Peri-operative management of diabetes mellitus Dr.Martin Whyte Consultant Diabetes & Endocrinology

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Peri-operative
management of
diabetes mellitus
Dr.Martin Whyte
Consultant Diabetes & Endocrinology
Peri-operative management of
diabetes mellitus
Why is peri-operative control important?
Metabolic response to surgery / infection risk
Evidence to support peri-operative glycaemic control
Pre-operative evaluation
Glycaemic target & choice of medication / regime
What to do on the day of surgery itself

Why is peri-operative glycaemic
control important?
2.5 million people with diabetes in UK
25% of diabetic patients will require
surgery at some point
12 to 25% of hospitalised patients have
DM

Hyperglycemia: an independent marker of
in-hospital mortality in patients with
undiagnosed diabetes
Umpierrez et al. JCEM 2002; 87; 978-982
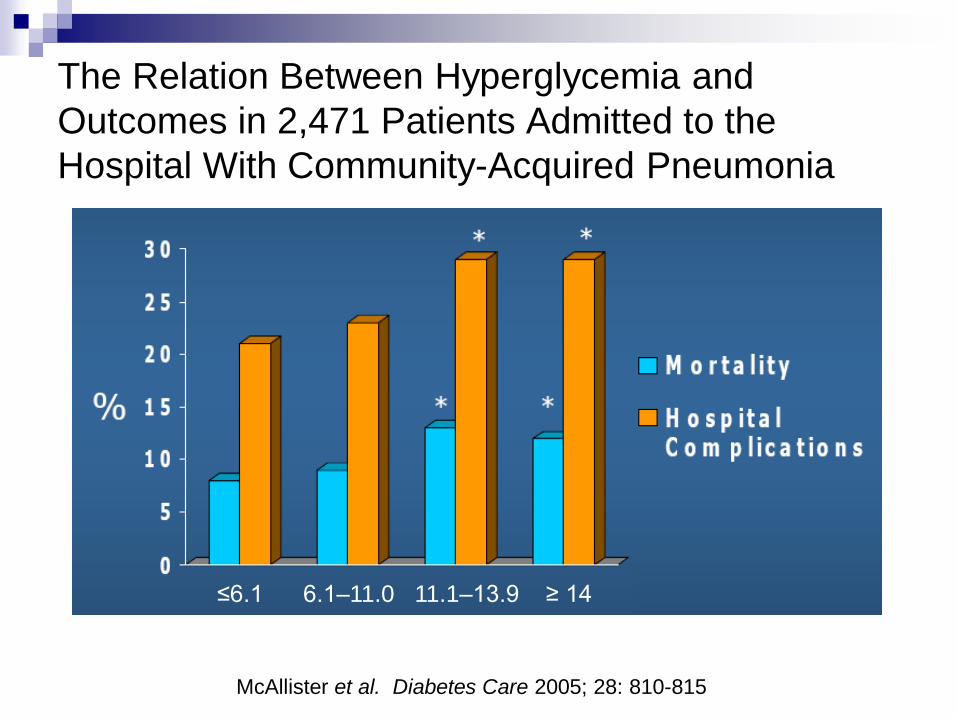
The Relation Between Hyperglycemia and
Outcomes in 2,471 Patients Admitted to the
Hospital With Community-Acquired Pneumonia
≤6.1 6.1–11.0 11.1–13.9 ≥ 14
McAllister et al. Diabetes Care 2005; 28: 810-815

