8 JACC Vol. 9, No. I January 1987:8-17 Percutaneous Transluminal Angioplasty of Stenotic Coronary Artery Bypass Grafts: 5 Years' Experience GILLES COTE, MD, FRCP, RICHARD K. MYLER, MD, FACC, SIMON H. STERTZER, MD, FACC, DAVID A. CLARK, MD, FACC, JODI FISHMAN-ROSEN, RN, MS, MARY MURPHY, RN, MS, RICHARD E. SHAW, PHD. Daly City. California In a 60 month period (January 1981 to December 1985), 82 patients (79% male with a mean age of 60 years) had 83 saphenous vein grafts and 5 internal mammary artery grafts with a total of 101 stenotic sites treated with per- cutaneous transluminal coronary angioplasty. The mean time between bypass surgery and angioplasty was 51.2 months. The procedure was technically successful in 85% of patients, 86% of grafts and 85% of the sites at- tempted. In these cases, the mean diameter stenosis was reduced from 77 ± 14 to 27 ± 20% (p < 0.001), the mean pressure gradient from 49 ± 16 to 7 ± 6 mm Hg (p < 0.001). Emergency coronary artery bypass graft surgery was necessary in one patient (1.2%) whereas myocardial infarction occurred in three patients (3.6%). There were no hospital deaths. Clinical follow-up was obtained in all 82 patients. Before angioplasty, 23% were in Canadian Cardiovas- cular Society functional class II, 60% in class III and 17% in class IV. With a mean clinical follow-up period of 21.4 ± 2.3 months, 71% are in class I, 17% in class Since the introduction of direct internal mammary-coronary artery anastomosis by Kolessov (I) in 1967 and use of saphenous vein-coronary artery grafts by Favaloro (2) in 1968, these conduits have been widely utilized in the treat- ment of ischemic heart disease. Long-term follow-up of patients with saphenous vein grafts has revealed a high incidence of recurrence. Angiographic studies (3-7) have shown occlusive disease at the anastomotic site or in the graft itself in over one-third of patients in the 10 years after From the San Francisco Heart Institute, Seton Medical Center, Daly City, California. Manuscript received April 21, 1986; revised manuscript received July 29, 1986, accepted August 20, 1986. Address for reprints: Richard K. Myler, MD, San Francisco Heart Institute, Seton Medical Center. 1900 Sullivan Avenue. Daly City, Cali- fornia 94015. © 1987 by the American College of Cardiology II and 12% in class III. There were two deaths, 3 months or more after angioplasty, one probably due to graft closure. So far, angiographic follow-up (at 7.9 ± 2.1 months) has been available in 26 patients. Ten patients (with 10 grafts) exhibited graft restenosis; six of them have had second successful repeat angioplasty. Among the many variables analyzed, statistically significant pre- dictors of success were a higher measured balloon/graft ratio (p < 0.001), smaller diameter graft (p < 0.001), and shorter lesion length (p < 0.01). The only predictor of complication was diffuseness of disease in the graft (p < 0.05). The statistically significant predictors of re- currence were the residual stenosis after the initial an- gioplasty (p < 0.01) and the measured balloon/graft ratio (p < 0.01). Angioplasty of coronary artery grafts appears to be a feasible and efficacious procedure with a low compli- cation rate. The technique is a satisfactory alternative to repeat surgery in selected patients. (J Am Coil Cardiol1987;9:8-17) surgery. In the nearly 2 decades since coronary bypass sur- gery has been in clinical use, more patients are now being reevaluated for symptomatic ischemic heart disease after revascularization surgery. Until recently, the approach to the treatment of this subset of patients has been either med- ical therapy or a repeat surgical revascularization procedure, the latter in patients in whom adequate symptomatic control could not be achieved. However, performing a second (or third) operation is not without serious implications. Being technically more difficult, the revascularization is frequently incomplete, and there are higher morbidity and mortality rates (8-12). Gruentzig et al. (13-16) and Stertzer et al. (17) were the first to report the use of an angioplasty balloon catheter in the treatment of coronary atherosclerotic disease in humans. Since 1977, because of significant technological improve- ment and greater experience, the original indications have 0735-1095/87/$3.50

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

8 JACC Vol. 9, No. IJanuary 1987:8-17
Percutaneous Transluminal Angioplasty of Stenotic Coronary ArteryBypass Grafts: 5 Years' Experience
GILLES COTE, MD, FRCP, RICHARD K. MYLER, MD, FACC, SIMON H. STERTZER, MD, FACC,
DAVID A. CLARK, MD, FACC, JODI FISHMAN-ROSEN, RN, MS, MARY MURPHY, RN, MS,
RICHARD E. SHAW, PHD.
Daly City. California
In a 60 month period (January 1981 to December 1985),82 patients (79% male with a mean age of 60 years) had83 saphenous vein grafts and 5 internal mammary arterygrafts with a total of 101 stenotic sites treated with percutaneous transluminal coronary angioplasty. The meantime between bypass surgery and angioplasty was 51.2months. The procedure was technically successful in 85%of patients, 86% of grafts and 85% of the sites attempted. In these cases, the mean diameter stenosis wasreduced from 77 ± 14 to 27 ± 20% (p < 0.001), themean pressure gradient from 49 ± 16 to 7 ± 6 mm Hg(p < 0.001). Emergency coronary artery bypass graftsurgery was necessary in one patient (1.2%) whereasmyocardial infarction occurred in three patients (3.6%).There were no hospital deaths.
Clinical follow-up was obtained in all 82 patients.Before angioplasty, 23% were in Canadian Cardiovascular Society functional class II, 60% in class III and17% in class IV. With a mean clinical follow-up periodof 21.4 ± 2.3 months, 71% are in class I, 17% in class
Since the introduction of direct internal mammary-coronaryartery anastomosis by Kolessov (I) in 1967 and use ofsaphenous vein-coronary artery grafts by Favaloro (2) in1968, these conduits have been widely utilized in the treatment of ischemic heart disease. Long-term follow-up ofpatients with saphenous vein grafts has revealed a highincidence of recurrence. Angiographic studies (3-7) haveshown occlusive disease at the anastomotic site or in thegraft itself in over one-third of patients in the 10 years after
From the San Francisco Heart Institute, Seton Medical Center, DalyCity, California.
Manuscript received April 21, 1986; revised manuscript received July29, 1986, accepted August 20, 1986.
Address for reprints: Richard K. Myler, MD, San Francisco HeartInstitute, Seton Medical Center. 1900 Sullivan Avenue. Daly City, California 94015.
© 1987 by the American College of Cardiology
II and 12% in class III. There were two deaths, 3 monthsor more after angioplasty, one probably due to graftclosure. So far, angiographic follow-up (at 7.9 ± 2.1months) has been available in 26 patients. Ten patients(with 10 grafts) exhibited graft restenosis; six of themhave had second successful repeat angioplasty. Amongthe many variables analyzed, statistically significant predictors of success were a higher measured balloon/graftratio (p < 0.001), smaller diameter graft (p < 0.001),and shorter lesion length (p < 0.01). The only predictorof complication was diffuseness of disease in the graft(p < 0.05). The statistically significant predictors of recurrence were the residual stenosis after the initial angioplasty (p < 0.01) and the measured balloon/graft ratio(p < 0.01).
