Vol. 22, No. 1 January 2000 Refereed Peer Review FOCAL POINT KEY FACTS #Arrhythmias are common in the perianesthetic period and should be recognized, thus the electrocardiograph is an important monitoring device that should be used in all anesthetized patients. Perianesthetic Arrhythmias Mississippi State University University of Georgia L ynne I. Kushner, DVM Clay A. Calvert, DVM ABSTRACT: The patients discussed in this article were presented to the Veterinary Teaching Hospital at Mississippi State University for a variety of surgical or medical procedures requir- ing anesthesia. The electrocardiograms of all patients were monitored during induction and maintenance of anesthesia. A variety of arrhythmias were recorded, including heart blocks, ex- trasystoles, escape complexes, and accelerated junctional or ventricular rhythms. Noncardiac causes were implicated in all cases. Some arrhythmias may produce hemodynamic instability, whereas others may not. Although specific antiarrhythmic agents were not required, alteration in anesthetic management was necessary in these patients to resolve the arrhythmia and avert serious consequences. T he incidence of cardiac arrhythmias in the perioperative period in human patients ranges from 18% to 70%. 1,2 Incidence varies with degree of monitoring, type of anesthetic, presence or absence of preexisting disease, and ventilatory status. Although specific statistics are unknown, cardiac arrhyth- mias are also common in anesthetized veterinary patients. 3,4 Causes of arrhythmia during anesthesia and surgery include altered physio- logic states, autonomic imbalance, and adverse effects of drugs and drug interac- tions. 2,3 In humans, arrhythmias may be more common when heart disease is present 2 ; in our opinion, most arrhythmias in veterinary patients have a noncar- diac cause. Although most arrhythmias are often benign (i.e., causing no physio- logic or circulatory impairment), some may result in significant cardiovascular impairment if unrecognized or potentiated by anesthetic agents. The following electrocardiograms a (ECGs) and case descriptions are of pa- tients presented to the V eterinary Medical Te aching Hospital at Mississippi State University. All patients were either normal and healthy or had only mild sys- temic disease and were presented for routine medical or surgical procedures. None of the patients had documented cardiac disease. This article describes some common arrhythmias, speculates on their causes, and discusses their rele- vance and possible treatment. CASE 1 A 5-year-old Boston terrier required anesthesia for dental cleaning and tooth extraction. The dog was premedicated with acepromazine (0.05 mg/kg intra- muscularly [IM]), oxymorphone (0.05 mg/kg IM), and glycopyrrolate (0.01 mg/kg IM) 40 minutes before the preinduction ECG was recorded (Figure 1). CE V I Preanesthetic and induction agents can alter autonomic balance, which can result in a variety of arrhythmias that may or may not be clinically significant. I Bradyarrhythmias and heart blocks may often result from opioid and tranquilizer administration but may not be clinically significant if cardiac output is not adversely affected. I Anticholinergics may produce such arrhythmias as complex second-degree atrioventricular block and extrasystole s. I Ventricular premature complexes can have a variety of noncardiac causes and often do not require specific antiarrhythmic drug administration but may require changes in anesthetic management to prevent serious consequences. a All ECGs were recorded in lead II at a paper speed of 25 mm/second; they were not stan- dardized for sensitivity.

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8/14/2019 Perianesthetic Arrhythmias
http://slidepdf.com/reader/full/perianesthetic-arrhythmias 1/10
Vol. 22, No. 1 January 2000
Refereed Peer Review
FOCAL POINT
KEY FACTS
#Arrhythmias are common in
the perianesthetic period and
should be recognized, thus
the electrocardiograph is an
important monitoring device
that should be used in all
anesthetized patients.
Perianesthetic Arrhythmias
Mississippi State University University of Georgia
Lynne I. Kushner, DVM Clay A. Calvert, DVM
ABSTRACT: The patients discussed in this article were presented to the Veterinary Teaching
Hospital at Mississippi State University for a variety of surgical or medical procedures requir-
ing anesthesia. The electrocardiograms of all patients were monitored during induction and
maintenance of anesthesia. A variety of arrhythmias were recorded, including heart blocks, ex-trasystoles, escape complexes, and accelerated junctional or ventricular rhythms. Noncardiac
causes were implicated in all cases. Some arrhythmias may produce hemodynamic instability,
whereas others may not. Although specific antiarrhythmic agents were not required, alteration
in anesthetic management was necessary in these patients to resolve the arrhythmia and avert
serious consequences.
The incidence of cardiac arrhythmias in the perioperative period in humanpatients ranges from 18% to 70%.1,2 Incidence varies with degree of monitoring, type of anesthetic, presence or absence of preexisting disease,
and ventilatory status. Although specific statistics are unknown, cardiac arrhyth-mias are also common in anesthetized veterinary patients.3,4
Causes of arrhythmia during anesthesia and surgery include altered physio-
logic states, autonomic imbalance, and adverse effects of drugs and drug interac-tions.2,3 In humans, arrhythmias may be more common when heart disease ispresent2; in our opinion, most arrhythmias in veterinary patients have a noncar-diac cause. Although most arrhythmias are often benign (i.e., causing no physio-logic or circulatory impairment), some may result in significant cardiovascularimpairment if unrecognized or potentiated by anesthetic agents.
The following electrocardiogramsa (ECGs) and case descriptions are of pa-tients presented to the Veterinary Medical Teaching Hospital at Mississippi StateUniversity. All patients were either normal and healthy or had only mild sys-temic disease and were presented for routine medical or surgical procedures.None of the patients had documented cardiac disease. This article describessome common arrhythmias, speculates on their causes, and discusses their rele-
vance and possible treatment.
CASE 1 A 5-year-old Boston terrier required anesthesia for dental cleaning and tooth
extraction. The dog was premedicated with acepromazine (0.05 mg/kg intra-muscularly [IM]), oxymorphone (0.05 mg/kg IM), and glycopyrrolate (0.01mg/kg IM) 40 minutes before the preinduction ECG was recorded (Figure 1).
