PERIODONTAL ASSESSMENT Nichole Dicke, LDH, BS

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

PERIODONTAL ASSESSMENT
Nichole Dicke, LDH, BS

Periodontal Assessment
Remember the dental hygiene process of care? The ADHA standards of clinical dental hygiene practice include2:
Assessment – collection, analysis, and documentation of a patient’s oral and overall health status and needs.
Evaluation – ongoing review and documentation of the outcomes of dental hygiene care

Periodontal Assessment
The AAP has stated that a comprehensive periodontal examination includes periodontal probe measurements:1
Probing depth (PD) Location of gingival margin (GM) Clinical attachment levels/loss (CAL) Mucogingival relationships (to identify
deficiencies of keratinized tissues)

Periodontal Assessment
The AAP also provides us with the guidelines for classifying our patients’ periodontal status.
1 to 2 mm CAL = Slight 3 to 4 mm CAL = Moderate 5 to 6 mm CAL = Severe.
Note bleeding and other soft tissue considerations are NOT included here. The classification is based on CAL only. Therefore, you may have a patient with moderate or even severe CAL from previous periodontitis who is currently “healthy”.

Periodontal Assessment Note!!!! Clinical Attachment LOSS and
Clinical Attachment LEVEL are synonyms. They are two phrases used as titles for the exact same thing. Example: CAL of 2 means:
Clinical attachment LEVEL is 2mm below the CEJ.
**OR**
Clinical attachment LOSS is 2mm.
Both statements mean the patient has had 2mm of their periodontal attachment destroyed. The terms are used interchangeably and are treated the same way.

Periodontal Assessment
Periodontitis is diagnosed when a there is progression of attachment loss, requiring documentation of increased CAL between at LEAST two time points. 1
Evaluating CAL is critical for deciphering between active periodontitis and gingivitis on a reduced but stable periodontium. 1
Measuring PD alone can result in unnoticed progression of CAL.
Periodontal Assessment
Common CPC approach:
1. Measure all probing depths2. Measure visible recession and enter this into
the “GM” section of the chart.3. Print out the graphics from Dentrix to use as
visual of the patient’s CAL as calculated by the software program.
4. If no recession was present, subtract the “normal” sulcus depth (such as 3mm) from probing depths to estimate CAL and use this for classifying the patient’s periodontal status.

Periodontal Assessment
The term recession is often used to describe the apical migration of the gingival margin. When the margin has migrated far enough for cementum to be exposed, this is called “visible recession” and is measured by the distance between the CEJ and the GM.
We need to re-focus on the migration of the ATTACHMENT towards the apex, rather than the migration of the GM. After all, the GM only recedes because the attachment is receding, right?
Which should we be more concerned about: the location of the gumline, or the amount of periodontal attachment ?

Periodontal Assessment
CAL = visible recession plus hidden recession (PD), as seen in this
diagram.
What if all of the recession (attachment loss) is hidden because there the recession has
not advanced that far yet? How do you know how much attachment has
been lost?
Nield-Gehrig, J. (2004).
FOOD FOR THOUGHT…

Periodontal Assessment The problems with the common CPC (we will discuss
each of these in detail):
1. GM is NOT the same as recession.2. Dentrix perio charts are not set up to be used this way.3. CAL is not always being measured accurately.4. CAL is not determined soon enough!5. Cannot determine amount of attachment gain achieved by NSPT.6. Mucogingival relationships are not being evaluated, thus not identifying deficiencies in attached gingiva.

Does gingival recession only exist after it has migrated PAST the CEJ (visible recession)?
Has recession occurred if a gingival margin that used to be 3mm coronal to the CEJ is now only 1mm coronal to it?
HIDDEN RECESSION – how to we catchreceding attachment before the CEJ is visible?
This is where it gets a little hairy….try to stay with me!
Problem #1. GM is NOT the same as recession.

Problem #1. GM is NOT the same as recession.
• GM is the position of the free gingival margin in relation to the CEJ (above OR below), measured in millimeters.
• If the GM is apical to the CEJ, the measurement is recorded in millimeters.
• If the GM is located right at the CEJ, the GM value is zero!
• If the GM is coronal to the CEJ, the measurement can be recorded as a negative (think of it as “negative recession”).

Problem #1. GM is NOT the same as recession.
Example:
GM = 1 GM = -3 GM = 0

Problem #2. Dentrix perio charts are not set up to be used the way
we are using them. Dentrix assumes we measure GM the
“correct” way, not equating GM with recession. Any box left blank will be treated as a zero, as if the GM margin is located right at the CEJ. The CAL is then automatically calculated as the PD+0.
But does a PD of 3 mean a CAL of 3? The graphic charts will also be
inaccurate, showing CAL in areas where there is no attachment loss.

Two ways to “fix” this problem:
1. Tell Dentrix to stop automatically calculating the CAL. The hygienist will need to manually enter the CAL values for areas where GM is measured.
2. Measure GM the “correct” way, which is a very tedious, time consuming, and often difficult task.
2. Dentrix perio charts are not set up to be used the way we are using
them.

