INTERNATIONAL JOURNAL OF IMMUNOPATHOLOGY AND PHARMACOLOGY Vol. 20, no. 1, 0-0 (2007) 0394-6320 (2006) Copyright © by BIOLIFE, s.a.s. This publication and/or article is for individual use only and may not be further reproduced without written permission from the copyright holder. Unauthorized reproduction may result in financial and other penalties 149 PENILE CUTANEOUS TEMPERATURE IN SYSTEMIC SCLEROSIS: A THERMAL IMAGING STUDY A. MERLA 1,2 , G. ROMANI 1,2 , A. TANGHERLINI 1 , S. DI ROMUALDO 1 , M. PROIETTI 3 , E. ROSATO 3 , A. AVERSA 4 and F. SALSANO 3 1 Department of Clinical Sciences and Bioimaging, University G. d’Annunzio, 2 ITAB, Institute for Ad- vanced Biomedical Technologies, University G. d’Annunzio Foundation, Chieti; 3 Department of Clinical Immunology and Allergy, 4 Department of Pathophysiology, University of Rome La Sapienza, Rome, Italy Received July 12, 2006 – Accepted November 22, 2006 Systemic Sclerosis is a connective tissue disorder featuring vascular alterations and an immunological activation leading to a progressive and widespread fibrosis of several organs such as the skin, lung, gastrointestinal tract, heart and kidney. Moreover men with systemic sclerosis (SSc) present an increased risk of developing erectile dysfunction (ED). Recently, we evaluated the extent of penile vascular damage in sclerodermic patients using Duplex ultrasonography. The aim of this paper is to investigate whether penile thermal differences exist between sclerodermic patients and healthy controls. For this reason 10 men with SSc receiving current treatment for their disease, and 10 healthy controls were enroled; penile thermal properties were assessed through non-contact thermal imaging (functional Infra Red Imaging fIRI); erectile function was evaluated using the sexual health inventory for men (SHIM) questionnaire. The SHIM results confirmed the presence of ED in sclerodermic patients. Baseline penile temperature in patients (32.1 ± 1.4°C) was lower than in controls (34.1 ± 0.9°C). Recovery from cooling test was seen to be faster in healthy controls than in patients, both in terms of recovery amplitude (patients 3.75 ± 2.09°C, controls 9.80 ± 2.77°C) and amplitude to time constant ratio (patients 1.21 ± 0.64°C/min, controls 1.96 ± 0.48°C/min). These results show that penile thermal abnormalities occur in almost all sclerodermic patients. Non-contact thermal imaging not only identifies thermal alterations but also clearly distinguishes between SSc patients and healthy controls and therefore could represent a valuable instrument in identifying early ED in S Sc patients. Mailing address: Dr Arcangelo Merla, Istituto Tecnologie Avanzate Biomediche, Fondazione “Università G. d’Annunzio”, Via dei Vestini 13, 66013 Chieti Scalo (Ch), Italy Tel: ++39 0871 3556901 Fax: ++39 0871 3556930 e-mail: [email protected] Keywords: scleroderma, erectile dysfunction, SHIM, penis, temperature, thermal imaging Systemic Sclerosis (SSc) is a connective tissue disorder featuring vascular alterations and immunological activation leading to progressive and widespread fibrosis of the skin and other visceral organs such as the lung, gastrointestinal tract, heart and kidney (1). Lally and Jimenez (2-3) were the first to describe the association of SSc with erectile dysfunction (ED) in 1981. Subsequent studies have shown that the prevalence of ED in men with SSc at various stages of the disease may be as high as 80%, and its incidence seems to be more frequent than in other connective tissue diseases; nevertheless, the majority of these studies have mainly focused on epidemiological data obtained by interviewing sclerodermic patients using the SHIM questionnaire (5). Recently, we investigated the extent of penile

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

INTERNATIONAL JOURNAL OF IMMUNOPATHOLOGY AND PHARMACOLOGY Vol. 20, no. 1, 0-0 (2007)
0394-6320 (2006)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties149
PENILE CUTANEOUS TEMPERATURE IN SYSTEMIC SCLEROSIS:A THERMAL IMAGING STUDY
A. MERLA1,2, G. ROMANI1,2, A. TANGHERLINI1, S. DI ROMUALDO1, M. PROIETTI3,E. ROSATO3, A. AVERSA4 and F. SALSANO3
1Department of Clinical Sciences and Bioimaging, University G. d’Annunzio, 2ITAB, Institute for Ad-vanced Biomedical Technologies, University G. d’Annunzio Foundation, Chieti; 3Department of Clinical Immunology and Allergy, 4Department of Pathophysiology, University of Rome La Sapienza, Rome, Italy
Received July 12, 2006 – Accepted November 22, 2006
