Perioperative Fluid Management In Pediatric Patient Arie Utariani Department of Anesthesiology & Reanimation Faculty of Medicine, Airlangga University Surabaya

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Perioperative Fluid Management
In Pediatric Patient
Arie Utariani
Department of Anesthesiology & Reanimation
Faculty of Medicine, Airlangga University
Surabaya
Physiology
- Percentage of body water exceeds that of adult.
- Expanded extracellular space which contracts during
first week of life :
1. Increasing glomerular filtration rate
2. Physiologic diuresis occurs with loss of about 10%
of total body weight
3. Some SGA / dysmature infants may not have
expanded extracelllar space
- By 6 months of age, healthy infants have kidney function
that is almost normal.
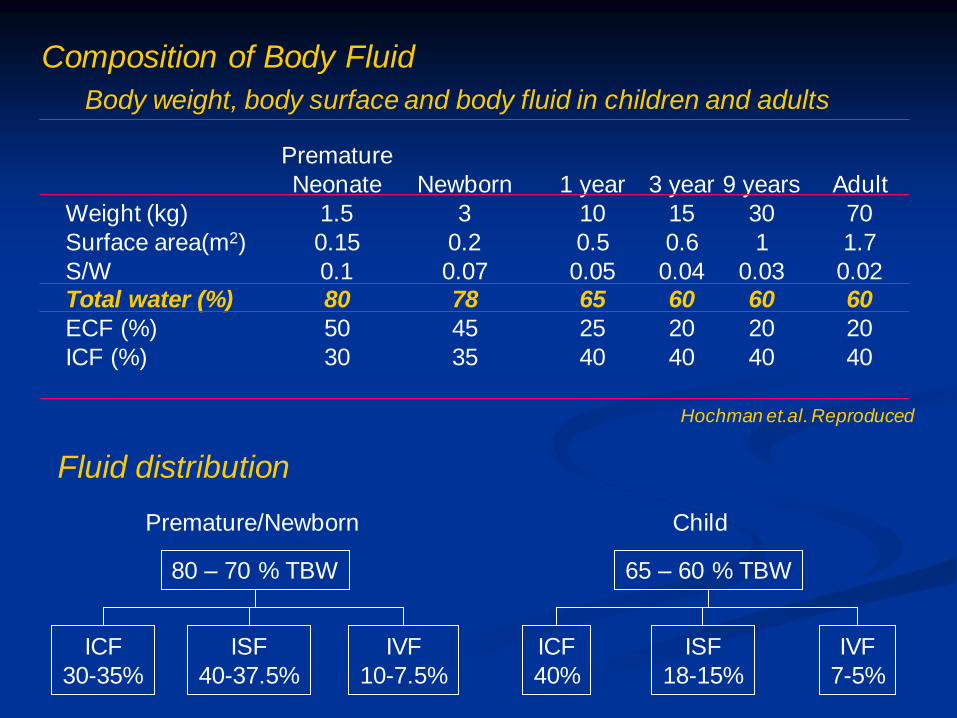
Body weight, body surface and body fluid in children and adults
Weight (kg)
Surface area(m2)
S/W Total water (%)