Angioplasty of coronary artery grafts appears to bea feasible and efficacious procedure with a low complication rate. The technique is a satisfactory alternativeto repeat surgery in selected patients.
(J Am Coil Cardiol1987;9:8-17)
surgery. In the nearly 2 decades since coronary bypass surgery has been in clinical use, more patients are now beingreevaluated for symptomatic ischemic heart disease afterrevascularization surgery. Until recently, the approach tothe treatment of this subset of patients has been either medical therapy or a repeat surgical revascularization procedure,the latter in patients in whom adequate symptomatic controlcould not be achieved. However, performing a second (orthird) operation is not without serious implications. Beingtechnically more difficult, the revascularization is frequentlyincomplete, and there are higher morbidity and mortalityrates (8-12).
Gruentzig et al. (13-16) and Stertzer et al. (17) were thefirst to report the use of an angioplasty balloon catheter inthe treatment of coronary atherosclerotic disease in humans.Since 1977, because of significant technological improvement and greater experience, the original indications have
0735-1095/87/$3.50

JACC Vol. 9, No. IJanuary 1987:8-17
COTE ET AL.ANGIOPLASTY OF CORONARY ARTERY BYPASS GRAFTS
9
widened considerably (18 ,19) , The use of this procedurehas become safer as well as more successful.
This report summarizes our experience using angioplastyas the revascularization technique for stenotic saphenousvein and internal mammary grafts in patients with anginarelatively refractory to medical management.
MethodsData acquisition. All cases of percutaneous translu
minal angioplasty of saphenous vein and internal mammaryartery bypass grafts performed at the San Francisco HeartInstitute between January 1981 and December 1985 inclusive (60 months) were retrospectively reviewed, The clinicalinformation was obtained by consulting the medical recordfiles as well as by contacting the patients or their referringphysicians, or both. The details of each procedure werecollected by review of the catheterization laboratory protocols . Angiographic data were obtained from the coronaryarteriograms before and after dilation, and at follow-up whenavailable ,
Two ratios were generated from the angiographic data.The " measured balloon/graft" ratio was defined as the measurement of the inflated balloon diameter at maximal inflation pressure (at the site of the lesion). The largest measurement in the various projections was used. A secondratio, which will be called "expected balloon/graft" ratio ,was derived from the commercially listed balloon size andthe measured graft diameter.
All of the dilation catheters used in this study were fromUSCI (United States Catheter and Instrument Co., Inc.) .The balloons in all cases but one were of polyvinyl chloride,a product with known compliance characteristics at variousinflation pressures (that is, balloon diameters are larger athigher inflation pressures) (20,21), Measurements were performed using electronic calipers and a computer-assistedsystem (A2D Protocol 110 I, Programmable Digital Caliper,Hewlett-Packard, Inc.) , calibrating to zero and to the diameter of the angioplasty guiding catheter (8F == 2 .67 mm) .Pre- and postangioplasty percent diameter stenosis and lesion length were measured in three angiographic views, thecomputer calculating the mean of these results.
The graf ts were divided into five anatomical sites: theproximal anastomosis (Fig. I), the proximal, mid and distalthird of the graft shaft and the distal anastomosis (Fig. 2and 3) . The distribution of the lesions at these various sitesis displayed in Table I .
Clinical patient profiles. Bypass graft angioplasty wasattempted in 82 patients. 65 male and 17 female , with anage range of 38 to 78 years (mean 59.7) . A total of 83saphenous vein grafts and 5 internal mammary artery graftswith 10I stenotic sites were dilated . Sixty-eight patientsunderwent angioplasty at one site, nine at two sites and fiveat three sites. The right coronary artery was the insertion
site for 18 of the "target" saphenous vein grafts, the leftcircumflex for 21 saphenous vein graft s and the left anteriordescending artery for 49 grafts (42 saphenous vein, 5 internal mammary artery and 2 Sewell graft s). All the patientshad disabling angina relatively refractory to medical therapyand an abnormal treadmill stress test if they were able toexercise. Symptomatic status was classified according to theCanadian Cardiovascular Society Functional Classificationcriteria (22) ; 23% were in class II, 60% in class III and 17%in class IV before angioplasty . Insulin-dependent diabetesmellitus was found in 21% of patients, elevated serum triglycerides in 35% and elevated serum cholesterol in 22%.Sixty-five percent of patients were smokers at the time ofangioplasty. The mean period since bypass surgery was51. 2 ± 40 months (range 2 to 144); of the 82 patients. 50(61%) had had their bypass surgery 12 months or morebefore coronary angioplasty , The mean duration of symptoms at the time of the procedure was 6 .7 ± 9 months(range I to 60) .
All patients were maintained on their original medicaltherapy until the angioplasty . Twelve to 24 hours before theprocedure. they were started On a regimen of aspirin (325mg daily) and dipyridamole (50 to 75 mg orally) three timesa day. All patients were given a premedication regimenincluding secobarbital sodium and a calcium channel blocker(usually nifedipine, 10 mg orally). A bolus of 10,000 unitsof heparin was administered after the cannulation of theentrance artery (femoral or brachial) and supplemented asneeded based on the duration of the angioplasty .
AngiopIasty technique. All the angioplasty procedureswere performed by one of three experienced physicians utilizing the femoral (52 grafts) or brachial (32 grafts) techniques, or both (4 grafts), as described elsewhere (19,23) .Various femoral guiding catheters were used to achieve themost stable position in the orifice of the graft (19). Themost commonly used femoral guiding catheters were a rightJudkins or left venous bypass style for saphenous vein-leftanterior descending and saphenous vein-left circumflex grafts,and a right venous bypass. multipurpose (King) , Stertzerfemoral or Arani style for the saphenous vein-right coronaryartery graft. Guiding catheter selection was determined bythe configuration and orientation of the saphenous vein graftand the diameter of the ascending aorta (19). All five internalmammary artery graft lesions involved the distal anastomosis of the left internal mammary and the left anteriordescending artery. Four of these procedures were performedusing an internal mammary artery guiding catheter from thefemoral approach and one by way of the left brachial arteryemploying a Stertzer brachial guiding catheter.