Problem #3. CAL is not always being measured accurately.
Hygienists are equating GM with recession, therefore making their CAL calculations inaccurate.
Just because there is no visible GM recession does not mean there is no attachment loss! Example:
No recession, PD = 3. No CAL?

Problem #3. CAL is not always being measured accurately.
In areas with no recession, we cannot assume the CAL by subtracting the “normal” sulcus depth of 3mm from the PD measurement. Why not? Several factors may influence the sulcus depth3, including: Blunted papilla Inflammation Malpositioning Gingival overgrowth Individual differences
Therefore, not all PD greater than 3 indicates CAL3, just as PD less than 3 does not always indicate health.

Problem #3. CAL is not always being measured accurately.
If determining progressive attachment loss is the key to diagnosing, treating, and maintaining periodontitis, why are we not taking great care to measure CAL precisely?
How can we classify as slight, moderate, or severe periodontitis without accurately measuring the criteria used for such classification?
Problem #4. CAL is not determined soon enough!
True or False: If there is no visible recession, there is no attachment loss.
True or False: You cannot identify CAL until recession has occurred.
BOTH ARE FALSE!
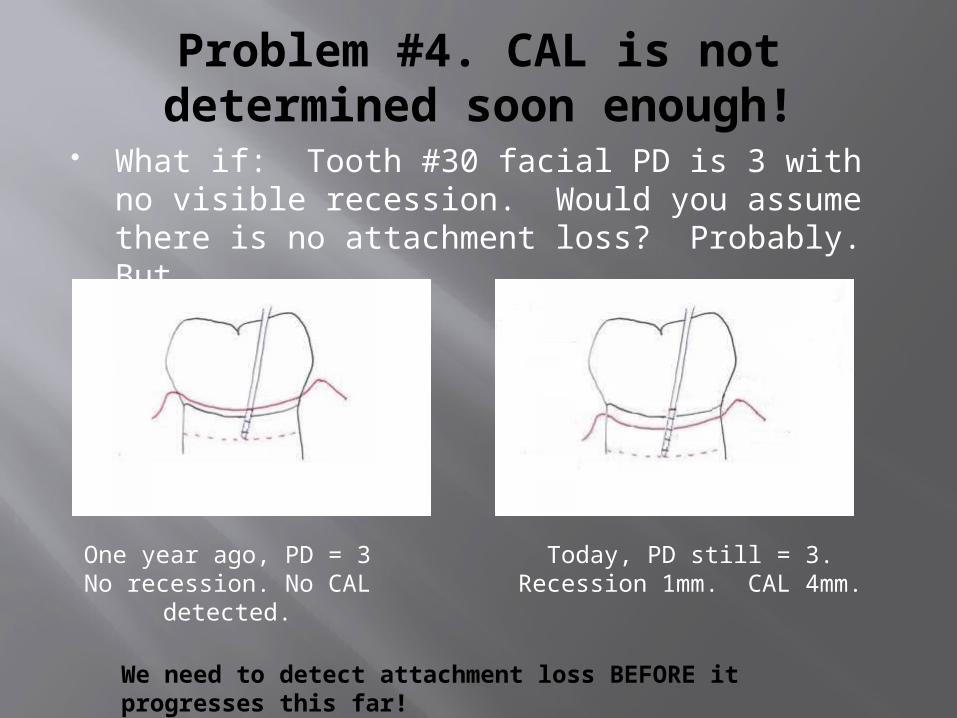
Problem #4. CAL is not determined soon enough!
What if: Tooth #30 facial PD is 3 with no visible recession. Would you assume there is no attachment loss? Probably. But…
We need to detect attachment loss BEFORE it progresses this far!
One year ago, PD = 3No recession. No CAL
detected.
Today, PD still = 3.Recession 1mm. CAL 4mm.

Problem #4. CAL is not determined soon enough!
Tooth 30 has a facial PD of 3 and 1mm of recession. CAL is calculated as 4mm.
WHY WAS THE ATTACHMENT LOSS NOT DISCOVERED UNTIL IT WAS MODERATE,
OR NEARLY SEVERE?
At this point, there may be minimal attached gingiva left….but we will discuss this later.

Problem #5. Cannot determine amount of attachment gain achieved by NSPT.
Example: Betty received NSPT on tooth #3, which originally had a PD of 8mm with no recession. The post-op PD is 3mm. How much attachment was gained?
If you did not measure the GM both before and after, you cannot assume that all 5mm reduction is due to attachment gain rather than reduction in inflammation.

Problem #6. Hygienists are not evaluating the mucogingival relationships, thus not
identifying deficiencies in attached gingiva.
Areas with deficient attached gingiva may be at higher risk for recession, damage from mechanical forces, or chronic inflammation. 4
Patients with deficient attached gingiva may need referred to a periodontist for evaluation.