Systemic Sclerosis is a connective tissue disorder featuring vascular alterations and an immunological activation leading to a progressive and widespread fibrosis of several organs such as the skin, lung, gastrointestinal tract, heart and kidney. Moreover men with systemic sclerosis (SSc) present an increased risk of developing erectile dysfunction (ED). Recently, we evaluated the extent of penile vascular damage in sclerodermic patients using Duplex ultrasonography. The aim of this paper is to investigate whether penile thermal differences exist between sclerodermic patients and healthy controls. For this reason 10 men with SSc receiving current treatment for their disease, and 10 healthy controls were enroled; penile thermal properties were assessed through non-contact thermal imaging (functional Infra Red Imaging fIRI); erectile function was evaluated using the sexual health inventory for men (SHIM) questionnaire. The SHIM results confirmed the presence of ED in sclerodermic patients. Baseline penile temperature in patients (32.1 ± 1.4°C) was lower than in controls (34.1 ± 0.9°C). Recovery from cooling test was seen to be faster in healthy controls than in patients, both in terms of recovery amplitude (patients 3.75 ± 2.09°C, controls 9.80 ± 2.77°C) and amplitude to time constant ratio (patients 1.21 ± 0.64°C/min, controls 1.96 ± 0.48°C/min). These results show that penile thermal abnormalities occur in almost all sclerodermic patients. Non-contact thermal imaging not only identifies thermal alterations but also clearly distinguishes between SSc patients and healthy controls and therefore could represent a valuable instrument in identifying early ED in S Sc patients.
Mailing address: Dr Arcangelo Merla, Istituto Tecnologie Avanzate Biomediche, Fondazione “Università G. d’Annunzio”, Via dei Vestini 13, 66013 Chieti Scalo (Ch), Italy Tel: ++39 0871 3556901 Fax: ++39 0871 3556930 e-mail: [email protected]
Keywords: scleroderma, erectile dysfunction, SHIM, penis, temperature, thermal imaging
Systemic Sclerosis (SSc) is a connective tissue disorder featuring vascular alterations and immunological activation leading to progressive and widespread fibrosis of the skin and other visceral organs such as the lung, gastrointestinal tract, heart and kidney (1). Lally and Jimenez (2-3) were the first to describe the association of SSc with erectile dysfunction (ED) in 1981. Subsequent studies have shown that the
prevalence of ED in men with SSc at various stages of the disease may be as high as 80%, and its incidence seems to be more frequent than in other connective tissue diseases; nevertheless, the majority of these studies have mainly focused on epidemiological data obtained by interviewing sclerodermic patients using the SHIM questionnaire (5).
Recently, we investigated the extent of penile

150 151Int. J. Immunopathol. Pharmacol.
vascular damage with the assessment of Duplex ultrasonography properties of cavernous vasculature (6). This study shows that penile fibrosis occurs in almost all sclerodermic patients, irrespective of clinical signs of erectile dysfunction. These results appear to confirm a biopsy evaluation performed on a single patient which is reported in literature (7). Despite the absence of indirect signs of early atherosclerosis, the presence of penile fibrosis may determine incomplete penile arterial and smooth muscle cell relaxation, thus resulting in ED. Duplex ultrasonography gives useful information on the penile structure and the way in which large vessels function (i.e. cavernous arteries), but it is well-known that these structures are involved in the latter fibrotic stage of the disease.
In another series of studies we used functional infrared imaging to differentiate patients with Primary Raynaud’s Phenomenon (PRP), from secondary to scleroderma Raynaud’s Phenomenon (SSc), and healthy controls. The response of fingertip temperature to standardized mild cold stress and the pattern of the cutaneous temperature of the hands clearly identified the differences between PRP, SSc and controls, as far as the local thermoregulatory properties are concerned. (8-10). For all these reasons, we considered evaluating whether penile thermal proprieties of SSc patients differ from healthy controls, using functional infrared imaging, with the assumption that local thermoregulatory properties depend on the microcirculation/endothelial function, and that their modification could represent an early sign of the onset of the disease.
