SIRKULASI JANIN Dr. Sevina Marisya, Mked(ped), SpA

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript
SIRKULASI JANIN
Dr. Sevina Marisya, Mked(ped), SpA
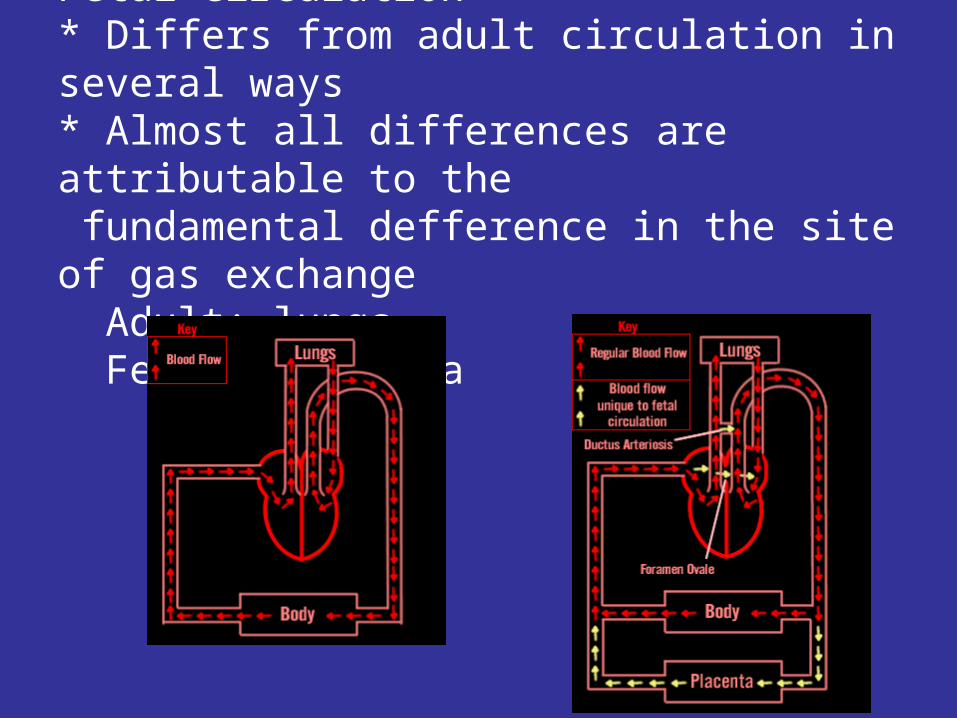
Fetal circulation* Differs from adult circulation in several ways* Almost all differences are attributable to the fundamental defference in the site of gas exchange Adult: lungs Fetus: placenta
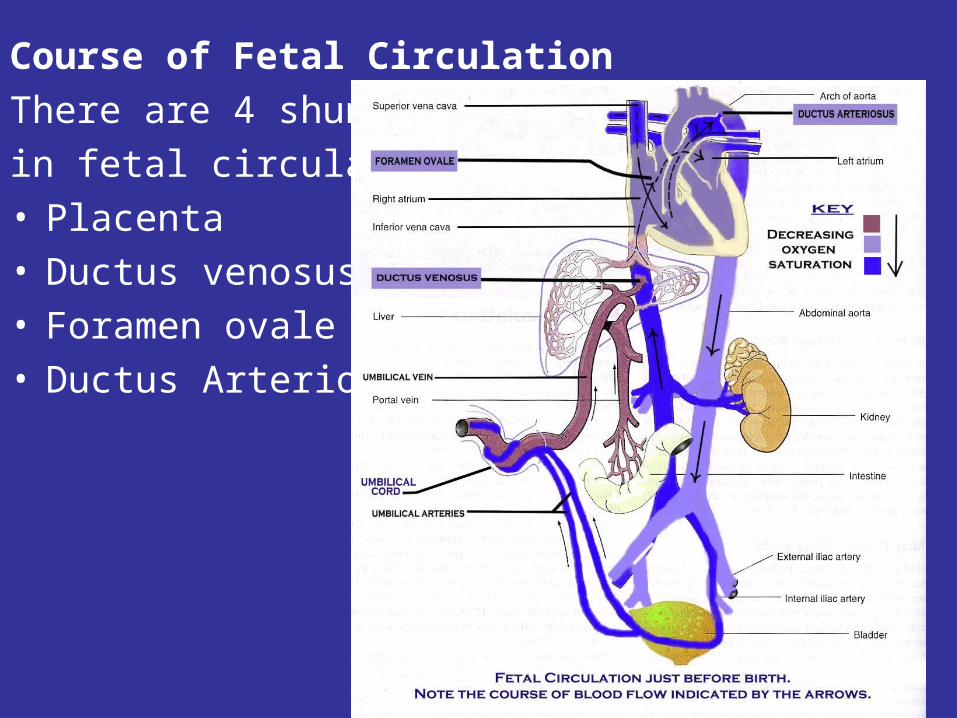
Course of Fetal CirculationThere are 4 shunts in fetal circulation:• Placenta• Ductus venosus• Foramen ovale• Ductus Arteriosus
Some important aspects of fetal circulation:1. The placenta receives the largest amount of
combined ventricular output(55%) and has the lowest vascular resistance in the fetus
2. SVC drains the upper part of the body, IVC drains the lower part of the body and placenta. O2 saturation in the IVC(70%) is higher than in the SVC(40%)
3. Most of SVC blood goes to the RV. One third of the IVC blood is directed by the crista dividens to the LA through the foramen ovale, the remaining two third enters the RV and PA.
4. Less oxygenated blood in the PA flows through the widely open ductus arteriosus to the descending aorta and then to the placenta for oxygenation.
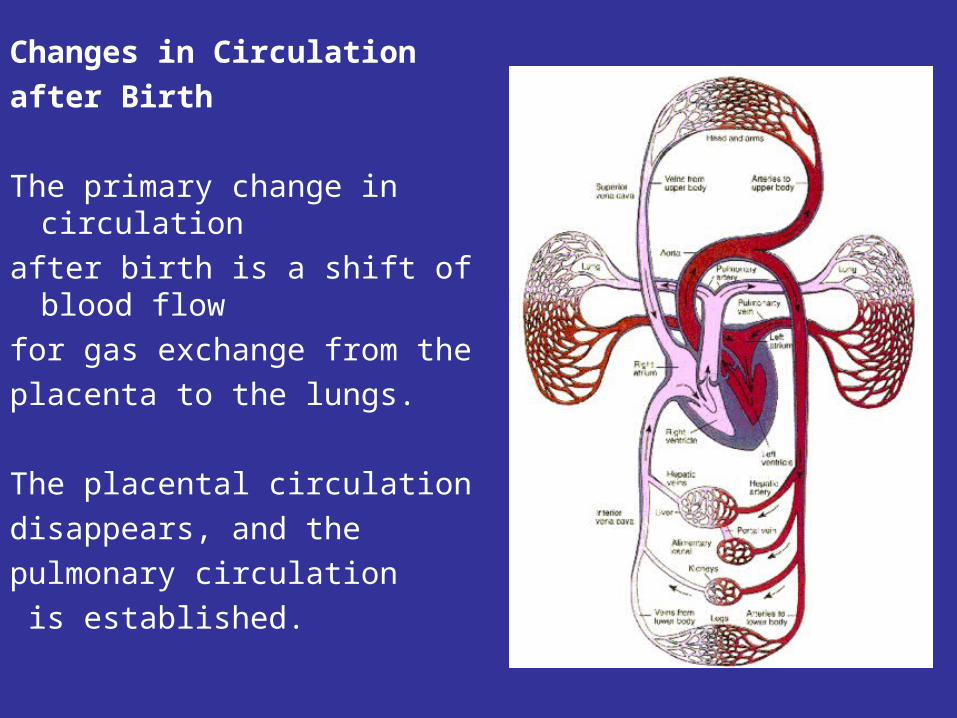
Changes in Circulation after Birth
The primary change in circulation
after birth is a shift of blood flow
for gas exchange from the placenta to the lungs.
The placental circulation disappears, and the pulmonary circulation is established.
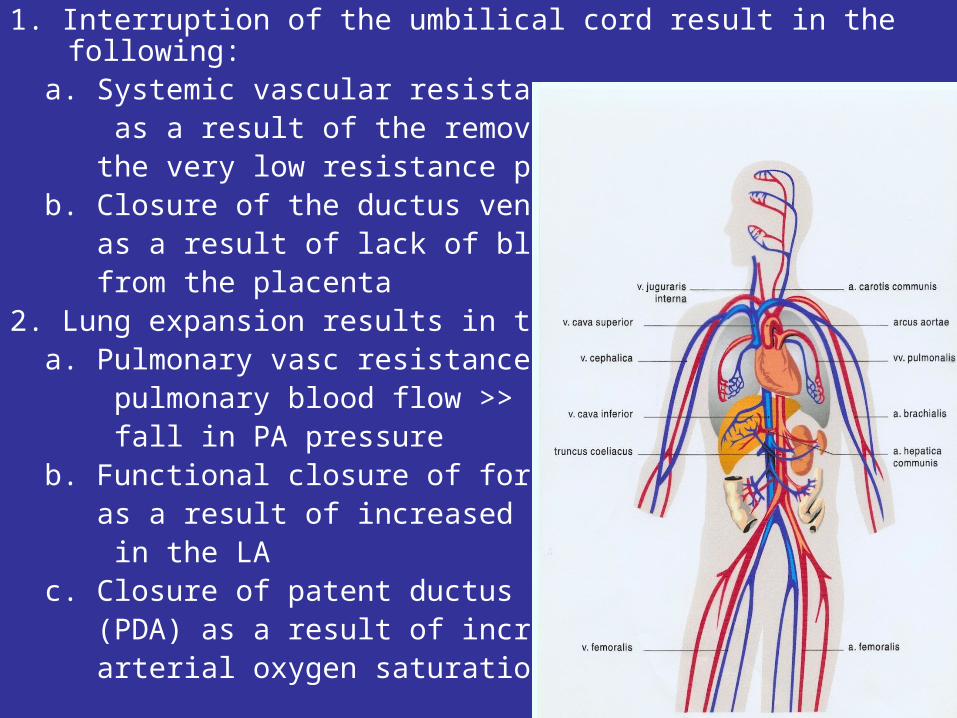
1. Interruption of the umbilical cord result in the following:
a. Systemic vascular resistance >> as a result of the removal of the very low resistance placenta b. Closure of the ductus venosus as a result of lack of blood return from the placenta2. Lung expansion results in the following: a. Pulmonary vasc resistance <<, pulmonary blood flow >> and fall in PA pressure b. Functional closure of foramen ovale as a result of increased pressure in the LA c. Closure of patent ductus arteriosus (PDA) as a result of increased arterial oxygen saturation.