The size of the balloon catheter was selected to matchas closely as possible the diameter of the saphenous veingraft or the internal mammary artery graft when dilating theproximal anastomosis and graft shaft lesions. The diameterof the native vessel was the determinant of balloon size for
10 COTE ET AL.ANGIOPLASTY OF CORONARY ARTERY BYPASS GRAFTS
JACC Vol. 9, No.1January 1987:8-17
c
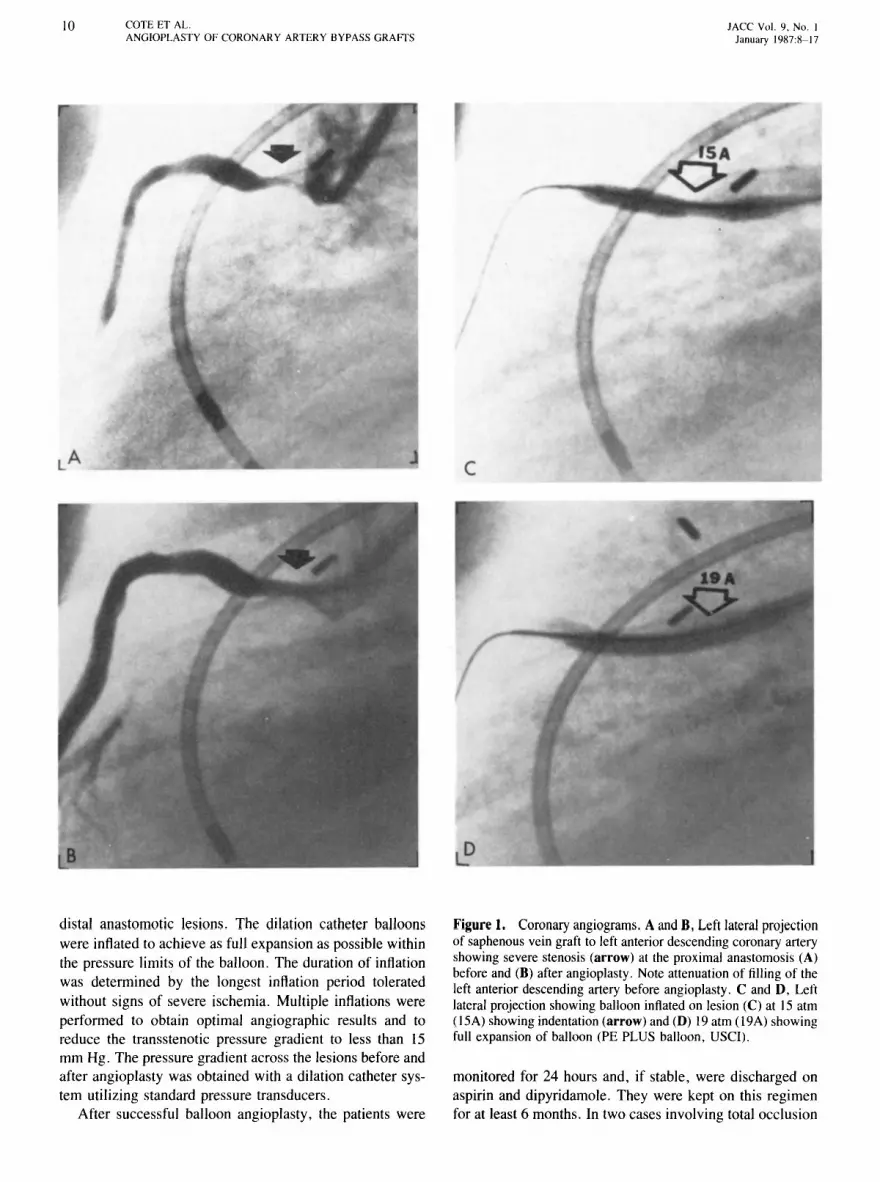
distal anastomotic lesions. The dilation catheter balloonswere inflated to achieve as full expansion as possible withinthe pressure limits of the balloon. The duration of inflationwas determined by the longest inflation period toleratedwithout signs of severe ischemia. Multiple inflations wereperformed to obtain optimal angiographic results and toreduce the transstenotic pressure gradient to less than 15mm Hg. The pressure gradient across the lesions before andafter angioplasty was obtained with a dilation catheter system utilizing standard pressure transducers.
After successful balloon angioplasty, the patients were
Figure1. Coronary angiograms. A and B, Left lateral projectionof saphenous vein graft to left anterior descending coronary arteryshowing severe stenosis (arrow) at the proximal anastomosis (A)before and (B) after angioplasty. Note attenuation of filling of theleft anterior descending artery before angioplasty. C and D, Leftlateral projection showing balloon inflated on lesion (C) at 15 atm(15A) showing indentation (arrow) and (D) 19 atm (l9A) showingfull expansion of balloon (PE PLUS balloon, USCI).
monitored for 24 hours and, if stable, were discharged onaspirin and dipyridamole. They were kept on this regimenfor at least 6 months. In two cases involving total occlusion

JACC Vol. 9. No. IJanuary 191\7:1\- 17
COTE ET AL.ANGIOPI.ASTY 0 1' CORONARY ARTERY BYPASS GRAfTS
II
I
I
Technical aspects. The mean maximal inflation pressurewas 9.5 :±: 2.2 atmospheres (range 5 to 19) with a meanmaximal inflation time of 52 :±: 18 seconds (range 25 to
Figure 3 . Coronary angiograms. Left lateral projection of internal mamm ary artery graft to the left anteri or descending arterywith severe stenos is (ar row) at distal anastomosis (A) before and(B) after angioplasty.
...
a
A
Figure 2. Coronary angiograms . Left anteri or oblique projectionof sequential saphenous vein graft to diagonal and left anteriordescending arteries showing mid-graft stenosi s (closed arrow) anda second stenosis (open arrow) at the distal anastomotic site (A)before and (B) after angioplasty . Note attenuation of flow into theleft anteri or descending artery before angioplasty.
of the saphenous vein graft, the patient s were dischargedon warfarin instead of aspirin . In addition , nitrates (oral ortopical) and a calcium channel blocker (nifedipine, 10 mgfour times a day) were used for at least 3 months afterangioplasty . Clinical follow-up was obtained in all the cases.