MATERIALS AND METHODS
This study was approved by the Institutional Review Boards and local Ethics Committees of the participating institutions, and all subjects gave their informed consent. Ten male patients suffering from SSc attending the Clinical Immunology and Allergology Unit (“La Sapienza” University, Rome, Italy), aged 33 to 50 years and 10 healthy controls were recruited from a list of volunteers made available by the Department of Clinical Sciences and Bioimaging (“G. d’Annunzio” University Chieti, Italy), and were enrolled in this study. All patients fulfilled the criteria of the American College of Rheumatology (11) and were affected by the diffuse form of the disease, according to the LeRoy
classification system (1). Patient exclusion criteria were: cigarette smoking, current use of immunosuppressive drugs, cardiovascular or neurovascular comorbidity, hypertension, any overt urological and/or andrological dysfunction, and depression.
Healthy controls exclusion criteria were: age more than 50 years, cigarette smoking, cardiovascular or neurovascular disorders, hypertension, any overt urological and/or andrological dysfunction, depression and any kind of therapeutic treatment.
The evaluation of patients and healthy controls included complete medical and sexual history, physical examination, routine (glucose, total cholesterol, creatinin, AST, ALT) blood analysis. Erectile function was investigated by means of the Sexual Health Inventory for Men (SHIM)-International Index of Erectile Function 5 (IIEF5) (12), with normal indexes higher than 21. All the subjects abstained from sexual activity and alcohol for at least 2 days before the measurement session.
Functional infrared imaging was performed using a 3–5 µm digital infrared camera (AEG Aim GmbH, Heilbronn, Germany), with 0.02 second time resolution, 0.1 K temperature sensitivity, and 0.02 K temperature noise. Emissivity of the skin was estimated as ≅ 0.95. The temperatures were blackbody calibrated. Acclimatization of the patient to the measurement room, with standardized temperature, humidity, and ventilation, lasted for at least 20 minutes (13-15).
Evaluation with functional infrared imaging was performed by obtaining penile thermal images, measuring the basal average temperature of the corpora cavernosa (henceforth named corpora), the glans penis, as well as the whole penis, and determining thermal recovery of the penis after mild cold thermal stress. Recording was performed for 5 minutes before and 20 minutes after cooling of the penis; images were acquired every 30 seconds.
Cooling was achieved by applying a dry patch to the penis. Dry patch temperature was set at 10°C. Thermal recovery showed an exponential pattern that can be characterized by the time constant of the best exponential fit and the amplitude of temperature variation. The ratio of amplitude to time constant expresses the recovery rate and depends directly on the thermal properties of the penis and its blood perfusion (14). Participants were seated comfortably during functional infrared imaging. The data was analyzed by using standard t-test. P < α = 0.05 was considered statistically significant.
RESULTS
Clinical and epidemiological data, as well as
A. MERLA ET AL.
150 151Int. J. Immunopathol. Pharmacol.
