DOI: 10.1016/j.athoracsur.2006.05.037 2006;82:1679-1687 Ann Thorac Surg Friedhelm Beyersdorf Sircar, Gàbor Szabò, Christian D. Etz, Maximilian Luehr, Patrick von Samson and Ernst Weigang, Marc Hartert, Michael P. Siegenthaler, Nicholas A. Beckmann, Ronen Thoracoabdominal Aortic Stent-Grafting Perioperative Management to Improve Neurologic Outcome in Thoracic or http://ats.ctsnetjournals.org/cgi/content/full/82/5/1679 located on the World Wide Web at: The online version of this article, along with updated information and services, is Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2006 by The Society of Thoracic Surgeons. is the official journal of The Society of Thoracic Surgeons and the The Annals of Thoracic Surgery by on May 30, 2013 ats.ctsnetjournals.org Downloaded from

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

DOI: 10.1016/j.athoracsur.2006.05.037 2006;82:1679-1687 Ann Thorac Surg
Friedhelm Beyersdorf Sircar, Gàbor Szabò, Christian D. Etz, Maximilian Luehr, Patrick von Samson and
Ernst Weigang, Marc Hartert, Michael P. Siegenthaler, Nicholas A. Beckmann, Ronen Thoracoabdominal Aortic Stent-Grafting
Perioperative Management to Improve Neurologic Outcome in Thoracic or
http://ats.ctsnetjournals.org/cgi/content/full/82/5/1679located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Print ISSN: 0003-4975; eISSN: 1552-6259. Southern Thoracic Surgical Association. Copyright © 2006 by The Society of Thoracic Surgeons.
is the official journal of The Society of Thoracic Surgeons and theThe Annals of Thoracic Surgery
by on May 30, 2013 ats.ctsnetjournals.orgDownloaded from
POSENMDCC
smanpgthd
pim3t
fw
Tpmira
ifAtdip
A
PT
ASF
©P
CA
RD
IOV
ASC
ULA
R
erioperative Management to Improve Neurologicutcome in Thoracic or Thoracoabdominal Aortictent-Grafting
rnst Weigang, MD, Marc Hartert, Michael P. Siegenthaler, MD,icholas A. Beckmann, Ronen Sircar, MD, Gàbor Szabò, MD, Christian D. Etz, MD,aximilian Luehr, Patrick von Samson, MD, and Friedhelm Beyersdorf, MD
epartments of Cardiovascular Surgery and Neurosurgery, University Hospital Freiburg, Freiburg, Germany; Department ofardiac Surgery, University Heidelberg, Heidelberg, Germany; and Department of Cardiothoracic Surgery, Mount Sinai Medical
enter, New York, New YorkEt(cbwet
fpsmoiua
Background. Thoracic or thoracoabdominal aortictent-graft repair has shown a reduction in morbidity andortality rates due to the procedure’s advantages (no
ortic cross-clamping, continuous distal aortic perfusion,o reperfusion injury). However, 3% to 12% of theatients are at risk of spinal cord ischemia. We investi-ated spinal cord protective measures with evoked po-entials, cerebrospinal fluid drainage, and prevention ofypotension to minimize postoperative neurologiceficit.Methods. Between November 2000 and July 2005, vital
arameters and spinal cord function were monitored,ncluding cerebrospinal fluid pressure and transcranial
otor-evoked and somatosensory-evoked potentials in6 stent-graft procedures (31 patients) on the thoracic orhoracoabdominal aorta.
Results. Stent-graft placement was technically success-ul in all patients. We achieved a survival rate of 100%
ithout neurologic deficit after fast-track extubation.pitsatdatta
toapsitsh
urgery, University Hospital Freiburg, Hugstetter Strasse 55, 79106reiburg, Germany; e-mail: [email protected].
2006 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
leven of 31 patients exhibited changes in evoked poten-ials during stent-graft deployment. In 12 of 31 patientsincluding the 11 with evoked potential alterations),erebrospinal fluid pressure exceeded 15 mm Hg. Cere-rospinal fluid drainage and vital parameter adjustmentere executed in those instances. We observed intraop-
rative evoked potential total recovery in 10 of 11 pa-ients after these interventions.
Conclusions. Interventions to improve spinal cord per-usion led to total recovery of spinal function in mostatients (10/11). Therefore, spinal cord protective mea-ures with motor- and somatosensory-evoked potentialonitoring, cerebrospinal fluid drainage, and prevention
f hypotension can reduce the incidence of spinal cordschemia and improve the neurologic outcome of patientsndergoing endovascular thoracic or thoracoabdominalortic repair.
(Ann Thorac Surg 2006;82:1679–87)
© 2006 by The Society of Thoracic Surgeonshe most dreaded complication of conventional openthoracic or thoracoabdominal aortic repair is para-
legia, which occurs in up to 21% of patients [1–4]. Theain risk factors for spinal cord damage are spinal cord
schemia during the aortic cross-clamping, unsuccessfuleimplantation of segmental arteries, and cytotoxic dam-ge caused by hypotension [5].After successful reimplantation of the segmental arter-
es, reperfusion injury can occur as cytotoxic metabolites,ormed during aortic clamping, are flushed back [6].nother mechanism for spinal cord ischemia is a rise in
he volume of blood supplied to the brain that occursuring cross-clamping and, in turn, leads to an increase
n intracranial pressure (ICP) and a drop in spinal corderfusion. Different surgical techniques and strategies to
ccepted for publication May 11, 2006.
resented at the Poster Session of the Forty-second Annual Meeting ofhe Society of Thoracic Surgeons, Chicago, IL, Jan 30–Feb 1, 2006.
