Pericardial effusion Dr.kefelegn D 15/6/2015

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Pericardial effusionDr.kefelegn D
15/6/2015

Relapsing or recurrent pericarditis can be classified as either incessant or intermittent
1. Incessant type.2. Intermittent type.

History Anatomy/phsiology Etiology Clinical presentation Diagnosis Take home message
outline

Pericardium first discribed 17-18th century
Anterior pericardial effusion by ECHO published in 1961 by Father of ECHO…Inge Edler
History

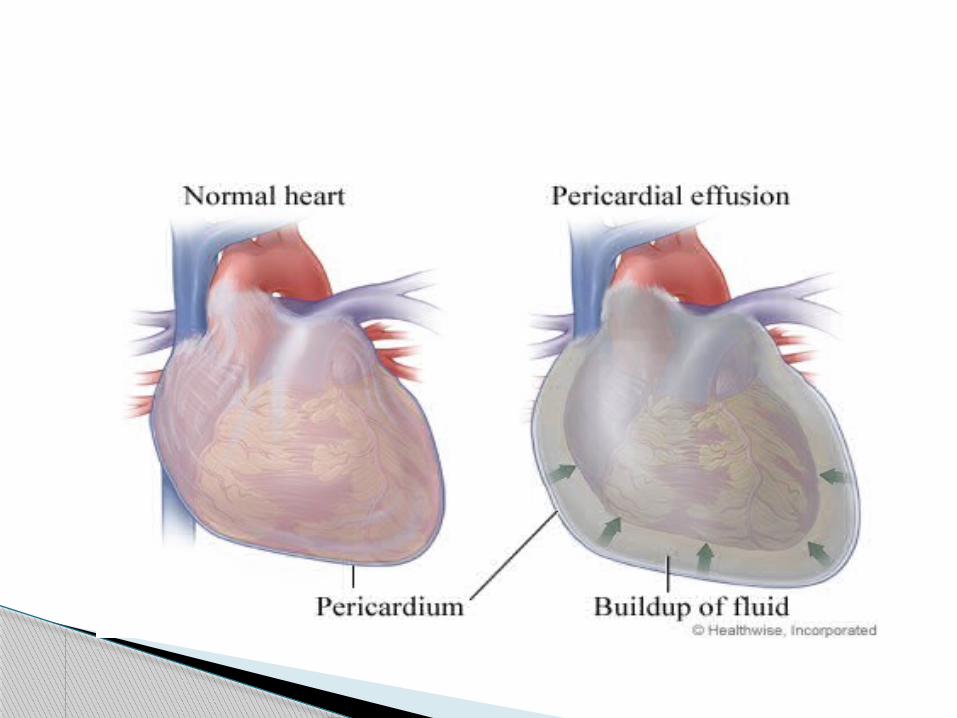
ANATOMY
◦ Limits the extent of acute dilatation of the ventricle
◦ Even distribution of pressure over the ventricles Balancing RV/LV outputs
◦ Decreasing friction ◦ Mechanical barrier to contiguous spread of
infection◦ provides structural support while also having a
substantial hemodynamic impact on the heart
Physiology
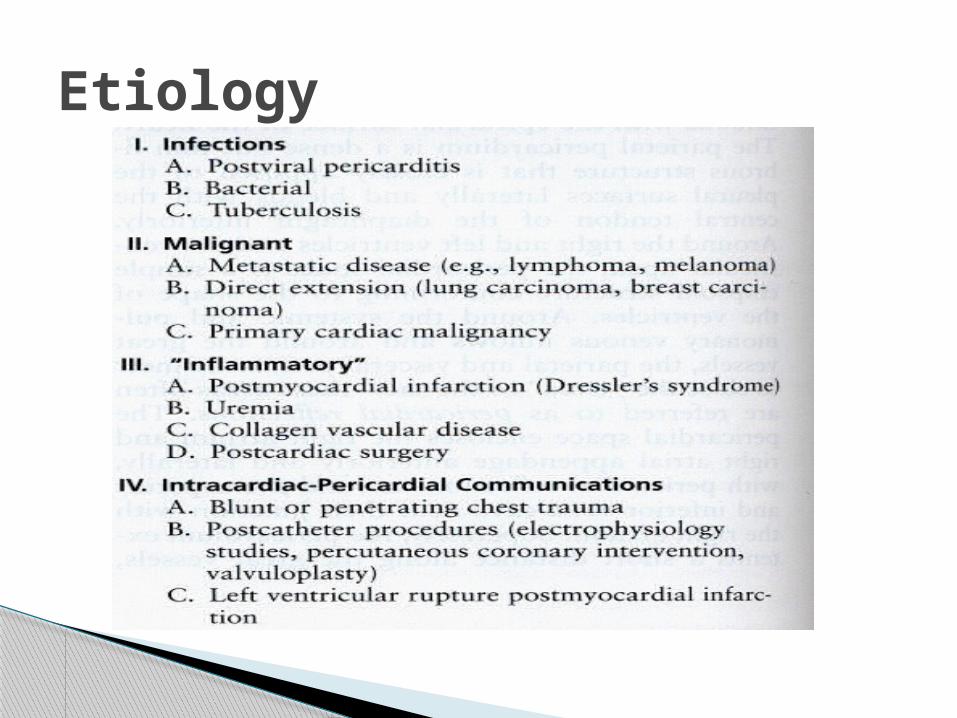
Etiology
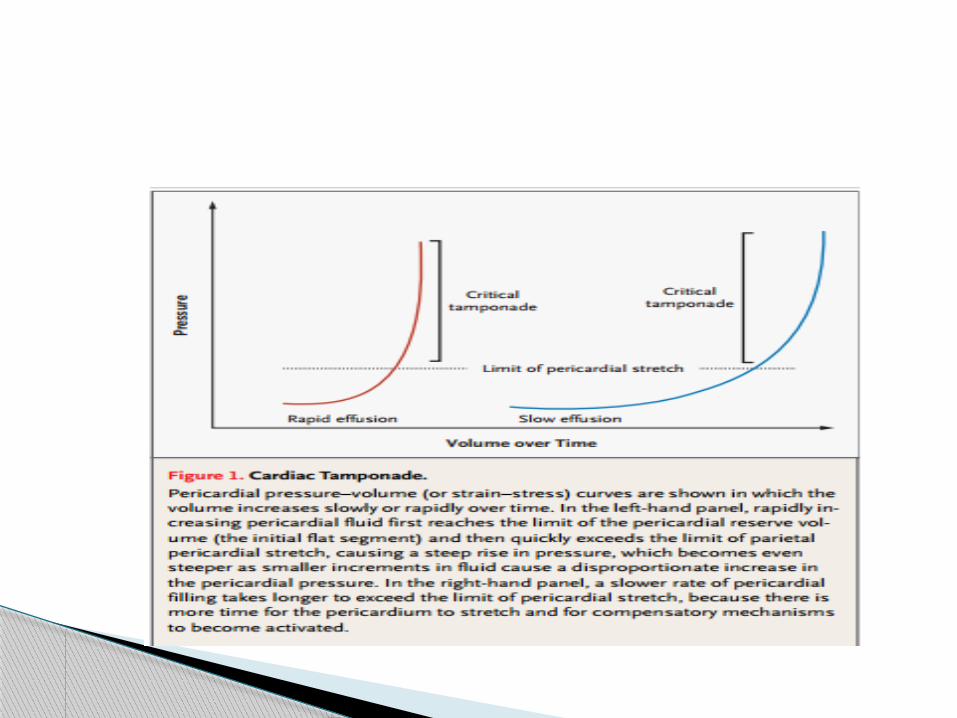
