Percutaneous circulatory support. IABP, Impella and beyond Holger Thiele Medical Clinic II (Cardiology/Angiology/Intensive Care) University Heart Center of Lübeck, Germany

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

Percutaneous circulatory support. IABP, Impella and beyond
Holger ThieleMedical Clinic II (Cardiology/Angiology/Intensive Care)
University Heart Center of Lübeck, Germany

Disclosures
Funding:German Research FoundationGerman Heart Research Foundation German Cardiac SocietyEUArbeitsgemeinschaft Leitende Kardiologische Krankenhausärzte
Consulting:None
Speaker Honoraria:Lilly, Astra Zeneca, Daiichi Sankyo, Boehringer Ingelheim, Maquet Cardiovascular, Medicines Company

In-hospital Mortality
Aissaoui et al. Eur Heart J 2012; 33:2535–2543
USIK 1995, USIC 2000, FAST-MI France National Registry
1995 2000 2005
9080706050403020100
Dea
th a
fter 3
0 da
ys (%
)
8.7(7.5-10.0) 4.2
(3.4-5.1)3.6
(3.0-4.4)
51(44-59)
63(56-70)
70(62-77)
ShockNo Shock

Trial n/N n/NRelative Risk
95% CIRelative Risk95% CI
0 0.5 1 2 3
Randomized Trials in Cardiogenic ShockFollow-up
Revascularization (PCI/CABG) SHOCK SMASH Total
81/152 22/32103/184
100/150 18/23118/173
1 year30 days
Early revascularization better
Medical treatment better
0.75 1.5 2.50.25Thiele et al. Eur Heart J 2015;36:1223-1230
0.72 (0.54;0.95)0.87 (0.66;1.29)0.82 (0.69;0.97)
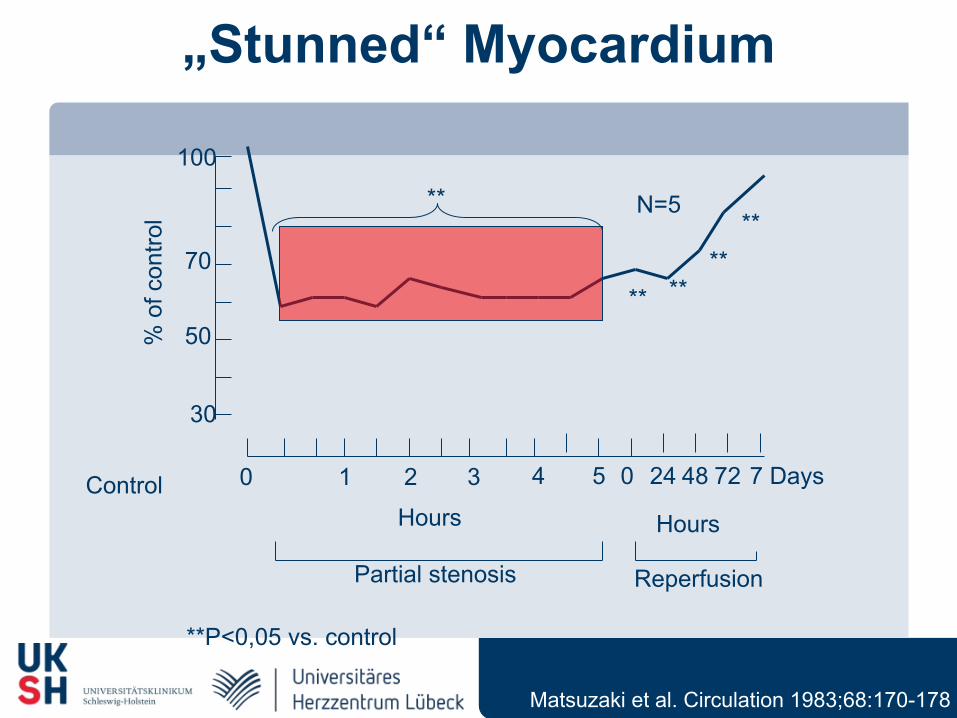
„Stunned“ Myocardium
Partial stenosis Reperfusion
Hours Hours
7 Days
N=5
Control 0 1 2 3 4 5 0 24 48 72
100
70
50
30
% o
f con
trol
**
** ****
**
**P<0,05 vs. control
Matsuzaki et al. Circulation 1983;68:170-178
IABP History
History: 1962 Animal trials
Moulopoulos et al, Am Heart J 1962;63:669-675
1968 1. clinical description in shock Kantrowitz et al, JAMA 1968;203:135-140
1973 Hemodynamic effects, mortality unchangedScheidt et al, NEJM 1973;288:979-984
