Perioperative Visual Loss Kevin Driscoll Matt Mitchell Carolyn Srinivasan

Perioperative Visual Loss Kevin Driscoll Matt Mitchell Carolyn Srinivasan.
Dec 18, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Perioperative Visual Loss
Kevin DriscollMatt MitchellCarolyn Srinivasan
Objectives
• Epidemiology• Anatomy• Physiology • Pathophysiology• Treatment• Prevention• Considerations

Vision Loss: Epidemiology & Anatomy

Vision Loss• Incidence of perioperative visual loss
(POVL) after non-ocular surgery– 0.002% of all surgeries (Newman, 2008)– 0.2% of cardiac and spine surgeries (Newman, 2008)
• Any portion of the visual pathway may be involved– Cornea to the occipital lobe– Optic nerve
• Most common site of permanent injury• Presumed mechanism is ischemia • Anterior ischemic optic neuropathy (AION)
– Cardiac surgery patients• Posterior ischemic optic neuropathy (PION)
– Spine and neck procedures. • Age 5 to 81 years

Vision Loss: Review of LiteratureRoth S, et al. Eye injuries after nonocular surgery: a study of
60,965 anesthetics from 1988 to 1992. Anesthesiology 1996;85:1020 –1027.– University of Chicago (1988-1992)– 60,965 patients undergoing non-ocular surgery– 1 patient (0.002%) suffered non-corneal POVL
Warner ME, et al. The frequency of perioperative vision loss. Anesth Analg 2001;93:1417–1421.– Mayo Clinic, retrospective study, excluded cardiac surgeries– 501,342 non-cardiac surgeries– 4 patients (0.0008%) developed POVL for longer than 30 days
Nuttall GA, et al. Risk factors for ischemic optic neuropathy after cardiopulmonary bypass: a matched case/control study. Anesth Analg 2001;93:1410–1416.– Mayo Clinic, retrospective study– 27,915 cardiopulmonary bypass (CABG) procedures – 17 (0.06%) patients were identified with peri-operative ION

Vision Loss: Review of LiteratureStevens WR, et al. Ophthalmic complications after spinal surgery.
Spine1997;22:1319 –1324.– 3 centers (1985-1994)– 3,450 spine surgeries – 7 cases (0.2%) with visual loss (2 patients with occipital infarctions, 4 patients
with ION, and 1 patient with a central retinal vein occlusion)
Roth S, et al. Postoperative visual loss: still no answers– yet. Anesthesiology 2001;95:575–577.– 15 year study of nearly 225,000 surgeries – 3 of 3,351 patients (0.09%) developed POVL after spinal surgery– 50-fold higher rate compared with all other non-ocular procedures
Chang SH, et al. The incidence of vision loss due to perioperative ischemic optic neuropathy associated with Spine surgery: the Johns Hopkins Hospital Experience. Spine 2005;30:1299 –1302.– 20 year retrospective review at Johns Hopkins Hospital– 14,102 spine surgeries – ION was identified in four cases (0.028%)

ASA POVL Registry
• In 1999, the ASA POVL Registry was established in response to concerns that POVL seemed to be increasing• Purpose:
– Meaningful analysis– Identify risk factors – Develop preventive measures
• The database consists of:– Voluntary, anonymously reported cases – Visual loss within seven days of non-ocular surgery– Standardized form that includes:
• detailed demographic, historical, examination, and intraoperative information • www.asaclosedclaims.org

ASA POVL Registry • June 2005 - 131 cases of POVL reported
– 95 spine cases– 12 cardiac cases– 6 major vascular cases– 5 orthopedic cases– 13 miscellaneous cases
• 2006 ASA Interim Report – in-depth analysis of 93 cases of POVL associated with spine surgery– 83 cases of ION
• 67% were PION• 23% AION• 10% unspecified ION
– 10 cases of central retinal artery occlusion • 73% of all cases in the setting of spine surgery• Age range: 5 to 81 years• MALES predominated among the spine cases• 82% had one pre-existing vascular risk factor• 64% had an ASA physical status I or II (healthy)

Vision Loss: Anterior Segment• The cornea is the
most commonly reported location of ocular injury during anesthesia
• Corneal abrasions and or exposure
• Usually NOT a cause of permanent visual loss

