EDUCATION EXHIBIT 1591 Pelvic Arterial Hemor- rhage in Patients with Pelvic Fractures: Detection with Con- trast-enhanced CT 1 ONLINE-ONLY CME See www.rsna .org/education /rg_cme.html. LEARNING OBJECTIVES After reading this article and taking the test, the reader will be able to: Identify the osse- ous, ligamentous, and vascular anat- omy of the pelvis on axial CT scans. Discuss the roles of contrast-enhanced CT in the detection of ongoing arterial hemorrhage in pa- tients with pelvic fractures. Describe the role of transcatheter emboli- zation for pelvic arte- rial hemorrhage in patients with pelvic fractures. Woong Yoon, MD ● Jae Kyu Kim, MD ● Yong Yeon Jeong, MD ● Jeong Jin Seo, MD ● Jin Gyoon Park, MD ● Heoung Keun Kang, MD Arterial hemorrhage is one of the most serious problems associated with pelvic fractures, and it remains the leading cause of death attribut- able to pelvic fracture. At many trauma centers, contrast material– en- hanced computed tomography (CT) is increasingly used for initial di- agnosis in the evaluation of patients with pelvic fractures. Extravasation of contrast material in the pelvis at contrast-enhanced CT is an accu- rate indicator of ongoing arterial hemorrhage in patients with pelvic fractures. Detection of such extravasation on CT scans can lead to prompt performance of angiographic embolization, which can be life- saving. Furthermore, the site of contrast material extravasation seen at CT corresponds well to the site of bleeding seen at angiography. This correspondence enables the interventional radiologist to selectively study the arteries most likely to be injured and therefore potentially reduce the patient’s morbidity and mortality. Knowledge of the rel- evant pelvic anatomy, including the osseous, ligamentous, and espe- cially axial vascular anatomy, is essential for understanding the rela- tionship between a site of contrast material extravasation at CT and the specific injured artery visualized at angiography. © RSNA, 2004 Abbreviation: TAE transcatheter arterial embolization Index terms: Arteries, iliac, 986.92 ● Arteries, injuries, 986.41 ● Arteries, therapeutic embolization, 986.1264 ● Hemorrhage, CT, 986.12912 ● Pelvis, fractures, 33.41, 44.41 RadioGraphics 2004; 24:1591–1606 ● Published online 10.1148/rg.246045028 ● Content Codes: 1 From the Department of Diagnostic Radiology, Chonnam National University Hospital, Chonnam National University Medical School, 8 Hak-dong, Dong-Ku, Gwangju 501–757, South Korea. Presented as an education exhibit at the 2003 RSNA scientific assembly. Received March 4, 2004; revi- sion requested April 7; received and accepted April 26. All authors have no financial relationships to disclose. Address correspondence to W.Y. (e-mail: [email protected]). See the commentary by Savage et al following this article. © RSNA, 2004 RadioGraphics

Welcome message from author
This document is posted to help you gain knowledge. Please leave a comment to let me know what you think about it! Share it to your friends and learn new things together.
Transcript

EDUCATION EXHIBIT 1591
Pelvic Arterial Hemor-rhage in Patients withPelvic Fractures:Detection with Con-trast-enhanced CT1
ONLINE-ONLYCME
See www.rsna.org/education/rg_cme.html.
LEARNINGOBJECTIVESAfter reading thisarticle and takingthe test, the reader
will be able to:
� Identify the osse-ous, ligamentous,and vascular anat-omy of the pelvis onaxial CT scans.
� Discuss the roles ofcontrast-enhancedCT in the detectionof ongoing arterialhemorrhage in pa-tients with pelvicfractures.
� Describe the role oftranscatheter emboli-zation for pelvic arte-rial hemorrhage inpatients with pelvicfractures.
Woong Yoon, MD ● Jae Kyu Kim, MD ● Yong Yeon Jeong, MD ● JeongJin Seo, MD ● Jin Gyoon Park, MD ● Heoung Keun Kang, MD
Arterial hemorrhage is one of the most serious problems associatedwith pelvic fractures, and it remains the leading cause of death attribut-able to pelvic fracture. At many trauma centers, contrast material–en-hanced computed tomography (CT) is increasingly used for initial di-agnosis in the evaluation of patients with pelvic fractures. Extravasationof contrast material in the pelvis at contrast-enhanced CT is an accu-rate indicator of ongoing arterial hemorrhage in patients with pelvicfractures. Detection of such extravasation on CT scans can lead toprompt performance of angiographic embolization, which can be life-saving. Furthermore, the site of contrast material extravasation seen atCT corresponds well to the site of bleeding seen at angiography. Thiscorrespondence enables the interventional radiologist to selectivelystudy the arteries most likely to be injured and therefore potentiallyreduce the patient’s morbidity and mortality. Knowledge of the rel-evant pelvic anatomy, including the osseous, ligamentous, and espe-cially axial vascular anatomy, is essential for understanding the rela-tionship between a site of contrast material extravasation at CT and thespecific injured artery visualized at angiography.©RSNA, 2004
Abbreviation: TAE � transcatheter arterial embolization
Index terms: Arteries, iliac, 986.92 ● Arteries, injuries, 986.41 ● Arteries, therapeutic embolization, 986.1264 ● Hemorrhage, CT, 986.12912 ● Pelvis,fractures, 33.41, 44.41
RadioGraphics 2004; 24:1591–1606 ● Published online 10.1148/rg.246045028 ● Content Codes:
1From the Department of Diagnostic Radiology, Chonnam National University Hospital, Chonnam National University Medical School, 8 Hak-dong,Dong-Ku, Gwangju 501–757, South Korea. Presented as an education exhibit at the 2003 RSNA scientific assembly. Received March 4, 2004; revi-sion requested April 7; received and accepted April 26. All authors have no financial relationships to disclose. Address correspondence to W.Y.(e-mail: [email protected]).
See the commentary by Savage et al following this article.