CE
V
I Preanesthetic and induction
agents can alter autonomic
balance, which can result in
a variety of arrhythmias that
may or may not be clinically
significant.
I Bradyarrhythmias and heart
blocks may often resultfrom opioid and tranquilizer
administration but may not be
clinically significant if cardiac
output is not adversely affected.
I Anticholinergics may produce
such arrhythmias as complex
second-degree atrioventricular
block and extrasystoles.
I Ventricular premature complexes
can have a variety of noncardiac
causes and often do not require
specific antiarrhythmic drug
administration but may require
changes in anesthetic
management to prevent serious
consequences.
a All ECGs were recorded in lead II at a paper speed of 25 mm/second; they were not stan-dardized for sensitivity.

8/14/2019 Perianesthetic Arrhythmias
http://slidepdf.com/reader/full/perianesthetic-arrhythmias 2/10
Second-degree atrioventricular (AV) block is charac-terized by an interruption of AV conduction that re-sults in one or more P waves that are not followed by aQRS-T complex.5 When found in normal dogs, it ismost often associated with sinus arrhythmia and othercauses of increased vagal tone.5 Brachycephalic breeds
as well as young or athletic dogs may have hyperactivevagal reflexes.6,7 Response to anticholinergic drug ad-ministration would verify a vagal cause and an anti-cholinergic drug is indicated if bradycardia adversely affects cardiac output. Although an ECG was not re-corded before premedication in this patient, ausculta-tion did not indicate preexisting bradyarrhythmia.
Many drugs, including α2 agonists (e.g., xylazine8)and opioids (e.g., oxymorphone,9 butorphanol10), pro-duce bradyarrhythmias as a result of increased vagaloutflow. Acepromazine may either increase or not havea significant effect on heart rate (HR) but may produceprofound bradycardia in susceptible dogs by increasingcentral cholinergic outflow.11 Acepromazine’s role inpotentiating vagal activity in brachycephalic breeds hasbeen reviewed.12,13
Oxymorphone was the most likely cause of the ar-rhythmia in this patient, with acepromazine being apotentiating factor. Glycopyrrolate was apparently inef-fective in producing vagal blockade. Although anti-cholinergic administration would increase HR and re-store rhythm, the dog was hemodynamically stable andinduction with thiopental proceeded with no complica-tions. The HR remained around 80 beats/min with nofurther evidence of heart block.
CASE 2 Anesthesia and surgery were planned for a healthy, 7-
year-old dachshund. The patient was premedicated with butorphanol (0.3 mg/kg IM) and midazolam (0.2mg/kg IM), and a preinduction ECG was recorded(Figure 2A). Because of the low HR, atropine (0.02mg/kg) was administered intravenously (IV).
In sinus block, the sinoatrial (SA) node discharges
but does not depolarize the atria; si-nus arrest occurs because no sinus im-pulse is formed.5 Electrocardiographi-cally, sinus block and sinus arrest aredifficult to differentiate; however, apause that encompasses exact multi-
ples of R-R intervals suggests sinusblock.5
In addition to pathologic conditionsof the atria, sinus arrest/block oftenoccurs with sinus arrhythmia causedby increased vagal tone.5 The brady-cardia (Figure 2A) may be attributed
to butorphanol, an opioid with mixed agonist–antago-nist activity. Butorphanol produces bradycardia similarto that caused by oxymorphone in acepromazine-sedat-ed dogs.9 Midazolam, a water-soluble benzodiazepine
with twice the potency of diazepam,14 was added in thiscase to improve the sedative effects of butorphanol. An
escape complex occurs when lower pacemakers dis-charge to rescue the heart.
Atropine, a competitive muscarinic-receptor antago-nist, is used to correct vagally mediated bradycardia.However, atropine often produces initial slowing of HR,
with or without AV block, especially at low dosages15;the causative mechanism initially proposed was centralstimulatory effects on vagal centers.15,16 Recent evidence,however, suggests a peripheral mechanism involvingaugmentation of acetylcholine release by high-affinity presynaptic muscarinic receptors, followed by blockadeof low-affinity postsynaptic muscarinic-receptor sub-types, which results in parasympatholytic effects.17 Inaddition, current hypotheses include a difference in sen-sitivity or distribution of muscarinic receptors at the SA and AV nodes, which may account for the differentialresponse in SA and AV nodal activity.16,17
A recent study demonstrated this biphasic responsein HR after IM and IV administration of atropine.17
This effect was also demonstrated in this case. Afterseveral minutes, the HR and rhythm improved and in-duction proceeded without complication or furtherheart block.
CASE 3
A healthy, 1.5-year-old Labrador retriever was anes-thetized for surgical correction of osteochondritis desic-cans. After moderate sedation with acepromazine (0.05mg/kg IM) and oxymorphone (0.05 mg/kg IM), anes-thesia was induced with thiopental (12 mg/kg IV admin-istered to effect) and maintained with halothane andoxygen. Approximately 3 to 5 minutes after inhalationanesthesia began, an arrhythmia was noted (Figure 3).
Ventricular premature complexes (VPCs) arise from
Small Animal/Exotics Compendium January 2000
S E C O N D - D E G R E E A T R I O V E N T R I C U L A R B L O C K I O X Y M O R P H O N E I S I N U S B L O C K
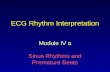
Figure 1—Second-degree atrioventricular (AV) block. The atrial and ventricular ratesare 100 and 60 beats/min, respectively. The P-R interval preceding the nonconduct-ed P wave (0.14 seconds) is slightly longer than the first P-R interval (0.12 seconds)of the pair. This describes a Mobitz type 1 (Wenckebach phenomenon) second-de-gree AV block.5

8/14/2019 Perianesthetic Arrhythmias
http://slidepdf.com/reader/full/perianesthetic-arrhythmias 3/10
ectopic foci in the ventricles and result in bizarre, wid-ened QRS complexes that are not associated with P waves.5
Classification of the severity of VPCs is based on (1)the number of single VPCs per minute; (2) whetherthey are multiform or uniform in appearance; (3) if they occur early on the preceding T wave (i.e., R-on-Tphenomenon); or (4) if they occur in pairs, runs, orparoxysms.5 If VPCs occur frequently enough to pro-duce circulatory impairment, treatment should be insti-tuted.