ECF (%)
ICF (%)
Premature
Neonate
1.5
0.15
0.1 80
50
30
Newborn
3
0.2
0.07 78
45
35
1 year
10
0.5
0.05 65
25
40
3 year
15
0.6
0.04 60
20
40
9 years
30
1
0.03 60
20
40
Adult
70
1.7
0.02 60
20
40
Hochman et.al. Reproduced
Premature/Newborn
80 – 70 % TBW
ICF
30-35%
ISF
40-37.5%
IVF
10-7.5%
Child
65 – 60 % TBW
ICF
40%
ISF
18-15%
IVF
7-5%
Fluid distribution
Composition of Body Fluid
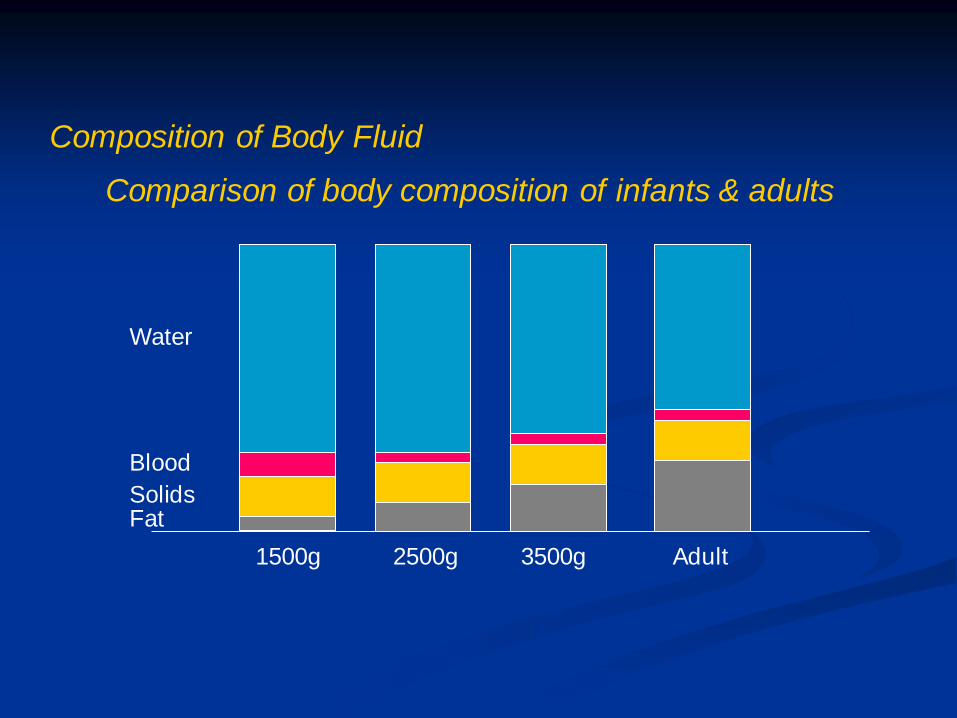
1500g 2500g 3500g Adult
Water
Blood
Solids Fat
Comparison of body composition of infants & adults
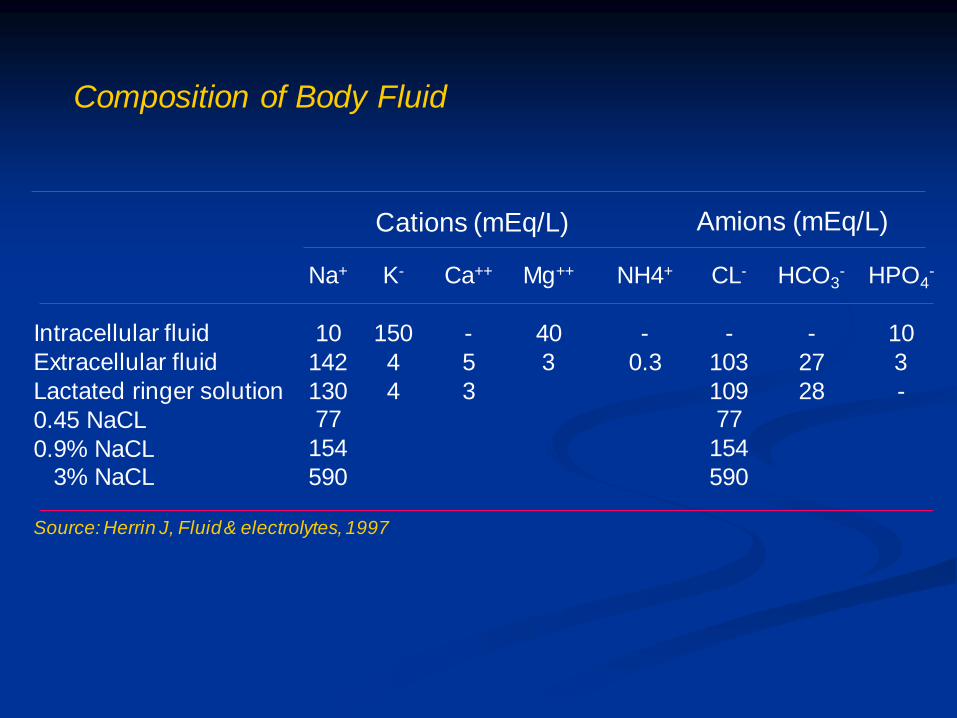
Composition of Body Fluid
Composition of Body Fluid
Intracellular fluid
Extracellular fluid
Lactated ringer solution
0.45 NaCL
0.9% NaCL 3% NaCL
Na+
10
142
130 77
154
590
K-
150
4
4
Ca++
-
5
3
NH4+
-
0.3
CL-
-
103
109 77
154
590
HCO3-
-
27
28
HPO4-
10
3
-
Cations (mEq/L) Amions (mEq/L)
Source: Herrin J, Fluid & electrolytes, 1997
Mg++
40
3
