Perioperative Management of Diabetes Karrie Berg, D.O., M.A.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Perioperative Management of DiabetesKarrie Berg, D.O., M.A.

Mounting evidence that perioperative hyperglycemia is
associated with worse outcomes• Malglycemia causes oxidative stress• Increased risk of inflammation and infection• Increased risk of thrombosis

• Many facilities do not have perioperative protocols or standards

Perioperative Recommendations
• Some evidence based recommendations • Many expert consensus recommendations• Do our best to keep the patients safe
Goal
• Help put together evidence-based guidelines to standardize the perioperative management of hyperglycemia
• Ensure that surgery patients with transient perioperative hyperglycemia, impaired glucose tolerance or diabetes receive optimal care

• Standardization• Preoperative Screening• Preoperative period• Intraoperative period• Postoperative period• Monitoring• Transitions• Case Study #1• Case Study #2• Questions

Standardize
• Recommendations/ protocols/ order sets• Develop a team to create recommendations
– Surgeons, anesthesiologists, intensivists hospitalists, endocrinologist, RNs, pharmacists, diabetic educators
– People who know national recommendations and end users
Standardize
• Determine what is currently happening perioperatively in your facility– How is the patient educated?– Is A1C being obtained?– When is BG being checked / how often?– Is there intervention for malglycemia?
• Measure before and after• Create an audit form for evaluation

Pre-Operative Screening
• Check HgbA1C of all diabetic patients preferably 30 days prior to procedure
• Consider checking A1C for those with a BMI over 30 or age over 40
Pre-Operative Screening
• Set A1C goals for elective surgeries – no established cut off point
• A1C can measure glucose control over the last 3 months
• An elevated A1C can lead to oxidative stress and poor wound healing
• Consider if it is reasonable for PCP or Endocrinologist to better manage glucose prior to surgery (postpone surgery)

Pre-Operative ScreeningSuggestions
• Some set target A1c of 8.5 or below• Will be based on type of patient
– Young pts without comorbidities are expected to have an A1C closer to 6.5 (tight control)
– Older patients with multiple comorbidities are allowed to have A1C closer to 8.5 (loose control)
– General control recommendation from the ADA
Patient Education
• Medications to take the day before surgery• Medications to take the morning of surgery• Medications to take after returning home or to
the hospital room
• A handout for the patient may be beneficial• How will patient get this information?
Patient EducationSuggestions
• Type 1 Diabetics– If on long acting insulin, give 80-100 % of
usual dose prior to surgery– If on NPH, take 100% of evening dose and
50-75% morning dose
– Specific recommendations should be recommended by the facility
Patient EducationSuggestions
• Type 2 Diabetics– Hold oral medications the day of surgery– Hold non-insulin injectable medications the
day of surgery

Patient Education Example
• Patient Directions
• Patient Directions

Pre-op/ Day of Surgery
• Check blood glucose• Emotional and physiological stress can cause
hyperglycemia• Directed change in home medications can
cause hyperglycemia• Determine if insulin needs to be given prior to
surgery

Set Targets and make plan
• What is your target glucose range?• What is the plan for hyperglycemia?
– Will you use IV or subcutaneous insulin– Create a protocol
• What is the plan for hypoglycemia?– Create a protocol

Set Targets and Make PlansSuggestions
• BG 100-180 mg/dL• Tighter control for special populations
(cardiac surgery) 100-150