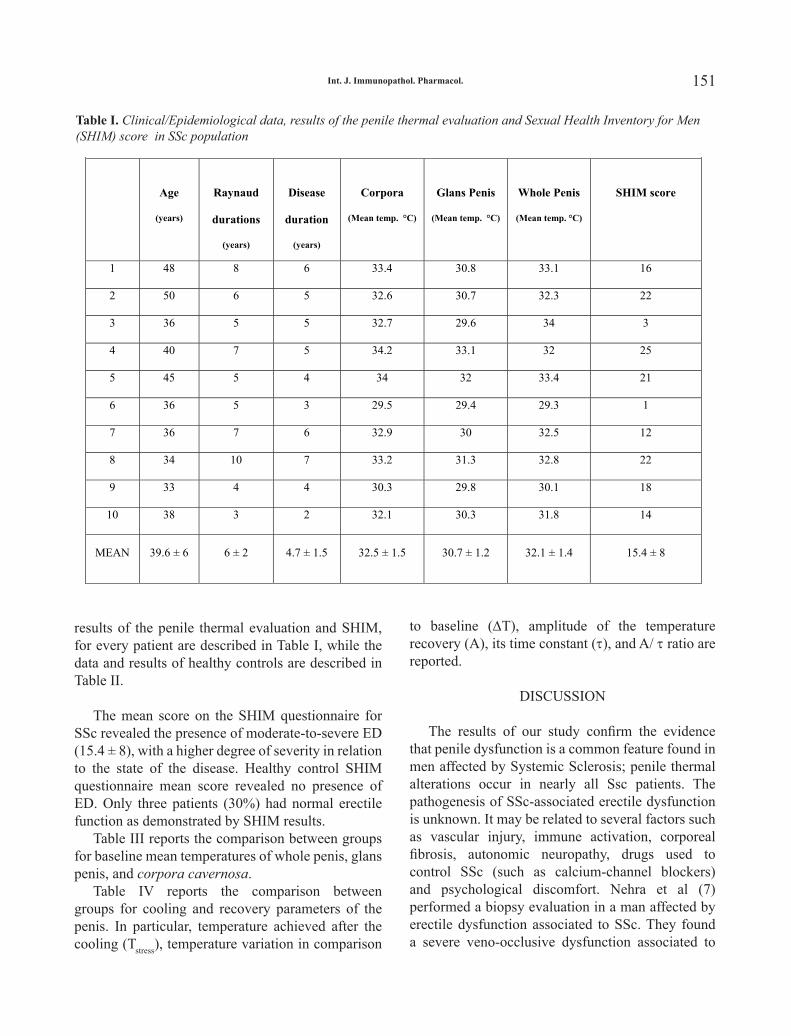
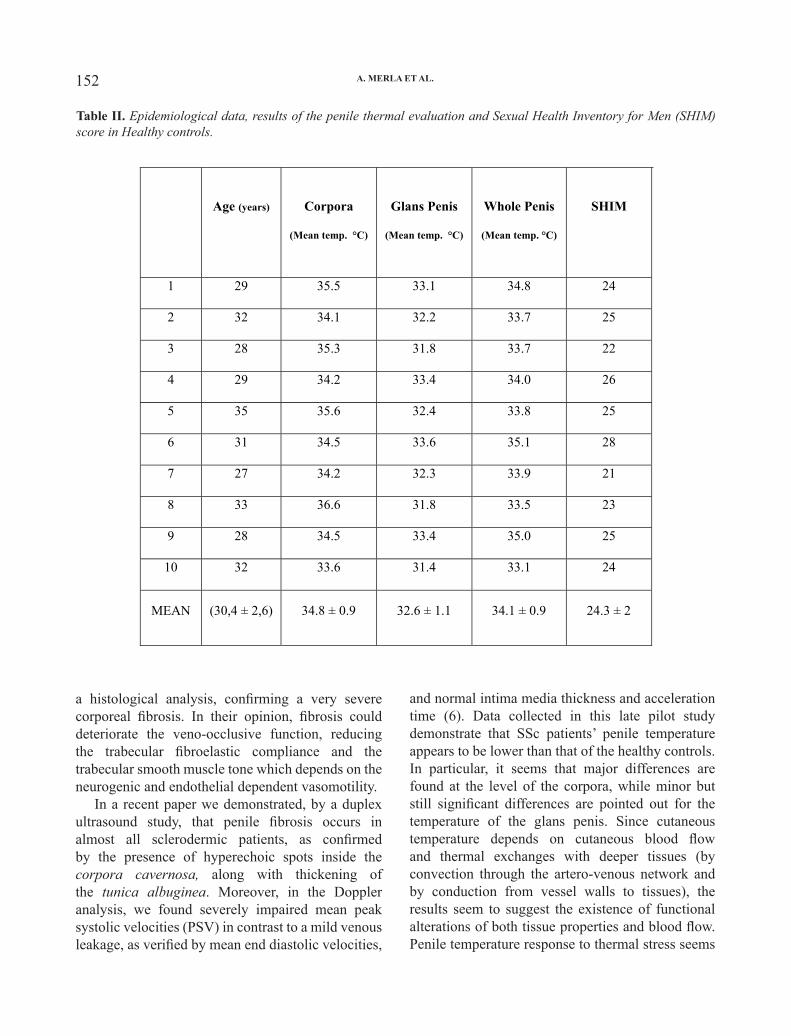
results of the penile thermal evaluation and SHIM, for every patient are described in Table I, while the data and results of healthy controls are described in Table II.
