PERIOPERATIVE RISK ASSESSMENT AND EVALUATION FOR NONCARDIAC SURGERY Consultative Medicine Jayne Barr, MD, FACP, FAAP

PERIOPERATIVE RISK ASSESSMENT AND EVALUATION FOR NONCARDIAC SURGERY Consultative Medicine Jayne Barr, MD, FACP, FAAP.
Dec 25, 2015
Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PERIOPERATIVE RISK ASSESSMENT AND EVALUATION FOR
NONCARDIAC SURGERY
Consultative Medicine
Jayne Barr, MD, FACP, FAAP

Outline
Role of consultantIntroductionRecommendations
Cardiac risk assessment Pulmonary assessment
MiscellaneousAlgorithm 2007

Introduction
In US, millions of patients undergo surgical procedures each year
Most morbidity & death occur in the post-op period & is of cardiac, pulmonary, neurologic, or infectious origin
MIs usually occurs w/in the first 4 days after surgery & is associated with a 15-25% mortality rate

Introduction
Nonfatal post-op MI is an independent risk factor for future infarction and death w/in 6 months after surgery
ACP guidelines similar to ACC/AHA except that ACP does not recommend use of exertional capacity (METs) to guage cardiovasc risk

Rationale for Perioperative Medicine Consultation
The cost of preoperative testing is estimated to be about $18 billion for the 30 million surgical cases performed annually in the US.
Average cost---$600 per casePreoperative clinic visits reduce the number
of tests ordered by approximately 55%
• Fischer S. 1996 Anesthesiology. Development and effectiveness of an anesthesisa preoperative evaluation clinic in a teaching hospital.

Perioperative Medical Assessment Goals
Efficient utilization of the sources and eliminating unnecessary tests and consults.
Reduce the length of stay and morbidityOptimizing the patient before surgery well in
advanceImproves the quality of perioperative careImproves surgical outcomesFamily and patient satisfaction

Role of the Consultant
Evaluate and optimize patient’s medical status
Treat modifiable risk factorsOffers opinions about operative risk and
perioperative managementRecommend measures to minimize
perioperative complicationsFocus over the entire perioperative periodLong term patient outcomes

What Not to Do
Recommend for or against surgeryTell anesthesiologist how to do their jobRecommend the obvious“clear” the patientSay nothing

Purpose of the Guidelines
Goal is not to “medically clear” ptProvide a risk profile based on pt’s medical
status and make recommendations concerning the management and risk of cardiac problems over the entire perioperative period

Methodology and Evidence
ACC/AHA conducted literature searches in PubMed, MEDLINE, and Cochrane Library from 2002-2007
Searches limited to English language and human subjects

Applying Classification of Recommendations and Level of Evidence (LOE)
Class I- Evidence that procedure is beneficial, useful, and effective
Class II- Conflicting Evidence Class IIa- Weight is in favor of usefulness/efficacy Class IIb- Efficacy is less well established
Class III- Evidence that procedure is not useful and may be harmful

Applying Classification of Recommendations and Level of
Evidence
Level of Evidence A- Data from multiple, randomized, clinical trials or meta-analysis
Level of Evidence B- Data from single-randomized trial or large non-randomized trial
Level of Evidence C- Only consensus opinion of experts, case studies, or retrospective studies, standard-of-care

ACC Guidelines—Clinical Risk Factors
Major Clinical Predictors
Unstable coronary syndromes ACS unstable angina
Recent MIAcute
decompensated HF
Significant arrhythmias VT Bradyarrhythmias High grade AV blocks Paced rhythms Uncontrolled SVT
Severe valvular disorders AS -- mean pressure gradient
> 40 mmHg or valve area < 1.0 cm2, or symptomatic
Symptomatic MS

Intermediate Predictors
Minor Clinical Predictors
History of prior MI History of
compensated or prior heart failure
History of CVADMRenal
insufficiency/CKD
Advanced ageAbnormal ekg
LVH, LBBB, ST-T abnormalities
Rhythm other than sinus rhythm
Low functional capacity
ACC Guidelines—Clinical Risk Factors

Cardiac Risk Stratification for Surgical Procedures
High (cardiac risk > 5%)
Intermediate(cardiac risk 1-5%)
Low(cardiac risk <1%)
Aortic and major vascular surgery
Peripheral vascular surgery
Emergent major operations, esp in elderly
Prolonged surgeries associated with large fluid shifts or blood loss
Intraperitoneal or intrathoracic surgery
Carotid endarterectomy
Head and neck surgery
Orthopedic surgery Prostate surgery
Endoscopic procedures
Superficial procedure
Cataract Breast surgery Ambulatory
procedure

