheral Nerve Injuries

Peripheral Nerve Injuries. AXILLARY NERVE A large nerve arising from the posterior cord of the brachial plexus Divided: Posterior branch: Innervates Teres.
Dec 16, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Peripheral Nerve Injuries
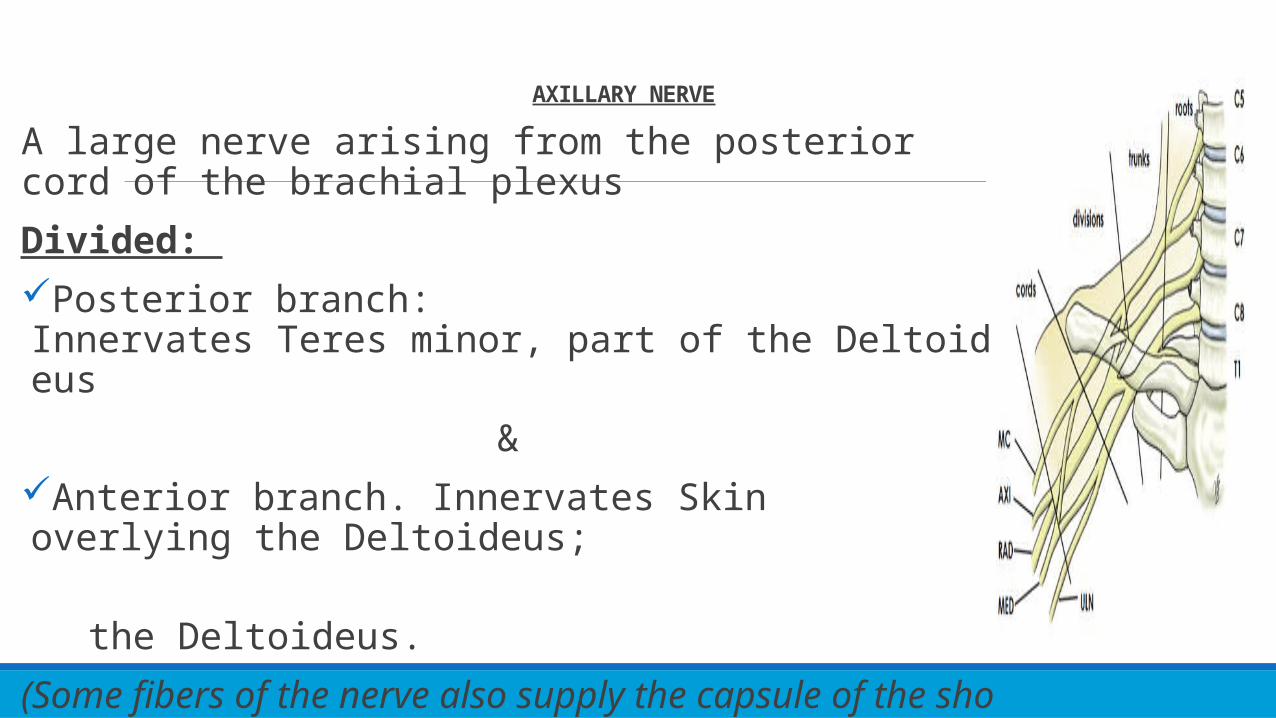
AXILLARY NERVE
A large nerve arising from the posterior cord of the brachial plexus
Divided: Posterior branch: Innervates Teres minor, part of the Deltoideus
&Anterior branch. Innervates Skin overlying the Deltoideus;
the Deltoideus.