12 COTE ET AL.ANGIOPLASTY OF CORONARY ARTERY BYPASS GRAFTS
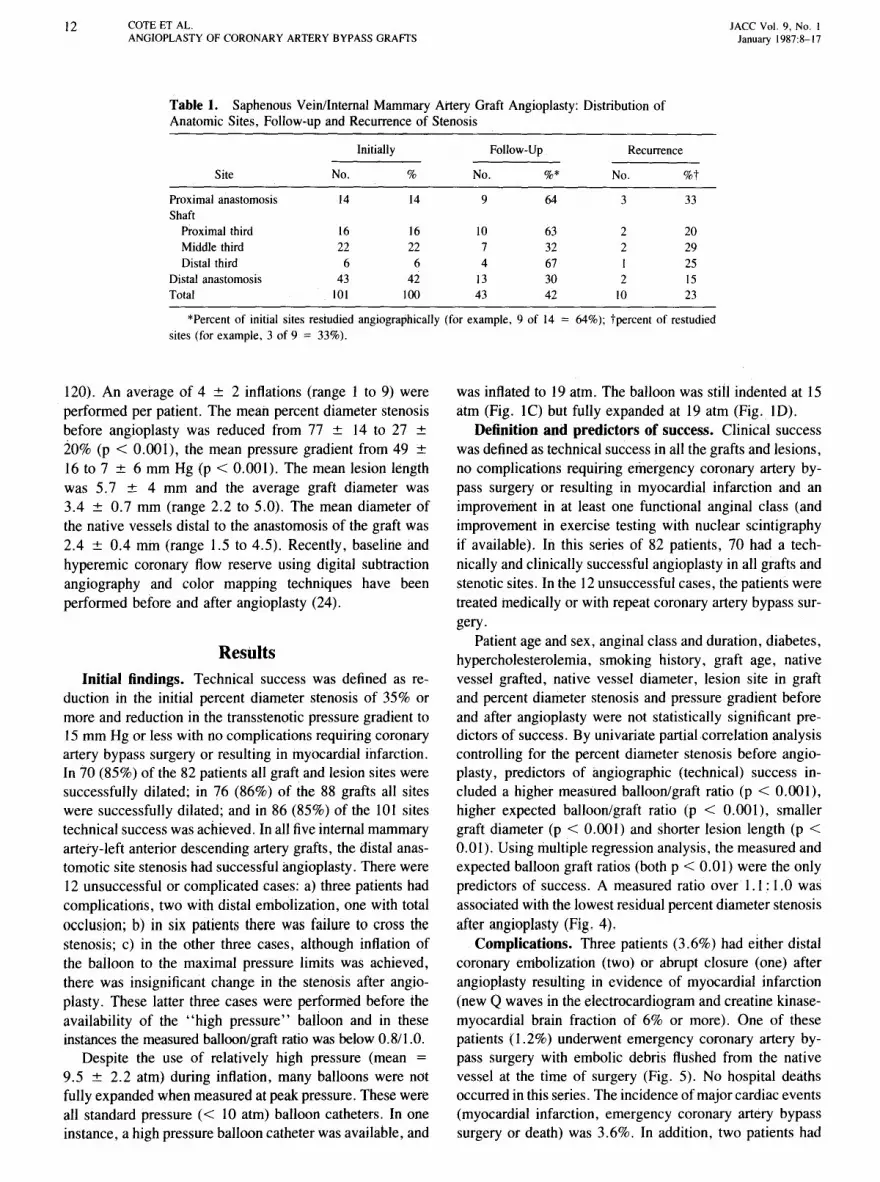
Table 1. Saphenous Vein/Internal Mammary Artery Graft Angioplasty: Distribution ofAnatomic Sites, Follow-up and Recurrence of Stenosis
Initially Follow-Up Recurrence
Site No. % No. %* No. %t
Proximal anastomosis 14 14 9 64 3 33Shaft
Proximal third 16 16 10 63 2 20Middle third 22 22 7 32 2 29Distal third 6 6 4 67 I 25
Distal anastomosis 43 42 13 30 2 15Total 101 100 43 42 10 23
*Percent of initial sites restudied angiographically (for example, 9 of 14 = 64%); tpercent of restudiedsites (for example, 3 of 9 = 33%).
JACC Vol. 9, No. IJanuary 1987:8-17
120). An average of 4 ± 2 inflations (range 1 to 9) wereperformed per patient. The mean percent diameter stenosisbefore angioplasty was reduced from 77 ± 14 to 27 ±20% (p < 0.001), the mean pressure gradient from 49 ±16 to 7 ± 6 mm Hg (p < 0.001). The mean lesion lengthwas 5.7 ± 4 mm and the average graft diameter was3.4 ± 0.7 mm (range 2.2 to 5.0). The mean diameter ofthe native vessels distal to the anastomosis of the graft was2.4 ± 0.4 mm (range 1.5 to 4.5). Recently, baseline andhyperemic coronary flow reserve using digital subtractionangiography and color mapping techniques have beenperformed before and after angioplasty (24).
ResultsInitial findings. Technical success was defined as re
duction in the initial percent diameter stenosis of 35% ormore and reduction in the transstenotic pressure gradient to15 mm Hg or less with no complications requiring coronaryartery bypass surgery or resulting in myocardial infarction.In 70 (85%) of the 82 patients all graft and lesion sites weresuccessfully dilated; in 76 (86%) of the 88 grafts all siteswere successfully dilated; and in 86 (85%) of the 101 sitestechnical success was achieved. In all five internal mammaryartery-left anterior descending artery grafts, the distal anastomotic site stenosis had successful angioplasty. There were12 unsuccessful or complicated cases: a) three patients hadcomplications, two with distal embolization, one with totalocclusion; b) in six patients there was failure to cross thestenosis; c) in the other three cases, although inflation ofthe balloon to the maximal pressure limits was achieved,there was insignificant change in the stenosis after angioplasty. These latter three cases were performed before theavailability of the "high pressure" balloon and in theseinstances the measured balloon/graft ratio was below 0.811.0.
Despite the use of relatively high pressure (mean =
9.5 ± 2.2 atm) during inflation, many balloons were notfully expanded when measured at peak pressure. These wereall standard pressure « 10 atm) balloon catheters. In oneinstance, a high pressure balloon catheter was available, and
was inflated to 19 atm. The balloon was still indented at 15atm (Fig. lC) but fully expanded at 19 atm (Fig. lD).
Definition and predictors of success. Clinical successwas defined as technical success in all the grafts and lesions,no complications requiring emergency coronary artery bypass surgery or resulting in myocardial infarction and animprovement in at least one functional anginal class (andimprovement in exercise testing with nuclear scintigraphyif available). In this series of 82 patients, 70 had a technically and clinically successful angioplasty in all grafts andstenotic sites. In the 12 unsuccessful cases, the patients weretreated medically or with repeat coronary artery bypass surgery.
Patient age and sex, anginal class and duration, diabetes,hypercholesterolemia, smoking history, graft age, nativevessel grafted, native vessel diameter, lesion site in graftand percent diameter stenosis and pressure gradient beforeand after angioplasty were not statistically significant predictors of success. By univariate partial correlation analysiscontrolling for the percent diameter stenosis before angioplasty, predictors of angiographic (technical) success included a higher measured balloon/graft ratio (p < 0.001),higher expected balloon/graft ratio (p < 0.001), smallergraft diameter (p < 0.001) and shorter lesion length (p <0.01). Using multiple regression analysis, the measured andexpected balloon graft ratios (both p < 0.01) were the onlypredictors of success. A measured ratio over 1.1: 1.0 wasassociated with the lowest residual percent diameter stenosisafter angioplasty (Fig. 4).
Complications. Three patients (3.6%) had either distalcoronary embolization (two) or abrupt closure (one) afterangioplasty resulting in evidence of myocardial infarction(new Q waves in the electrocardiogram and creatine kinasemyocardial brain fraction of 6% or more). One of thesepatients (1.2%) underwent emergency coronary artery bypass surgery with embolic debris flushed from the nativevessel at the time of surgery (Fig. 5). No hospital deathsoccurred in this series. The incidence of major cardiac events(myocardial infarction, emergency coronary artery bypasssurgery or death) was 3.6%. In addition, two patients had

JACC Vol. 9. No. IJanuary 19H7 :8-1 7
COTE ET AL.ANGIOPLASTY OF CORONARY ARTERY BYPASS GRAFTS
13
0."....--------------.....----.11 .7 .8 .9 1.0 1.1 1.2 1.3 1.4 1.5 1.11
8ALLOON GRAFT RATIO
J
, 11\ I II
B
A
in at least one site. The patients with patent grafts hadnormalization (or significant improvement) in exercise(treadmill) testing and no evidence of reversible ischemi aby nuclear scintigraphy. In the 10 patient s with recurrence,7 had no change in clinical classification and had exerci se
Figure 5. A. Angiogram (right anterior oblique [30°1 projection)of saphenous vein graft to the right coro nary artery showing numerous stenotic lesions (a r rows) before attempted angioplasty.Immediately after angioplasty, there was evidence of evolvinginferior myocardial infarction and the patient was taken for emergency surgery. Emboli c debris was flushed from the distal nativeright coro nary artery. A new saphenous vein graft was placed. B,The old saphenous vein graft was removed and showed evidenceof friable atheromatous mater ial and old and recent thrombus.