©RSNA, 2004
Radio
Gra
phic
s

IntroductionPelvic fractures have been known to occur in 4%–9.3% of patients with blunt trauma (1,2). Thesefractures should be considered a marker of severeinjury and are often associated with significantinjuries to the abdominal and pelvic organs. Thereported prevalence of associated organ injuriesranges from 11% to 20.3% (1).
Pelvic fractures have long been associated withsignificant mortality, which ranges from 5.6% to15% (1–7). Recent studies, by well-organizedtrauma centers, have shown that the mortalityrate is still high in patients who have hypotensionattributable to pelvic fractures. The reportedmortality rate for pelvic fracture patients withhemorrhagic shock ranges from 36.4% to 54%(7,8).
Life-threatening hemorrhage related to pelvicfractures may originate from fractured bone, thepelvic venous plexus, major pelvic veins, and/oriliac arterial branches. Pelvic fracture hemorrhagecaused by venous injury and the fracture site canbe effectively treated with external fixation by re-ducing the pelvic volume and stabilizing the frac-ture (9). Arterial hemorrhage is the most seriousproblem associated with pelvic fractures (5), andit remains the leading cause of death. Several au-thors have suggested that the external fixation isnot likely to be sufficient to stop arterial bleeding.Urgent angiography and subsequent transcatheterembolization are currently accepted as the mosteffective methods for controlling ongoing arterialbleeding in pelvic fractures (3,5,10).
Patient death caused by the hemorrhage of apelvic fracture frequently occurs within the first24 hours of injury. The early identification of pa-tients who might benefit from angiographic em-bolization could reduce blood loss, prevent latecomplications related to transfusion, and improveoutcome (2). Several investigators have tried todefine clinical or radiologic predictors to deter-mine which patients with pelvic fractures are athigh risk of arterial hemorrhage and thus mightbenefit from angiography and embolization.These predictors include the response to initialresuscitation (7), pelvic fracture pattern accord-ing to radiography results (8,11), the volume andlocation of pelvic hematoma according to the re-sults of computed tomography (CT) (6,12), andthe extravasation of injected contrast materialaccording to the results of a contrast-enhanced
CT examination (5,13–16). In patients with bothhypotension and pelvic fracture, a lack of re-sponse to initial resuscitation and contrast mate-rial extravasation seen on a CT scan are the mostreliable indicator of significant arterial bleedingregardless of the fracture pattern (7).
Several studies have shown that the presence ofcontrast material extravasation on contrast-en-hanced CT scans is a strong predictor of arterialbleeding later seen during angiography (13–16).Moreover, the presence of contrast material ex-travasation can be an indicator of injury to a spe-cific artery passing through the region of the pel-vis where the extravasation is noted on CT scans.Interventional radiologists can use the location ofcontrast material extravasation on CT scans todirect the performance of more specific selectiveand superselective investigations of arteries athigh risk for injury.
In this article, we describe the role of contrast-enhanced CT in predicting arterial hemorrhage inpatients with pelvic fractures. The specific topicsdiscussed are the relevant pelvic anatomy, theaxial CT anatomy of the internal iliac artery andits branches, the correlation between findings of
Figure 1. Angiogram shows the internal iliac arteryand its branches: the iliolumbar artery (1), lateral sacralarteries (2), superior gluteal artery (3), obturator artery(4), internal pudendal artery (5), inferior gluteal artery(6), and vesical arteries (7).
1592 November-December 2004 RG f Volume 24 ● Number 6
Radio
Gra
phic
s

contrast-enhanced CT and those of angiography(relationship between a CT-determined extrava-sation site and an angiographically determinedbleeding site), and transcatheter arterial emboli-zation (TAE) in patients with arterial hemorrhageand pelvic fractures.
Essential Pelvic AnatomyThe internal iliac artery, which is also known asthe hypogastric artery, begins at the bifurcation ofthe common iliac artery, anterior to the sacroiliacjoint at the level of the lumbosacral disk. It sup-plies the walls of the pelvis, the pelvic viscera, thebuttock, the genital organ, and part of the medialthigh. The internal iliac artery divides into an an-
terior and posterior trunk. The branches of theinternal iliac artery may be grouped as follows:(a) Visceral branches: umbilical, superior vesical,inferior vesical, middle rectal, uterine, and vagi-nal. (b) Branches to the limb and perineum: su-perior gluteal, inferior gluteal, obturator, and in-ternal pudendal. (c) Somatic segmental branches:iliolumbar and lateral sacral. Usually, the superiorgluteal and the two somatic segmental branchesstem from the posterior division and the othersfrom the anterior division (Figs 1, 2).
The internal iliac artery and its branches have aclose relationship with the pelvic ligaments andforamina throughout their course in the pelvis.Knowledge of the precise anatomy of pelvic bonyand ligamentous structures is required to under-stand the mechanism of arterial injury in patientswith acute pelvic trauma. The door throughwhich all vessels and nerves pass on leaving thepelvis to enter the gluteal region is the greater sci-atic foramen (Fig 3). It is bounded by the sacrumposteriorly, by the sacrospinous ligament inferi-orly, by the ischium anteriorly, and by the iliumsuperiorly. The sacrospinous ligament attachesthe lateral and inferior aspects of the sacrum tothe ipsilateral ischial spine, and it forms the infe-rior border of the greater sciatic foramen belowthe greater sciatic notch of the hip bone. The piri-formis muscle arises from the anterior sacrum andpasses out of the pelvis through the greater sciaticforamen. Coursing laterally, this muscle insertson the greater trochanter of the femur (Fig 4).
Figures 2, 3. (2) Drawing of the left hemipelvis shows the major branches of the internal iliac artery. IS � ischialspine, IT � ischial tuberosity. (3) Drawing of the right hemipelvis shows the anatomy of the greater (G) and lesser(L) sciatic foramina.
Figure 4. Drawing of the posterior righthemipelvis shows the gluteal arteries exiting thepelvis. GT � greater trochanter of the femur,IS � ischial spine, IT � ischial tuberosity.