ddress correspondence to Dr Weigang, Department of Cardiovascular
rotect the spinal cord have been described to reduce thencidence of spinal cord ischemia, including identifica-ion and reimplantation of critical segmental arteries,ystemic hypothermia, adjunctive pharmacologic ther-py, and cerebrospinal fluid (CSF) drainage [7]. Despitehese measures, the risk of postoperative neurologiceficits in patients with thoracic or thoracoabdominalortic open surgical repair remains significant. All in all,he main cause for spinal cord ischemia during openhoracic or thoracoabdominal aortic surgical repair isortic cross-clamping.CSF drainage has been used as an adjunct during
horacic or thoracoabdominal aortic open surgical repairver the last 15 years [8–11]. The rationale is based onnimal experiments that suggest that decreasing the CSFressure during cross-clamping of the aorta enhancespinal cord perfusion and thereby decreases the risk ofschemia-induced paraplegia. Specifically, a decrease inhe distal aortic pressure also causes a decrease in thepinal artery pressure. Therefore femorofemoral or left
eart bypass is used after the proximal aorta is cross-0003-4975/06/$32.00doi:10.1016/j.athoracsur.2006.05.037
by on May 30, 2013 als.org
ciicsataddd
tdtsmctn
vpTatbpusrr
nmsrco
tnppgi
M
DpJmtacaa3t(d
prtCr
Ta
A
R
C
P
MS
a
dcm
C
T
a
Dt
1680 WEIGANG ET AL Ann Thorac SurgIMPROVED OUTCOME AFTER STENT-GRAFTING 2006;82:1679–87
CA
RD
IOV
ASC
ULA
R
lamped to improve the distal aortic pressure by increas-ng the extracorporeal circulatory pump flow. A concom-tant rise in the CSF pressure can lead to a spinal cordompartment syndrome [12]. By draining CSF, the pres-ure is reduced, relieving the compartment syndromend increasing the perfusion to the spinal cord. Thisheory is supported in a recent clinical literature reviewrticle analyzing a large number of patients from manyifferent institutions undergoing thoracic or thoracoab-ominal surgery with and without concomitant CSFrainage [11].Intraoperative neurophysiologic monitoring is another
echnique implemented in open thoracic or thoracoab-ominal aortic surgery. Here, the functional integrity of
he spinal cord can be evaluated by measuring somato-ensory-evoked potentials (SSEPs) as well as transcranialotor-evoked potentials (tcMEPs), which exhibit a
hange upon induced ischemia. Studies have supportedhe value of this technique in thoracic or thoracoabdomi-al aortic open surgical repair [13–18].The interventional aortic repair technique with endo-
ascular stent-graft implantation enhances the generalrospects of a positive outcome for these patients [19].he stent-graft implantation technique itself has severaldvantages. Aortic cross-clamping is not necessary, andhe proximal hypertension with negative effects on cere-rospinal cord perfusion are thus avoided. Distal aorticerfusion remains uninterrupted, guaranteeing a contin-ous blood flow to the spinal cord. During endovasculartent-graft implantation, segmental arteries were noteimplanted. Thus, this technique is not accompanied byeperfusion injury to the spinal cord. The frequency of
able 1. Preoperative Risk Factors, Comorbidity, Priorities,nd Demographic Data
neurysm EtiologyAtherosclerotic(n � 17)a (%)
Dissection(n � 14)a (%)
isk factorsArterial hypertension 13 (76) 12 (86)Hyperlipidemia 7 (41) 3 (21)Diabetes 9 (53) 4 (29)Smoking history 8 (47) 2 (14)
omorbidityCoronary arterydiseaseb
10 (59) 4 (29)
Renal insufficiencyc 8 (47) 5 (36)COPD 8 (47) 1 (7)
riorityElective 6 (35) 2 (14)Urgent 9 (53) 7 (50)Emergent 2 (12) 5 (36)ean age (range) in years 69 (39–81) 62 (53–78)
ex ratio (male/female) 9:7 12:3
Data are numbers (%) or mean (Range) b Criteria for coronary arteryisease: stenosis of the coronary arteries � 50% (stenosis hemodynami-ally effective) c Criteria for renal insufficiency: serum creatinin � 1.4g/dL
rOPD � Chronic obstructive pulmonary disease
ats.ctsnetjournDownloaded from
eurologic complications with this minimally invasiveethod appears to be reduced compared with open
urgical aortic repair. However, endovascular stent-graftepair of the thoracic or thoracoabdominal aorta is asso-iated with a risk of perioperative spinal cord ischemiaccurring in 3% to 12% of patients [20–25].The aim of our study was to evaluate whether adjunc-
ive techniques such as CSF drainage combined witheurophysiologic monitoring (SSEPs and tcMEPs) andrevention of hypotension can reduce the risk of para-legia and decrease the mortality rate in patients under-oing thoracic or thoracoabdominal stent-graft
mplantation.
aterial and Methods
uring 36 thoracic and thoracoabdominal stent-graftrocedures in 31 patients between November 2000 and
uly 2005, vital parameters and spinal cord function wereonitored, including cerebrospinal fluid pressure,
cMEPs, and SSEPs. The indication for thoracoabdominalortic stent-graft repair was set in patients with a highomorbidity rate and reduced life expectancy, for whomn open surgical procedure would be too hazardous. Theneurysms were caused by atherosclerosis in 17 (55%) of1 patients and dissection in 14 (45%). The mean age ofhe patients with atherosclerotic aneurysms was 69 yearsrange, 39 to 81 years). The mean age of the patients withissection was 62 years (range, 53 to 78 years) (Table 1).Of the 31 patients who had procedures, 13 of the
atients with atherosclerotic aneurysms were catego-ized according to the Crawford classification (CC) sys-em (type I to IV): CC type I, 1 (3%); CC type II, 6 (19%);C type III, 4 (13%); and CC type IV, 2 (7%) (Table 2). The
emaining 4 patients (13%) showed atherosclerotic aneu-
able 2. Aneurysm Etiology and Crawford Extent Type
n (%)
Atherosclerosis 17 (55)DTA 4 (13)CC type I 1 (3)CC type II 6 (19)CC type III 4 (13)CC type IV 2 (7)
Acute dissection (All type B) 5 (16)LSA to proximal RA 2 (6)LSA to below RA 3 (10)
Chronic dissectionType Aa 3 (10)Type Ba 6 (19)CC type I 3 (10)CC type II 5 (16)CC type III 1 (3)
With secondary development of an aortic aneurysm.
TA � descending thoracic aorta; CC � Crawford Classifica-ion; LSA � left subclavian artery; RA � renal arteries.
ysms only in the area of the descending thoracic aorta.
by on May 30, 2013 als.org

Ttrrr
AabCabisb25pthoitrnoi(
tppmrSaac
piptnc
EAdmpt(TZuw
tp
rovtatam
Fdpsa
1681Ann Thorac Surg WEIGANG ET AL2006;82:1679–87 IMPROVED OUTCOME AFTER STENT-GRAFTING
CA
RD
IOV
ASC
ULA
R
he procedures in 6 aneurysm patients (35%) were elec-ive, urgent in 9 (53%) with acute pain but no signs ofupture on CT-scan, and emergent in 2 (12%) withupture (Table 1). In patients with atherosclerotic aneu-ysms, we covered the widening of the aorta.
Of the 14 patients with dissections, 3 had chronic typedissections with secondary formation of an aortic
neurysm (1 CC type I, 2 CC type II). An aortic aneurysmased on a type-B dissection developed in 6 patients (2C type I, 3 CC type II, 1 CC type III). Five patients hadn acute type B dissection. In 2 patients, the dissectionegan past the left subclavian artery and extended prox-
mally as far as the renal arteries; in 3 patients with theame location of the entry, the dissection extended up toelow the renal arteries. The procedures were elective in(14%), urgent in 7 (50%), and emergent in 5 (36%). In thepatients with acute, complicated type B dissection, theroximal entry was primarily covered to correct persis-
ent pain refractory to medical treatment, persistentypertension despite medical therapy, contain rupturen CT scan, or correct malperfusion in one or more of the
ntestinal, renal or pelvic arteries, and thus to reestablishhe continuity of perfusion in those regions. Each patienteceived a variety of intraoperative monitoring tech-iques including CSF pressure monitoring, neurophysi-logic monitoring with tcMEPs and SSEPs, and monitor-
ng of vital parameters with mean arterial pressureMAP) and central venous pressure (CVP).
High-risk patients were defined as 11 with a distincthoracoabdominal aneurysm of the aorta and 5 withrevious open surgical infrarenal aortic replacement. Atarticularly high risk were 11 patients who receivedultiple stent-graft implantations and 2 patients who
eceived infrarenal Y-Dacron (Vascutek Ltd, Glasgow,cotland) prostheses with occlusion of the internal iliacrteries and occlusion of a high number of segmentrteries caused by poor collateral flow into the spinalord.