Pericardial effusions may develop rapidly (acute) or more gradually (subacute or chronic).
The normal pericardium can stretch to accommodate increases in pericardial volume, with the amount of stretch related to how quickly the effusion develops.
CLINICAL PRESENTATION
The presence of pericardial effusion may be suspected from the history, physical examination, ECG, and chest x-ray.
May have symptoms related to the underlying cause
Unless cardiac tamponade is present, physical signs are so insensitive and nonspecific.
Fluid accumulation within the pericardial space resulting in
◦ increased intracardiac pressure◦ progressive limitation of ventricular diastolic filling◦ reduction of stroke volume and cardiac output
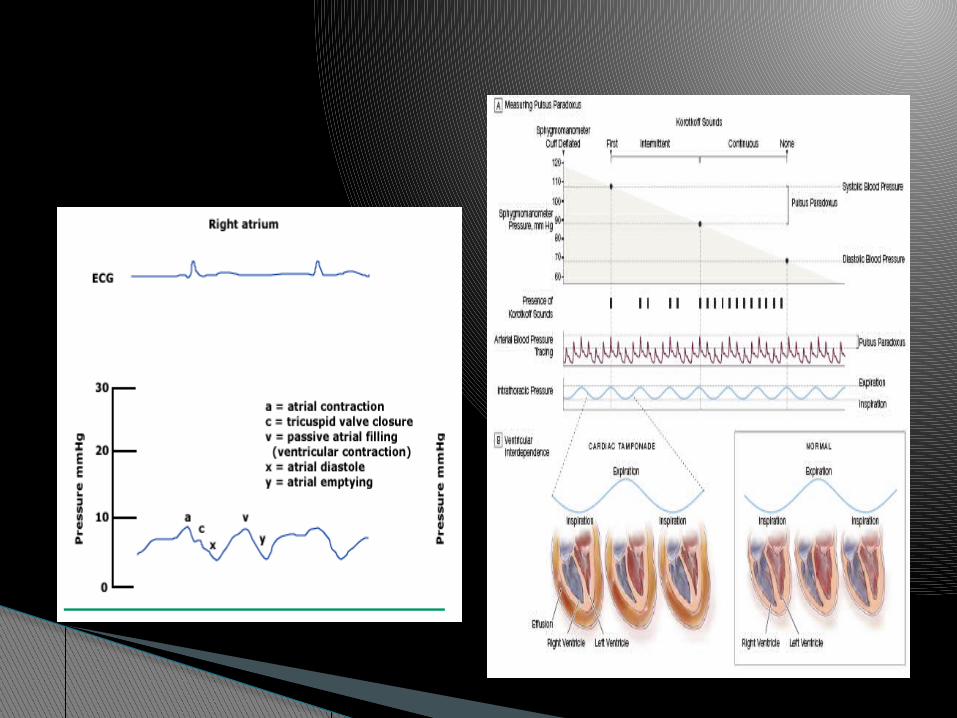
left to right heart interdependence
◦ Competition for room in the abnormally fixed pericardial space (chamber interaction) is by far the principal mechanism
Tamponade covers a spectrum of clinical severity.
Is there tamponade??