> 40 years > 1 Million patients treated, low complication rate, Benchmark registry Ferguson et al, JACC 2001;38:1456-1462
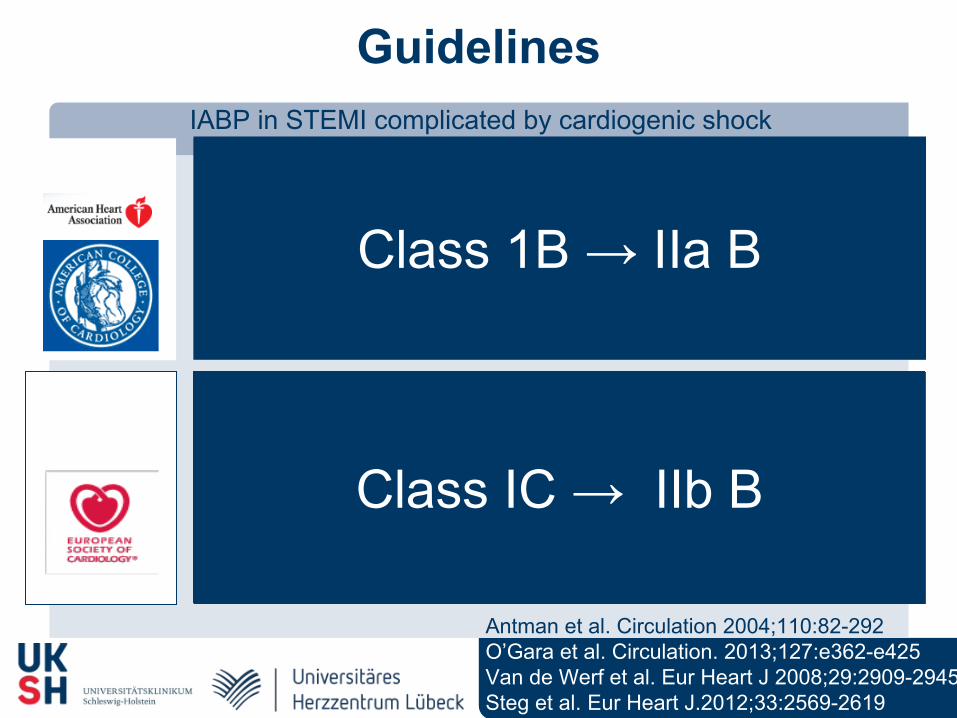
GuidelinesIABP in STEMI complicated by cardiogenic shock
Class 1B → IIa B
ACC/AHA
ESC
Class IC → IIb B
Antman et al. Circulation 2004;110:82-292O’Gara et al. Circulation. 2013;127:e362-e425Van de Werf et al. Eur Heart J 2008;29:2909-2945Steg et al. Eur Heart J.2012;33:2569-2619

Sjauw et al. Eur Heart J 2009;30:459-468
Mortality IABP vs IABP - Metaanalysis
-1 -0.5 0.5 10
No IABP betterIABP better
30-Day MortalityRisk Difference
IABPn/N
No IABPn/N
Trial
-0.18 (-0.20 to -0.16)Total
ThrombolysisStomel
Kovack
BengtsonWaksman
GUSTO-1SHOCK registry
NRMI-2 TT
28/51
10/2748/9911/20
30/62220/439
1068/2180
1415/2878
10/1313/19
58/10117/21
146/248300/417
2346/3501
2890/4320
-0.11 (-0.13 to -0.09)Total 2488/5146 3332/5283
Total 1049/2234 0.06 (0.03 to 0.10)
Primary PCINRMI-2 PCIAMC CS
956/2035
93/199401/955
26/93427/1048
-0.29 (-0,47 to -0.12)
No reperfusion
24/34
24/34
15/15
15/15
Moloupoulos
Total
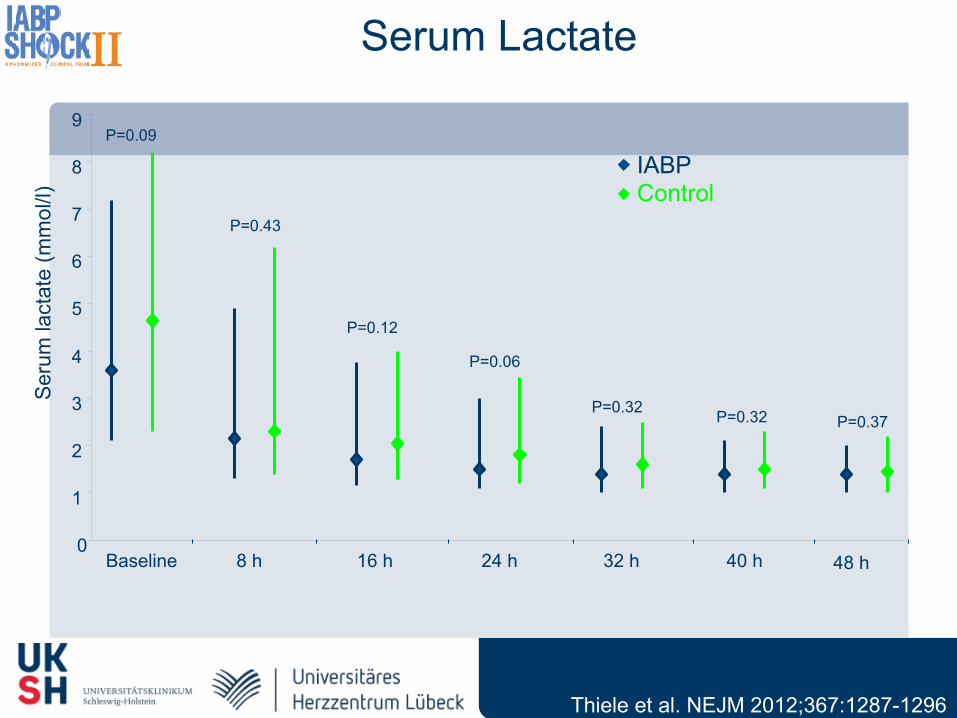
0
1
2
3
4
5
6
7
8
9
P=0.43
P=0.12
P=0.06
P=0.32 P=0.32 P=0.37
Baseline 8 h 16 h 24 h 32 h 40 h 48 h
Ser
um la
ctat
e (m
mol
/l)
P=0.09
ControlIABP
Serum Lactate
Thiele et al. NEJM 2012;367:1287-1296
Mor
talit
y (%
)
Time after randomization (days)
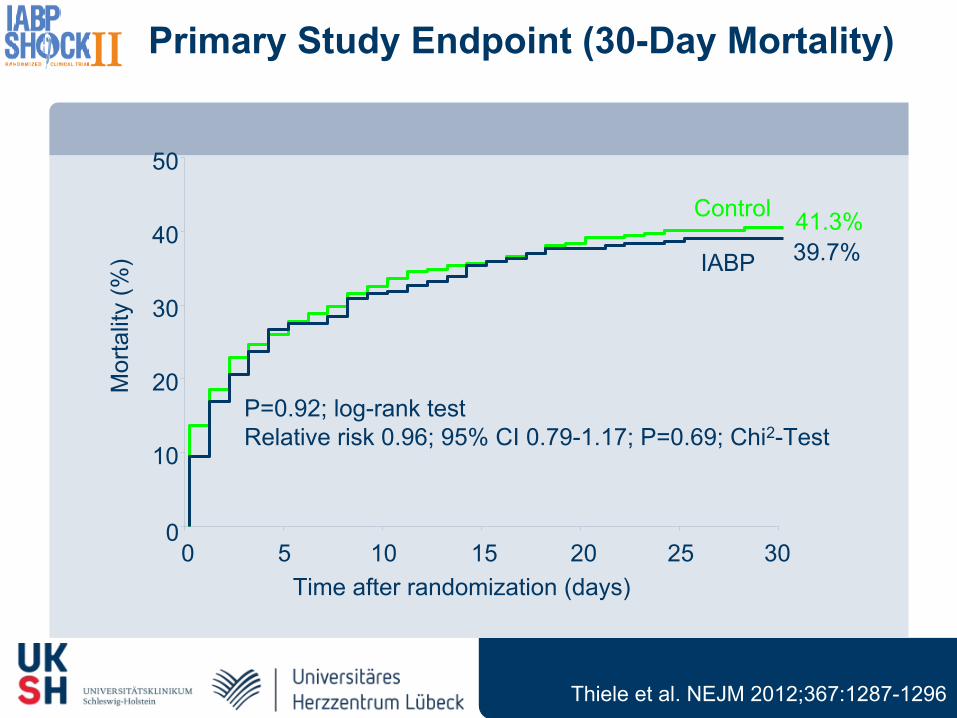
P=0.92; log-rank testRelative risk 0.96; 95% CI 0.79-1.17; P=0.69; Chi2-Test
Primary Study Endpoint (30-Day Mortality)
Control 41.3%
IABP 39.7%
0
10
20
30
40
50
0 5 10 15 20 25 30
Thiele et al. NEJM 2012;367:1287-1296
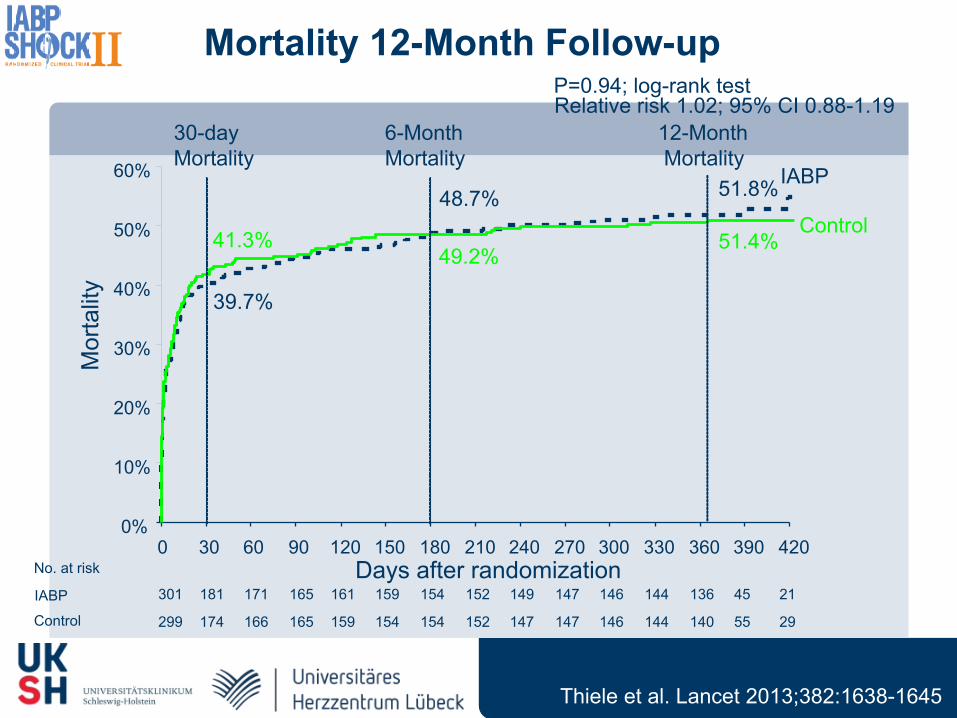
Mortality 12-Month Follow-up
Control
IABP
0%
10%
20%
30%
40%
50%
60%
0 30 60 90 120 150 180 210 240 270 300 330 360 390 420
Mor
talit
y
Days after randomization
P=0.94; log-rank testRelative risk 1.02; 95% CI 0.88-1.19
12-Month Mortality
49.2%
48.7%
6-MonthMortality
30-dayMortality
41.3%
39.7%