The university ethics committee reviewed and ap-roved the study (study approval number 108/2001). Full
nformed consent was obtained from all patients forarticipation in the study, including stent-graft implan-
ation, neurophysiologic monitoring, placement of a spi-al catheter to measure and drain spinal fluid, and dataollection with analysis.
ndovascular Stent-Graft Implantationll patients received preoperative CT or angiography toetermine individual aortic anatomy and obtain exacteasurements for stent-graft sizing (Fig 1). All stent-graft
rocedures were performed in the operating room bywo cardiovascular surgeons. Endovascular stent-graftsTalent and Valiant, Medtronic AVE, Minneapolis, MN;AG Excluder, W. L. Gore and Assoc, Flagstaff, AZ; andenith, Cook Group Inc, Bloomington, IN) were placednder fluoroscopic guidance. No branched stent-graftsere used.The patients were in the supine position. For implan-
ations near the aortic arch, a roll was placed under each
atient’s left side for the left anterior oblique views wats.ctsnetjournDownloaded from
equired for precise positioning. After exposing the fem-ral artery and correctly positioning the stent-graft de-ice, the self-expanding endoprosthesis was deployed inhe target region of the thoracic or thoracoabdominalorta. Intraoperative angiography was used to confirmhe stent-graft position and patency of aortic branchesnd to exclude endoleaks. In cases of endoleaks and forost Talent and Valiant implantations, the stent-graft
ig 1. Preoperative angiography of a Crawford type II thoracoab-ominal aortic aneurysm. The greatest widening of the aorta isresent in the thoracic and infrarenal areas. The aorta is onlylightly widened in the area surrounding the visceral and renalrteries.
as subsequently molded by balloon catheter. If neces-
by on May 30, 2013 als.org
scsl
ATctflmtgbtaoi
SWisatmgcm1mcIH
CWerwsmwIttdtKCtmbiraterinaucs
IAtvip
tcoa
Fttai
1682 WEIGANG ET AL Ann Thorac SurgIMPROVED OUTCOME AFTER STENT-GRAFTING 2006;82:1679–87
CA
RD
IOV
ASC
ULA
R
ary, an additional stent-graft was placed. Before dis-harge, all patients underwent CT scanning to checktent-graft position and exclude endoleak and stent dis-ocation (Fig 2).
nesthesia Managementhe anesthesiologist, neurophysiologist, and cardiovas-ular surgeon collaborated in the stent-graft implanta-ion. Because a complete neuromuscular blockade con-icts significantly with the ability to perform tcMEPonitoring [26–28], vecuronium was applied as a short-
erm muscle relaxant only once at the beginning ofeneral anesthesia. Benzodiazepine (0.01 to 0.03 mg/kgody weight) was given for sedation, and fentanyl (0.004
o 0.007 mg/kg body weight) was administered as annalgesic. Patients were not given any further relaxantsr inhaled anesthetics during the operation to prevent
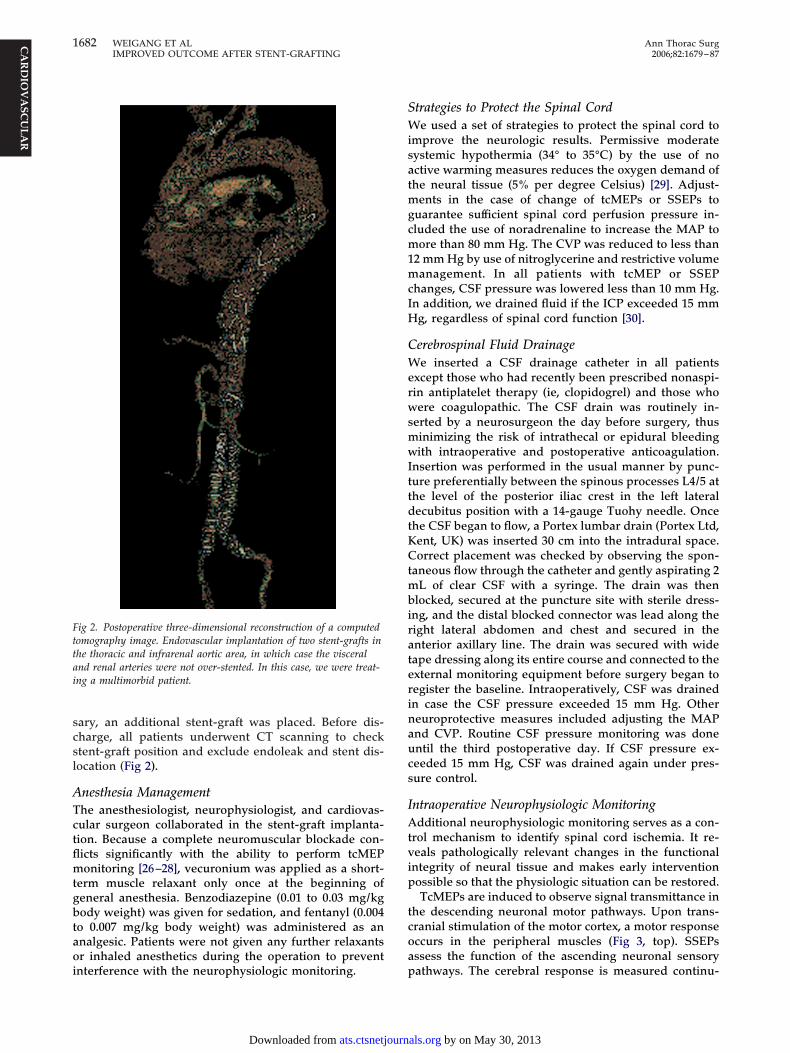
ig 2. Postoperative three-dimensional reconstruction of a computedomography image. Endovascular implantation of two stent-grafts inhe thoracic and infrarenal aortic area, in which case the visceralnd renal arteries were not over-stented. In this case, we were treat-ng a multimorbid patient.
nterference with the neurophysiologic monitoring. p
ats.ctsnetjournDownloaded from
trategies to Protect the Spinal Corde used a set of strategies to protect the spinal cord to
mprove the neurologic results. Permissive moderateystemic hypothermia (34° to 35°C) by the use of noctive warming measures reduces the oxygen demand ofhe neural tissue (5% per degree Celsius) [29]. Adjust-
ents in the case of change of tcMEPs or SSEPs touarantee sufficient spinal cord perfusion pressure in-luded the use of noradrenaline to increase the MAP toore than 80 mm Hg. The CVP was reduced to less than
2 mm Hg by use of nitroglycerine and restrictive volumeanagement. In all patients with tcMEP or SSEP
hanges, CSF pressure was lowered less than 10 mm Hg.n addition, we drained fluid if the ICP exceeded 15 mmg, regardless of spinal cord function [30].
erebrospinal Fluid Drainagee inserted a CSF drainage catheter in all patients
xcept those who had recently been prescribed nonaspi-in antiplatelet therapy (ie, clopidogrel) and those whoere coagulopathic. The CSF drain was routinely in-
erted by a neurosurgeon the day before surgery, thusinimizing the risk of intrathecal or epidural bleedingith intraoperative and postoperative anticoagulation.