Tamponade is a pathophysiologic continuum
Occurrences of tamponade can be
Acute cardiac tamponade sudden in onset, may be associated with
chest pain, tachypnea, and dyspnea, and is life-threatening if not promptly treated.
Subacute cardiac tamponade usually a less dramatic. may be
asymptomatic early in the course, but, once intrapericardial pressure reaches a critical value, they become symptomatic.
Low pressure cardiac tamponade — Patients are severely hypovolumic. The intracardiac and pericardial diastolic
pressures are only 6 to 12 mmHg . Demonstrated on echocardiography by
tamponade signs, NOT CLINICALY. A fluid challenge with a rapid infusion of one
liter of isotonic saline will usually elicit typical cardiac tamponade hemodynamics.
Regional cardiac tamponade A loculated, eccentric effusion or localized
hematoma . selected chambers are compressed. The typical physical, hemodynamic, and
echocardiographic signs of cardiac tamponade are often absent.
Sxs◦ Chest Pain, dyspnea, near-syncope◦ Generally more comfortable sitting forward◦ Sxs of the underlying cause of tamponade
Physical Exam◦ Beck’s Triad 1935 - Elev’d JVP, hypotension, ↓ heart
sounds JVP with preserved x descent and dampened or absent y
descent Generally with narrow pulse pressure
◦ Tachycardia, other signs of HF (tachypnea, diaphoresis, cool extremities, cyanosis, etc)
◦ Pulsus paradoxus◦ Dec’d or absent cardiac impulse◦ +/- Friction rub
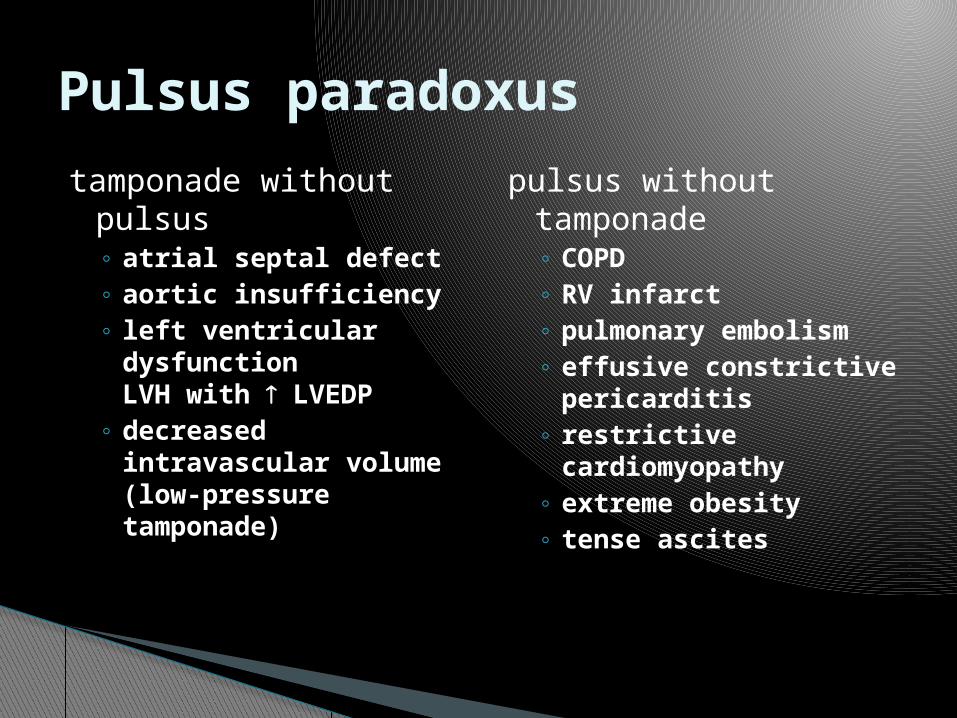
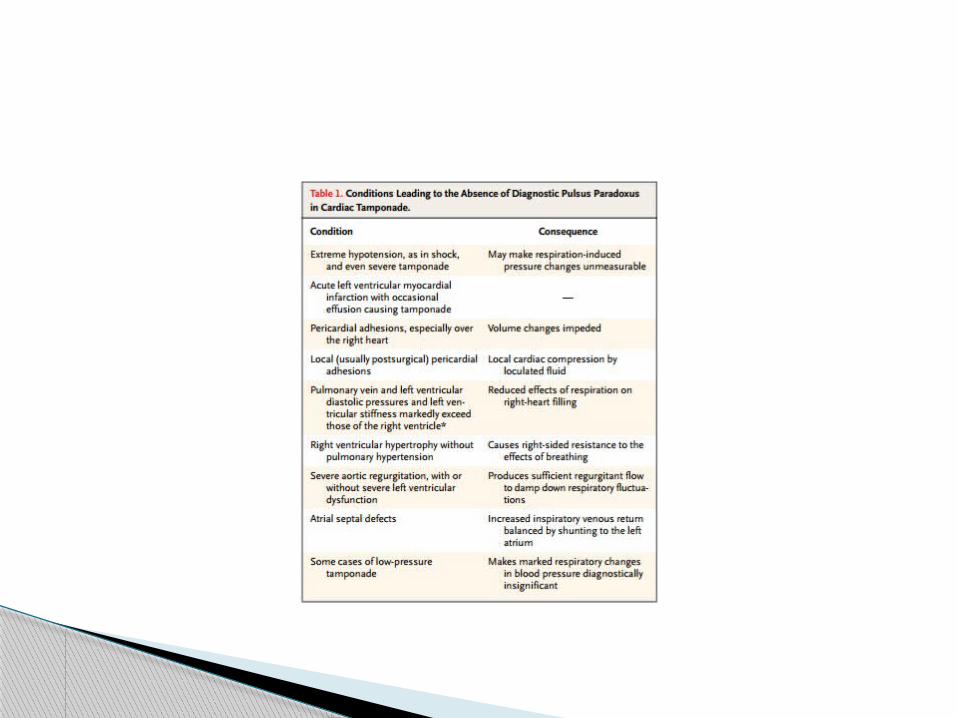
tamponade without pulsus◦ atrial septal defect◦ aortic insufficiency◦ left ventricular
dysfunctionLVH with LVEDP
◦ decreased intravascular volume (low-pressure tamponade)
pulsus without tamponade◦ COPD◦ RV infarct◦ pulmonary embolism◦ effusive constrictive
pericarditis◦ restrictive
cardiomyopathy◦ extreme obesity◦ tense ascites
Pulsus paradoxus
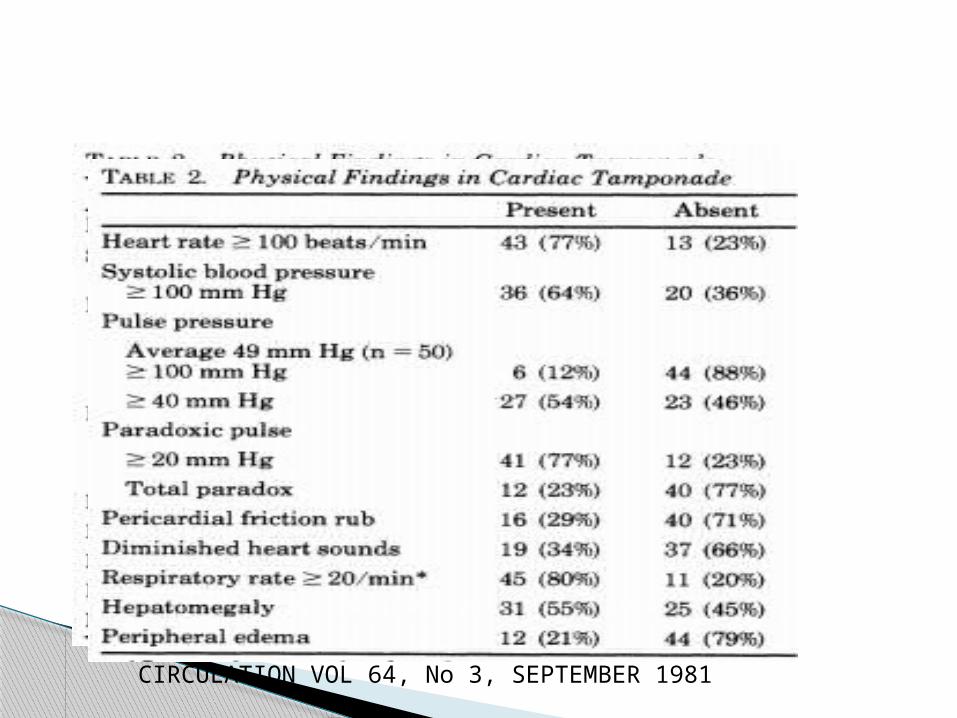
CIRCULATION VOL 64, No 3, SEPTEMBER 1981