Vision Loss: Retina• Most common retinal cause of
visual loss is central retinal artery occlusion (CRAO)
• Due to systemic or local arterial embolism
• Cardiac and other vascular surgeries
• Prone position spine surgeries– external compression of the
globe due to malposition of head
• ASA POVL Registry – 93 spine surgery cases with
postoperative visual loss• 10 patients had CRAO• all unilateral• 7 (of the 10) had additional
evidence of peri-ocular trauma, (ipsilateral decreased supraorbital sensation, ptosis, erythema, corneal abrasion, and ophthalmoplegia)
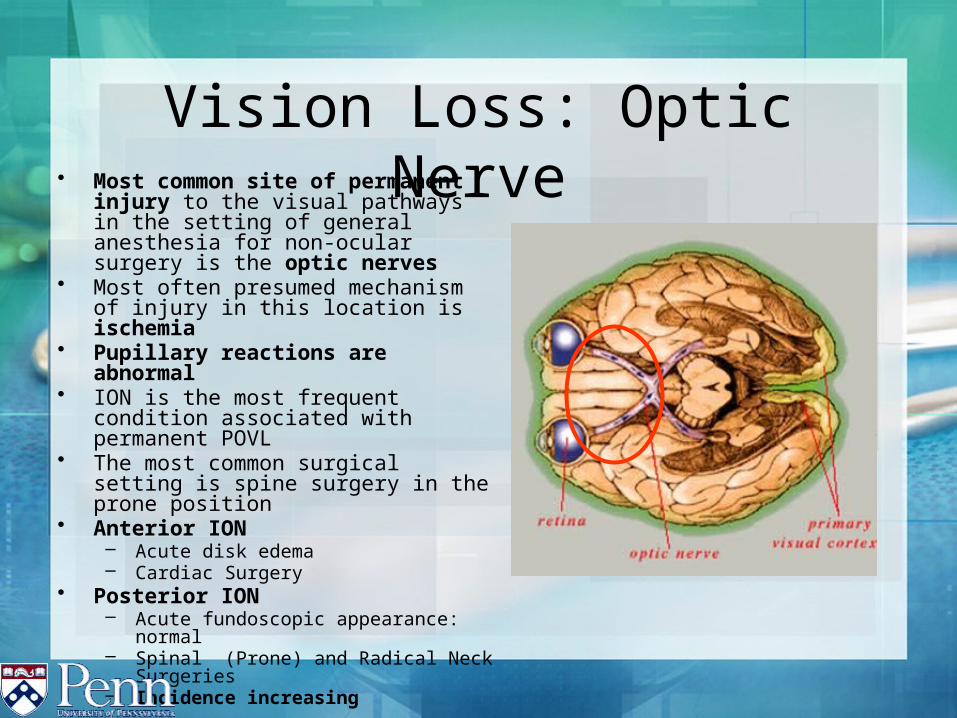
Vision Loss: Optic Nerve• Most common site of permanent
injury to the visual pathways in the setting of general anesthesia for non-ocular surgery is the optic nerves
• Most often presumed mechanism of injury in this location is ischemia
• Pupillary reactions are abnormal• ION is the most frequent condition
associated with permanent POVL• The most common surgical setting is
spine surgery in the prone position• Anterior ION
– Acute disk edema– Cardiac Surgery
• Posterior ION – Acute fundoscopic appearance:
normal– Spinal (Prone) and Radical Neck
Surgeries– Incidence increasing

Vision Loss: Retrochiasmal Visual Pathways
• Homonymous hemianopsia (unilateral) versus cortical visual impairment (bilateral)
• Pupillary reactions are normal• Usually ischemic in origin - embolic
cerebral infarction (posterior cerebral arteries)– Other mechanisms - neck
trauma during intubation• Risk of stroke after general,
noncardiac procedures is 0.08% to 0.7%
• Resection of head and neck tumors and cardiac and vascular surgeries are associated with higher risks
• Most peri-operative strokes are infarctions and are embolic in origin
• Incidence of visual loss from retro-chiasmal infarction in the peri-operative period is unknown