nsertion was performed in the usual manner by punc-ure preferentially between the spinous processes L4/5 athe level of the posterior iliac crest in the left lateralecubitus position with a 14-gauge Tuohy needle. Once
he CSF began to flow, a Portex lumbar drain (Portex Ltd,ent, UK) was inserted 30 cm into the intradural space.orrect placement was checked by observing the spon-
aneous flow through the catheter and gently aspirating 2L of clear CSF with a syringe. The drain was then
locked, secured at the puncture site with sterile dress-ng, and the distal blocked connector was lead along theight lateral abdomen and chest and secured in thenterior axillary line. The drain was secured with wideape dressing along its entire course and connected to thexternal monitoring equipment before surgery began toegister the baseline. Intraoperatively, CSF was drainedn case the CSF pressure exceeded 15 mm Hg. Othereuroprotective measures included adjusting the MAPnd CVP. Routine CSF pressure monitoring was donentil the third postoperative day. If CSF pressure ex-eeded 15 mm Hg, CSF was drained again under pres-ure control.
ntraoperative Neurophysiologic Monitoringdditional neurophysiologic monitoring serves as a con-
rol mechanism to identify spinal cord ischemia. It re-eals pathologically relevant changes in the functionalntegrity of neural tissue and makes early interventionossible so that the physiologic situation can be restored.TcMEPs are induced to observe signal transmittance in
he descending neuronal motor pathways. Upon trans-ranial stimulation of the motor cortex, a motor responseccurs in the peripheral muscles (Fig 3, top). SSEPsssess the function of the ascending neuronal sensory
athways. The cerebral response is measured continu-by on May 30, 2013 als.org

o(mmtSuipreegpoIG
oo6tf
plrg3t
rdtsabcirttgva
eapatpit
R
Sp1raaiotrasgoo
atpptwt
e(
Fm(G
1683Ann Thorac Surg WEIGANG ET AL2006;82:1679–87 IMPROVED OUTCOME AFTER STENT-GRAFTING
CA
RD
IOV
ASC
ULA
R
usly after electrical stimulation of a peripheral nerveFig 3, bottom). Both the tcMEP and SSEP monitoring
ethods assess spinal cord function and have a comple-entary controlling character: tcMEP recordings reflect
he functional integrity of the anterolateral tract, andSEP recordings the posterior tract of the spinal cord. Wesed the 10-20 system for electroencephalogram record-
ngs, in which tcMEP stimulation electrodes are attachedercutaneously in the area corresponding to the C3/C4egion of the motor cortex, and the SSEP recordinglectrodes are positioned at Cz/Fz [31]. TcMEP recordinglectrodes are placed into the anterior tibial muscles andastrocnemius muscles. SSEP stimulating electrodes areercutaneously inserted lateral and caudal to the malle-lus medialis to stimulate the tibial nerve (EWACS andSIS IOM; inomed, Medizintechnik GmbH, Teningen,ermany) [31].Stimulation impulses for the tcMEPs consist of a series
f five anodal impulses each lasting 200 to 400 �s at a ratef 200 to 500 Hz. These tcMEPs are carried out every 30 to0 seconds by a direct current electrical stimulator (Digi-imer DS7H; Digitimer Ltd, Welwyn Garden City, Hert-
ig 3. Normal transcranial motor-evoked potentials (top) and so-atosensory-evoked potentials (bottom) during stent graft procedure
ISIS IOM system; inomed Medizintechnik GmbH, Teningen,ermany).
ordshire, UK). The patient is grounded by use of a e
ats.ctsnetjournDownloaded from
ercutaneous needle electrode fixed between the stimu-ating and recording electrodes (preferably in the kneeegion). With this method, the resulting electromyo-raphic response does not require signal averaging (Fig). To change the stimulation side, we alter the polarity ofhe stimulus.
After the patient has been anesthetized, a baselineecording is made. The baseline guarantees a correctefinition of the patient’s preoperative spinal cord func-
ion. The basic method to gain SSEP recordings involvesignal averaging. Usually, the responses of 200 stimulire averaged because of the relatively long distanceetween the recording electrodes and the somatosensoryortex [31]. This removes any “noise” and allows for annterpretable signal. It is important to obtain the baselineecordings before surgery, because interference fromechnical equipment precludes viable recordings. Fur-hermore, the comparison between intraoperativelyained potentials and the patient’s individual baselinealues enables the neurophysiologic monitoring team tossess acute spinal cord function [16, 17].The sequence and placement of tcMEP and SSEP
lectrodes follows a careful plan to avoid hindering thenesthetic preparations and to save precious time. Thelacement of the percutaneous needle electrodes occursfter the patient has been anesthetized and positioned onhe operating table. Once placed, the electrodes canrovide stable recordings for many hours, even once the
ntervention has ceased [31]. We stopped recording afterhe patients were awake.
esults
tent-graft placement was technically successful in allrocedures, and the postprocedure survival rate was00%. Six patients with thoracoabdominal aortic aneu-ysms (4 CC type II, 2 CC type III) received a thoracic andbdominal stent-grafts in which the visceral and renalrteries were not over-stented (Fig 1 and 2). Those casesnvolved multimorbid patients who could not undergopen surgical aortic replacement. Three had postopera-ive complications. Because of a type I endoleak thatesulted from incomplete sealing of the device at thettachment site, 2 patients had to undergo additionaltent-graft implantation. One patient had bleeding in theroin that had to be revised. There were no other post-perative complications, including no malperfusion orther vascular complications.The 5 patients with acute type B dissection still showedslight retrograde flow in the false lumen postopera-
ively that was barely noticeable at discharge. The rate ofostoperative complications was also minor in thoseatients who presented with high perioperative risk in
erms of a potential spinal cord ischemia, namely thoseith an extensive thoracoabdominal aortic aneurysm or
hose with previous surgery on the abdominal aorta.We performed neurophysiologic monitoring during
ndovascular stent-graft implantation in 36 procedures31 patients). Both tcMEPs and SSEPs remained intraop-
ratively stable in 20 (65%) of 31 patients. We recorded aby on May 30, 2013 als.org
liI1stasSa(nris(ipibettat
Cdcmpascot
npi
t1etsdrwp
C
SdrtsnittctH
rppptntsrisast
T
C
I
P
a
Cp � soC
1684 WEIGANG ET AL Ann Thorac SurgIMPROVED OUTCOME AFTER STENT-GRAFTING 2006;82:1679–87
CA
RD
IOV
ASC
ULA
R
oss or changes of evoked potentials (tcMEPs and SSEPs)n 11 patients (35%) (3 CC type I, 3 CC type II, 2 CC typeII, 1 CC type IV, 1 descending thoracic aortic aneurysm,acute Stanford type B dissection) immediately after the
tent-graft deployment (Table 3). We observed a loss incMEPs in 3 patients (10%), with 1 to 2 minutes’ latencyfter stent-graft deployment. Seven patients (23%)howed a drop in tcMEP amplitudes of 50% to 70%. TheSEP amplitudes decreased during the 7 to 12 minutesfter the deployment of the stent-grafts in 8 patients26%) and disappeared briefly in 4 patients (13%). Inone of these cases was intraoperative blood loss theeason behind the loss of the evoked potentials. Thencidences of neurophysiologic potential decrease in ourtudy were accompanied by decreases in blood pressure42%) and heart rate (31%). In addition, we recorded anncrease in CVP by 76% and in ICP by 112% in thoseatients. These comparisons are based on each patient’s
ndividual preoperative baseline values (preoperativeaseline ICP values were 8 to 10 mm Hg). Furthermore,xperience has shown that tcMEPs react more sensitivelyo intraoperatively implemented interventions than dohe SSEPs. SSEPs respond with delayed alterations inmplitude, latency, and recovery after changes in thecMEP.