RG f Volume 24 ● Number 6 Yoon et al 1593
Radio
Gra
phic
s

The piriformis muscle separates the greater sciaticforamen into superior and inferior portions.
Superior gluteal vessels and nerves are locatedat the upper border of the piriformis muscle. Infe-rior gluteal vessels and nerves, internal pudendalvessels and nerves, and the sciatic nerve are lo-cated at the lower border of the piriformis muscle.Internal pudendal vessels and nerves leave thepelvis through the inferior part of the greater sci-atic foramen and at once reenter through thelesser sciatic foramen (Figs 2, 4).
The lesser sciatic foramen is bounded by theischial tuberosity anteriorly, by the ischial spineand sacrospinous ligament superiorly, and by thesacrotuberous ligament posteriorly (Fig 3). Thesacrotuberous ligament attaches the lateral sa-crum to the ipsilateral ischial tuberosity. The ver-tical band of this ligament extends up to the pos-terior superior spine of the ilium, where it blendswith the vertical bands of the posterior sacroiliacligament.
The obturator foramen is a large, rounded ap-erture that separates the pubis anterosuperiorlyfrom the ischium posteroinferiorly. The fibrous
obturator membrane completely covers the obtu-rator foramen except superiorly, where a deepgroove allows communication between the pelvisand the anterior thigh. Through this obturatorcanal, the obturator vessels and nerves exit thepelvis (Figs 2, 3).
It is essential to subsequently apply the de-scribed anatomy to axial CT images for the inter-pretation and prediction of arterial injury in pa-tients with pelvic fracture hemorrhage. On arterialCT images from a multidetector CT scanner, thefine branches of the internal iliac artery can beeasily traced from its origin through their coursesin the pelvis.
Vascular Anatomy at Axial CTThe increasing use of contrast-enhanced CT inthe evaluation and management of patients with
Figures 5–7. Iliolumbar artery. (5) CT scan shows theright iliolumbar artery (arrow) arising from the posterolat-eral aspect of the internal iliac artery (arrowhead). I � ili-acus muscle, Pm � psoas major muscle. (6) CT scanshows the iliolumbar artery (arrows) running anterior tothe sacroiliac joint. Pm � psoas major muscle. (7) CTscan shows the iliolumbar artery, which divides into aniliac branch (arrows) running anterior to the iliacus mus-cle (I) and a lumbar branch (arrowhead) ascending ven-tral to the sacrum.
1594 November-December 2004 RG f Volume 24 ● Number 6
Radio
Gra
phic
s

pelvic fractures necessitates a greater knowledgeof the relevant pelvic anatomy, including thebony, ligamentous, and especially axial vascularanatomy. Knowledge of axial CT vascular anat-omy of the pelvis is essential for understandingthe relationship between a contrast material ex-travasation site seen on a CT scan and the spe-cific injured arteries seen during angiography.Contrast-enhanced CT studies performed with amultidetector scanner can provide a clear imageof the branches of the internal iliac artery andtheir course in relation to the pelvic bony andligamentous structures.
The iliolumbar artery is usually the first branchof the internal iliac artery, and it arises from theposterior division. It courses upward and laterallyanterior to the sacroiliac joint and divides into alumbar and an iliac branch just above the pelvic
inlet and behind the psoas major muscle (Figs5–7). The iliac branch of the iliolumbar arteryruns laterally anterior to the iliacus muscle. Itsupplies the iliacus muscle, the gluteal and ab-dominal muscles, and the ilium. The iliolumbarartery is known to be the largest nutrient artery tothe ilium. The lumbar branch of the iliolumbarartery ascends anterior to the sacral ala and lateralto the L5 body.
The lateral sacral arteries arise from the poste-rior trunk of the internal iliac artery; there areusually two arteries, a superior and an inferior.They supply branches to the anterior surface ofthe sacrum, the sacral foramina and sacral canal,and the skin and muscles of the dorsal surface ofthe sacrum (Figs 8–10). On CT scans, the lateralsacral arteries are seen to descend along the sa-crum and divide into branches that enter the sa-cral foramina.
The superior gluteal artery is the largest branchof the internal iliac artery. It exits from the pelvisthrough the greater sciatic foramen, above thesuperior border of the piriformis muscle. On CTimages, it is located posterior to the ilium andsuperior to the piriformis muscle at the greatersciatic foramen. After leaving the pelvis, it dividesinto superficial and deep branches, which are
Figures 8–10. Lateral sacral arteries. (8) CT scanshows the superior lateral sacral artery (arrow) arisingfrom the posterior trunk of the internal iliac artery (arrow-head) and extending into a sacral foramen. (9) CT scanobtained inferior to 8 shows the inferior lateral sacral ar-tery (arrow). (10) CT scan shows bilateral sacral arteries(arrows) running downward anterior to the sacrum.
RG f Volume 24 ● Number 6 Yoon et al 1595
Radio
Gra
phic
s

Figures 11–16. Superior and inferior gluteal arteries. (11) CT scan shows the superior gluteal artery arising fromthe posterior division of the internal iliac artery (arrow). (12) CT scan obtained inferior to 11 shows the superior glu-teal artery (arrow) exiting the pelvis through the greater sciatic foramen, posterior to the ilium (I) and above the piri-formis muscle (P). (13) CT scan shows the superficial (arrows) and deep (arrowheads) branches of the superior glu-teal artery. The superficial branch runs between the gluteus maximus (1) and gluteus medius (2) muscles. The deepbranch runs between the gluteus medius (2) and gluteus minimus (3) muscles. (14) CT scan shows the inferior glu-teal artery (arrow) approaching the greater sciatic foramen, anterior to the piriformis muscle. (15) CT scan obtainedinferior to 14 shows the inferior gluteal artery (solid arrow) leaving the pelvis through the lower part of the greatersciatic foramen, above the sacrospinous ligament (arrowheads) and posterior to the ischial spine (S). Note the ac-companying internal pudendal artery (open arrow). (16) CT scan shows the inferior gluteal artery (arrow), whichtravels down the posterior buttock and is covered by the gluteus maximus muscle (M).
