Peptic Ulcer Disease Done by : PROF/GOUDA ELLABBAN

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
Peptic Ulcer Disease
Done by :
PROF/GOUDA ELLABBAN
What is a peptic ulcer?
A peptic ulcer is a hole in the gut lining of Stomach (gastric ulcer) Duodenum (duodenal ulcer) Esophagus (esophageal ulcer)

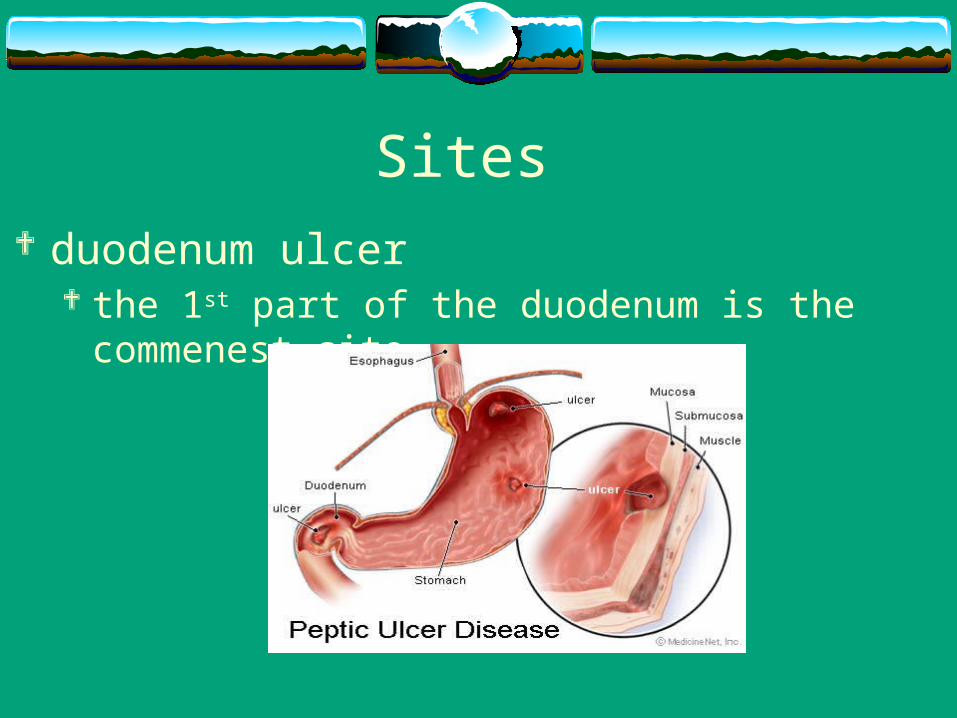
Sites duodenum ulcer
the 1st part of the duodenum is the commenest site
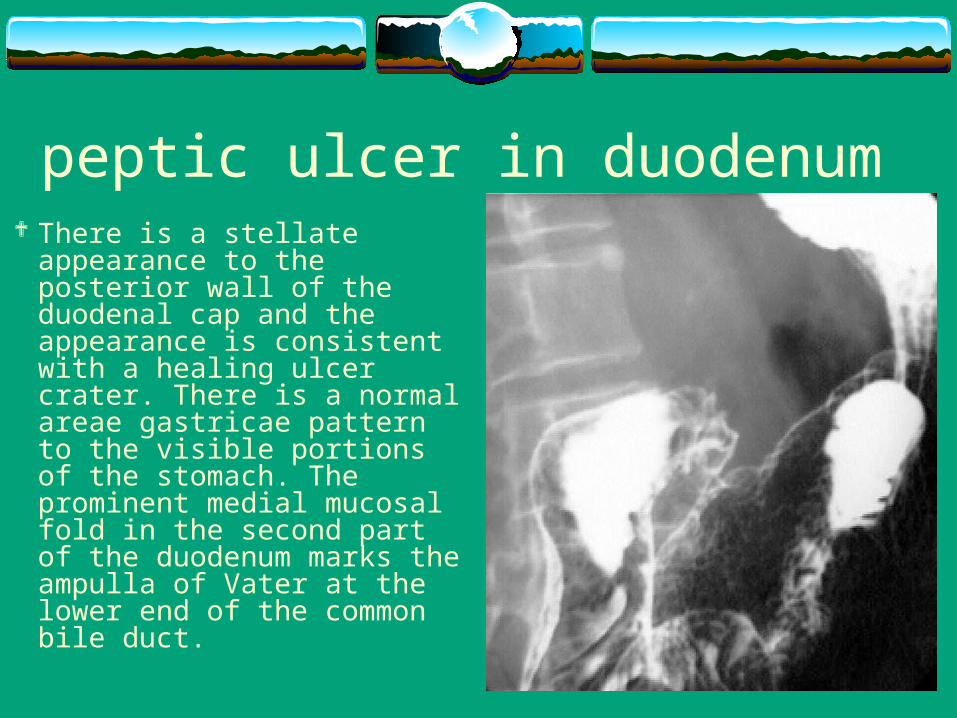
peptic ulcer in duodenum There is a stellate appearance to
the posterior wall of the duodenal cap and the appearance is consistent with a healing ulcer crater. There is a normal areae gastricae pattern to the visible portions of the stomach. The prominent medial mucosal fold in the second part of the duodenum marks the ampulla of Vater at the lower end of the common bile duct.
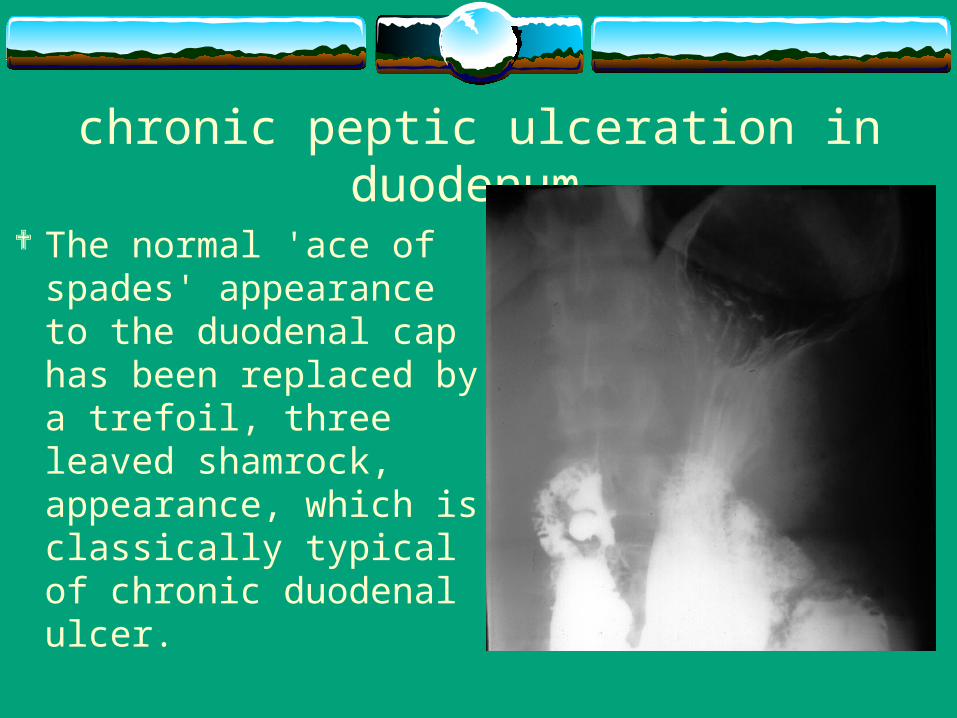
chronic peptic ulceration in duodenum
The normal 'ace of spades' appearance to the duodenal cap has been replaced by a trefoil, three leaved shamrock, appearance, which is classically typical of chronic duodenal ulcer.