Physiology and Pathophysiology
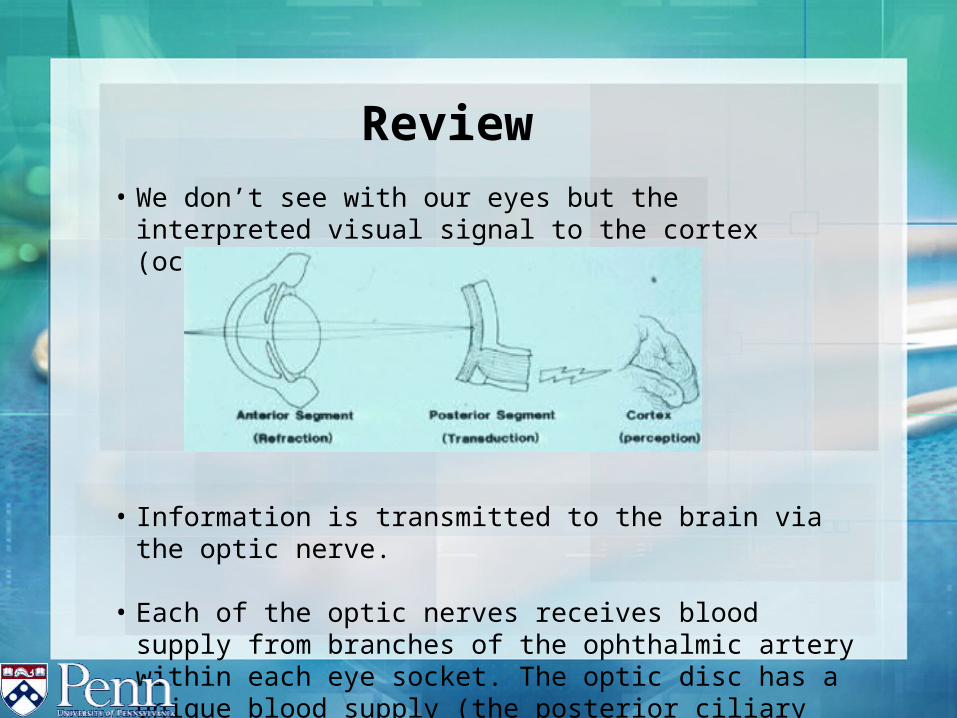
Review• We don’t see with our eyes but the interpreted visual signal to the
cortex (occipital lobe).
• Information is transmitted to the brain via the optic nerve.
• Each of the optic nerves receives blood supply from branches of the ophthalmic artery within each eye socket. The optic disc has a unique blood supply (the posterior ciliary arteries).

A Closer look at the blood supply• Blood supply to the chorid is thru the opthalmic artery (1)
• one branches becomes the central retinal artery(2).• 2 branches which become the posterior ciliary arteries (3).
• These are the main arteries indicated for peri-operative visual loss
1
2
3
3

Perioperative Vision loss
• Corneal Damage• Central Retinal Artery Occlusion
(CRAO)• Ischemic Optic Neuropathy (ION)
• Defined by where the lesion occurs on the optic nerve:• Anterior ION• Posterior ION

Direct Corneal Damage• Most Common preventable reason for Unilateral Vision Loss

Central Retinal Artery Occlusion (CRAO)• The neurons of the retina, like those in the
rest of the nervous system, are extremely susceptible to hypoxia.
• Central retinal artery occlusions may
follow thrombosis of the retinal artery, as in atherosclerosis or giant cell arteritis, or emboli of various types. Intracellular edema, manifested by retinal pallor, is prominent, especially in the macula where the ganglion cells are most numerous.
The vacularized choroid beneath the center of the macula (foveola) stands out in sharp contrast as a prominent “cherry red spot”.
www.surgical-pathology.com/retinal_artery.htm

• Usually caused by external pressure on the globe (positioning) • Common findings are unilateral vision loss with signs of external
periorbital swelling or ecchymosis.• Prone position causes increase in intraocular pressure. Coupled
with malposition this insult may lead susceptible patient populations to vision loss.
• Direct Compression has been implicate. Mimics an accelerated glaucoma. pressure from malposition or direct pressure on the globe is translated from the Optic disk to the Central Retinal Artery.
Central Retinal Artery Occlusion (CRAO)
Ischemic Optic Neuropathy (ION)• Etiology is still unclear. But there is a decreased
delivery of O2 to the optic nerve.• Procedural dependent factors associated with ION
elicited from the ASA closed claims:• Anemia• Prolonged procedures (>6.5hrs)• Sustained blood loss (44.7% of EBV)• Combination of the above
• ION is further defined by where the lesion occurs and findings on retinal exam.