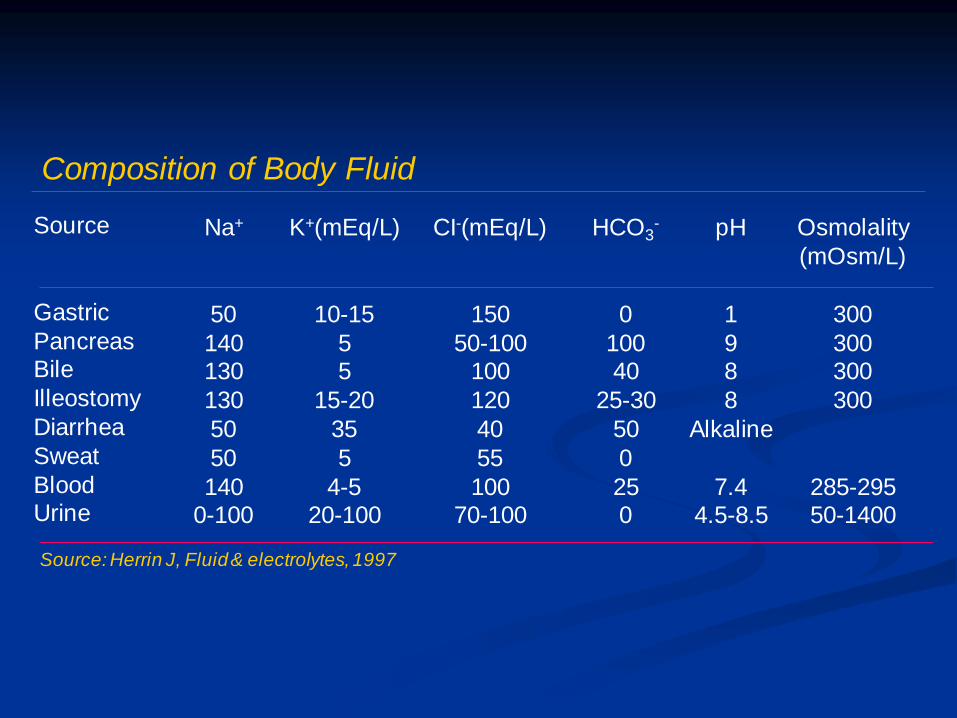
Composition of Body Fluid
Source
Gastric
Pancreas Bile
Illeostomy
Diarrhea
Sweat
Blood Urine
Na+
50
140 130
130
50
50
140 0-100
K+(mEq/L)
10-15
5 5
15-20
35
5
4-5 20-100
CI-(mEq/L)
150
50-100 100
120
40
55
100 70-100
HCO3-
0
100 40
25-30
50
0
25 0
pH
1
9 8
8
Alkaline
7.4 4.5-8.5
Osmolality
(mOsm/L)
300
300 300
300
285-295 50-1400
Source: Herrin J, Fluid & electrolytes, 1997
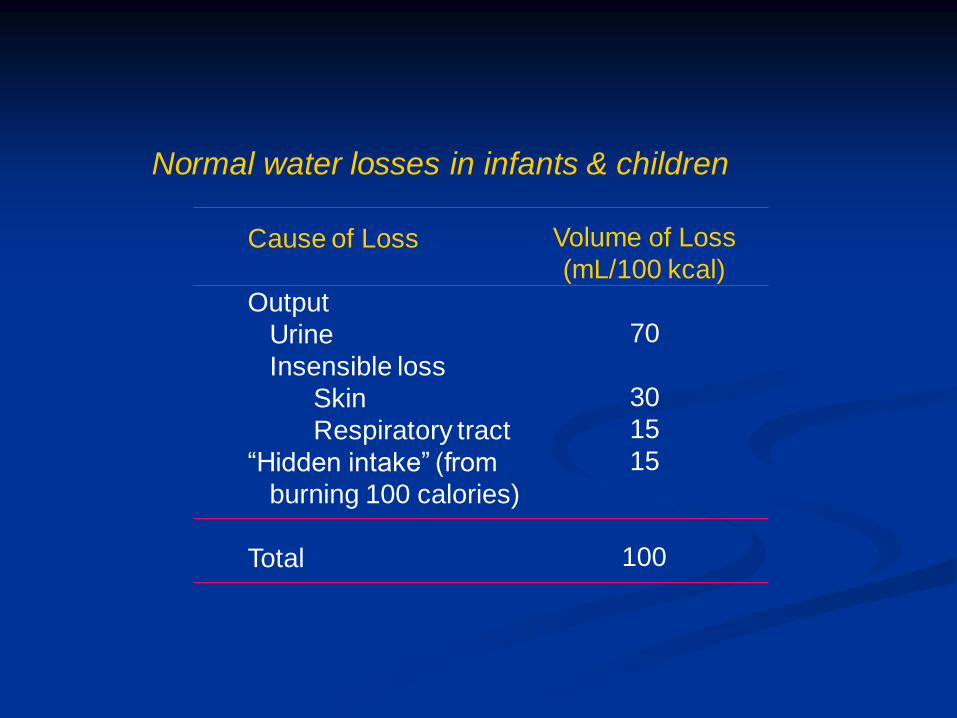
Cause of Loss
Output
Urine
Insensible loss
Skin
Respiratory tract
“Hidden intake” (from
burning 100 calories)
Total
Volume of Loss
(mL/100 kcal)
70
30
15
15
100
Normal water losses in infants & children

Perioperative fluid management
I. Maintenance
II. Deficit
III. Replacement
How should be given ?
What kind of fluid ?
How much ?
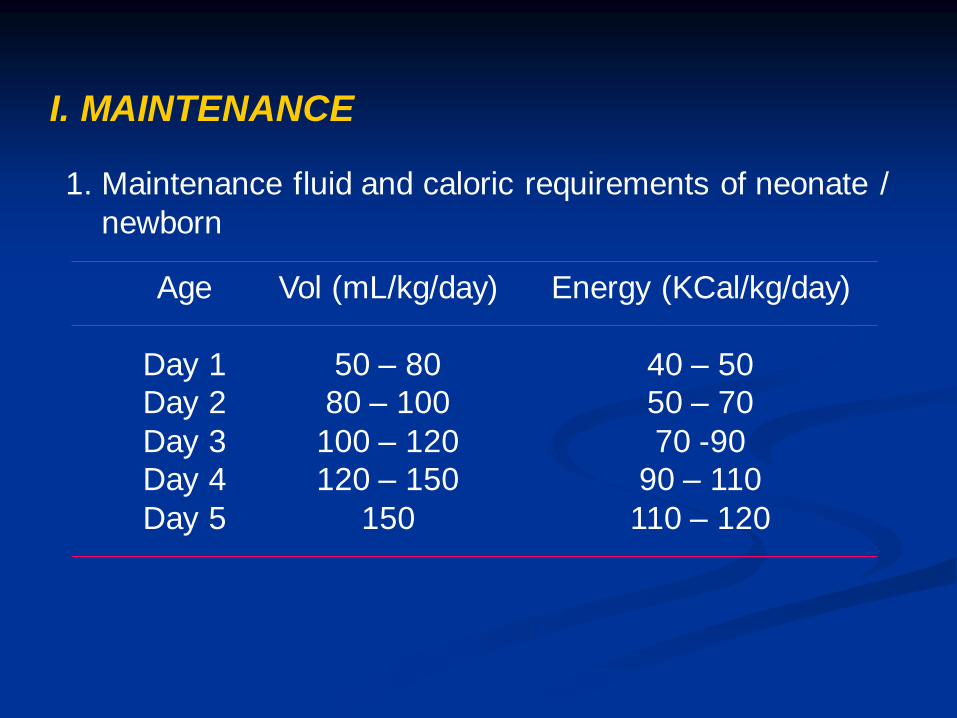
I. MAINTENANCE
1. Maintenance fluid and caloric requirements of neonate /
newborn
Age
Day 1
Day 2
Day 3
Day 4