Glycaemic control before surgery
Non-cardiac surgery 1991 – 2001
Candidate cases were 904 deaths
occuring within 30-days of surgery
1247 case controls matched to age,
gender, year of op, type of surgery
Comparison of pre-operative glucose
values
Noordzij et al. Eur J Endo 2007;156:137-142
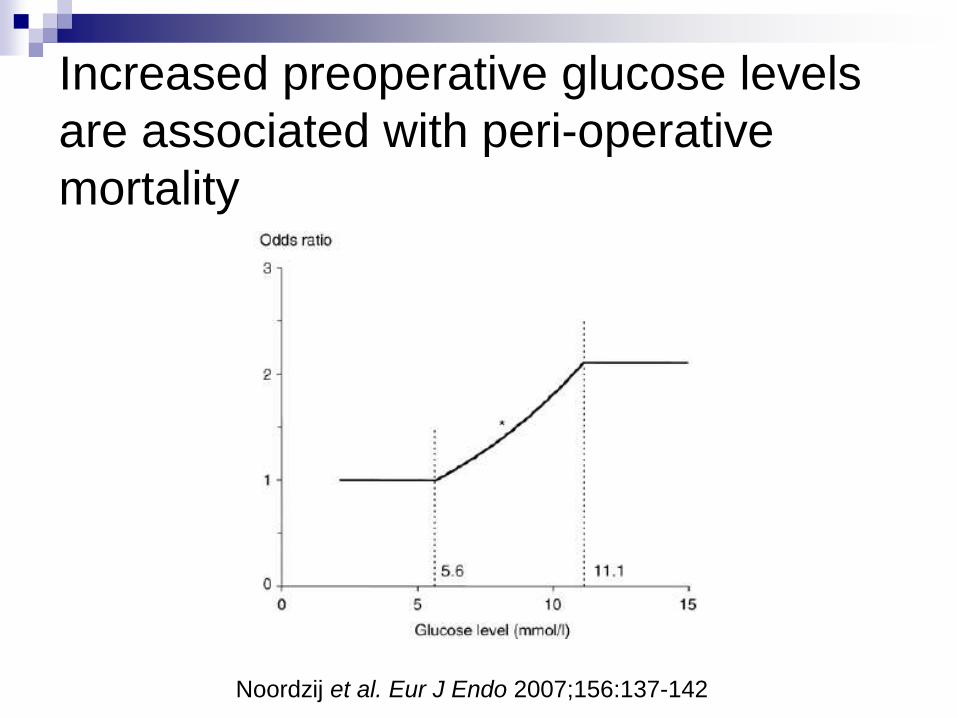
Increased preoperative glucose levels
are associated with peri-operative
mortality
Noordzij et al. Eur J Endo 2007;156:137-142
Peri-operative management of
diabetes mellitus
Why is peri-operative control important?
Metabolic response to surgery / infection risk
Evidence to support peri-operative glycaemic control
Pre-operative evaluation
Glycaemic target & choice of medication / regime
What to do on the day of surgery itself
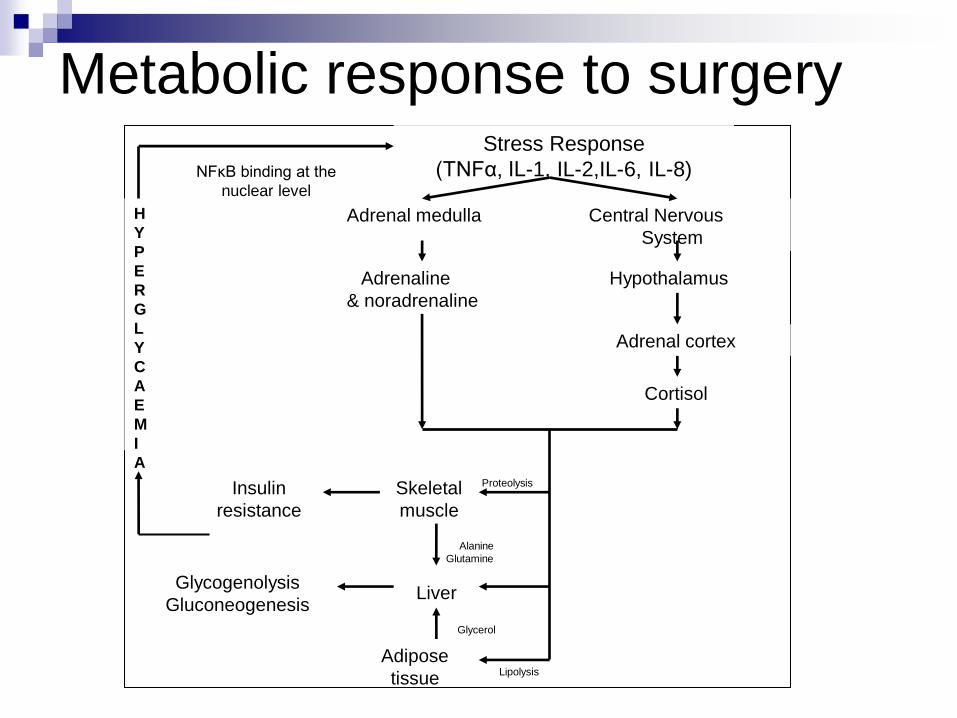
Metabolic response to surgery
Stress Response
(TNFα, IL-1, IL-2,IL-6, IL-8)
Adrenal medulla Central Nervous
System
Adrenaline Hypothalamus
& noradrenaline
Adrenal cortex
Cortisol
Liver
Skeletal
muscle
Adipose
tissue
Glycogenolysis
Gluconeogenesis
Insulin
resistance
NFκB binding at the
nuclear level
H
Y
P
E
R
G
L
Y
C
A
E
M
I
A
Lipolysis
Proteolysis
Glycerol
Alanine
Glutamine

BS > 11.1 mmol/L
Renal threshold for glycosuria (normal GFR)
Impaired WBC function
Chemotaxsis
Phagocytosis
Impaired wound healing