In addition to cardiac disease, VPCs can have numer-ous noncardiac causes, including electrolyte and acid–base imbalance, autonomic imbalance, hypoxia, andhypercapnia.5 Circulating catecholamines can increasebecause of stress, pain, and excitement and exert theirpotential arrhythmogenic effects by binding to α- andβ-adrenergic receptors within the myocardium.18 Themyocardial sensitization to epinephrine by anesthetic
agents has recently been reviewed.19
The arrhythmo-genicity of a drug can be measured by determining itseffect on the arrhythmogenic dose of epinephrine(ADE). One study determined the receptor mechanismthat mediates epinephrine-induced arrhythmias duringhalothane administration; the ADE was increased thegreatest after α1 blockade, suggesting that mediation of sensitization by halothane is predominantly an α1 re-ceptor–effector mechanism.18 Anesthetic agents that have
lowered the ADE include thiobarbiturates,20,21 pro-pofol,22 and halothane.23 Xylazine and ketamine may ormay not enhance arrhythmogenicity.24–27
Thiopental or halothane administration, hypoxia,and hypercapnia are potential precipitating causes inthis healthy dog. It is well established that thiopentalpotentiates halothane-epinephrine–induced arrhyth-mias.20,21 In addition, the duration of this potentiationcan exceed 4 hours, well beyond thiopental’s clinical ef-fects.20,21 This arrhythmia was noticed soon after halo-thane was administered, but anesthetic concentrationsof halothane were not measured. Myocardial epi-nephrine sensitization may occur with halothane con-centrations as low as 0.1%.28
Because oxygen–hemoglobin saturation and partialpressure of arterial carbon dioxide concentrations werenot measured, it cannot be stated with certainty wheth-er hypoxia and/or hypercapnia played a role in the
genesis of this arrhythmia. The dog was immediately ventilated with several breaths to ensure adequate oxy-genation and ventilation, but normal rhythm was notrestored and ventricular ectopic beats continued withsimilar frequency. Because the dog’s mucous membranecolor, capillary refill time, pulse quality, and depth of anesthesia were assessed as adequate, surgery proceeded
with vigilant monitoring. Halothane was replaced withisoflurane with little response in the frequency of the
Compendium January 2000 Small Animal/Exotics
V E N T R I C U L A R P R E M A T U R E C O M P L E X E S I A R R H Y T H M O G E N I C D O S E O F E P I N E P H R I N E I H A L O T H A N E
Figure 2A
Figure 2B
Figure 2—( A
) Marked sinus arrhythmia with a ventricular rate of 60 to 80 beats/min. Sinus block/arrest results in long pausesequal to or greater than two R-R intervals. An escape complex, probably either atrioventricular (AV) nodal or high septal in ori-gin, interrupts the block. The P wave can be seen after the QRS complex (arrow) . (B) An advanced second-degree AV block oc-curs. More than one consecutive P wave is not conducted. The atrial rate is 130 beats/min, and the ventricular rate is 60beats/min. Escape beats, which may be AV nodal or high ventricular in origin, occur independent of the rhythm of sinoatrialnode depolarization. P waves occur before, within, and after the QRS of the escape complexes.

8/14/2019 Perianesthetic Arrhythmias
http://slidepdf.com/reader/full/perianesthetic-arrhythmias 4/10
arrhythmia. Although indirect blood pressure remainedsatisfactory, lidocaine (2 mg/kg IV) was eventually ad-ministered and was successful in restoring normal sinusrhythm.
CASE 4 A healthy, 3-year-old, 32-kg rottweiler was presented
for ovariohysterectomy. Because of a history of potentialaggression, heavy sedation was accomplished with xy-lazine (0.3 mg/kg IM), butorphanol (0.2 mg/kg IM),and glycopyrrolate (0.015 mg/kg IM). An IV catheter
was placed with little physical restraint. A preinductionECG (not depicted) revealed sinus rhythm with an HR of 140 beats/min. Induction with thiopental was about tobegin when an arrhythmia suddenly emerged (Figure 4).
In bigeminal or trigeminal rhythms, the interval be-tween the sinus and ectopic beat is constant (fixed cou-pling). This indicates that the sinus beat controls thedischarge of the ectopic focus by a reentry mechanism inthe myocardium.29
Noncardiac causes were considered in this normal,healthy dog. Drugs administered to this dog that couldbe implicated in the genesis of ventricular extrasystoles
include glycopyrrolate and xylazine. Dogs receiving gly-copyrrolate, xylazine, and butorphanol exhibited de-creases in cardiac index with ST segment depression,pulsus alternans, and occasional VPCs.30
Xylazine either decreased8,24 or did not alter the ADE25 in anesthetized dogs, but differences in method-ologies and end points may have accounted for dis-agreement in the results. Dexmedetomidine, a highly selective α2 agonist, inhibited the arrhythmogenic effect
of epinephrine in halothane-anesthetized dogs.31 Bilat-eral vagotomy abolished this antiarrhythmogenic effect,suggesting protection from parasympathetic tone.32
Parasympatholytics may induce autonomic imbal-ance, resulting in extrasystoles. Atropine administrationin dogs resulted in a higher frequency of ectopicrhythm disturbances than in control dogs that did notreceive atropine.15 However, in a recent study, choliner-gic blockade increased the threshold to epinephrine-in-duced arrhythmias in halothane- and isoflurane-anes-thetized dogs.33
In this case, induction was delayed while the ECG, which improved over several minutes, was observed.Because the dog’s mucous membrane color, capillary re-fill time, and pulses were good, induction was stillplanned but thiopental was no longer considered be-cause of its potential arrhythmogenicity. Diazepam(0.3 mg/kg IV) followed by ketamine (2 mg/kg IV)
was administered, and intubation was easily accom-plished. Normal sinus rhythm remained, and no fur-ther arrhythmia was observed.