Thank you
PENYAKIT JANTUNG BAWAAN
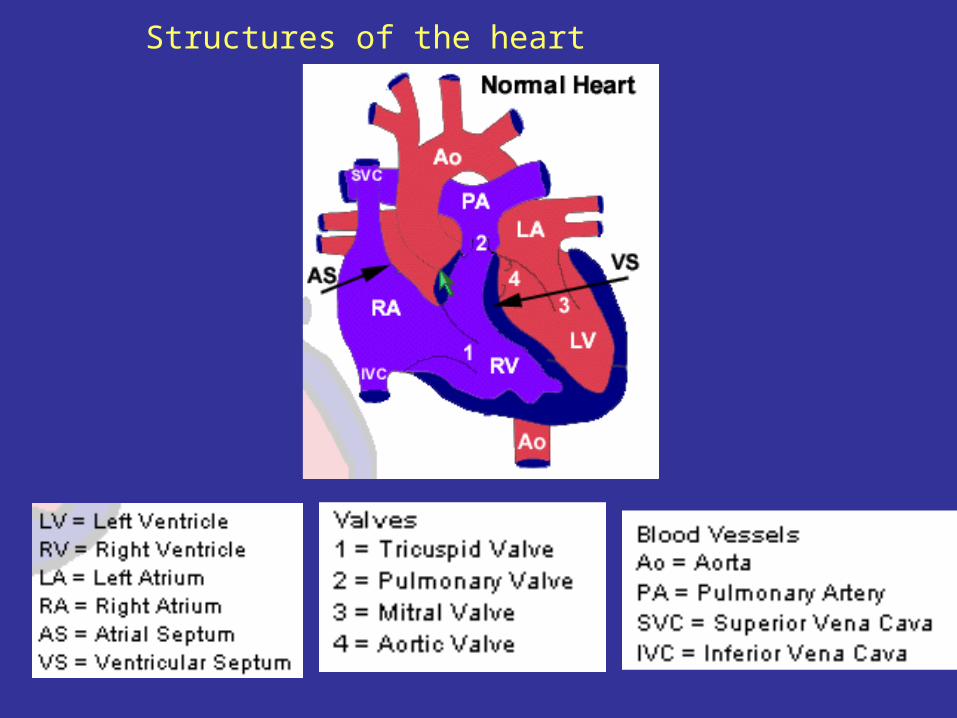
Structures of the heart
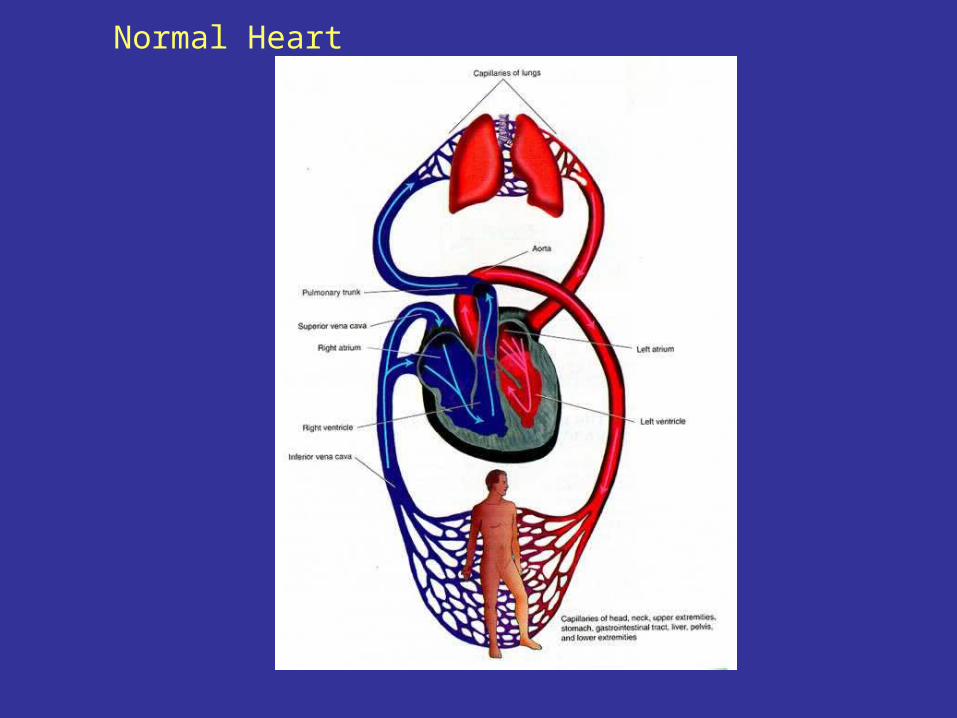
Normal Heart
• Penyakit jantung bawaan (PJB):– Non-sianotik terbesar
•Defek Septum Ventrikel (DSV) : 30%•Defek Septum Atrium (DSA)•Duktus Arteriosus Persisten (DAP)•Stenosis Pulmonal
– Sianotik•TOF (Tetralogi of Fallot)•Atresia Pulmonal•TGA (Tranposisi Great Artery)•Single Ventrikel
Defek Septum Ventrikel•Insiden
30 % dari PJB
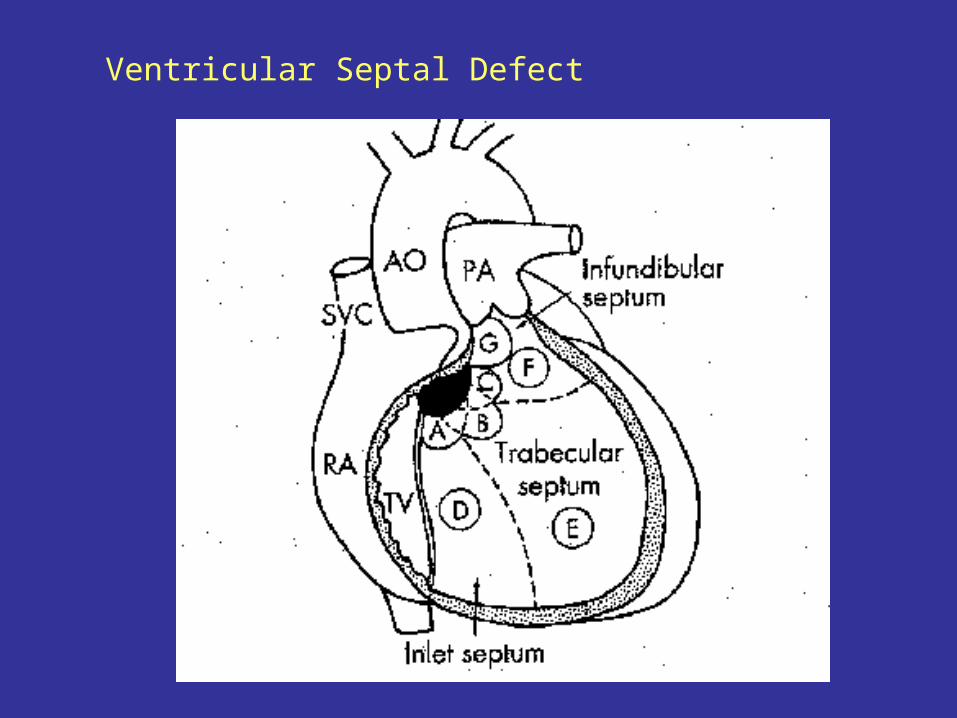
•Anatomi Defek subarteri : di bawah katup aorta dan pulmonal Defek Perimembran: below aortic valve at pars membranous septum Defek Muskular
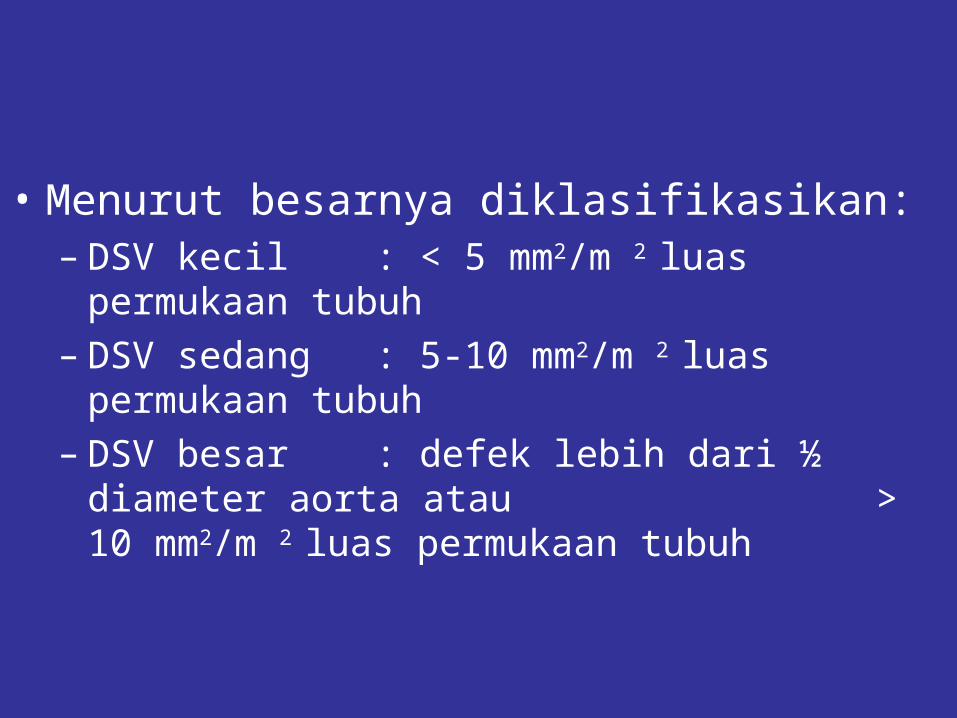
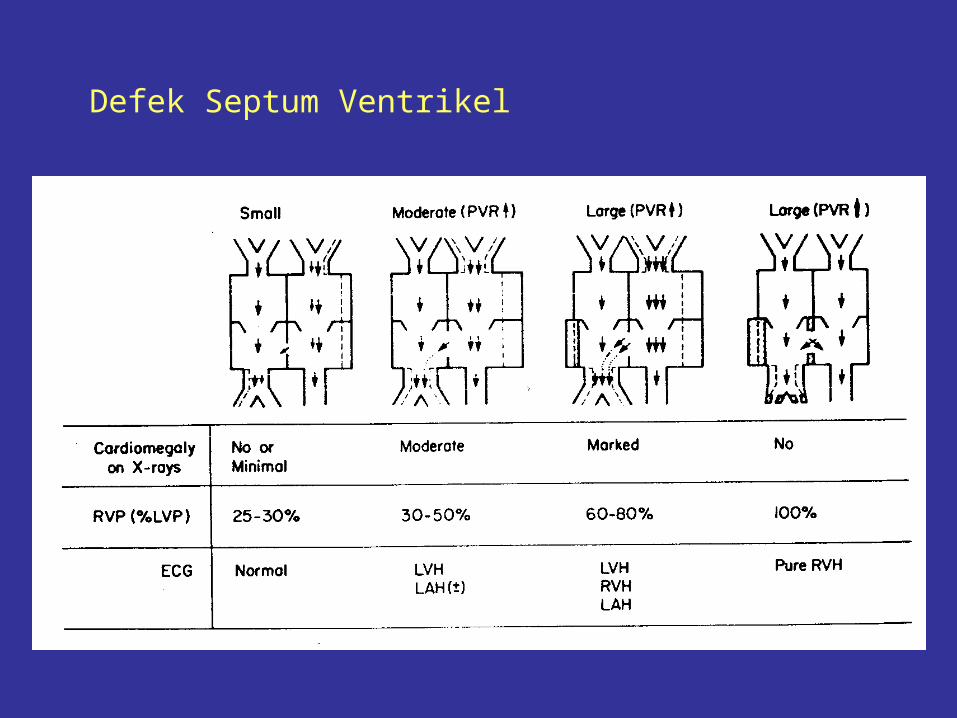
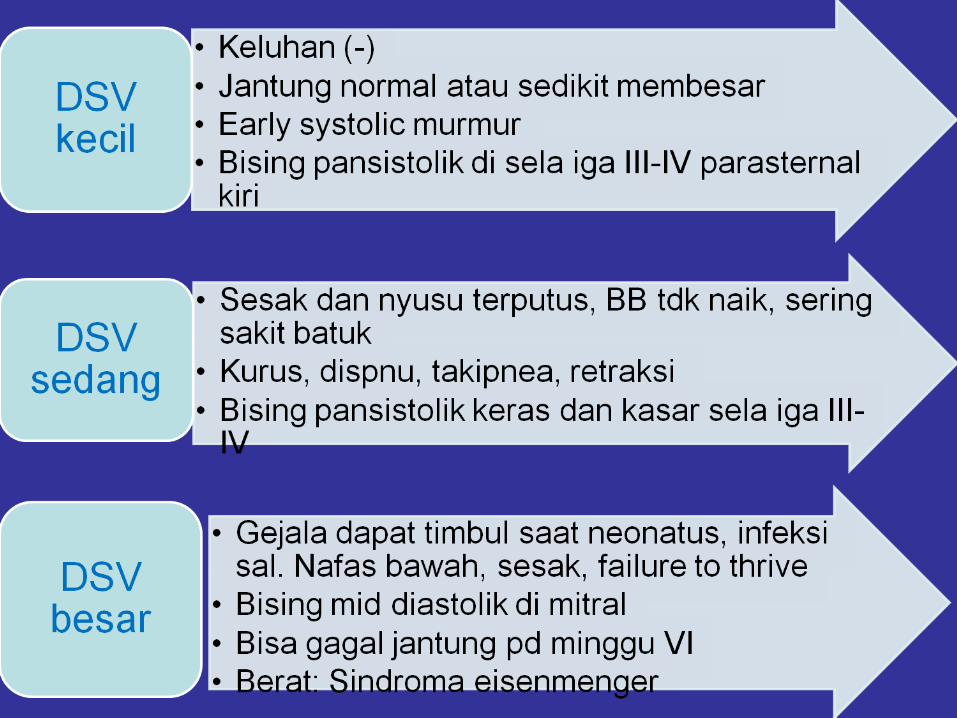
• Menurut besarnya diklasifikasikan:– DSV kecil : < 5 mm2/m 2 luas permukaan tubuh
– DSV sedang : 5-10 mm2/m 2 luas permukaan tubuh