CAN BE NORMAL sinus tachycardia low voltage, if pericarditis is
present, the ECG findings typical of it.
Electrical alternans is relatively specific but not so sensitive for tamponade; rarely, this phenomenon is seen with very large pericardial effusions alone
Lab and ECG

enlarged cardiac silhouette with clear lung fields may be seen in slowly developing cardiac tamponad e.
Cardiomegaly is not usually seen in acute cardiac tamponade since at least 200 mL of pericardial fluid must accumulate before the cardiac silhouette enlarges
Chest x-ray
Establish the presence of effusion
Quantification of the pericardial effusion ( site ,distribution)
Assess hemodynamic impact
?etiology ( nature of fliud) FOLLOW UP
ECHOCARDIOGRAPHY

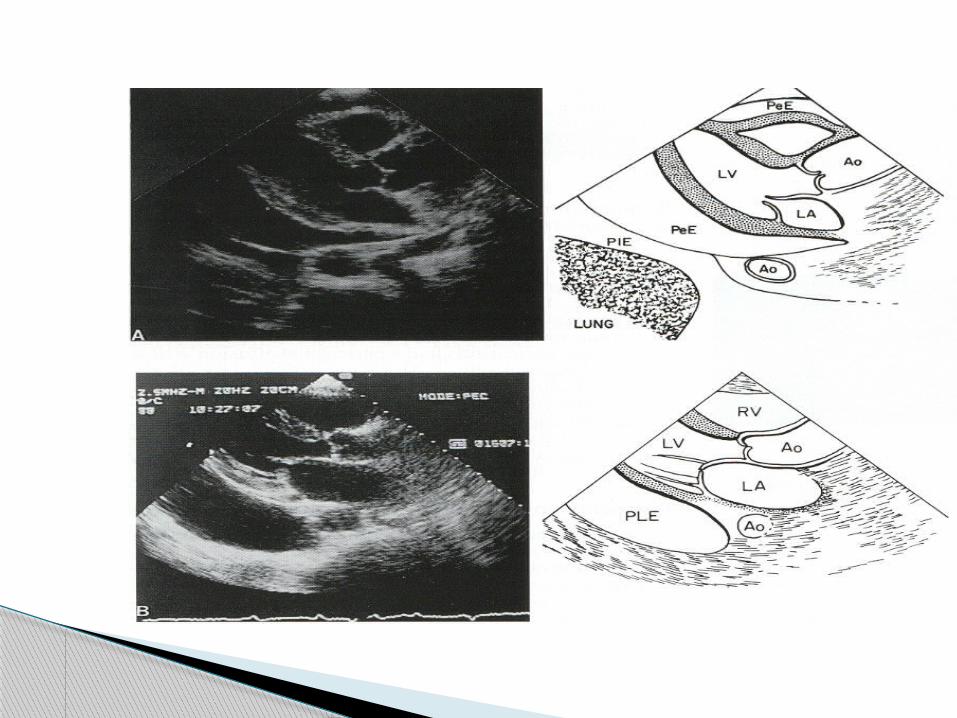
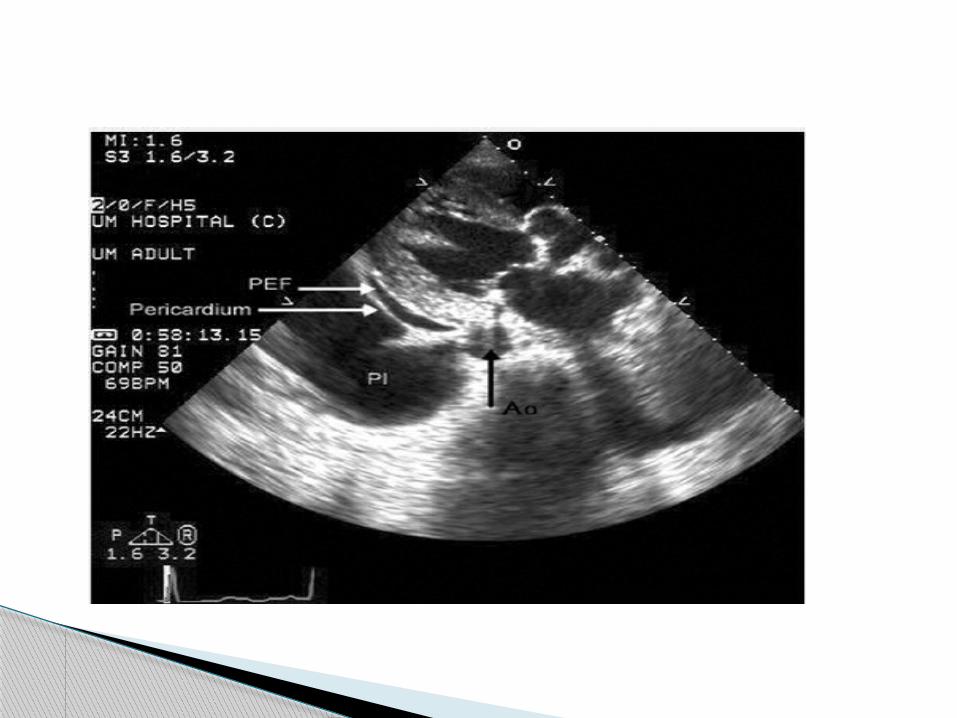
1.PLEURAL EFFUSION In PLAX view anterior(pericardial) or
posrterior ( pleural fluid) to desending aorta.
2.Epicardial fat …slightly echogenic and moves with heart cycle.
IS THIS PERICARDIAL EFFUSION?
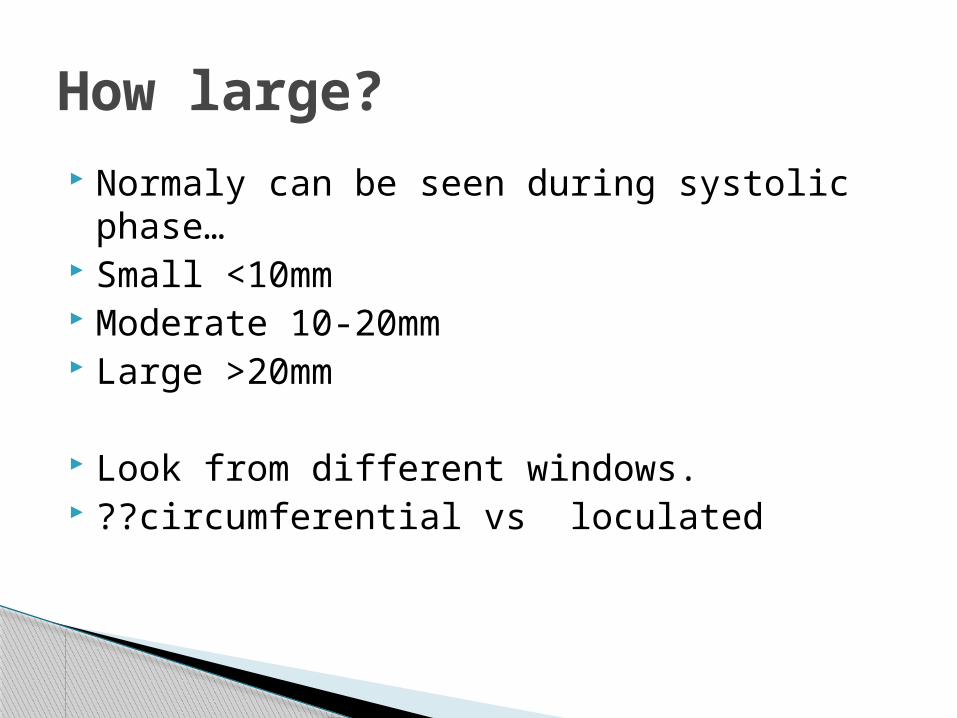
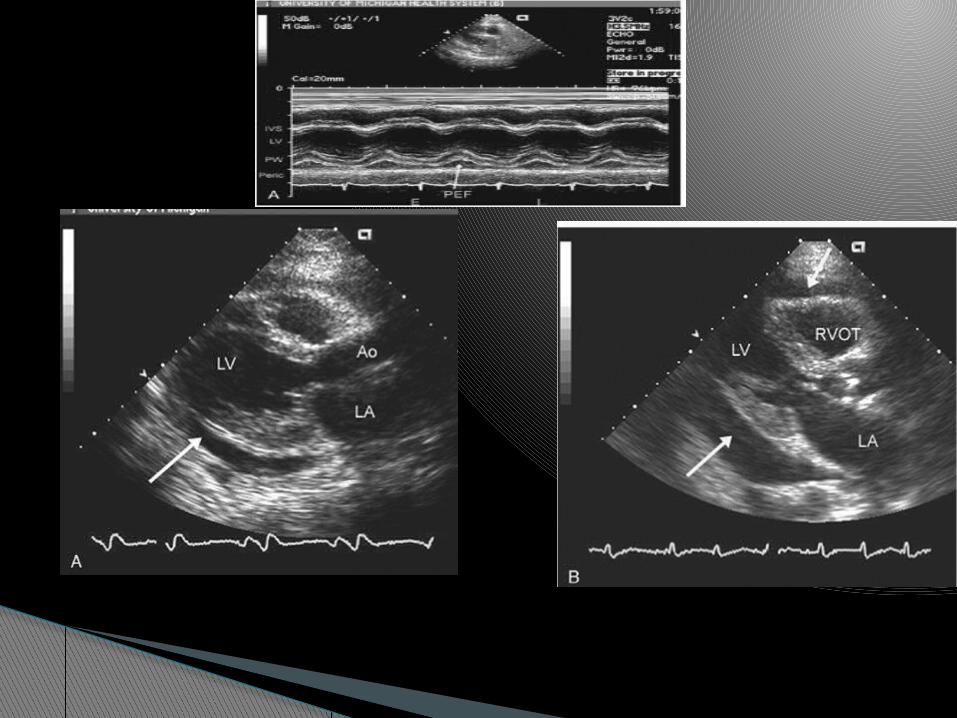
Normaly can be seen during systolic phase…
Small <10mm Moderate 10-20mm Large >20mm
Look from different windows. ??circumferential vs loculated
How large?