(Some fibers of the nerve also supply the capsule of the shoulder joint)
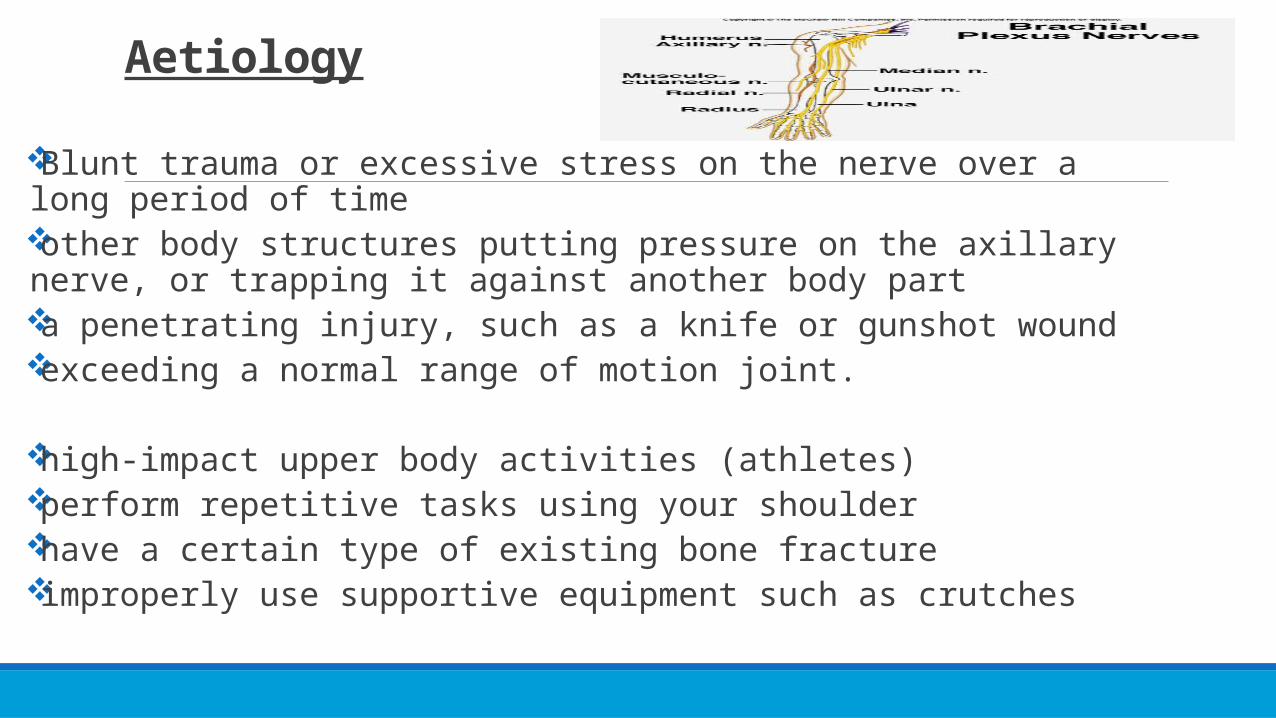
Aetiology
Blunt trauma or excessive stress on the nerve over a long period of timeother body structures putting pressure on the axillary nerve, or trapping it against another body parta penetrating injury, such as a knife or gunshot woundexceeding a normal range of motion joint.
high-impact upper body activities (athletes)perform repetitive tasks using your shoulderhave a certain type of existing bone fractureimproperly use supportive equipment such as crutches

most common peripheral nerve injury to affect the shoulder. It most often is seen after glenohumeral joint dislocation, proximal humerus fracture, or a direct blow to the deltoid muscle. Compression neuropathy has been reported to occur in the quadrilateral space syndrome, true pathophysiology of this disorder remains unclear. vulnerable during any operative procedure involving the inferior aspect of the shoulder and iatrogenic injury (Referring to injuries caused by a doctor.).
Pathophysiology
Pathophysiology
most common peripheral nerve injury to affect the shoulder.
It most often is seen after glenohumeral joint dislocation, proximal humerus fracture, or a direct blow to the deltoid muscle.