Day 5
Vol (mL/kg/day)
50 – 80
80 – 100
100 – 120
120 – 150
150
Energy (KCal/kg/day)
40 – 50
50 – 70
70 -90
90 – 110
110 – 120
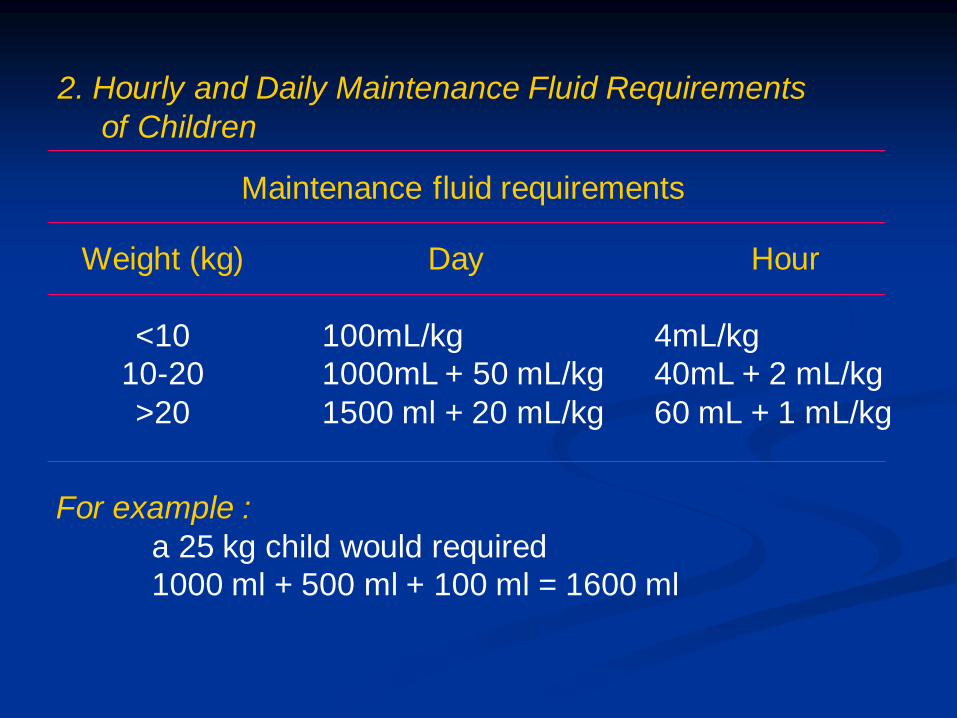
Weight (kg)
<10
10-20
>20
Day
100mL/kg
1000mL + 50 mL/kg
1500 ml + 20 mL/kg
Hour
4mL/kg
40mL + 2 mL/kg
60 mL + 1 mL/kg
Maintenance fluid requirements
2. Hourly and Daily Maintenance Fluid Requirements
of Children
For example :
a 25 kg child would required
1000 ml + 500 ml + 100 ml = 1600 ml
3. Fluid requirements to be based on BSA
1500ml / m2 BSA / day
For example :
3 kg infant : 1500 ml x 0.2 x day = 300 ml/day
Source: Holiday MA, Segar WE; The maintenance need
for water in parenteral fluid therapy padiatrics
Choice of the maintenance fluid
• Crystalloid :
Depent on the glucose and electrolyte needs
Hypotonic : D 10% 0.18 NS
D 5% 0.225 NS
D 5% 0.45 NS
• Neonate & premature or small for gestation age are at risk
for perioperative of hypoglycaemia.