– DSV besar : defek lebih dari ½ diameter aorta atau > 10 mm2/m 2 luas permukaan tubuh

VSD
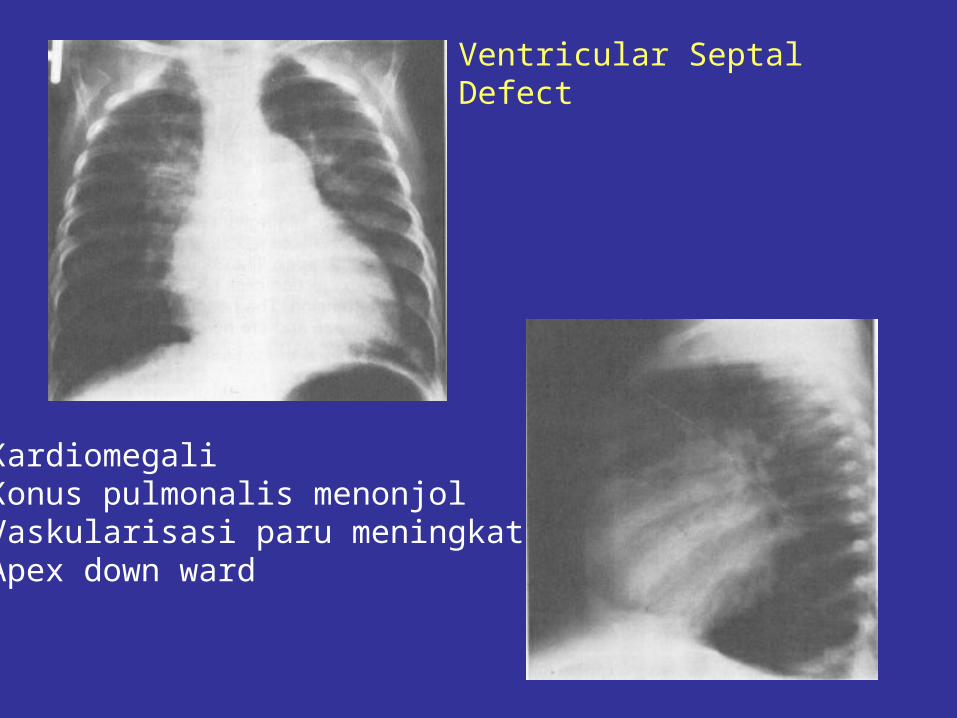
Ventricular Septal Defect
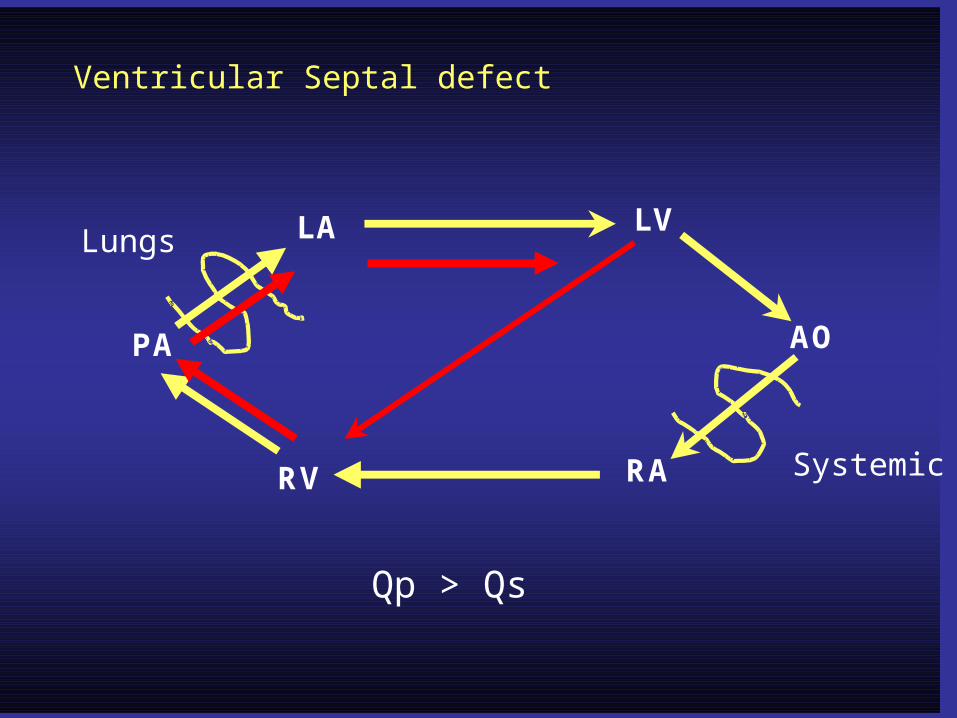
LA LV
RV RA
PA AO
Systemic
Lungs
Qp > Qs
Ventricular Septal defect
RA
RV
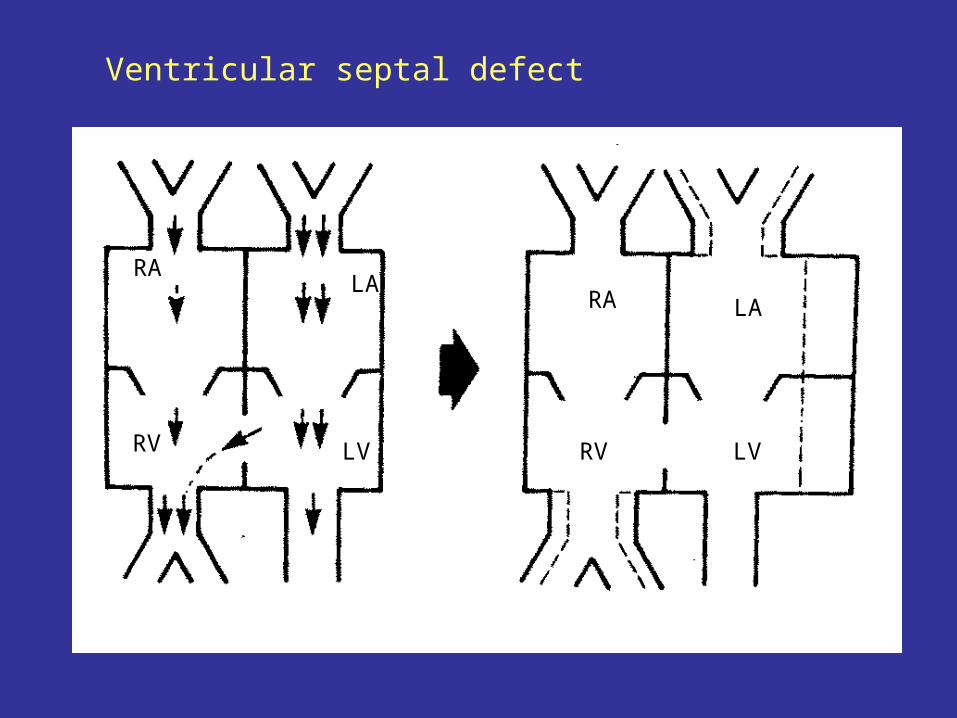
RA LALA
RV LVLV
Ventricular septal defect
Defek Septum Ventrikel
Defek Septum Ventrikel
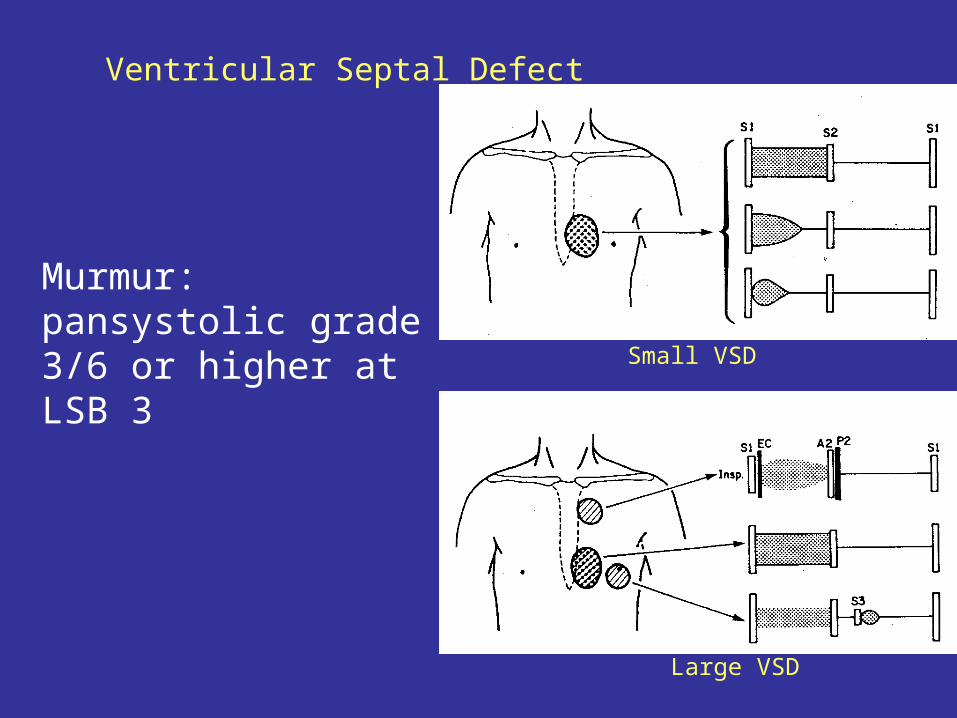
• Clinical findingsDay 1st after birth: murmur (-)After 2-6 weeks : murmur (+)Murmur : pansystolic grade 3/6 or higher at LSB 3 Small muscular defect: early systolic murmurSignificant defect: Mid diastolic murmur at apex
Small VSD
Large VSD
Ventricular Septal Defect
Murmur: pansystolic grade 3/6 or higher at LSB 3
Ventricular Septal Defect
KardiomegaliKonus pulmonalis menonjolVaskularisasi paru meningkatApex down ward
Defek septum Ventrikel
Diagnosis Differential
PDA with PH Tetralogy Fallot non cyanotic Inoscent murmur