Peri-operative management of
diabetes mellitus
Why is peri-operative control important?
Metabolic response to surgery / infection risk
Evidence to support peri-operative glycaemic control
Pre-operative evaluation
Glycaemic target & choice of medication / regime
What to do on the day of surgery itself
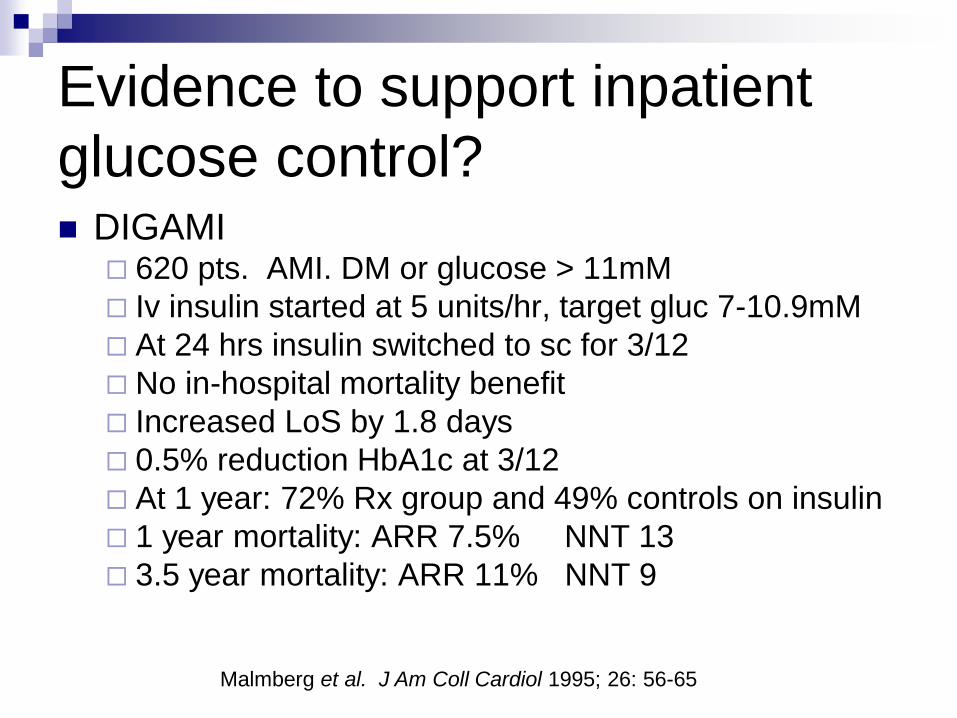
DIGAMI 620 pts. AMI. DM or glucose > 11mM
Iv insulin started at 5 units/hr, target gluc 7-10.9mM
At 24 hrs insulin switched to sc for 3/12
No in-hospital mortality benefit
Increased LoS by 1.8 days
0.5% reduction HbA1c at 3/12
At 1 year: 72% Rx group and 49% controls on insulin
1 year mortality: ARR 7.5% NNT 13
3.5 year mortality: ARR 11% NNT 9
Evidence to support inpatient
glucose control?
Malmberg et al. J Am Coll Cardiol 1995; 26: 56-65

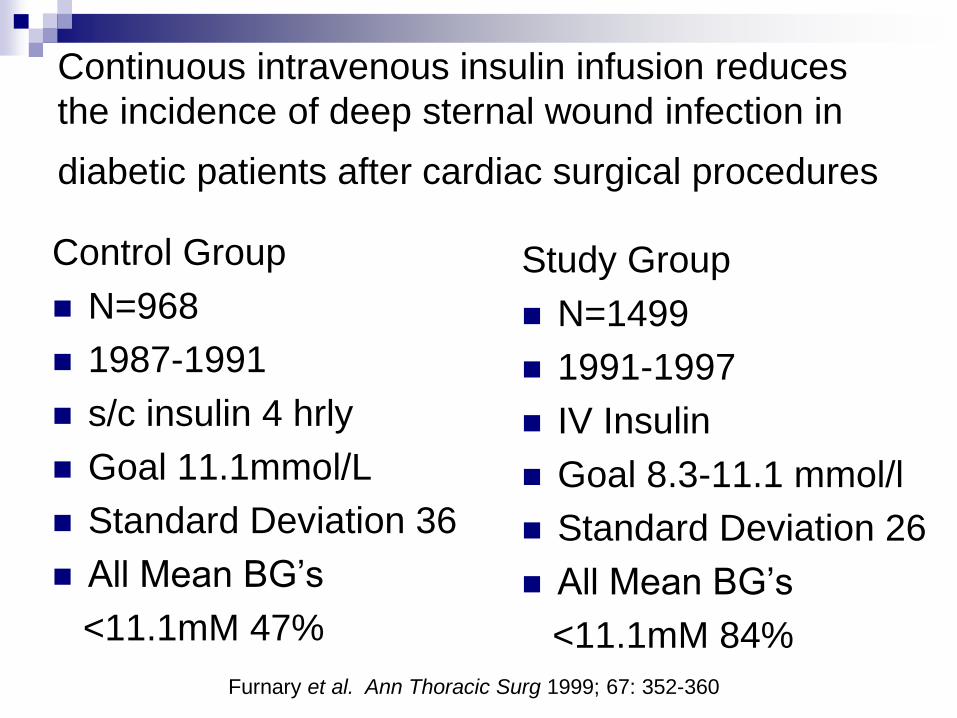
Control Group
N=968
1987-1991
s/c insulin 4 hrly
Goal 11.1mmol/L
Standard Deviation 36
All Mean BG‟s
<11.1mM 47%
Study Group
N=1499
1991-1997
IV Insulin
Goal 8.3-11.1 mmol/l
Standard Deviation 26
All Mean BG‟s
<11.1mM 84%
Continuous intravenous insulin infusion reduces
the incidence of deep sternal wound infection in
diabetic patients after cardiac surgical procedures
Furnary et al. Ann Thoracic Surg 1999; 67: 352-360