Hypoglycemia Suggestions
• If BG is 50-69 mg/dL, give 12.5 gram (25 ml) D50 slow IV push
• If BG is less than 50 mg/dL, give 25 gm (50 ml) D50 slow IV push
• Recheck FSBG in 15 min• If no IV access, give glucagon 1 mg IM
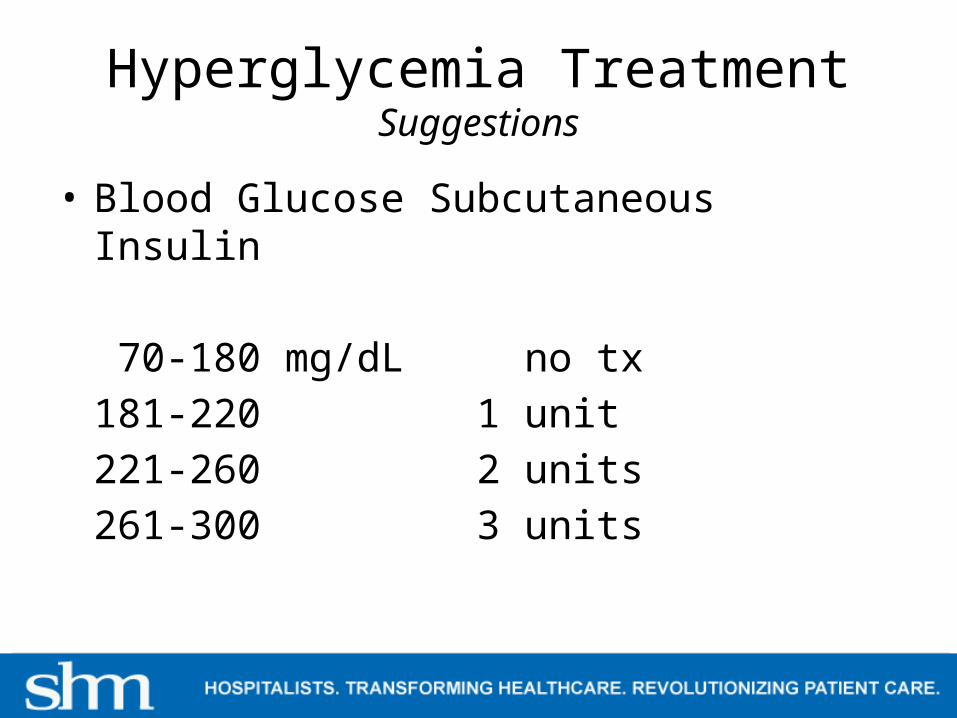
Hyperglycemia TreatmentSuggestions
• Blood Glucose Subcutaneous Insulin
70-180 mg/dL no tx
181-220 1 unit
221-260 2 units
261-300 3 units

Hyper- and hypoglcemic treatment
• Hyper- and hypoglycemia protocols
• Hyper- and hypoglycemia protocols

Intraoperative
• Determine a plan before the surgery starts– No longer use sliding scale insulin dosing– Insulin gtt vs. subcutaneous insulin vs.
basal insulin
• Provide recommendations for insulin use during surgery -standardize

IntraoperativeSuggestions
• Use subcutaneous insulin to control BG during short surgeries
• Use IV insulin drip – for longer surgeries– type 1 diabetics– Type 2 diabetics who normally take insulin
• Pts who use basal insulin should have already received a dose
Intraoperative Protocol
• SHM Perioperative Management\OR Insulin Drip (Draft).pdf
• OR Insulin Drip

Intraoperative
• Create a protocol to transition from IV to Subcutaneous Insulin
• IV to subcutaneous insulin
• IV to subcutaneous insulin

Postoperative Period
• Many studies show an association between hyperglycemia in the postoperative period and adverse outcomes, including infections, arrhythmias and renal impairment
– Whitcomb et.al (2005)– Freire et. al (2005)
• Some published studies show that intervention to improve glucose levels reduce the risk of these complications
– Zerr KJ, et al (1997)

Post-operative Period
• Provide detailed history of BG results and insulin treatment to be given to the post op RN
• Provide a plan for future treatment– Transition to oral medications– Treat with subcutaneous insulin– Continue IV insulin drip– Communicate this to care team and patient
• Treat post-operative nausea and vomiting to promote oral intake

Monitoring
• Blood Glucose (POC) machine available? Or does sample need to be run to lab?
• Develop a system to record BG, treatment and time
• Recommended times to check BG– Upon arrival to pre-op area– Prior to induction of anesthesia or prior to
incision– Upon awaking from anesthesia– On transfer to post-op

Monitoring
• For longer surgeries check BG every hour, especially if on insulin drip
• Check more frequently if hyper- or hypoglycemic treatment was required (every 15 minutes)
Transitions
• Very important• Place where many errors occur• Home to pre-op or hospital room to pre-op• Pre-op to surgery• Surgery to recovery• Recovery to hospital room or home

TransitionWhat to include in handoff
• Did hyper- or hypoglycemia occur?• How was it treated?• How did they respond?• What have the last few blood glucoses been?• What type of monitoring or treatment did they
receive during surgery?• How frequently is blood glucose being checked?• What is the plan for medication after recovery?