Compression neuropathy has been reported to occur in the quadrilateral space syndrome, although the true pathophysiology of this disorder remains unclear. The axillary nerve is vulnerable during any operative procedure involving the inferior aspect of the shoulder and iatrogenic injury remains a serious complication of shoulder surgery. During the acute phase of injury, the shoulder should be rested, and when clinically indicated, a patient should undergo an extensive rehabilitation program emphasizing range of motion and strengthening of the shoulder girdle muscles. If no axillary nerve recovery is observed by 3 to 6 months after injury, surgical exploration may be indicated, especially if the mechanism of injury is consistent with nerve rupture. Patients who sustain injury to the axillary nerve have a variable prognosis for nerve recovery although return of function of the involved shoulder typically is good to excellent, depending on associated ligamentous or bony injury.
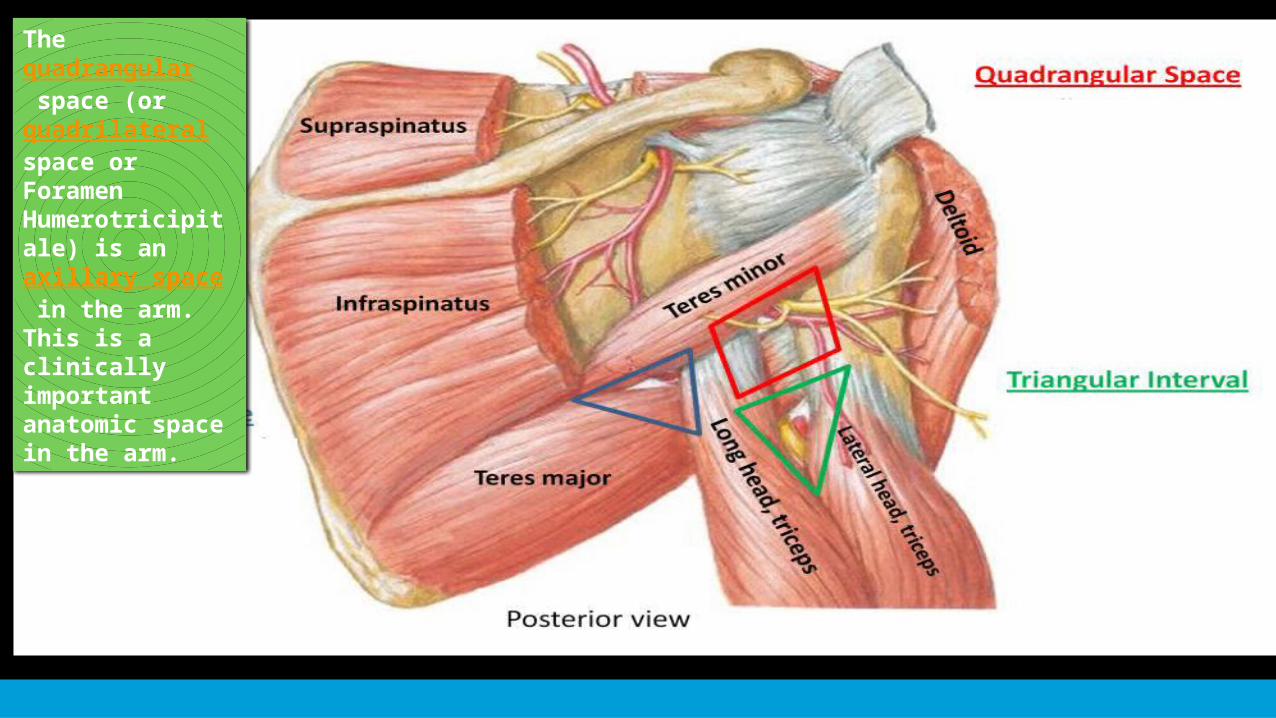
The quadrangular space (or quadrilateralspace or Foramen Humerotricipitale) is an axillary space in the arm. This is a clinically important anatomic space in the arm.