In 12 (39%) of 31 patients (3 CC type I, 5 CC type II, 2C type III, 1 CC type IV, 1 acute Stanford type-Bissection) including the 11 patients with noticeablehanges in evoked potentials, CSF pressure exceeded 15m Hg (Table 3). In these instances, as defined in our
rocedure protocol, CSF drainage and vital measurementdjustments were executed. By using our CSF drainagetrategy, we were not confronted with any hazardousomplications such as spinal intrathecal or epidural hem-rrhage, neurologic deficits, or infections with consecu-ive meningitis.
An increase in blood pressure was obtained throughoradrenaline infusion; a decrease in central venousressure was achieved with nitroglycerin infusion. Ow-
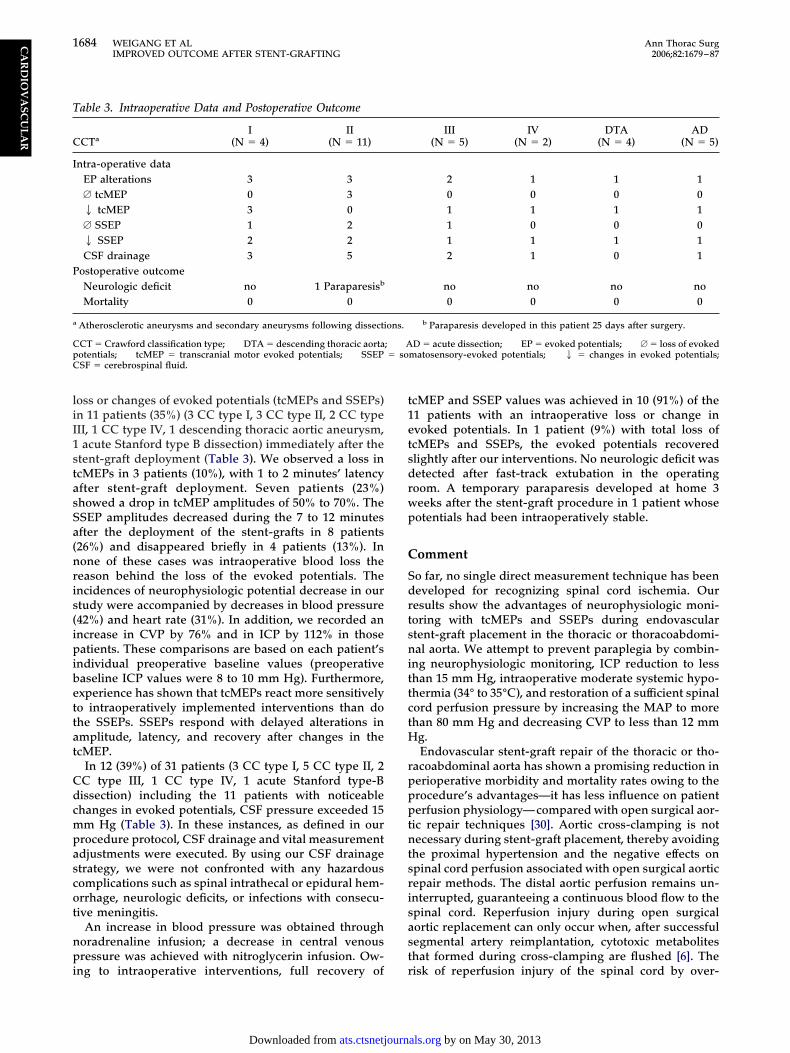
able 3. Intraoperative Data and Postoperative Outcome
CTaI
(N � 4)II
(N � 11)
ntra-operative dataEP alterations 3 3A tcMEP 0 32 tcMEP 3 0A SSEP 1 22 SSEP 2 2CSF drainage 3 5
ostoperative outcomeNeurologic deficit no 1 Paraparesisb
Mortality 0 0
Atherosclerotic aneurysms and secondary aneurysms following dissecti
CT � Crawford classification type; DTA � descending thoracic aortaotentials; tcMEP � transcranial motor evoked potentials; SSEPSF � cerebrospinal fluid.
ng to intraoperative interventions, full recovery of r
ats.ctsnetjournDownloaded from
cMEP and SSEP values was achieved in 10 (91%) of the1 patients with an intraoperative loss or change invoked potentials. In 1 patient (9%) with total loss ofcMEPs and SSEPs, the evoked potentials recoveredlightly after our interventions. No neurologic deficit wasetected after fast-track extubation in the operatingoom. A temporary paraparesis developed at home 3eeks after the stent-graft procedure in 1 patient whoseotentials had been intraoperatively stable.
omment
o far, no single direct measurement technique has beeneveloped for recognizing spinal cord ischemia. Ouresults show the advantages of neurophysiologic moni-oring with tcMEPs and SSEPs during endovasculartent-graft placement in the thoracic or thoracoabdomi-al aorta. We attempt to prevent paraplegia by combin-
ng neurophysiologic monitoring, ICP reduction to lesshan 15 mm Hg, intraoperative moderate systemic hypo-hermia (34° to 35°C), and restoration of a sufficient spinalord perfusion pressure by increasing the MAP to morehan 80 mm Hg and decreasing CVP to less than 12 mm
g.Endovascular stent-graft repair of the thoracic or tho-
acoabdominal aorta has shown a promising reduction inerioperative morbidity and mortality rates owing to therocedure’s advantages—it has less influence on patienterfusion physiology—compared with open surgical aor-
ic repair techniques [30]. Aortic cross-clamping is notecessary during stent-graft placement, thereby avoiding
he proximal hypertension and the negative effects onpinal cord perfusion associated with open surgical aorticepair methods. The distal aortic perfusion remains un-nterrupted, guaranteeing a continuous blood flow to thepinal cord. Reperfusion injury during open surgicalortic replacement can only occur when, after successfulegmental artery reimplantation, cytotoxic metaboliteshat formed during cross-clamping are flushed [6]. The
III(N � 5)
IV(N � 2)
DTA(N � 4)
AD(N � 5)
2 1 1 10 0 0 01 1 1 11 0 0 01 1 1 12 1 0 1
no no no no0 0 0 0
b Paraparesis developed in this patient 25 days after surgery.
D � acute dissection; EP � evoked potentials; A � loss of evokedmatosensory-evoked potentials; 2 � changes in evoked potentials;
ons.
; A
isk of reperfusion injury of the spinal cord by over-
by on May 30, 2013 als.org

siit[
dcissutqtwwatuaus
iogcoholmvdop
iw(npcsti(oi
eoscitebt
opecou
iiipCvs
aSfAioices
wtdamsibdclmrwaSt
ctitrdt
srsrdlS
1685Ann Thorac Surg WEIGANG ET AL2006;82:1679–87 IMPROVED OUTCOME AFTER STENT-GRAFTING
CA
RD
IOV
ASC
ULA
R
tenting segmental arteries during stent-graft placements low. Unfortunately, however, the risk of spinal cordschemia remains in 3% to 12% of patients who undergohoracic or thoracoabdominal stent-graft placement20–25].