1596 November-December 2004 RG f Volume 24 ● Number 6
Radio
Gra
phic
s
noted in the fat planes between gluteus muscleson CT scans (Figs 11–13).
The inferior gluteal artery leaves the pelvis to-gether with the internal pudendal artery through thelower part of the greater sciatic foramen, betweenthe piriformis muscle and the coccygeus muscle. Itis distributed to the buttocks and back of the thighand continues down the posterior thigh. On CTscans, the inferior gluteal artery is seen anterior tothe piriformis muscle, posterior to the ischial spine,and above the sacrospinous ligament at the greatersciatic foramen. It travels down the posterior but-tock and is covered by the gluteus maximus muscleafter leaving the pelvis (Figs 14–16).
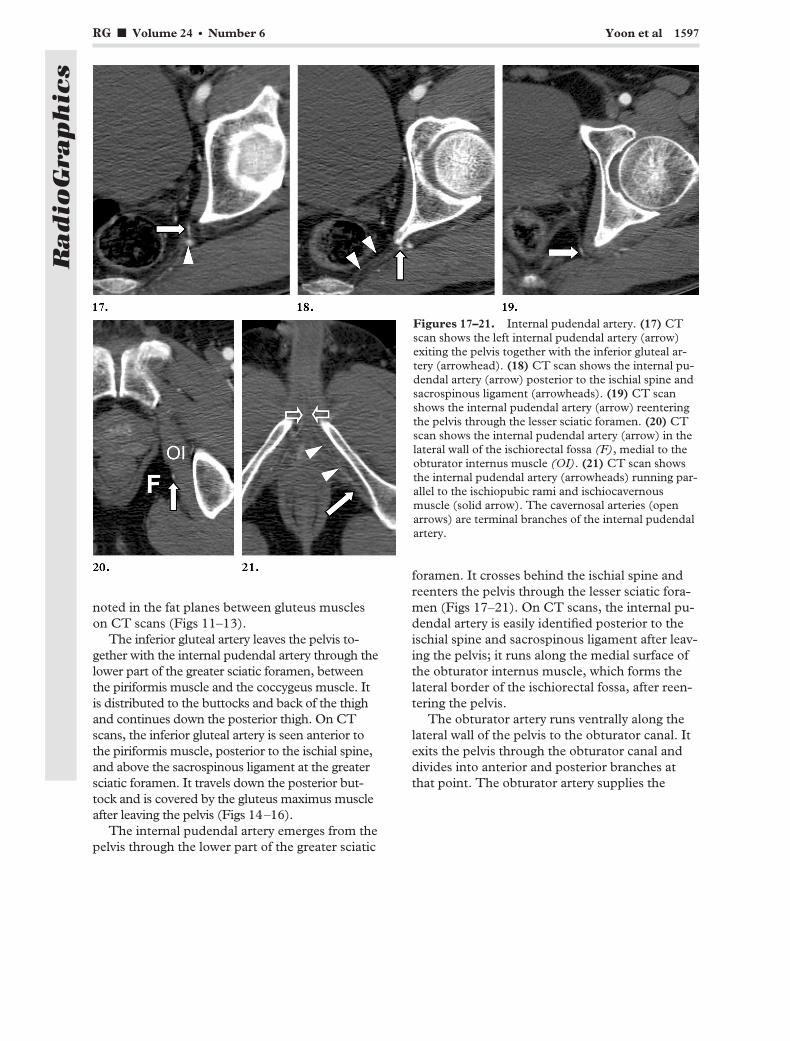
The internal pudendal artery emerges from thepelvis through the lower part of the greater sciatic
foramen. It crosses behind the ischial spine andreenters the pelvis through the lesser sciatic fora-men (Figs 17–21). On CT scans, the internal pu-dendal artery is easily identified posterior to theischial spine and sacrospinous ligament after leav-ing the pelvis; it runs along the medial surface ofthe obturator internus muscle, which forms thelateral border of the ischiorectal fossa, after reen-tering the pelvis.
The obturator artery runs ventrally along thelateral wall of the pelvis to the obturator canal. Itexits the pelvis through the obturator canal anddivides into anterior and posterior branches atthat point. The obturator artery supplies the
Figures 17–21. Internal pudendal artery. (17) CTscan shows the left internal pudendal artery (arrow)exiting the pelvis together with the inferior gluteal ar-tery (arrowhead). (18) CT scan shows the internal pu-dendal artery (arrow) posterior to the ischial spine andsacrospinous ligament (arrowheads). (19) CT scanshows the internal pudendal artery (arrow) reenteringthe pelvis through the lesser sciatic foramen. (20) CTscan shows the internal pudendal artery (arrow) in thelateral wall of the ischiorectal fossa (F), medial to theobturator internus muscle (OI). (21) CT scan showsthe internal pudendal artery (arrowheads) running par-allel to the ischiopubic rami and ischiocavernousmuscle (solid arrow). The cavernosal arteries (openarrows) are terminal branches of the internal pudendalartery.
RG f Volume 24 ● Number 6 Yoon et al 1597
Radio
Gra
phic
s

muscles around the hip (Figs 22–24). On CT im-ages, the artery runs along the anterior pelvicsidewall, medial to the upper portion of the obtu-rator internus muscle, and it has a close relation-ship to the acetabulum. It is easily seen in the ob-turator canal as it divides into anterior and poste-rior branches.
It is not easy to identify the visceral branches ofthe internal iliac artery on CT images, except forthe uterine artery. The uterine artery extends tothe uterine cervix within the broad ligament andruns cephalad along the uterine body, anastomos-ing with the ovarian artery. On CT images, theuterine artery and its branches have a typicalcorkscrew appearance within the broad ligament.The superior vesical artery can be seen lateral tothe bladder on CT images. The inferior vesicalartery is rarely visualized on CT images (Figs25, 26).