Nerve Injury◦ Nerve regeneration takes place at a rate of ~1mm/day
◦ Seddon's Classification of Nerve Injury◦ Neuropraxia The axon and all 3 connective tissue layers
(endoneurium, perineurium, and epineurium) remain intact with a decrease in conduction
◦ Axonotmesis Axonal damage is present with preservation of the endoneurium
◦ Neurotmesis Axonal damage is present
Pathophysiology

Anterior shoulder dislocation is the most common occurring dislocation at the shoulder.
Men and women 3:1 9-65% involve axillary nerve injury
Traction and compression to the axillary nerve
Blunt trauma
Pathophysiology
Clinical Presentation # Variable and can go undetected, as the concomitant dislocation or fracture may mask the symptoms.
Subjective Examination
◦ Generalized mild, dull, and achy pain to the deep or lateral shoulder, with occasional radiation to the proximal arm
◦ Numbness and tingling of the lateral arm and/or posterior aspect of the shoulder
◦ In some cases, persisting 2-4 weeks post-injury
◦ Feeling of instability
◦ Weakness, especially with flexion, abduction, and external rotation
◦ Fatigue, especially with overhead activities, heavy lifting, and/or throwing
◦ May/or may not reveal a history of trauma to the shoulder region
◦ Easing Factors include: rest, ice, analgesics, and anti-inflammatory medications
Clinical Presentation
“Unhappy Triad”
Quadrilateral Space Syndrome (QSS)Posterior Cord of the Brachial Plexus Injury
C5-6 Cervical Radiculopathy
Parsonage-Turner Syndrome (PTS)
Clinical Presentation
"Unhappy Triad"
The “Unhappy Triad” consists of a shoulder dislocation that results in both a rotator cuff tear and axillary nerve injury.
Occurs in 9-18% of anterior shoulder dislocations
Risk of an “unhappy triad” with anterior shoulder dislocation increases after the age of 40.
Differential Diagnosis
Quadrilateral space syndrome(QSS)
QSS is an “uncommon condition that involves the compression of the posterior humeral circumflex artery and the axillary nerve within the quadrilateral space,” secondary to an acute trauma or from overuse, especially with overhead sports like throwing and swimming.
Symptoms are typically present with the arm in an overhead position, especially in late cocking or the early acceleration phases of throwing
Parsonage-Turner Syndrome(PTS)
PTS is an uncommon, idiopathic condition.
Characterized by an acute onset of intense pain, without a mechanism of injury, that subsides within days-weeks, leaving behind residual weakness/paralysis in upper extremity muscles.