51.8%
51.4%
301 181 171 165 161 159 154 152 149 147 146 144 136 45 21
299 174 166 165 159 154 154 152 147 147 146 144 140 55 29
No. at risk
IABP
Control
Thiele et al. Lancet 2013;382:1638-1645
Trial n/N n/NRelative Risk
95% CIRelative Risk95% CI
0 0.5 1 2 3
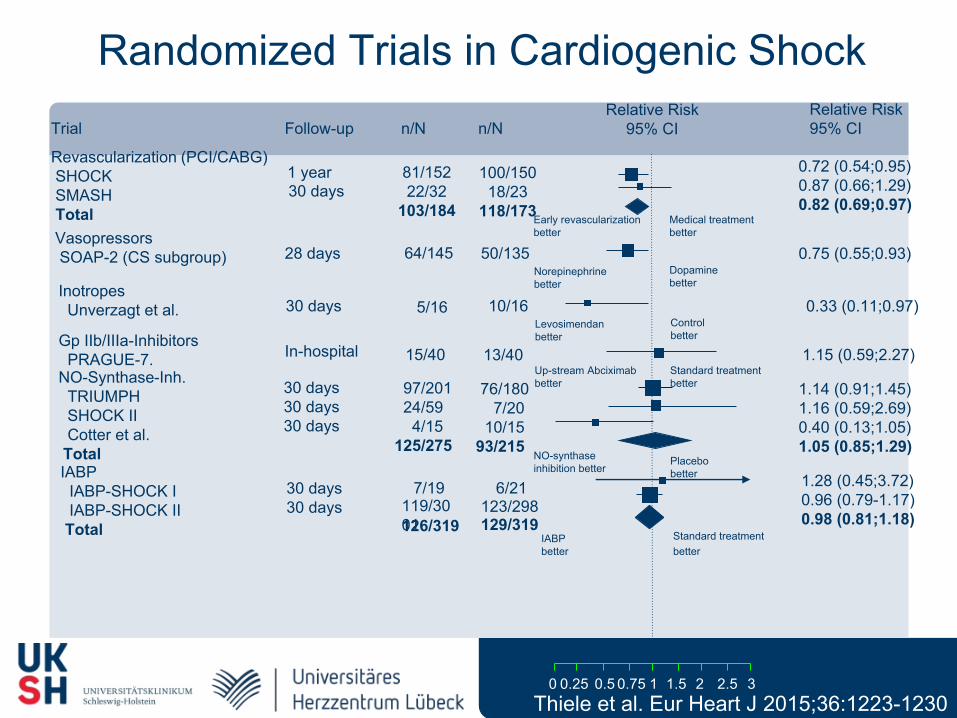
Randomized Trials in Cardiogenic ShockFollow-up
Revascularization (PCI/CABG) SHOCK SMASH Total
81/152 22/32103/184
100/150 18/23118/173
1 year30 days
Early revascularization better
Medical treatment better
0.75 1.5 2.50.25
0.72 (0.54;0.95)0.87 (0.66;1.29)0.82 (0.69;0.97)
0.75 (0.55;0.93)64/145 50/13528 daysNorepinephrinebetter
Dopamine better
Vasopressors SOAP-2 (CS subgroup)
0.33 (0.11;0.97)5/16 10/1630 daysLevosimendanbetter
Controlbetter
Inotropes Unverzagt et al.
Gp IIb/IIIa-Inhibitors PRAGUE-7. In-hospital 15/40 13/40 1.15 (0.59;2.27)
Up-stream Abciximabbetter
Standard treatmentbetter
30 days30 days
7/19 6/21
IABPbetter
Standard treatmentbetter
1.28 (0.45;3.72)0.96 (0.79-1.17)0.98 (0.81;1.18)
119/3001
123/298126/319 129/319
IABP IABP-SHOCK I IABP-SHOCK II Total
30 days30 days30 days
97/201 24/59 4/15125/275
76/180 7/20 10/1593/215
1.14 (0.91;1.45)1.16 (0.59;2.69)0.40 (0.13;1.05)1.05 (0.85;1.29)
NO-synthase inhibition better
Placebobetter
NO-Synthase-Inh. TRIUMPH SHOCK II Cotter et al. Total
Thiele et al. Eur Heart J 2015;36:1223-1230

ESC Revascularization Guidelines 2014IABP in cardiogenic shock
ESC
Class IC → IIb B → III
Windecker et al. Eur Heart J. 2014;35:2541-2619

LVAD/ECMO or IABP?
Bleeding Invasiveness
+ -
Implantation procedure
LVAD
Hemodynamic Support Better LV-unloading
Costs
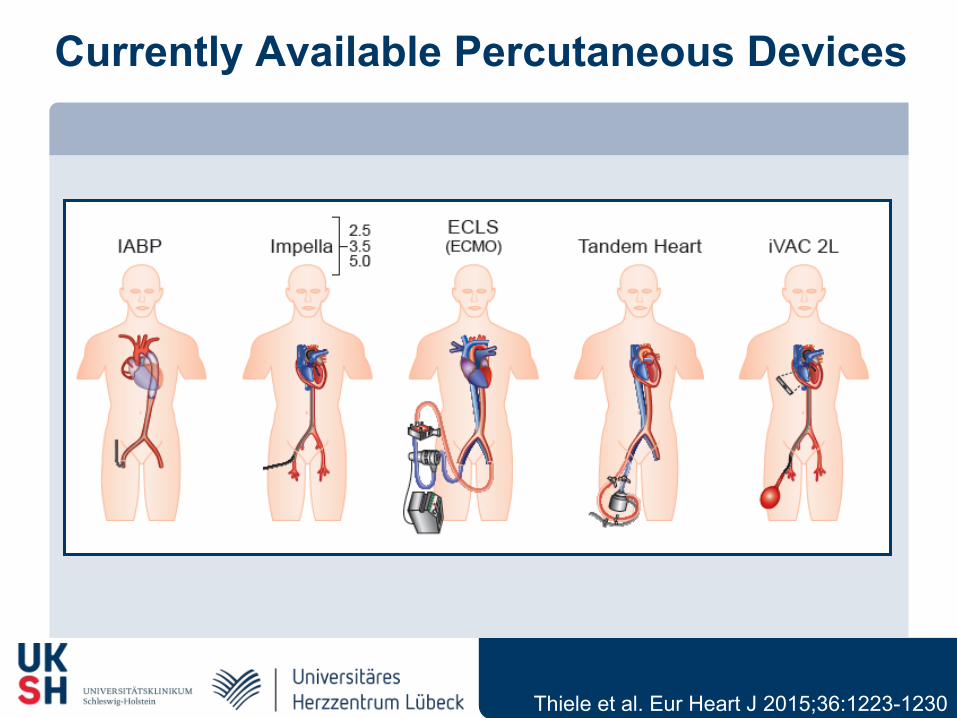
Currently Available Percutaneous Devices
Thiele et al. Eur Heart J 2015;36:1223-1230

Technical Parameters
Currently Available Percutaneous Devices
Thiele et al. Eur Heart J 2015;36:1223-1230
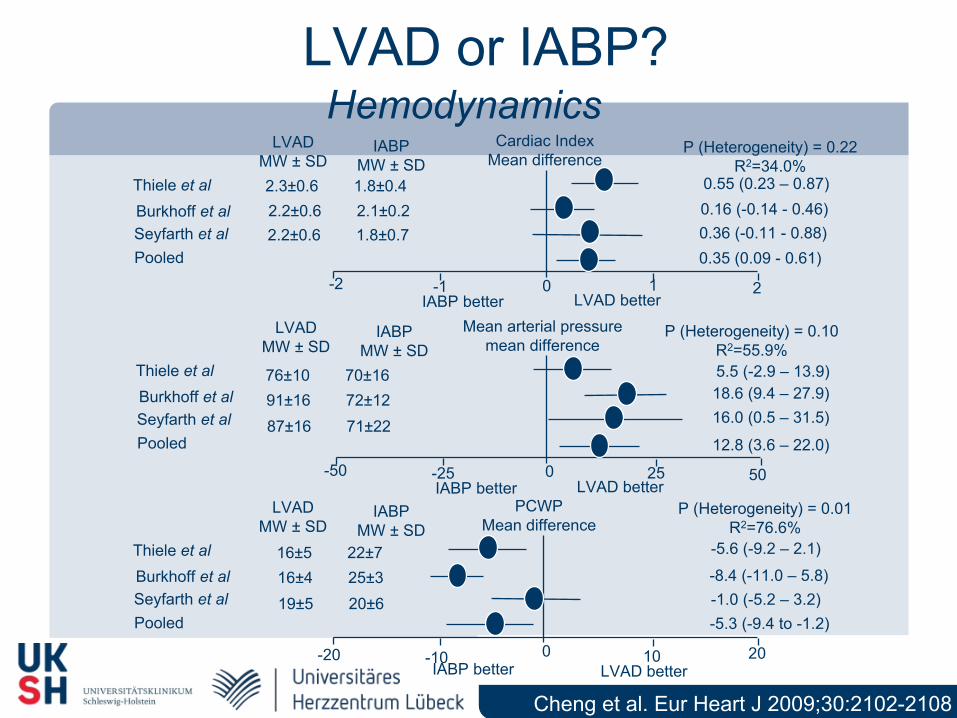
LVAD or IABP?