Defek septum ventrikel
Management:
Definitive : VSD closure Surgery Transcatheter closure
Gagal Jantung : Digoksin 0.01 mg/kg/hari dibagi 2 dosisInfeksi Sal. Nafas: antibiotik
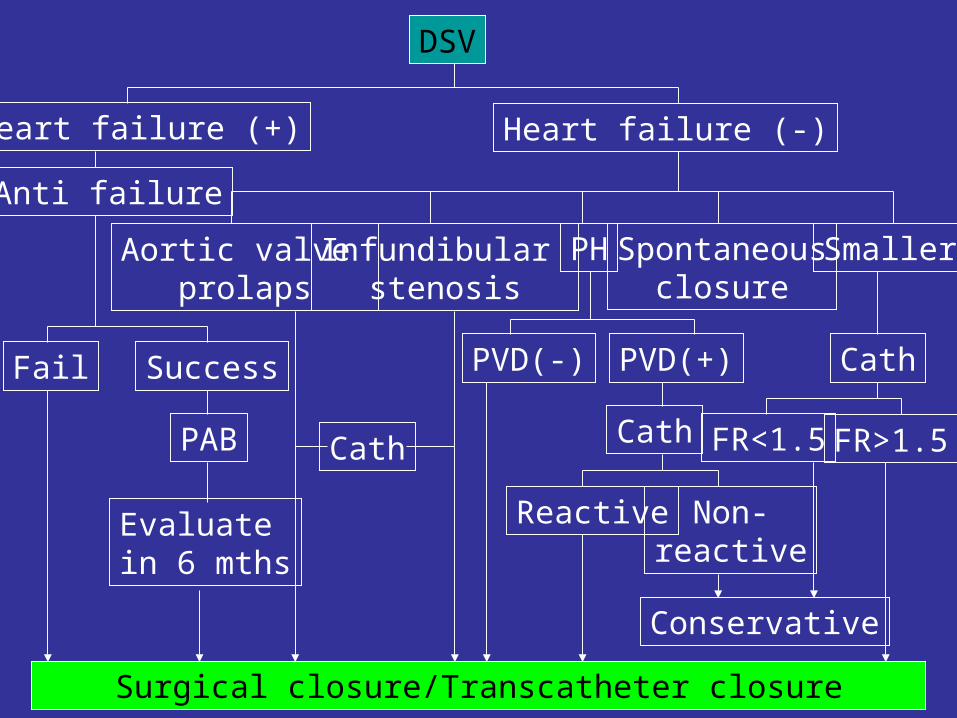
DSV
Heart failure (+) Heart failure (-)Anti failure
Fail Success
PAB
Evaluate in 6 mths
Surgical closure/Transcatheter closure
Aortic valve prolaps
Infundibular stenosis
PH SmallerSpontaneousclosure
Cath
PVD(-) PVD(+) Cath
Cath
Reactive Non-reactive
Conservative
FR>1.5FR<1.5
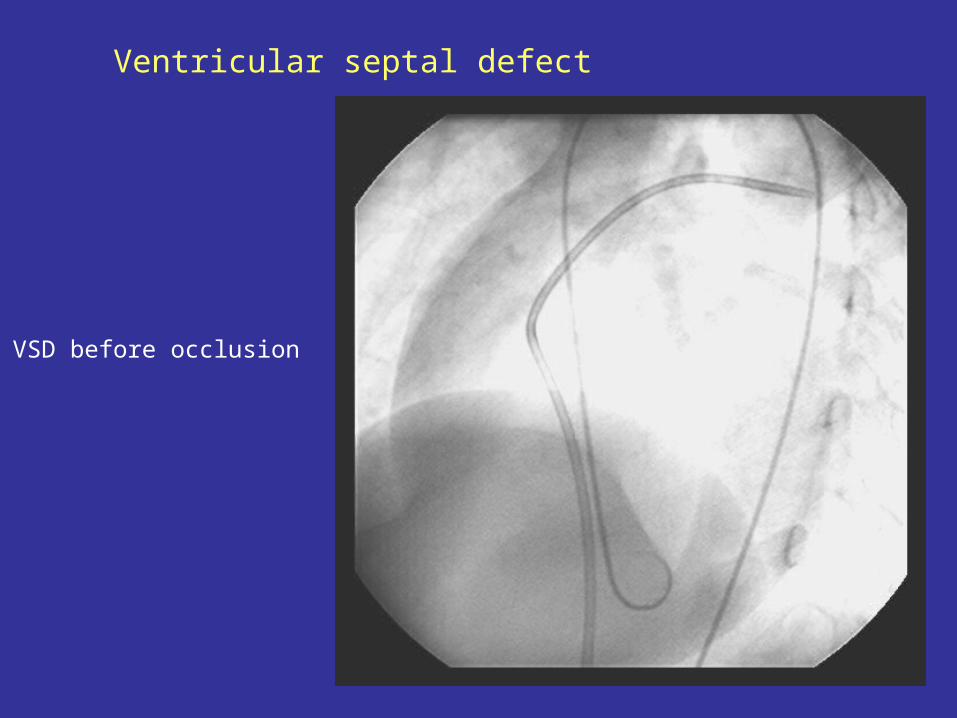
Ventricular septal defect
VSD before occlusion
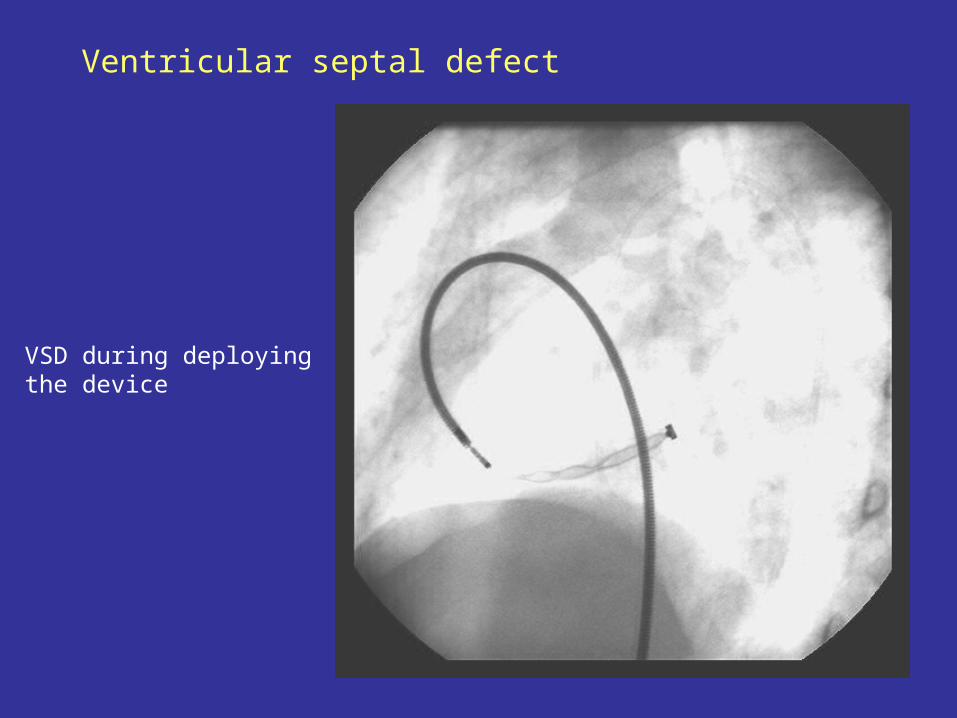
Ventricular septal defect
VSD during deploying the device
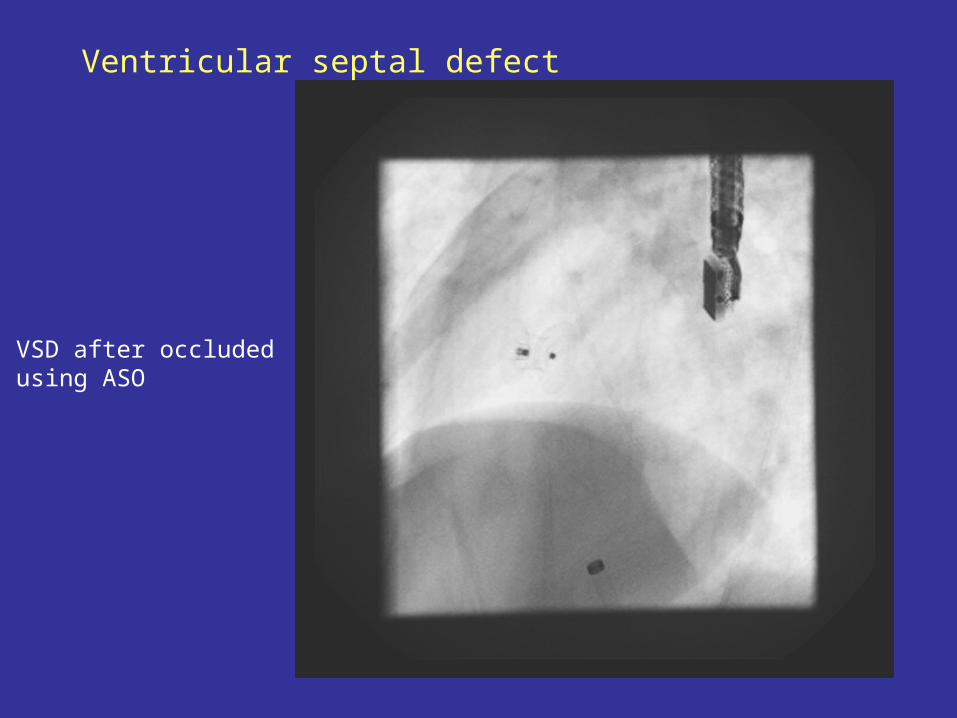
Ventricular septal defect
VSD after occludedusing ASO
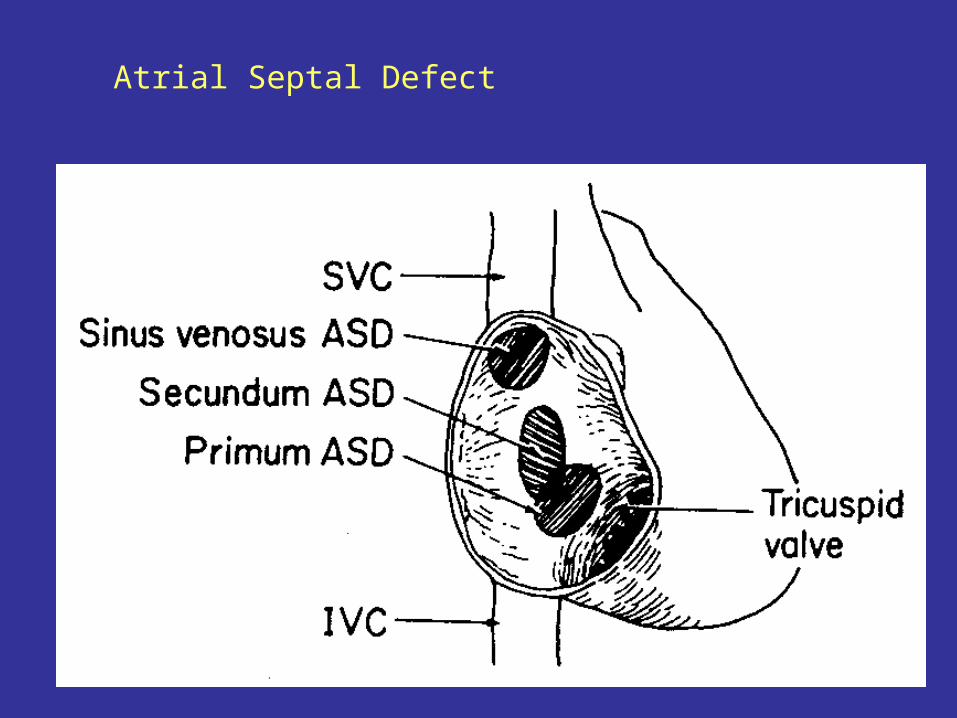
Defek Septum Atrium (DSA)