It should be emphasized that cardiac tamponade is a clinical diagnosis.
The use of echocardiography in cardiac tamponade is a class I indication.
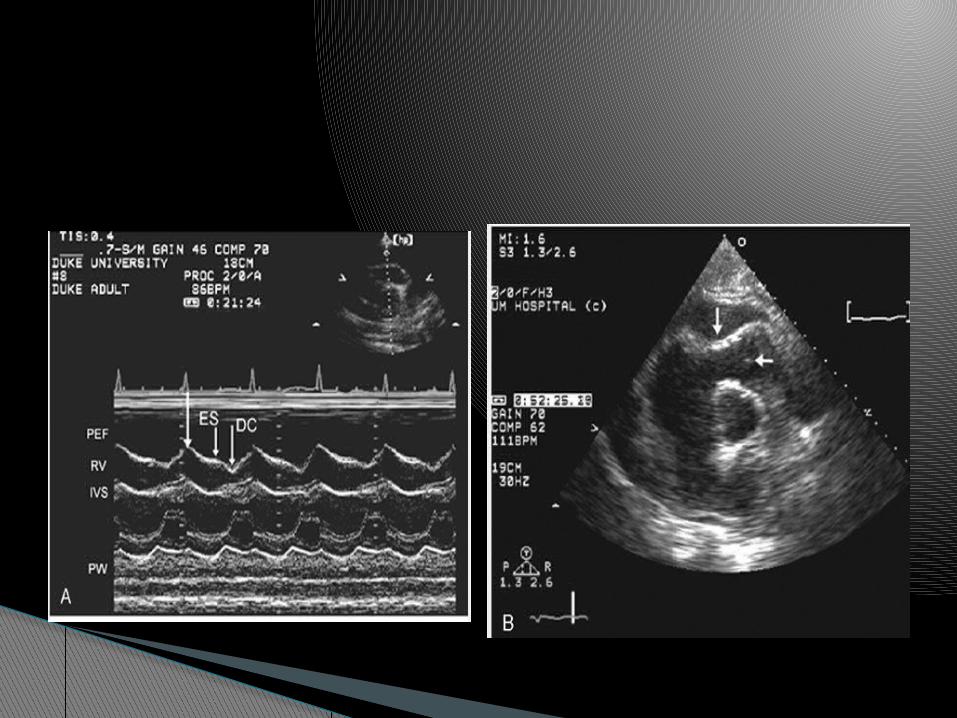
M-mode ,2D,Doppler Swinging heart,PSEUDOHYPERTROPHY Bouncing of IVS Collapse of chambers IVC and HV phletora Doppler flow velocity,sv,co
How severe?

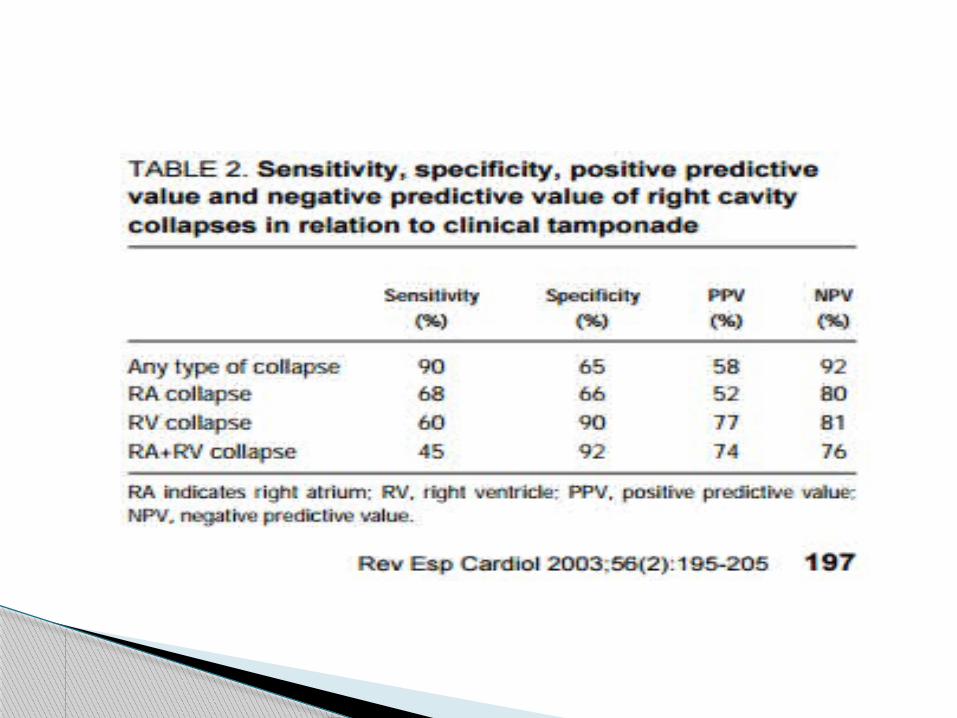
Right atrial collapse occurs immediately after normal atrial systolic contraction
If RA collapse 1/3 of the cardiac cycle it is sensetive and specific.
early diastolic collapse of the RV
The collapse of right heart chambers does not occur even with tamponade if right heart pressure is elevated, these signs may be absent in low-pressure tamponade
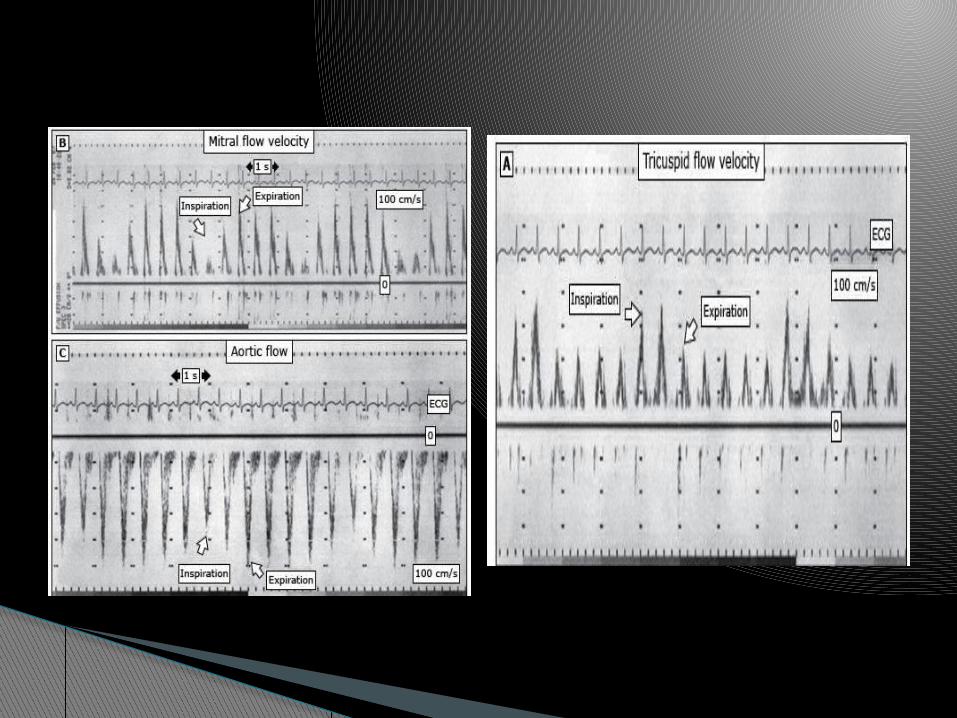
peak velocity of mitral inflow varies by 15% or more with respiration and tricuspid inflow by 25% or more.
Variation in peak velocity and time velocity integral of aortic and pulmonary flow profiles typically is less than 10%
Transmitral resp varn > 25% and transtricuspid varn > 50% are characterestic of tamponade.
Doppler Findings in Tamponade