Figure 4. Relation of average percent diameter stenosis (PDS)after angioplasty (PTCA) versus balloon/graft ratio.
10
20
AVERAGE PDSPOST PTeI'
40
a minor complication: one had transient heart block and theother an episode of ventricular tachycardia that respondedto an intravenous bolus injection of lidocaine .
Patient age. sex . anginal class and duration . diabetesmellitus. hypercholesterolemi a. smoking history, graft age,graft or native vessel diameter. balloon size, native vesselgrafted, site of lesion in graft, percent diameter stenosis orpressure gradient before and after angioplasty were not statistically significant predictors of procedural complications.By univariate analysis, the only significant predictor of complications was the presence of diffuse atheromatous diseasein the grafts (p < 0.05). These grafts were all surgicallyplaced 4 years or more before angioplasty.
Follow-up. Of the 70 patients in whom angiopl asty wasperformed successfully, 26 so far have had angiographicrestudy at a mean of 7.9 ± 2. I months after angioplasty.Of the remaining 44 patients, 21 have not yet passed their6 month postangioplasty follow-up and therefore (by protocol) have not yet had repeat angiography. The remainin g23 patients, who are more than 6 months postangioplasty.have so far refused angiographic restudy because they areclinically asymptomatic. have negative (normal) exercisestudies, or both . In our experience. postoperati ve patients.unless symptomatic after angioplasty (or, for that matter.after coronary bypass surgery) are more difficult to convinceto have repeat angiography. no doubt because they havealready had several prior invasive procedures.
In the 26 patients with postangioplasty angiographic documentation , all anatomic sites were represented in the follow-up and there was no statistically significant differencein their distribut ion (Table I). Restenosis was defined as adecrease of 50% or more of the luminal diameter gain atthe time of angioplasty. Of these 26 patients , 16 had alllesions patent and 10 had evidence of recurrence in at leastone site. In these 26 patients, 43 grafts had been dilated:33 grafts were patent and 10 showed evidence of recurrenc e
14 COTE ET AL.ANGIOPLASTY OF CORONARY ARTERY BYPASS GRAFTS
JACC Vol. 9, No.1January 1987:8-17
75
oL- _
Figure 6. Average percent diameter stenosis after angiop1astyversus patentgrafts and recurrent graft stenosis.
PDSPOST PTCA
100
testing abnormalities similar to their preangioplasty test results. The other three patients with recurrence had improvement in their anginal class (class I or II) as well as exercisetesting results. These three patients had double graft (orvessel) angioplasty with recurrence in only one graft; theyhave been continued on medical therapy. Of the seven patients with angiographic recurrence and subjective and objective evidence of ischemia, six have had a second successful angioplasty and one had uncomplicated elective repeatcoronary bypass surgery.
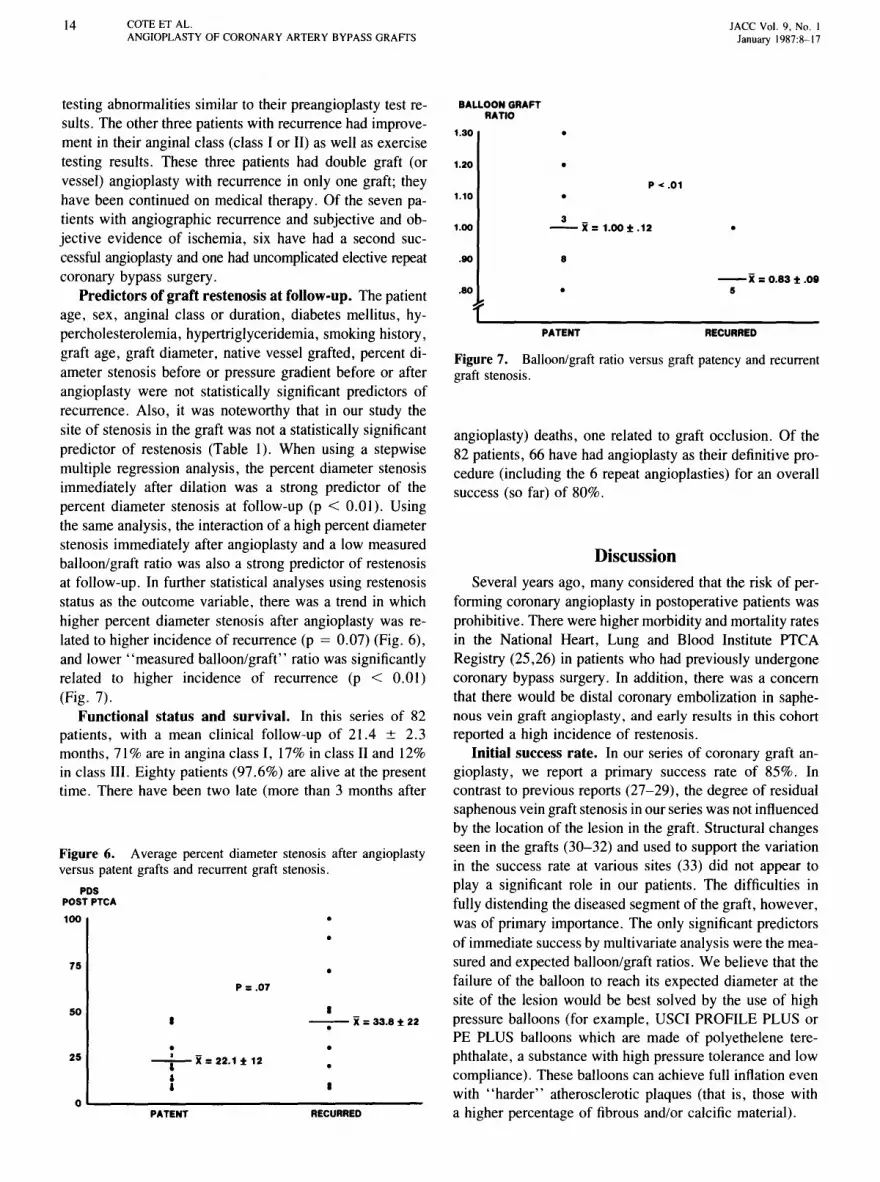
Predictors of graft restenosis at follow-up. The patientage, sex, anginal class or duration, diabetes mellitus, hypercholesterolemia, hypertriglyceridemia, smoking history ,graft age, graft diameter, native vessel grafted, percent diameter stenosis before or pressure gradient before or afterangioplasty were not statistically significant predictors ofrecurrence. Also, it was noteworthy that in our study thesite of stenosis in the graft was not a statistically significantpredictor of restenosis (Table I). When using a stepwisemultiple regression analysis, the percent diameter stenosisimmediately after dilation was a strong predictor of thepercent diameter stenosis at follow-up (p < 0.01). Usingthe same analysis, the interaction of a high percent diameterstenosis immediately after angioplasty and a low measuredballoon/graft ratio was also a strong predictor of restenosisat follow-up. In further statistical analyses using restenosisstatus as the outcome variable, there was a trend in whichhigher percent diameter stenosis after angioplasty was related to higher incidence of recurrence (p = 0.07) (Fig. 6),and lower "measured balloon/graft" ratio was significantlyrelated to higher incidence of recurrence (p < 0.01)(Fig. 7).