• Insiden : + 10 % : ratio = 1,5 to 2 : 1• Anatomi : DSA Sekundum: Defect on foramen ovale DSA Sinus venosus: Defect at SVC and RA junction DSA primum: Defect at ostium primum

ASD
Atrial Septal Defect
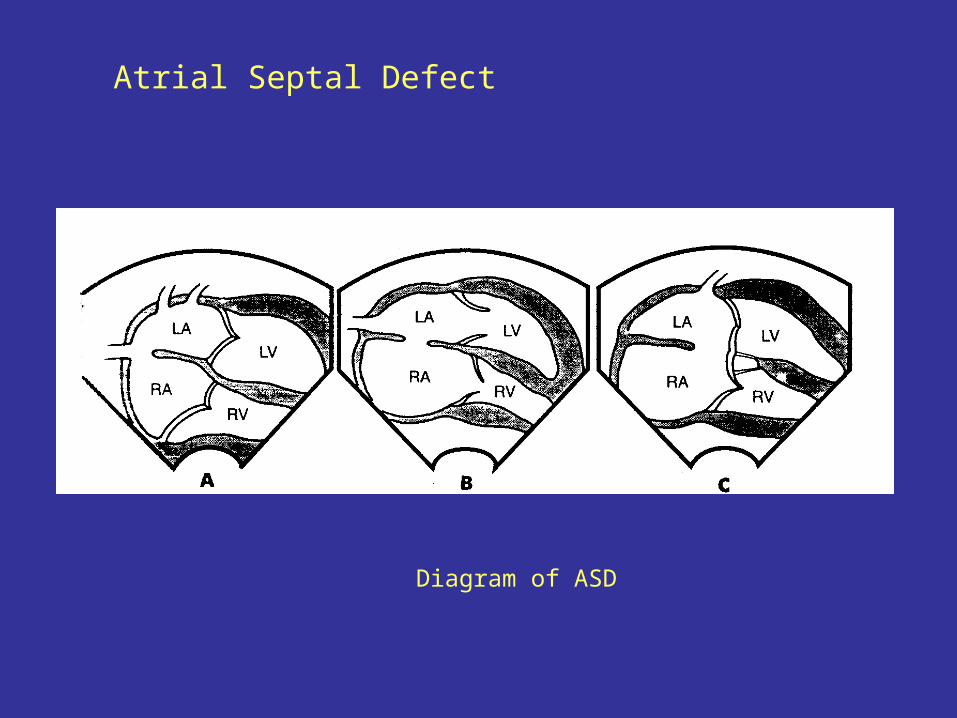
Atrial Septal Defect
Diagram of ASD

LA LV
RV RA
PA AO
Systemic
Lungs
Qp > Qs
Atrial septal defect
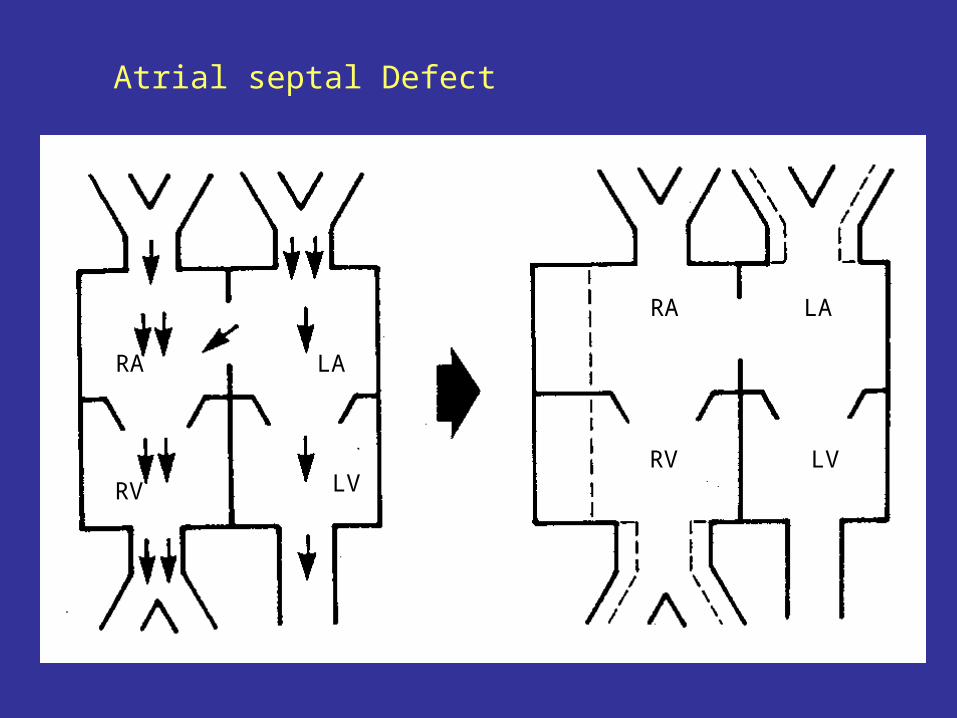
RA
RV
LA
LV
RA
RV
LA
LV
Atrial septal Defect
Klinis- Asymptomatic- Auskultasi: - Bunyi jantung I normal atau mengeras - Bising ejeksi sistolik di daerah pulmonum - Bising diastolik daerah trikuspid
Defek Septum Atrium
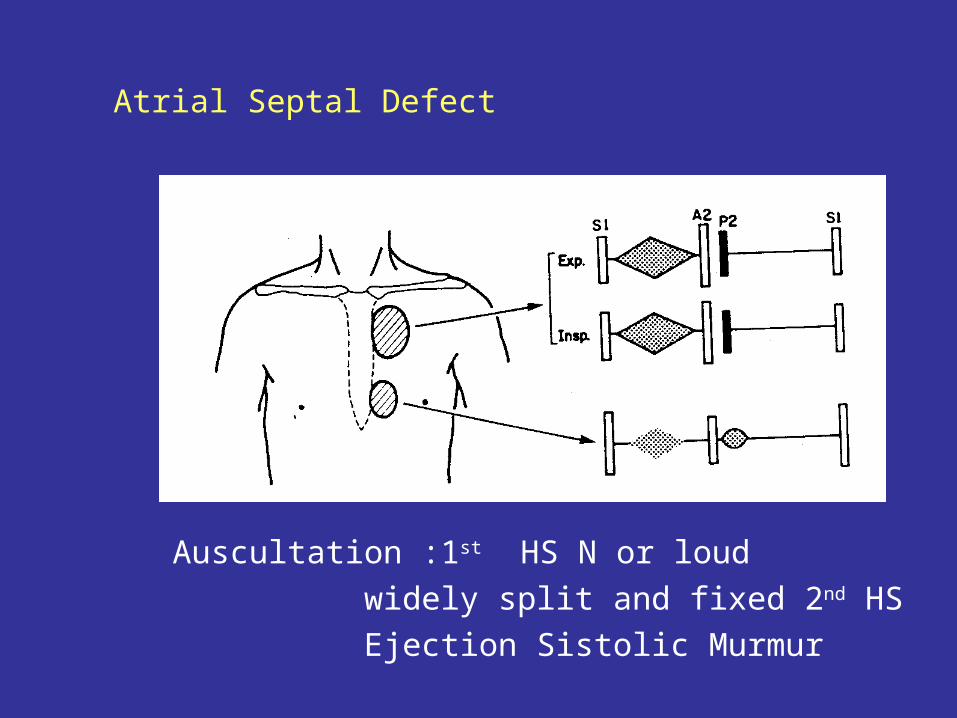
Atrial Septal Defect
Auscultation :1st HS N or loudwidely split and fixed 2nd HS Ejection Sistolic Murmur
ECG : RBBB right ventricular hypertrophy
Atrial Septal Defect
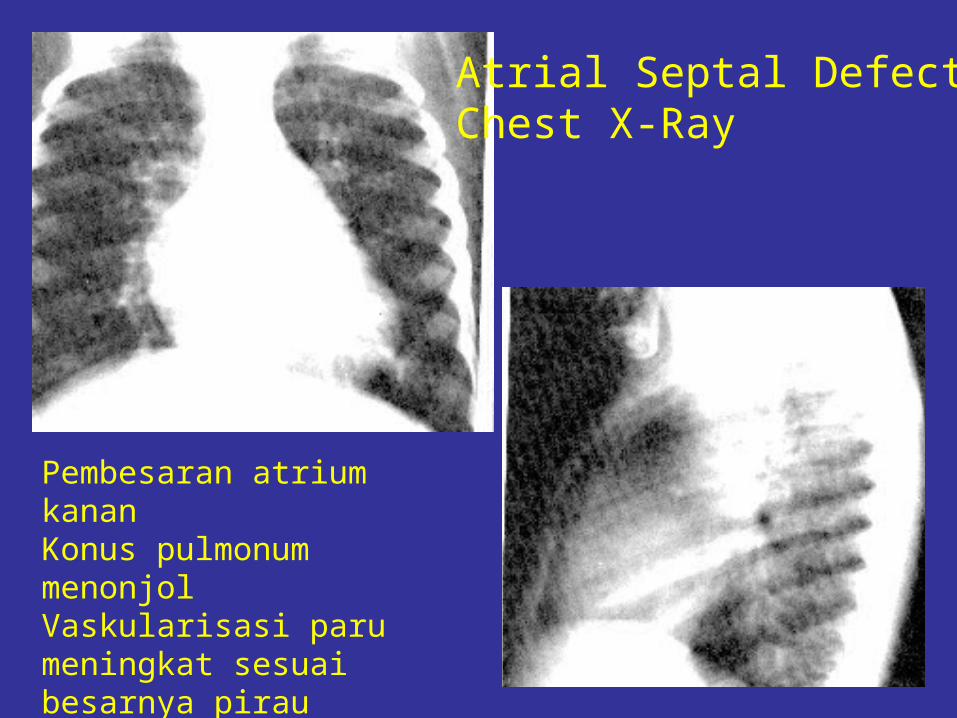
Pembesaran atrium kananKonus pulmonum menonjolVaskularisasi paru meningkat sesuai besarnya pirau
Atrial Septal DefectChest X-Ray