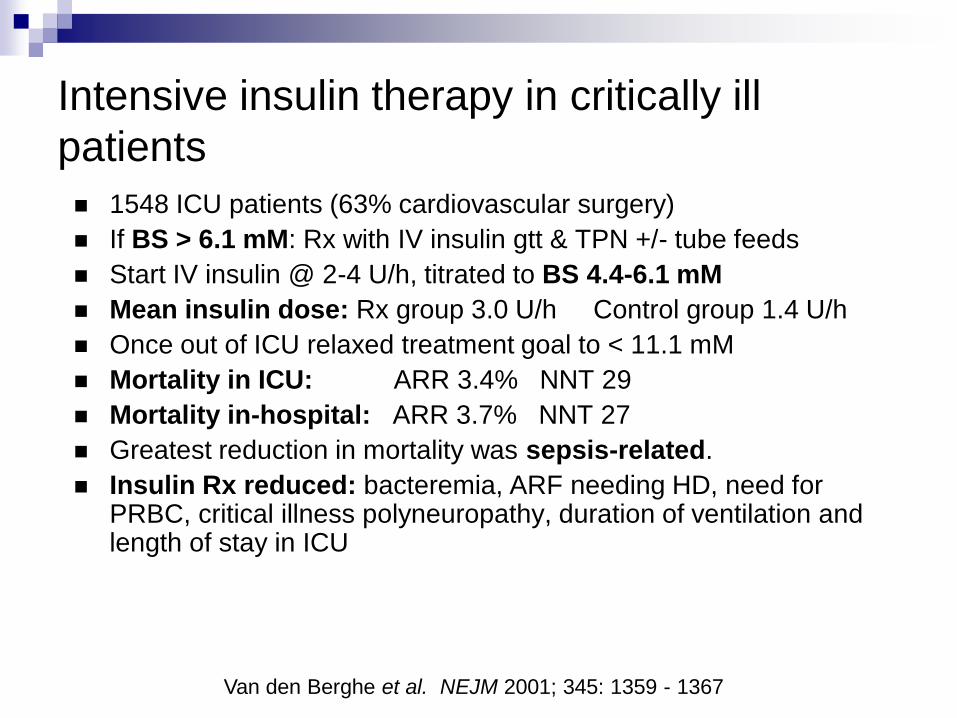
1548 ICU patients (63% cardiovascular surgery)
If BS > 6.1 mM: Rx with IV insulin gtt & TPN +/- tube feeds
Start IV insulin @ 2-4 U/h, titrated to BS 4.4-6.1 mM
Mean insulin dose: Rx group 3.0 U/h Control group 1.4 U/h
Once out of ICU relaxed treatment goal to < 11.1 mM
Mortality in ICU: ARR 3.4% NNT 29
Mortality in-hospital: ARR 3.7% NNT 27
Greatest reduction in mortality was sepsis-related.
Insulin Rx reduced: bacteremia, ARF needing HD, need for PRBC, critical illness polyneuropathy, duration of ventilation and length of stay in ICU
Intensive insulin therapy in critically ill
patients
Van den Berghe et al. NEJM 2001; 345: 1359 - 1367
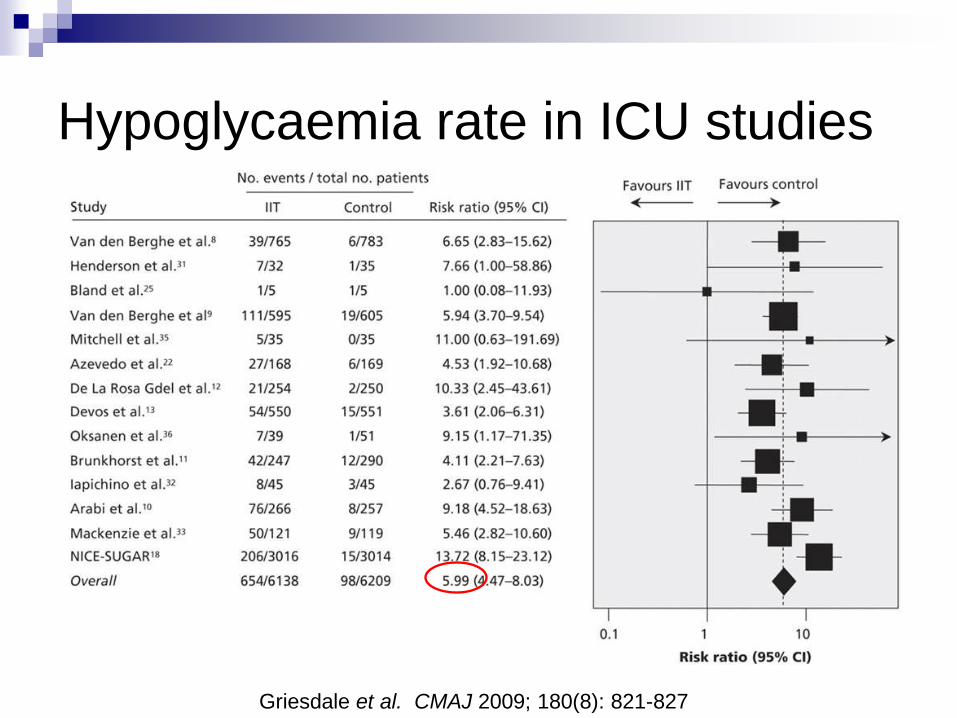
Hypoglycaemia rate in ICU studies
Griesdale et al. CMAJ 2009; 180(8): 821-827