• Monitoring of blood glucose concentration is recommended

II. DEFICIT
Preoperative fluid deficits :
Maintenance + fluid deficit
1. Fasting period
2. Hydration
3. Electrolyte imbalance
Solids
4
6
8
Age
< 6 months
6-36 months
> 36 months
Clear liquids
2
3
3
Fasting time (Hours)
1. Fasting period
Fasting (NPO) guidelines for children and adults

Replacement of fasting
Hourly fluid requirement x length of fasting (hours)
For example : a 5 kg child
5 kg x 4ml/kg/h x 4 h = 80 ml
Given : 50% in the first hour
25% in the second and third hour
Choice of fasting fluid : Crystalloid fluid
- Hypotonic solution
- Isotonic solution

Clinical findings
% body weight loss
Estimation fluid defisit
Pulse
Blood pressure
Respiration
Skin turgor
Mucous membranes
Peripheral perfusion
Urine
Mild
4-5%
40-50ml/kg
Normal
Normal
Normal
Normal
Moist
Normal
Reduced
Moderate
6-9%
60-90 ml/kg
↑, Weak
Normal of low
Deep
↓
Dry
Poor
Oliguria
Severe
>10%
100-110 ml/kg
↑↑, feeble
Reduced
Deep & rapid
↓ ↓
Very dry
Poor, cool, extremitas
Marked oliguria
Assessment of the degree of dehydration
2. Hydration :
Source: Nelson W
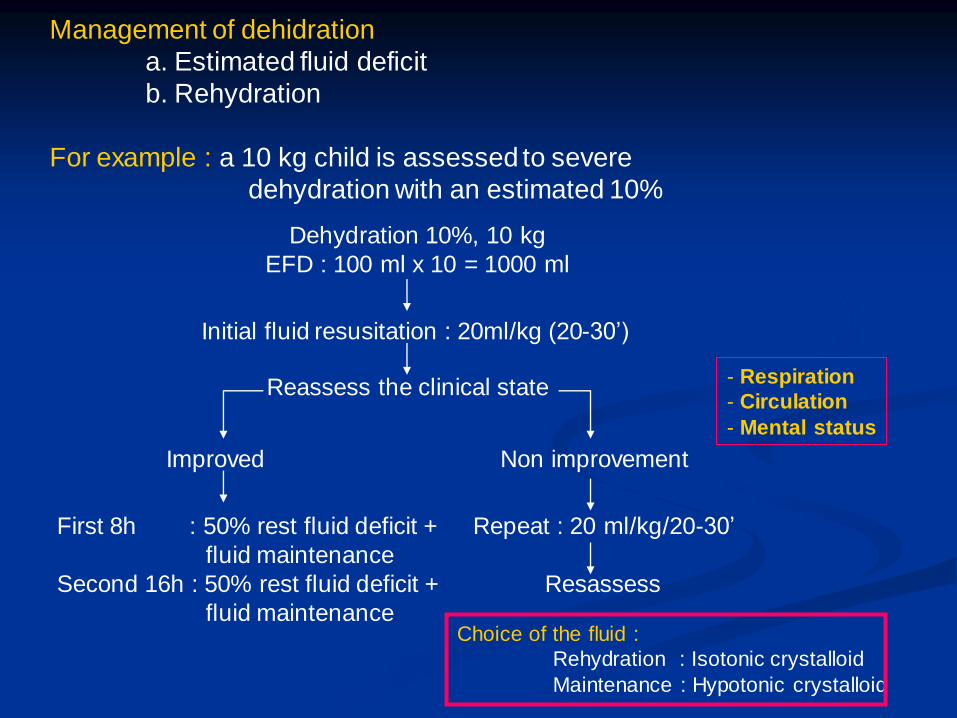
Management of dehidration
a. Estimated fluid deficit
b. Rehydration
For example : a 10 kg child is assessed to severe
dehydration with an estimated 10%
Dehydration 10%, 10 kg
EFD : 100 ml x 10 = 1000 ml
Initial fluid resusitation : 20ml/kg (20-30’)
Reassess the clinical state
Improved Non improvement
First 8h : 50% rest fluid deficit +
fluid maintenance
Second 16h : 50% rest fluid deficit +
fluid maintenance
Repeat : 20 ml/kg/20-30’