CASE 5
A 13-year-old cocker spaniel required anesthesia formammary tumor removal. A preoperative radiographicevaluation for possible metastasis revealed no signifi-cant abnormalities of the lung fields or cardiac silhou-ette. The dog was premedicated with oxymorphone(0.05 mg/kg IM), midazolam (0.2 mg/kg IM), and gly-copyrrolate (0.015 mg/kg IM). Normal sinus rhythm
was noted immediately before induction with thiopen-tal (10 mg/kg IV to effect). During endotracheal intu-
Small Animal/Exotics Compendium January 2000
V E N T R I C U L A R T R I G E M I N Y I X Y L A Z I N E I P A R A S Y M P A T H O L Y T I C S
Figure 3—Heart rate is 160 beats/min with ventricular premature complexes (arrows) . These complexes are not followed by apause and are called interpolated ; they do not disrupt the ventricular rhythm.
Figure 4—Ventricular trigeminy (two sinus beats followed by ventricular premature complexes [arrows] in a repetitive pattern).The ventricular rate is 140 beats/min. The arrhythmia persisted for approximately 10 minutes.

8/14/2019 Perianesthetic Arrhythmias
http://slidepdf.com/reader/full/perianesthetic-arrhythmias 5/10
bation, an arrhythmia was noted and recorded (Figures5A and 5B). Immediately after intubation, normal si-nus rhythm was restored (Figure 5C).
Supraventricular premature complexes originate inatrial or AV nodal tissue.5 The P waves, if visible, shoulddiffer slightly from the sinus P waves and can occur be-fore, during, or after the QRS complex. The QRS com-plex should usually have a similar conformation to thatassociated with sinus beats. When AV nodal prematurebeats are indistinguishable from those of atrial origin,supraventricular is the appropriate terminology. Atrialpremature complexes are often associated with heart dis-
ease, although they can occur in normal dogs.5
In oneexperimental study, atrial arrhythmias preceded ventric-ular arrhythmias during epinephrine-induced sensitiza-tion with halothane and isoflurane.21
The fact that the arrhythmia resolved immediately after intubation argues strongly for laryngeal stimula-tion as the precipitating cause. Stimulation of the lar-ynx by laryngoscopy and intubation can cause tachy-cardia, hypertension, and cardiac arrhythmias by an
absolute or relative increase in sympathetic tone. How-ever, parasympathetic stimulation is also possible.1,4 Ec-topic complexes resolved after the HR decreased (180to 100 beats/min), which supports a mechanism of au-tonomic imbalance from increased sympathetic stimu-lation.
Hypoxia and hypercapnia can induce cardiac ar-rhythmia indirectly by release of catecholamines or di-rectly by depression of cardiac cells and stimulation of the vasomotor centers of the brain.4 However, manualventilation was not required to restore the rhythm inthis case. If intubation had not been initially successful,
ceasing attempts at intubation would have been advis-able. Delivery of oxygen via a face mask using highoxygen flow rates before further attempts at intubationmay help avoid a more serious arrhythmia and its con-sequences. After intubation, no further arrhythmia wasobserved and surgery and recovery were uneventful.
CASE 6 A 10-month-old cat was administered tiletamine–zo-
Compendium January 2000 Small Animal/Exotics
S U P R A V E N T R I C U L A R P R E M A T U R E C O M P L E X E S I A T R I A L A R R H Y T H M I A S I L A R Y N G E A L S T I M U L A T I O N
Figure 5C
Figure 5—( A ) Ventricular premature complexes (VPCs; arrows ) occur regularly following three sinus complexes. The ventricularheart rate (HR) is 170 beats/min. (B) There are supraventricular complexes of either atrial or atrioventricular nodal origin (small arrows) occurring in a bigeminal pattern; T waves preceding each supraventricular beat appear deeper, suggesting an additive neg-ative P-wave effect. VPCs are also present (large arrows) . (C) Immediately after intubation, the HR is 100 beats/min with no pre-mature complexes.
Figure 5A
Figure 5B

8/14/2019 Perianesthetic Arrhythmias
http://slidepdf.com/reader/full/perianesthetic-arrhythmias 6/10
lazepam (4 mg/kg IM), intubated, and maintained withhalothane for ovariohysterectomy. Approximately 30minutes later, during surgery, abnormal complexes werenoted on the ECG (Figure 6).
Fusion beats are the result of simultaneous activationof the ventricle by impulses from the SA node and ven-tricular ectopic foci.29 The QRS is intermediate in formbetween the sinus and ectopic QRS. Ventricular ectopic
beats were not noted until the viscera was manipulated.Catecholamine release from painful stimuli, especially in the presence of halothane, can result in ventriculararrhythmias.4,34 Palpebral reflex and jaw tone suggesteda light plane of anesthesia. Attempts were made to in-crease the anesthetic plane by increasing ventilation andvaporizer concentration. Because isoflurane was readily available, halothane was discontinued. The rhythm wasquickly restored with no further abnormalities. Discon-tinuation of halothane may not have been necessary—increasing halothane concentration has been shown toresult in resolution of ventricular arrhythmias.34
Tiletamine–zolazepam is an unlikely factor in the gen-esis of this arrhythmia. It did not affect ADE in catsanesthetized with halothane.35
CASE 7 A 1-year-old domestic shorthair cat was given tile-
tamine–zolazepam (4 mg/kgIM) for castration and ony-chectomy. Because the anes-thetic depth was judged tobe inadequate, halothane wasadministered by face mask.During surgery, an abnormal
rhythm was noted on the ul-trasonic Doppler flow detec-tor, which was recording pulserhythm at the metatarsal ar-tery. An ECG was recorded(Figure 7).