Cardiac Risk Evaluation
Surgery induces changes that predispose to ischemia Anemia Hypotension Hypothermia Increased catecholamine levels
The revised cardiac risk index is helpful to stratify risk

Revised Cardiac Risk Index6 factors that indicate increased risk
Ischemic heart diseaseCompensated or prior heart failureCerebrovascular diseaseDiabetes mellitusRenal insufficiency (creatinine > 2 mg/dL)High risk surgical procedure
Intraperitoneal/intrathoracic, vascular
Based on 4315 pts undergoing elective major surgery. Lee, TH et al, Circulation 1999, 100:1043-1049

Risk of Major Cardiac Event(Lee Criteria)
POINTS(# of risk factors)
CLASS RISK(%
complication)
0 I 0.4%
1 II 0.9%
2 III 6.6%
≥ 3 IV 11%“Major Cardiac Event” includes MI, pulm edema, vfib, cardiac arrest, complete heart block

Recommendations- Who needs these tests prior to surgery?
EKGCXRAssess LV function--echocardiogramNoninvasive stress testingPre-op coronary revascularizationBeta-blocker therapy

Who needs it? Relevant data
CAD or other CAD risk factors
Hypertension, diabetes
History of arrhythmia
? men > 40? Women > 50
ArrhythmiasIschemic changesProlonged QTc
EKG

Recommendations for Pre-op EKG
Class I & II 0-1 clinical risk factor & vasc surgery (LOE: B) 1 risk factor & intermediate risk surgery (LOE: B) Abnormal preoperative ekgs added no benefit in
predicting postoperative cardiovascular complications compared to a properly performed medical history.
Class III Not indicated in asymptomatic persons & low risk
procedure (LOE: B) Preoperative routine ekg testing in asymptomatic
patients undergoing low risk surgical procedures was found to be not only not useful, but harmful in some cases

Who needs it? Relevant data
ACTIVE pulmonary process
?? History of pulmonary disease
Highly overutilized!
Can have implications for anesthesia and/or prognosis
Facilitate peri-operative medical management
CHF
Chest Xray

Recommendation for Noninvasive Evaluation of LV
function
Class IIa Dyspnea of unknown origin (LOE: C) Current or prior HF with worsening dyspnea or other
change in clinical status (LOE: C) Rest echo for LV assessment should be considered in
patients undergoing high risk surgeryClass IIb
Stable cardiomyopathy may not need (LOE: C)Class III
Routine echo in pts not recommended (LOE: B)

Recommendations for Noninvasive Stress Testing
Stress testing has a very high negative predictive value for postoperative cardiovascular events (between 90-100%, but a low positive predictive value between 6-67%)
Stress testing is more useful for reducing estimated risk if negative (or normal) than for identifying patients at very high risk when positive
Less established evidence for the preoperative stress tests: Patients with at least one clinical risk factor and poor functional
capacity who are scheduled for intermediate risk surgery when such testing will change the management
Patients with at least one clinical risk factor and good functional capacity who are scheduled for vascular surgery.

Recommendations for Noninvasive Stress Testing
Class I Active cardiac conditions should be treated prior to
surgery (LOE: B)
Class IIa 3+ clinical risk factors & < 4 METS who require
vascular surgery (LOE: B) Stress testing considered when such testing will
change the management

Energy Requirements
1 MET Take care of self Eat, dress, use toilet
2-3 METs Walk indoors around the house Walk a block
4 METs Light housework like dusting or washing dishes

Energy Requirements
4-5 METs Climb stairs, walk up a hill
6-9 METs Run a short distance Heavy housework Moderate recreational activities
10 METs Strenuous activities (swimming, tennis, skiing)

Recommendations for Noninvasive Stress Testing
Class IIb- considered for: 1-2 clinical risk factors & < 4 METS & intermediate
risk surgery 1-2 clinical risk factors & > 4 METS & vascular
surgeryClass III
Not needed if no risk factors & intermediate surgery Not needed if low risk procedure

What stress test to order
Depends on the expertise of facilityExercise ekg
Sensitivity 74%, specificity 69%
MPI, mostly dipyridamole stress Sensitivity 83%, specificity 49%
Dobutamine echocardiography Sensitivity 85%, specificity 70%

Recommendations for Pre-op Revascularization with CABG or
PCI
Class I Stable angina & left main stenosis Stable angina & 3 vessel disease Stable angina & 2 vessel disease (prox LAD
stenosis) & either EF < 50% or ischemia on stress test
High risk unstable angina or NSTEMI Acute STEMI