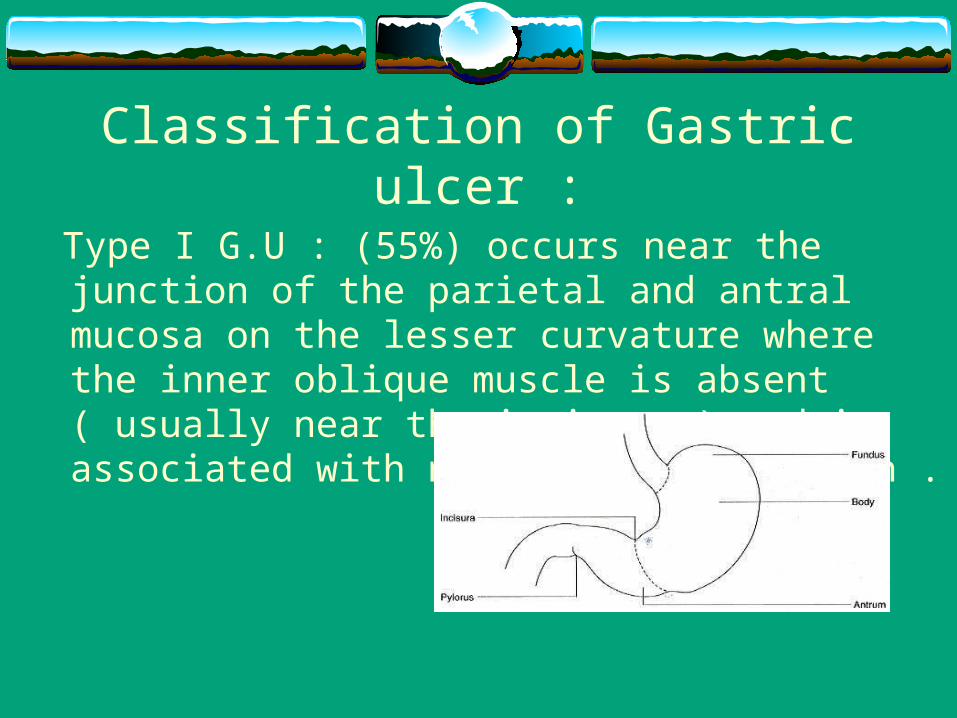
Classification of Gastric ulcer :
Type I G.U : (55%) occurs near the junction of the parietal and antral mucosa on the lesser curvature where the inner oblique muscle is absent ( usually near the incisura ) and is associated with normal acid secretion .
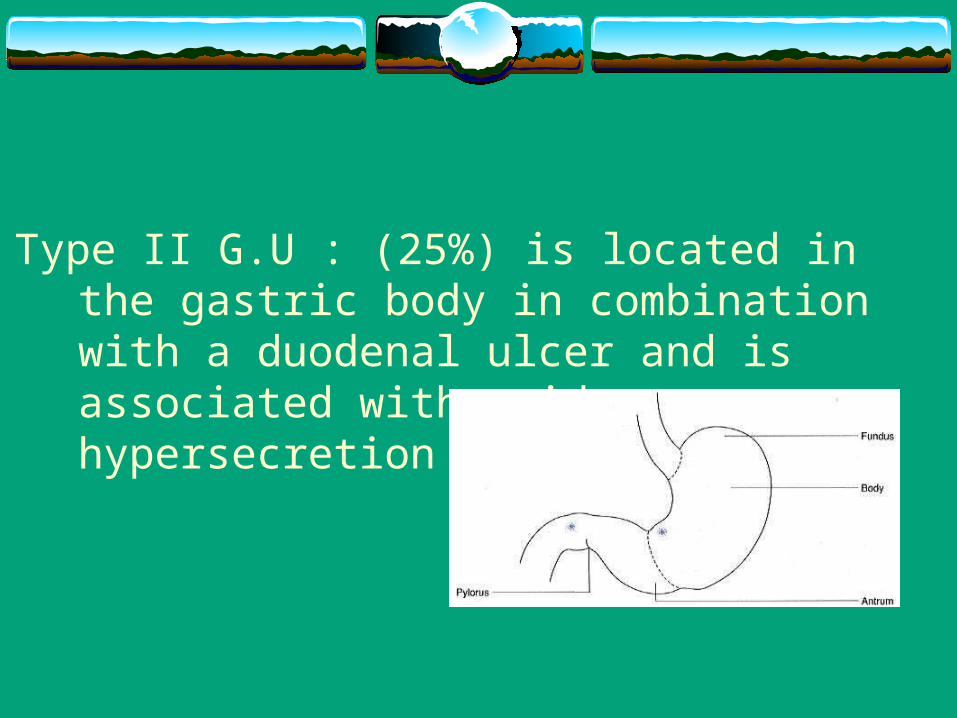
Type II G.U : (25%) is located in the gastric body in combination with a duodenal ulcer and is associated with acid hypersecretion .
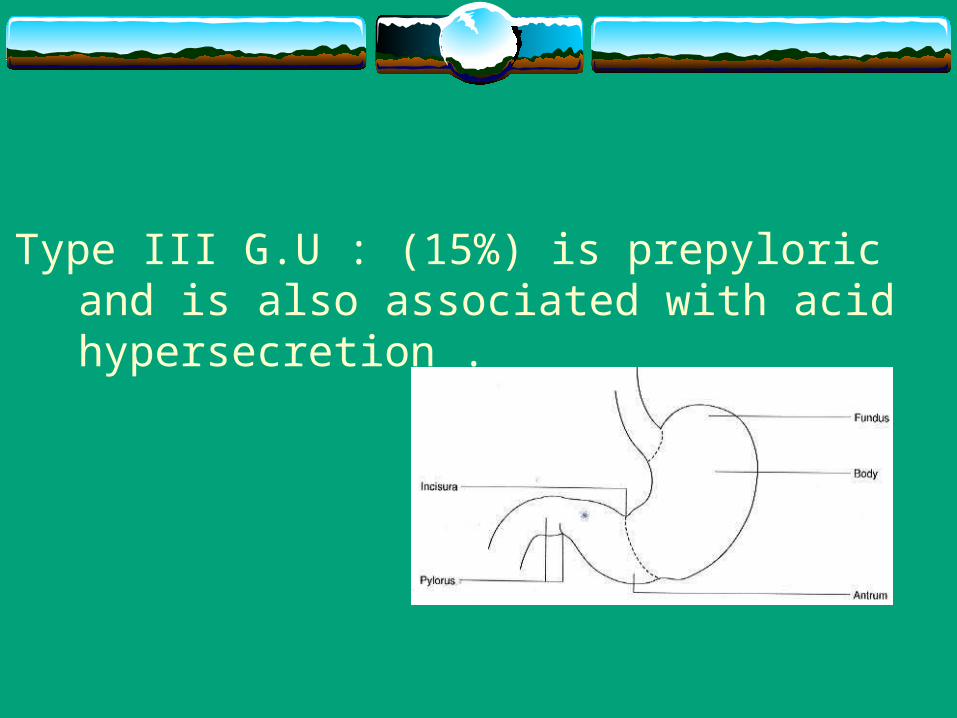
Type III G.U : (15%) is prepyloric and is also associated with acid hypersecretion .
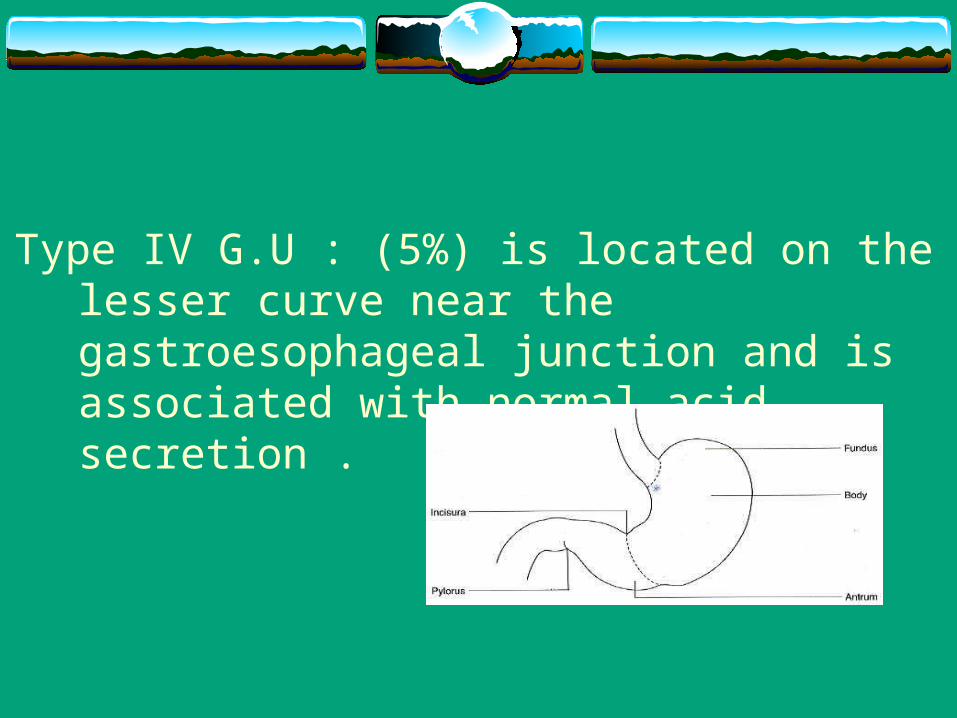
Type IV G.U : (5%) is located on the lesser curve near the gastroesophageal junction and is associated with normal acid secretion .