Vital signs and anestheticdepth were quickly evaluat-ed. There was no palpebral
reflex or jaw tone, and the va-porizer was turned off tem-porarily. Because there wasno patent airway, the cat wasimmediately intubated. Sinusrhythm was restored with the
administration of one or twobreaths. Surgery and recovery proceeded uneventfully.
Although the cat was nei-ther apneic nor cyanotic, res-
piration was assumed to be inadequate because the ar-rhythmia disappeared immediately after intubation. If anECG had not been eventually monitored, change inmanagement may have been unlikely. Rapidly occurringmultiform VPCs may lead to ventricular tachycardia andfibrillation.5 This case demonstrates the importance of adequate oxygenation, supportive care, and monitoring.
CASE 8 A 10-year-old Labrador retriever with upper airway
stridor was to be anesthetized for possible laryngoplasty. After premedication with butorphanol and diazepam,the ECG was monitored in preparation for induction.
An irregular rhythm with abnormal complexes wasrecorded (Figure 8). The surgeon’s concern that heartdisease was present prompted cancellation of surgery until cardiac evaluation was completed.
Right bundle branch block (RBBB) is a delay or in-terruption of conduction through the right bundlebranch. Normally, the right ventricle is activated by animpulse that passes from the bundle of His to the rightbundle branch. With RBBB, the right ventricle is acti-vated by an impulse that passes from the left bundlebranches to the right side of the septum below theblock, with delay causing the QRS to be wide andbizarre.36 In this case, P-P intervals become progressive-
ly shorter and P-R intervalsremain the same. The AV impulse enters the conduct-ing system before the rightbundle branch has a chanceto repolarize, thereby pro-ducing aberrant conduction.
This pattern persisted through-out the ECG.Criteria of complete RBBB
includes a QRS complexlonger than 0.08 seconds; aright axis deviation; anddeep S waves in leads I, II,III, and aVF. RBBB can beassociated with heart disease
Small Animal/Exotics Compendium January 2000
F U S I O N B E A T S I C A T E C H O L A M I N E R E L E A S E I O X Y G E N A T I O N
Figure 7—In a repetitive pattern, triplets of multiform ven-tricular premature complexes (large arrows) can be seen fol-lowing two possible sinus complexes. However, the second“sinus beat” (small arrow) may be an atrial premature com-plex because, compared with the previous sinus beat, the P
wave is smaller and there is no S wave on the subsequentQRS complex.
Figure 6—The ventricular rate is 170 beats/min. In addition to sinus complexes, there are mul-tiform ventricular complexes with both right (1) and left (2) bundle branch block patterns.Fusion beats (F) resemble both forms of ventricular premature complexes.

8/14/2019 Perianesthetic Arrhythmias
http://slidepdf.com/reader/full/perianesthetic-arrhythmias 7/10
but also can occur in normal, healthy dogs or as an in-cidental finding in dogs with noncardiac diseases.36
RBBB alone does not require treatment, produces no
hemodynamic problems, and should not present a con-cern for anesthesia. It is important not to confuseRBBB with VPCs; the former can be distinguished by preceding consistent P-R intervals.
An echocardiogram demonstrated normal cardiac di-mensions and function. Anesthesia and surgery pro-ceeded without complication.
CASE 9 A 6-year-old cat was diagnosed with leukocytopenia
of undetermined cause. An echocardiogram revealed nosignificant findings. Months later, the cat was presentedfor an ovariohysterectomy and follow-up bone-marrowbiopsy. There were no significant findings on physical orhematologic examination. Ketamine (5 mg/kg), butor-phanol (0.2 mg/kg), and midazolam (0.1 mg/kg ) wereadministered IM and produced adequate sedation. A preinduction ECG was not recorded. Thiopental wasadministered IV to effect for intubation, and anesthesia
was maintained with isoflurane. An ECG was recordedduring surgical preparation (Figure 9A).
A pararrhythmia is an abnormal rhythm in whichtwo pacemakers discharge independently of each other,and each can activate the ventricle at different times.38
AV dissociation is one example in which the dominant
pacemaker (AV junction or ventricle) controls ventricu-lar activation and another pacemaker (SA node or atri-al) controls the atria. Incomplete AV dissociation oc-curs if an impulse from the SA node conducts to theventricle, producing a ventricular capture beat. This oc-curs after every second or third QRS complex (Figure9A). AV dissociation is a sign of a primary disturbanceand is not an ECG rhythm diagnosis. This disturbancecan result from depressed SA node automaticity allow-
ing an AV junctional or ventricular focus totake over, increased AV junctional or ven-tricular automaticity, disturbed AV conduc-tion, or a combination of mechanisms.37
Decreased SA node automaticity and an ac-celerated ventricular rhythm may be the
mechanisms involved in this case. Although AV dissociation may be associated withheart disease, it has been reported in ahealthy cat during inhalation anesthesia.39
Isoflurane slows the rate of SA pacemakerdischarge by direct and indirect effects onSA node automaticity.40 In addition, isoflu-rane at increased concentrations lengthens
AV nodal conduction time. The depressanteffects of anesthetics on AV nodal conduc-
tion with depression of sinus nodal automaticity couldfavor an occurrence of AV dissociation.40
AV dissociation resulting from accelerated junc-
tional rhythms can be caused by sympathetic stimula-tion of AV nodal pacemaker cells or parasympatheticoverriding of the sympathetic nervous system as a re-sult of autonomic imbalance. These arrhythmias havebeen successfully treated with propranolol41 and at-ropine.42 Atropine was administered in the cat in thiscase because of the low HR and marginally low sys-tolic pressures. Although atropine increased HR toonly 100 beats/min, sinus rhythm was restored (Fig-ure 9C).