Stent-graft implantation in the thoracic or thoracoab-ominal position might have drawbacks vis-à-vis spinalord perfusion owing to an occlusion of segmental arter-es. Surprisingly, over-stenting and occluding of largeegments of segmental arteries lead to a low incidence ofpinal cord ischemia. One possible explanation is anninterrupted distal aortic perfusion guaranteeing a con-
inuous collateral blood flow to the spinal cord. Conse-uently, this risk factor appears to be less important than
he overall advantages of this procedure, particularlyhen stent-graft procedures are performed on patientsith chronic atherosclerotic aneurysm compared with
cute aortic dissection, because collaterals develop withime and are able to compensate. Many studies havenderlined the importance of these individual collateralrterial networks supplying the spinal cord in patientsndergoing thoracic or thoracoabdominal endovasculartent-graft repair [20, 32, 33].
Endoluminal stent-grafting restricts maneuverabilityn case of permanent loss of evoked potentials, despite allf our neuroprotective measures. Endovascular stent-raft implantation may still be preferable to open thora-oabdominal repair, however, because it lowers the ratef paraplegia and mortality [20, 21, 36]. A few case reportsave been published on this subject [37–39]. According tour experience, endovascular stent-graft implantation
owers both the rate of neurologic complications andortality compared with open surgical procedures in-
olving the prosthetic replacement of the thoracoab-ominal aorta [16]. This correlates with our low incidencef changes in SSEPs and tcMEPs during the stent-graftrocedures.Yet, more patients presented with changes during
ntraoperative neurophysiologic monitoring than thereere postoperative neurologic complications. Only 1
3%) of our 31 patients had a delayed postoperativeeurologic deficit; this corresponds with published re-orts [20–25]. One can assume that a temporary spinalord malperfusion occurs during the over-stenting of theegmental arteries during stent-graft implantation thatriggers obvious changes during neurophysiologic mon-toring. By taking additional neuroprotective measuresMAP � 80 mm Hg, CVP � 12 mm Hg, ICP � 15 mm Hg),ne can counter the malperfusion, and collateral flow
nto the spinal cord is improved.We were able to demonstrate in our study that the
voked potentials (SSEPs and tcMEPs) recovered duringur neuroprotective measures. One might therefore con-ider some of these measurements as false-positives. It isertainly true that paraplegia would not have developedn all of these patients, but we are convinced that all ofhem had some degree of temporary spinal cord isch-mia. These measurements do not permit the distinctionetween mild and severe forms of spinal cord ischemia;
herefore, it is mandatory to act immediately if any sign w
ats.ctsnetjournDownloaded from
f spinal cord ischemia is suspected. The measures weropose to improve spinal cord perfusion are relativelyasy to perform, are associated with low morbidity, andan safely be administered to all patients showing signsf spinal cord ischemia, even when paraplegia would notltimately develop in all of them.Evoked potentials are a valuable tool for monitoring
ntraoperative spinal cord function, which allows thenterdisciplinary team to assess any potential ischemicncident and act accordingly to minimize the risk ofostoperative neurologic complications. The study ofheung and colleagues [22] has suggested a potentialalue of SSEPs combined with CSF drainage in thoracictent-graft repair.
A distinction must be made regarding the relevancend prognostic value of tcMEP loss compared with aSEP loss [13]. The tcMEPs allow insight into spinal cord
unction within several minutes after an intervention.lso, the tcMEPs can be remeasured after only a short
nterim. The SSEPs, on the other hand, gradually deteri-rate and exhibit a retarded restoration period and an
mpending long-term loss, even after an intervention toounteract any potential malperfusion. Both types ofvoked potentials gauge different anatomic spinal cordtructures having a different vascular supply.
Given these differences between tcMEPs and SSEPs,e conclude that measuring tcMEP has greater prognos-
ic value than measuring SSEP, also because tcMEPsirectly assess the integrity of the motor pathways. Thisllows the detection of impending motor deficit, which isore important for the postoperative outcome than sen-
ory deficits. Despite the SSEP limitation, we recommendmplementation of both of these monitoring methods,ecause SSEPs provide additional safety as well as moreiagnostic advantages. Moreover, the reversibility ofhanged potentials coinciding with an uneventful neuro-ogic outcome stresses the fact that neurophysiologic
onitoring is able to detect an impending deficit at aeversible stage. Based upon our positive results, weould like to expand Cheung and colleagues’ [22] thesis
nd recommend the routine implementation of tcMEP,SEP, and CSF pressure monitoring for all thoracic or
horacoabdominal stent-graft implantations.CSF drainage is an additional tool to minimize spinal
ord ischemia. Our experiences during open surgicalhoracic or thoracoabdominal repair have shown that thisntervention is followed by a recovery of evoked poten-ials and consequently has a positive effect on the neu-ologic outcome of our patients [16, 17]. We therefore alsoecrease ICP to less than 15 mm Hg during thoracic or
horacoabdominal stent-graft implantation.We insert the CSF drain at least 12 hours before
urgery for two main reasons. First, it is necessary toegister a baseline of the patient’s individual CSF pres-ure under healthy conditions; only then can an aber-ance of pressure in a pathologic situation be reliablyetected and it permits a controlled insertion versus a
ate insertion only in case of neurologic complication.econd, an early insertion (at a time when the patient is
ithout anticoagulation) can reliably decrease the risk ofby on May 30, 2013 als.org

helIt
Ccopuea
nrimsnteiappMseccpa
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
1686 WEIGANG ET AL Ann Thorac SurgIMPROVED OUTCOME AFTER STENT-GRAFTING 2006;82:1679–87
CA
RD
IOV
ASC
ULA
R
azardous complications such as a spinal intrathecal orpidural hemorrhage with possible consecutive neuro-ogic deficits, as our and other data show [16, 17, 34, 35].n addition, we did not detect any problems with infec-ions and consecutive meningitis using this strategy.
We took other neuroprotective measures in addition toSF drainage, such as adjusting the MAP and CVP. The
ombination of various neuroprotective measures basedn actual spinal cord function (measured via evokedotentials) is more differentiated than using only contin-ous nonpressure-adapted CSF drainage because it low-rs the risk of CSF drainage-induced complications, suchs headaches.From these results we conclude that monitoring the
europhysiologic functions of patients undergoing tho-acic or thoracoabdominal aortic endovascular stent-graftmplantation is a valid method to detect spinal cord
alperfusion and serves as a guideline for therapeuticpinal cord protective interventions. At our institution,europhysiologic monitoring has become routine during
horacic and thoracoabdominal aortic repair because it isasy to implement and does not hinder perioperative andntraoperative activity [31]. Loss of tcMEP and SSEP isssociated with spinal cord ischemia [14]. Most of theseatients have a higher risk for paraplegia or death thanatients without tcMEP or SSEP loss [16, 40]. By raisingAP and reducing central venous and CSF pressure,
pinal cord perfusion is presumably improved and recov-ry of tcMEP and SSEP can be achieved. These spinalord protective measures lower the incidence of spinalord ischemia and improve the neurologic outcome ofatients undergoing endovascular thoracic and thoraco-bdominal aortic repair.
eferences
1. Naslund TC, Hollier LH, Money SR, Facundus EC, Sken-deris BS. Protecting the ischemic spinal cord during aorticclamping. The influence of anesthetics and hypothermia.Ann Surg 1992;5:409–15.