PCI: angioplasty
Delay surgery for > 14 days to allow healing of vessel injury
Should continue aspirin perioperatively (vs bleeding risk)

PCI: bare-metal stent
Delay surgery for 4-6 wks to allow for at least partial endothelialization
Clopidogrel usually not needed after 4 wksShould continue aspirin perioperatively (vs
bleeding risk)

PCI: Drug-eluting stents
Delay surgery for 12 months due to risk of in-stent thrombosis
Should continue aspirin perioperatively (vs bleeding risk)
Thrombosis may occur up to 1.5 years after implantation, particularly in the context of discontinuing antiplatelet agents before surgery

Why perioperative Beta Blockade
Perioperative myocardial ischemia may be caused by an activation of sympathetic nervous system.
Beta blockade limits the increase in heart rate and myocardial contractility, prevents the imbalance of myocardial oxygen supply and demand
Diastolic time reduces rapidly above 75 bpm, as left ventricular coronary perfusion occurs predominately during the diastole
Beta blockers have antiarrhythmic and antirenin effects.

Perioperative Beta Blockade con’t
Perioperative increase in catecholamine and cortisol level contribute to increased oxygen demand and endothelial dysfunction mediated by a rise in the BP, HR
Beta blockers limit activation of inflammatory responses in the myocardium and systemic circulation
Beta blockers affects leukocyte chemotaxis and recruitment, metalloproteinase activity and monocyte activation.

Beta-blockers
Since 2002, few randomized trials have not demonstrated efficacy of beta-blockers but weight of evidence still suggests benefit esp high-risk pts
Should be started 7-10 days before elective surgery and continue up to 30 days
Long-acting agents may be better than short-acting ie metoprolol, atenolol

Beta-blocker therapy
Class I Continue if already on beta-blocker Vascular surgery & high cardiac risk (ischemia on pre-
op testing)Class IIa- probably recommended for:
Vascular surgery & coronary disease Vascular surgery & > 1 clinical risk factor Intermediate surgery & > 1 clinical risk factor

Beta-blocker therapy
Class IIb- uncertain for: Intermediate/high risk surgery & 1 clinical risk factor High risk/Vascular surgery & no clinical risk factors
Class III Do not use with Contraindication to beta-blockers Routine administration of high-dose beta blockers w/o
dose titration is not useful and may be harmful to pts
not currently taking beta blockers (POISE trial)

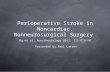
Poise Trial Results
0
1
2
3
4
5
6
30d nonfatal mi all cause mort cva
Placebometoprolol
Reduction in nonfatal mi; significant hypotension, bradycardia; increase mortalityEvidence does not support the use of beta blocker for the prevention of perioperative clinicaloutcomes in patients having noncardiac surgery.

Decrease IV Trial
Beta blocker group had a lower incidence of perioperative cardiac death and nonfatal MI
Beta blocker group had significant reduction of 30 day cardiac death and nonfatal MI
Use of statins showed a trend for improved outcome

Beta-blockers
Accumulating evidence suggests HR target is 60-80 beats/min
Should continue beta-blocker therapy through peri-op period & titrate to tight HR control
Start at a low dose and gradually up-titrate in a week.
Follow conventional dosing and holding parameters Hold if HR< 50 bpm; Systolic BP< 100

ACC/AHA 2007 Guidelines
How do we risk stratify?

ACC Algorithm for 2007

Misc Points
Pre-op labsMedicationsPulmonary issuesCerebrovascular issueChronic anticoagulationDVT prophylaxisCode status

Pre-op lab testing
Order fewer selective, evidence based tests30-60% of abnormalities found on pre-op
tests are generally ignored anywayLab tests normal in last 4 months and no
clinical change probably do not require repeat tests

Labs Studies: Hematology
H/H Anemia suspected. High surgical blood loss possible
WBC Clinic signs of infections *usually of little value
Platelets History of bleeding. High risk if surgical blood loss occurs (intracranial, spinal)
PT/PTT/INR History of bleedingSuggestive history (liver disease)High risk of surgical bleeding.