Defek Septum Atrium
Diagnosis Differential
Primary Atrial Septal DefectECG : LAD
Partial Anomalous Pulmonary Vein Drainage Pulmonary Stenosis Innocent Murmur
Defek Septum Atrium
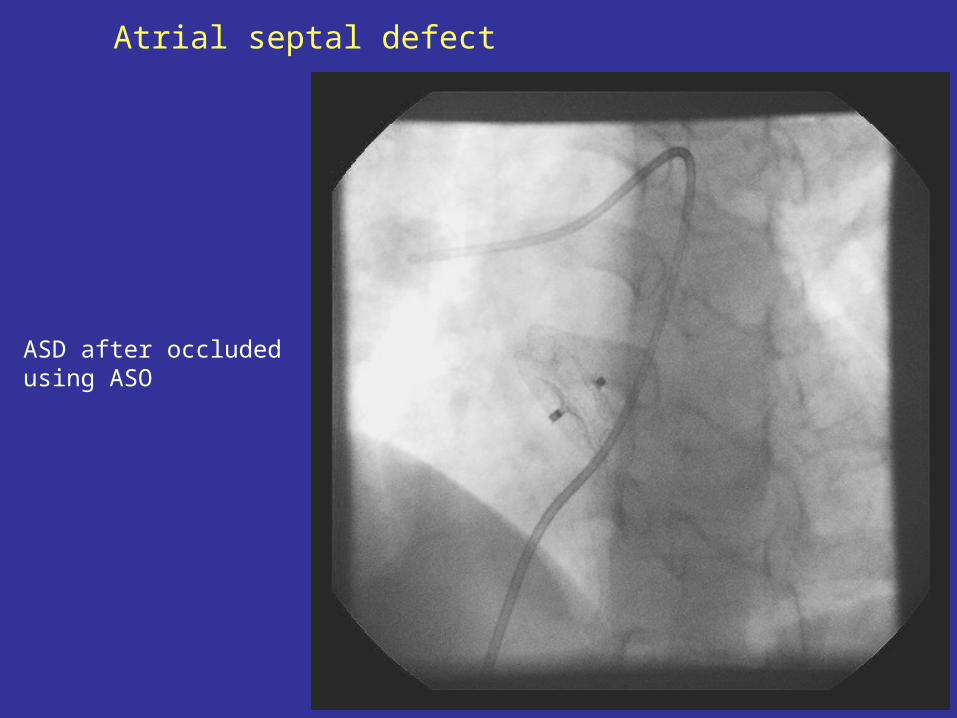
ManagementSurgery : Preschool age 4-5 thnRecent treatment: transcatheter closure using ASO (Amplatzer septal occluder)
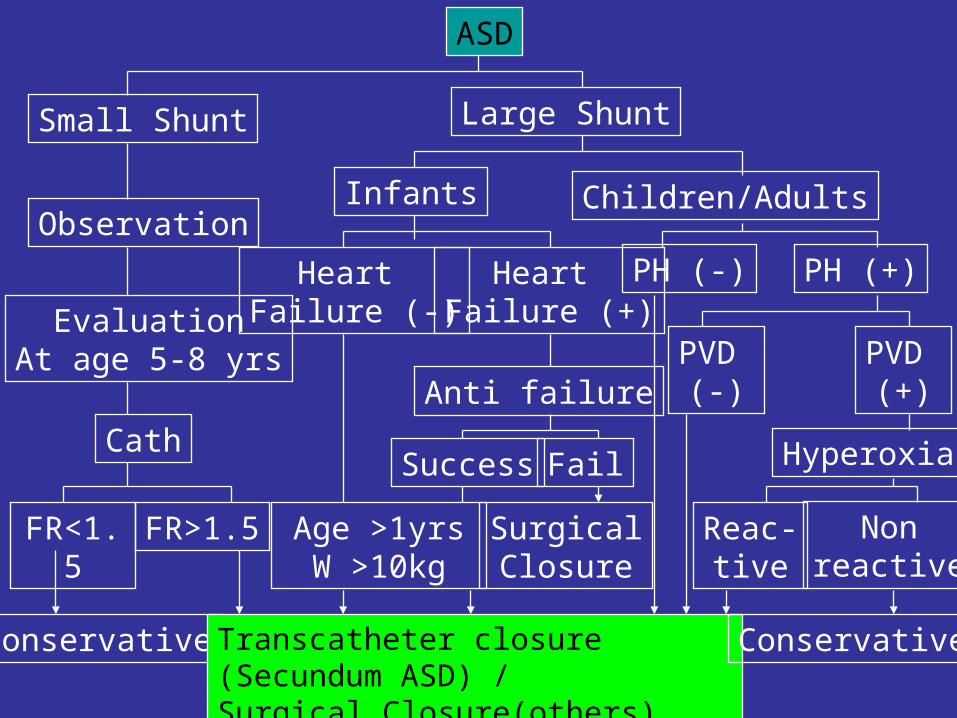
ASD
Small Shunt Large Shunt
Observation
EvaluationAt age 5-8 yrs
Cath
FR<1.5
FR>1.5
Conservative
Infants Children/Adults
Heart Failure (-)
Heart Failure (+)
Age >1yrsW >10kg
Transcatheter closure (Secundum ASD) /Surgical Closure(others)
Conservative
Anti failure
FailSuccess
PH (-) PH (+)
PVD (-)
PVD (+)
Hyperoxia
Reac-tive
Nonreactive
SurgicalClosure
Atrial septal defect
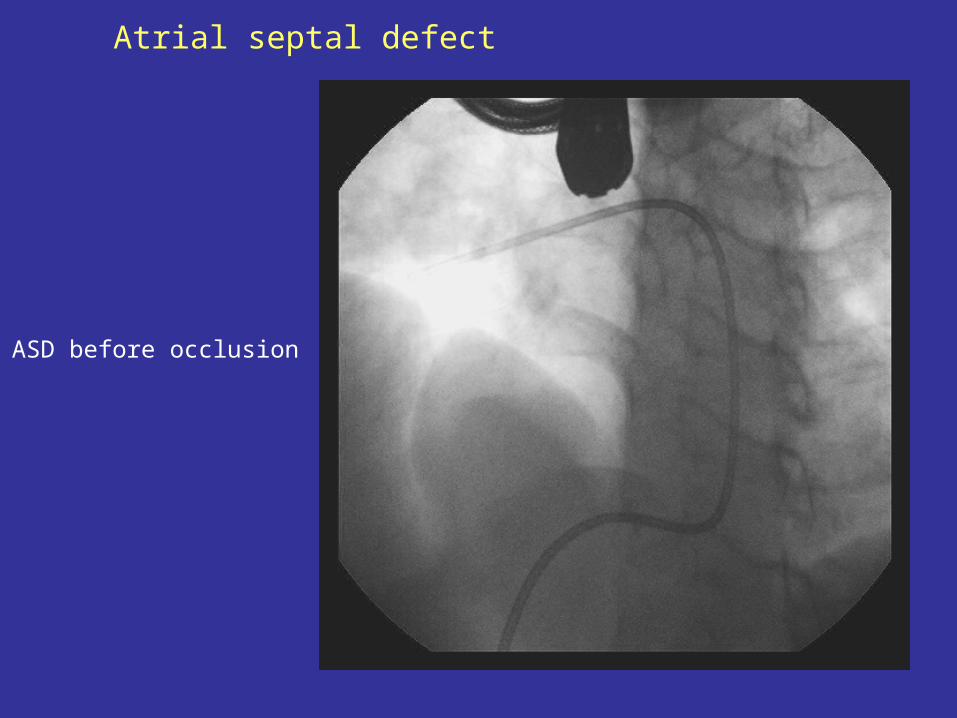
Atrial septal defect
ASD before occlusion
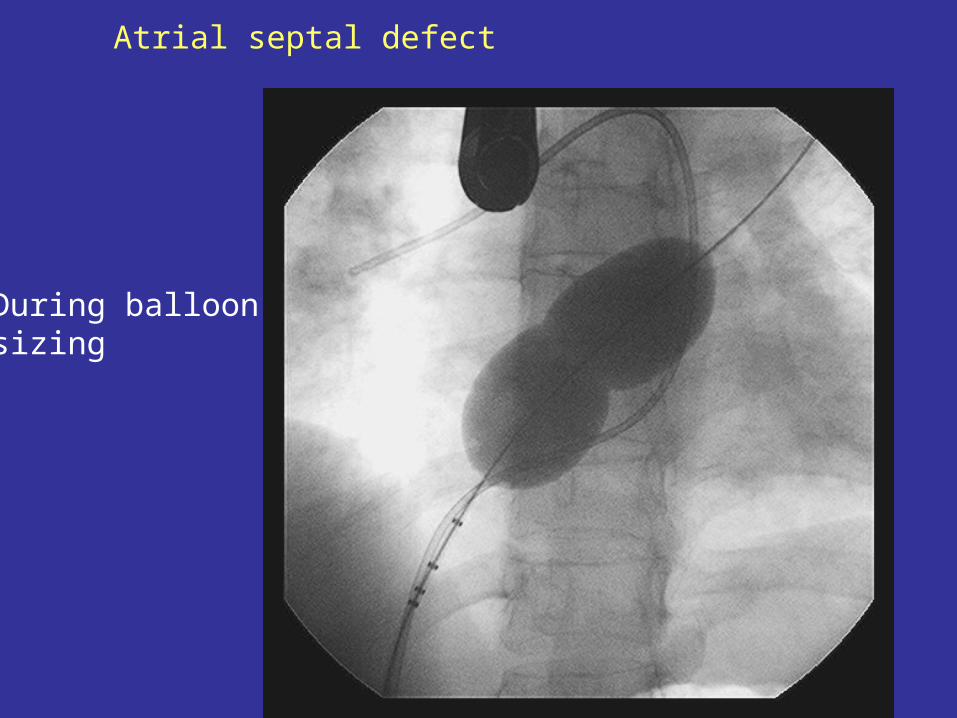
During balloon sizing
Atrial septal defect