Ischemic Optic Neuropathy (ION)
Anterior ION:• Occurs in watershed area of Posterior Ciliary Artery (2 branches)• Anterior Optic Nerve supplied by multiple sources• Located in or near optic disk visible on retinal exam as edema.
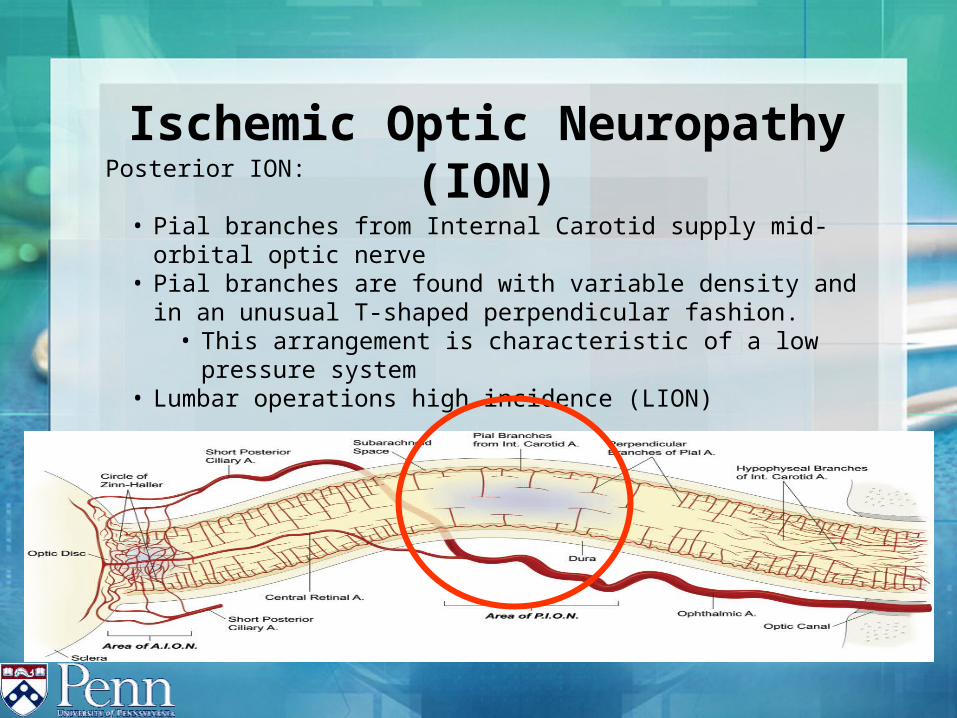
Ischemic Optic Neuropathy (ION)Posterior ION:
• Pial branches from Internal Carotid supply mid-orbital optic nerve• Pial branches are found with variable density and in an unusual T-shaped
perpendicular fashion.• This arrangement is characteristic of a low pressure system
• Lumbar operations high incidence (LION)

Contributing factors to ION
• Hypotension• Hypovolemia• Hypoxemia• Hemodilution• Facial edema• Use of Vasopressors• Prone• Head down• Increase in venous pressure

Treatment & Prevention
Prevention is a good thing• Prevention starts with:
• Understanding of etiology• Understanding of Pathophysiology• Understanding of Risk Factors• Understanding the modalities to truly prevent POVL • UTILIZING the modalities to treat POVL

How to appropriately prevent POVL• Understanding the risk factors
– Procedure dependent risk factors– CABG, prone cases, neck, nose and sinus surgery,
• Intra-operative events- large EBL, systemic Hypotension, long duration of procedure (>5 hrs), and anemia
How to appropriately prevent POVL
• Understanding the risk factors– Patient dependent risk
factors• Hypertension• Atherosclerosis• Tobacco use• Diabetes Mellitus• Morbid obesity
How to appropriately prevent POVL• Understanding the risk factors
– Procedural issues related to decrease oxygen delivery to the optic nerve• large EBL, prolonged Hypotension(52%), anemia, OR (9.9hrs)
• ASA POVL registry as of 2000 had 23 incidents of POVL– Prone spine cases most common position (57%)– CABG (22%)
• Ischemic optic neuropathy was the chief diagnosis in 20/23 reported cases