Lab Studies: Chemistry
Electrolytes Medications that can affect this (bp meds, diuretics)Dehydration: other clinical signs
BUN/Cr Clinical history with risk of renal diseaseCardiac or pulmonary disease
Glucose Poorly controlled diabetes
Liver function tests
Suggestive clinical historyAlbumin is part of pulmonary risk model
Urinalysis Clinical signs of infection*usually of little value

Medications
Continue beta-blockers, oral nitrates, & most antihypertensives until the morning of surgery
Suggest holding ACE-I & ARBs on morning of surgery to decrease risk of renal dysfunction Inhibition of ACE may prevent events related to
myocardial ischemia and LV dysfunction Perioperative treatment with ACE inhibitors may have
beneficial effects on post-operative outcomes Noted increase risk on renal failure in patients
undergoing CV surgery

Diuretics
Hypertensive patients -- discontinue diuretic on the day of surgery and resume orally when possible
Heart failure patients -- Continue use up to the day of surgery, resume intravenously perioperatively, and continue orally when possible
Correct electrolytes before surgery

Other Medications
Aspirin, aggrenox, clopidogrel- stop 7 days prior
Cilastazol, COX-1 inh cause reversible platelet inhibition- stop 2-3 days prior
COX-2 inh do not affect platelets

Other Medications
NSAIDS affect renal function- stop 1-3 days prior
SSRIs increase bleeding by depleting serotonin stores- stop days prior depending on half-life
Hormones, Raloxifene, Tamoxifen increase risk of thromboemboli
Anti-convulsant/psychotic/depressant meds should be continued
Metformin held to reduce lactic acidosis

Herbal Medications
Supplements or herbal meds- stop 1 wk prior Ginger, ginkgo, ginseng, garlic, & feverfew can cause
bleeding Ginseng assoc w/ hypoglycemia Garlic assoc w/ hypoglycemia, hypotension Kava, echinacea assoc w/ hepatotoxicity

What about statins?
Several observational studies suggest benefit from peri-operative statins.
Randomized trials less clearBottom line-prescribe only if statin is
indicated regardless of surgery

Endocarditis prophylaxis
Revised recommendations have limited indications Prosthetic valve Previous endocarditis Cardiac transplantation with valvulopathy Certain congenital heart diseases
Cyanotic, recent use of prosthetic material, residual defects
Indicated only for Dental, respiratory, skin/soft-tissue/muscular
procedures Not for GI/GU

Preoperative Pulmonary Assessment and
Postoperative Risk Reduction
Patient Factors Advanced Age Poor functional status COPD CHF Tobacco abuse OSA Low albumin, high BUN
Surgical Factors Aortic, thoracic, upper
abdominal Prolonged surgery General anesthesia Emergency surgery Routine NG tube placement

Preoperative Pulmonary Function Testing
Indicated for all lung resection patientsFail to consistently predict pulmonary complications
Abnormal exam, CXR, and Goldman risk index more predictive Low rate of complications in patients with severe obstruction Use the “if they walked into my office” principle
Evaluate unexplained dyspnea Establish baseline for patients with known lung disease

Reducing Postoperative Pulmonary Complications
Incentive SpirometerSelective NG decompression after general surgeryCigarette cessation*Medically optimize COPDAvoid sedating medsNeuraxial anesthesia
No clear benefit with Nutritional supplementation Pulmonary arterial catheterization
*If pt stops smoking for <8 weeks prior to surgery, rates of pulm complications may be higher than not stopping at all.

Cerebrovascular risk evaluation
Vascular and cardiac surgery pose greatest risk of stroke
Principle risk factor is symptomatic carotid stenosis
Carotid revascularization should strongly be considered in these pt’s prior to vascular/cardiac surgery Unclear benefits of stenting vs surgery or other types
of surgeryNo evidence of benefit for asymptomatic
carotid stenosis

CHADS2 score
1 pt each Heart failure (EF < 30%) HTN age ≥ 75 yrs diabetes
2 pts Prior stroke

Low Bleed Risk
Continue warfarin (can consider lower INR of 1.3-1.5) Cataract Endoscopy, colonoscopy, ERCP w/o sphincterotomy Superficial dermatologic Dental procedures Joint and soft tissue aspirations or injections Minor podiatric procedures (nail avulsions)

Low risk- bridging not advised
One remote VTE (>6 months ago)Intrinsic cerebrovascular disease (carotid
atherosclerosis) w/o recurrent stroke or TIAAtrial fib w/o multiple risks for cardiac
embolism (CHADS2 1-2)Newer model mech valve in aortic position
(St. Jude)

High Risk- Bridging advised
DVT/PE or arterial thromboemboli < 3 moThromboembolic event + hypercoaguable problem
(i.e. protein C or S def…)Recurrent arterial or idiopathic VTERheumatic atrial fibAcute intracardiac thrombusAtrial fib + mech heart valve in any positionOlder mech valves in mitral position (single disk or
ball-in-cage)Recently placed mech valve (<3 months)Atrial fibrillation with h/o cardioembolism

Intermediate Risk- Bridging on case-by-case basis
Newer model mech valve in mitral position (St. Jude)
Older model mech valve in aortic positionAtrial fib w/o cardioembolism but with
multiple risks for cardioembolism (CHADS2 ≥ 3)
VTE > 3-6 months ago

DVT prophylaxis
DVT riskUp to 30% in general
surgeryUp to 60% in
orthopedic surgery Especially hip fracture
surgery

2008 ACCP guideline VTE prophylaxisNon-orthopedic surgery
Pharmacologic prophylaxis with UH, LMWH, or fondaparinux should be considered for all but the lowest risk ambulatory surgical patients
Add mechanical compression for those at highest risk
Continue until discharge Consider continuing LMWH for 28 days after discharge
in highest risk
Prophylaxis may be omitted in entirely laparoscopic procedures without other risk factors.