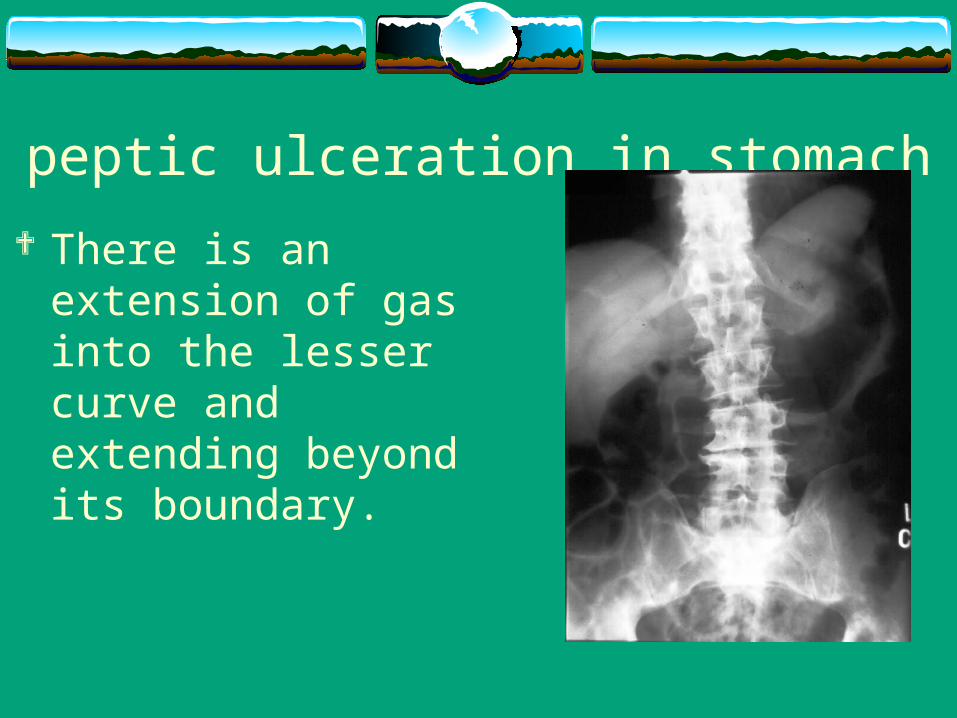
peptic ulceration in stomach There is an extension of
gas into the lesser curve and extending beyond its boundary.
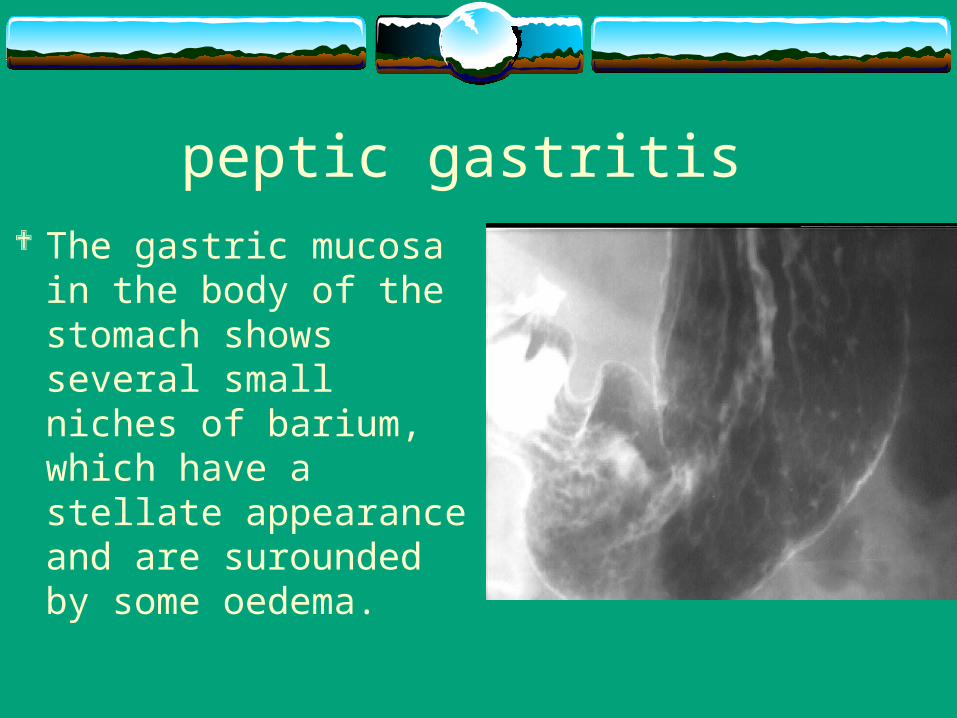
peptic gastritis The gastric mucosa in
the body of the stomach shows several small niches of barium, which have a stellate appearance and are surounded by some oedema.
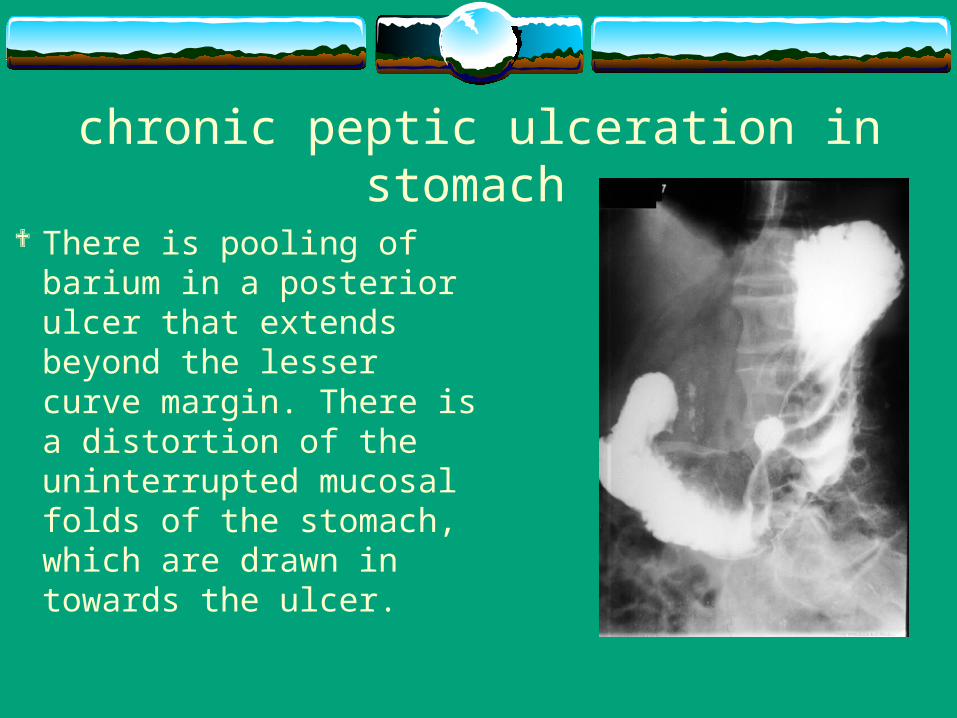
chronic peptic ulceration in stomach
There is pooling of barium in a posterior ulcer that extends beyond the lesser curve margin. There is a distortion of the uninterrupted mucosal folds of the stomach, which are drawn in towards the ulcer.