CASE 10 A 6-year-old Brittany spaniel was admitted for surgery
1 day after being hit by a car. The dog, which had anopen fracture of the radius and ulna, was bright and alert.Radiographs of the thorax revealed mild changes consis-tent with heartworm disease; there were no significantfindings on abdominal films. Minimal laboratory data,consisting of packed cell volume, total protein, blood ureanitrogen, and glucose estimation, were within referenceranges.43
The following day, surgery was scheduled for internalfixation of the radius and ulna. The dog was premedi-cated with acepromazine (0.05 mg/kg IM) and oxy-morphone (0.05 mg/kg IM). A preinduction ECG was
normal (not depicted). Anesthesia was induced withthiopental and maintained with isoflurane. Forty-fiveminutes after surgery began, bradycardia with first- andsecond-degree AV block (not depicted) was noted. HR and indirect blood pressure began to drop quickly over10 minutes. P waves were no longer recognized (Figure10A). Atropine (0.02 mg/kg IV) was administered,producing electrocardiographic changes (Figure 10B).Blood was collected for electrolyte, chemistry, pH, and
Small Animal/Exotics Compendium January 2000
R I G H T B U N D L E B R A N C H B L O C K I A T R I O V E N T R I C U L A R D I S S O C I A T I O N I I S O F L U R A N E
Figure 8—Intermittent right bundle branch block (RBBB). QRS duration is0.12 seconds with deep S waves (arrows) . This is an example of phasic aber-rant conduction taking the usual form of rate-dependent RBBB. The R-R in-tervals preceding the RBBB become progressively shorter until RBBB occurs.
A marked sinus (vagal) arrhythmia is also evident. The ventricular rate is 80 to100 beats/min.

8/14/2019 Perianesthetic Arrhythmias
http://slidepdf.com/reader/full/perianesthetic-arrhythmias 8/10
blood gas determinations.Chemistry results that werenot within reference ranges43
included potassium (9.89mEq/L), blood urea nitro-gen (90 mg/dL), creatinine
(3.9 mg/dL), and albumin(1.4 g/dL). Blood gas re-sults using lingual venousblood were also out of ref-erence range43 and indicat-ed a respiratory and meta-bolic acidosis (pH, 7.14;partial pressure of carbondioxide, 66 mm Hg; par-tial pressure of oxygen, 450mm Hg; bicarbonate, 23mEq/L; base deficit, 8.3mEq/L).
Regular insulin (20 units)and 5% dextrose were add-ed to normal saline and ad-ministered at a rate of 20ml/kg IV. Sodium bicar-bonate (0.5 mEq/L IV) wasadministered slowly. Twen-ty minutes after the treat-ment, P waves were notice-able and a normal ECG wasrestored 30 minutes there-after (not depicted).
Loss of P-wave morphol-ogy with spiked T waves ishighly suggestive of hyper-kalemia.44,45 The restingmembrane potential (RMP)of cardiac muscle dependson a normal ratio of extracellular:intracellular potassiumconcentration.44 During hyperkalemia, the RMP is raised(becomes less negative). Fewer sodium channels are open,and thus depolarization to threshold potential (TP) is re-duced. The action potential duration is shortened, andthe rate of repolarization increases. The earliest manifes-tations of hyperkalemia on the ECG are peaked, narrow-
based T waves. The RMP decreases with further increas-es in potassium concentration, which in turn slowsintraventricular conduction and increases the duration of the QRS complex. Automaticity, conductivity, contrac-tility, and excitability are decreased.45
Various cardiac cells have a differential sensitivity torising extracellular potassium. Purkinje fibers and my-ocardial cells are the most sensitive, atrial cells more sothan ventricular.44,45 Experimental studies have shown
that the SA node continues to discharge and impulses aretransmitted to the AV node, and thereby to the ventri-cles, by specialized internodal conducting pathways. Theatria are not activated, and thus no P wave is recorded. 45
This is termed sinoventricular conduction .Insulin administration with glucose will result in
movement of potassium into the cells. Sodium bicar-
bonate also induces an intracellular potassium shift.Calcium can be administered in severe cases to restore anormal gradient of RMP to TP and to increase myocar-dial conduction and contractility.46
The fracture in this patient was quickly repaired. A ruptured bladder was suspected and confirmed by ultra-sound. Potassium enters the abdominal cavity from a rup-tured bladder and is reabsorbed, causing serum potassiumto increase. A celiotomy was performed, and approxi-
Compendium January 2000 Small Animal/Exotics
H Y P E R K A L E M I A I R E S T I N G M E M B R A N E P O T E N T I A L I T H R E S H O L D P O T E N T I A L
Figure 9C
Figure 9—( A ) The ventricular rate is 100 beats/min. The dominant rhythm occurs regularly at80 beats/min, with abnormal QRS morphology suggesting a ventricular origin. P waves (arrows ),although not clearly visible, may be present and are dissociated from the dominant rhythm. Oth-er leads might better delineate their presence. A P wave is also barely visible (arrow) in the T
waves preceding the capture beats (C) . Capture beats are sinus impulses that occasionally capturethe ventricles, making this a type of incomplete atrioventricular dissociation.37 (B) After atropine
(0.02 mg/kg IV) is administered, P waves are more clearly evident—demonstrating their occur-rence before, within, and after the QRS. The ventricular rate is 80 beats/min, and another cap-ture beat can be seen after the fourth complex. (C) After atropine is readministered, the ventricu-lar rate increases to only 100 beats/min but sinus rhythm is restored.
Figure 9A
Figure 9B

8/14/2019 Perianesthetic Arrhythmias
http://slidepdf.com/reader/full/perianesthetic-arrhythmias 9/10
mately 1 L of fluid was suc-tioned from the abdomen. A 3-cm rent was observed in thebladder and repaired. Serumpotassium was 6.1 mmol/L atthe completion of surgery, and
recovery occurred with support-ive care without further com-plications.
A ruptured bladder was notexpected either at the time of admission or on the day of surgery because of the dog’sbright attitude and lack of ra-diographic and clinical signs.More complete hematologicand biochemical evaluationmay have induced suspicionof a ruptured bladder. The
relatively high fluid rate of 10ml/kg/hour during anesthesiamost likely produced rapidurine production and bladderdistention to maintain paten-cy of the tear in the bladder.