Cheng et al. Eur Heart J 2009;30:2102-2108
HemodynamicsLVAD
MW ± SDIABP
MW ± SDCardiac Index
Mean differenceP (Heterogeneity) = 0.22
R2=34.0%Thiele et alBurkhoff et alSeyfarth et alPooled
-2 -1 0 1 2LVAD betterIABP better
0.55 (0.23 – 0.87)0.16 (-0.14 - 0.46)0.36 (-0.11 - 0.88)0.35 (0.09 - 0.61)
2.3±0.6 1.8±0.42.2±0.6 2.1±0.22.2±0.6 1.8±0.7
LVAD betterIABP better
LVADMW ± SD
IABPMW ± SD
Mean arterial pressuremean difference
P (Heterogeneity) = 0.10R2=55.9%
Thiele et alBurkhoff et alSeyfarth et alPooled
-50 -25 0 25 50
5.5 (-2.9 – 13.9)18.6 (9.4 – 27.9)16.0 (0.5 – 31.5)
12.8 (3.6 – 22.0)
76±10 70±1691±16 72±1287±16 71±22
16±5 22±716±4 25±319±5 20±6
LVADMW ± SD
IABPMW ± SD
PCWPMean difference
P (Heterogeneity) = 0.01R2=76.6%
Thiele et alBurkhoff et alSeyfarth et alPooled
-20 -10 0 10 20LVAD betterIABP better
-5.6 (-9.2 – 2.1)
-8.4 (-11.0 – 5.8)-1.0 (-5.2 – 3.2)-5.3 (-9.4 to -1.2)
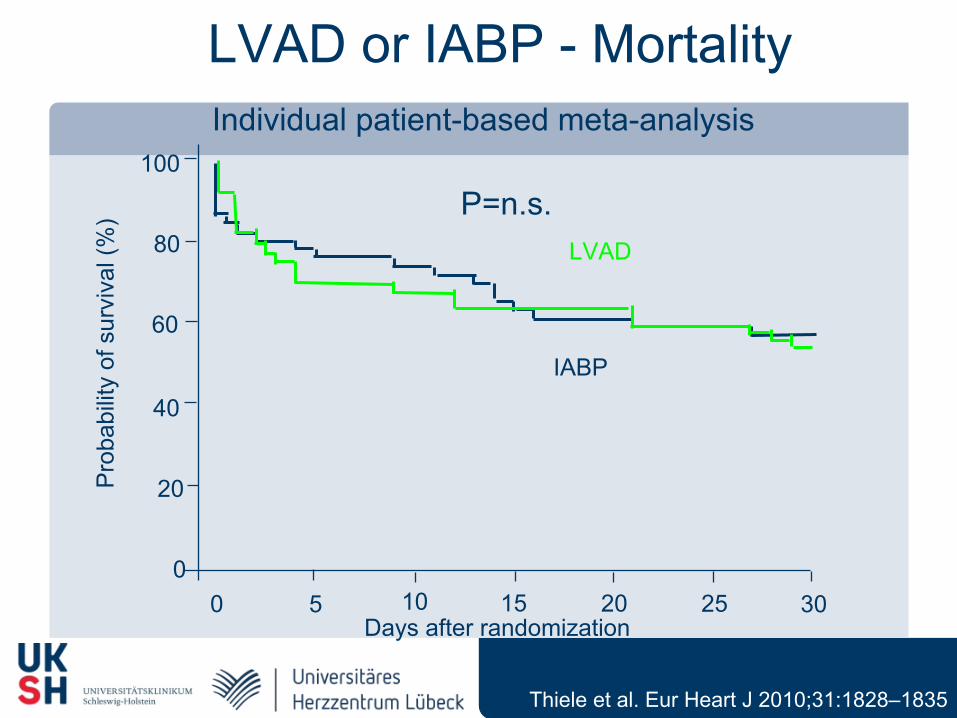
LVAD or IABP - MortalityIndividual patient-based meta-analysis
0 5 10 15 20 25 300
20
40
60
80
100
Pro
babi
lity
of s
urvi
val (
%)
Days after randomization
IABP
LVAD
P=n.s.
Thiele et al. Eur Heart J 2010;31:1828–1835
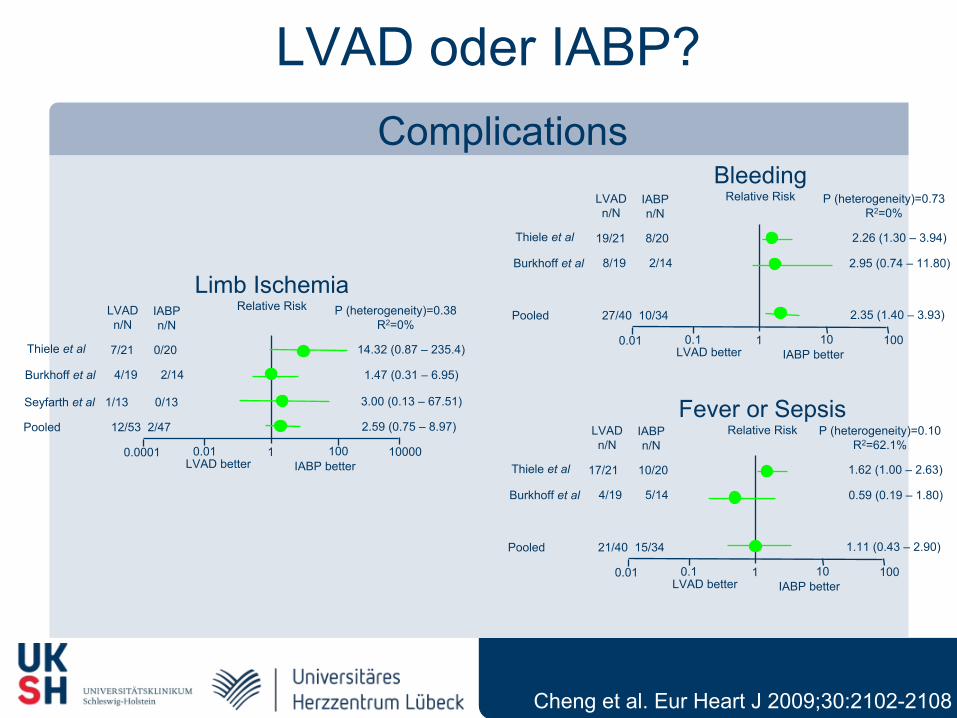
LVAD oder IABP?Complications
Cheng et al. Eur Heart J 2009;30:2102-2108
LVADn/N
IABPn/N
Limb IschemiaRelative Risk P (heterogeneity)=0.38
R2=0%
Thiele et al
Burkhoff et al
Seyfarth et al
Pooled
0.0001 0.01 1 100 10000IABP betterLVAD better
14.32 (0.87 – 235.4)
1.47 (0.31 – 6.95)
3.00 (0.13 – 67.51)
2.59 (0.75 – 8.97)
7/21 0/20
4/19 2/14
1/13 0/13
12/53 2/47