Standardized Hand-off Form
• Hand-off form• One form for each transition• One form showing progress through each
transition

Case Study #1
• 54 yo F with T1DM• Takes glargine 20 units qhs, lispro 5 units
with meals and 1:20 glucose correction• Scheduled for a Colonoscopy• 1 week prior, PCP orders preop labs, gives
handout for preop instructions and gives rx for bowel prep
• HgbA1C 8.1, H/H 11.2/33.4, K 3.8, creatinine 0.8, INR 1.1
• Instructions:– Start Golytle night before procedure– Clear liquid diet after noon and NPO after midnight– Take glargine 16 units the night before (= 80%)– Take lispro for correction but not nutritional dose– For Hypoglycemia take 4 oz of orange juice or 2
glucose tabs, recheck in 15 minutes and retreat if necessary. Tell anesthesiologist of BG and TX

Day of Procedure
• Am BG at home 145 mg/dL• Upon arrival to surgery center BG 230 mg/dL• Pt assures anesthesiologist that she took
nothing by mouth this am• Likely case of stress hyperglycemia• Pt given 2 units lispro

• Pt taken to procedure room 90 minutes after arrival
• BG checked prior to sedation 155 mg/dL• Pt given light sedation• Procedure takes 20 minutes with 2 polyps
removed.
• Pt taken to post-op• Anesthesia takes BG prior to handing off to
post-op nurse, BG 145 mg/dL

Hand off report
• On arrival at 0815 BG 230 mg/DL• Pt given 2 units of lispro at 0822• 0935 BG155 mg/dL• 0940 sedation given• 1000 procedure ended• 1015 taken to post-op• 1017 BG 145 mg/dL

Post-op
• BG checked hourly for the next 2 hours, 127 mg/dL and 146 mg/dL
• Pt awake and ready to return home

Transition to home
• Pt told to resume BG checks at home under previous schedule, more frequently if symptomatic
• OK to take lispro correction dose• OK to take evening glargine dose 100%• Restart nutritional dose when eating greater
than 50% of meals.

Case Study #2
• 64 yo male with T2DM• Takes Metformin and Glipizide• Colorectal surgeon planning for colectomy to
remove a large mass• 1 week prior he sees the surgeon in the office
who does preop labs and gives him preop instructions, including diabetes instructions that the surgeon gives to all his diabetic patients.

• HgbA1C 6.8, INR 0.9, Hgb 8.2• Bowel prep started the day before surgery• NPO after 2000 (8 pm)• Morning oral medications taken the day
before surgery• Evening doses held • Medications held on day of surgery

Day of Surgery
• BG in preop 195• Pt started on insulin drip by anesthesia• IV Bolus of 1.5 units Regular insulin given• IV drip started at 1.5 units per hour• D5 ½ NS was started at 100 ml/hr

Pt taken to OR
• BG checked prior to incision, 145 mg/dL• Infusions remain unchanged• Surgery lasted for 5 hours• BG checks hourly, 162, 141, 153, 128, 136

Pt taken to ICU
• Hand off report given to ICU nurse, including• BG 195, 162, 141, 153, 128, 136• Gave 1.5 unit bolus of regular insulin for BG
195. • Pt remained on insulin drip of 1.5 units per
hour without hyper- or hypoglycemia• IVF D5 ½ NS at 100 ml/hr

Treatment in ICU
• Pt remained intubated for 24 hours• Pt remained NPO for 48 hours• Continued insulin drip and IVF during this
time. • After 3 consecutive normal BG checks
without changing insulin drip or IVF, BG checks were changed to q 2 hours

Transition
• Clear liquid diet was started• BG levels increased to 195 and 255 mg/dL• Insulin drip was increased to 3 units per hour• BG stabilized again with hourly checks at 143,
134, 148, 156,132• Insulin drip was converted to subcutaneous
insulin• Pt transfer to med/surg floor• BG and treatment was given to med/surge nurse

Case Study #2 Procedure and Order Set Usage
• Pt education• Insulin drip protocol- intra-op• Insulin drip ICU• Hypoglycemia procedure• Transition from IV to Subcutaneous insulin• History of treatment report

Questions?