The mean score on the SHIM questionnaire for SSc revealed the presence of moderate-to-severe ED (15.4 ± 8), with a higher degree of severity in relation to the state of the disease. Healthy control SHIM questionnaire mean score revealed no presence of ED. Only three patients (30%) had normal erectile function as demonstrated by SHIM results.
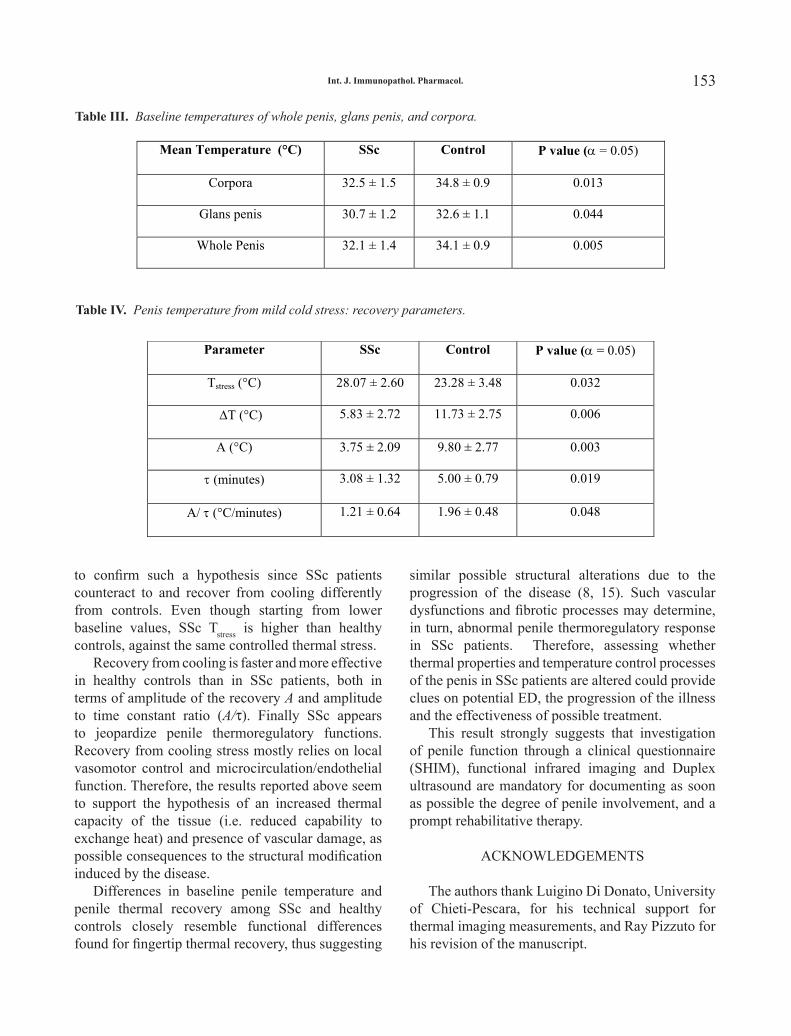
Table III reports the comparison between groups for baseline mean temperatures of whole penis, glans penis, and corpora cavernosa.
Table IV reports the comparison between groups for cooling and recovery parameters of the penis. In particular, temperature achieved after the cooling (Tstress), temperature variation in comparison
to baseline (∆T), amplitude of the temperature recovery (A), its time constant (τ), and A/ τ ratio are reported.
DISCUSSION
The results of our study confirm the evidence that penile dysfunction is a common feature found in men affected by Systemic Sclerosis; penile thermal alterations occur in nearly all Ssc patients. The pathogenesis of SSc-associated erectile dysfunction is unknown. It may be related to several factors such as vascular injury, immune activation, corporeal fibrosis, autonomic neuropathy, drugs used to control SSc (such as calcium-channel blockers) and psychological discomfort. Nehra et al (7) performed a biopsy evaluation in a man affected by erectile dysfunction associated to SSc. They found a severe veno-occlusive dysfunction associated to 5
Table I. Clinical/Epidemiological data, results of the penile thermal evaluation and Sexual Health
Inventory for Men (SHIM) score in SSc population.