CT-AngiographicCorrelation of Arte-rial Hemorrhage Re-
lated to Pelvic FracturesContrast-enhanced CT has been reported to bean accurate, noninvasive technique for identifyingongoing arterial hemorrhage in patients with pel-vic fractures (13–16). The presence of the ex-
travasation of contrast materials on contrast-en-hanced CT scans is highly predictive of arterialinjury that will require angiographic embolization(15) and has been found to be a reliable indicatorof arterial hemorrhage, with a sensitivity of 66%–90%, a specificity of 85%–98%, and an accuracyof 87%–98% being reported (5,14–16). It is wellknown that extravasated contrast material can bedistinguished from clotted blood by measuringCT attenuation. Shanmuganathan et al (13) re-ported that the CT attenuation of active contrastmaterial extravasation ranged from 85 to 370 HU(mean, 132 HU), whereas clotted blood revealeda CT attenuation range of 40–70 HU (mean, 51HU).
The detection of contrast material extravasa-tion on CT scans facilitates timely, life-savingangiographic embolization. Furthermore, the siteof contrast material extravasation seen on CTscans corresponds well to the site of bleeding seenduring angiography in patients with pelvic frac-ture hemorrhage. Thus, it enables the interven-
Figures 22–24. Obturator artery. (22) CT scan showsthe obturator artery (arrow) running along the pelvic side-wall, close to the acetabulum. B � urinary bladder, GM �gluteus maximus, R � rectum. (23) CT scan shows theobturator artery (arrow) within the obturator canal beforeleaving the pelvis. GM � gluteus maximus, SPR � supe-rior pubic ramus. (24) CT scan shows the obturator arterydividing into anterior and posterior branches (arrows) inthe obturator canal.
1598 November-December 2004 RG f Volume 24 ● Number 6
Radio
Gra
phic
s
tional radiologist to selectively study the arteriesthat are most likely to be bleeding. This can leadto more rapid transcatheter embolization, whichhas the potential to reduce a patient’s morbidityand mortality.
Recently, the introduction of multidetectorhelical CT has markedly decreased the time re-quired for scanning, and it has now become a di-agnostic modality of choice in the evaluation ofpatients with pelvic fractures in many trauma cen-ters, even in patients with some degree of hemo-dynamic instability.
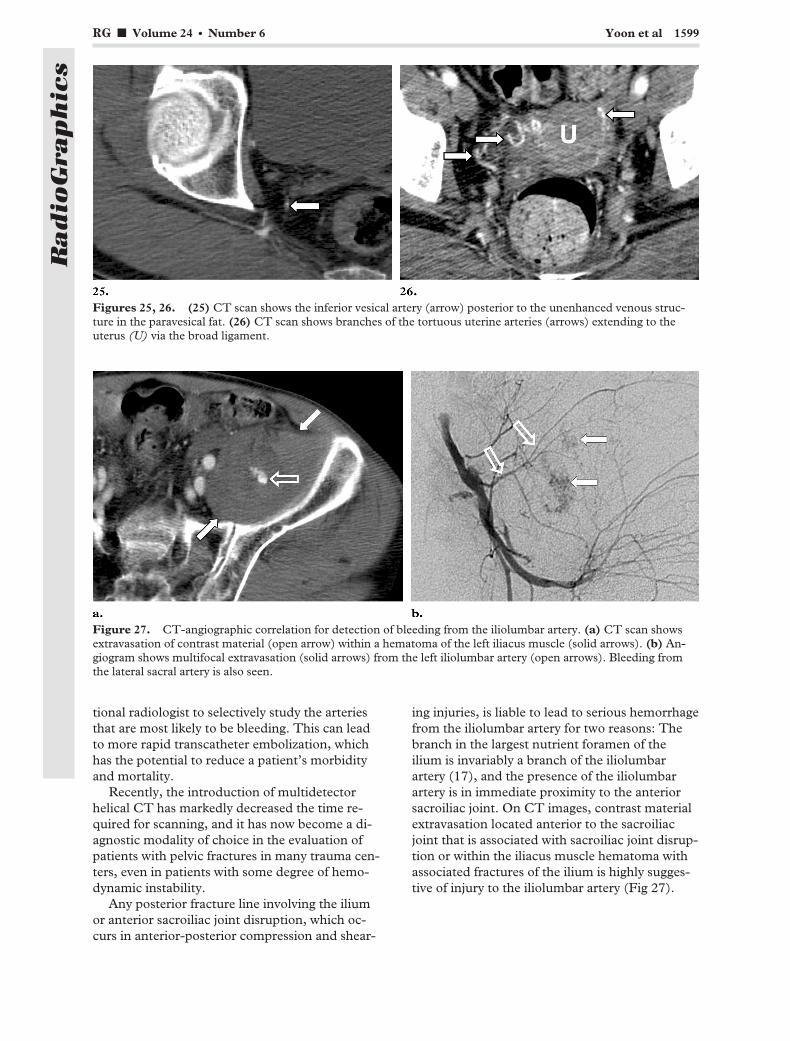
Any posterior fracture line involving the iliumor anterior sacroiliac joint disruption, which oc-curs in anterior-posterior compression and shear-
ing injuries, is liable to lead to serious hemorrhagefrom the iliolumbar artery for two reasons: Thebranch in the largest nutrient foramen of theilium is invariably a branch of the iliolumbarartery (17), and the presence of the iliolumbarartery is in immediate proximity to the anteriorsacroiliac joint. On CT images, contrast materialextravasation located anterior to the sacroiliacjoint that is associated with sacroiliac joint disrup-tion or within the iliacus muscle hematoma withassociated fractures of the ilium is highly sugges-tive of injury to the iliolumbar artery (Fig 27).
Figures 25, 26. (25) CT scan shows the inferior vesical artery (arrow) posterior to the unenhanced venous struc-ture in the paravesical fat. (26) CT scan shows branches of the tortuous uterine arteries (arrows) extending to theuterus (U) via the broad ligament.