LVADn/N
IABPn/N
BleedingRelative Risk P (heterogeneity)=0.73
R2=0%
Thiele et al
Burkhoff et al
Pooled
0.01 0.1 1 10 100IABP betterLVAD better
2.26 (1.30 – 3.94)
2.95 (0.74 – 11.80)
2.35 (1.40 – 3.93)
19/21 8/20
8/19 2/14
27/40 10/34
LVADn/N
IABPn/N
Fever or SepsisRelative Risk P (heterogeneity)=0.10
R2=62.1%
Thiele et al
Burkhoff et al
Pooled
0.01 0.1 1 10 100IABP betterLVAD better
1.62 (1.00 – 2.63)
0.59 (0.19 – 1.80)
1.11 (0.43 – 2.90)
17/21 10/20
4/19 5/14
21/40 15/34
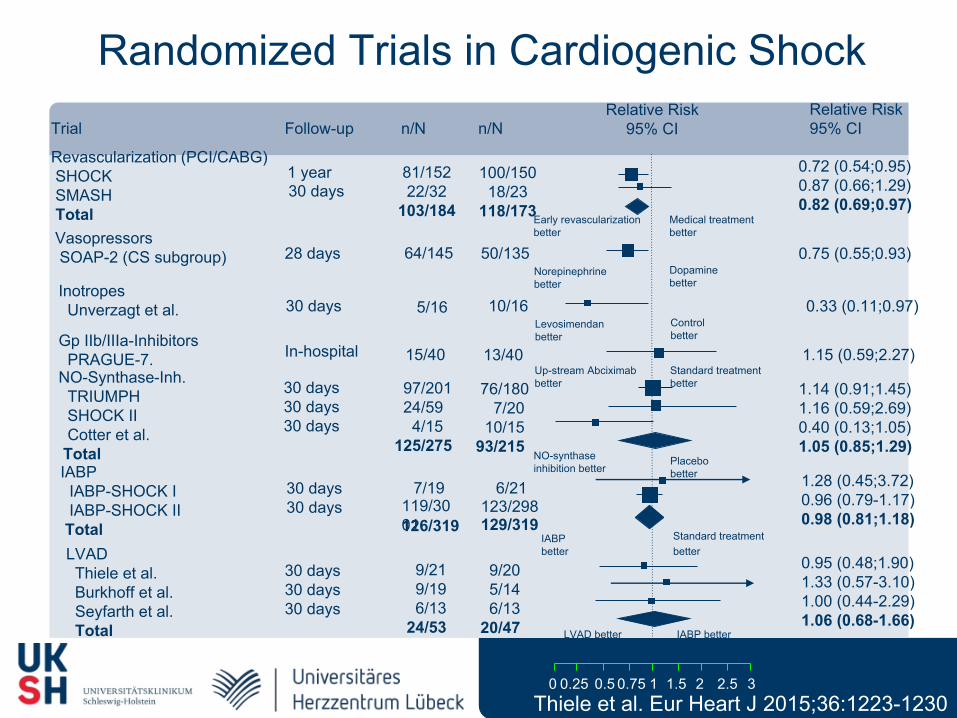
Trial n/N n/NRelative Risk
95% CIRelative Risk95% CI
0 0.5 1 2 3
Randomized Trials in Cardiogenic ShockFollow-up
Revascularization (PCI/CABG) SHOCK SMASH Total
81/152 22/32103/184
100/150 18/23118/173
1 year30 days
Early revascularization better
Medical treatment better
0.75 1.5 2.50.25
0.72 (0.54;0.95)0.87 (0.66;1.29)0.82 (0.69;0.97)
0.75 (0.55;0.93)64/145 50/13528 daysNorepinephrinebetter
Dopamine better
Vasopressors SOAP-2 (CS subgroup)
0.33 (0.11;0.97)5/16 10/1630 daysLevosimendanbetter
Controlbetter
Inotropes Unverzagt et al.
Gp IIb/IIIa-Inhibitors PRAGUE-7. In-hospital 15/40 13/40 1.15 (0.59;2.27)
Up-stream Abciximabbetter
Standard treatmentbetter
30 days30 days
7/19 6/21
IABPbetter
Standard treatmentbetter
1.28 (0.45;3.72)0.96 (0.79-1.17)0.98 (0.81;1.18)
119/3001
123/298126/319 129/319
IABP IABP-SHOCK I IABP-SHOCK II Total
30 days30 days30 days
97/201 24/59 4/15125/275
76/180 7/20 10/1593/215
1.14 (0.91;1.45)1.16 (0.59;2.69)0.40 (0.13;1.05)1.05 (0.85;1.29)
NO-synthase inhibition better
Placebobetter