Resassess
- Respiration
- Circulation
- Mental status
Choice of the fluid :
Rehydration : Isotonic crystalloid
Maintenance : Hypotonic crystalloid
20
40
60
80
100
120
140
160
H+
K+
Cl+
K+
Na+
HCO3
Cl+
Cl+ K+
HCO3 Na+
Stomach Small bowel Diarrhea
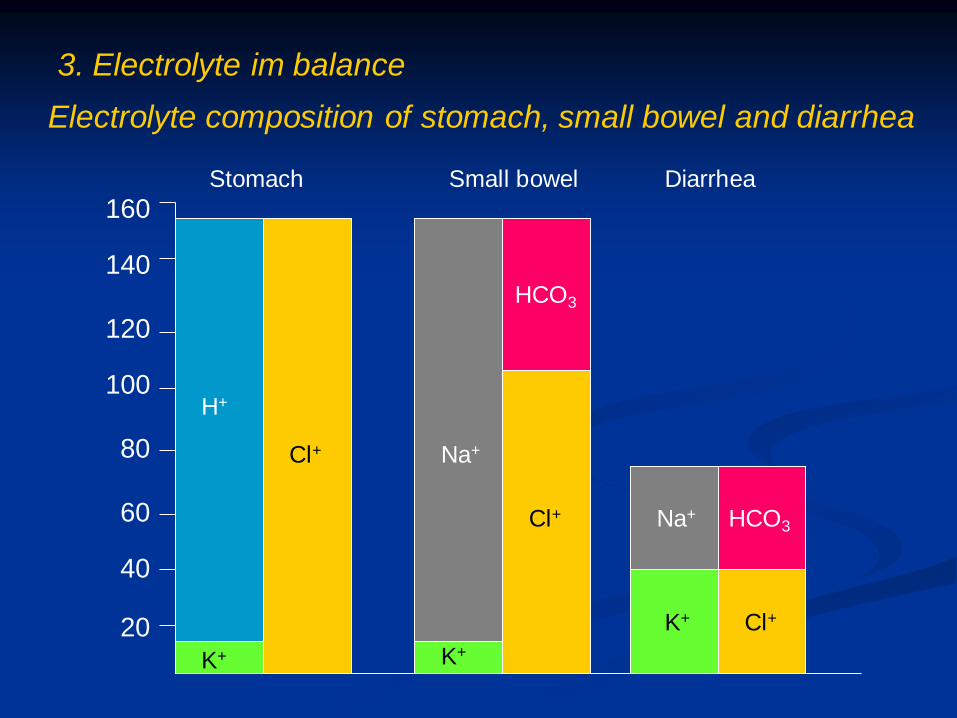
Electrolyte composition of stomach, small bowel and diarrhea
3. Electrolyte im balance
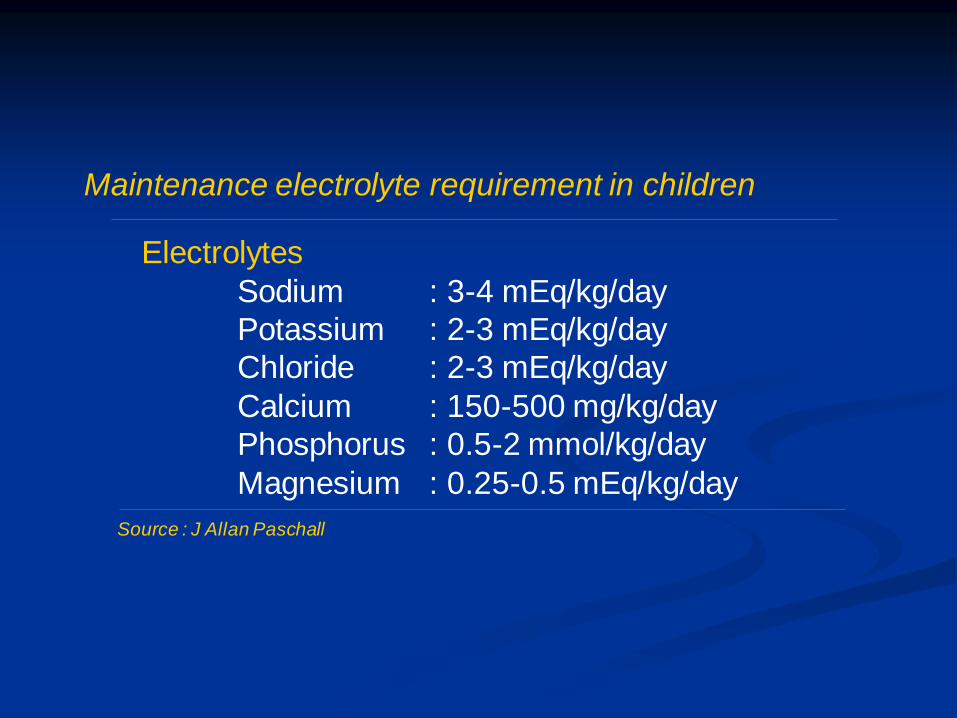
Electrolytes
Sodium : 3-4 mEq/kg/day
Potassium : 2-3 mEq/kg/day
Chloride : 2-3 mEq/kg/day
Calcium : 150-500 mg/kg/day
Phosphorus : 0.5-2 mmol/kg/day
Magnesium : 0.25-0.5 mEq/kg/day
Maintenance electrolyte requirement in children
Source : J Allan Paschall
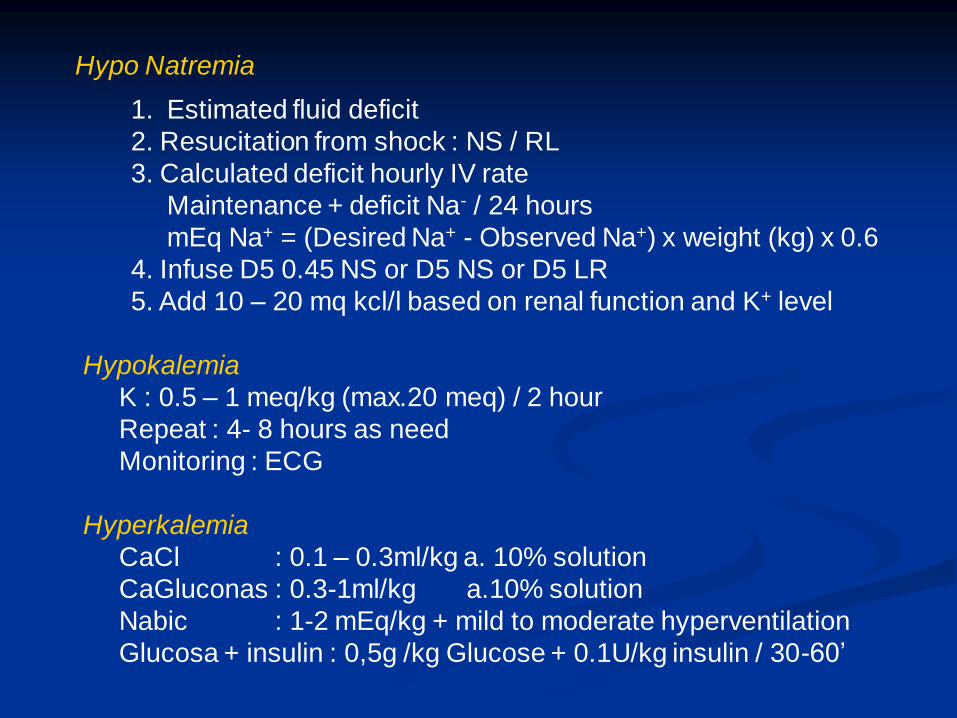
Hypo Natremia
1. Estimated fluid deficit
2. Resucitation from shock : NS / RL
3. Calculated deficit hourly IV rate
Maintenance + deficit Na- / 24 hours
mEq Na+ = (Desired Na+ - Observed Na+) x weight (kg) x 0.6
4. Infuse D5 0.45 NS or D5 NS or D5 LR
5. Add 10 – 20 mq kcl/l based on renal function and K+ level
Hypokalemia
K : 0.5 – 1 meq/kg (max.20 meq) / 2 hour
Repeat : 4- 8 hours as need
Monitoring : ECG
Hyperkalemia
CaCl : 0.1 – 0.3ml/kg a. 10% solution
CaGluconas : 0.3-1ml/kg a.10% solution
Nabic : 1-2 mEq/kg + mild to moderate hyperventilation
Glucosa + insulin : 0,5g /kg Glucose + 0.1U/kg insulin / 30-60’
III. REPLACEMENT
Intraoperative fluid management
- Maintenance
- Replacement
Replacement
- Third space lossess
- On going lossess

1. First hour, hydrating solution:
Age ≤ 3 year : 25ml/kg, plus item 3
Age ≥ 4 year :15 ml/kg, plus item 3