Causes Etiology of DU and GU is multifactorial . H. pylori gastritis is present in >80% of DU and >60% of
GU. Imbalance between aggressive factors (e.g. gastric acid,
pepsin, bile salts, pancreatic enzymes) and defensive factors maintaining mucosal integrity (e.g. mucus, bicarbonate, blood flow, prostaglandins, cell turnover) which may relate to H. pylori infection
Causes (cont. ) Ulcerogenic drugs (e.g. NSAIDs) Zollinger-Ellison syndrome Other hyper secretory syndromes Retained gastric antrum
H. pylori gram –ve spirochetal bacteriam found in the antral and duodenal macosa Mechanism:
it is urease +ve split urea and lead to formation of ammonia alkaline media around the bacteria 2ry high acid ULCER
also it affect the cells through cytotoxin
Diagnosis
1. histology : Spiral bacteria rod adjacent to gastric epithelium
2. direct culture: only done when an antibiotic resistant organism is
suspected
3. CLO ( urease ) test :4. serology :
High anti – H. pylori
A burning pain in abdomin is the most common symptom
Abdominal pain nausea vomiting weight loss fatigue heartburn chest pain vomiting blood bloody or dark tarry stools
Clinical presentation
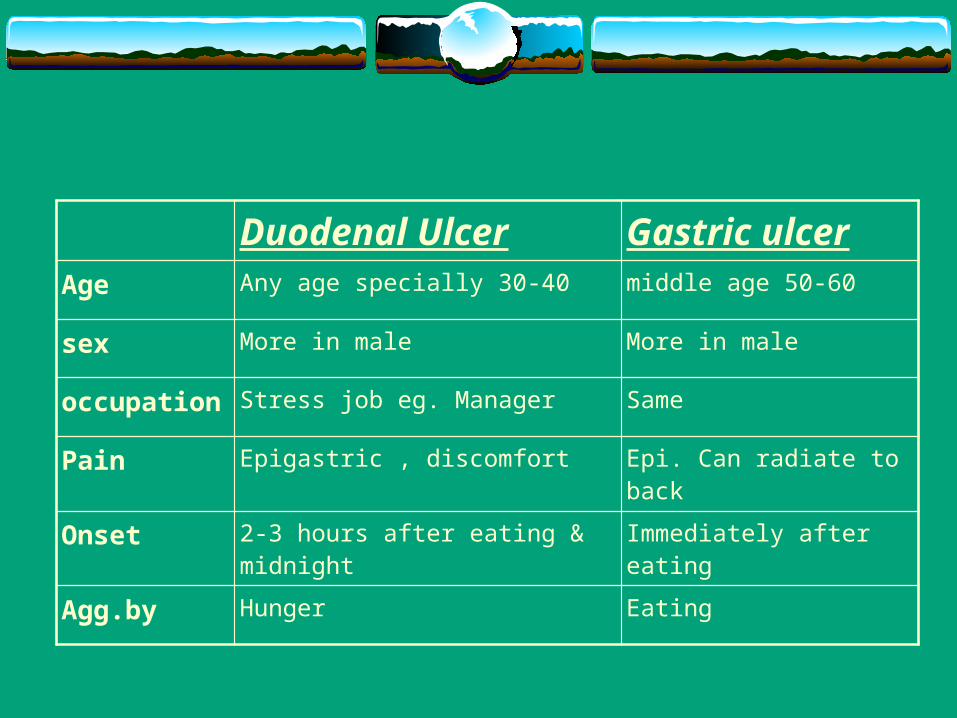
Duodenal Ulcer Gastric ulcerAge Any age specially 30-40 middle age 50-60
sex More in male More in male
occupation Stress job eg. Manager Same
Pain Epigastric , discomfort Epi. Can radiate to back
Onset 2-3 hours after eating & midnight Immediately after eating
Agg.by Hunger Eating
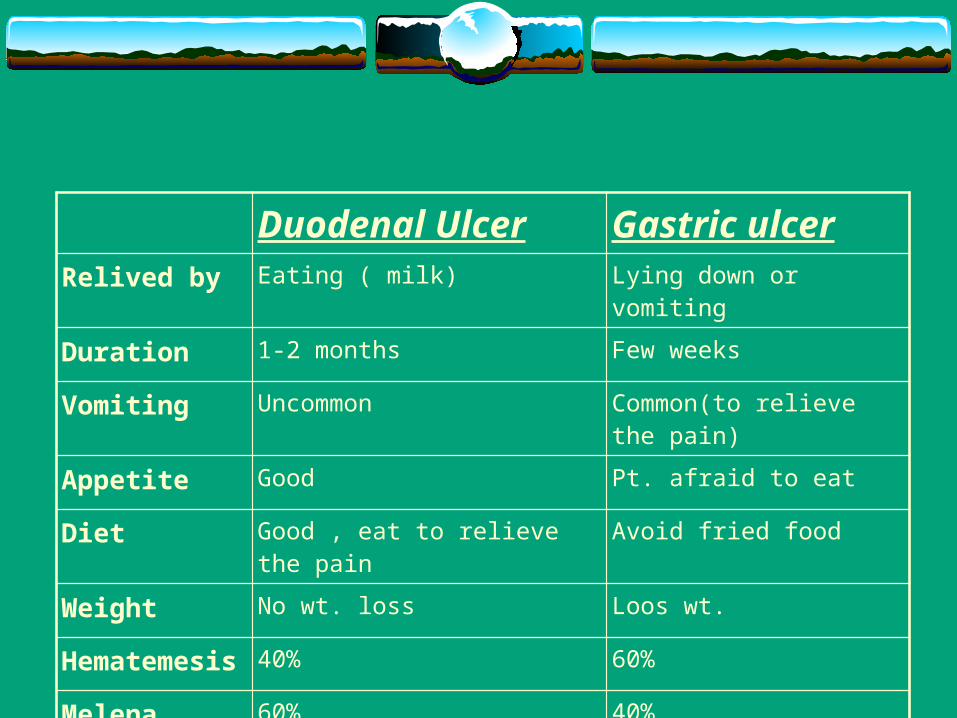
Duodenal Ulcer Gastric ulcerRelived by Eating ( milk) Lying down or vomiting
Duration 1-2 months Few weeks
Vomiting Uncommon Common(to relieve the pain)
Appetite Good Pt. afraid to eat
Diet Good , eat to relieve the pain Avoid fried food
Weight No wt. loss Loos wt.
Hematemesis 40% 60%
Melena 60% 40%
Risk Factors
Strongly associated Drugs (NSAIDs)
Family history Smoking
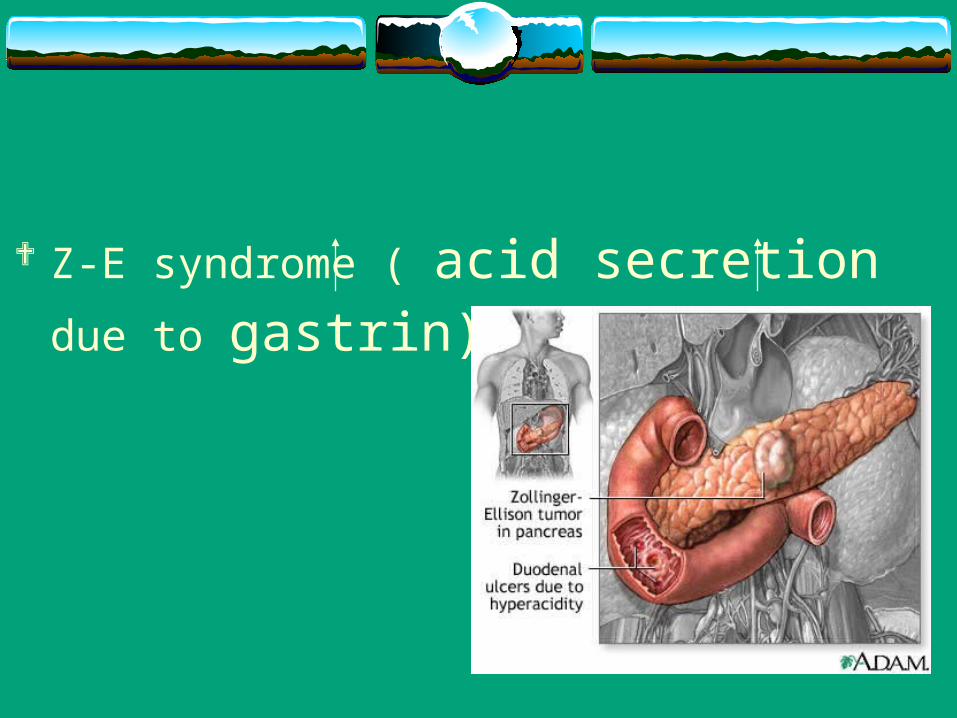
Z-E syndrome ( acid secretion due to gastrin)
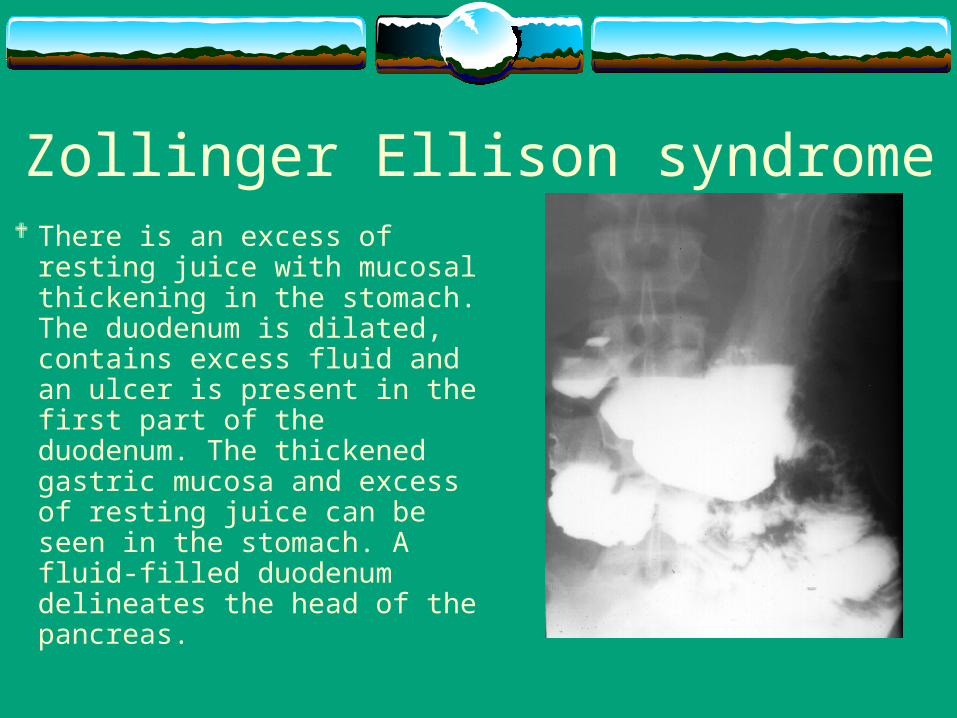
Zollinger Ellison syndrome There is an excess of resting juice
with mucosal thickening in the stomach. The duodenum is dilated, contains excess fluid and an ulcer is present in the first part of the duodenum. The thickened gastric mucosa and excess of resting juice can be seen in the stomach. A fluid-filled duodenum delineates the head of the pancreas.