References• Akhtar S, Barash PG, Inzucchi SE. (2010). Scientific principles and clinical implications of
perioperative glucose regulation and control. Anesth Analg 110:478 –97 • American Diabetes Association. Standards of medical care in diabetes—2009. Diabetes Care
2009;32:S13– 61• Drange AS, Perkal MF, Kancir S, Concato J, Aslan M, Rosentahl RA. Long-term glycemic control and
postoperative infectious complications. Arch Surg 2006;141:375– 80• Griesdale DEG, de Souza RJ, van Dam RM, Heyland DK, Cook DJ, Malhotra A, Dhaliwal R,
Henderson WR, Chittock DR, Finfer S, Talmor D. (2009). Intensive insulin therapy and mortality among critically ill patients: a meta-analysis including NICE SUGAR study data. CMAJ 180:821–7
• Joshi G, Chung F, Vann M, Ahmad S et al. (2010). Society for ambulatory anesthesia consensus statement on perioperative blood glucose management in diabetic patients undergoing ambulatory surgery. Anesthesia & Analgesia 111: 1378-1387.
• Kao LS, Meeks D, Moyer VA, Lally KP. Peri-operative glycemic control regimens for preventing surgical site infections in adults. Cochrane Database of Systematic Reviews 2009;3: CD006806
• Latham R, Lancaster A, Covington J et al. (2001). The association of diabetes and glucose control with surgical-site infections among cardiothoracic surgery patients. Infect Control Hosp Epidemiol 22(10):607-612.
• Lauruchskat A. (2005). Prevalence and risks of undiagnosed diabetes mellitus in patients undergoing CABG. Circulation 112(16): 2397-2402.
• Maynard G, O’Malley CW, Kirsh SR.(2008) Perioperative care of the geriatric patient with diabetes or hyperglycemia. Clin Geriatr Med 24:649 – 65

References• Nathan DM, Buse JB, Davidson MB, Ferrannini E, Holman RR, Sherwin R, Zinman B (2009) American
Diabetes Association, European Association for Study of Diabetes Consensus Committee. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 32:193–203
• Pichardo-Lowden A, Gabbay, RA (2012). Management of hyperglycemia during the perioperative period. Curr Diab Rep 12: 108-118
• Polk HC Jr. Renewal of surgical quality and safety initiatives: a multispecialty challenge. Mayo Clin Proc 2006;81:345–52 5. Moghissi ES, Korytkowski MT, Dinardo M, Einhorn D, Hellman R, Hirsch IB, Inzucchi SE, Ismail-Beigi F, Kirkman MS, Umpierrez GE. Am Association of Clinical Endocrinologists and Am Diabetes Association consensus statement on inpatient glycemic control. Diabetes Care 2009; 32:1119 –31
• Swenne CL, Lindholm C, Borowiec J et al. (2005). Peri-operative glucose control and development of surgical wound infections in patients undergoing coronary artery bypass graft. J Josp Infect 61:201-212.
• Vann MA. Perioperative management of ambulatory surgical patients with diabetes mellitus. Curr Opin Anesthesiol 2009;22: 718 –24
• Whitcomb BW, Pradhan EK, Pittas AG et al (2005) Impact of admission hyperglycaemia on hospital mortality in various intensive care unit populations. Crit Care Med 33 (12): 2772-2777.
• Wiener RS, Wiener DC, Larson RJ. Benefits and risks of tight glucose control in critically ill adults: a meta-analysis. JAMA 2008;300:933– 44
• Wong J, Zoungas S, Wright C,Teede H (2010). Evidenc-based guidelines for perioperative management of diabetes in cardiac and vascular surgery. World J Surg 34:500-513.
• Zerr KJ, Furnary AP, Grunkemeier GL et al (1997) Glucose control lowers the risk of wound infection in diabetics after open heart operations. Ann Thorac Surg 63: 356-361.
Related Documents