2. All other hours basic hourly fluid plus item 3 below
Maintenance fluid = 4 mL/kg
Maintenance + trauma = basic hourly fluid
4 mL/kg + mild trauma (2 mL/kg) = 6 mL/kg
4 mL/kg + moderate trauma (4 mL/kg) = 8 mL/kg
4 mL/kg + maximal trauma (6 mL/kg) = 10 mL/kg
3. Blood replacement with 3:1 volume replacement with crystalloid
or colloid, or blood
Guidelines for intraoperative fluids in pediatric patiens
From: Berry Reproduced
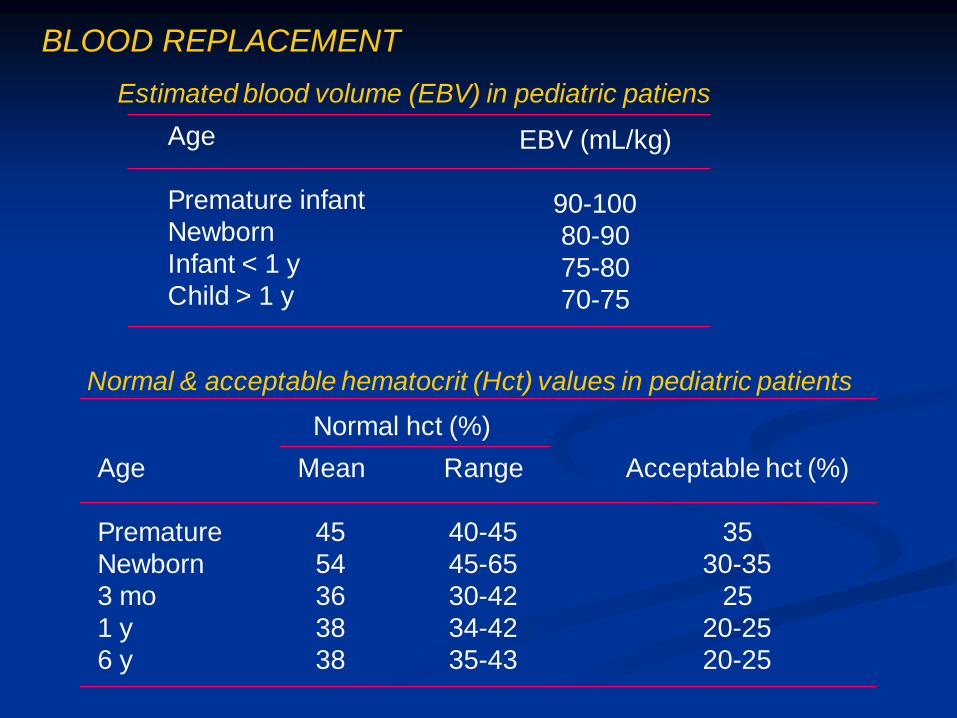
Age
Premature infant
Newborn
Infant < 1 y
Child > 1 y
EBV (mL/kg)
90-100
80-90
75-80
70-75
Estimated blood volume (EBV) in pediatric patiens
BLOOD REPLACEMENT
Age
Premature
Newborn
3 mo
1 y
6 y
Mean
45
54
36
38
38
Range
40-45
45-65
30-42
34-42
35-43
Acceptable hct (%)
35
30-35
25
20-25
20-25
Normal hct (%)
Normal & acceptable hematocrit (Hct) values in pediatric patients
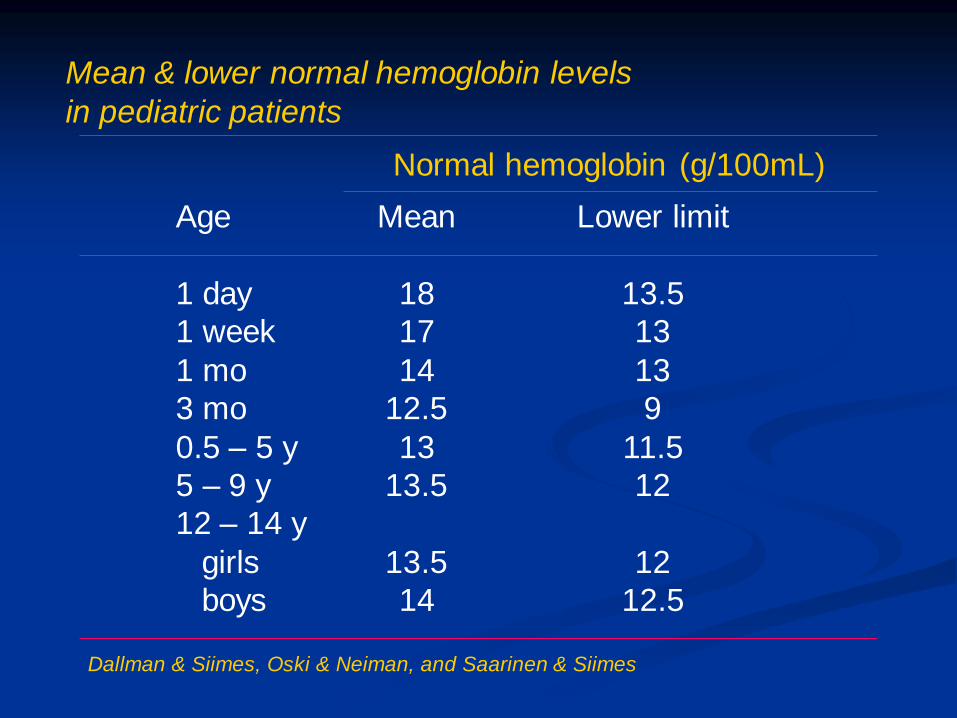
Age
1 day
1 week
1 mo
3 mo
0.5 – 5 y
5 – 9 y
12 – 14 y
girls
boys
Mean
18
17
14
12.5
13
13.5
13.5
14
Lower limit
13.5
13
13
9
11.5
12
12
12.5
Normal hemoglobin (g/100mL)
Mean & lower normal hemoglobin levels
in pediatric patients
Dallman & Siimes, Oski & Neiman, and Saarinen & Siimes

1. Blood required =
Hct 1 – Hct 2
Hct 3
X EBV
2. Blood required (PRC) = (Hct 1 – Hct 2) x body weight (kg) x 1.5
(WB) = (Hct 1 – Hct 2) x body weight (kg) x 2.5
Hct1 : Haematocrit before transfusion, the measured
haematocrit
Hct2 : Haematocrit required after transfusion, the desired
haematocrit
Hct3 : Haematocrit of the blood to be given (60% if packed cells)
EBV : Estimated blood volume