Atropine was administered forthe sudden bradycardia butproduced a more aberrant cardiac rhythm.
SUMMARYIt is hoped that these cases demonstrate the impor-
tance of ECG monitoring in anesthetized patients. Al-though it is not a substitute for simple clinical assess-ments of pulse quality, mucous membrane color, andrespiration, ECG monitoring provides important infor-mation not available by any other means. Most of thearrhythmias described in this article did not require spe-cific treatment, but some required alteration in manage-ment that may have prevented serious consequences.
ACKNOWLEDGMENTThe authors thank Mr. Tom Thompson for his pho-
tographic assistance.
REFERENCES1. Katz RL, Bigger JT: Cardiac arrhythmias during anesthesiaand operation. Anesthesiology 23(2):193–213, 1970.
2. Atlee JL: Perioperative cardiac dysrhythmias: Diagnosis andmanagement. Anesthesiology 86(6):1397–1424, 1997.
3. Cohen RB, Tilley LP: Cardiac arrhythmias in the anes-thetized patient. Vet Clin North Am Small Anim Pract 9(1):155–162, 1979.
4. Hubbell JAE, Muir WW, Bednarski RM, Bednarski LS:Change of inhalation anesthetic agents for management of ventricular premature depolarizations in anesthetized cats
and dogs. JAVMA 185(6):643–646, 1984.5. Tilley LP: Analysis of common canine cardiac arrhythmias,
in Tilley LP (ed): Essentials of Canine and Feline Electrocar- diography Interpretation and Treatment . Philadelphia, Lea &Febiger, 1992, pp 127–207.
6. Bolton GR: Bradycardia, in Kirk RW (ed): Current Veteri- nary Therapy VII. Small Animal Practice. Philadelphia, WBSaunders Co, 1980, pp 376–380.
7. Branch CE, Robertson BT, Williams JC: Frequency of sec-ond-degree atrioventricular heart block in dogs. JAVMA 36:925–929, 1975.
8. Muir WW, Werner LL, Hamlin RJ: Effects of xylazine andacetylpromazine upon induced ventricular fibrillation indogs anesthetized with thiamylal and halothane. Am J Vet Res 36(9):1299–1303, 1975.
9. Cornick JL, Hartsfield SM: Cardiopulmonary and behav-ioral effects of combinations of acepromazine/butorphanoland acepromazine/oxymorphone in dogs. JAVMA 200(12):1952–1956, 1992.
10. Trim CM: Cardiopulmonary effects of butorphanol tartratein dogs. Am J Vet Res 44(2):329–331, 1983.
11. Muir WW: Anesthetics and techniques, in Slatter D (ed):Textbook of Small Animal Surgery . Philadelphia, WB Saun-ders Co, 1993, pp 2245–2250.
12. Brock N: Acepromazine revisited. Can Vet J 35:458–459,1994.
13. Dodman NH, Court MH: Questions about ECG interpre-tations. JAVMA 197(2):169–170, 1990.
14. Reves JG, Fragen RJ, Vinik RH, Greenblatt DJ: Midazolam:Pharmacology and uses. Anesthesiology 62(3):310–324, 1985.
15. Muir WW: Effects of atropine on cardiac rate and rhythm in
Small Animal/Exotics Compendium January 2000
S I N O V E N T R I C U L A R C O N D U C T I O N I R U P T U R E D B L A D D E R
Figure 10B
Figure 10—( A ) The ventricular rate of 50 to 60 beats/min with absence of P waves suggests ei-ther sinoventricular conduction or a junctional rhythm. The QRS morphology is abnormal,
which could be the result of aberrant conduction from increased serum potassium. T wavesare more than half the size of the R wave. (B) Because of the sudden development of brady-cardia, atropine is administered, after which the complexes are more aberrant, particularly atthe faster rates (i.e., S waves are deeper and wider [arrows] ); this may be caused by rate-de-pendent aberrant conduction in addition to that caused by the increased serum potassium.
Figure 10A

8/14/2019 Perianesthetic Arrhythmias
http://slidepdf.com/reader/full/perianesthetic-arrhythmias 10/10
dogs. JAVMA 172(1):917–921, 1978.16. Kantelip JP, Alatienne M, Gueorguiev G, Duchene-Marul-
laz P: Chronotropic and dromotropic effects of atropine andhyoscine methobromide in unanesthetized dogs. Br J
Anaesth 57:214–219, 1985.17. Rishniw M, Tobias AH, Slinker BK: Characterization of
chronotropic and dysrhythmogenic effects of atropine in
dogs with bradycardia. Am J Vet Res 57(3):337–341, 1996.18. Maze M, Smith CM: Identification of receptor mechanismmediating epinephrine-induced arrhythmias during halo-thane anesthesia in the dog. Anesthesiology 59(4):322–326,1983.
19. Lemke KA, Tranquilli WJ: Anesthetics, arrhythmias, andmyocardial sensitization to epinephrine. JAVMA 205(12):1679–1684, 1994.
20. Bednarski RM, Majors LJ, Atlee JL: Epinephrine-inducedventricular arrhythmias in dogs anesthetized with halothane:Potentiation by thiamylal and thiopental. Am J Vet Res 46(9):1829–1832, 1985.
21. Atlee JL, Malkinson CE: Potentiation by thiopental of halothane-epinephrine-induced arrhythmias in dogs. Anes- thesiology 57(4):285–288, 1982.
22. Kamibayashi T, Hayashi Y, Sumikawa K, et al: Enhance-ment by propofol of epinephrine-induced arrhythmia indogs. Anesthesiology 75(6):1035–1040, 1991.
23. Zink J, Sasyniuk BI, Dresel PE: Halothane-epinephrine-in-duced cardiac arrhythmias and the role of heart rate. Anes- thesiology 43(5):548–555, 1975.