NO-Synthase-Inh. TRIUMPH SHOCK II Cotter et al. Total
30 days30 days30 days
9/21 9/19 6/1324/53
9/20 5/14 6/1320/47
0.95 (0.48;1.90)1.33 (0.57-3.10)1.00 (0.44-2.29)1.06 (0.68-1.66)
IABP better
LVAD Thiele et al. Burkhoff et al. Seyfarth et al. Total LVAD better
Thiele et al. Eur Heart J 2015;36:1223-1230
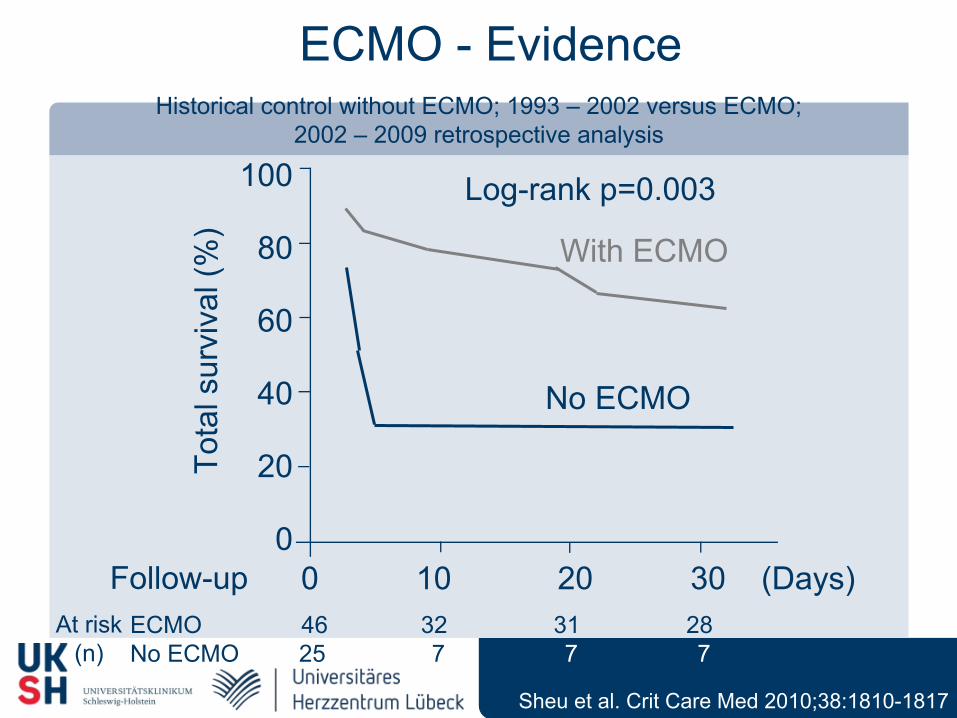
Sheu et al. Crit Care Med 2010;38:1810-1817
ECMO - EvidenceHistorical control without ECMO; 1993 – 2002 versus ECMO;
2002 – 2009 retrospective analysis
Log-rank p=0.003
0 10 20 30 (Days)
100
80
60
40
20
0Follow-up
At risk(n)
ECMO 46 32 31 28No ECMO 25 7 7 7
Tota
l sur
viva
l (%
)With ECMO
No ECMO
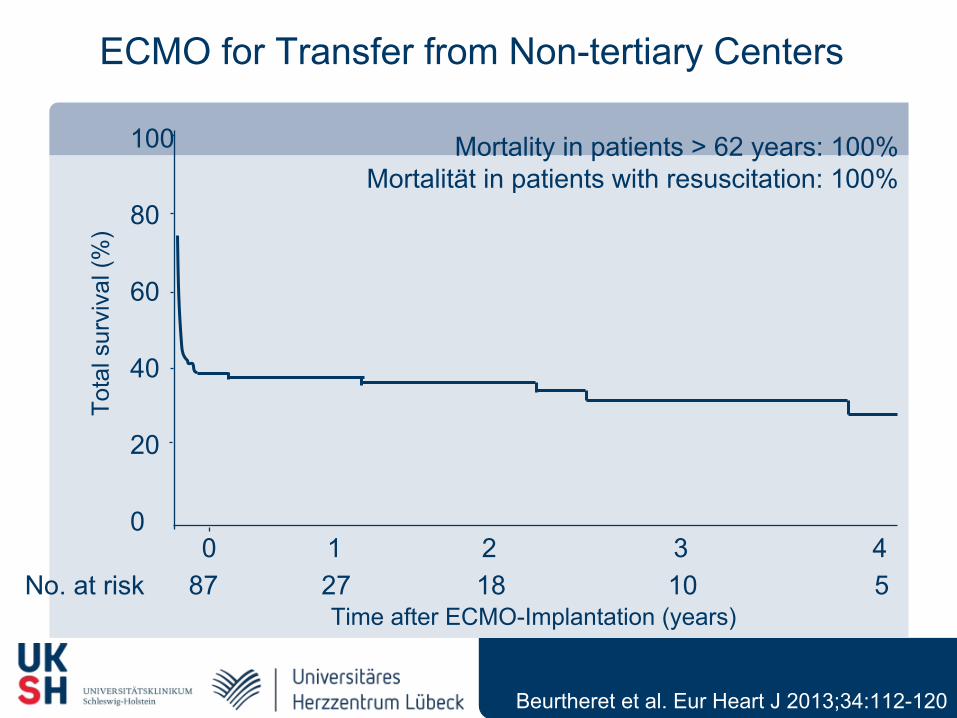
Time after ECMO-Implantation (years)
Tota
l sur
viva
l (%
)
0 1 2 3 4
100
80
60
40
20
0
No. at risk 87 27 18 10 5
Beurtheret et al. Eur Heart J 2013;34:112-120
ECMO for Transfer from Non-tertiary Centers
Mortality in patients > 62 years: 100%Mortalität in patients with resuscitation: 100%
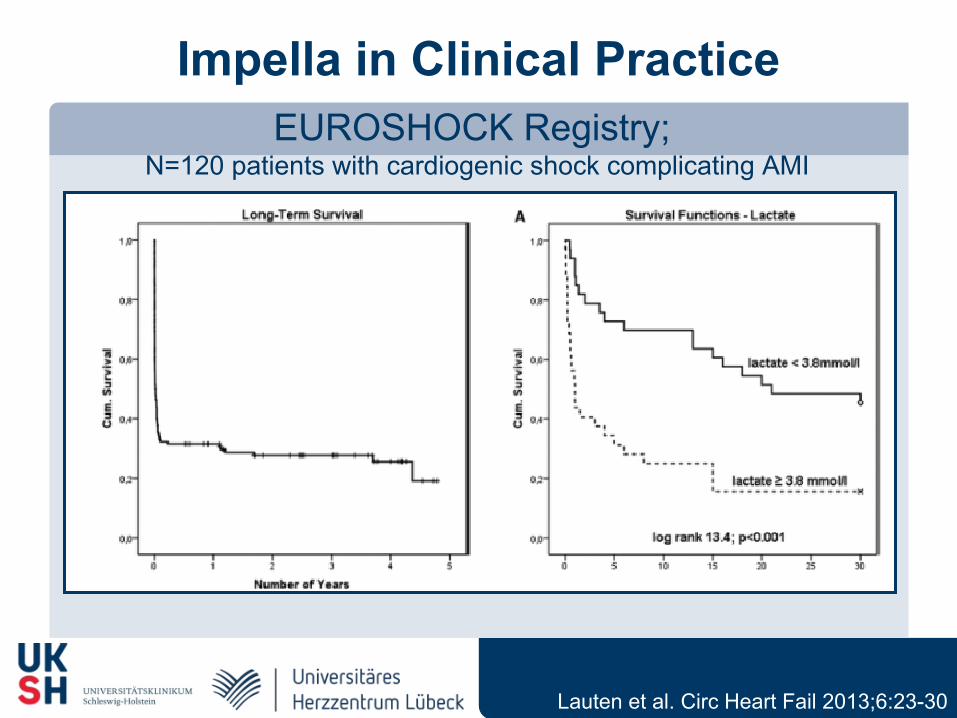
Impella in Clinical PracticeEUROSHOCK Registry;
N=120 patients with cardiogenic shock complicating AMI
Lauten et al. Circ Heart Fail 2013;6:23-30
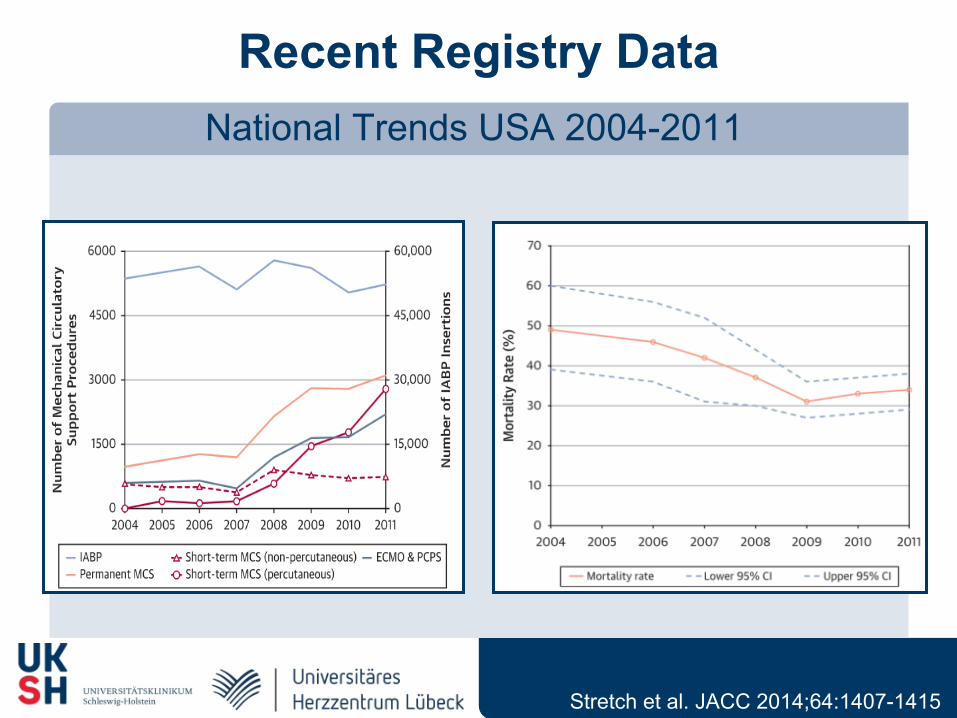
Recent Registry DataNational Trends USA 2004-2011
Stretch et al. JACC 2014;64:1407-1415
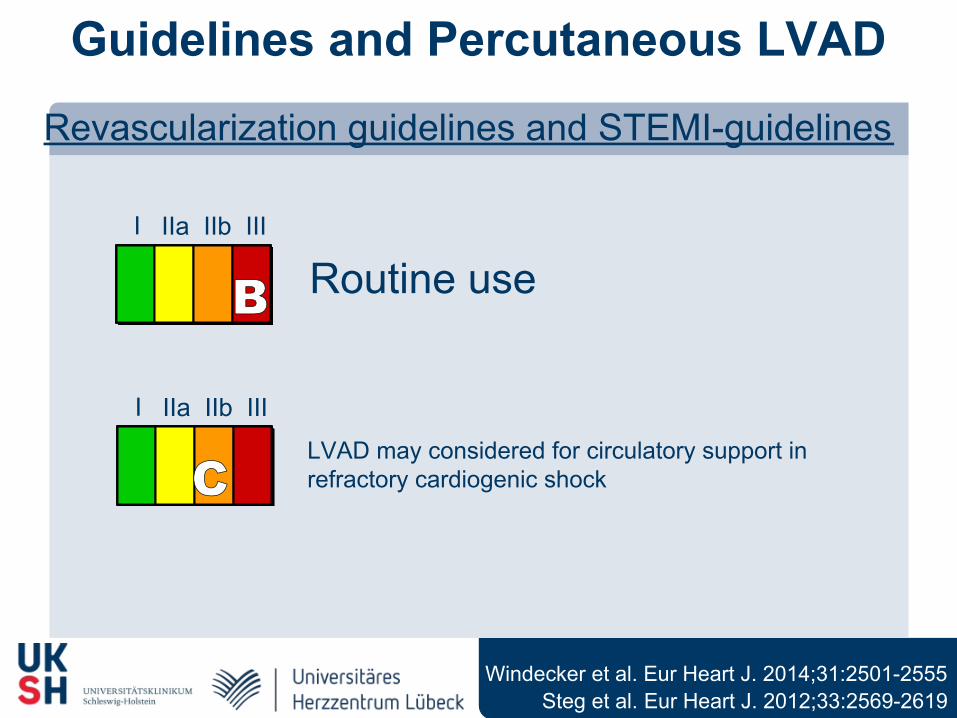
Guidelines and Percutaneous LVAD
Revascularization guidelines and STEMI-guidelines
Steg et al. Eur Heart J. 2012;33:2569-2619
I IIa IIb III
CLVAD may considered for circulatory support in refractory cardiogenic shock
I IIa IIb III
B Routine use