2008 ACCP guideline VTE prophylaxisOrthopedic surgery
Procedure Prophylaxis Duration
Total hip replacement LMWH 10 – 35 days
Total knee replacement
LMWH, fondaparinux therapeutic warfarin
10 – 35 days
Knee arthroscopy (uncomplicated)
Ambulation N/A
Knee arthroscopy (complicated)
LMWH until discharge
Hip fracture surgery LMWH, fondaparinux, therapeutic warfarin
10 – 35 days
Mechanical compression
Use alone if high bleeding risk and in combination for very high risk patients.

What to do with a DNR?
Anesthetic or surgical techniques may be considered resuscitative
Some procedures cause asystoleCounsel patients on how to manage the DNR
peri-operativelyInstitutional policies may dictate
OSU recommends suspending the DNR until leaving the PACU or for 24 hours in SICU

Conclusions
Successful peri-operative evaluation and management requires careful teamwork
Use of noninvasive and invasive pre-op testing should be limited to circumstances in which the results will affect pt management
Goal is to make recommendations to lower immediate peri-operative cardiac risk

References
Fleisher, LA, et al., ACC/AHA 2007 Guidelines on Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery: Executive Summary, Circulation, Oct 23, 2007, 1-26.
Beckman, JA, et al., ACC/AHA 2006 Guidelines on Perioperative Cardiovascular Evaluation and Care for Noncardiac Surgery: Focused Update on Perioperative Bets-Blocker Therapy, JACC, Vol. 47.
Lee, TH, et al., Derivation and prospective validation of a simple index for prediction of cardiac risk in major noncardiac surgery. Circulation 1999;100:1043-1049.
Geerts, WH, et al. Prevention of venous thromboembolism: American college of chest physicians evidenced-based clinical practice guidelines (8th edition). Chest 2008; 133: 381S-453S.
King MS. Preoperative evaluation. Am Fam Physician. 2000; 62:387-396.

Review questions
Which of the following must occur before EVERY surgery can safely be performed?
a. The patient must be medically “cleared” by their physician
b. The patient must undergo EKG and basic labs testsc. The patient must have a discussion of the risks and
benefits of the surgery and provide informed consent
d. Both a and c

Which of the following patients should receive beta-blockers before elective surgery?
a. 50 year old male scheduled for inguinal hernia repair who has past medical history of hypertension
b. 34 year old female scheduled for hysterectomy with history of poorly controlled type 1 dm, ckd with cr 3, and well controlled asthma on steroid inhaler and albuterol.
c. 55 year old female scheduled for lumpectomy for breast cancer with history of stroke at age 40 due to inherited thombophilia and takes warfarin
d. None of the above.

Which of the following patients should hold their respective anti-hypertensive on the morning of surgery?
a. 50 year old with hypertension and history of MI on metoprolol
b. 35 year old female with dm, ckd taking lisinopril
c. 78 year old male with CHF and EF 25% taking losartan whose dose was decreased recently due to low bp
d. Both b and c.

Which of the following patients should undergo stress testing prior to surgery?
a. 75 yo scheduled for hemicolectomy for colon ca with history of RCA stent 18 months ago. Able to walk and swim without anginal symptoms
b. 65 yo female with dm, htn, cad scheduled for lumpectomy. Wheelchair bound due to obesity and lymphedema. No chest pain or dyspnea
c. 80 yo with dm, htn scheduled for total hip replacement. No chest pain or dyspnea with walking.
d. 40 yo with no pmh scheduled for abdominoplasty. Reports over the past 1-2 months chest tightness while running that is increasingly precipitated by less activity.

For questions or comments contact:Jayne Barr, MD FACP FAAPEmail: [email protected]

Survey
We would appreciate your feedback on this module. Click on the button below to complete a brief survey. Your responses and comments will be shared with the module’s author, the LSI EdTech team, and LSI curriculum leaders. We will use your feedback to improve future versions of the module.
The survey is both optional and anonymous and should take less than 5 minutes to complete.
Survey
Related Documents