Figure 27. CT-angiographic correlation for detection of bleeding from the iliolumbar artery. (a) CT scan showsextravasation of contrast material (open arrow) within a hematoma of the left iliacus muscle (solid arrows). (b) An-giogram shows multifocal extravasation (solid arrows) from the left iliolumbar artery (open arrows). Bleeding fromthe lateral sacral artery is also seen.
RG f Volume 24 ● Number 6 Yoon et al 1599
Radio
Gra
phic
s

Posterior transsacral fractures or a fracture lineinvolving the sacral foramina, through which thelateral sacral arteries exit the pelvis, is prone tocause injury of the lateral sacral arteries. The in-jury of the lateral sacral arteries is commonly as-
sociated with lateral compression pelvic fracturesor vertical shear injury. On CT images, contrastmaterial extravasation noted within the presacralhematoma associated with a fracture line that in-volves the sacral foramina is highly indicative ofinjury to the lateral sacral arteries (Fig 28).
Figure 28. CT-angiographic correlation for detection of bleeding from the lateral sacral artery. (a) CT scanshows a comminuted fracture of the sacrum with extravasation of contrast material (arrows) anterior to the sa-crum. (b) Left common iliac angiogram shows bleeding from the superior lateral sacral artery (arrow).
Figure 29. CT-angiographic correlation for detection of bleeding from the superior gluteal artery. (a) CT scanshows a comminuted fracture of the right ischium and extravasation of contrast material (arrow) at the level of thesuprapiriformis compartment of the greater sciatic foramen. (b) Angiogram shows cutoff of the superior gluteal arteryat the origin site with active bleeding (arrow).
1600 November-December 2004 RG f Volume 24 ● Number 6
Radio
Gra
phic
s

The superior gluteal artery can be injured bythe sharp fascia of the piriformis muscle as it exitsthe pelvis through the greater sciatic foramenabove the piriformis muscle (Fig 29). Outside thepelvis, the superficial and deep branches of thesuperior gluteal artery can be traumatized whenthe gluteal muscles are severely contused, as incases of anterior-posterior compression injury (9).The main branch of the inferior gluteal artery canbe injured as it exits the pelvis just posterior andsuperior to the midportion of the sacrospinousligament. Fracture lines involving the greater sci-atic foramen, the superior part of the ischial tu-berosity, and the ischial spine are prone to causeinjury of both the superior and inferior glutealarteries. On CT images, contrast material ex-travasation within the gluteal hematoma is indica-tive of an injury to the superior gluteal artery.
The internal pudendal artery can be trauma-tized in anterior-posterior compression, the so-called “open-book” fracture, type II and III in-jury. Fractures of the inferior ramus of the pubicbone may be responsible for injury to the internalpudendal artery because of its close proximity tothe ischiopubic ramus. Fractures that involve thelesser sciatic foramen can also lead to an injury ofthe internal pudendal artery. On CT images, con-
trast material extravasation seen in the region ofthe ischiorectal fossa or urogenital diaphragm fatplane that is associated with diastasis of the sym-physis pubis or vertical fractures through the is-chiopubic ramus is highly indicative of injury tothe internal pudendal artery (Fig 30).
The branches of the anterior and posterior di-visions of the obturator artery supply the superiorpart of the surroundings of the obturator foramenand the anteroinferior and posteroinferior parts ofthe acetabulum. Thus, fracture lines involving thesuperior part of the obturator foramen, the supe-rior pubic ramus, or the pubic acetabulum areprone to cause injury to the obturator artery. OnCT images, contrast material extravasation seenin the region of the pelvic sidewall or within anobturator internus muscle hematoma that is asso-ciated with fractures involving the superior pubicramus or pubic acetabulum is highly suggestive ofinjury to the obturator artery (Fig 31). Pelvic arte-rial bleeding due to injury of visceral branches inpatients with pelvic fracture is quite rare. Extrava-sation of contrast material in the bladder wall can
Figure 30. CT-angiographic correlation for detection of bleeding from the internal pudendal artery. (a) CTscan shows a fracture of the right inferior pubic ramus with extravasation of contrast material (arrow) within ahematoma in the ischiorectal fossa. (b) Superselective angiogram obtained with a microcatheter shows activebleeding (solid arrow) from the internal pudendal artery. Note the normal angiographic blush in the perineum(open arrow).