24. Tranquilli WJ, Thurmon JC, Benson GJ: Alterations inepinephrine-induced arrhythmogenesis after xylazine andsubsequent yohimbine administration in isoflurane-anes-thetized dogs. Am J Vet Res 49(7):1072–1074, 1988.
25. Lemke KA, Tranquilli WJ, Thurmon JC, et al: Alterationsin the arrhythmogenic dose of epinephrine after xylazine ormedetomidine administration in isoflurane-anesthetizeddogs. Am J Vet Res 54(12):2139–2144, 1993.
26. Bednarski RM, Sams RA, Majors LJ, Ashcraft S: Reduction
of the ventricular arrhythmogenic dose of epinephrine by ketamine administration in halothane-anesthetized cats. Am J Vet Res 49(3):350–354, 1988.
27. Bednarski RM, Majors LJ: Ketamine and the arrhythmo-genic dose of epinephrine in cats anesthetized with halo-thane and isoflurane. Am J Vet Res 47(10):2122–2126, 1986.
28. Hayashi Y, Sumikawa K, Yamatodani A, et al: Myocardialepinephrine sensitization with subanesthetic concentrationsof halothane in dogs. Anesthesiology 74(1):134–137, 1991.
29. Goldman MJ: The ventricular arrhythmias, in Goldman MJ(ed): Principles of Clinical Electrocardiology. Los Altos, CA,Lang Medical Publications, 1986, pp 260–277.
30. Jacobson JD, McGrath CJ, Ko JCH, Smith EP: Cardiore-spiratory effects of glycopyrrolate-butorphanol-xylazine com-bination with and without nasal administration of oxygen indogs. Am J Vet Res 55(6):835–841, 1994.
31. Hayashi Y, Sumikawa K, Maze M, et al: Dexmedetomidineprevents epinephrine-induced arrhythmias through stimula-tion of central α2 adrenoceptors in halothane-anesthetizeddogs. Anesthesiology 75(1):113–117, 1991.
32. Kamibayashi T, Hayashi Y, Sumikawa K, et al: A role of va-gus nerve in antiarrhythmic effects of doxazosin anddexmedetomidine on halothane-epinephrine arrhythmias.
Anesthesiology 77(3A):A642, 1992.33. Lemke KA, Tranquilli WJ, Thurmon JC, et al: Influence of
cholinergic blockade on the development of epinephrine-in-
Compendium January 2000 Small Animal/Exotics
duced ventricular arrhythmias in halothane and isofluraneanesthetized dogs. Vet Surg 23:61–66, 1994.
34. Muir WW, Hubbell JAE, Flaherty S: Increasing halothaneconcentration abolishes anesthesia-associated arrhythmias incats and dogs. JAVMA 192(12):1730–1736, 1988.
35. Bednarski RM, Muir WW: Ventricular arrhythmogenicdose of epinephrine in dogs and cats anesthetized with tile-
tamine/zolazepam and halothane. Am J Vet Res 51(9):1468–1470, 1990.36. Tilley LP: Analysis of P-QRS-T deflections, in Tilley LP
(ed): Essentials of Canine and Feline Electrocardiography Inter- pretation and Treatment . Philadelphia, Lea & Febiger, 1992,pp 59–123.
37. Tilley LP: Interpretation of complex arrhythmias, in Tilley LP (ed): Essentials of Canine and Feline Electrocardiography Interpretation and Treatment . Philidelphia, Lea & Febiger,1992, pp 385–416.
38. Goldman MJ: The pararrhythmias, in Goldman MJ (ed):Principles of Clinical Electrocardiology. Los Altos, CA, LangMedical Publications, 1986, pp 271–281.
39. Gaynor JS, Mason DE: ECG of the month. JAVMA 199(11):1574–1575, 1991.
40. Atlee JL, Brownlee SW, Burstrom RE: Conscious-state com-
parisons of the effects of inhalation anesthetics on specializedatrioventricular conduction times in dogs. Anesthesiology 64(6):703–710, 1986.
41. Breslow MJ, Evers AS, Lebowitz P: Successful treatment of accelerated junctional rhythm with propranolol: Possiblerole of sympathetic stimulation in the genesis of this rhythmdisturbance. Anesthesiology 62(2):180–182, 1985.
42. de Leon-Casasola OA, Lema MJ: Atrioventricular dissocia-tion resulting from combined thoracic epidural and generalanesthesia. Acta Anaesthesiol Scand 36:165–169, 1992.
43. DiBartola SP, Autran de Morais HS: Appendix, in DiBarto-la SP (ed): Fluid Therapy in Small Animal Practice. Philadel-phia, WB Saunders Co, 1992, pp 599–688.
44. Rardon DP, Fisch C: Electrolytes and the heart, in Hurst JW,Schlant RC, Rackley CE, et al (eds): The Heart Arteries and
Veins . New York, McGraw-Hill Inc, 1990, pp 1557– 1570.45. Goldman MJ: Miscellaneous abnormal electrocardiographic
patterns, in Goldman MJ (ed): Principles of Clinical Electro- cardiology . Los Altos, CA, Lang Medical Publications, 1986,pp 297–322.
46. Senior DF: Fluid therapy, electrolytes and acid base control,in Ettinger SJ (ed): Textbook of Veterinary Internal Medicine .Philadelphia, WB Saunders Co, 1989, pp 429–449.
About the AuthorsAt the time this article was submitted for publication, Dr.
Kushner was affiliated with the Animal Health Center,
Mississippi State University, Mississippi State, Mississip-
pi. Dr. Kushner is currently affiliated with the VeterinaryHospital of the University of Pennsylvania, Philadelphia,
Pennsylvania; she is a Diplomate of the American Col-
lege of Veterinary Anesthesiologists. Dr. Calvert is affiliat-
ed with the Department of Small Animal Medicine, Col-
lege of Veterinary Medicine, University of Georgia, Athens,
Georgia; he is a Diplomate of the American College of
Veterinary Internal Medicine.
Related Documents