Windecker et al. Eur Heart J. 2014;31:2501-2555
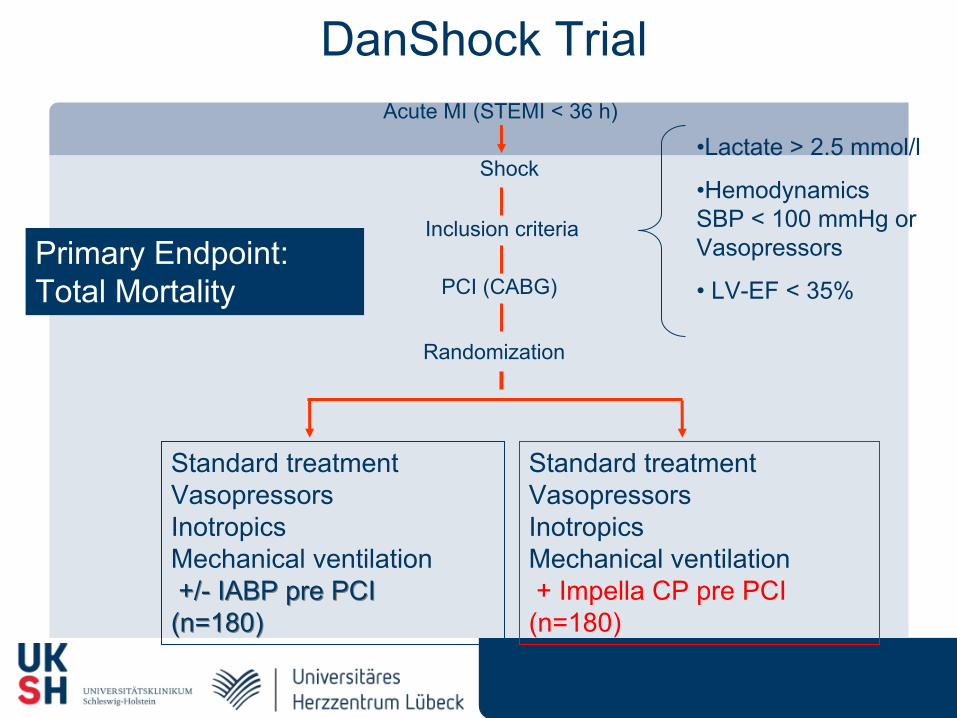
•Lactate > 2.5 mmol/l
•Hemodynamics SBP < 100 mmHg or Vasopressors
• LV-EF < 35%
Standard treatment Vasopressors Inotropics Mechanical ventilation +/- IABP pre PCI +/- IABP pre PCI (n=180)(n=180)
Acute MI (STEMI < 36 h)
Shock
PCI (CABG)
Inclusion criteria
Randomization
Standard treatment Vasopressors Inotropics Mechanical ventilation + Impella CP pre PCI (n=180)
DanShock Trial
Primary Endpoint:Total Mortality
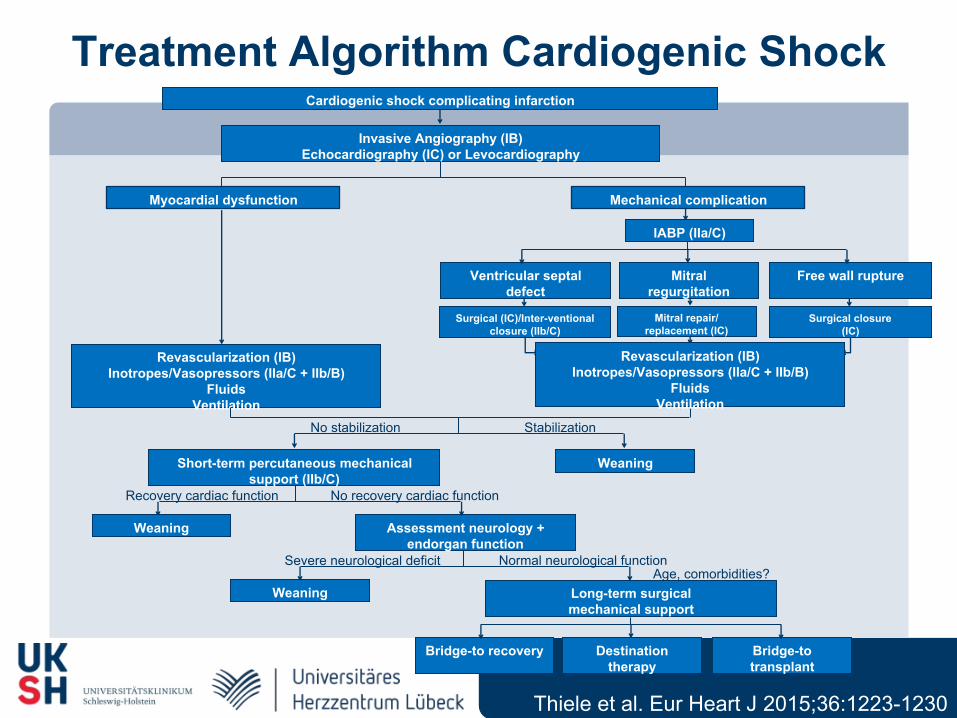
Treatment Algorithm Cardiogenic Shock
No stabilization
Short-term percutaneous mechanical support (IIb/C)
Revascularization (IB)Inotropes/Vasopressors (IIa/C + IIb/B)
FluidsVentilation
Weaning
Stabilization
Assessment neurology +endorgan function
Age, comorbidities?
Cardiogenic shock complicating infarction
Invasive Angiography (IB)Echocardiography (IC) or Levocardiography
Myocardial dysfunction
Recovery cardiac function
Mechanical complication
No recovery cardiac function
Weaning
Severe neurological deficit Normal neurological function
Weaning Long-term surgical mechanical support
Bridge-to recovery Bridge-to transplant
Destination therapy
Ventricular septal defect
Free wall ruptureMitral regurgitation
Mitral repair/replacement (IC)
Surgical closure(IC)
Surgical (IC)/Inter-ventional closure (IIb/C)
IABP (IIa/C)
Revascularization (IB)Inotropes/Vasopressors (IIa/C + IIb/B)
FluidsVentilation
Thiele et al. Eur Heart J 2015;36:1223-1230
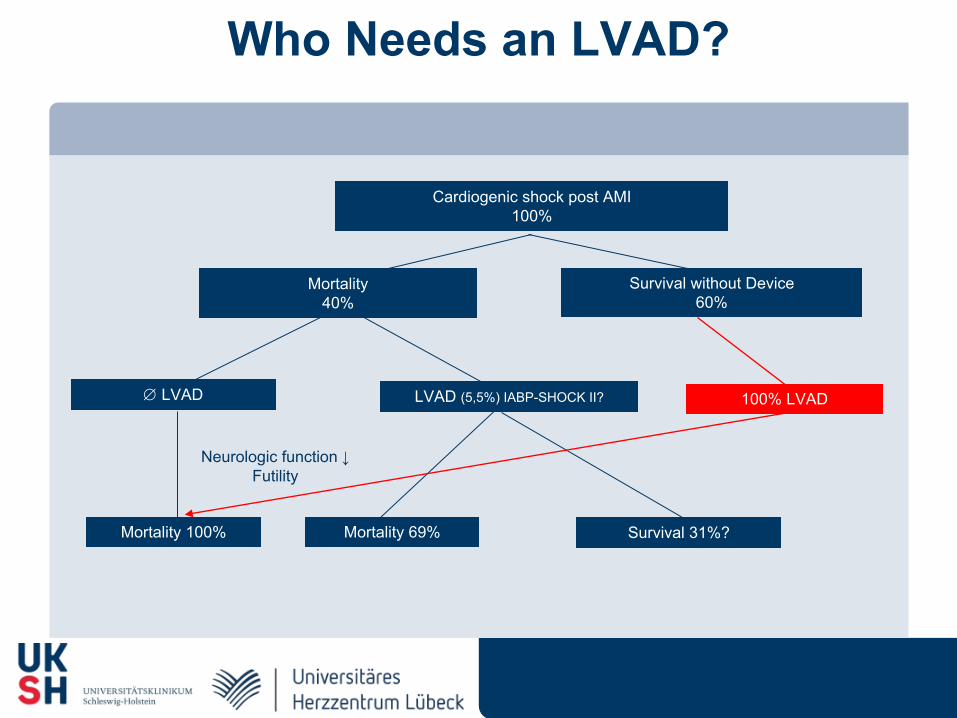
Who Needs an LVAD?