BLOOD REPLACEMENT TO USE HAEMOTOCRIT LEVEL
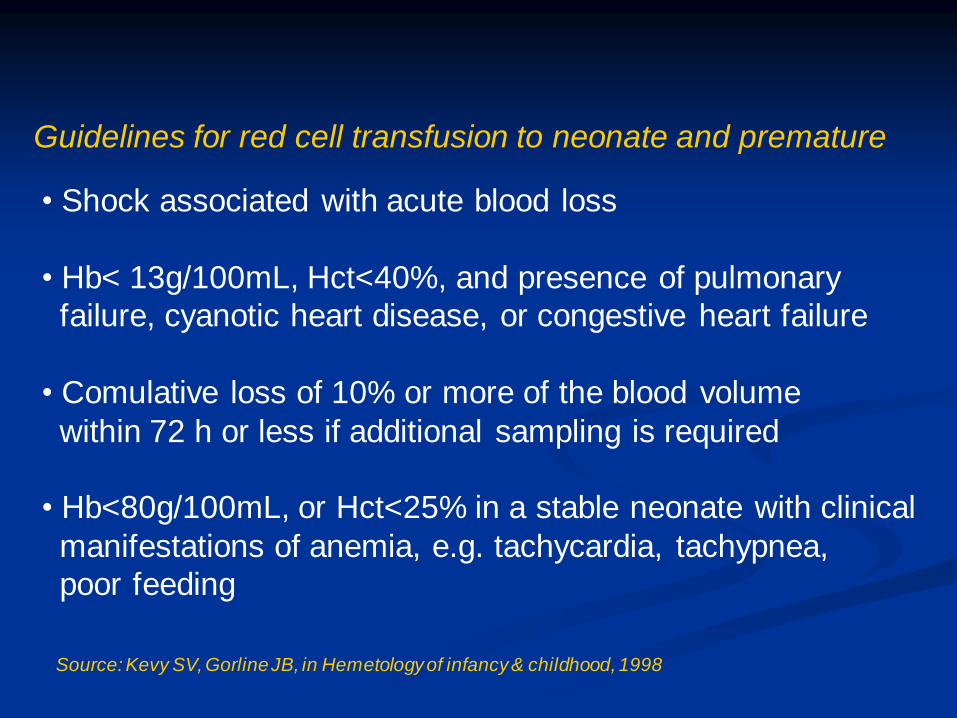
Guidelines for red cell transfusion to neonate and premature
• Shock associated with acute blood loss
• Hb< 13g/100mL, Hct<40%, and presence of pulmonary
failure, cyanotic heart disease, or congestive heart failure
• Comulative loss of 10% or more of the blood volume
within 72 h or less if additional sampling is required
• Hb<80g/100mL, or Hct<25% in a stable neonate with clinical
manifestations of anemia, e.g. tachycardia, tachypnea,
poor feeding
Source: Kevy SV, Gorline JB, in Hemetology of infancy & childhood, 1998

Postoperative Fluid Management
• Maintenance fluid
• Replacement of fluid deficit
• Replacement of other losses
- Chest tube
- Nasogastric tube
- Weeping incision
- Continous slow bleeding
• Correction of electrolyte inbalance
• Maintenance fluid requirement on the first most operation
day are decreased to 2/3 of the usual daily amount

Conclusion
• Fluid therapy for pediatric patients must be based on the knowledge
of the fluid and electrolyte needs in healthy infants and children
on physiologic responses to the surgical procedure
• Formula for fluid therapy are guidelines that need to be revaluated
according the patients response
• Even more than in the adult, improper fluid management in
infants and children can cause life threatening consequences
• The inadverten administration of a seemingly minuscule excess
of fluid may couse problems.
For example :
100 ml fluid in full term neonate is comparable to 1 to 2
liter excess in an dault

Related Documents