Risk Factors (cont . )
Possibly associated Corticosteroid Blood group O Stress Lower socioeconomic status
COMLICATION :
Hemorrhage : Leading cause of death due to peptic ulcer disease Hypotension , hematemesis , melena bleeding duodenal ulcer : are usually located on
the posterior duodenal wall within 2 cm of the pylorus and typically erode into the gastroduodenal artery.
Perforation peptic ulcer : Sudden onset of severe abdominal pain Result in generalize peritonitis ( or localize
peritonitis when the perforation is walled off by adjacent viscera and structure ).
N.B: G.U. in posterior wall erode to pancreas G.U. in anterior wall erode to liver
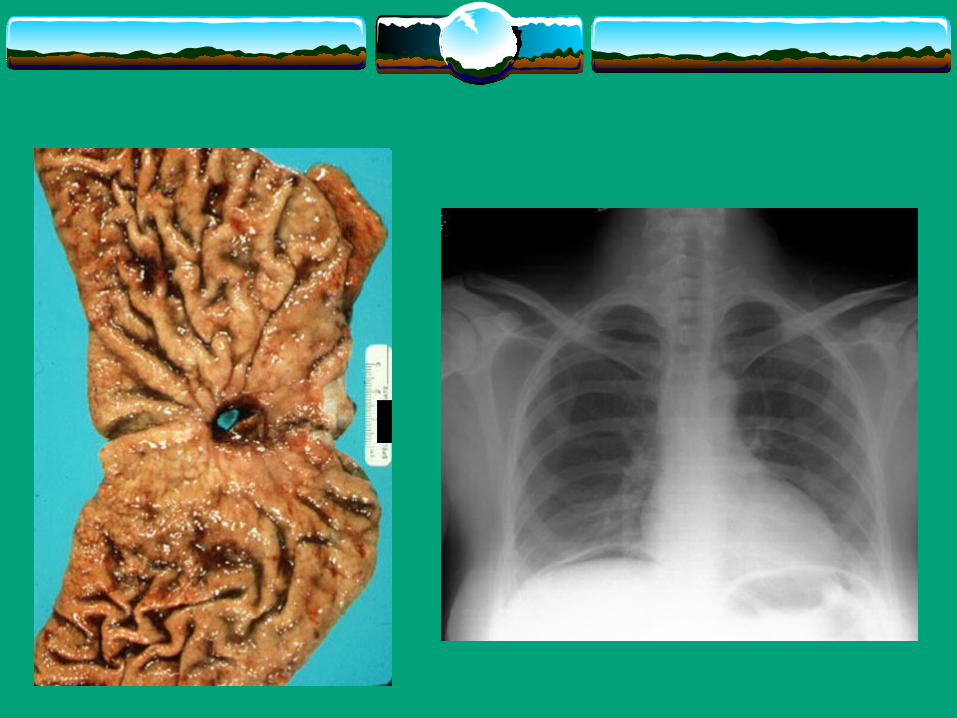
Perforation peptic ulcer : By examination : Low grade fever Tachycardia Abdominal wall rigidity Leukocytosis Subdiaphragmatic gas in X-ray
Gastric outlet obstruction Can occur as a chronic process due to fibrosis and
scarring of the pylorus and duodenum from chronic ulcer disease or as a consequence of acute inflammation superimposed on previous scarring of the gastric outlet .