Clinical Presentation
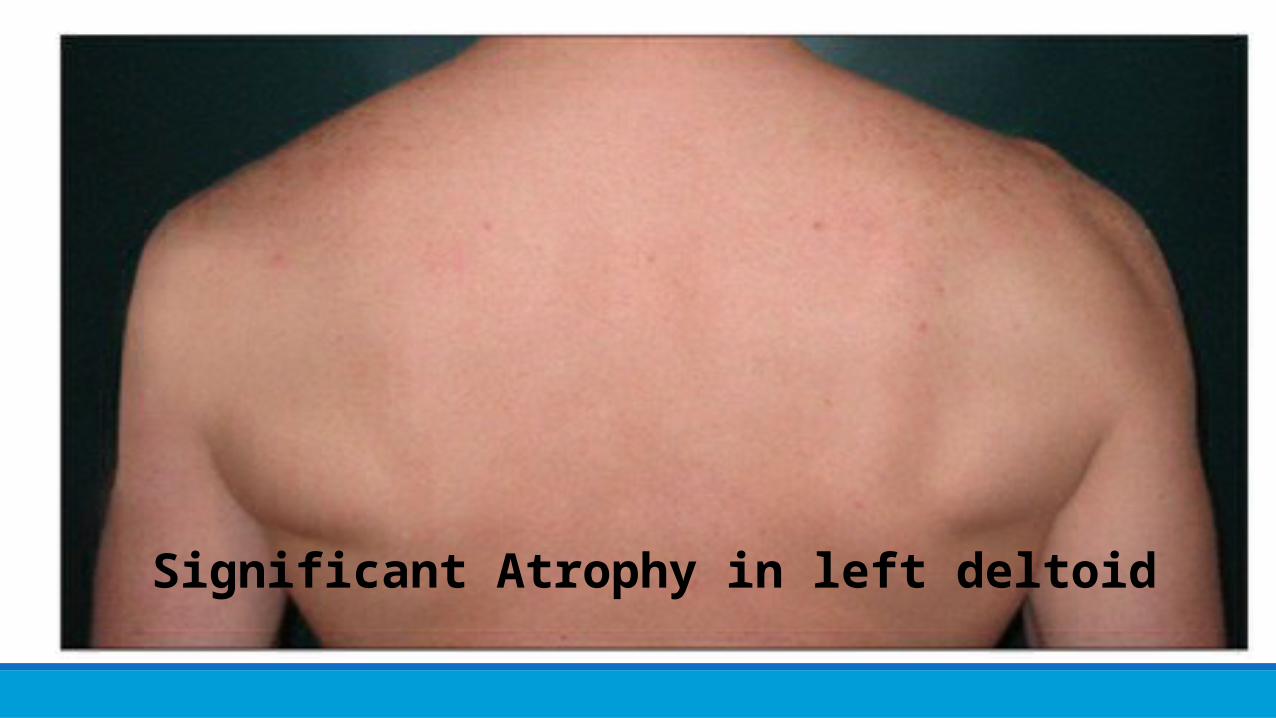
Significant Atrophy in left deltoid
Symptoms Numbness over part of the outer shoulder
Shoulder weakness, especially when lifting the arm up and away from the body
May experience weakness in the shoulders and have problems with normal physical activities, such as lifting your arms above your head. Difficulty lifting objects can also be a sign of AND.
Over time, your shoulder muscles may become smaller because they cannot be worked out regularly.
ExaminationPhysical examination should begin with a screening consisting of an evaluation of the head and neck which shouldn’t reveal any abnormalities.
If the patient presents with a recent shoulder dislocation, presence of a radial pulse and sensation and movement of the digits should also be assessed as part of the initial screening
Medical Management

Medical Management
SurgeryIndications for surgerySuspicion of osteophyte formation or
compression in the quadrilateral space.No axillary nerve recovery observed by 3 to
4 months following injury.No improvements seen after 3 to 6 months
of conservative treatment.No EMG/NCV evidence of recovery by 3 to
6 months after injury.
Surgical ProceduresNeurolysisNeurorrhaphyNerve grafting
Nonsurgical Reduction Reduction eliminates the need for surgical
intervention, and is followed by immobilization and physical therapy management.
Immobilization for young adult males 4-6 weeks
Immobilization for older patients 7-10 days
Precaution should be taken during manipulative reduction of a dislocation,
NSAIDS, rest, ice

Physical Therapy Management (current best evidence)
Current research encompassing treatment and intervention of axillary nerve injuries following shoulder dislocation is limited.
Non-Surgical Physical Therapy Treatment
0-2 weeks
Shoulder immobilization via sling after reduction◦ There is insufficient evidence to support whether physical therapy should be initiated during or after
immobilization.
Isometric Strengthening; Dosing: 10 seconds X 6 repetitions X 2 day within limits of pain◦ Shoulder(Flex, Ext, Abd, Add, IR)
Joint Mobility◦ Active Range of Motion(AROM); Dosing 10 repetitions X 2 day
◦ Elbow(Flex, Ext ,Pronation, Supination)◦ Wrist (Flex, Ext, Radial/Ulnar deviation)◦ Hand (Opening/Closing Fist)
2-4 weekJoint Mobility
PROM/AAROM); Dosing 10 repetitions X 2 day Shoulder (Flex, IR, Add)
Avoid end-range ER/Abd until later stages of treatment!