Age
(years)
Raynaud
durations
(years)
Disease
duration
(years)
Corpora
(Mean temp. °C)
Glans Penis
(Mean temp. °C)
Whole Penis
(Mean temp. °C)
SHIM score
1 48 8 6 33.4 30.8 33.1 16
2 50 6 5 32.6 30.7 32.3 22
3 36 5 5 32.7 29.6 34 3
4 40 7 5 34.2 33.1 32 25
5 45 5 4 34 32 33.4 21
6 36 5 3 29.5 29.4 29.3 1
7 36 7 6 32.9 30 32.5 12
8 34 10 7 33.2 31.3 32.8 22
9 33 4 4 30.3 29.8 30.1 18
10 38 3 2 32.1 30.3 31.8 14
MEAN 39.6 ± 6 6 ± 2 4.7 ± 1.5 32.5 ± 1.5 30.7 ± 1.2 32.1 ± 1.4 15.4 ± 8
Table I. Clinical/Epidemiological data, results of the penile thermal evaluation and Sexual Health Inventory for Men (SHIM) score in SSc population
152 153Int. J. Immunopathol. Pharmacol.
a histological analysis, confirming a very severe corporeal fibrosis. In their opinion, fibrosis could deteriorate the veno-occlusive function, reducing the trabecular fibroelastic compliance and the trabecular smooth muscle tone which depends on the neurogenic and endothelial dependent vasomotility.
In a recent paper we demonstrated, by a duplex ultrasound study, that penile fibrosis occurs in almost all sclerodermic patients, as confirmed by the presence of hyperechoic spots inside the corpora cavernosa, along with thickening of the tunica albuginea. Moreover, in the Doppler analysis, we found severely impaired mean peak systolic velocities (PSV) in contrast to a mild venous leakage, as verified by mean end diastolic velocities,
and normal intima media thickness and acceleration time (6). Data collected in this late pilot study demonstrate that SSc patients’ penile temperature appears to be lower than that of the healthy controls. In particular, it seems that major differences are found at the level of the corpora, while minor but still significant differences are pointed out for the temperature of the glans penis. Since cutaneous temperature depends on cutaneous blood flow and thermal exchanges with deeper tissues (by convection through the artero-venous network and by conduction from vessel walls to tissues), the results seem to suggest the existence of functional alterations of both tissue properties and blood flow. Penile temperature response to thermal stress seems
Table II. Epidemiological data, results of the penile thermal evaluation and Sexual Health Inventory for Men (SHIM) score in Healthy controls.
6
Table II. Epidemiological data, results of the penile thermal evaluation and
Sexual Health Inventory for Men (SHIM) score in Healthy controls.
Age (years) Corpora
(Mean temp. °C)
Glans Penis
(Mean temp. °C)
Whole Penis
(Mean temp. °C)
SHIM
1 29 35.5 33.1 34.8 24
2 32 34.1 32.2 33.7 25
3 28 35.3 31.8 33.7 22
4 29 34.2 33.4 34.0 26
5 35 35.6 32.4 33.8 25
6 31 34.5 33.6 35.1 28
7 27 34.2 32.3 33.9 21
8 33 36.6 31.8 33.5 23
9 28 34.5 33.4 35.0 25
10 32 33.6 31.4 33.1 24
MEAN (30,4 ± 2,6) 34.8 ± 0.9 32.6 ± 1.1 34.1 ± 0.9 24.3 ± 2
The mean score on the SHIM questionnaire for SSc revealed the presence of moderate-to-
severe ED (15.4 ± 8), with a higher degree of severity in relation to the state of the disease.
Healthy control SHIM questionnaire mean score revealed no presence of ED. Only three patients
(30%) had normal erectile function as demonstrated by SHIM results.
Table III reports the comparison between groups for baseline mean temperatures of whole
penis, glans penis, and corpora cavernosa.
A. MERLA ET AL.
152 153Int. J. Immunopathol. Pharmacol.
to confirm such a hypothesis since SSc patients counteract to and recover from cooling differently from controls. Even though starting from lower baseline values, SSc Tstress is higher than healthy controls, against the same controlled thermal stress.
Recovery from cooling is faster and more effective in healthy controls than in SSc patients, both in terms of amplitude of the recovery A and amplitude to time constant ratio (A/τ). Finally SSc appears to jeopardize penile thermoregulatory functions. Recovery from cooling stress mostly relies on local vasomotor control and microcirculation/endothelial function. Therefore, the results reported above seem to support the hypothesis of an increased thermal capacity of the tissue (i.e. reduced capability to exchange heat) and presence of vascular damage, as possible consequences to the structural modification induced by the disease.