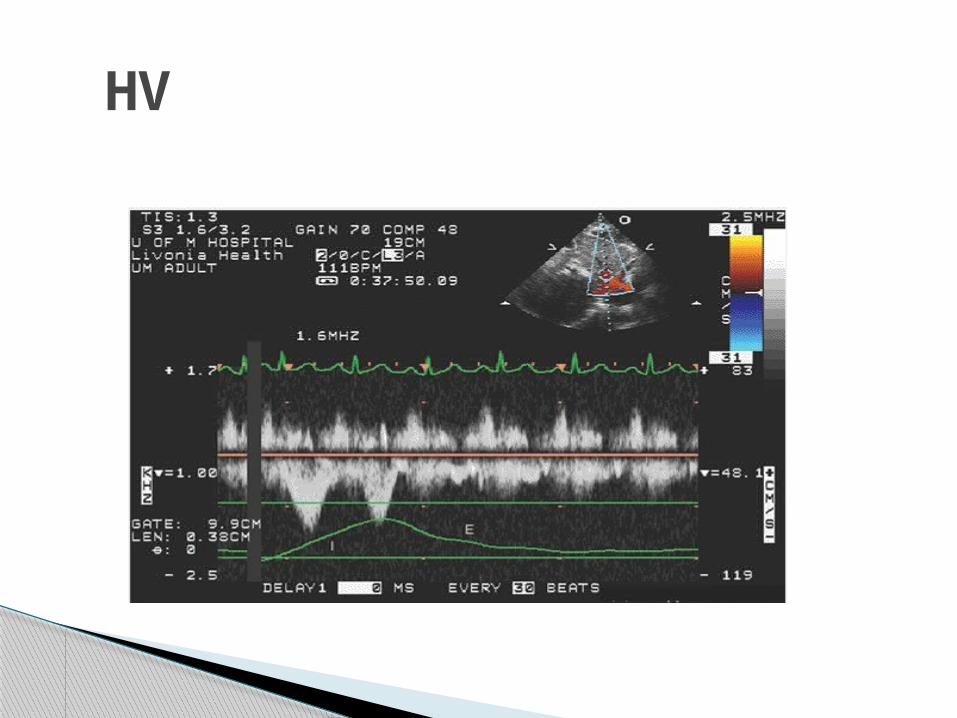
HV

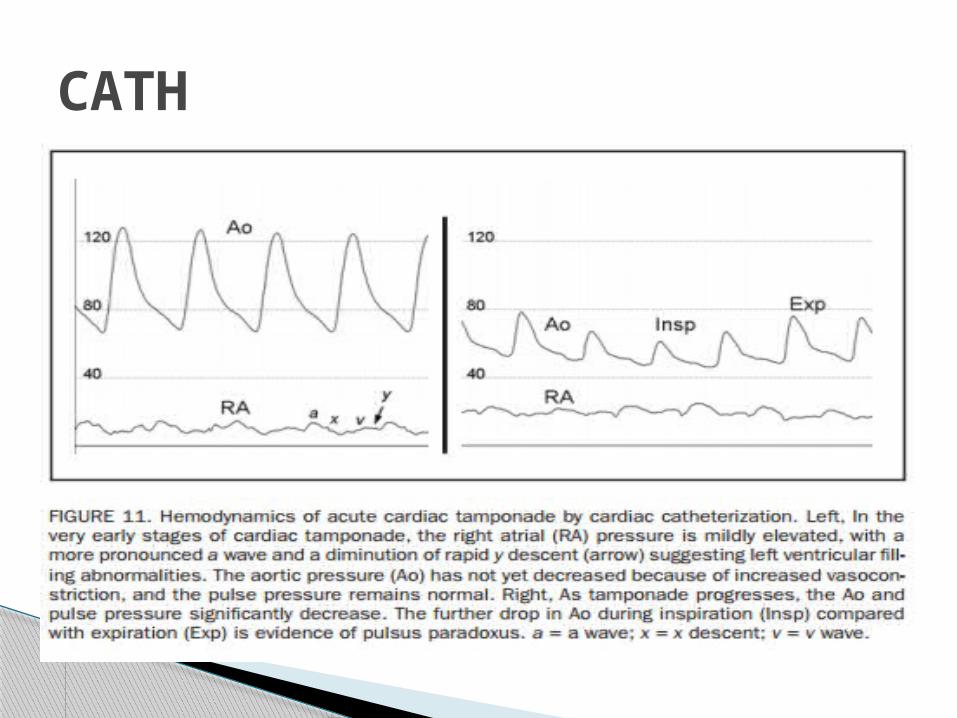
CATH
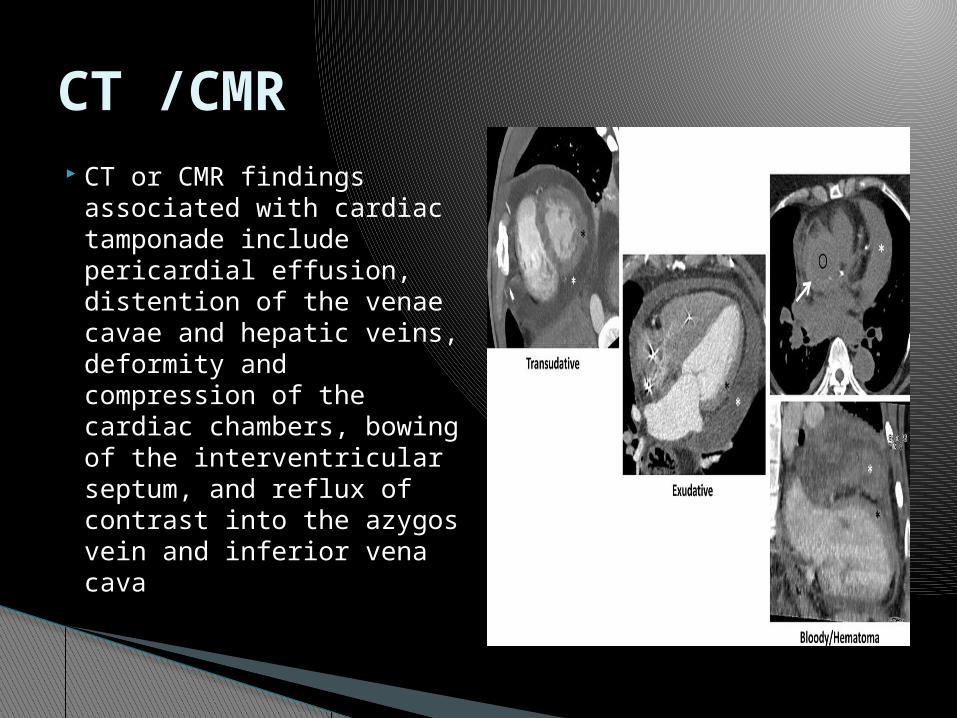
CT or CMR findings associated with cardiac tamponade include pericardial effusion, distention of the venae cavae and hepatic veins, deformity and compression of the cardiac chambers, bowing of the interventricular septum, and reflux of contrast into the azygos vein and inferior vena cava
CT /CMR
Effusive–constrictive pericarditis is a clinical–haemodynamic syndrome in which there is constriction of the heart by the visceral pericardium in the presence of effusion in free pericardial space.
The hallmark of effusive–constrictive pericarditis is the demonstration of persistently raised right atrial and end diastolic ventricular pressures after the intrapericardial pressure is reduced to normal levels by removal of pericardial fluid.
Effusive–constrictive pericarditis

summary

Nanda,compresive texetbook of Echocardiography Feigenbaum's Echocardiography, 7th Edition
Pathophysiology of Cardiac Tamponade* David H. Spodick, MD, DSc, FCCP (CHEST 1998; 113:1372-78)
Spodick DH. Acute cardiac tamponade. N Engl J Med 2003; 349:684.
Sagristà-Sauleda J, Angel J, Sambola A, et al. Low-pressure cardiac tamponade: clinical and hemodynamic profile. Circulation 2006; 114:94