Patient present with recurrent vomiting of poorly digested food, dehydration, and hypochloremic hypokalemic metabolic alkalosis .
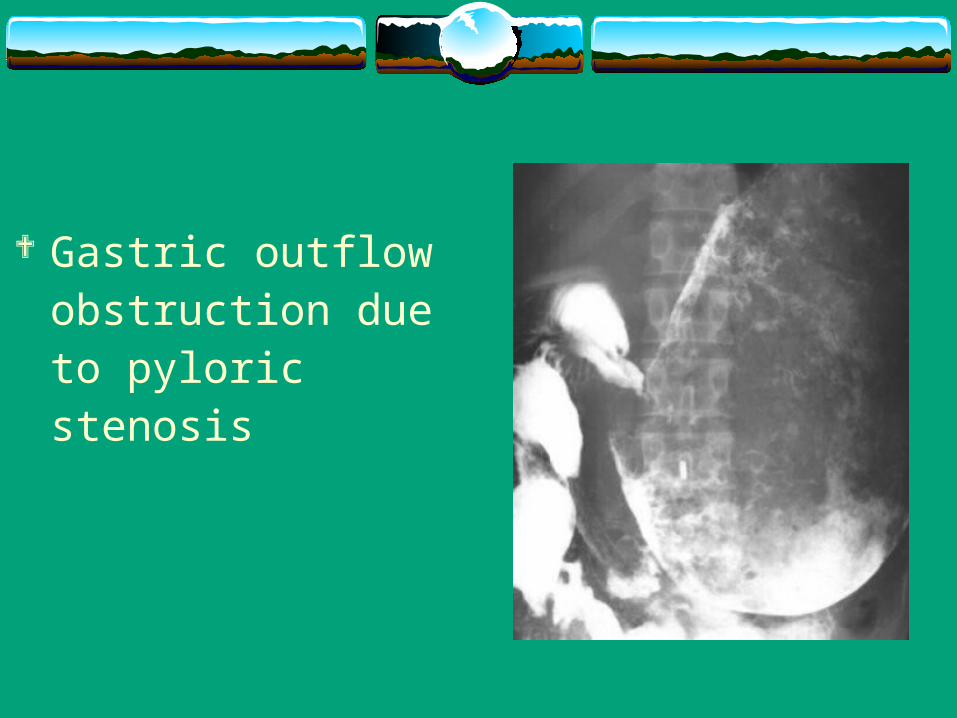
Gastric outflow obstruction due to pyloric stenosis
Differential Diagnosis Atrophic gastritis Cholecystitis Pancreatitis Reflex esophagitis
Investigation • Gastroduedenoscopy
Medical Management Goals
relieve symptoms promote mucosal healing by controlling gastric acid prevent or detect complications prevent recurrence by eradicating H. pylori
Management Program diet modification rest medications
Management: Medications Drug Therapy
Antacids H2-receptor blocking agents Anticholinergics Cytoprotective and antisecretory drugs Proton pump inhibitors Antibiotics
Role of Surgery in the Mangement of PUD
Surgery is mainstay for emergency tx of life-threatening complications of aggressive and advanced PUD
Fundamental goals of surgery permit ulcer healing prevent or treat ulcer complications address underlying ulcer diathesis