Differences in baseline penile temperature and penile thermal recovery among SSc and healthy controls closely resemble functional differences found for fingertip thermal recovery, thus suggesting
similar possible structural alterations due to the progression of the disease (8, 15). Such vascular dysfunctions and fibrotic processes may determine, in turn, abnormal penile thermoregulatory response in SSc patients. Therefore, assessing whether thermal properties and temperature control processes of the penis in SSc patients are altered could provide clues on potential ED, the progression of the illness and the effectiveness of possible treatment.
This result strongly suggests that investigation of penile function through a clinical questionnaire (SHIM), functional infrared imaging and Duplex ultrasound are mandatory for documenting as soon as possible the degree of penile involvement, and a prompt rehabilitative therapy.
ACKNOWLEDGEMENTS
The authors thank Luigino Di Donato, University of Chieti-Pescara, for his technical support for thermal imaging measurements, and Ray Pizzuto for his revision of the manuscript.
Table III. Baseline temperatures of whole penis, glans penis, and corpora.
7
Table IV reports the comparison between groups for cooling and recovery parameters of the
penis. In particular, temperature achieved after the cooling (Tstress), temperature variation in
comparison to baseline (�T), amplitude of the temperature recovery (A), its time constant (�),
and A/�� ratio are reported.
DISCUSSION
The results of our study confirm the evidence that penile dysfunction is a common feature
found in men affected by Systemic Sclerosis; penile thermal alterations occur in nearly all Ssc
patients. The pathogenesis of SSc-associated erectile dysfunction is unknown. It may be related
to several factors such as vascular injury, immune activation, corporeal fibrosis, autonomic
neuropathy, drugs used to control SSc (such as calcium-channel blockers) and psychological
discomfort. Nehra et al (7) performed a biopsy evaluation in a man affected by erectile
dysfunction associated to SSc. They found a severe veno-occlusive dysfunction associated to a
Table III. Baseline temperatures of whole penis, glans penis, and corpora.
Mean Temperature (°C) SSc Control P value (� = 0.05)
Corpora 32.5 ± 1.5 34.8 ± 0.9 0.013
Glans penis 30.7 ± 1.2 32.6 ± 1.1 0.044
Whole Penis 32.1 ± 1.4 34.1 ± 0.9 0.005
Table IV. Penis temperature from mild cold stress: recovery parameters.
Parameter SSc Control P value (� = 0.05)
Tstress (°C) 28.07 ± 2.60 23.28 ± 3.48 0.032
�����T (°C) 5.83 ± 2.72 11.73 ± 2.75 0.006
A (°C) 3.75 ± 2.09 9.80 ± 2.77 0.003
� (minutes) 3.08 ± 1.32 5.00 ± 0.79 0.019
A/ � (°C/minutes) 1.21 ± 0.64 1.96 ± 0.48 0.048
Table IV. Penis temperature from mild cold stress: recovery parameters.
7
Table IV reports the comparison between groups for cooling and recovery parameters of the
penis. In particular, temperature achieved after the cooling (Tstress), temperature variation in
comparison to baseline (�T), amplitude of the temperature recovery (A), its time constant (�),
and A/�� ratio are reported.
DISCUSSION
The results of our study confirm the evidence that penile dysfunction is a common feature
found in men affected by Systemic Sclerosis; penile thermal alterations occur in nearly all Ssc
patients. The pathogenesis of SSc-associated erectile dysfunction is unknown. It may be related
to several factors such as vascular injury, immune activation, corporeal fibrosis, autonomic
neuropathy, drugs used to control SSc (such as calcium-channel blockers) and psychological
discomfort. Nehra et al (7) performed a biopsy evaluation in a man affected by erectile
dysfunction associated to SSc. They found a severe veno-occlusive dysfunction associated to a
Table III. Baseline temperatures of whole penis, glans penis, and corpora.
Mean Temperature (°C) SSc Control P value (� = 0.05)
Corpora 32.5 ± 1.5 34.8 ± 0.9 0.013
Glans penis 30.7 ± 1.2 32.6 ± 1.1 0.044
Whole Penis 32.1 ± 1.4 34.1 ± 0.9 0.005
Table IV. Penis temperature from mild cold stress: recovery parameters.