Problem #6. Students are not evaluating the mucogingival relationships, thus not identifying
deficiencies in attached gingiva.
This section of the Dentrix perio chart is not often , may hygienists do not know how to:
Identify the mucogingival junction (MGJ) Measure the MGJ width Subtract the PD from the MGJ to determine
AG.

Problem #6. Students are not evaluating the mucogingival
relationships, thus not identifying deficiencies in attached gingiva.
True or False: There is always attached gingiva if the recession has not extended past the MGJ.
FALSE! If the PD is deeper than the MGJ width, there is no longer any attached gingiva on that surface. This is why it is critical to measure the MGJ width and subtract the PD depth from it in any areas with CAL. Example:

Now What?
WHAT? Inadequate/inaccurate CAL and MGJ assessments
SO WHAT? We are not assessing the patients’ periodontal attachments.
NOW WHAT? Rethink how you assess your patients! What are you really measuring? What should you be measuring?

How to correct the CAL problems by measuring GM.
Measure GM as distance from the CEJ to the gingival margin, either coronal or apical.
If this is not done, the Dentrix software must be told to STOP automatic CAL calculation.

How to correct the CAL problems by measuring GM.
How to measure GM coronal to the CEJ: Using the periodontal probe, feel for the CEJ. If
it is hard to feel, increase the angle of the probe beyond 10 ° (no longer keeping it parallel to the long axis).
Once the tip of the probe is located at the CEJ, use the probe markings to determine the distance between the CEJ and the GM with the probe held between 0º and 10° to the tooth.
Consistency is the key to detecting changes!!!

How to correct the CAL problem by measuring GM.
The GM measurements must be taken at the same site as the PD measurements! Why???
A distal GM measurement must be measured where the distal PD measurement was taken. You are going to combine the PD with the GM to assess the CAL for that surface, therefore these numbers must come from the same location! Do not measure three areas on a Buccal surface and then enter them as DB,B,and MB readings.

How to correct the CAL problems by measuring GM
Common error: Hygienist takes all three (D, B, and M) measurements along different points of the BUCCAL surface.
Tooth #30 (Buccal side)
D B M
PD 6 2 5
GM 1 2 3
CAL 7 4 8
Is the CAL accurate for all three surfaces? Is there really 8mm of CAL on the mesial of this tooth???

How to identify deficiencies in attached gingiva
Measure the mucogingival width. Identify the MGJ by one of three methods:5
1. Look for the visible line where mucosa and attached gingiva meet
2. Use the side of the probe, held horizontally against the mucosa, and use short vertical movements to detect where the moveable mucosa turns into fixed gingiva.
3. For facial areas, pull the lip/cheek taught until you can see where the loose, stretchy mucosa merges with the attached gingiva.

Probe Method of Identifying MGJ
Nield-Gehrig, J. (2004).

How to identify deficiencies in attached gingiva
Measure the distance from the MGJ to the GM. To calculate how much of this measurement is indeed “attached”, subtract the PD from the MGJ5. Example:

How to identify deficiencies in attached gingiva
True or False: You need to calculate AG by subtracting PD from MJG for all buccal/facial and lingual surfaces of all teeth.
False. Why? The palatal tissue is completely attached. There
is no MGJ. Trick Question? Maybe….but I have seen hygienists chart MGJ measurements for the maxillary linguals!

So....what shall we do?
This style of periodontal charting is:
Time consuming! More difficult to do. Not performed in most private practice
offices in this area.

So....what shall we do?
However, Consider:
What is our goal as dental hygienists? What are the ADHA standards for clinical practice? What are the AAP standards for periodontal evaluation?
Some offices actually DO perform periodontal assessments this way….and many more may begin to do so.
Our main concern in periodontics is attachment, therefore, attachment should be the focus of patient assessment.

So....what shall we do?
Could there be a compromise? Turning off the automatic calculation on the software will remove the “false CAL” on the charts. Manually calculating the correct CAL where visible recession is present would be a minimal effort.
While measuring GM above the CEJ may not be realistic for some offices, hygienists should at LEAST note “zero” GM, which is easy to detect and would allow us to detect CAL sooner.

References
American Academy of Periodontology. (2000). Parameter on comprehensive periodontal examination. Journal of Periodontology , 71, 847-848.
American Dental Hygienists' Association. (2008). Standards of clinical dentla hygiene practice. Retrieved October 6, 2010, from http://www.adha.org/ downloads/adha_standards08.pdf
Amir, S., Eaton, K.A., Moles, D.R., Needleman, I. (2009). A systemic review of definitions of periodontitis and methods that have been used to identify this disease. Journal of Periodontology, 36, 458-467.
Camargo, P. M., Melnick, P. R., & Kenney, E. B. (2001). The use of free gingival grafts for aestheticpurposes. Periodontology 2000 , 27, 72-96.
Nield-Gehrig, J. (2004). Fundamentals of Periodontal Instrumentation and Advanced Root Instrumentation. Baltimore: Lippincott Williams & Wilkins.
Related Documents