Griesdale et al. CMAJ 2009; 180(8): 821-827
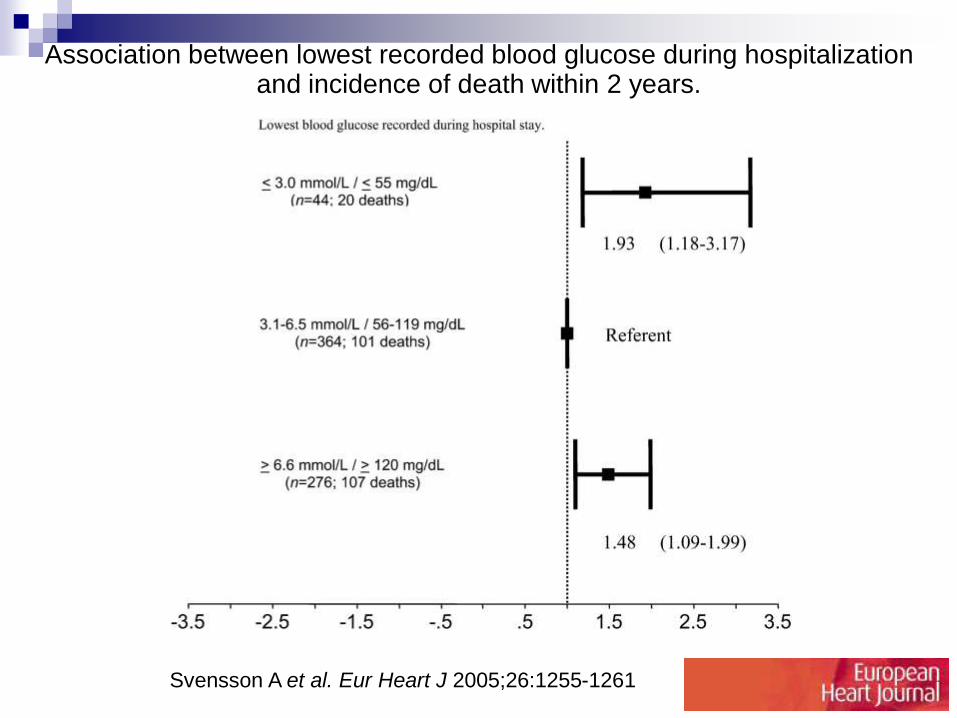
Association between lowest recorded blood glucose during hospitalization and incidence of death within 2 years.
Svensson A et al. Eur Heart J 2005;26:1255-1261
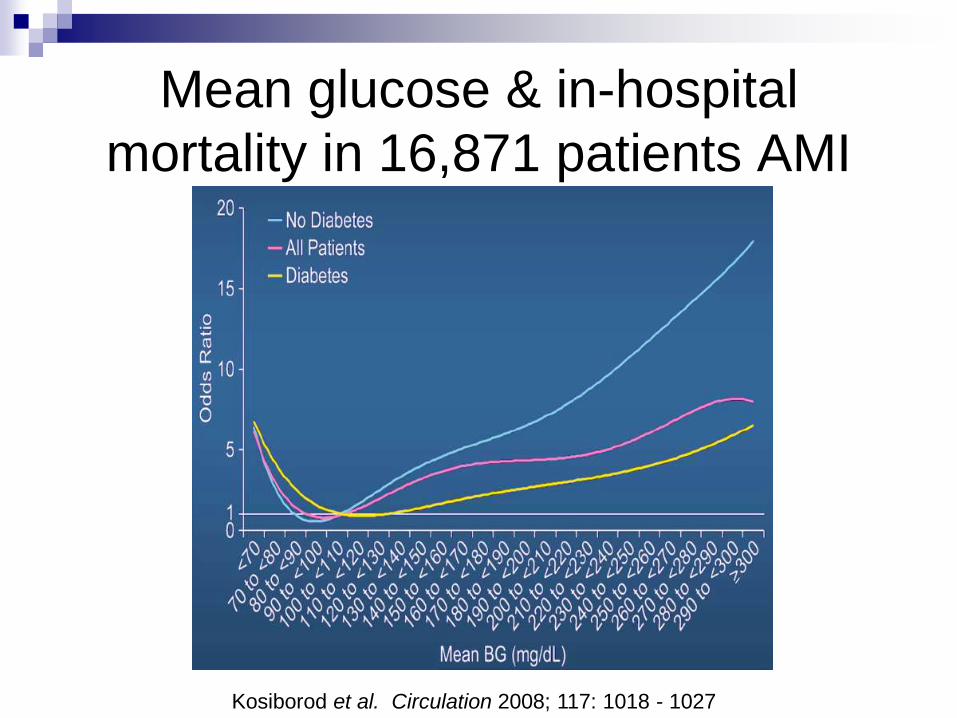
Mean glucose & in-hospital
mortality in 16,871 patients AMI
Kosiborod et al. Circulation 2008; 117: 1018 - 1027

Peri-operative management of
diabetes mellitus
Why is peri-operative control important?
Metabolic response to surgery / infection risk
Evidence to support peri-operative glycaemic control
Pre-operative evaluation
Glycaemic target & choice of medication / regime
What to do on the day of surgery itself

Pre-operative evaluation
Cardiopulmonary risk
Greater risk of CAD and silent ischaemia
Long-term complications of DM
Baseline glycaemic control – HbA1c
If >9% liase with diabetes team
If >12% consider delaying surgery to achieve better control
Medication
Type of surgery