Mortality40%
Cardiogenic shock post AMI100%
Survival without Device 60%
LVAD
Mortality 100%
Neurologic function ↓Futility
LVAD (5,5%) IABP-SHOCK II?
Survival 31%?Mortality 69%
100% LVAD
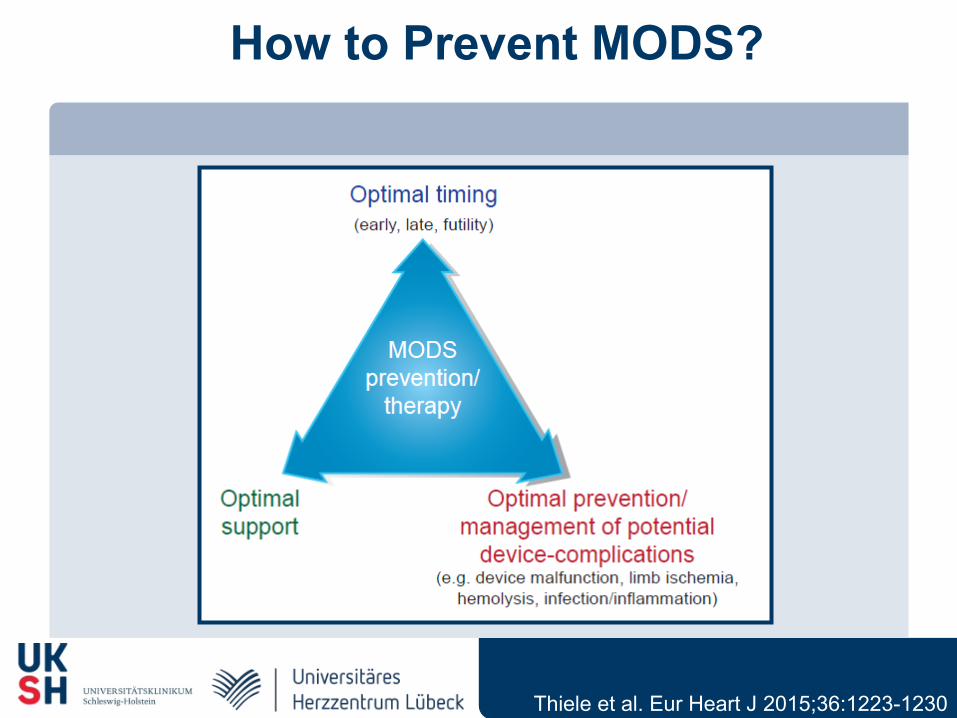
How to Prevent MODS?
Thiele et al. Eur Heart J 2015;36:1223-1230
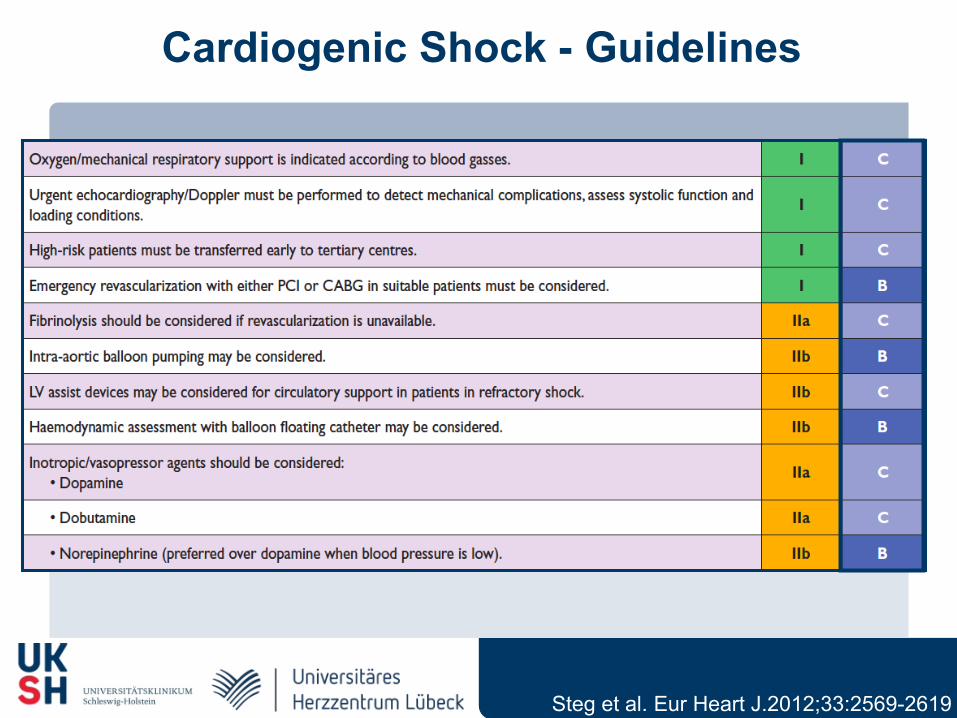
Cardiogenic Shock - Guidelines
Steg et al. Eur Heart J.2012;33:2569-2619
N P
atie
nts
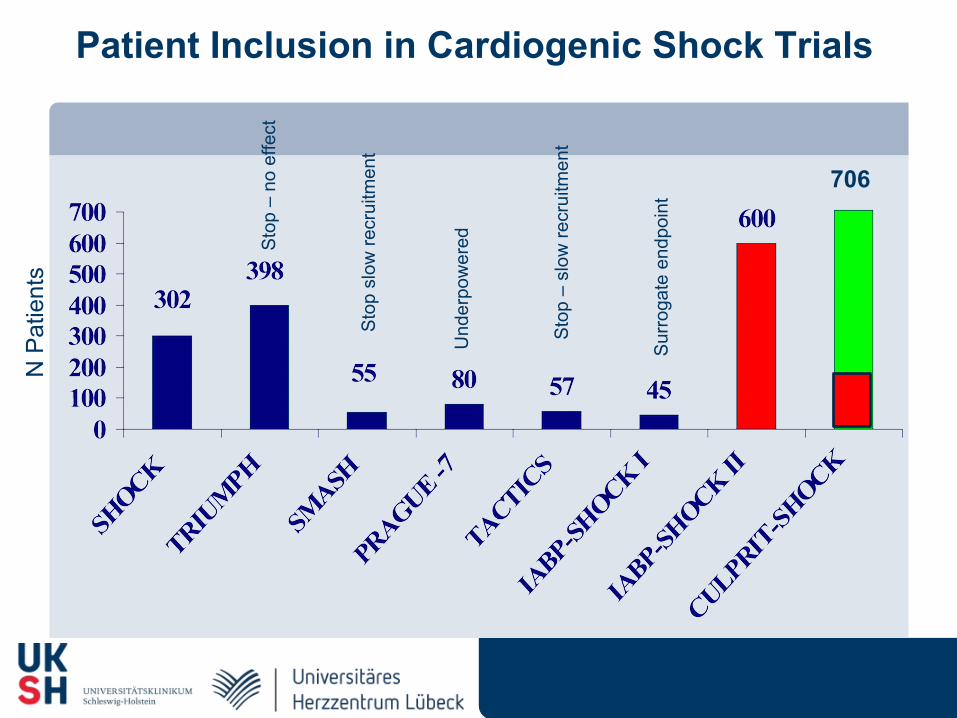
Patient Inclusion in Cardiogenic Shock Trials
Sto
p –
no e
ffect
Sto
p sl
ow re
crui
tmen
t
Und
erpo
wer
ed
Sur
roga
te e
ndpo
int
706
Sto
p –
slow
recr
uitm
ent
Related Documents