AROM; Dosing 10 repetitions X 2 dayElbow(Flex, Ext ,Pronation, Supination) Wrist (Flex, Ext, Radial/Ulnar deviation) Hand (Opening/Closing Fist)
Pendulum Exercises 3 sets x 30 secondsPostural/Periscapular Muscular Strengthening/Neuromuscular Re-education
Target MusclesDeltoid Serratus Anterior Rhomboid Major/Minor Upper/Middle/Lower Trapezium
PRECAUTION: against shoulder abduction & flexion beyond 90 degrees, and ER beyond neutral in the first 3 weeksOlder individuals have lower rates of reoccurrence of shoulder dislocation and an increase in incidence of joint stiffness.
4-6 weeksD/C slingStrengthening Program light resistive exercises Proprioceptive Techniques
PNF diagonalsClosed Chained Activities
Wall push-ups -->Table-->FloorWeight Shifts
6 weeks-Discharge
Continue ROM, glenohumeral and scapulothoracic stabilization/strengthening exercises,
Proprioception, and joint mobility, while maintaining optimal conditions for tissue healing
Begin to initiate sport/job specific activities, progressing to full return as patient’s functional status allows
Medical Management
ConclusionDuring the acute phase of injury, the shoulder should be rested, and when clinically indicated, a patient should undergo an extensive rehabilitation program emphasizing range of motion and strengthening of the shoulder girdle muscles.
If no axillary nerve recovery is observed by 3 to 6 months after injury, surgical exploration may be indicated, especially if the mechanism of injury is consistent with nerve rupture.
Patients who sustain injury to the axillary nerve have a variable prognosis for nerve recovery although return of function of the involved shoulder typically is good to excellent, depending on associated ligamentous or bony injury.

References http://www.merriam-webster.com/medical/axillary%20nerve
http://medical-dictionary.thefreedictionary.com/axillary+nerve
https://www.google.gy/search?q=axillary+nerve+definition&rlz=1C1CHFX_enGY629GY629&espv=2&biw=1242&bih=606&site=webhp&source=lnms&tbm=isch&sa=X&ei=VrwLVYO_GYmhyQT29IH4Aw&sqi=2&ved=0CAYQ_AUoAQ&dpr=1.1#imgdii=_&imgrc=tSupG6p00N1nmM%253A%3B1nKZj2k2ocSGDM%3Bhttp%253A%252F%252Fwww.usra.ca%252Fimages%252Fbp2.jpg%3Bhttp%253A%252F%252Fwhat-is-this.net%252Ffr%252Fdefinition%252Faxillary%3B420%3B310
https://www.google.gy/search?q=axillary+nerve+definition&rlz=1C1CHFX_enGY629GY629&espv=2&biw=1242&bih=606&site=webhp&source=lnms&tbm=isch&sa=X&ei=VrwLVYO_GYmhyQT29IH4Aw&sqi=2&ved=0CAYQ_AUoAQ&dpr=1.1#imgdii=_&imgrc=2rlRRBWo8cRukM%253A%3BiaN2Ymik8NlmvM%3Bhttp%253A%252F%252Flegacy.owensboro.kctcs.edu%252Fgcaplan%252Fanat%252Fnotes%252FImage544.gif%3Bhttp%253A%252F%252Flegacy.owensboro.kctcs.edu%252Fgcaplan%252Fanat%252Fnotes%252Fapi%252520notes%252520m%252520%252520peripheral%252520nerves.htm%3B640%3B480
http://www.healthline.com/health/axillary-nerve-dysfunction#Overview1
http://www.physio-pedia.com/Axillary_Nerve_Injury
http://www.ncbi.nlm.nih.gov/pubmed/10613150
http://www.nlm.nih.gov/medlineplus/ency/article/000689.htm
Related Documents