Functional status and survival. In this series of 82patients, with a mean clinical follow-up of 21.4 ± 2.3months, 71% are in angina class I, 17% in class II and 12%in class III. Eighty patients (97.6%) are alive at the presenttime. There have been two late (more than 3 months after
--x =0.83 ± .095
RECURRED
P -c .01
•
•
8
3 _--x= 1.00±.12
PATENT
.80
BALLOON GRAFTRATIO
.90
1.30
1.10
angioplasty) deaths, one related to graft occlusion. Of the82 patients, 66 have had angioplasty as their definitive procedure (including the 6 repeat angioplasties) for an overallsuccess (so far) of 80%.
Figure 7. Balloon/graft ratio versus graft patency and recurrentgraft stenosis.
1.00
1.20
L _
DiscussionSeveral years ago, many considered that the risk of per
forming coronary angioplasty in postoperative patients wasprohibitive. There were higher morbidity and mortality ratesin the National Heart, Lung and Blood Institute PTCARegistry (25,26) in patients who had previously undergonecoronary bypass surgery. In addition, there was a concernthat there would be distal coronary embolization in saphenous vein graft angioplasty , and early results in this cohortreported a high incidence of restenosis.
Initial success rate. In our series of coronary graft angioplasty, we report a primary success rate of 85%. Incontrast to previous reports (27-29), the degree of residualsaphenous vein graft stenosis in our series was not influencedby the location of the lesion in the graft. Structural changesseen in the grafts (30-32) and used to support the variationin the success rate at various sites (33) did not appear toplaya significant role in our patients. The difficulties infully distending the diseased segment of the graft, however,was of primary importance. The only significant predictorsof immediate success by multivariate analysis were the measured and expected balloon/graft ratios. We believe that thefailure of the balloon to reach its expected diameter at thesite of the lesion would be best solved by the use of highpressure balloons (for example, USCI PROFILE PLUS orPE PLUS balloons which are made of polyethelene terephthalate, a substance with high pressure tolerance and lowcompliance). These balloons can achieve full inflation evenwith "harder" atherosclerotic plaques (that is, those witha higher percentage of fibrous and/or calcific material).RECURRED
•
•--X=33.8±22·•P = .07
•-~- x=22.1 ± 12
ai
PATENT
50
25

JACC Vol. 9. No. IJanuary 1987:8-17
COTE ET AL.ANGIOPLASTY OF CORONARY ARTERY BYPASS GRAFTS
15
Morbidity and mortality. The previously noted highercomplication rate of patients who were postoperative or hadgraft angioplasty (25,26) has been countered by recent studies that showed a low incidence of morbidity (27,29,33-36).Our series is comparable with other published data in thatregard, showing a major cardiac event incidence of 3.6%.The low morbidity and mortality reported are most likelyrelated to technologic improvements (19) in the last fewyears as well as to increasing experience of those physicianswho perform angioplasty. Incidentally, it is of interest tocompare this angioplasty data with the results from surgicalcenters reporting morbidity and mortality in repeat coronarybypass operations (8-11). In these centers, there were perioperative myocardial infarction incidences of 2 to 12% andmortal ity rates of I to 17%.
Distal coronary embolization of an atheroma was reported by Aueron and Gruentzig (37). In two of our patients,both of whom had diffusely diseased grafts that were at least4 years old, distal embolization was noted (one proved atsurgery). Therefore, we strongly urge avoiding angioplastyin older grafts that show angiographic evidence of diffusedisease (Fig. 5); if medical management cannot control theangina in these patients with diffuse disease in old grafts,then we recommend surgery rather than angioplasty as asecond line of therapy.
The needfor emergency bypass surgery occurred in onlyone patient in our series. Yet, we firmly believe that emergency revascularization surgery after unsuccessful graft angioplasty represents a more significant challenge to the car
diovascular surgical team. Surgeons with extensive experiencewith myocardial revascularization and, in particular, emer
gency surgery after unsuccessful angioplasty should be atstandby for these cases. It may be advisable to utilize anintraaortic balloon pump in patients in whom abrupt reclosure of a dilated graft occurs after angioplasty (38). Thismay be especially important in patients who have had priorcardiac surgery, because chest wall and pleuro-pericardialfibrosis may delay reexposure of the heart during the second(emergency) operation. The intraaortic balloon pump mayeffectively stabilize the patient during this critical period.Fortunately, this was only necessary in one of our patients.
Follow-up results: graft restenosis. Our clinical follow-up results compare favorably with previously reportedsaphenous vein graft angioplasty studies (34-36) and alsoto reports of patients submitted to reoperation for coronaryartery disease (8-11). However, the true restenosis "rate"in our series is not precisely known. Only 53% of the 49successfully treated patients who have reached their 6 monthpostangioplasty period have had follow-up angiography. Yet,even if we use as the denominator only those patients whohave had angiographic documentation postangioplasty, ourrecurrence rates were 38% for the 26 patients and 23% forthe 43 grafts. This would probably be the "worst case"restenosis rate. On the other hand, it would not be fair to
state that we had a 14% (10 of the 70 successful cases)restenosis rate, because 21 patients have not passed throughthe 6 month "window of recurrence" (39,40). In addition,23 patients who are more than 6 months postangioplastyhave so far refused restudy because they are asymptomaticand have improved exercise studies. But "silent" recurrence has been reported in 5 to 14% of cases after angioplasty (39,41). Also, it should be noted that re-recurrencewill affect our restenosis incidence as well as the costeffectiveness of this technique compared with repeat coronary bypass surgery (42).
Restenosis rates of 50% were reported by EI Gamal etal. (36) and Reeder et al. (43). Dorros et al. (44) reported50 and 53% recurrence rates at the proximal anastomoticand graft shaft sites, respectively, and only 18% restenosisrate at the distal anastomotic site. Douglas and coworkers(28) noted the same discrepancy in restenosis rates, withthe lowest incidence occurring at the distal anastomotic site.This site variation in recurrence was not corroborated in ourstudy (Table I). However, none of these studies, or, forthat matter, ours, had 100% follow-up angiographic documentation. Each recurrence site "cell" was small in theseseries, as well as in ours, reducing the power of statisticalevaluation, making conclusions less reliable.
Nevertheless, one might implicate various pathologicphenomena (30-32,35,45,46) at different sites in the graft.Furthermore, Hollman (35) also noted a higher recurrencerate (as well as acute embolic events) in older grafts. Hesuggested that this may be related to changing graft diseasewith age. Early changes in vein grafts are those of intimalhyperplasia (47). In patients with normal lipids, unique atherosclerotic changes develop after about 3 years (earlier inhyperlipidemic patients) (45). Foam cells may erode throughthe graft intima and the entire atheromatous plaque may bemore friable and more likely to embolize than those seenin the native coronary arterial circulation.