Atrial septal defect
ASD after occluded using ASO
PENYAKIT JANTUNG BAWAAN SIANOTIK
Tetralogy FallotInsiden5-8% dari PJBAnatomiCause: Left-anterior deviation of infundibular septumSindroma consist of 4 items:
VSD pulmonal stenosis aortic over-riding RVH
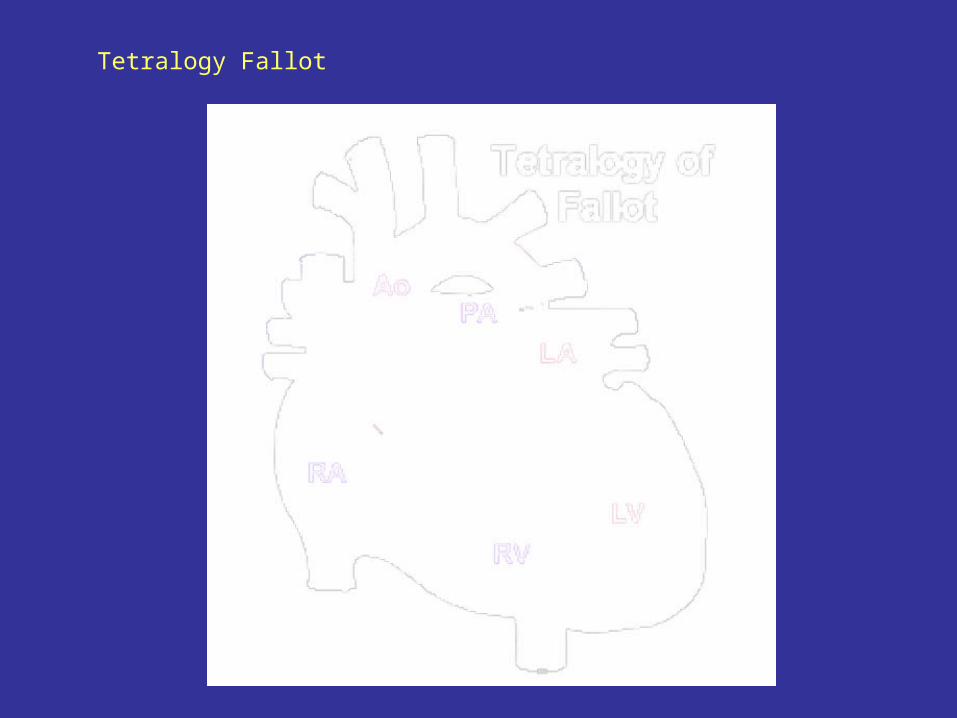
Tetralogy Fallot
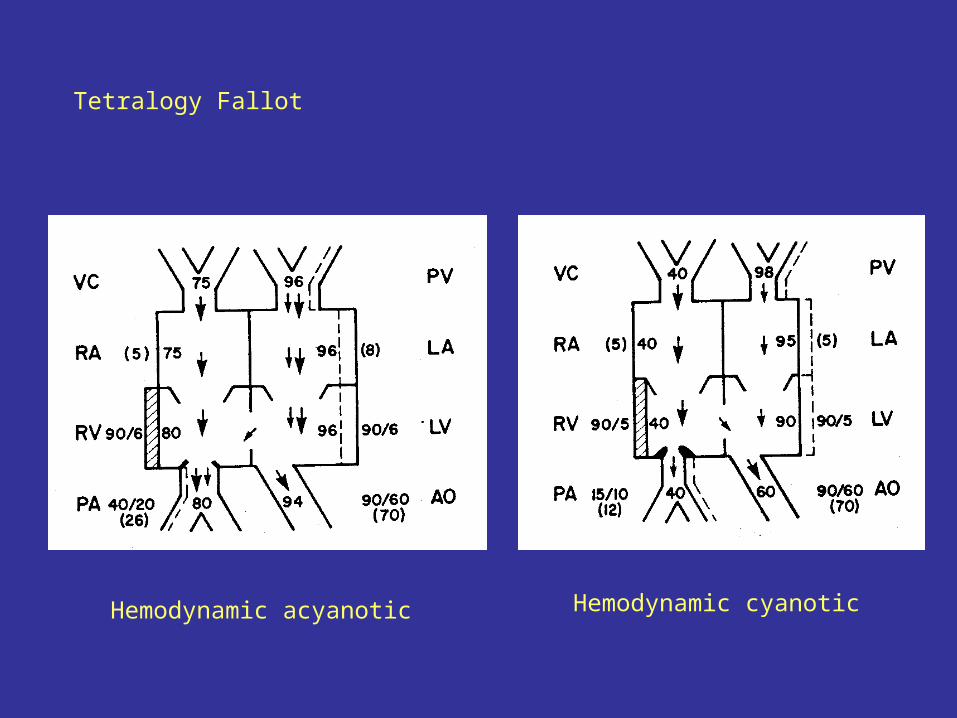
Tetralogy Fallot
Hemodynamic acyanotic Hemodynamic cyanotic
Tetralogy Fallot
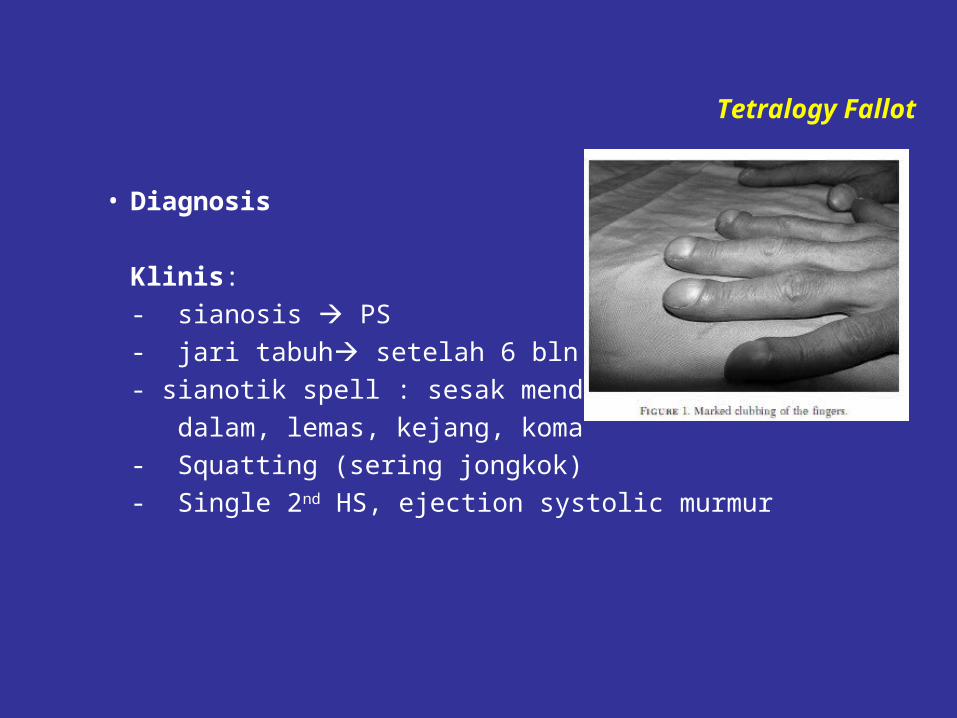
• Diagnosis
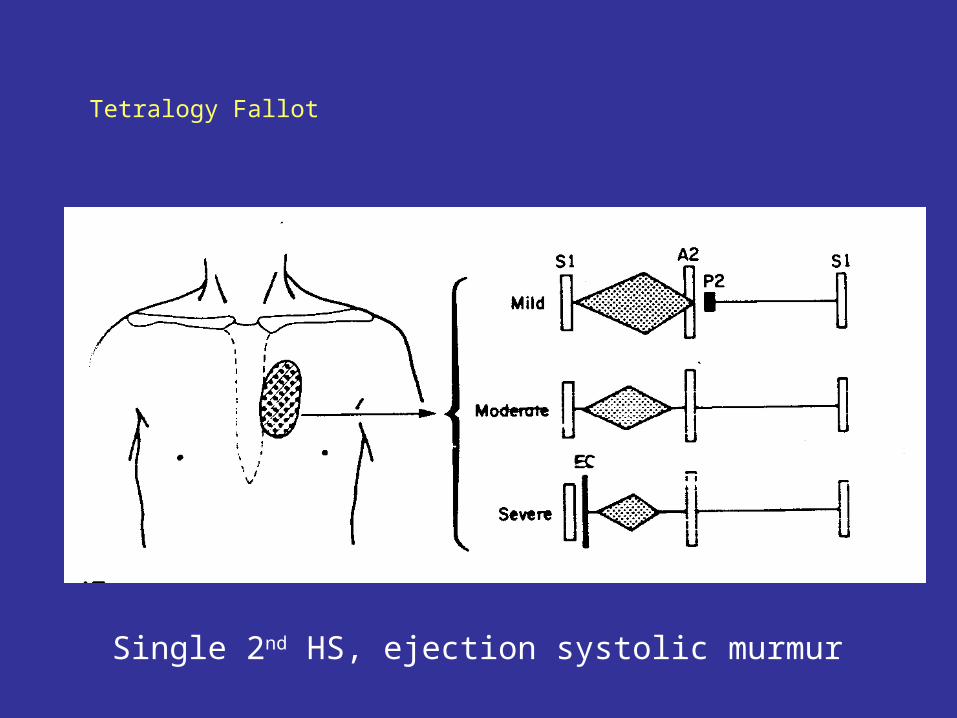
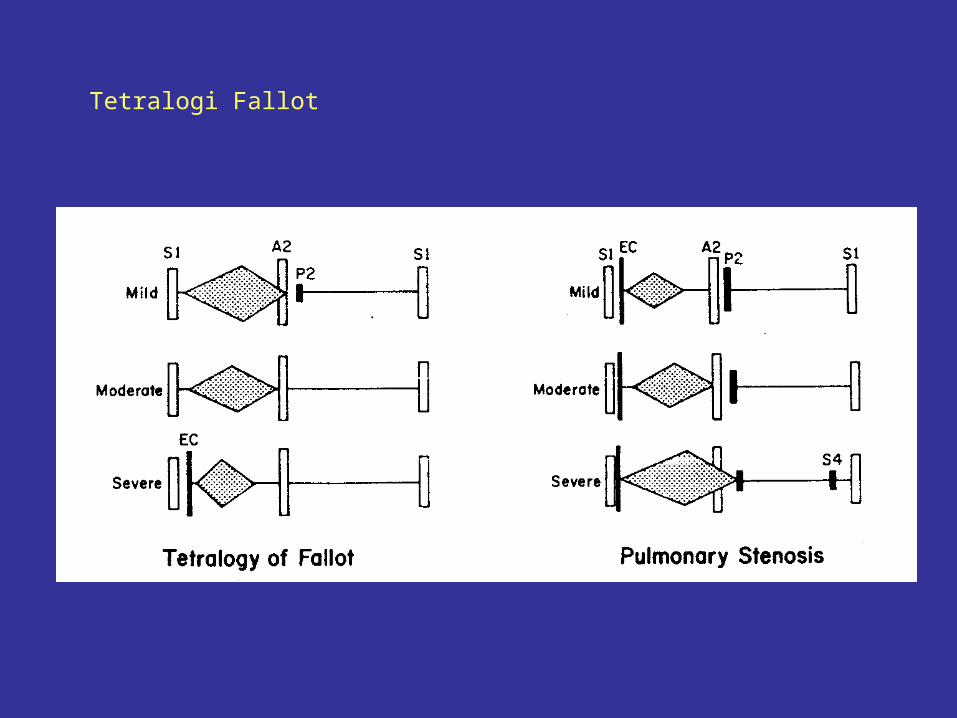
Klinis:- sianosis PS- jari tabuh setelah 6 bln- sianotik spell : sesak mendadak, nafas cepat dalam, lemas, kejang, koma- Squatting (sering jongkok)- Single 2nd HS, ejection systolic murmur
Tetralogy Fallot
Single 2nd HS, ejection systolic murmur
Tetralogi Fallot
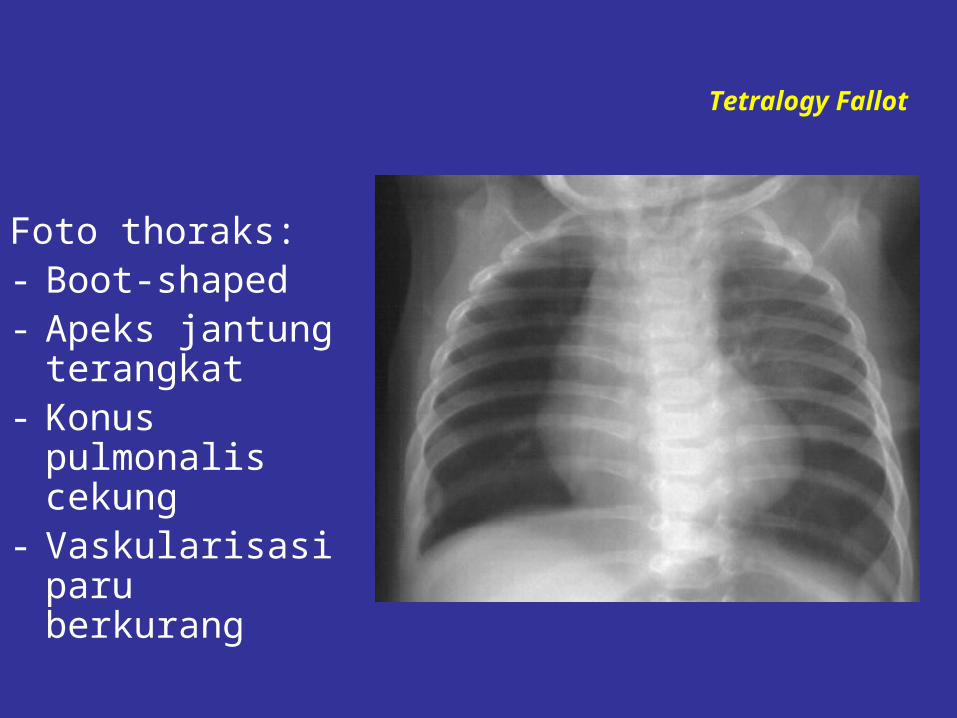
Foto thoraks: - Boot-shaped- Apeks jantung terangkat