2. Kouchoukos NT, Masetti P, Rokkas CK, Murphy SF, Black-stone EH. Safety and efficacy of hypothermic cardiopulmo-nary bypass and circulatory arrest for operations on thedescending thoracic and thoracoabdominal aorta. Ann Tho-rac Surg 2001;72:699–707.
3. Safi HJ, Miller CC 3rd, Azizzadeh A, Iliopoulos DC. Obser-vations on delayed neurologic deficit after thoracoabdomi-nal aortic aneurysm repair. J Vasc Surg 1997;26:616–22.
4. Estrera A, Miller CC 3rd, Huynh TT, et al. Preoperative andoperative predictors of delayed neurologic deficit followingrepair of thoracoabdominal aortic aneurysm. J Thorac Car-diovasc Surg 2003;126:1288–94.
5. Svensson LG. An approach to spinal cord protection duringdescending or thoraco-abdominal aortic repairs. Ann ThoracSurg 1999;67:1935–6.
6. Faden AI, Simon RD. A potential role for excitotoxins in thepathophysiology of spinal cord injury. Ann Neurol 1998;23:623–6.
7. Wan IYP, Angelini GD, Bryan AJ, Ryder I, Underwood MJ.Prevention of spinal cord ischaemia during descendingthoracic and thoracoabdominal aortic surgery. Eur J Cardio-thorac Surg 2001;19:203–13.
8. Estrera AL, Rubenstein FS, Miller CC 3rd, Huynh TT, Letsou
GV, Safi HJ. Descending thoracic aortic aneurysm: surgicalapproach and treatment using the adjuncts cerebrospinalats.ctsnetjournDownloaded from
fluid drainage and distal aortic perfusion. Ann Thorac Surg2001;72:481–6.
9. Coselli JS, Lemaire SA, Koksoy C, Schmittling ZC, CurlingPE. Cerebrospinal fluid drainage reduces paraplegia afterthoracoabdominal aortic aneurysm repair: results of a ran-domized clinical trial. J Vasc Surg 2002;35:631–9.
0. Ling E, Arellano R. Systematic overview of the evidencesupporting the use of cerebrospinal fluid drainage in thora-coabdominal aneurysm surgery for prevention of paraple-gia. Anesthesiology 2000;93:1115–22.
1. Cinà CS, Abouzahr L, Arena GO, Laganà A, Devereaux PJ,Farrokhyar F. Cerebrospinal fluid drainage to prevent para-plegia during thoracic and thoracoabdominal aortic aneu-rysm surgery: a systematic review and meta-analysis. J VascSurg 2004;40:36–44.
2. Estrera AL, Rubenstein FS, Miller CC 3rd, Huynh TT, LetsouGV, Safi HJ. Descending thoracic aortic aneurysm: surgicalapproach and treatment using the adjuncts cerebro-spinalfluid drainage and distal aortic perfusion. Ann Thorac Surg2001;72:481–6.
3. Meylaerts SA, Jacobs MJ, van Iterson V, de Haan P, KalkmanCJ. Comparison of transcranial motor evoked potentials andsomatosensory evoked potentials during thoracoabdominalaortic aneurysm repair. Ann Surg 1999;230:742–9.
4. MacDonald DB, Janusz M. An approach to intraoperativeneurophysiologic monitoring of thoracoabdominal aneu-rysm surgery. J Clin Neurophysiol 2002;19:43–54.
5. Jacobs MJ, Mess WH. The role of evoked potential monitor-ing in operative management of type I and type II thoraco-abdominal aortic aneurysms. Semin Thorac Cardiovasc Surg2003;15:353–64.
6. Weigang E, Hartert M, von Samson P, et al. Thoracoabdomi-nal aortic aneurysm repair: interplay of spinal cord protect-ing modalities. Eur J Vasc Endovasc Surg 2005;30: 624–31.
7. Weigang E, Hartert M, von Samson P, et al. Improved spinalcord perfusion during thoracoabdominal aortic repair. Tho-rac Cardiovasc Surg 2005;53:69–73.
8. de Haan P, Kalkman CJ, de Mol BA, Ubags LH, Veldman DJ,Jacobs MJHM. Efficacy of transcranial motor-evoked myo-genic potentials to detect spinal cord ischemia during oper-ations for thoracoabdominal aneurysms. J Thorac Cardio-vasc Surg 1997;113:87–101.
9. Criado FJ, Abul-Khoudoud OR, Domer GS, et al. Endovas-cular repair of the thoracic aorta: lessons learned. AnnThorac Surg 2005;80:857–63.
0. Gravereaux EC, Faries PL, Burks JA, et al. Risk of spinal cordischemia after endograft repair of thoracic aortic aneurysms.J Vasc Surg 2001;34:997–1003.
1. Greenberg R, Resch T, Nyman U, Lindh M, Brunkwall J,Brunkwall P. Endovascular repair of descending thoracicaortic aneurysms: an early experience with intermediate-term follow-up. J Vasc Surg 2000;31:147–56.
2. Cheung AT, Pochettino A, McGarvey ML, et al. Strategies tomanage paraplegia risk after endovascular stent repair ofdescending thoracic aortic aneurysms. Ann Thorac Surg2005;80:1280–9.
3. Lamme B, de Jonge IC, Reekers JA, de Mol BA, Balm R.Endovascular treatment of thoracic aortic pathology: feasi-bility and mid-term results. Eur J Vasc Endovasc Surg2003;25:532–9.
4. Lepore V, Lonn L, Delle M, Mellander S, Radberg G, RisbergB. Treatment of descending thoracic aneurysms by endovas-cular stent grafting. J Card Surg 2003;18:436–43.
5. Makaroun MS, Dillavou ED, Kee ST, et al. Endovasculartreatment of thoracic aortic aneurysms: results of the phaseII multicenter trial of the Gore TAG thoracic endoprosthesis.J Vasc Surg 2005;41:1–9.
6. Sloan TB, Heyer EJ. Anesthesia for intraoperative neuro-physiologic monitoring of the spinal cord. J Clin Neuro-physiol 2002;19:430–43.
7. Lotto MJ, Banoub M, Schubert A. Effects of anesthetic agents
and physiologic changes on intraoperative motor evokedpotentials. J Neurosurg Anesthesiol 2004;16:32–42.by on May 30, 2013 als.org

2
2
3
3
3
3
3
3
3
3
3
3
4
I
IwvnimHaphpappvtt
idhdtboIosospoas
m
1687Ann Thorac Surg WEIGANG ET AL2006;82:1679–87 IMPROVED OUTCOME AFTER STENT-GRAFTING
©P
CA
RD
IOV
ASC
ULA
R
8. Banoub M, Tetzlaff JE, Schubert A. Pharmacologic andphysiologic influences affecting sensory evoked potentials:implication for perioperative monitoring. Anesthesiology2003;99:716–37.
9. Michenfelder JD, Milde JH. The effect of profound levels ofhypothermia (below 14 de-grees C) on canine cerebralmetabolism. J Cereb Blood Flow Metab 1992;12:877–80.