RG f Volume 24 ● Number 6 Yoon et al 1601
Radio
Gra
phic
s
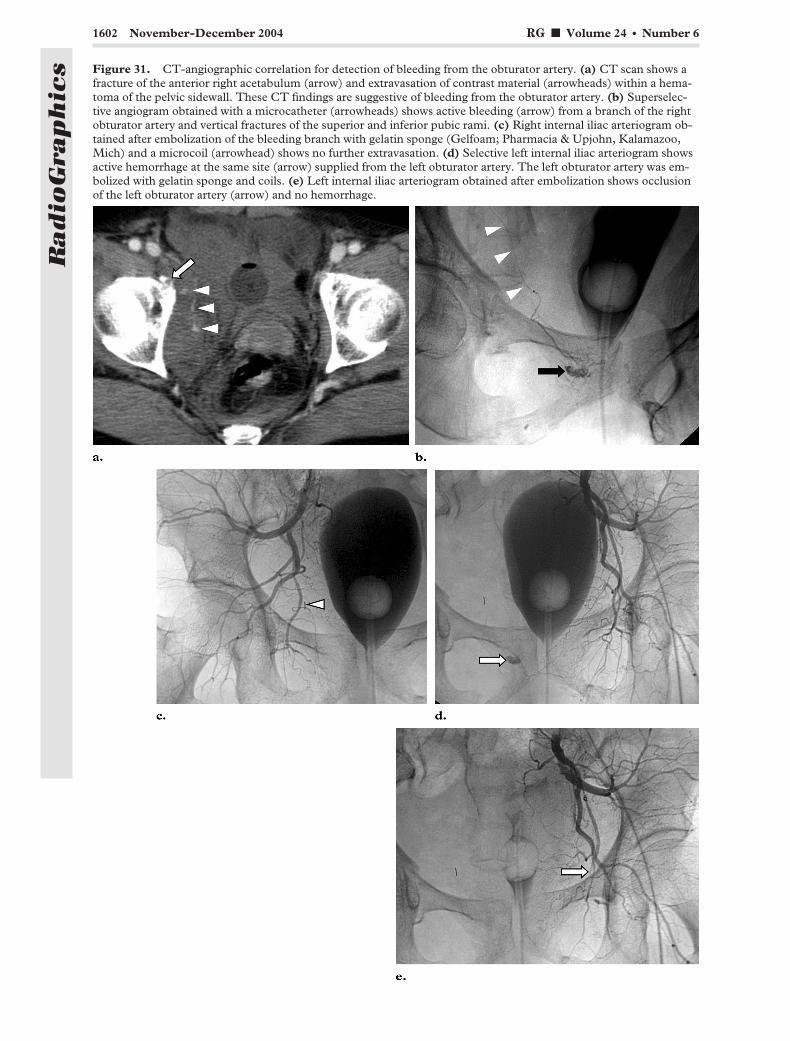
Figure 31. CT-angiographic correlation for detection of bleeding from the obturator artery. (a) CT scan shows afracture of the anterior right acetabulum (arrow) and extravasation of contrast material (arrowheads) within a hema-toma of the pelvic sidewall. These CT findings are suggestive of bleeding from the obturator artery. (b) Superselec-tive angiogram obtained with a microcatheter (arrowheads) shows active bleeding (arrow) from a branch of the rightobturator artery and vertical fractures of the superior and inferior pubic rami. (c) Right internal iliac arteriogram ob-tained after embolization of the bleeding branch with gelatin sponge (Gelfoam; Pharmacia & Upjohn, Kalamazoo,Mich) and a microcoil (arrowhead) shows no further extravasation. (d) Selective left internal iliac arteriogram showsactive hemorrhage at the same site (arrow) supplied from the left obturator artery. The left obturator artery was em-bolized with gelatin sponge and coils. (e) Left internal iliac arteriogram obtained after embolization shows occlusionof the left obturator artery (arrow) and no hemorrhage.
1602 November-December 2004 RG f Volume 24 ● Number 6
Radio
Gra
phic
s

be seen on contrast-enhanced CT scans when thevesical arteries are injured (Fig 32).
Arterial extravasation of contrast materialsmust be distinguished from contrast material thatmay have leaked from the urinary tract (15). Ret-rograde urethrography or cystography should notbe performed before contrast-enhanced CT andangiography in patients with pelvic fractures andhemorrhagic shock because leaked contrast mate-rial obscures the view of the arterial extravasationsites and therefore makes difficult the early diag-nosis and treatment of such critically ill patients(18).
TranscatheterArterial Embolization
Transcatheter arterial embolization (TAE) is nowconsidered to be the treatment of choice in pa-tients with arterial hemorrhage related to pelvicfractures (3,5,10,19). If a patient is hemodynami-cally unstable despite initial resuscitation, urgentarteriography and embolization are recom-mended. In patients who undergo contrast-en-hanced CT, angiographic embolization should beperformed to control potentially life-threateningarterial hemorrhage when contrast material ex-travasation is seen on CT scans.
The efficacy of TAE in the management ofarterial hemorrhage caused by pelvic fractures hasbeen demonstrated. The success rate, expressedin terms of hemorrhage control and reduction intransfusion requirement, ranges from 85% to
100% (3,10,19). TAE should be performed asearly as possible, because effective embolizationmust be achieved before severe systemic coagu-lopathy and multiple organ failure develop (20).Agolini et al (3) reported that the mortality ratewas 14% (1 of 7) in embolized patients who ar-rived in the angiography suite within 3 hours oftheir injury but was 75% (6 of 8) for patients whoarrived after 3 hours. Eastridge et al (8) reportedthat the mortality rate was 25% (1 of 4) in pa-tients with unstable pelvic fracture patterns whounderwent TAE before celiotomy but was 60% (6of 10) for patients who underwent celiotomy be-fore TAE. They concluded that angiographyshould be considered an initial intervention inpatients with unstable pelvic fractures, even in thepresence of hemoperitoneum.
In addition, there are several issues that shouldbe taken into account when performing TAE inpatients with pelvic fracture hemorrhage. Even ifno significant bleeding is seen on the aortogram,selective injection of the internal iliac arteries isnecessary, because the bleeding may be intermit-tent and the characteristics of the arteries thatmay be injured are more evident (Fig 33). It is alsoimportant to selectively study the contralateral inter-nal iliac artery to search for other potential bleedingsites and collateral flow that may contribute to theoriginal bleeding site (19) (Fig 31).
Figure 32. CT-angiographic correlation for detection of bleeding from the vesical artery. (a) CT scan shows asmall focus of extravasated contrast material (arrow) in the wall of the urinary bladder. (b) Aortogram shows activebleeding (arrow) from the left vesical artery.
RG f Volume 24 ● Number 6 Yoon et al 1603
Radio
Gra
phic
s

A capillary and venous phase blush in the regionof the distal branches of the internal pudendal arterythat simulates bleeding can sometimes be seen onarteriograms of male patients who are not bleeding(Fig 30b). This normal variation, which is called the“cavernosal blush,” is characterized by a bilaterallysymmetric, homogeneous stain at the base of thepenis that washes out, and it should not be confusedwith active hemorrhage (21).
In general, patients who need angiographytend to be older, require more transfusion beforeangiography, and have worse injury severityscores than those who do not (4,10). Thus, it isnot surprising that the mortality rate is still high inpatients who undergo angiographic embolization.The mortality rates among patients who undergosuccessful TAE have been reported to be 17.6%–47% (3,5,10).