ASA POVL Registry• Patient dependent related risk factors
Variable All Cases (n=23)Median Age (range) 58 (24-73) yearsObesity (percent cases) 13 (56 percent)Hypertension 11 (48 percent)Diabetes Mellitus 5 (22 percent)Smoking History 12 (52 percent)Atherosclerosis 12 (52 percent)
Lee, LA: Postoperative visual loss data gathered and analyzed. ASA Newsletter 64(9): 25-27, 2000.

ASA POVL Registry 2006
Variables n (% of 83 cases)Mean age 50 +/- 14yrsObesity 44 (53%)Hypertension 34 (41%)Diabetes Mellitus 13 (16%)Smoking History 38 (46%)Atherosclerosis (CAD) 8 (10%)Cerebrovascular disease 3 ( 4%)Increased Cholesterol/Lipids 11 (13%)1 Coexesting diseases 68 (82%)Lee, L. et al. (2006). The American society of anesthesiologist postoperative visual loss registry. Anesthesiology. 105, 652-9. Lee, L. et al. (2006). The
American society of anesthesiologist postoperative visual loss registry. Anesthesiology. 105, 652-9.

Considerations

Current recommendations from ASA Task Force on Peri-operative Blindness
Current recommendations for major spine surgery1. Consider risk explanation in consenting process
2. Use arterial catheters to monitor BP, consider CVP monitoring with CVC
3. Use colloids along with Crystalloids for replacement of volume
4. Position Head of Bed so that it is EQUAL or ABOVE the level of the HEART.
5. Consider staging surgeries. (decrease anesthesia time)
Lee, L. (2008). Solutions to POVL mystery requires research. The Official Journal of the Anesthesia Patient Safety Foundation. 23(1), P.3

Prone position Related Devices

Anesthesia Related Prone Position Devices
Summary
• Remember the Etiology of POVL• Remember the Case/Anesthetic
specific considerations of POVL• Remember the Patient specific
considerations• APSF recommendations based on
current literature to reduce the incidence of POVL

References• Baig M, Lubow M, Immesoete P, et al. Vision loss after spine surgery:
review of the literature and recommendations. Neurosurgery Focus. 2007; 23 1-9.
• Chang SH, Miller NR. The incidence of vision loss due to perioperative ischemic optic neuropathy associated with Spine surgery: the Johns Hopkins Hospital Experience. Spine 2005;30:1299 –1302.
• Hayreh, SS. Posterior ischemic optic neuropathy: clinical features, pathogenesis, and management. Eye. 2004; 18:1188-1206.
• Lee, LA: Postoperative visual loss data gathered and analyzed. ASA Newsletter. 2000;64:25-27.
• Lee, L. Solutions to POVL mystery requires research. The Official Journal of the Anesthesia Patient Safety Foundation. 2008;23:p.3.
• Newman, NJ. Perioperative Visual Loss After Nonocular Surgeries. Am J Opthalmol 2008;145:4:604-610.
• Nuttall GA, Garrity JA, Dearani JA, et al. Risk factors for ischemic optic neuropathy after cardiopulmonary bypass: a matched case/control study. Anesth Analg 2001;93:1410–1416.
References• Roth S, Barach P. Postoperative visual loss: still no answers– yet.
Anesthesiology 2001;95:575–577.• Roth S, Thisted RA, Erickson JP, Black S, Schreider BD. Eye injuries
after nonocular surgery: a study of 60,965 anesthetics from 1988 to 1992. Anesthesiology 1996;85:1020 –1027.
• Stevens WR, Glazer PA, Kelley SD, Lietman TM, Bradford DS. Ophthalmic complications after spinal surgery. Spine1997;22:1319 –1324.
• Warner ME, Warner MA, Garrity JA, et al. The frequency of perioperative vision loss. Anesth Analg 2001;93:1417–1421.
Related Documents