Perhaps the higher residual stenosis after angioplasty reported at the proximal anastomotic site (26,44) may explainthe higher recurrence rates previously noted. In our series,however, there was no significant difference in postangioplasty percent diameter stenosis at the various sites in thegrafts. The measured balloon-graft ratios were the only statistically significant predictor of immediate (technical) success and long-term results (Fig. 4 and 7).
Prior reports (28,34,44) as well as our data suggest thata significant residual stenosis after angioplasty may affectthe long-term patency (Fig. 6). Higher postangioplasty residual stenoses may be due to atheroma that are "hard"(high percentage of fibrous or calcific material) or due tothe use of a balloon that is too small relative to the graftdiameter. The use of high pressure balloons will certainlypermit more effective compaction of "hard" lesions. Furthermore, it would appear that using balloons large enoughto achieve balloon/graft ratios of at least I. I : 1.0 may achieve

16 COTE ET AL.ANGIOPLASTY OF CORONARY ARTERY BYPASS GRAFTS
JACC Vol. 9. No. JJanuary 1987:8-17
more optimal initial technical results and, perhaps, increaselong-term patency. It should be emphasized, however, thatthere may be an increased risk of dissection with indiscriminate oversizing of balloons in relation to grafts or nativecoronary arteries. Therefore, oversizing balloons should beavoided with eccentric lesions on sharp curves in nativecoronary arteries or grafts (48).
Finally, we suggest that because of problems associatedwith identifying recurrence "rates" in series with less than90% angiographic follow-up, "risk" of recurrence may bea more meaningful concept. In this context, risk means thelikelihood, as predicted by certain factors, of recurrence ofstenosis in a particular patient (for example, patients withlower balloon/graft ratio at baseline may be at higher riskfor recurrence). Therefore, risk refers to the cohort of patients who present for angiographic follow-up and is lessaffected by the number of patients in the original sample.
Conclusions. Saphenous vein and internal mammary artery graft stenoses can be successfully treated with the coronary angioplasty technique. An 85% initial success rate isreported along with an emergency bypass incidence of 1.2%,myocardial infarction incidence of 3.6% and major cardiacevent rate of 3.6%. No hospital deaths occurred. Theseinitial results compare favorably with similar angioplastystudies and with the results of reoperation for saphenousvein grafts stenosis. Careful selection of appropriate patients, avoiding those with diffusely diseased older grafts,will further enhance the success rate and decrease the complication rate. The problem of recurrence following nativecoronary angioplasty has been described in detail elsewhere(41,49-52), but graft angioplasty may offer particular insights into this problem because of the different pathologicprocesses in saphenous vein grafts. Higher pressure balloonsand efforts to achieve slightly larger balloon/graft ratios maylead to a decrease in recurrence rates. Also certain pharmacologic regimens may favorably affect the recurrence rateafter graft angioplasty (53,54).
With identification of those factors responsible for success, complications and recurrence, coronary angioplastymay well be the treatment of choice in symptomatic patientswith saphenous vein or internal mammary artery graft stenosis.
ReferencesI. Kolessov VI. Mammary artery-coronary artery anastomosis as method
of treatment for angina pectoris. J Thorac Cardiovasc Surg1967;54:535-44.
2. Favaloro RG. Saphenous vein auto graft replacement of severe segmental coronary artery occlusion: operative technique. Ann ThoracSurg 1968;5:334-9.
3. Campeau L, Enjalbert M, Lesperance J, et a!. The relationship of riskfactors to the development of atherosclerosis in saphenous vein graftsand the progression of disease in the native circulation: a study 10
years after aortocoronary bypass surgery. N Engl J Med1984;311:1329-32.
4. Seides SF, Borer JS, Kent KM, Rosing DR, Mcintosh CL, EpsteinSE. Long-term anatomic fate of coronary-artery bypass grafts andfunctional status of patients five years after operation. N Engl J Med1978;298:1213-7.
5. Guthaner OF, Robert EW, Alderman EL, Wexler L. Long-term serialangiographic studies after coronary artery bypass surgery. Circulation1979;60:250-9.
6. Kouchoukos NT, Karp RB, Oberman A, Russel RO Jr, Allison HW.Holt JH Jr. Long-term patency of saphenous veins for coronary bypassgrafting. Circulation 1979;58(Suppl 1):1-96-9.
7. Hamby RI, Aintablian A, Handler M, et al. Aortocoronary saphenousvein bypass grafts. Long-term patency, morphology and blood flowin patients with patent grafts early after surgery. Circulation1979;60:901-9.
8. Reu1 GJ, Cooley DA, Ott DA, Coelho A, Chapa L, Eterovic I. Reoperation for recurrent coronary artery disease. Arch Surg1979;114:1269-75.
9. Vouhe P, Grondin CM. Reoperation for coronary graft failure: clinicaland angiographic results in 43 patients. Ann Thorac Surg1979;27:328-34.
10. Krause AH Jr, Page US, Bigelow JC, Okies JE, Dunlap SF. Reoperation in symptomatic patients after direct coronary artery revascularization. J Thorac Cardiovasc Surg 1978;75:499-504.
II. Loop FD, Thurer RL, Lytie BW, Cosgrove DM. Reoperation formyocardial revascularization. World J Surg 1968;2:719-29.
12. Norwood WI, Cohn LH, Collins 11. Results of reoperation for recurrent angina pectoris. Ann Thorac Surg 1977;23:9-13.
13. Gruentzig AR, Myler RK, Hanna EH, Turina MI. Coronary transluminal angioplasty (abstr). Circulation 1977;84(Suppl III):III-55-6.
14. Gruentzig A. Transluminal dilatation of coronary-artery stenosis (letter). Lancet 1978; I:263-6.
15. Gruentzig AR, Myler RK, Stertzer SH, Kaltenbach M, Turina MI.Coronary percutaneous transluminal angioplasty: preliminary results(abstr). Circulation 1978;58(Suppl 11):11-56.
16. Gruentzig AR, Senning A, Siegenthaler WE. Non-operative dilatationof coronary artery stenosis. Percutaneous transluminal coronary angioplasty. N Engl J Med 1979;301:61-8.
17. Stertzer SH, Myler RK, Bruno JP, Wallsh E. Transluminal coronaryartery dilatation. Pract Cardiol 1979;5:25-30.
18. Dorros G, Stertzer SH, Cowley MJ, Myler RK. Complex coronaryangioplasty: Multiple coronary dilatations. Am J Cardiol1984;53: I26c-30c.
19. Myler RK. Transfemoral approach to percutaneous coronary angioplasty. In: Jang GD, ed. Angioplasty. New York: McGraw-Hill,1986:198-259.
20. Topol E, Myler RK, Stertzer SH. Selection of dilatation hardware forPTCA, 1985. Cathet Cardiovasc Diagn 1985;11:629-37.
21. Jain A, Derner LL, Raizner AE, Roberts R. Effect of inflation pressures on coronary angioplasty balloons. Am J Cardiol 1986;57:26-8.