Peri-operative Beta-blockade Diabetic Postoperative Mortality and Morbidity
(DIPOM) trial Diabetics >39 years old.
Non-cardiac surgery.
Naive to beta-blockers
Metoprolol started the night before surgery (100mg) and continued for ~ five days
Outcomes: all-cause mortality, acute MI, USAP, and CHF, measured for a median of 18 months
2066 patients were eligible. Only 921 were randomized (45% of eligible patients)
99 events Metoprolol group vs 93 placebo
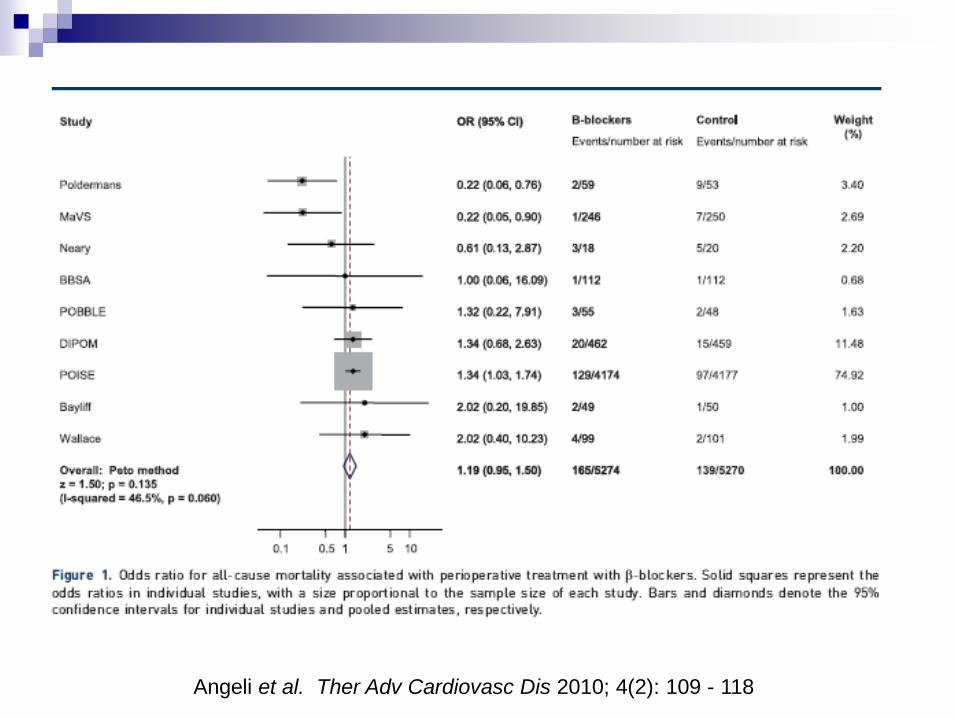
Angeli et al. Ther Adv Cardiovasc Dis 2010; 4(2): 109 - 118

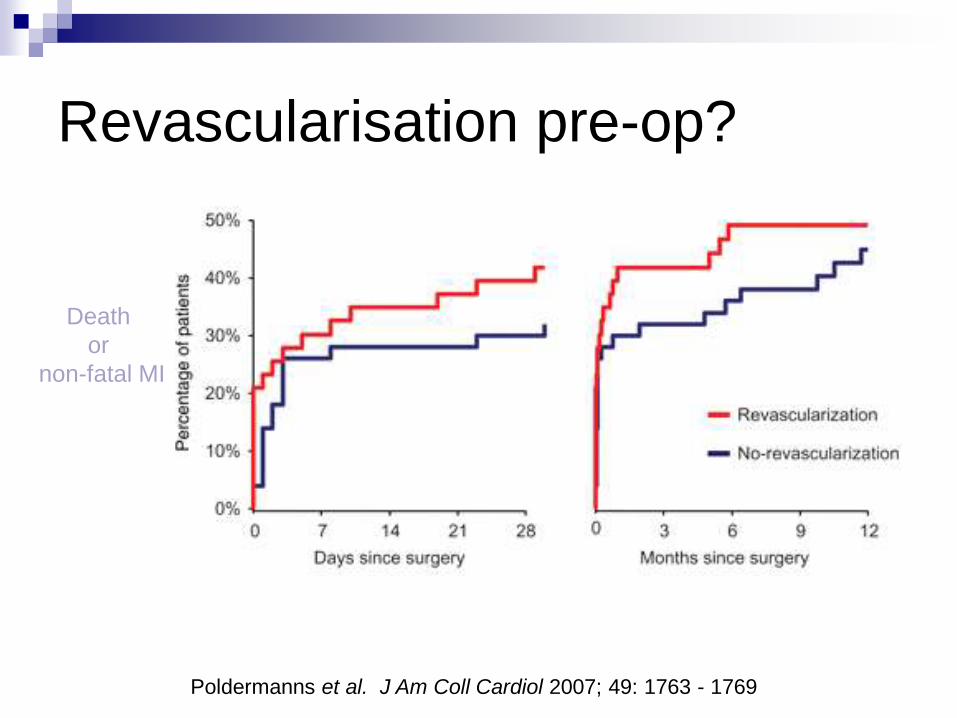
Revascularisation pre-op?
Death
or
non-fatal MI
Poldermanns et al. J Am Coll Cardiol 2007; 49: 1763 - 1769

Peri-operative management of
diabetes mellitus
Why is peri-operative control important?
Metabolic response to surgery / infection risk
Evidence to support peri-operative glycaemic control
Pre-operative evaluation
Glycaemic target & choice of medication / regime
What to do on the day of surgery itself

Start oral medication?
No
Contraindications or SEs of oral meds
Little flexibility or opportunity for titration in a setting where acute changes demand these characteristics.
Therefore use insulin