- Konus pulmonalis cekung
- Vaskularisasi paru berkurang
Tetralogy Fallot
Tetralogy Fallot
ECG : RADEchocardiography : to confirm diagnosis
Tetralogy Fallot
• Diagnosis Differential Pulmonary Atresia Double outlet right ventricle and pulmonary stenosis Transposisi of great arteri and pulmonary stenosis
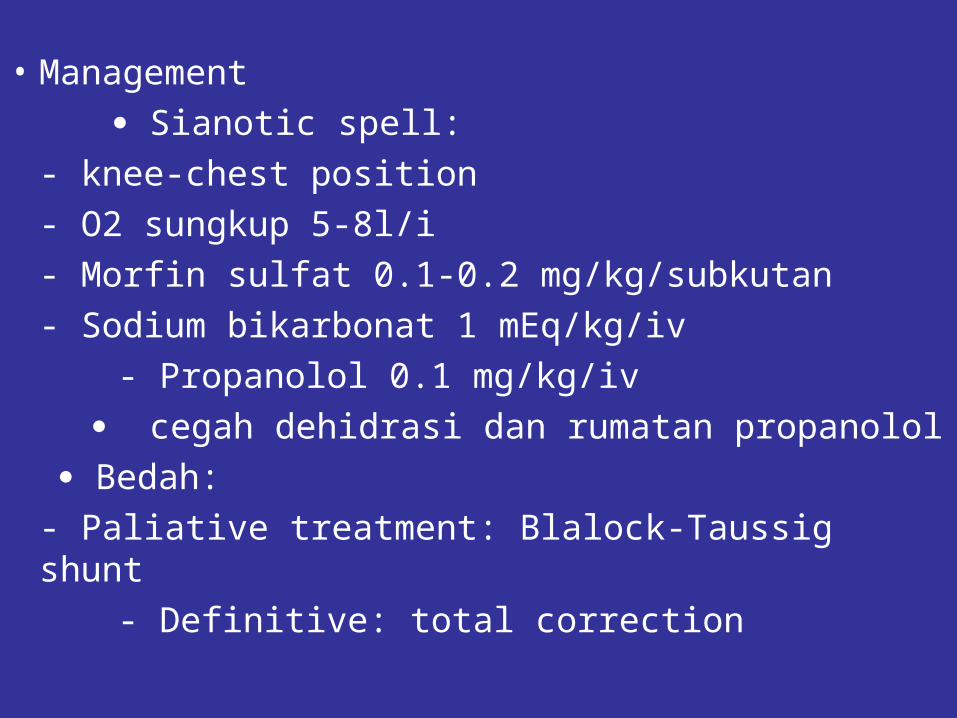
• Management Sianotic spell:- knee-chest position- O2 sungkup 5-8l/i- Morfin sulfat 0.1-0.2 mg/kg/subkutan- Sodium bikarbonat 1 mEq/kg/iv - Propanolol 0.1 mg/kg/iv
cegah dehidrasi dan rumatan propanolol Bedah:- Paliative treatment: Blalock-Taussig shunt - Definitive: total correction
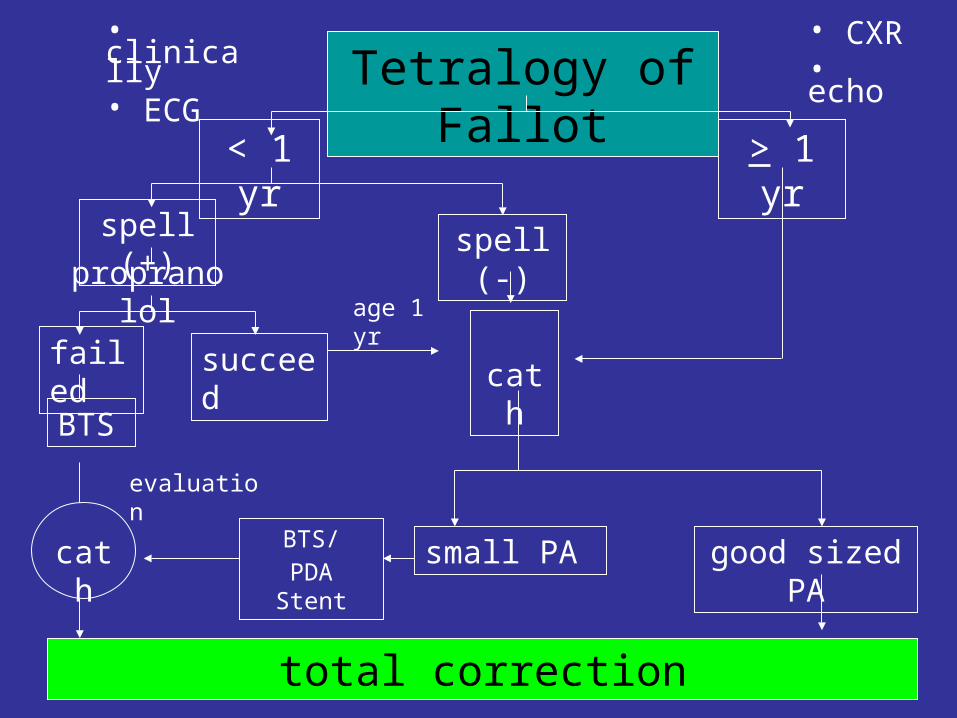
Tetralogy of Fallot< 1
yr> 1 yr
spell (+) spell
(-)propranolol
failed
succeed
BTS
total correction
cath
small PA good sized PA
• clinically• ECG
• CXR• echo
age 1 yr
cath
BTS/PDA Stent
evaluation
Tetralogy Fallot
Tetralogy Fallot


Related Documents