ConclusionsEvidence of active extravasation of contrast mate-rials on contrast-enhanced CT scans is highlysuggestive of arterial bleeding in patients withpelvic fractures. Contrast-enhanced CT allowsidentification of contrast material extravasations
in locations that are predictive of injuries to spe-cific arterial branches of the internal iliac artery.Thus, CT can guide interventional radiologists inthe selective angiographic investigation and em-bolization of specific injured arteries. This canlead to more rapid transcatheter embolization ofbleeding arteries, which has the potential to re-duce patient morbidity and mortality.
References1. Biffl WL, Smith WR, Moore EE, et al. Evolution of a
multidisciplinary clinical pathway for the manage-ment of unstable patients with pelvic fractures. AnnSurg 2001; 233:843–850.
2. Demetriades D, Karaiskakis M, Toutouzas K, Alo K,Velmahos G, Chan L. Pelvic fractures: epidemiologyand predictors of associated abdominal injuries andoutcomes. J Am Coll Surg 2002; 195:1–10.
3. Agolini SF, Shah K, Jaffe J, et al. Arterial emboliza-tion is a rapid and effective technique for controllingpelvic fracture hemorrhage. J Trauma 1997; 43:395–399.
4. Starr AJ, Griffin DR, Reinert CM, et al. Pelvic ringdisruptions: prediction of associated injuries, transfu-sion requirement, pelvic arteriography, complications,and mortality. J Orthop Trauma 2002; 16:553–561.
5. Hagiwara A, Minakawa K, Fukushima H, Murata A,Masudo H, Shimazaki S. Predictors of death in pa-
Figure 33. Bleeding from the iliolumbarartery detected with selective injection ofthe internal iliac artery. (a) Contrast-en-hanced CT scan shows a fracture and dis-placement of the left ala of the sacrum withextravasation of contrast material (arrows)between the L5 body and fractured sa-crum. (b) Pelvic arteriogram shows nodefinite site of hemorrhage. (c) Selectiveleft internal iliac arteriogram shows activeextravasation (solid arrow) from the ilio-lumbar artery (open arrow). (d) Leftinternal iliac arteriogram obtained afterembolization of the iliolumbar artery withmicrocoils (arrows) shows no furtherhemorrhage.
1604 November-December 2004 RG f Volume 24 ● Number 6
Radio
Gra
phic
s

tients with life-threatening pelvic hemorrhage aftersuccessful transcatheter arterial embolization.J Trauma 2003; 55:696–703.
6. Blackmore CC, Jurkovich GJ, Linnau KF, CummingsP, Hoffer EK, Rivara FP. Assessment of volume ofhemorrhage and outcome from pelvic fracture. ArchSurg 2003; 138:504–509.
7. Miller PR, Moore PS, Mansell E, Meredith JW,Chang MC. External fixation or arteriogram in bleed-ing pelvic fracture: initial therapy guided by markersof arterial hemorrhage. J Trauma 2003; 54:437–443.
8. Eastridge BJ, Starr A, Minei JP, O’Keefe GE. The im-portance of fracture pattern in guiding therapeutic deci-sion-making in patients with hemorrhagic shock andpelvic ring disruptions. J Trauma 2002; 53:446–451.
9. Ben-Menachem Y, Coldwell DM, Young JW, Bur-gess AR. Hemorrhage associated with pelvic frac-tures: causes, diagnosis, and emergent management.AJR Am J Roentgenol 1991; 157:1005–1014.
10. Wong YC, Wang LJ, Ng CJ, Tseng IC, See LC. Mor-tality after successful transcatheter arterial emboliza-tion with unstable pelvic fractures: rate of bloodtransfusion as a predictive factor. J Trauma 2000;49:71–74.
11. Hamill J, Holden A, Paice R, Civil I. Pelvic fracturepattern predicts pelvic arterial haemorrhage. Aust NZ J Surg 2000; 70:338–343.
12. Sheridan MK, Blackmore CC, Linnau KF, HofferEF, Lomoschitz F, Jurkovich GF. Can CT predictthe source of arterial hemorrhage in patients with pel-vic fractures? Emerg Radiol 2002; 9:188–194.
13. Shanmuganathan K, Mirvis SE, Sover ER. Value ofcontrast-enhanced CT in detecting active hemor-
rhage in patients with blunt abdominal or pelvictrauma. AJR Am J Roentgenol 1993; 161:65–69.
14. Cerva DS, Mirvis SE, Shanmuganathan K, Kelly IM,Pais SO. Detection of bleeding in patients with majorpelvic fracture: value of contrast-enhanced CT. AJRAm J Roentgenol 1996; 166:131–135.
15. Stephen DJ, Kreder HJ, Day AC, et al. Early detec-tion of arterial bleeding in acute pelvic trauma.J Trauma 1999; 47:638–642.
16. Pereira SJ, O’Brien DP, Luchette FA, et al. Dynamichelical computed tomography scan accurately detectshemorrhage in patients with pelvic fracture. Surgery2000; 128:678–685.
17. Yiming A, Baque P, Rahili A, et al. Anatomical studyof the blood supply of the coxal bone: radiologicaland clinical application. Surg Radiol Anat 2002; 24:81–86.
18. Coldwell DM. Interventional radiology in the man-agement of pelvic fractures. Semin Intervent Radiol2003; 20:89–95.
19. Velmahos GC, Toutouzas KG, Vassiliu P, et al. Aprospective study on the safety and efficacy of angio-graphic embolization for pelvic and visceral injuries.J Trauma 2002; 52:303–308.
20. Wholey M, Peterson S, Silvestri B. Case 2: pelvicfracture with tear of the left internal pudendal artery.AJR Am J Roentgenol 1998; 171:844, 847, 848.
21. Schrumpf JD, Sommer G, Jacobs RP. Bleeding simu-lated by the distal internal pudendal artery stain. AJRAm J Roentgenol 1978; 131:657–659.
This article meets the criteria for 1.0 category 1 credit toward the AMA Physician’s Recognition Award. To obtaincredit, see www.rsna.org/education/rg_cme.html.
RG f Volume 24 ● Number 6 Yoon et al 1605
Radio
Gra
phic
s
Related Documents