22. Campeau L. Grading of angina pectoris (letter). Circulation1976;54:522-3.
23. Stertzer SH. Percutaneous transluminal angioplasty the brachial approach. In: Ref 19, 260-94.
24. Vogel RA. Digital radiographic assessment of coronary flow reserve.In: Buda AJ, Delp EJ, eds. Digital Cardiac Imaging. Boston: MartinusNijhoff, 1985:106-18.
25. Kent KM, Bentivoglio LG, Block PC, et al. Percutaneous transluminalcoronary angioplasty: report from the Registry of the National Heart,Lung, and Blood Institute. Am J Cardiol 1982;49:2011-20.
26. Mock MB, Kent KM, Bentivoglio LG. The National Heart, Lung,and Blood Institute Percutaneous Transluminal Coronary AngioplastyRegistry: the first 1116 cases. In: Kaltenbach M, Gruentzig A, Rentrop

JACC Vol. 9. No. IJanuary 1987:8-1 7
COTE ET AL.ANGIOPLASTY OF CORONARY ARTERY BYPASS GRAFTS
17
K. Bussmann WD; eds. Transluminal Coronary Angioplasty and Intracoronary Thrombolysis . Coronary Heart Disease. IV. Berlin . Heidelberg . New York: Springer-Verlag . 1982:1-9 .
27. Douglas JS Jr. Gruentzig AR. King SB III . et al. Percutaneous transluminal coro nary angioplasty in patients with prior coronary bypasssurgery . J Am Coli Cardiol 1983;2:745- 54.
28. Douglas JS Jr . Gruentzig AR. King SB III. Ho llman J. Long-termresults of percutaneous transluminal angioplasty for aorto-coronarysaphenous vein graft stenosis (abstr). Circulation I982;66(Suppl 1\):11124.
29. Corbelli J . FrancoI , Hollman J. Simpfendorfer C. Galan K. Percutaneous transluminal coronary angioplasty after previous coronary artery bypass surgery . Am J Cardio l 1985;56:398- 403.
30 . Griffith LSC. Bulkley BH. Hutchins GM. Brawley RK. Occlusivechanges at the coronary artery-bypass graft anastomosis. Morphologicstudy of 95 grafts . J Thorac Cardiovasc Surg 1977;73:668- 79.
31. Spray TL . Roberts We. Changes in saphenous veins used as aortocoronary bypass grafts. Am Heart J 1977;94:500-1 6.
32. Waller BF. Rothbaum DA. Gorfinkel HJ. et at. Morphologic observations after percutaneous transluminal balloon angioplasty of earlyand late aortocoronary saphenous vein bypass grafts. J Am Coli Cardiol i98 4:4:784-92.
33. Ford WB. Wholey Mil Zikria EA. Somadani SR. Sullivan ME.Percutaneous transluminal dilatation of aortocoro nary saphenous veinbypass grafts. Chest 1981:79:529-35 .
34. Block PC. Cowley MJ. Kaltenbach M. Kent KM. Simpson J . Percutaneous angioplasty of stenoses of bypass grafts or of bypass graftanastomotic sites. Am J Cardiol 1984;53:666-8.
35. Hollman J. Percutaneous transluminal angioplasty in patients withfailed coronary bypass grafts . In: Ref 19. 346-56.
36. EI Gamal M. Runnier H. Michels R. Heijman 1. Stassen E. Percutaneous transluminal angioplasty of stenosed aortocoronary bypassgrafts. Br Heart J 1984;52:617-28.
37. Aueron F. Gruentzig AR. Distal embolization of a coronary arterybypass graft atheroma during percutaneous transluminal coronary angioplasty. Am J Cardiol 1984;53:953-4.
38. Alcan KE. Stertzer SH. Wallsh E. De Pasquale NP. Bruno MS. Therole of intra-aortic balloon counterpulsation in patients undergoingpercutaneous transluminal angioplasty . Am Heart J 1983:105:527-30 .
39. Holmes DR Jr. Vlietstra RE. Smith HC. et at. Restenosis after percutaneous transluminal coronary angioplasty (PTCA): a report fromthe PTCA Registry of the National Heart. Lung and Blood Institute .Am J Cardiol 1984:53:77c-8I c .
40 . Myler RK. Gruentzig AR. Stertzer SH. Coronary angioplasty . In:Rapaport E. ed . Cardiology Update III. New York: Elsevier Biomedical.1983:1-66.
4 1. Hall RJ. Virendra M. Massumi A. Garcia E. Fighali S. Percutaneoustransluminal coronary angioplasty update. Tex Heart InstJ 1984;11:10-6 .
42. Jang GC . Gruentzig AR. Block Pc. Myler RK. Stertzer SH. Delayedeffect of vessel restenosis on the procedure cost of coronary angioplasty (abstr) . Circulation 1982:66:11- 330 .
43. Reeder GS. Bresnahan JF. Holmes DR. et at. Angioplasty for aortocoronar y bypass graft stenosis. Mayo Clin Proc 1986;61:14- 19 .
44. Dorros G. Johnson WD. Tector AJ. Schmahl TM . Kalush SL. JankeL. Percutaneous transluminal coronary angioplasty in patients withprior coronary artery bypass grafting. J Thorac Cardiovasc Surg1984:87:17- 26 .
45. Smith SH. Geer Je. Morphology of saphenous vein-coronary arterybypass grafts . Arch Pathoi Lab Med 1983;107:13-8.
46. Griffith LSC. Bulkley BH. Hutchins GM. Brawley RK. Occlusivechanges at the coronary artery-bypass graft anastomosis. morphologicstudy of 95 grafts. J Thorac Cardiovasc Surg 1977;73:668-79.
47. Bulkley RH. Hutch ins GM. " Accelerated atherosclerosis." A morphologic study of 97 saphenous vein coronary artery bypass grafts .Circulation 1977:55:163- 9 .
48. Cowley M1. Dorros G. Kelsey SF. Van Raden M. Detre KM. Acutecoronary event associated with percutaneous transluminal coronaryangioplasty . Am J Cardiol 1984;53:12c-16c .
49. George B. Myler RK. Stertzer SH. et al. Balloon angioplasty ofcoronary bifurcation lesions-the kissing balloon techn ique. CathetCardiovasc Diagn 1986;12:124- 38.
50 . Myler RK. Topo l EJ. Shaw RE. et al. Multiple vessel coronary angioplasty: classification. results and patteni s of restenosis in 494 consecutive patients. Cathet Cardiovasc Diagn (in press).
51. Leimgruber PP. Roubin GS. Hollman J. et al. Restenosis after successful coronary angioplasty in patients with single-vessel disease.Circulation 1986:73:710-7.
52. Myler RK. Shaw RE. Stertzer SH. Clark DA. Fishman-Rosen J.Murphy MC. Recurrence after coronary angioplasty. Cathet Cardiovase Diagn (in press).
53 . Chesebro JH. Fuster V. Elveback LR. et al. Effect of dipyridamoleand aspirin on late vein-graft patency after coronary bypass operations.N Engl J Med 1984;310:209-14.
54. Fuster V, Chesebro JH. Role of platelets and platelet inhibitors inaortocoronary artery vein-graft disease . Circulation 1986;73:227- 32.
Related Documents