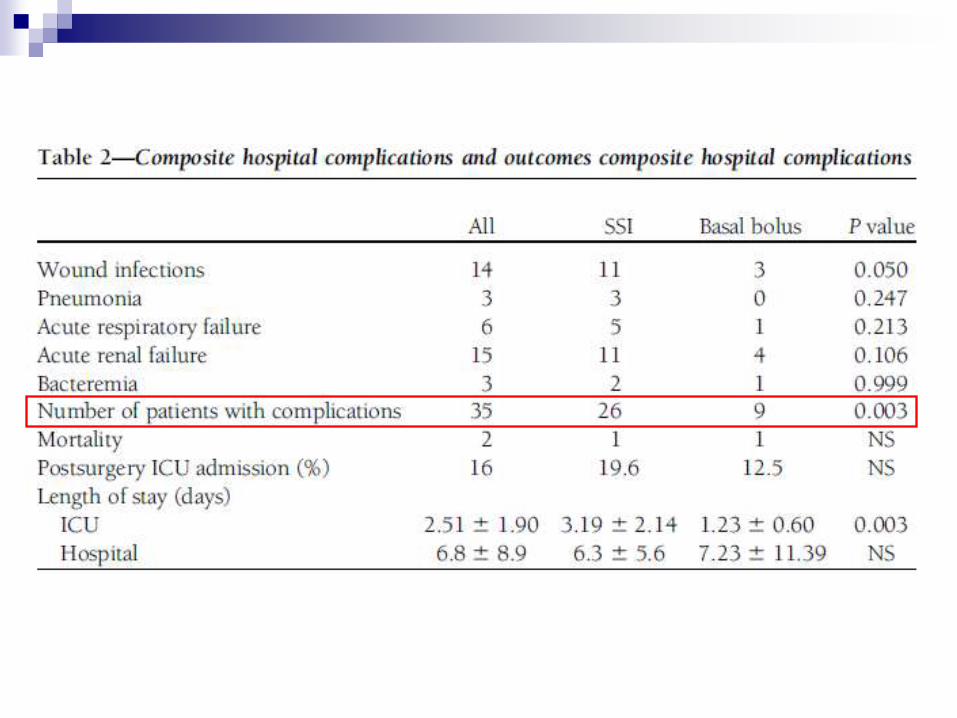
Randomised study of Basal Bolus insulin therapy
in the Inpatient Management of Patients with Type
2 Diabetes undergoing General Surgery
(RABBIT2)
Patients with DM for ≥3/12. Admission glucose 140-400mg/dL. Insulin ≤0.4U/kg
Elective or emergency surgery. Not expected to need ICU
Glargine + glulisine (n=104) vs PRN Actrapid (n=107; QDS max)
Target fasting 100-140mg/dL
OHAs discontinued. Basal bolus 0.5U/kg (50% as basal, 50% as bolus)
Outcomes: daily blood glucose (BG); wound infection, pneumonia, bacteraemia, and respiratory and acute renal failure.
On admission 17.1% diet, 63% oral, 9.5% oral + insulin, 10.4% insulin alone
HbA1c 7.72 ± 2.2%
Umpierrez et al. Diabetes Care 2011; 34(2): 256-261

PRN Actrapid
Basal bolus

<3.8mmol/L
<2.2mmol/L
<3.3mmol/L

Comparison of in-patient regimens with
Detemir plus Aspart versus NPH plus
regular in Medical Patients with Type 2
diabetes multicentre trial
130 nonsurgical patients BG 7.8 to 22.2 mmol/L to detemir OD plus aspart before meals (n = 67)
neutral protamine Hagedorn (NPH) and regular insulin twice daily (n = 63).
Insulin dose started at 0.4 U/kg/d for BG between 7.8 and 11.1 mmol/L or 0.5 U/kg/d for BG 11.1-22.2 mmol/L.
Study outcomes: differences in mean daily BG levels
frequency of hypoglycemic events
Umpierrez et al. JCEM 2009; 94: 564 - 569
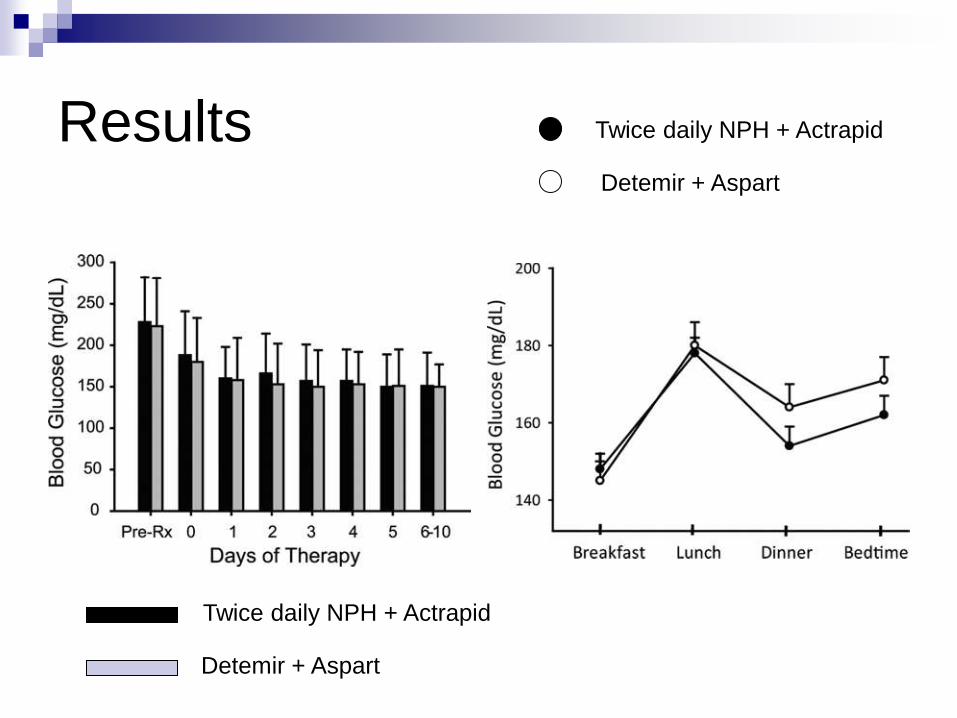
Results Twice daily NPH + Actrapid
Detemir + Aspart
Detemir + Aspart
Twice daily NPH + Actrapid