ACC/AHA/ASE 2003 guideline Gillam LD, Guyer
DE, Gibson TC, et al. Hydrodynamic compression of the right atrium: a new echocardiographic sign of cardiac tamponade. Circulation 1983; 68:294.
Little WC, Freeman GL. Pericardial disease. Circulation 2006; 113:1622 ESC GUIDLINESS ON PERICARDIAL DISEASE 2004
Reference
Thank you!!

Test of choice for rapid assessment of pericardial effusions, but these findings are often absent in pts w/ pulm HTN or RVH
Characteristic Findings◦ Pericardial effusion
Size often correlates w/ risk of tamponade but not always◦ End-diastolic chamber collapse
RV expiratory collapse in early diastole (low sens, high spec) RA expiratory collapse in late diastole (high spec if inward movement lasts
> 30% of cardiac cycle) LA collapse (present in ~ 25%, highly spec)
◦ Respiratory variation in transvalvular velocities during passive diastolic filling. Transmitral resp varn > 25% transtricuspid varn > 50% are char of
tamponade. ◦ IVC dilated & fails to collapse w/ inspiration (reflects elev’d CVP) ◦ Small cardiac chambers◦ Swinging of the heart anteroposteriorly w/in the pericardial effusion◦ Reciprocal size changes w/ respiration b/w RV & LV & their valves
Related Documents