Indications for surgery in ulcer disease bleeding perforation obstruction Malignant change
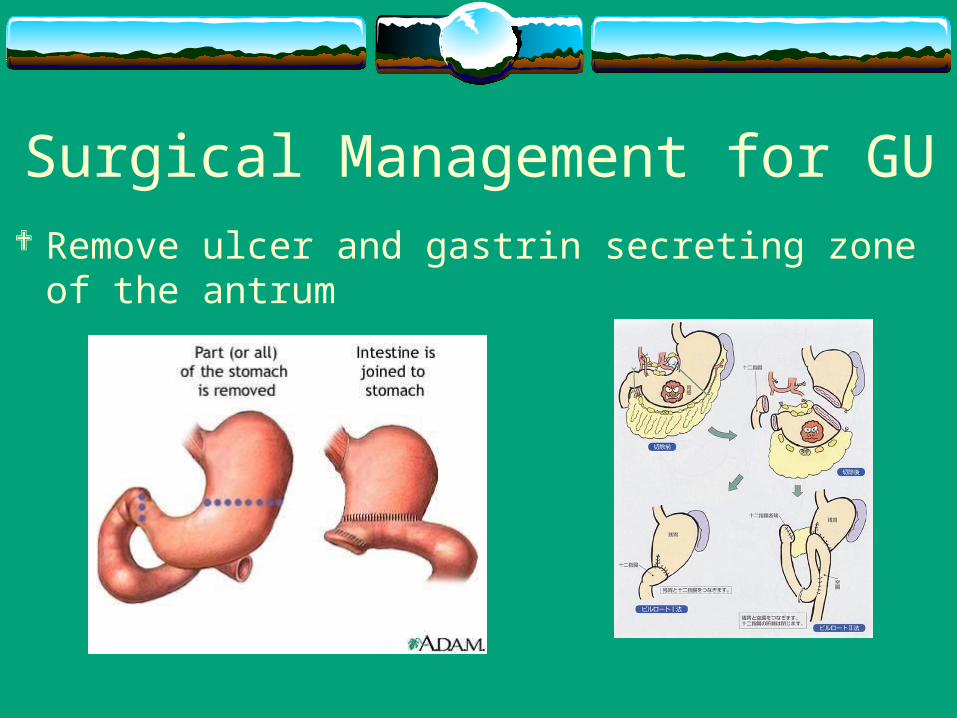
Surgical Management for GU Remove ulcer and gastrin secreting zone of the antrum
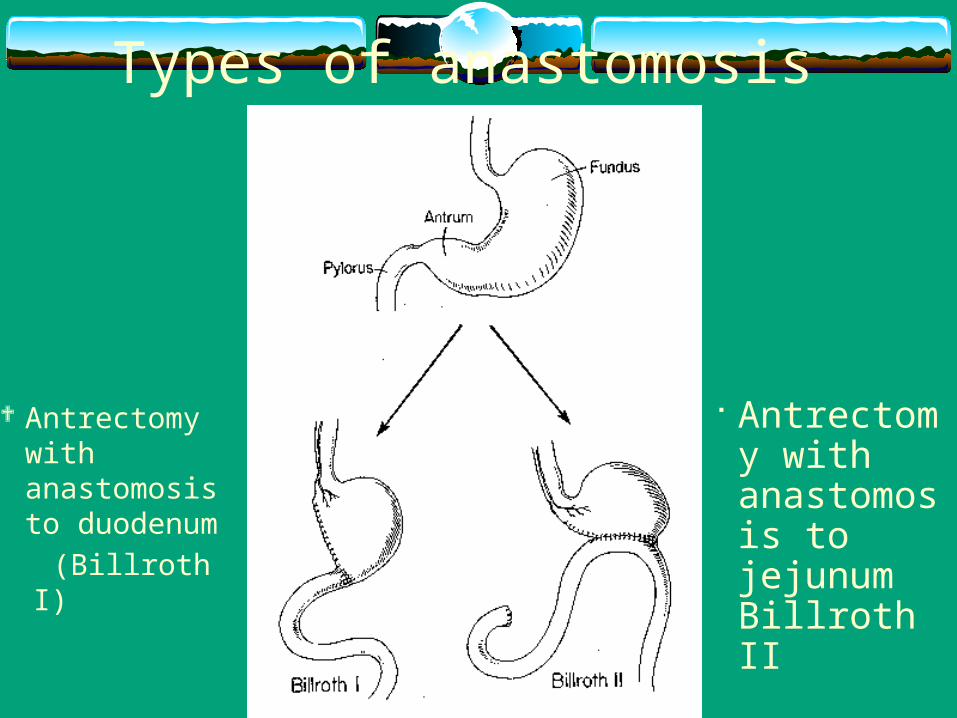
Types of anastomosis
Antrectomy with anastomosis to duodenum
(Billroth I)
Antrectomy with anastomosis to jejunum Billroth II
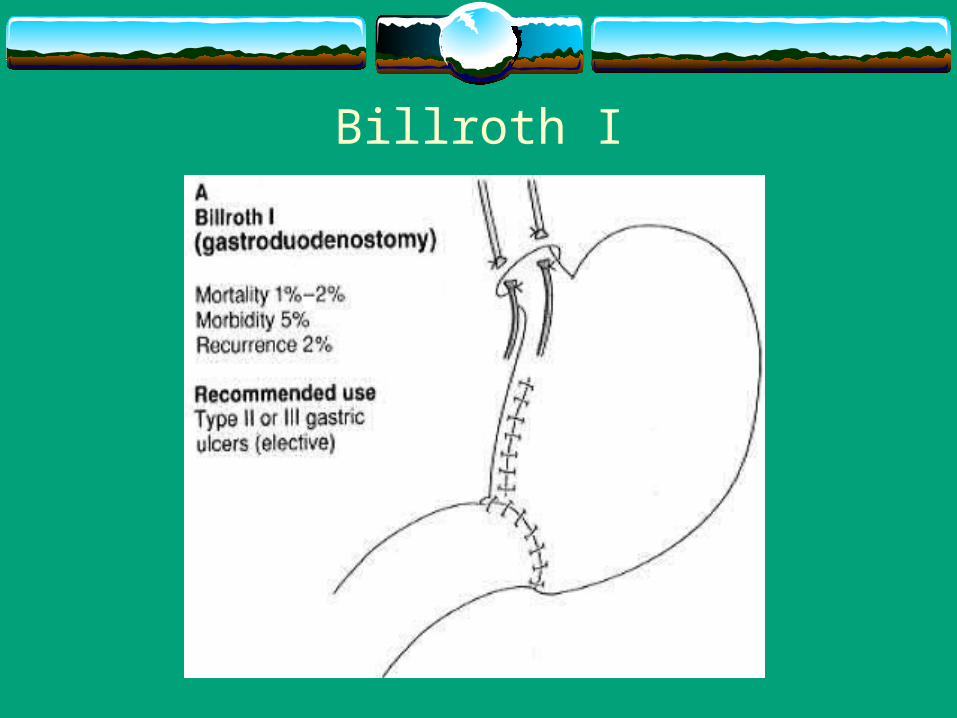
Billroth I
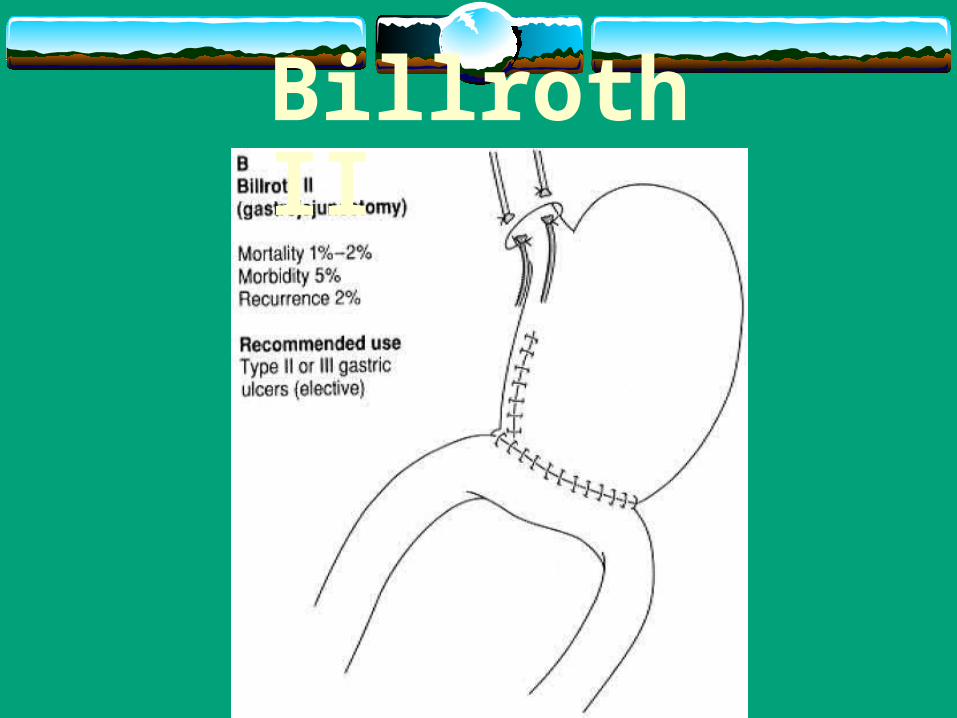
Billroth II
Complication of partial gastroctomy Immediate complication:
Bleeding :Bleeding following partial gastroctomy usually occuer frome
gastric side of anastomosis
Complication con. Early complications :
a) Anastomotic leak: which lead toi. Subphrenic abscessii. Pelvic abscess iii. Abdominal collection
b) Obstruction :i. Of afferent loopii. Of efferent loop
c) internal herniation
Complication con. Late complications :
1. Small stomach syndrome
2. Iron deficiency anemia
3. Dumping syndrom
4. Stomal ulcer
5. Stomach cancer