Starting Insulin Regimen
TDD = 0.3-0.5 U/kg
“2/3, 1/3” Regimens 2/3 of TDD before Breakfast, 1/3 before Dinner
Pre-mix (30/70)
MDI Regimens basal 50%, bolus 50% (divided by 3)

How to calculate correctional doses
Correction dose to lower blood glucose = 100/TDD
If taking 20 units per day then 100/20 = 5mM
Hence 1 unit will lower by 5mmol/L.
If taking 50 units per day then 100/50 = 2mM
Hence 1 unit will lower by 2mmol/L

Guideline for Insulin Adjustments
1. Adjust the insulin that accounts for the high or low
reading.
2. Always compare an abnormal BS reading with the one
previous.
3. If insulin dose is:
• Less than 8U, adjust by 1U
• 8-20U, adjust by 2U
• > 20 U, adjust by 10% (increase), 20% (decrease)
4. Don‟t forget to compensate for a successful
adjustment

Consensus Recommendations for Target
Inpatient Blood Glucose Concentrations
Patient population Blood glucose target Rationale
General medical /
surgical*
Fasting 5 - 7
Random < 11.1 (?<10)
↓ mortality, LoS,
↓ infection rates
Cardiac surgery* < 8.3 ↓mortality
↓Sternal wound infection
Critically ill† < 8.3 ↓mortality, morbidity, LoS
Acute neurologic
disorders ‡
4.4 – 7.8 No data!!
*ADA
† Society of Critical Care Medicine
‡ American Heart Association / American Stroke Association

Peri-operative management of
diabetes mellitus
Why is peri-operative control important?
Metabolic response to surgery / infection risk
Evidence to support peri-operative glycaemic control
Pre-operative evaluation
Glycaemic target & choice of medication / regime
What to do on the day of surgery itself

Non-insulin antidiabetic medications
Short acting eg glicazide, replaginide Omit on day of surgery
Long acting eg glicazide MR, glipizide Omit on day prior to surgery
Thiazolidinediones eg rosiglitazone, pioglitazone Omit on day of surgery
Metformin Stop 48 hours before surgery
Acarbose Omit day of surgery
Gliptins eg sitagliptin Omit day of surgery
Incretin mimetics eg exenatide Omit on day of surgery

Metformin
Contraindications eGFR < 30mls/min
CHF symptomatic (> NYHA class III, E.F. < 35-40%)
Liver failure
Alcoholism
Hypoxic respiratory condition
Active moderate to severe infection
Radio-contrast or Surgery with GA
Hold metformin for 24 - 48h
Restart after documented preservation of renal
function

Pre-operative insulin administration
Type of insulin Morning list Afternoon list
Twice daily Mix
eg Novomix
Omit morning
S/scale 0800
50% in morning
S/scale 1200
Twice daily intermed.
acting eg insulatard
Omit morning
S/scale 0800
50% in morning
S/scale at 1200
Once day long acting
in morning eg
glargine
75% day prior
Omit morning
S/scale 0800
Omit morning
S/scale at 1200
Once a day long
acting in evening
75% day prior
S/scale 0800
75% day prior
S/scale 1200
Short acting eg
Novorapid, Actrapid
Omit morning 75% morning
Omit lunch

Management of patients on insulin
(Type 1 and Type 2)
For morning surgery Ensure that no sc rapid acting or pre-mixed insulin given on the day
of surgery The last dose of either type of insulin should be on the previous evening
Check the blood glucose
Commence sliding scale
Continue to check the blood glucose hourly pre, intra and post-operatively
Post-operatively Change to sc insulin post-operatively when eating normally
Important to continue sliding scale for 60 mins after first sc insulin injection
Day-case surgery Aim for “first on list”
For those on multiple injection regimen, continue usual basal (long acting) insulin on evening prior to procedure
For patients on bd insulin, continue the usual evening insulin prior to the procedure
Fast from midnight and omit the morning insulin
Check BM before and after the procedure
Resume the usual insulin and diet after the procedure. If a BD insulin regimen is restarted at lunchtime give half of normal „breakfast‟
insulin dose with lunch after procedure
The above applies if rapid recovery is expected i.e. the patient is expected to be eating within 2 hours of the procedure
If the patient is unable to tolerate diet or the blood glucose is >14 mmol/L, then a sliding scale may be required
Take-home messages - 1
Hyperglycaemia is frequent in hospitalised
patients with and without a history of diabetes
Hyperglycaemia (?hypoglycaemia) is a marker
of poor outcome in critically and non-critically ill
patients
Improvement in clinical outcome has been
shown by improved glycaemic control in a
variety of inpatient settings.
Patients with T1DM & insulin-treated T2DM should continue usual therapy.
Avoid using purely PRN Actrapid
No data to support benefit of insulin analogues (esp basal) in hospital.
Take-home messages - 2

Related Documents