Parameter SSc Control P value (� = 0.05)
Tstress (°C) 28.07 ± 2.60 23.28 ± 3.48 0.032
�����T (°C) 5.83 ± 2.72 11.73 ± 2.75 0.006
A (°C) 3.75 ± 2.09 9.80 ± 2.77 0.003
� (minutes) 3.08 ± 1.32 5.00 ± 0.79 0.019
A/ � (°C/minutes) 1.21 ± 0.64 1.96 ± 0.48 0.048
154 INTERNATIONAL JOURNAL OF IMMUNOPATHOLOGY AND PHARMACOLOGY Vol. 20, no. 1, 0-0 (2007)
0394-6320 (2006)Copyright © by BIOLIFE, s.a.s.
This publication and/or article is for individual use only and may not be furtherreproduced without written permission from the copyright holder.
Unauthorized reproduction may result in financial and other penalties155
REFERENCES
1. LeRoy E.C., C. Black, R. Fleischmajer, S. Jablonska, T. Krieg, T.A. Medsger Jr, et al. 1988. Scleroderma (systemic sclerosis): Classification, subsets and pathogenesis. J. Rheumatol. 15:202.
2. Lally E.V. and S.A. Jimenez. 1981. Impotence in progressively systemic sclerosis. Ann. Intern. Med. 95:150.
3. Lally E.V. and S.A. Jimenez. 1990. Erectile failure in systemic sclerosis. N. Engl. J. Med. 322:1398.
4. Lotfi M.A., J. Varga and I.H. Hirsch. 1995. Erectile dysfunction in systemic sclerosis. Urology 45:879.
5. Hong P., J.E. Pope, J.M. Ouimet, E. Rullan and J.R. Seibold. 2004. Erectile dysfunction associated with scleroderma: a case-control study of men with scleroderma and rheumatoid arthritis. J. Rheumatol. 31:508.
6. Aversa A., M. Proietti, R. Bruzziches, F. Salsano and G. Spera. 2005. The penile vasculature in systemic sclerosis: A duplex ultrasound study. J. Sex. Med. 3:554.
7. Nehra A., S.J. Hall, G. Basile, E.B. Bertero, R. Moreland, P. Toselli, A. de las Morenas and I. Goldstein. 1995. Systemic sclerosis and impotence: a clinicopathological correlation. J. Urol. 153:1140.
8. Merla A. and G.L. Romani. 2005. Functional Infrared Imaging in Clinical Applications, in The Biomedical Engineering Handbook, ed. CRC Press, J.D. Bronzino, p. 32.
9. Merla A., G.L. Romani, S. Di Luzio, M. Proietti,
S. Pisarri and S. Salsano. 2002. Raynaud’s Phenomenon: infrared functional imaging applied to diagnosis and drug effects. Int. J. Immunopathol. Pharmacol. 15:41.
10. Merla A., L. Di Donato, S. Pisarri, M. Proietti, F. Salsano and G.L. Romani. 2002. Infrared Functional Imaging Applied to Raynaud’s Phenomenon. IEEE Eng. Med. Biol. Mag. 21:73.
11. Subcommittee for scleroderma criteria of the American Rheumatism Association diagnostic and therapeutic criteria committee. 1980. Preliminary criteria for the classification of systemic sclerosis (scleroderma). Arthritis Rheum. 23:581.
12. Rosen R.C., A. Riley, G. Wagner, I.H. Osterloh, J. Kirkpatrick and A. Mishra. 1997. The International Index of Erectile Function (IIEF): A multidimensional scale for assessment of erectile dysfunction. Urology 49:822.
13. Merla A., A. Ledda, L. Di Donato and G.L. Romani. 2004. Assessment of the effects of the varicocelectomy on the thermoregulatory control of the scrotum. Fertil. Steril. 81:471.
14. Merla A., A. Ledda, L. Di Donato and G.L. Romani. 2002. Use of Infrared Functional Imaging to detect impaired thermoregulatory control in men with asymptomatic varicocele. Fertil. Steril. 78:199.
15. Merla A., L. Di Donato, S. Di Luzio and G.L. Romani. 2002. Quantifying the Relevance and Stage of Disease with the Tau image Technique. IEEE Eng. Med. Biol. Mag. 22:86.
A. MERLA ET AL.
Related Documents