Surgical Management for DU• You can do one of the following procedures:
Truncal vagotomy with drainage High selective vagotomy Partial gastroctomy with G-J anastomosis Truncal vagotomy with antrectomy and G-J anastomosis
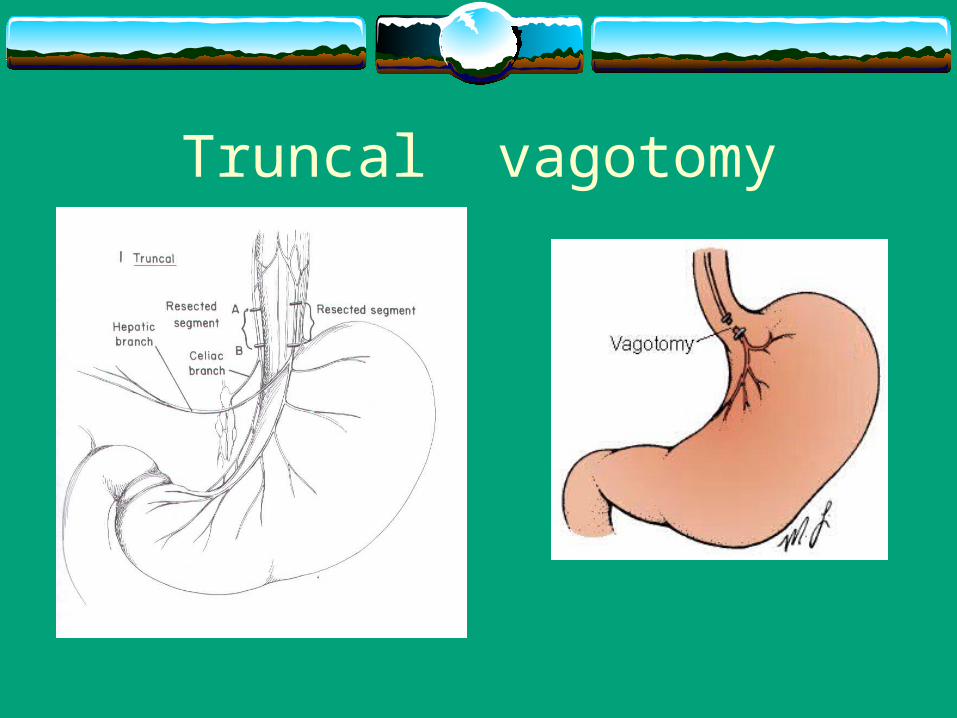
Truncal vagotomy
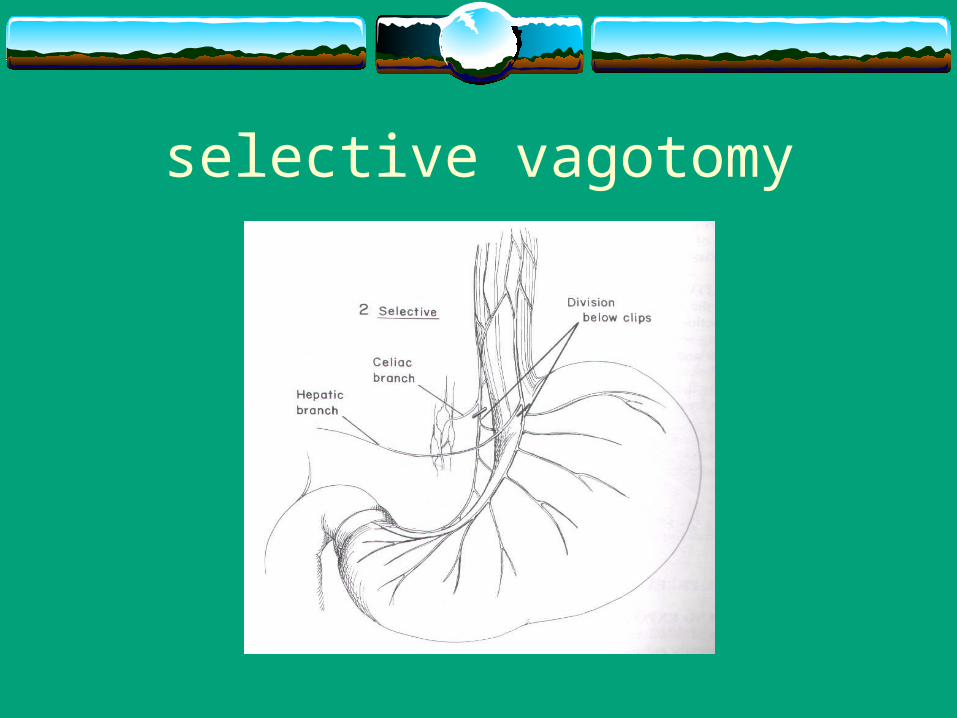
selective vagotomy
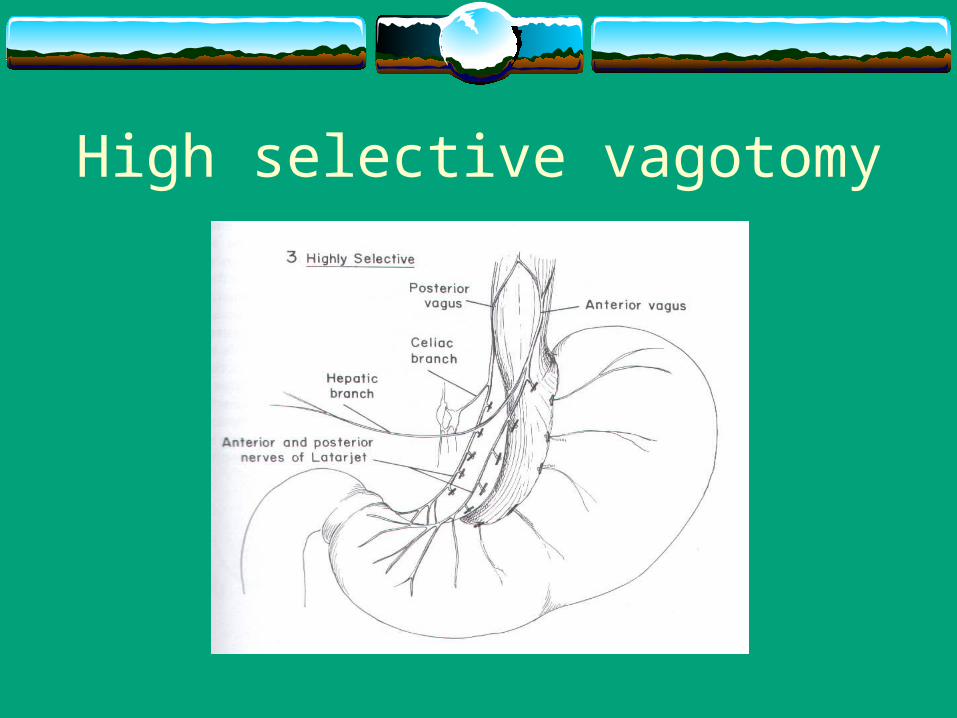
High selective vagotomy

Drainage Methods of drainage :
Pyloroplasty gastrojejunostomy
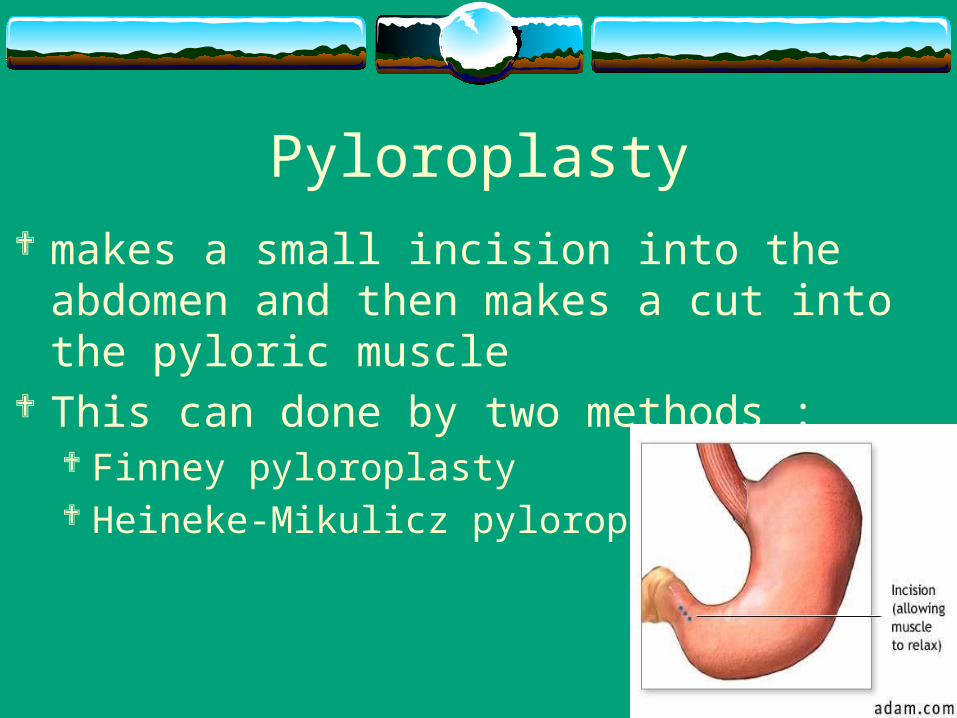
Pyloroplasty makes a small incision into the abdomen and then
makes a cut into the pyloric muscle This can done by two methods :
Finney pyloroplasty Heineke-Mikulicz pyloroplasty
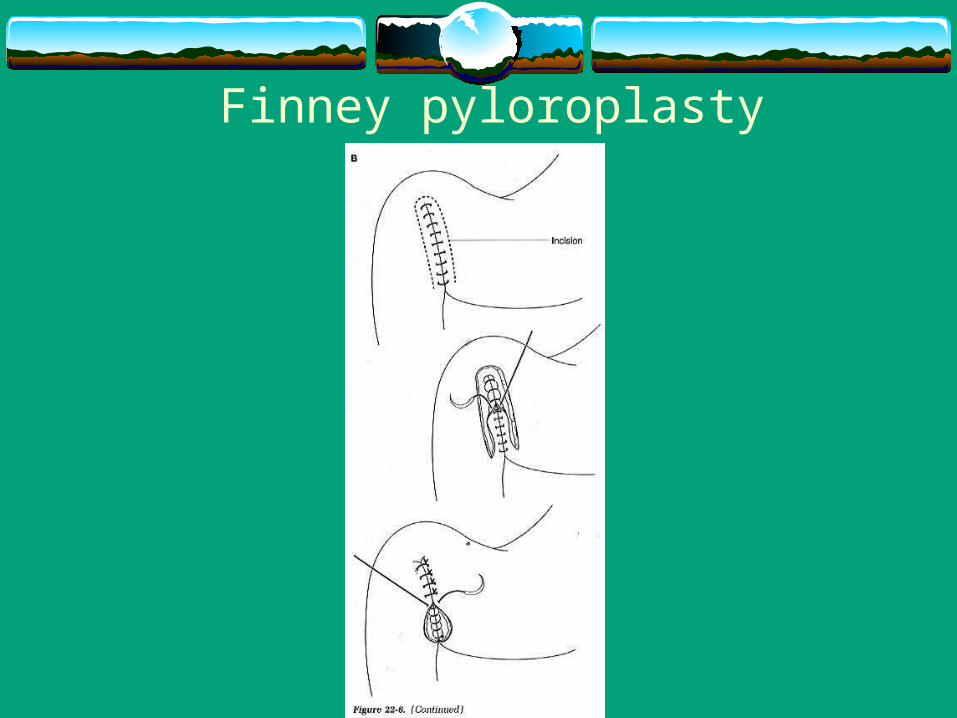
Finney pyloroplasty
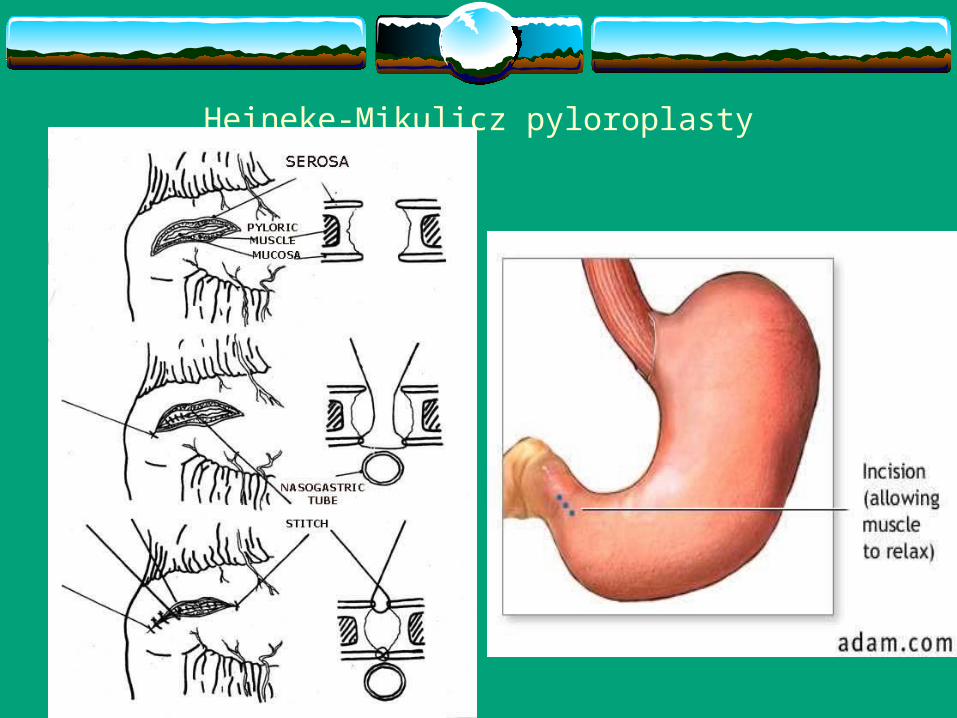
Heineke-Mikulicz pyloroplasty
Postvagotomy complications
1. Dysphagia
2. Gall stone
3. Postvagotmy diarrhea
4. Recurrent ulceration
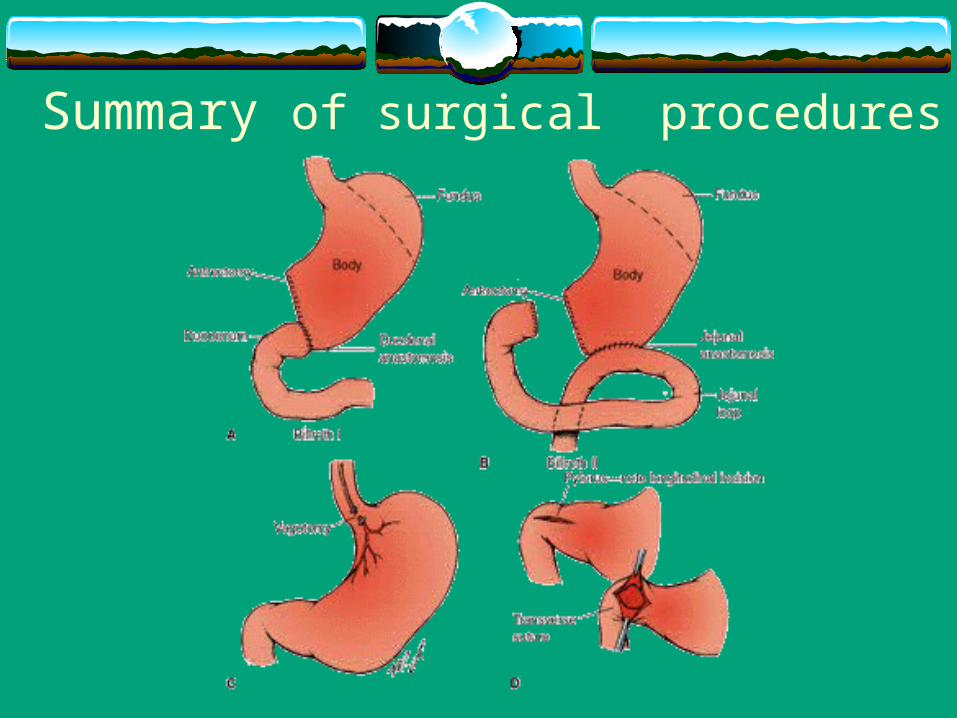
Summary of surgical procedures
THANK YOU
Related Documents