0. Carroccio A, Marin ML, Ellozy S, Hollier LH. Pathophysiol-ogy of paraplegia following endovascular thoracic aorticaneurysm repair. J Card Surg 2003;18:359–66.
1. Weigang E, Hartert M, Sircar R et al. Setup of neurophysiolog-ical monitoring with tcMEP/SSEP during thoracoabdominalaneurysm repair. Thorac Cardiovasc Surg 2005;53:28–32.
2. Huilgol R, Verhagen H, Harris JP, White GH. Endoluminalrepair of a complex tortuous descending thoracic aorticaneurysm. Eur J Vasc Endovasc Surg 2003;25:175–7.
3. Shimazaki T, Ishimaru S, Kawaguchi S, Yokoi Y, WatanabeY. Blood coagulation and fibrinolytic response after endo-vascular stent grafting of thoracic aorta. J Vasc Surg 2003;37:1213–18.
4. Weaver KD, Wiseman DB, Farber M, Ewend MG, MarstonW, Keagy BA. Complications of lumbar drainage after tho-racoabdominal aortic aneurysm repair. J Vasc Surg 2001;34:
623–7.entation of spinal cord protective measures. Cerebrospi-
npsgaecsost
fseantiacc
M
DJTFe
R
1
2006 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ats.ctsnetjournDownloaded from
5. Fitzgibbon DR, Glosten B, Wright I, Tu R, Ready B. Paraple-gia, epidural anesthesia, and thoracic aneurysmectomy. An-esthesiology 1995;83:1355–9.
6. Cambria RP, Brewster DC, Lauterbach SR, Kaufman JL,Geller S, Fan CM. Evolving experience with thoracic aorticstent graft repair. J Vasc Surg 2002;35:1129–36.
7. Ortiz-Gomez JR, Gonzalez-Solis FJ, Fernandez-Alonso L,Bilbao JI. Reversal of acute paraplegia with cerebrospinalfluid drainage after endovascular thoracic aortic aneurysmrepair. Anesthesiology 2001;95:1288–89.
8. Fleck T, Hutschala D, Weissl M, Wolner E, Grabenwöger M.Cerebrospinal fluid drainage as a useful treatment option torelieve paraplegia after stent-graft implantation for acuteaortic dissection type B. J Thorac Cardiovasc Surg 2002;123:1003–5.
9. Fuchs RJ, Lee WA, Seubert CN, Gelman S. Transient para-plegia after stent grafting of a descending thoracic aorticaneurysm treated with cerebrospinal fluid drainage. J ClinAnesth 2003;15:59–63.
0. Reuter DG, Tacker WA Jr, Badylak SF, Voorhees WD 3rd,Konrad PE. Correlation of motor-evoked potential responseto ischemic spinal cord damage. J Thorac Cardiovasc Surg
1992;104:262–72.NVITED COMMENTARY
n this report [1], the authors describe their experienceith spinal cord protective measures, known from con-
entional aortic surgery, in the setting of thoracoabdomi-al aortic stent grafting. The incidence of spinal cord
schemia, resulting in paraplegia, after stent graft place-ent in the descending thoracic aorta is a rare event.owever, patients who had previous abdominal aortic
neurysm repair followed by endovascular stent graftlacement in the thoracic aorta are at an increased risk ofaving paraplegia develop. The same holds true foratients that have combined stent grafting of the thoracicnd abdominal aorta. It seems that in this subset ofatients, neurophysiologic monitoring and spinal cordrotective measures as implemented by the authors arealuable tools to reduce the risk of paraplegia. There arewo aspects of this report that merit detailed comment ashey affect perioperative paraplegia in different ways.
The use of intraoperative neurophysiologic monitor-ng, using somatosensory and motor evoked potentials toetect spinal cord ischemia and help prevent paraplegia,as been successfully implemented in open thoracoab-ominal aortic surgery. Both types of evoked potentials
arget different spinal cord structures with a differentlood supply. Therefore many groups use a combinationf both methods as the authors have done in their report.nterestingly they have shown that spinal cord ischemiaccurs during endovascular stent grafting, which is not aurprising finding, considering that a significant numberf intercostal and lumbar arteries are covered by thetent graft. It would have been intriguing to know, if inatients that received two stent grafts, spinal cord ischemiaccurred after placement of the first or second stent graftnd whether it was more common when an abdominaltent graft was placed in combination with a thoracic one.
The second important concept in this report is the imple-
al fluid drainage is being used by many centers to preventerioperative and delayed paraplegia. With regard to en-uring adequate spinal cord perfusion, endovascular stentrafting is distinctly different from open repair in that itlways leaves segmental arteries to the spinal cord uncov-red in the region of the visceral arteries. Therefore aollateral blood supply is always preserved, unless previousurgery of the abdominal aorta has occurred. Second, it isur experience that during stent graft procedures, hypoten-ion rarely presents a problem. Usually we have to coun-eract hypertension to enable safe stent graft placement.
As an additional treatment option in type B dissections,enestration of the false lumen can restore blood flow toelected malperfused segments and should be consid-red. In summary, both neurophysiologic monitoringnd spinal cord protective measures positively impacteurologic outcome after open aortic surgery and are
hus attractive concepts for thoracoabdominal stent graft-ng as well. The authors’ contention that these steps offern effective prevention of adverse events with minimalomplications, although based on a small patient group,ertainly merits further evaluation in a larger cohort.
irko Doss, MD
epartment of Thoracic and Cardiovascular Surgery.W. Goethe University Frankfurt am Mainheodor Stern Kai 7rankfurt am Main, 60599 Germany-mail: [email protected]
eference
. Weigang E, Hartert M, Siegenthaler MP, et al. Periopera-tive management to improve neurologic outcome in tho-racic or thoracoabdominal aortic stent-grafting. Ann Tho-
rac Surg 2006;82:1679 – 87.0003-4975/06/$32.00doi:10.1016/j.athoracsur.2006.06.075
by on May 30, 2013 als.org

DOI: 10.1016/j.athoracsur.2006.05.037 2006;82:1679-1687 Ann Thorac Surg
Friedhelm Beyersdorf Sircar, Gàbor Szabò, Christian D. Etz, Maximilian Luehr, Patrick von Samson and
Ernst Weigang, Marc Hartert, Michael P. Siegenthaler, Nicholas A. Beckmann, Ronen Thoracoabdominal Aortic Stent-Grafting
Perioperative Management to Improve Neurologic Outcome in Thoracic or
& ServicesUpdated Information
http://ats.ctsnetjournals.org/cgi/content/full/82/5/1679including high-resolution figures, can be found at:
References http://ats.ctsnetjournals.org/cgi/content/full/82/5/1679#BIBL
This article cites 39 articles, 11 of which you can access for free at:
Citations
shttp://ats.ctsnetjournals.org/cgi/content/full/82/5/1679#otherarticleThis article has been cited by 14 HighWire-hosted articles:
Subspecialty Collections
http://ats.ctsnetjournals.org/cgi/collection/great_vessels Great vessels
following collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
[email protected]: orhttp://www.us.elsevierhealth.com/Licensing/permissions.jsp
in its entirety should be submitted to: Requests about reproducing this article in parts (figures, tables) or
Reprints [email protected]
For information about ordering reprints, please email:
by on May 30, 2013 ats.ctsnetjournals.orgDownloaded from
Related Documents











